Pharmacokinetics of anti-tuberculosis drugs in HIV-positive and HIV-negative adults in Malawi
description

Human Resources for HIV Scale Up
in Malawi Vienna, 2010
Frank M Chimbwandira, S Makombe, E Mhango, J Njala, L Tenthani, P Moses, E Schouten, Z Chirwa, A Jahn

Malawi Indicators• 13.06 million people• 12 % HIV prevalence
• among 15-49 year olds
• About 1 million PLWH• 384 000 in need of ART
– 211 246 PLHIV alive and on ART by March, 2010
• Approx. 700 000 orphans due to AIDS epidemic
• 1 Physician : 49 000 people• 1 Nurse :1 800 people

Human Resources for Health IMalawi situation in 2004:• 64% vacancies among nurses;
– Over half of 29 districts have less than 1.5 nurses per facility, and five districts have less than one
•53% vacancies among clinical officers; •85%-100% vacancies among specialists– 10 districts without a MoH doctor, four districts
without any doctor at all

Human Resources for Health II
• In 2004 Dr Peter Piot (UNAIDS) and Dr Suma Chakrabarti (DFID) were concerned
“ ….. that without a substantial increase in health
workers, it would not be possible [for Malawi] to roll out antiretroviral treatment without further undermining the already weak health system.”
Palmer D, ………
Reproductive Health Matters 2006; 14(27):27-39…………

Human Resources for Health III
• Inadequate workforce in the health delivery system was aggravated by – Poor recruitment systems– Limited or non-responsive trainings– Poor staff retention mechanisms – Inadequate finances

Emergency HRP I: Plan
• Drawn up for 2004 – 2010 period• Focused on retention, deployment,
recruitment, training and tutor incentives• Targeted 11 cadres
– Physicians, nurses, COs, MAs, pharmacists, lab technicians, … and expansion of community health worker cadres
• Budget: ~US$200 m US$270 m– GoM, DFID, GFATM, Health SWAp ……

Emergency HRP II: Approaches• Short-term interventions
– Recruit unemployed or retired staff– Expatriate staff for TA and mentoring– Salary top-ups– Recruitment of community health workers
• Long-term interventions– In-country pre-service training– Comprehensive Monitoring and Evaluation
Systems

Emergency HRP III: Outcomes I
• More posts were filled between 2003 and 2007– 30% increase in nurses, 40% in medical
doctors, and 50% in clinical officers• Reduced emigration of nurses• Over 5600 community health workers
were recruited• Training institutions created more room
for enrollment: infrastructure development

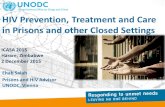
Emergency HRP IV: Outcomes II
-
50
100
150
200
250
2003 2004 2005 2006 2007 2008 2009
Relative change in MOH and CHAM staffing for5 main cadres in Malawi from 2003 to 2009 (2003=100)
Clinical Officer
Nurse
Medical Assistant
Laboratory Technician
Physician


Some Cadres and TasksCadre Counseling HIV
Testing Clinical Staging
ARV Drug Initiation
Follow up
“Non-health workers” +++
Health Surveillance Assistants
+++ +++ ?
Laboratory Technicians +++
Nurses ++ ++ ++ ++ +++
Medical Assistants + + +++ +++ +++
Clinical Officers + + +++ +++ +++
Medical Doctors + +++ +++ +++

ART Scale Up: Malawi
2006Sites: 141
Alive: 59,980Coverage: 17%
2009Sites : 377
Alive: 198,846Coverage: 53%
2008Sites: 221
Alive: 147,497Coverage: 41%
Doctors and Clinical Officers (COs)
Doctors , Clinical Officers, Medical Assistants (MAs)
Doctors, COs, MAs and Nurses
2007Sites: 163
Alive: 100,649Coverage: 28 %
2004Sites: 24
Alive: 10,761Coverage: 3%
Policy Changes: Who should initiate ART? >………………..
2003Sites: 9Alive: ??
Coverage: ??


ART Sites In Malawi

HIV Testing and Counseling
Year

HIV Testing and Counseling 2009

HTC Scale Up• Approaches
– Door-to-Door HIV testing and Counseling – National HTC Campaigns
• HTC weeks, targeted sites or functions – Mobile and Outreach HTC– Task shifting:
• Health Surveillance Assistants do HTC – Task sharing:
• Provider Initiated Testing and Counseling

Challenges
• Need for more workforce– Increasing number of clients on ART– Implementation of new WHO ART/PMTCT
guide– Task shifting has a limit: HSAs may not
initiate ART nor follow up clients• Central posts need strengthening
– Eg Central Medical Stores & technical posts • Donor-dependence on staff retention:
– TAs, Salary top ups ….

Plans• New Programme of Work/SWAp
– Under discussion with donors, HR still • Decentralise HIV services
– Opening of more clinics – Engage expert patients through support groups– Strengthen Integration of HIV services
• Use of new and better regimens (in ART)– Triomune Atripla from 2011

Conclusions
• HR will determine further scale up of HIV services including implementation of the new adopted WHO ART/PMTCT Guidelines.– Training of more personnel (Physicians,
COs, nurses and MAs) still remains an option for Malawi
• Sustainable retention mechanisms are essential too.