Human respiratory muscles: fibre morphology and capillary ... · comprise approximately 50%...
15
Eur Aesplr J 1991, 4, 587-601 REVIEW Human respiratory muscles: fibre morphology and capillary supply M. Mizuno Human respiratory muscles: fibre morphology and capillary supply. M. Mizuno. ABSTRACT: In man the diaphragm (DIA) and abdominal muscles comprise approximately 50% slow-twitch (ST) fibres, whereas a higher proportion (60%) is found in intercostal muscles and the scalenes. All respiratory muscles show an equal distribution of fast-twitch (Ffa and b) fibres with the exception of the expiratory Intercostal muscles which have few Ffb fibres. The inspiratory muscles have a uniformly small fibre size, in contrast to the expiratory intercostal muscle fibres which are large. The fibre size of the inspiratory muscles Is maintained with ageing, whereas that of the expiratory Intercostal muscles appears to be reduced after the age of 50 yrs. Capillary supply Is most abundant in the expiratory muscles followed by DIA and the inspiratory intercostal muscles. In patients with chronic obstructive pulmonary disease (COPD) it is unknown whether a reduction in fibre size of the thoracic respiratory muscles is caused by extreme use due to increased ventilatory work, or by disuse due to an increased Involve- ment of the extrathoracic respiratory muscles. Histochemical character· istlcs suggest that, in normal humans, the load on the inspiratory muscles is relatively small during contractions, whereas the expiratory intercostal muscles are exposed to severe continuous activity with a heavy load. Eur Respir ]., 1991, 4, 587-601. Skeletal muscles possess a large plasticity to altered pattern of use. The same muscle adapts differently to recruitment for either short intense or prolonged activity with low or high force development [1). Structural and metabolic characteristics of muscle fibres will therefore depend on a combination of the pattern and workload in which the muscle is engaged. Dept of Anaesthesia, Rigshospitalet and August Krogh Institute, University of Copenhagen, DK-2100 Copenhagen 0, Denmark. Correspondence: M. Mizuno, Dept of Biochemistry A, Panum Institute, University of Copenhagen, Blegdamsvej 3C, DK-2200 Copenhagen N, Denmark. Keywords: Ageing; chronic obstructive pulmonary disease; diaphragm; intercostal muscles; muscle capillaries; muscle fibre types. Received: March 27, 1990; accepted after revision November 20, 1990. Supported by the Danish Medical Research Council (12·8198), the Danish National Association against Pulmonary Disease, Organon, Denmark and Simonsen & Weel's Foundation. Poatarlor The respiratory muscles provide the pump for venti- lation. To move and/or to stabilize the rib cage the respiratory muscles have to overcome a certain resist- ance to contractions. During quiet breathing inspiration is associated with electromyographic (EMG) activity from the diaphragm, scalenes, sternomastoid, internal intercostal muscles (INT) of the parasternal region and external intercostal muscles (EXT) of the posterior part [2-6] (fig. 1). During expiration EMG activity is lim- ited to the lateral INT. Accordingly, studies have focused on inspiratory muscles [5, 6, 8-10] and regimes have been provided for training inspiratory rather than expiratory muscles [11-15]. Mid-ex llary llneMid-clavlcular line In addition to ventilation, the respiratory muscles play a role during coughing, talking and singing where the expiratory muscles, e.g. the lateral INT and the abdominal muscles, would be considered to contribute significantly (4]. Also, the expiratory muscles dominate the contribution of the respiratory muscles to postural Fig. 1. - Schematic illustration demonstrating intercostal regions where electromyographic activity is recorded during breathing at rest (hatched area for expiration; crossed area for inspiration). The locations of sampling sites for external (EXT) and internal (INT) intercostal muscles as well as for the costal diaphragm (DIA) are marked. Q: inspiratory muscles; 0 : expiratory muscles. Adapted from MIZUNO and SECHER [1) .
Transcript of Human respiratory muscles: fibre morphology and capillary ... · comprise approximately 50%...

Eur Aesplr J 1991, 4, 587-601
REVIEW
Human respiratory muscles: fibre morphology and capillary supply
M. Mizuno
Human respiratory muscles: fibre morphology and capillary supply. M. Mizuno. ABSTRACT: In man the diaphragm (DIA) and abdominal muscles comprise approximately 50% slow-twitch (ST) fibres, whereas a higher proportion (60%) is found in intercostal muscles and the scalenes. All respiratory muscles show an equal distribution of fast-twitch (Ffa and b) fibres with the exception of the expiratory Intercostal muscles which have few Ffb fibres. The inspiratory muscles have a uniformly small fibre size, in contrast to the expiratory intercostal muscle fibres which are large. The fibre size of the inspiratory muscles Is maintained with ageing, whereas that of the expiratory Intercostal muscles appears to be reduced after the age of 50 yrs. Capillary supply Is most abundant in the expiratory muscles followed by DIA and the inspiratory intercostal muscles. In patients with chronic obstructive pulmonary disease (COPD) it is unknown whether a reduction in fibre size of the thoracic respiratory muscles is caused by extreme use due to increased ventilatory work, or by disuse due to an increased Involvement of the extrathoracic respiratory muscles. Histochemical character· istlcs suggest that, in normal humans, the load on the inspiratory muscles is relatively small during contractions, whereas the expiratory intercostal muscles are exposed to severe continuous activity with a heavy load. Eur Respir ]., 1991, 4, 587-601.
Skeletal muscles possess a large plasticity to altered pattern of use. The same muscle adapts differently to recruitment for either short intense or prolonged activity with low or high force development [1). Structural and metabolic characteristics of muscle fibres will therefore depend on a combination of the pattern and workload in which the muscle is engaged.
Dept of Anaesthesia, Rigshospitalet and August Krogh Institute, University of Copenhagen, DK-2100 Copenhagen 0, Denmark.
Correspondence: M. Mizuno, Dept of Biochemistry A, Panum Institute, University of Copenhagen, Blegdamsvej 3C, DK-2200 Copenhagen N, Denmark.
Keywords: Ageing; chronic obstructive pulmonary disease; diaphragm; intercostal muscles; muscle capillaries; muscle fibre types.
Received: March 27, 1990; accepted after revision November 20, 1990.
Supported by the Danish Medical Research Council (12·8198), the Danish National Association against Pulmonary Disease, Organon, Denmark and Simonsen & Weel's Foundation.
Poatarlor
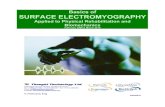
The respiratory muscles provide the pump for ventilation. To move and/or to stabilize the rib cage the respiratory muscles have to overcome a certain resistance to contractions. During quiet breathing inspiration is associated with electromyographic (EMG) activity from the diaphragm, scalenes, sternomastoid, internal intercostal muscles (INT) of the parasternal region and external intercostal muscles (EXT) of the posterior part [2-6] (fig. 1). During expiration EMG activity is limited to the lateral INT. Accordingly, studies have focused on inspiratory muscles [5, 6, 8-10] and regimes have been provided for training inspiratory rather than expiratory muscles [11-15].
Mid-ex llary llneMid-clavlcular line
In addition to ventilation, the respiratory muscles play a role during coughing, talking and singing where the expiratory muscles, e.g. the lateral INT and the abdominal muscles, would be considered to contribute significantly (4]. Also, the expiratory muscles dominate the contribution of the respiratory muscles to postural
Fig. 1. - Schematic illustration demonstrating intercostal regions where electromyographic activity is recorded during breathing at rest (hatched area for expiration; crossed area for inspiration). The locations of sampling sites for external (EXT) and internal (INT) intercostal muscles as well as for the costal diaphragm (DIA) are marked. Q: inspiratory muscles; 0 : expiratory muscles. Adapted from MIZUNO and SECHER [1).

588 M. MIZUNO
support during rotation of the trunk as well as during lifting, carrying and reaching in performing a Valsalvalike manoeuvre. Furthermore, during forced expiration, as in ventilation during intense exercise, and notably in patients with asthma, the expiratory muscles are of utmost importance.
The respiratory muscles may be impaired or severely taxed in several disease and clinical states. In patients with chronic obstructive pulmonary disease (COPD), or with other lung disease, the ventilatory load is increased and respiratory muscle fatigue may develop [16]. In patients with muscle dystrophy or with postoperative partial curarization, weakness of respiratory muscles may cause an inadequate alveolar gas exchange [17].
In previous reviews on respiratory muscles, functional rather than morphological aspects have been emphasized [4-6, 8-10]. In this review the histochemical fibre morphology, capillary supply and biochemical observations on the inspiratory and expiratory muscles are described and compared with data from limb skeletal muscles. Adaptive responses of respiratory muscle morphology to inspiratory and expiratory function as well as to ageing are discussed. In addition, the effects of neuromuscular blocking agents on the respiratory muscle are summarized.
Classification of skeletal muscle fibres
With the use of histochemical staining for myofibrillar adenosine triphosphatase (ATPase) [18], two major fibre types have been classified as type I and type II, respectively [19]. Because a direct coupling exists between contraction speed and ATPase activity [20], it is more descriptive to call them slow- (ST) and fasttwitch (FT) fibres [21). Although a large proportion of muscle fibres show a coexistence of ST and FT myosin heavy chain isoforms [22), those fibres histochemically classified as ST contract slower than FT fibres [23-25). FT fibres can be further subdivided into FTa or FTb, identified following preincubations at different pH values [26) (fig. 2, left panels). ST fibres fatigue less during repetitive contractions than FTb fibres, whereas FTa fibres are able to maintain tension similar to ST fibres (24).
ST fibres are surrounded by a slightly larger number of capillaries (4-5) than FTa and FTb fibres (2-4) (fig. 2, middle right panel). Accordingly, ST fibres possess high mitchondrial and low glycolytic enzyme activity represented by, e.g. nicotinamide adenine dinucleotide tetrazolium reductase (NADH-TR, fig. 2, upper right panel) and alpha-glycerophosphate dehydrogenase (a-GPD, fig. 2, lower right panel), respectively. In contrast, the reverse is true for FTb fibres. Metabolic characteristics of FTa fibres resemble those of the ST fibres [1]. Although the metabolic profile has been used to classify muscle fibres, the use of A TPase staining has been most widely accepted. One of the reasons for this is that there is not a complete coupling between fibre classification based on histochemical
~a FTb ST
Fig. 2. - Photomicrograpbs of serial transverse sections from human vastus lateralis muscle incubated for myofibrillar ATPase activity with preincubations at different pH indicated (left panels), for NADH-TR activity (mitochondrial enzyme, upper right panel), for capillaries with the amylase-PAS method (middle right panel) and for a-GPD activity (glycolytic enzyme, lower right panel). Ff: fast-twitch; ST: slow-twitch; NADH-TR: nicotinamide adenine dinucleotide tetra~olium reductase; a-GPD: alpha-glycerophosphate dehydrogenase; ATPase: adenosine triphosphatase; CAP: capillaries.
staining for metabolic enzymes and for myofibrillar ATPase, in particular, among subgroups of FT fibres (27). Furthermore, at postmortem, metabolic enzyme activities decrease more rapidly than ATPase activity (28, 29).
As may be expected, skeletal muscles such as antigravity muscles comprise a larger proportion of ST fibres when compared with muscles recruited less during daily life (30, 31). Successful endurance athletes possess a dominance of ST fibres (and few FTb fibres) in their leg muscles, while a high proportion of FT fibres is found in elite sprinters [1). These findings are probably dominated by genetic factors (32]. However, following endurance training a conversion of myosin heavy chain isoforms is noted towards ST fibres [33-35]. Endurance training alters FTb fibres in the direction of FTa fibres (36, 37) and may also partly be responsible for the dominance of ST fibres in endurance trained athletes. In contrast, no significant change in fibre type proportion has been observed following strength training (38, 39) (table 1).
Skeletal muscle adapts differently to recruitment depending on the pattern of activity. Endurance training causes relatively less increase in muscle mass than strength training. Muscle hypertroph y following

INSPIRATORY AND EXPIRATORY MUSCLES 589
Table 1. - Fibre morphology and capillary supply in human skeletal muscles
Fibre type Mean Cap. Fibre Fibre distribution fibre per area per circumf.
% area fibre cap. per cap.
Subjects ST FT a FTb ~m~ n !liD~ 1-lffi Ref.
Vastus lateralis muscle
Untrained 40 32 28 4900 1.8 990 55 [7} Endurance
trained• 66 32 2 4700 2.6 710 38 (37] Strength
trained 48 30 22 8700 2.1 1300 [38] [39]
Triceps branchii muscle
Untrained 42 58 .. 5000 1.9 990 [40] Endurance
trained 44 55 1 6900 3.1 820 38 (37] Strength
trained 49 51°* 11000 2.5 1740 (41]
•: data obtained from gastrocnemius muscles; ••: no sub-classification of FT fibres performed; ST: slow-twitch; FT: fast-twitch.
training is probably due to an increase in the size of individual muscle fibres (table 1) rather than in the total number of fibres. "Fibre-splitting" may account for only a marginal increase in muscle volume [42), or alternatively, represent muscle fibre damage [43). Capillary supply in muscle fibres increases more with endurance than strength training (table 1).
Histochemical profile of human respiratory muscles
The diaphragm
Autopsy materials. In contrast to biopsies from limb skeletal muscles, which have been obtained largely by the needle technique [1, 44), samples from respiratory muscles have most often been acquired during thoracotomy and autopsy. From postmortem studies, where diaphragm muscle biopsies were obtained from previously healthy individuals who had suffered a sudden accidental death, the mean relative occurrence of ST fibres is approximately 50% [7, 45] (table 2). The remaining proportion is evenly divided into FT a (25%) and Ffb fibres (25%). Thus, fibre type distribution of the diaphragm resembles the pattern existing in limb skeletal muscles of untrained subjects (table 1).
A comparison of the size of individual muscle fibres between the diaphragm and limb skeletal muscles is complicated by the use of two different methods. In order to reduce errors resulting from measurements of obliquely sectioned fibres [53), muscle fibre size of the diaphragm has been frequently expressed as "the least (lesser) diameter" [47-49, 51, 52]. However, determinations based on measurements of cross-sectional area by planimetry are more accurate because a curvilinear relationship exists between fibre cross-sectional
area and least fibre diameter (fig. 3) [40, 50] . Furthermore, an implicit assumption of the least diameter method is that cross-sections of muscle fibres are circular, whereas either a pentagonal or hexagonal shape is more accurate (fig. 2) [7, 50). Thus, the crosssectional area of muscle fibres will be constantly underestimated with the use of the least diameter.
The average fibre size of the costal diaphragm determined using the cross-sectional area is 2,200 ~-tm2 in normal subjects [7, 45] (table 3). ST fibres (800 ~-tm2) are slightly larger than both FTa (2,200 ~-tm2) and Ffb fibres (1,800 ~-tm2). Thus, the size of diaphragmatic muscle fibres is relatively small as compared with that of limb skeletal muscles (table 1).
The mean number of capillaries per fibre determined in the costal diaphragm is 1.9 (1.5-2.4) [7). ST fibres are surrounded by 4--6 capillaries, whereas slightly less (3-5) are found around FTa and Ffb fibres. These values are similar to those reported for limb skeletal muscles of untrained individuals. However, the calculated values for the fibre area surrounded by each capillary are smaller in the diaphragm (table 4) than in leg or arm muscles (table 1) [7].
The reason for taking the cross-sectional area of muscle fibres into account when expressing capillary supply is that this inde:x may serve as an indicator for diffusing distance between the capillary and muscle fibres. According to tlie Krogh concept, capillaries in skeletal muscles are assumed to serve a certain cylinder of tissue [55), and thereby indices based on capillaries pet mm2 of tissue area or conversely tissue area per capillary have been used [1, 36). Justification for these indices is the finding that the index for capillary supply related to fibre area has been shown to be closely linked to the oxidative potential of muscle fibres and also to aerobic work capacity [1, 56].

590 M. MlZUNO
Table 2. - Fibre type distribution of human respiratory muscles
Subjects Inspiratory Expiratory
Diaphragm Intercostal muscles
n Age External Internal Ref.
Costal% Lateral% Parasternal % Lateral %
MIF yrs ST Ffa Fib ST Ffa Fib ST Ffa Fib ST Ffa Fib
Postmortem 4/3 2-59 54 46 69 31 62 38 [46) 3/2 17-72 50 21 26 52 25 21 [45) 8/0 17-51 49 28 23 62 14 24 61 27 12 64 35 1 [7)
Thoracotomy
8 65 35 [25] 4/4 <60 57 43 [47]
N 7 30-72 55 21 24 [45] N 8 54 53 47 63 37 60 40 [48) N 10 47 53 47 [49) N 5/1 28-67 59 14 27 64 36 0 [50]
COPD 18 47 57 43 62 38 62 38 [48) COPD 8 55 53 47 [49) COPD 22 24-77 48 52 48 52 [51) COPD 17-39 60 47 53 47 53 . 47 53 (52)
N: Normal ventilatory capacity; COPD: chronic obstructive pulmonary disease; ST: slow-twitch; Ff: fast-twitch.
Fibre area x1o2 1-1m2
80
60
40
20
30 40 50 60 70 80 1-1m
L.eeaer diameter
Fig. 3. - Relationship between lesser diameter and cross-sectional area of the fibre types determined by planimetry in external and internal intercostal muscles laterally placed. External intercostal muscles: e: ST; 0: FTa; t.: FTb. Internal intercostal muscles: • : ST; Q: FTa. ST: slow-twitch; FT: fast·twitch. Adapted from MIZ\JNO
et al. [SO].
Patients. The mean relative occurrence of ST (54%), FT a (21%) and Fib fibres (21%) of the diaphragm in patients with normal ventilatory function and with COPD is the same as in autopr.y materials (table 2) [48, 49, 52, 57). Regional distribution of fibre types in the diaphragm
has been studied showing no difference between the crural and costal parts [49]. However, the costal part possesses a 15% larger diameter of muscle fibres than the crural part, and this finding applies to patients with normal ventilatory function as well as those with COPD [49).
In postmortem studies of COPD patients measurements of the total size of the diaphragm have revealed conflicting results indicating both hypertrophy [58, 59) and atrophy [60). Muscle atrophy has been attributed to an impaired use of the diaphragm as seen on radiography [61). A small muscle mass of the diaphragm in COPD is related to low body weight of the patients [62, 63) . Consequently, the increased ventilatory work in COPD is not reflected by an in· crease in muscle fibre size of the diaphragm. On the contrary, a 16% reduction in the least diameter of diaphragmatic muscle fibres has been found, and this reduction in fibre size is present in both ST (15%) and FT fibres (18%) (48, 49). The small muscle fibre size of the diaphragm in COPD patients may indicate over-use atrophy as observed in limb skeletal muscle of extremely endurance-trained athletes (64). However, at present, this aspect is debated, since values are not available on either subgroups of FT fibres or capillary supply in the diaphragm of COPD patients. Furthermore, the effect of COPD on the diaphragm is probably more complicated than disuse or over-use atrophy, because COPD patients have generalized muscle weakness to which d ifferent factors contribute [16).

INSPIRATORY AND EXPIRATORY MUSCLES 591
Table 3. - Fibre size of human respiratory muscles
Subjects Inspiratory Expiratory
Diaphragm Intercostal muscles
n Age External Internal Ref.
Costal% Lateral% Parasternal % Lateral %
M/F yrs ST Ffa Ffb ST Ffa Ffb ST Ffa Ffb ST Ffa Ffb
Fibre cross-sectional area 1-1m2
Postmortem 3/2 17-72 2640 1960 1520 2830 2060 1810 (45] 8/0 17-51 2320 2350 2120 2790 3350 2980 2600 3350 3000 3680 5360 (7]
Thoracotomy N 5/1 28-67 2720 2760 2820 2840 4560 - [50]
Fibre diameter 1-1m
Thoracotomy 4/4 <60 49 50 (47]
N 8 54 62 59 48 47 48 47 (48] N 10 47 60 55 (49] N 5/1 28-67 45 44 45 45 57 (50]
COPD 18 47 50 47 47 46 49 56 (48] COPD 8 55 54 47 (49] COPD 22 24- 77 so 41 49 40 (54] COPD 17- 39 60 48 40 44 44 42 41 (52]
N: normal ventilatory function; COPD: chronic obstrucitve pulmonary disease; ST: slow-twitch; Ff: fast-twitch .
Relation to ventilatory function. Although fibre type distribution and the number of capillaries in the diaphragm are similar to those obtained from limb skeletal muscles of untrained individuals, the lower diffusing distance, indicating a greater oxidative potential, represents an adaptive response to the constant use of the diaphragm during ventilation.
A regional difference in muscle fibre size indicates an adaptive response to different function. The costal parts of the diaphragm have inspiratory functions not only to lower the central aponeurosis but also to expand the lower rib cage [65, 66]. This finding may imply that the costal part carries relatively larger loads during contractions. Indirect evidence is a positive correlation between forced vital capacity (FVC) or forced expiratory volume in one second (FEV ) and muscle fibre size of the costal diaphragm [49j. However, such a correlation has not be established for muscle fibres of the crural diaphragm [ 49] or for the inspiratory intercostal muscles [50-52].
Intercostal muscles
Autopsy materials. Because of the inspiratory function of the EXT, and the expiratory role of the lateral INT (fig. 1), morphological characteristics of these two muscle layers are considered to be different. Further-
more, the functional difference between the inspiratory parasternal INT and the expiratory lateral INT may induce similar histochemical differences. Indeed it has been shown that fibre morphology and capillary supply of intercostal muscles are bound to functional differences rather than to anatomical classification as EXT or INT [7].
The relative occurrence of ST fibres is the same for all the investigated intercostal muscles (62% ), while the expiratory INT have more FTa fibres (35%) than the inspiratory INT and EXT (22%) (fig. 1 and table 2) [7, 45]. Accordingly, the expiratory INT have far fewer Fib fibres (1 %) than the inspiratory intercostal muscles (19%) (fig. 4). Thus, fibre type distribution of the inspiratory intercostal muscles is similar to that of limb skeletal muscles in non-athletes, whereas the almost complete lack of Fib fibres in the expiratory INT makes them resemble, and even exceed, fibre type distribution of muscles from extremely well-trained athletes in endurance events (table 1). Both the inspiratory and expiratory intercostal muscles have at least 10% more ST fibres than the diaphragm and most other skeletal muscles [1]. The absence of FTb fibres in the expiratory INT together with a proportion of ST fibres similar to the inspiratory INT and EXT suggests independent control of factors governing fibre type expression according to the two major types (ST vs FT) and the subgroups of FT fibres (FT a vs FTb ). Of note is the

592 M. MIZUNO
Table 4. - Diffusing distance between capillaries and muscle fibres
Inspiratory Expiratory
Diaphragm Intercostal muscles
External Internal
Costal Lateral Parasternal Lateral
Fibre area per capillary ~-tm2
Postmortem (7)
ST 450:t30 630:t40 Ffa 520:40 790:t80 Ffb 540:40 750:t80
Thoracotomy [50)
ST 620:t40 Ffa 740:t70 Ffb 890:t70
570:50 680:t20 700±50 940:t40 790:t80
560:40 940:tl20
Fibre circumference per capillary ~-tm
Postmortem (7)
ST 37±1 48:t2 Ffa 43:t2 55:t3 Ffb 45:t2 57:t3
Thoracotomy (50)
ST 45:t2 Ffa 55:t4 Ffb 67±4
ST: slow-twitch; Ff: fast-twitch.
43:t2 42:tl 49:t3 47:t2 57:t2
39:2 52:3
finding that the range of relative occurrence of ST fibres is less in the intercostal muscles (55-80%) than in vastus lateralis muscles (10-70%) [7). A narrow range of the ST fibre proportion has been suggested to occur as an adaptive response to an increased use of leg muscles [67].
The mean cross-sectional area for the expiratory INT is large ( 4,300 f..lm2) as compared with the inspiratory INT and EXT (2,900 J.tm2
) (table 3). The inspiratory intercostal muscles show no significant difference in the cross-sectional area between sample sites (7] and have a similar value to the diaphragm (table 3). The larger fibre area of the expiratory INT is reflected by a greater area for both ST (3, 700 j.tm2
) and FT a fibres (5,400 14m2) [7). Thus, the expiratory INT have large muscle fibres, and FTa fibres are the largest. This result is in contrast to the inspiratory intercostal muscles in which a similar area is seen among the different fibre types.
The expiratory INT have a greater number of capillaries per fibre (2.3) than the inspiratory INT and EXT (1.6). Accordingly, more capillaries are found around both ST and FTa fibres (5-6) than in the inspiratory intercostal muscles ( 4-5). These differences are further emphasized by the finding that the expiratory INT in the eighth intercostal space, which are the most active for expiration during normal breathing as well as non-ventilatory tasks [2, 3, 68-71 ], show the fewest F1b fibres (0.3%) and the largest fibre area (4,000 J.tm2 for ST and 5,900 J.tm2 for FTa fibres) supplied by the highest number of capillaries (2.4 capillaries per fibre) among the investigated intercostal muscles [7].
50 pm
Fig. 4. - Photomicrographs of serial transverse sections from the inspiratory external (left panels) and the expiratory internal intercostal muscle (right panels) obtained from the 5th intercostal space in the mid-axillary line and incubated for myofibrillar ATPase activity with preincubations at pH 4.6 (upper panels) and pH 4.3 (lower panels). Three fibre types are observed in the external intercostal muscles, whereas only ST and FTa fibres are distinguished in the internal intercostal muscles. For abbreviations see legend to figure 2.

INSPIRATORY AND EXPIRATORY MUSCLES 593
When diffusing distance is expressed as fibre area per capillary, the large fibres of the expiratory EXT (table 3) have the largest area per capillary and thus the longest diffusion distance among all the respiratory muscles studied [7] (table 4). However, for a muscle containing large fibres induced by increased use, the area per capillary ratio may not be an appropriate index for diffusing distance. It is evident in electron-microscopic characteristics of human limb skeletal muscles that the predominant location of mitochondria is underneath the sarcolemma. Furthermore, a pronounced increase in mitochondrial volume under the surface is observed for both ST and FT fibres following endurance training [72, 73). When the intracellular localization of mito- chondria is considered with the use of fibre circumference per capillary, the large fibres of the expiratory INT show a value similar to the inspiratory INT and EXT as well as the diaphragm [7] (table 4). Furthermore, all respiratory muscles show the lowest value for ST fibres (37-48 14m) with slightly higher values for FT a fibres ( 43-55 14m) and the highest value for Frb fibres (45-67 !!ffi). This order of diffusing distance is constant with that of oxidative potential such as mitochondrial enzyme activities which are highest in ST, intermediate in FTa and lowest in Frb [1). Thus, the circumference per capillary index may be of value to describe the diffusing distance, in particular for muscles generating relatively high tension during repetitive contractions as suggested in limb skeletal muscles [45]. In the respiratory muscles this is the case for the expiratory INT.
Patients. Results from patients with normal ventilatory function or with COPD are consistent with the histochemical profile of intercostal muscles obtained from autopsy of normal humans. Thus, the relative occurrence of ST fibres is the same (62%, table 2) [25, 47, 48, 50]. Some patients with COPD have a slightly lower value for ST fibre proportion ( 49% ), and this applies for both the inspiratory EXT and expiratory INT [51, 52]. The difference in relative occurrence of FTa and FTb fibres between the inspiratory intercostal muscles and the expiratory INT in normal subjects is represented in patients as well [50].
A second similarity among patients and normal subjects is the relative size of FTa fibres which are larger in the expiratory INT than in the inspiratory EXT, expressed as the cross-sectional area [50) (table 3). SANcHEZ et al. [48] did not observe such a difference in muscle fibre size expressed by the least diameter. Since a curvilinear relationship exists between the crosssectional area and the least diameter of muscle fibres (fig. 3), the difference in fibre size between inspiratory and expiratory intercostal muscles may have been too small to be detected by the use of the least diameter. Like the diaphragm, however, patients with COPD have a 15% reduction in the least diameter of FT fibres of the expiratory INT [51, 52]. On the contrary, this reduction is not observed in the inspiratory EXT [51).
Thirdly, when capillary supply is considered, the highest values are observed for the expiratory INT in patients with normal ventilatory function [50]. Thus,
the number of capillaries per fibre and surrounding each fibre are 1.6 and 5 for the expiratory INT and 1.3 and 4 for the inspiratory EXT. These values for capillary supply are 20-30% lower than values observed in normal subjects. The area index for diffusing distance is greater in the expiratory INT than in the inspiratory EXT, whereas a similar value for the circumference index is observed among these two muscle groups in patients undergoing thoracotomy (table 4). The values for both indices are similar among normal subjects and patients with normal ventilatory function. No data on capillary supply in intercostal muscles are available for COPD patients.
FTb
Relative fibre type r.
dletrlbullon ~
Expiratory lntercottal
lnaplratory Cotter mute!.. diaphragm
6 0 <)
M. vaatua leterelle
Fig. 5. - Schematic illustration of findings in expiratory and inspiratory intercostal muscles, the costal diaphragm and m. vastus lateralis of normal subjects (MIZUNO and SECHER [7]. Relative fibre cross-sectional area and the number of capillaries are indicated. Relative fibre type distribution; e: ST; 0: FTa;O: FTb. ST: slow· twitch; FT: fast-twtich.
Relation to ventilatory function. A lack of FTb fibres, muscle fibre hypertrophy and capillary proliferation in the expiratory INT (fig. 5) indicates that these muscles are intensively recruited with relatively large force development during repeated contractions. One explanation for the apparent intense use of the expiratory INT is that their relative small mass is recruited extensively even during quiet breathing. In contrast, inspiration is shared among the diaphragm, parasternal INT, EXT, scalene and sternomastoid muscles [2, 3, 71, 74-78]. Thus, it is likely that the inspiratory muscles are loaded below training stress, while the expiratory INT are overloaded routinely. This aspect on the expiratory INT is further confirmed with the observation that a positive correlation between forced expiratory function (FVC, FEY) or maximal ventilatory volume (MVV) and fibre size of the expiratory INT is found in patients, including those with COPD [48, 50-52).
In dogs sonomicrometric measurements of muscle length during spontaneous breathing have suggested that the lateral INT and EXT are antagonistic to rotation of the trunk rather than to moderate ventilatory efforts [79).

594 M. MIZUNO
However, postural function alone does not explain the distinct histochemical characteristics of the expiratory INT, because the abundant, large and capillary rich FTa fibres are found only in humans and not in rats [46, 80], cats [81, 82), dogs [83] or baboons [84]. Thus, despite the correlation found between ventilatory function and fibre size of the expiratory INT, their apparent histochemical characteristics may reflect an adaptive response to non-ventilatory tasks such as vocalization and upright posture in performing Valsalva-like manoeuvres during lifting, carrying and reaching.
Extrathoracic muscles
The relative occurrence of ST (59%), FTa (22%) and FTh (17%) fibres in the scalene muscles of autopsy materials is similar to that reported for the inspiratory intercostal muscles [ 45]. The proportion of ST fibres exceeds that found in most of the skeletal muscles including the diaphragm (tables 1 and 2). The fibre cross-sectional area of the scalenes (1,900 ~m2) is smaller than that reported for the other inspiratory muscles [45]. This difference is reflected by a smaller cross-sectional area of FTa (1,500 ~m2) and FTb fibres (1,200 ~m2), whereas the ST fibres (2,300 ~m2) have a similar area to that of the other inspiratory muscles (table 3). Thus, ST fibres are larger than FT fibres in the scalenes, as also found in the diaphragm.
In patients with COPD intense EMG activity is recorded in the scalenes and hypertrophy is visually recognized (85], suggesting that these muscles are involved increasingly during normal breathing. The increased work of the scaleoes in severe COPD probably reflects the impaired function of the diaphragm due to its lower position caused by emphysema.
The sternomastoid muscles have a smaller proportion of ST fibres (35%) than other respiratory muscles [86]. Explanation of this finding, as well as information on the proportion of subgroups of FT fibres is lacking. The size of muscle fibres in patients with COPD is smaller than in normal subjects [87).
The expiratory extrathoracic muscles, the abdominal muscles including the rectus and transverse as well as the external and internal oblique, have 54% ST fibres in normal humans [86] and in patients undergoing abdominal surgery [88]. In these patients FTa (20%) and FTb fibres (23%) are evenly distributed. The fibre size, expressed as the mean least diameter, is similar among the abdominal muscles and among three fibre types (52 ~m) with the exception of FTa fibres (45 ~m) in the transverse abdominal muscle, which are smaller [88]. These values are within the range determined in other respiratory muscles (table 3). As noticed for the scalene muscles, patients with severe COPD use the abdominal muscles extensively during breathing [89, 90]. However, the fibre size of abdominal muscles in COPD patients has not been reported.
Relative occurrence of ST fibres %
100
80
60
40
20
0 ~~~~~·-r-r~~~~~--·· 24-37 1-4 1-3 7-24 ..___. ~
Weeks Months I
Unborns Infants
20 40 60
Age yrs
Fig. 6. -The relative occurrence of ST fibres determined in expiratory internal (lNT), inspiratory external intercostal muscles (EXT) and the costal diaphragm (DIA) in relation to age. •· Q, eg from KEENS et al. (91); e, 0, ®from MIZUNO and SECKER (7) and MIZUNO et al. [50]; ! from SANcKEz et al. [48, 49] and~ from LlEBERMAN et al. [57]. The values from autopsy materials and patients with normal ventilatory capacity are plotted as mean±sD .• e .6: INT; Q 0 6: EXT; eg ® 4 ~: DIA; ST: slow-twitch.
60
40
20
Mean fibre croea-aectlonal area, :~e102 14m2
+ + r 2o
+ + ~
40 60 Age yra
Fig. 7. - Mean fibre cross-sectional area of expiratory internal (INT), inspiratory external intercostal mus~les (EXT) and the costal diaphragm (DIA) in relation to age. The values are pooled data from M1ZUNO and S.ECKER [7] and MIZUNO et al. (50], and expressed as mean±sn. The number of observations is 6 for 24 yrs. 5 for 47 yrs and 3 for 65 yrs. Among INT the value for 65 yrs is significantly lower than those for the other two groups (•p<0.05). e: INT; 0: EXT; ®: DIA.
Histochemical changes with ageing
In the diaphragm and inspiratory as well as in expiratory intercostal muscles, fibre type differentiation is completed by the age of two years [91, 92). Thereafter,

INSPIRATORY AND EXPIRATORY MUSCLES 595
Table 5. - Enzyme activities of human respiratory muscles
Subjects Muscles Phosphorylase Hexokinase Lactate Succinic Citrate 3-hydroxyacyl- Ref. 0 Age dehydro- dehydro- synthase coenzyme A MIF yrs geoase genase dehydrogenase
Normal ventilatory function
10 50 DIA 6.7:0.6 1060:110 34:3 59:3 [102] 5/1 28-67 EXT 42 (26-52) 8.1 (6.1-9.7) 29 (22-40) 29 (20- 38) [50] 9 53 EXT 6.1 (5.6-6.6) 1160 (90Q-1500) 30 (26-33) 41 (35-48) (103] 5!1 28-67 INT 44 (21-60) 7.8 (6.8-8.5) 26 (21- 33) 26 (20- 35) (50] 9 53 INT 6.1 (5.6-6.6) 1160 (1000-1400) 26 (22-31) 35 (30-42) (103)
Chronic obstructive pulmonary disease
11 8 DIA 4.8:t0.6 630:70 32:3 50:5 (102] 22 24-77 EXT 39:5 (51] 11 52 EXT 6.7 (6.0-7.3) 980 (80Q-1100) 38 (33-47) 54 (45- 67) (103] 22 24-77 INT 37:4 (51] 11 52 INT 6.9 (6.2-8.0) 970 (70Q-1200) 34 (28-39) 47 (41- 55) (103]
DIA: costal diaphragm; EXT: external intercostal muscles; INT: internal intercostal muscles. Enzyme activities are expressed as j.lmol·min·1·g·1 dry weight of protein determined at 25°C. Values are means:tSEM or with a range in parenthesis.
Table 6. - Substrata concentrations of human respiratory muscles
Subjects Muscles ATP PCr Glycogen Lactate Ref. n Age MIF yrs
Normal ventilatory function
4/8 48-78 EXT 13:1 48:t2 191:9 6:t2 (54] 511 28-67 EXT 277 (158-362) 20 (11-33) [108]
INT 380 (221-575) 18 (9-26) (108)
Chronic obstructive pulmonary disease
10/2 46-75 EXT 10:2 46:5 204:30 12:2 (54] 22 24-77 EXT 19:1 70:t3 250:t16 lO:tl [51]
INT 19:t1 69:t3 310:t25 10:t2 (51] 15-40 60 EXT 19 65 255 10 [52]
INT 19 63 302 10 [52] DIA 20 55 315 10 [52]
Substrate concentrations are expressed as ~-tmol·g·' dry weight. Values are means:seM or with a range in parenthesis. EXT: external intercostal muscles; INT: internal intercostal muscles; DIA: diaphragm; ATJ>: adenosine triphosphate; PCr: phospho-creatine.
the relative occurrence of ST fibres remains constant (fig. 6), as has been observed in limb skeletal muscles [93-96). A lower proportion of ST fibres. in the diaphragm than in intercostal muscles appears to exist at all ages (fig. 6).
The diaphragmatic muscle mass is maintained from early youth (19 yrs) to old age (91 yrs) [62). Accordingly, the fibre cross-sectional area of inspiratory muscles remains fa irly constant from the 20th to 65th year (fig. 7). In contrast, the expiratory INT appears to be approximately 20% smaller in fibre cross-sectional area after the age of fifty years due to a reduction of
both ST and Ff fibre areas. Muscle mass of the thigh decreases (30%) more than the fibre cross-sectional area (15%) after the age of fifty years, suggesting that muscle atrophy with age reflects· not only a decrease in fibre cross-sectional area but also in the number of muscle fibres [97] .
A functional equivalent to the reduced muscle mass in the thigh is a similar reduction in both static strength and dynamic power (97]. However, training maintains or even increases the work performance in elderly individuals [98, 99]. In the respiratory muscles, the reduced fibre cross-sectional area observed in the

596 M. MIZUNO
expiratory INT may explain the reduction in FEV1
and MVV after the age of 35 yrs [100, 101). Conversely, the constant fibre size of inspiratory muscles with ageing is an indication of maintained use of these muscles. As previously mentioned, the large fibre size of expiratory INT is considered to be an adaptation to non-ventilatory rather than to ventilatory function so that their reduced size with age may reflect a more sedentary life style.
Enzyme activities and substrate contents
Mitochondrial and glycolytic enzyme activities
Quantitative biochemical de terminations of substrate contents and enzyme activities are other expressions of altered degree of use. Mitochondrial enzyme activities represented by e.g. citrate synthase (CS) and 3-hydroxyacyl-coenzyme A dehydrogenase (HAD) are within a range of values reported for skeletal muscles in the extremities of non-athletes [1) (table 5). The differences noted between the histochemical characteristics of the expiratory INT and the inspiratory muscles is not reflected in the reported mitochondrial enzyme activities. In contrast to histochemical characteristics, mitochondrial enzyme activities adapt at an early stage of training or inactivity [104-107]. Thus, the fact that most biochemical data are obtained from patients admitted for surgery and not from normal individuals may have influenced the results due to reduced physical activity of patients during hospitalization. Additional evidence for this assumption is the finding that when biopsies have been obtained from patients with COPD, the mitochondrial enzyme activities in both inspiratory and expiratory intercostal muscles are higher than in other skeletal muscles [103).
In patients with normal ventilatory function, HAD activity is slightly higher in the costal diaphragm (102) than in both the EXT and expiratory INT. CS activity as well as glycolytic enzyme activities, represented as hexokinase (HK) and lactate dehydrogenase (LDH), are similar among these muscles (table 5) [50, 78, 102]. In COPD patients both HK and LDH activity in the costal diaphragm are lower than in intercostal muscles, while CS and HAD activities are similar [102].
In both inspiratory EXT and expiratory INT, CS and HAD activity are higher in patients with moderate COPD than in patients with normal ventilatory function [103). However, in patients with severe COPD, a similar mitochondrial enzyme activity exists for both the inspiratory EXT and expiratory INT [51].
Glycogen and lactate
In the diaphragm and intercostal muscles the average glycogen content is 190-380 ~mol·g·1 dry weight and lactate varies from 7 to 20 ~-tmol·g·1 dry weight (table 6). The values observed in respiratory muscles
are within a range reported for limb skeletal muscles. The wide range of values partly reflects the circumstances under which the muscle biopsies were obtained. In normal subjects relatively high muscle lactate concentrations of 20 J.tmol·g·' dry weight are seen only after intense exercise [109). Such values observed in patients may be associated 'with metabolic acidosis due to muscle hypoperfusion during surgery. More likely the high concentration of lactate in intercostal muscles is caused by the use of a depolarizing muscle relaxant, such as suxamethonium for tracheal intubation, leading to muscle fibrillations which result in lactate accumulation (17).
Independent of ventilatory function of the patients, the inspiratory intercostal muscles have 20% less glycogen content than the expiratory INT and the diaphragm in surgical biopsies (table 6). However, when biopsies were taken during spontaneous breathing, and thus without the use of muscle relaxants, the inspiratory and expiratory intercostal muscles have similar glycogen contents [54). The ventilatory problems of patients with COPD appear to be reflected by a high lactate concentration in the inspiratory intercostal muscles [54].
Phosphagen
Mean values of adenosine triphosphate (ATP) concentration in the diaphragm and intercostal muscles range between 10 and 20 J,Amol·g·1 dry weight (table 6). The concentration of phosphocreatine (PCr) ranges from 60 to 70 J,Amol·g·1 dry weight. These values are similar to those reported for limb skeletal muscles [1). A slightly lower PCr content (47 J.tmol·g·1 dry weight) has been reported in intercostal muscles obtained during spontaneous breathing. This value may have resulted from biopsies being taken from working muscles as compared with others obtained from relaxed muscles during surgery.
Effect of muscle relaxants
It is a classical observation in animals that muscle relaxants affect respiratory muscles less than other skeletal muscles [110). This difference in effects among skeletal muscles exists in man and holds for both depolarizing and non-depolarizing neuromuscular blocking agents [111, 112]. Thus, a popular test for post-operative patients is to evaluate the ability for lifting the head in order to ensure that the strength of the respiratory muscles is restored after the use of neuromuscular blocking agents (113),
In human [114, 115) as well as animal skeletal muscles [110, 116) it has been demonstrated that the nondepolarizing muscle relaxant tubocurarine affects ST fibres to a greater extent than FT fibres after a single dose which produce partial neuromuscular blockade. The larger proportion of ST fibres exists in intercostal and scalene muscles (approximately 65%) as compared with

INSPIRATORY AND EXPIRATORY MUSCLES 597
the diaphragm (approximately 50%). This difference may partly explain the greater effects of non-depolarizing neuromuscular blocking agents on the scalenes and intercostal muscles as compared with the diaphragm (117). The fact that EMG activity in the diaphragm increases after the administration of Pavulon suggests that more unblocked diaphragmatic fibres are recruited when the other inspiratory muscles are blocked [117).
In intercostal muscles a substantial decrease in intramuscular glycogen and accumulation of muscle lactate takes place following the administration of the depolarizing agent suxamethonium for tracheal intubation. Under this circumstance a marked glycogen depletion occurs particularly in FTb fibres [17]. More FTb fibres are present in the inspiratory intercostal muscles than in the expiratory INT. As noted previously, this finding may explain the lower glycogen content in the inspiratory than the expiratory intercostal muscles among patients undergoing surgery, whereas no difference is noted in normal subjects. Thus, muscle fasciculations induced by the use of depolarizing agents appear to affect in particular the FTb fibres.
On a broader comparison between different muscles, the histochemical classification of ST and FT fibres does not explain a difference in effects between nondepolarizing and depolarizing neuromuscular blocking agents. Moreover, the diaphragm is less affected by nondepolarizing agents than other skeletal muscles [111), which cannot be explained by the relative proportion of ST fibres alone. Therefore, unknown differences must exist at the neuromuscular junction between muscles or between muscle fibre types. This difference appears to be independent of the relative proportion of ST fibres.
The heterogeneity of fibre types in the respiratory muscles, however, gives rise to some clinical considerations for postoperative patients. The head-lift test depends mainly on the strength of the sternomastoid muscle, which possesses only 35% ST fibres. Thus, the ability to perform head-lift may be less affected by non-depolarizing agents than the respiratory muscles. Furthermore, with the combined use of depolarizing and non-depolarizing neuromuscular blocking agents during surgery, postoperative ventilatory function may be impaired for two reasons: 1) persistent neuromuscular blockade of particularly ST fibres; and 2) weakness caused by the development of fatigue in glycogen depleted FT fibres.
Conclusion
Histochemical profiles indicate that the expiratory intercostal muscles have adapted to heavy and continuous activity in man. Because no similar characteristics reflecting training effects are observed in the inspiratory muscles, the inspiratory work load seems to be insufficient to elicit such an adaptation.
With ageing the expiratory (but not inspiratory) intercostal muscles appear to show atrophy, indicating that the larger fibre size of the expiratory intercostal muscles is adapted to non-ventilatory rather than to ventilatory
function despite a correlation with the results of standard ventilatory functional tests. The demands on the expiratory intercostal muscles for vocalization and for performing Valsalva-like manoeuvres during lifting and reaching may cause this adaptation. The atrophy of these muscle fibres with age may simply reflect an increasingly sedentary life style.
In patients with only moderate COPD, increased mitochondrial enzyme activities exist in both the inspiratory and expiratory intercostal muscles. In patients with severe COPD the activity of these enzymes decreases, and a reduction in muscle fibre size occurs, particularly in the diaphragm and the expiratory intercostal muscles. Thus, the increased work of breathing in these patients seems to be accomplished by intense involvement of extrathoracic muscles, even during quiet breathing.
Following the use of the depolarizing neuromuscular agent suxamethonium, a selective depletion of muscle glycogen occurs in fast-twitch (particularly FTb) fibres. Thus, the glycogen content of the expiratory muscles, which possess the fewest FTb fibres, appears to be greater than that of the inspiratory intercostal muscles in surgical patients. The lowest proportion of slow-twitch fibres in the diaphragm may account for the minimal effect of non-depolarizing neuromuscular agents on respiratory muscles. This characteristic does not, however, explain the similar effect of depolarizing neuromuscular blocking agents. Thus, differences in muscle morphology alone do not provide an adequate explanation for the different sensitivity to neuromuscular blocking agents which exists between thoracic and extrathoracic respiratory muscles as well as between the respiratory muscles and limb skeletal muscles.
Acknowledgements: The author wishes to express gratitude to Dr N.H. Secher, Department of Anaesthesia, Rigshospitalet, University of Copenhagen, for stimulating constructive criticism.
References
1. Saltin B, Gollnick PD. - Skeletal muscle adaptability. Significance for metabolism and performance. In: Handbook of physiology. Section 10: Skeletal muscle. L.D. Peachey, R.H. Adrian eds, Am Physiol Soc, Bethesda, 1983 pp. 555-631. 2. Taylor A. - The contribution of the intercostal muscles to the effort of respiration in man. J Physio/ (Lond), 1960, 151, 39~02. 3. Tokizane T, Kawamata K, Tokizane H. -Electromyographic studies on the human respiratory muscles. Studies on the activity pattern of neuromuscular units. Jap J Physio/, 1951-1952, 2, 232-247. 4. Campbell EJM, Agostoni E, Newson Davis J. -In: The Respiratory Muscles. Mechanics and Neural Control. LloydLuke, London, 1970. 5. De Troyer A, Loring SH. - Action of the respiratory muscles. In: Handbook of physiology, section 3: The respiratory system, vol. III, part 2. A.P. Fishman ed., Am Physiol Soc, Bethesda, 1986, pp. 443-461. 6. Loring SH, De Troyer A. - Actions of respiratory

598 M. MIZUNO
muscles. In: The thorax. Part A. C. Roussos, P.T. Macklem eds, Marcel Dekker Inc, New York, 1985, pp. 327-349. 7. Mizuno M, Secher NH.- Histochemical characteristics of human expiratory and inspiratory muscles. J Appl Pllysiot 1989, 67, 592-598. 8. Derenne J-PH, Macklem PT, Roussos C. - The respiratory muscles. Mechanics, control and pathophysiology. Am Rev Respir Dis, 1978, 118, 119-133, 373-390, 581--601. 9. Edwards RHT, Faulkner JA. - Structure and function of respiratory muscles. In: The thorax. Part A. C. Roussos, P.T. Macklem eds, Marcel Dekker Inc., New York, 1985, pp. 297-326. 10. Roussos C, Macklem PT. - The respiratory muscles. N Engl J Med, 1982, 23, 786-797. 11. Delhez L, Bottin R, Thomon A, Vierset J. - Modifications du diagramme-pression-volume maximum de l'appareil thoracopulmonaire apr~s entrainement des muscles respiratoires par des exercises statiques. Arch lnt Physiol Biochem, 1966, 74, 335-336. 12. Leith DE, Bradley M. - Ventilatory muscle strength and endurance training. J Appl Physiol, 1976, 41, 508-516. 13. Belman MJ, Sieck GC. - The ventilatory muscles. Fatigue, endurance and training. Chest, 1982, 6, 761-766. 14. Flenley DC.- Inspiratory muscle training. Eur J Respir Dis, 1985, 67, 153-158. 15. Pardy RL, Leith D. - Ventilatory muscle training. In: The thorax. Part B. C. Roussos, P.T. Macklem eds, Marcel Dekker Inc, New York, 1985, pp. 1353-1371. 16. Decramer M. - Effects of hyperinflation on the respiratory muscles. Eur Respir J, 1989, 2, 299-302. 17. Secher NH, Mizuno M, Saltin B. - Adaptation of skeletal muscles to training. Bull Eur Physiopathol Respir, 1984, 20, 453-457. 18. Padykula HA, Herman E. - The specificity of the histochemical method for adenosine triphosphatase. J Histocllem Cytochem, 1955, 107-195. 19. Engel WK.- The essentiality of histo- and cytochemical studies of skeletal muscle in the investigation of neuromuscular disease. Neurology (Minneapolis) , 1962, 12, 778-794. 20. B6r6ny M.- ATPase activity of myosin correlated with speed of muscle shortening. J Gen Physiol, 1967, 50 (part 2), 197-218. 21. Saltin B, Henriksson J, Nygaard E, Andersen P, Jansson E. - Fiber types and metabolic potentials of skeletal muscles in sedentary man and endurance runners. Ann A N A cad Sci, 1977, 301, 3-29. 22. Biral D, Betto R, Danieli-Betto D, Salviati G. - Myosin heavy chain composition of single fibres from normal human muscle. Biochem J, 1988, 250, 307-308. 23. Buchthal F, Schmalbruch H. - Contraction times and fibre types in intact human muscle. Acta Physiol Scand, 1970, 79, 435-452. 24. Garnett RAF, O'Donovan MJ, Stephens JA, Taylor AMotor unit organization of human medial gastrocnemius. J Physiol (Lond), 1979, 33-43. 25. Hanson J. - Effects of repetitive stimulation on membrane potentials and twitch in human and rat intercostal muscle fibres. Acta Physiol Scand, 1974, 92, 238-248. 26. Brooke MH, Kaiser KK. - Three "myosin adenosine triphosphatase" systems. The nature of their pH !ability and sulfhydryl dependence. J Histochem Cytochem, 1970, 18, 670-672. 27. Sj!ifgaard G, Houston ME, Nygaard E, Saltin B. -Sub-grouping of fast twitch fibres in skeletal muscles of man: A critical appraisal. Histochemistry, 1978, 58, 79-87.
28. Eriksson P-0, Eriksson A, Ringqvist M, Thomell L-E.The reliability of histochemical fibre typing of human necropsy muscles. Histochemistry, 1980, 65, 193-205. 29. Maxwell LC, Kuehl TJ, Robotham JL, McCarter RJM. -Temporal changes after death in primate diaphragm muscle oxidative enzyme activity. Am Rev Respir Dis, 1984, 130, 1147-1151. 30. Monster A W, Chan HC, O'Connor D. - Activity patterns of human skeletal muscles: relation to muscle fiber type composition. Science, 1978, 200, 314-317. 31. Warmolts JR, Engel WK. - Open-biopsy electromyography. I. Correlation of motor unit behavior with histochemical muscle fiber type in human limb muscle. Arch Neurol, 1972, 27, 512-517. 32. Komi PV, Vitasalo JHT, Havu M, Thorstensson A. -Skeletal muscle fibres and muscle enzyme activities in monozygous and dizygous twins of both sexes. Acta Physiol Scand, 1977, 100, 385-392. 33. Baumann H, Jliggi M, Soland F, Howald H, Schaub MC. - Exercise training induced transitions of myosin isoform subunits within histochemically typed human muscle fibres. Pjlugers Arch, 1987, 409, 349-360. 34. Billeter R, Weber H, Lutz H, Howald H, Eppenberger HM, Jenny E.- Myosin types in human skeletal muscle fibers. Histochemistry, 1980, 65, 249-259. 35. Schantz P, Dhoot GK. - Coexistence of slow and fast isoforms of contractile and regulatory proteins in human skeletal muscle fibres induced by endurance training. Acta Physiol Scand, 1987, 131, 147-154. 36. Andersen P, Henriksson J. - Capillary supply of the quadriceps femoris muscle of man. Adaptive response to exercise. J Physiol (Lond), 1977, 270, 677--690. 37. Mizuno M, Juel C, Bro-Rasmussen T, Mygind E, Schibye B, Rasmussen B, Saltin B. - Limb skeletal muscle adaptation in athletes following training at altitude. J Appl Physiol, 1990, 68, 496-502. 38. Costil DL, Coyle EF, Fink WF, Lesmes GR, Witzmann FA. - Adaptations in skeletal muscle following strength training. J Appl Physiol: Respirat Environ Exercise Physiol, 1979, 46, 96-99. 39. Tesch PA, Thorsson A, Kaiser P. - Muscle capillary supply and fiber type characteristics in weight and power lifters. J Appl Physiol, 1984, 56, 35-38. 40. Sj!ifgaard G. - Capillary supply and cross-sectional area of slow and fast twitch muscle fibres in man. Histochemistry, 1982, 76, 547-555. 41. Schantz P. - Capillary supply in heavy-resistance trained non-postural human skeletal muscle. Acta Physiol Scand, 193, 117, 153-155. 42. Appell H-J, Forsberg S, Hollmann W. - Satellite cell activation in human skeletal muscle after training: evidence for muscle fiber neoformation. lnt J Sports Med, 1988, 9, 297-299. 43. Gollnick PD, Timson BF, Moore RL, Riedy M. -Muscular enlargement and number of fibers in skeletal muscles of rats. J Appl Physiol: Respirat Environ Exercise Physiol, 1981, 50, 936-943. 44. BergstrOm 1. - Muscle electrolytes in man. Determined by neutron activation analysis on needle biopsy specimens. A study on normal subjects, kidney patients, and patients with chronic diarrhoea. Scand J Clin Lab lnvest, 1962, 14 (Suppl.) 68. 45. McKenzie DK, Gandevia SC, Shorey CD. - A histochemical study of human inspiratory muscles. (Abstract). In: Proc lnt Un Physiol, vol XV, Sydney, 1983 p. 351. 46. Keens TG, Chen V, Pate! P, O'Brien P, Levison H, Ianuzzo CD. - Cellular adaptations of the ventilatory

INSPIRATORY AND EXPIRATORY MUSCLES 599
muscles to a chronic increased respiratory load. J Appl Physiol, 1978, 44, 905-908. 47. Stern LZ, Payne CM, Gruener R, Anderson RM, Hannapel LK. - Intercostal muscle biopsy in human neuromuscular disease. Histochemical and electron microscopic studies. J Neurol Neurosurg Psychiat, 1975, 38, 900-910. 48. SAnchez J, Derenne JP, Debesse B, Riquet M, Monod H. - Typology of the respiratory muscles in normal men and in patients with moderate chronic respiratory diseases. Bull Eur Physiopathol Respir, 1982, 18, 901-914. 49. S~nchez J, Medrano G, Debesse B, Riquet M, Derenne JP. - Muscle fibre types in costal and crural diaphragm in normal men and in patients with moderate chronic respiratory disease. Bull Eur Physiopathol Respir, 1985, 21, 351-356. 50. Mizuno M, Secher NH, Saltin B. - Fibre types, capillary supply and enzyme activities in human intercostal muscles. Clin Physiol, 1985, 5, 121-135. 51. Campbell JA, Hughes RL, Sahgal V, Frederiksen J, Shields TW. - Alterations in intercostal muscle morphology and biochemistry in patients with obstructive lung disease. Am Rev Respir Dis, 1980, 122, 679-686. 52. Hughes RL, Katz H, Sabgal V, Campbell JA, Hartz R, Shields W. - Fiber size and energy metabolites in five separate muscles from patients with chronic obstructive lung disease. Respiration, 1983, 44, 321-328. 53. Dubolwitz V, Brooke MH. - In: Muscle biopsy: a modern approach. W.B. Saunders Company, London, 1973. 54. Gertz I, Hedenstierna G, Hellers G, Wahren J.- Muscle metabolism in patients with chronic obstructive lung disease and acute respiratory failure. Clin Sci Mol Med, 1977, 52, 395-403. 55. Krogh A. - The number and distribution of capillaries in muscles with calculations of the oxygen pressure head necessary for supplying the tissue. J Physiol (Lond), 1918-19, 52, 409-415. 56. Saltin B, Rowell LB. - Functional adaptations to physical activity and inactivity. Fed Proc, 1980, 39, 1506-1513. 57. Lieberman DA, Faulkner JA, Craig Jr AB, Maxwell LC. - Performance and histochemical composition of guinea pig and human diaphragm. J Appl Physiol, 1973, 34, 233-237. 58. Ishikawa S, Hayes JA. - Functional morphometry of the diaphragm in patients with chronic obstructive lung disease. Am Rev Respir Dis, 1973, 108, 135-138. 59. Scott KWM, Hoy J. - The cross-sectional area of diaphragmatic muscle fiber in emphysema, measured by an automated image analysis system. J Pathol, 1976, 120, 121-128. 60. Steele RH, Heard BE. - Size of the diaphragm in chronic bronchitis. Thorax, 1973, 28, 55-60. 61. Barach AL. - Restoration of diaphragmatic function and breathing exercise in pulmonary emphysema. NY State J Med, 1956, 56, 3319-3332. 62. Arora NS, Rochester DF. - Effect of body weight and muscularity on human diaphragm muscle mass, thickness, and area. J Appl Physiol: Respirat Environ Exercise Physiol, 1982, 52, 64-70. 63. Arora NS, Rochester DF.- COPD and human diaphragm muscle dimension. Chest, 1987, 91, 719-724. 64. Jansson E, Kaijser L. - Muscle adaptation to extreme endurance training in man. Acta Physiol Scand, 1977, 100, 315-324. 65. De Troyer A, Sampson MG, Sigrist S, Macklem PT. -Action of costal and crural parts of the diaphragm on the rib
cage in dog. J Appl Physiol: Respirat Environ Exercise Physiol, 1982, 53, 30-39. 66. Stewart MB, Hanson RE, De Troyer A, Macklem PT. -Radiology of the diaphragm as two muscles. Invest Radio/, 1983, 18, 155-159. 67. Terrados N, Melichna J, Sylv~n C, Jansson E, Kaijser L. - Effects of training at simulated altitude on performance and muscle metabolic capacity in competitive road cyclists. Eur J Appl Physiol, 1988, 57, 203-209. 68. Draper MH, Ladefoged P, Whitteridge D.- Respiratory muscles in speech. J Speech Hearing Res, 1959, 2, 16-27. 69. Munro RR, Adams C. - Electromyography of the intercostal muscles in connected speech. Electromyography, 1971, 11, 365-378. 70. Munro RR, Adams C. - The patterns of internal intercostal muscle activity used by some non-native speakers of English. Electromyogr Clin Neuropltysiol, 1973, 13, 271-288. 71. Murphy AJ, Koepke GH, Smith EM, Dickinson DG. -Sequence of action of the diaphragm and intercostal muscles during respiration. II. Expiration. Arch Phys Med Rehabil, 1959, 40, 337-342. 72. Hoppeler H, Howald H, Conley K, Lindstedt S, Claassen H, Vock P, Weibel ER. - Endurance training in humans. Aerobic capacity and structure of skeletal muscle. J Appl Physiol, 1985, 59, 320-327. 73. Howald H, Hoppeler H, Claassen H, Mathieu 0, Straub R. - Influences of endurance training on the ultrastructural composition of different muscle fiber types in humans. Pflugers Arch, 1985, 403, 369-376. 74. De Troyer A, Estenne M. - Coordination between rib cage muscles and diaphragm during quiet breathing in humans. J Appl Physiol: Respirat Environ Exercise Physiol, 1984, 57, 899-906. 75. De Troyer A, Sampson MG. - Activation of the parasternal intercostals during breathing efforts in human subjects. J Appl Physiol: Respirat Environ Exercise Physiol, 1982, 52, 524-529. 76. Koepke GH, Smith EM, Murphy AJ, Dickinson DG. -Sequence of action of the diaphragm and intercostal muscles during respiration. I. Inspiration. Arch Phys Med Rehabi/1958, 39, 426-430. 77. Raper AJ, Thompson Jr WT, Shapiro W, Patterson Jr JL. - Scalene and sternomastoid muscle function. J Appl Physiol, 1966, 21, 497-502. 78. Sampson MG, De Troyer A. - Role of intercostal muscles in the rib cage distortions produced by inspiratory loads. J Appl Physiol: Respirat Environ Exercise Physiol, 1982, 52, 517-523. 79. Decramer M, Kelly S, De Troyer A. - Respiratory and postural changes in intercostal muscle length in supine dogs. J Appl Physiol, 1986, 60, 1686-1691. 80. Schraufnagel DE, Roussos CH, Macklem P, Wang N-S. - The geometry of the microvascular bed of the diaphragm. Comparison to intercostals and triceps. Microvasc Res, 1983, 26, 291-306. 81. Nishiyama A. - Histochemical studies on the red, white and intermediate muscle fibers of some skeletal muscles. I. Succinic dehydrogenase activity and physiological function of intercostal muscle fibers. Acta Med Okayama, 1965, 19, 177-189. 82. Nishiyama A. - Histochemical studies on the red, white and intermediate muscle fibers of some skeletal muscles. 11. Histochemical demonstration of oxidative enzymes, phosphorylase and glycogen in respiratory muscle fibers. Acta Med Okayama, 1966, 20, 137-146.

600 M. MIZUNO
83. Reid MB, Ericson GC, Feldman HA, Johnson Jr RL. -Fiber types and fiber diameters in canine respiratory muscles. J Appl Physiol, 1987, 62, 1705-1712. 84. Maxwell LC, McCarter RJM, Kuehl TJ, Robotham JL. - Development of histochemical and functional properties of baboon respiratory muscles. J Appl Physiol: Respirat Environ Exercise Physiol, 1983, 54, 551-561. 85. Thompson Jr WT, Patterson Jr JL, Shapiro W. -Observations on the scalene respiratory muscles. Arch Inter Med, 1964, 113, 856-865. 86. Johnson MA, Polgar J, Weightman D, Appleton D. -Data on the distribution of fibre types in thirty six human muscles. An autopsy study. J Neurol Sci, 1973, 18, 111-129. 87. Arora NS, Rochester DF.- Effect of chronic obstructive pulmonary disease on sternocleidomastoid muscle. (Abstract). Am Rev Respir Dis, 1982, 125, 252. 88. Haggmark T, Thorstensson A. - Fibre types in human abdominal muscles. Acta Physiol Scand, 1979, 107, 319-325. 89. Delgado HR, Braun SR, Skatrud JB, Reddan WG, Pegelow DF. - Chest wall and abdominal motion during exercise in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis, 1982, 126, 200-205. 90. Sharp JT. - The chest wall and respiratory muscles in airflow. In: The thorax. Part B. C. Roussos, P.T. Macklem eds, Marcel Dekker Inc, New York, 1985 pp. 1155- 1202. 91. Keens TG, Bryan AC, Levison H, Ianuzzo CD. -Developmental pattern of muscle fiber types in human ventilatory muscles. J Appl Physiol: Respirat Environ Exercise Physiol, 1978, 44, 909-913. 92. Keens TG, Ianuzzo CD. - Development of fatigueresistant muscle fibers in human ventilatory muscles. Am Rev Respir Dis, 119 (part 2), 1979, 139-141. 93. Aniansson A, Grimby G, Nygaard E, Saltin B. -Muscle f iber composition and fiber area in various age groups. (Abstract). Muscle Nerve, 1980, 3, 271-272. 94. Colling-Saltin A-S. - Enzyme histochemistry on skeletal muscle of the human fetus. J Neurol Sci, 1978, 39, 169-185. 95. Colling-Saltin A-S. - Skeletal muscle development in the human fetus and during childhood. In: Children and Exercise. IX. K. Berg, B. Eriksson eds, University Park Press, Baltimore, 1980, pp. 193-207. 96. Grimby G, Aniansson A, Zetterberg C, Saltin B. -Is there a change in relative muscle fibre composition with age? Clin Physiol, 1984, 4, 189-194. 97. Grimby G, Saltin B. - The ageing muscle. Clin Physiol, 1983, 3, 209-218. 98. Aniansson A, Gustafsson E. - Physical training in elderly men with specific reference to quadriceps muscle strength and morphology. Clin Physiol, 1981, 1, 87-98. 99. Larsson L. - Physical training effects on muscle morphology in sedentary males at different ages. Med Sci Sports Exerc, 1982, 14, 203-206. 100. Berglund E, Birath G, Bjure J, Grimby G, Kjellmer I, Sandqvist L, Soerholm B. - Spirometric studies in normal subjects. I. Forced expirograms in subjects between 7 and 70 years of age. Acta Med Scand, 1963, 173, 185-192. 101. Birath G, Kjellmer I, Sandqvist L. - Spirometric studies in normal subjects. II. VentiJatory capacity testing in adults. Acta Med Scand, 1963, 173, 193-198. 102. Sanchez J, Bastien C, Medrano G, Riquet M, Derenne JP. - Metabolic enzymatic activities in the diaphragm of normal men and patients with moderate chronic obstructive pulmonary disease. Bull Eur Physiopathol Respir, 1984, 20, 535-540.
103. Sanchez L, Brunei A, Medrano G, Debesse B, Derenne JP. - Metabolic enzymatic activities in the intercostal and serratus and in the latissimus dorsi of middle-aged normal men and patients with moderate obstructive pulmonary disease. Eur Respir J, 1988, 1, 376-383. 104. Bangsbo J, Mizuno M. - Morphological and metabolic alterations in soccer players with detraining and retraining and their relation to performance. In: Science and Football. T. Reilly, T. Lees, K. Davids, W.J. Murphy eds, E. & F.N. Spon, New York, 1988, pp. 114-124. 105. Coyle EF, Martin III WH, Sinacore DR, Joyner MJ, Hagberg JM, Holloszy JO. - Time course of loss of adaptations after stopping prolonged intense endurance training. J Appl Physiol: Respirat Environ Exercise Physio/, 1984, 57, 1857-1864. 106. Henriksson J, Reitman JS.- Time course of changes in human skeletal muscle succinate dehydrogenase and cytochrome oxidase activities and maximal oxygen uptake with physical activity and inactivity. Acta Physiol Scand, 1977, 99, 91-97. 107. Richter EA, Kiens B, Mizuno M, Strange S. - Insulin action in human thighs after one-legged immobilization. J Appl Physiol, 1989, 67, 19-23. 108. Mizuno M, Secher NH, Saltin B. -Biochemical findings in external and internal intercostal muscles in man. Acta Physiol Scand, 1984, 121, 12A. 109. Bangsbo J, Gollnick PD, Graham TE, Juel C, Kiens B, Mizuno M, Saltin B. - Anaerobic energy production and 0
2 deficit-debt relationship during exhaustive exercise in
humans. J Physiol (Lond), 1990, 422, 539-559. 110. Paton WDM, Zaimis EJ. -The action of D-tubocurarine and of decamethonium on respiratory and other muscles in the cat. J Physiol (Lond), 112, 311-331. 111. Johansen SH, Jl'!rgensen M, Molbech S. - Effect of tubocurarine on respiratory and nonrespiratory muscle power in man. J Appl Physiol, 1964, 19, 990-994. 112. Jl'!rgensen M, Molbech S, Johansen SH. - Effect of decamethonium on head lift, hand grip and respiratory muscle power in man. J Appl Physiol, 1966, 21, 509-512. 113. Dam WH, Guldmann N. - Inadequate postanesthetic ventilation. Anesthesiology, 1961, 22, 699-707. 114. Leonard B, Mitchell JH, Mizuno M, Rube N, Saltin B, Secher NH. -Partial neuromuscular blockade and cardiovascular responses to static exercise in man. J Physiol (Lond), 1985, 359, 365-379. 115. Secher NH, Rube N, Secher 0.- Effects of tubocurarine on human soleus and gastrocnemius muscles. Acta Anaesth Scand, 1982, 26, 231-234. 116. Jewell PA, Zaimis EJ. - A differentiation between red and white muscle in the cat based on response to neuromuscular blocking agents. J Physiol (Lond), 1954, 417-428. 117. De Troyer A, Bastenier J, Delhez L. - Function of respiratory muscles during partial curarization in humans. J Appl Physiol: Respirat Environ Exercise Physiol, 1980, 49, 1049-1056.
Muscles respiratoires humains: morphologie des fibres et apport cqpillaire. M. Mizuno. . RESUME: Chez l'homme, le dtaphragme (DIA) et les muscles abdominaux comportent approximativement 50% de fibres a reaction lente, alors qu'une proportion superieure (60%) est decelee dans les muscles intercostaux et les scal~nes. Tous les muscles respiratoires ont une distribution egale de fibres a reaction rapide (FTa et b) a !'exception des muscles intercostaux expiratoires, qui n'ont que peu de fibres FTb.

INSPIRATORY AND EXPIRATORY MUSCLES 601
Les muscles inspiratoires ont des fibres d'une taille uniform6ment petite, A !'oppose des muscles intercostaux expiratoires dont les fibres sont plus grandes. La dimension des fibres des muscles inspiratoires se maintient au cours du vieillissement, alors que celle des muscles intercostaux expiratoires semble diminuer apres l'age de 50 ans. L'apport capillaire est plus abondant dans les muscles expiratoires, suivis par le diaphragme et les muscles inspiratoires intercostaux. Chez les patients atteints de bronchopneumopathies chroniques obstructives, on ignore si
une reduction de la taille des fibres des muscles respiratoires thoraciques est causee par leur surutilisation due au travail ventilatoire accru ou par une mauvaise utilisation due a une implication accrue des muscles respiratoires extra-thoraciques. les caracteristiques histochimiques suggerent que, chez les sujets humains normaux, la charge des muscles inspiratoires est relativement faible au cours des contractions, alors que les muscles intercostaux expiratoires sont exposes a une activite continue marquee avec un charge importante. Eur Respir J., 1991, 4, 587-601.