SPINAL CORD ANATOMY & PHYSIOLOGY HONORS ANATOMY & PHYSIOLOGY.

BIO 151 01 (3 credits) & BIO 151L 1 credit) HUMAN ANATOMY AND PHYSIOLOGY II
Nazareth College Department of Biology Rochester, NY 14618 (585) 389-2554
2
COURSE DESCRIPTION: This course is a continuation of BIO 150, Human Anatomy and Physiology I. The chapters not covered in BIO 150 (17-29) will be dealt with this semester. BIO 150 is a prerequisite, and BIO 151L (Human Anatomy and Physiology II Laboratory) is a co-requisite. The chapters in the textbook should be read before coming to lecture. Note taking is encouraged as I occasionally may add material not specifically detailed in your textbook. This is a rigorous course but it can be highly instructive and fun for anyone, but particularly so for those who plan to continue their career in any biological discipline, particularly the health care professions. I hope you enjoy this course as much as I enjoy teaching it. TEXTBOOK: Human Anatomy and Physiology: 9th Edition - Elaine N. Marieb & Katja Hoehn, Authors. SUGGESTED MATERIAL: Class Notes for Human Anatomy & Physiology II. Brian W.
Witz, Author. STATEMENT ON STUDENTS WITH DISABILITY: If you are a student with a
documented disability that requires special accommodation, please notify the instructor as soon as possible.
STATEMENT ON ACADEMIC HONESTY: Students are expected to do their own
original work within the confines of the course objectives and evaluation procedures. The expectation is that students will act in accordance with the Nazareth College Policy on Academic Integrity, which can be found in the Student Policies and Procedures Handbook.
TESTING: Four unit examinations will be given during the course. Each examination
will cover approximately 3-4 chapters in the textbook. The examinations may consist of multiple choice, short answer, and essay questions, or any combination thereof, for a total of 100 points per examination. Failure to take an examination will result in a grade of zero for that test. Regrade requests must be in writing and no later than one week after a given examination. You are also required to take the MasteringA&P quizzes associated with each chapter (see below).
FINAL EXAMINATION: A mandatory, cumulative final examination will be given during final examination week. The examination will consist of 100 multiple choice questions worth two points each, for a total of 200 points. You must pass this test to pass the course. GRADING: Grades will be determined by averaging the individual's scores on the five

3
examinations and the MasteringA&P quizzes. Your final grade will be determined using a normal curve system.
Percent method 93.00 – 100.00 A 90.00 – 92.99 A- 87.00 – 89.99 B+ 83.00 – 86.99 B 80.00 – 82.99 B- 77.00 – 79.99 C+ 73.00 – 76.99 C 70.00 – 72.99 C- 60.00 – 69.99 D
0.00 – 59.99 F Percentage is based on accumulated points divided by a total point of 700 points.
*NO EXTRA CREDIT WILL BE GIVEN FOR THIS COURSE! ATTENDANCE: Attendance in lecture is mandatory. No make-up examinations will
be given without a valid, written excuse (e.g. note from physician, police report, etc.). Nazareth’s medical center is NOT a valid excuse to miss an examination. Make-up examinations will be given no later than 1 week after the missed examination and they can be in the essay format. It is your responsibility to contact me (with a written excuse) and arrange for a make-up examination. Failure to attend class will result in the student's name being dropped from the roll. It is both required and courteous to come to class on time and remain in the class for the full duration of my lecture. Continued, unexcused absences and/or tardiness will result in a lowering of your grade.

4
MULTIMEDIA STUDY AIDS: • Moodle – I have established a course management system at this site. You can
access this site by clicking on the Moodle courses link on the Nazareth College web site (use the “Quick Links” drop down menu). You should have been automatically enrolled in this web site. Your Nazareth College user name and password should allow you access. You should check this site daily for information including related powerpoints, messages, and your grades.
• MasteringA&P – I have established a website for the course in www.masteringaandp.com. Please register in MasteringA&P immediately. The course ID is MAPDODGE37484. Course is registered under the title BIO 151-01. You will need the student access code that came with your textbook. You will be required to take a chapter quiz for each chapter that we cover during the semester. I will calculate an average for all quizzes, and this average will be equivalent to one unit test in your final grade calculation. You will find links to A.D.A.M. Interactive Physiology® and PhysioEx® in the “External Links” folder. It is recommended that you complete several assignments in these programs during the semester.
• A.D.A.M. Interactive Anatomy Program – This program is available to you on the computers in Peckham Hall. Please be certain to use the Dissectible Anatomy module to help you learn the terminology and gain a reasonably good 3D perspective of the human body.
• Human Anatomy Program – This interactive cadaver dissection program is available to you on the computers in Peckham Hall.

5
STUDENT LEARNING OBJECTIVES FOR HUMAN ANATOMY AND PHYSIOLOGY II
Upon successful completion of this course, the student should be able to: 1. Identify the key components of human blood, including plasma composition, and the number (per
mm3) of each of the formed elements. 2. Describe the general function of each of the formed elements. 3. Describe the detailed function of erythrocytes and platelets. 4. Describe the process of hematopoeisis. 5. Describe the cellular/biochemical events involved in blood clotting. 6. Discuss the purpose of common diagnostic blood tests and describe common blood pathologies. 7. Identify the location and normal position of the heart in the thoracic cavity. 8. Label the gross anatomical and histological features of the heart and heart muscle tissue,
respectively. 9. Describe the chronological events of atrial and ventricular systole/diastole. 10. Describe the components of the intrinsic conduction system of the heart and describe the pathway of
conduction. 11. Interpret an electrocardiogram and calculate the electrical axis of the heart. 12. Discuss the cellular/biochemical/electrical basis of cardiac muscle cell contraction. 13. Identify the components of the coronary circulation and the area supplied by each vessel. 14. Discuss common pathologies associated with the heart. 15. Compare and contrast the histological structure and function of arteries, veins, and capillaries. 16. Define the terms blood pressure, blood velocity, and peripheral resistance. 17. Calculate cardiac output using heart rate and stroke volume. 18. Calculate stroke volume using end-systolic and end-diastolic volumes. 19. Discuss the application of Poiseule’s Law to movement of blood through a blood vessel. 20. Contrast the physiological mechanisms involved in moving blood through arteries, veins, and
capillaries. 21. List and describe the neural, renal, and endocrine mechanisms for regulation of blood pressure. 22. Describe the roles of oncotic and hydrostatic pressures in capillary dynamics. 23. Identify the major arteries of the body and the region supplied by each. 24. Identify the major veins of the body and the region drained by each. 25. Discuss common blood vessel pathologies and their genetic and environmental causes. 26. Identify the major organs and vessels of the lymphatic system. 27. Describe the interaction between the lymphatic system and the circulatory system. 28. Discuss the general function of the lymphatic system in the body’s defenses. 29. Describe the histological structure and function of lymph nodes and other lymphoid organs. 30. Discuss common pathologies of the lymphatic system. 31. Compare and contrast non-specific and specific (immune system) defenses. 32. Describe the gross anatomical, cellular, and biochemical aspects of non-specific defenses. 33. Compare and contrast cell-mediated and humoral immunity. 34. Identify each of cell types associated with cell-mediated immunity and describe the function of each. 35. Compare and contrast the terms antigen and antibody (immunoglobulins). 36. Describe the function of B-lymphocytes, plasma cells, and memory cells. 37. List the main types of immunoglobulins and describe the function of each type. 38. Describe common pathologies of the immune system, with particular focus on HIV and AIDS. 39. Label the gross anatomical components of the respiratory system. 40. Describe the difference between pulmonary ventilation, external respiration, gas transport and internal
6
respiration. 41. Discuss the events and anatomical components of respiratory mechanics. 42. Describe the chemical/physical properties of gases and gas exchange. 43. Describe the events of gas exchange at the respiratory membrane. 44. Describe the mechanisms for oxygen and carbon dioxide transport in the blood. 45. Discuss the neural control of respiration. 46. Describe the respirator adjustments occurring during exercise and at high altitudes. 47. Discuss common respiratory system pathologies and their causes. 48. Label the gross anatomical components of the digestive system. 49. Discuss the histological aspects of each area of the digestive system. 50. Discuss the mechanical and biochemical processes occurring in each region of the digestive system. 51. Compare and contrast enzymatic hydrolysis, emulsification, and absorption. 52. Identify macronutrients and micronutrients and describe the uses of each. 53. Label the gross anatomical features of the urinary system. 54. Label the microscopic components of the kidney. 55. Describe the physiology of urine production, including filtration, reabsorption, and secretion. 56. Discuss the interaction between the urinary and endocrine systems. 57. Discuss the role of both the respiratory and urinary systems in fluid, electrolyte, and acid-base
balance. 58. Discuss common pathologies of the urinary system and fluid, electrolyte and acid-base balance. 59. Compare and contrast the gross anatomical features of male and female reproductive systems. 60. Describe the cellular/biochemical events occurring during gamete production. 61. Describe the role of the endocrine system in both male and female reproductive cycles. 62. Compare and contrast the sexual response of male and female humans. 63. Describe the methods of contraception. 64. Identify the symptoms of the major sexually transmitted diseases. 65. Identify the chronological events occurring during human embryological and fetal development. 66. Discuss the anatomical and physiological effects of pregnancy on the mother. 67. Describe the events of parturition (birth). 68. Discuss the maternal and infant events occurring post-partum. 69. Describe common congenital defects/genetic abnormalities of newborns.
Biology and Environmental Science Program Student Learning Outcomes (SLOs) Students who have completed the biology or environmental science program will be able to:
• Describe and analyze biological phenomena at the cellular level. • Describe and analyze biological phenomena at the organismal level. • Describe and analyze biological phenomena at the ecological level. • Perform the basic laboratory skills of observation, measurement, recording of data, and analysis of
data. • Use the scientific method to address new biological questions in the laboratory, field, or literature. • Present research data and analysis in written, visual, and oral formats to biologists and to the general
public. • Exhibit ethical reasoning and action, which encompasses the following: scientific integrity in data
collection, analysis, and reporting; laboratory safety; cooperation with others in teams; animal and human safety; and appropriate use of biological knowledge.

7
BIO 151L HUMAN ANATOMY AND
PHYSIOLOGY LABORATORY II
Nazareth College Department of Biology Rochester, NY 14618

8
COURSE DESCRIPTION: This course is a continuation of BIO 150L, Human Anatomy and
Physiology Laboratory I. BIO 151, Human Anatomy and Physiology II, is a co-requisite course. This laboratory is a hands-on course designed to reinforce the principles discussed in lecture. Every attempt will be made to have the laboratory exercises coincide with the related lecture material. TEXT: Human Anatomy & Physiology Laboratory Manual 11th ed., Cat Version – Elaine Marieb &
Susan Mitchell, Authors. NOTE: If you have a different edition/version than the most recent human (main) version, you should still be able to use it; however, the exercise/page numbers will probably not be the same; you’ll have to adjust accordingly based upon the name of the exercise/organ system being studied.
EQUIPMENT: The College will furnish all laboratory equipment, as the laboratory fee covers it. METHODOLOGY/TESTING: The policies of BIO 150L will be followed. Lab examinations will be of the practical type with some question-answer material added to cover the physiological aspects of the exercises. Your final grade will be determined by calculating the average of all your examination scores. MAINTENANCE: The student is expected to keep the laboratory clean. This includes washing all dissecting equipment, trays, tabletops, etc; you mess it up, you clean it up! All animal-type waste should be disposed of in the proper wastebasket. Broken scalpel blades should be disposed of in the appropriate Biohazards Sharps container. HOMEWORK ASSIGNMENTS: There are a number of homework assignments throughout the semester.
They involve accessing the PhysioEx Computer Simulation modules through Mastering A&P. Please obtain the Mastering A&P course ID # from your lab instructor immediately. Each instructor will set up a Mastering A&P site for each section of lab (be sure to get the correct ID# for your section).The instructions for completing these simulations are located in your laboratory manual. You may complete these exercises either during the lab period or on your own outside of class time. After you’ve completed each assignment your grade will appear in the Mastering A&P grade book. The homework assignments are due as listed on the schedule page. Failure to complete all homework assignments will result in a reduction of your final point score in the course.
TYPICAL GRADING SCALE A ≥ 92 A- 88 – 91 B+ 84 – 87 B 80 – 83 B- 77 – 79 C+ 74 – 76 C 71 – 73 C- 68 – 70 D+ 65 – 67 D 63 – 64
9
D- 61 – 62 F ≤ 60 MULTIMEDIA STUDY AIDS:
• Moodle – We have established a course management system at this site. Each laboratory section has its own Moodle site, which is different from the lecture site. You can access this site by clicking on the Moodle course link on the Nazareth College web site (use the “Quick Links” drop down menu). You should have been automatically enrolled in this web site. Your Nazareth College user name and password should allow you access. You should check this site daily for information including related links, messages, and your grades.
• Mastering A&P – We will be using the Mastering A&P website. Your lecture instructors will
provide you the course ID for their section via E-mail. From this site you can access Interactive Physiology, PAL and PhysioEx homework assignments.
• A.D.A.M. Interactive Anatomy Program – This program is available to you on the computers in
the Peckham Hall computer lab and on the computers in the A & P laboratory (P-15). Please be certain to use the Dissectible Anatomy module to help you learn the terminology and gain a reasonably good 3D perspective of the human body. Please see you instructor for further directions.
• Human Anatomy Program – This interactive cadaver dissection program is also available to you
on the computers in Peckham Hall. ACADEMIC INTEGRITY:
Academic integrity is essential to the educational mission of Nazareth College of Rochester, for the free pursuit of knowledge and understanding is seriously impeded by any form of academic dishonesty. Hence, no form of academic dishonesty will be condoned by the college. “Academic dishonesty” is understood as any act of deceit bearing on one’s own or another’s academic work, where “academic work” is understood to mean any activity pertaining to the educational mission of the college. Such acts include, but are not limited to, plagiarism in any form and the use during an exam of information of materials not authorized by the instructor for such use.
BIOLOGY, ENVIRONMENTAL SCIENCE, AND TOXICOLOGY PROGRAM MISSION STATEMENT The mission of the Department of Biology is to enable biology and environmental science majors and non-majors to investigate parts of the natural world which are or were living. Students are engaged in the process of science through challenging courses and undergraduate research experiences. Our faculty fosters collaboration and the development of the problem-solving skills necessary to pursue

10
contemporary questions in biology. Students are prepared to pursue careers in research, health science, and science education.
STUDENT LEARNING OUTCOMES NAZARETH COLLEGE CORE CURRICULUM PERSPECTIVE-ENDURING QUESTIONS STUDENT LEARNING OUTCOMES: Students should be able to:
• Identify, evaluate, and engage in scientific and empirical modes of inquiry. BIOLOGY, ENVIRONMENTAL SCIENCE, AND TOXIOCLOGY PROGRAM STUDENT LEARNING OUTCOMES (PSLOs): Upon completion of the programs specified above students should be able to:
• Describe and analyze biological phenomena at the cellular level • Describe and analyze biological phenomena at the organismal level • Describe and analyze biological phenomena at the ecological level • Describe the central role of evolution in biology • Perform the basic laboratory skills of observation, measurement, recording of data, and analysis
of data • Use the scientific method to address the student's own biological questions in the laboratory,
field, or literature • Demonstrate competency in scientific writing through formal assignments • Present research data and analysis in written (W), visual (V), and oral (O) formats to biologists
and/or the general public • Acquire competency in laboratory safety relevant to each laboratory course • Exhibit ethical reasoning and action, which encompasses one or more of the following: scientific
integrity in data collection, analysis, and reporting; cooperation with others in teams; animal and human safety; and appropriate use of biological knowledge

11
BIO 151L – STUDENT LEARNING OUTCOMES Using a combination of cat cadavers, human anatomical models, and computer programs, students who have completed Human A&P II laboratory will be able to:
1. Identify the anatomical components and describe the general physiology of the endocrine system. 2. Identify the components and describe the general physiology of blood. 3. Identify the anatomical components and describe the general physiology of the heart. 4. Complete and analyze a simple 3-lead ECG on a human subject using CardioComp® 5. Identify the major arteries and veins and describe the general function of blood vessels 6. Measure standard cardiovascular physiology variables (BP, HR) 7. Identify the anatomical components and describe the general physiology of the respiratory
system. 8. Measure respiratory rates, volumes and capacities on a human subject using iWorx Labscribe®. 9. Measure the rate of CO2 production using an acid/base titration system on a human subject at
rest and after hyper and hypoventilation conditions are induced. 10. Identify the anatomical components and describe the general physiology of the digestive system. 11. Identify the anatomical components and describe the general physiology of the urinary system. 12. Complete a detailed urinalysis on themselves. 13. Identify the anatomical components and describe the general physiology of the reproductive
system.

12
STUDENT RESPONSIBILITY STATEMENT FOR WORKING WITH BODILY FLUIDS
Guidelines: During this semester in Human Anatomy and Physiology Laboratory II (Bio 151L) at Nazareth College of Rochester, we will be working with human body fluids, specifically, human urine. It is imperative that body substance isolation (BSI) precautions (specifically, latex, vinyl or other synthetic gloves) be taken, and that the student works ONLY with his or her own urine while conducting these laboratory procedures. Any objects that have been exposed to human urine (e.g. test tubes, test strips, specimen cups, etc.), must be disposed of in the proper biohazard bag provided in the laboratory classroom. Waste urine is to be disposed of ONLY in the restroom toilets. I have read, understand, and agree to comply with the above guidelines. Signed: _______________________________________ Date: ________________________________

13
ATTACHMENTS
Bio 151L – Human Anatomy & Physiology II – Heart & Blood Vessel Identification List – Use Marieb’s Lab Manual:
Cat Version - note: use A.D.A.M, Human Anatomy (Gold Standard Media – both are on the computers in Peckham Hall) and your lab manual to help you identify the human structures on the cadavers
Week 2
Cat Heart
• L & R Ventricles • Auricles of L & R Atria • Anterior interventricular sulcus • Superior & Inferior vena cavae • Ascending/descending aorta & aortic arch • Brachiocephalic artery (trunk) • Left subclavian artery • Coronary arteries
Sheep Heart – students should use the figures to identify: External
• Aorta • Pulmonary trunk • Superior/Inferior vena cavae • Anterior/posterior interventricular sulci • L & R ventricles • L & R auricles/atria • Ligamentum arteriosum
Internal • L & R ventricular chambers • Interventricular septum • L & R atrial chambers • Interatrial septum • R & L - AV valves • Aortic & pulmonary semilunar valves • Papillary muscles • Chordae tendineae • Trabeculae carneae • Pectinate muscles • Moderator band (septomarginal trabeculae) • Fossa ovalis

14
Week 3 – Exercise 32: (Human) and Exercise 4: (cat)
Arteries of the Ventral Body Cavity & Lower Extremities • Ascending/descending aorta & aortic arch • Brachiocephalic artery • L & R subclavian arteries • L & R common carotid arteries • Coronary arteries • Thoracic aorta • Internal thoracic (mammary) artery • Abdominal aorta • Celiac trunk
o Left gastric artery o Hepatic artery o Splenic artery
• Superior mesenteric artery o Intestinal arteries
• Adrenolumbar arteries • Renal arteries • Genital (Gonadal) arteries • Inferior mesenteric artery • Iliolumbar arteries • External iliac arteries • Internal iliac arteries • Common iliac artery (human only) • Femoral artery • Popliteal artery • Saphenous artery (cat only) • Anterior/posterior tibial arteries • Deep femoral (a.k.a. profunda femoris or deep artery of the thigh) artery (human only) • Peroneal artery (human only)
Veins of the Ventral Body Cavity & Lower Extremities • Superior/inferior vena cavae • L & R subclavian veins • Intercostal veins • Internal thoracic (mammary) vein • Azygous vein • Phrenic veins • Hepatic veins • Adrenolumbar veins • Renal veins • Genital (Gonadal) veins • Iliolumbar veins • Common iliac veins • External/internal iliac veins • Femoral veins • Popliteal veins • Great saphenous veins • Anterior/posterior tibial veins
15
• Peroneal veins (human only)
Week 4 - Exercise 32: (Human) and Exercise 4: (cat) Arteries of the Head, Neck, and Upper Extremities • Brachiocephalic artery • Common carotid arteries • Subclavian arteries • External carotid arteries • Internal carotid arteries • Superior/Inferior thyroid arteries • Lingual arteries • External maxillary arteries • Vertebral arteries • Thyrocervical trunk • Costocervical trunk • Transverse scapular arteries • Subscapular arteries • Internal mammary (thoracic) arteries • Axillary arteries • Brachial arteries • Radial arteries • Ulnar arteries Veins of the Head, Neck, and Upper Extremities • Brachiocephalic veins • Subclavian veins • External jugular veins • Internal jugular veins • Anterior facial veins • Posterior facial veins • Inferior thyroid vein • Vertebral veins • Transverse scapular veins • Axillary veins • Subscapular veins • Long thoracic veins • Internal mammary veins • Median cubital veins • Radial veins • Ulnar veins • Costocervical vertebral trunk Hepatic Portal System • Hepatic portal vein • Gastrosplenic vein • Anterior pancreaticoduodenal vein • Posterior pancreaticoduodenal vein • Superior mesenteric vein • Intestinal branches • Inferior mesenteric vein

16
HUMAN ELECTROCARDIOGRAM 1USING THE CARDIOCOMP SYSTEM
MATERIALS Cardiocomp hardware & software Dell Wireless Notebook computer For the human heart to work efficiently, the contractions of muscle fibers in both the ventricles and atria must be strictly coordinated. This coordination is achieved with the intrinsic conduction system or nodal system of the heart, consisting of a group of highly specialized, non-contractile cardiac muscle fibers that can conduct electrochemical impulses. The electrochemical stimulus for heart muscle contraction begins in a specialized group of cells called the sinoatrial (SA) node, located in the superior wall of the right atrium. From the SA node, the impulse is transmitted throughout the atrial muscle. Just before the atria contract, the impulse reaches another group of specialized fibers located in the lower atrial septum, the atrioventricular (AV) node, where the impulse is stalled just long enough for the atria to contract simultaneously. From the AV node, the impulse continues to the AV bundle (bundle of His) then the right and left bundle branches, located in the interventricular septum. The impulse continues throughout the ventricular myocardium via the Purkinje fibers. The highly ramified Purkinje fibers cause depolarization of ventricular myocardium, and the ventricles contract simultaneously.
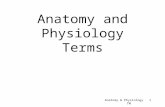
The electrical activity of the nodal system spreads throughout the body, and such activity can be measured on the body’s surface with an electrocardiograph. This device contains a signal amplifier to boost the electrical signal from the nodal system of the heart transmitted to electrode plates placed on the body’s surface. The amplified signal is then displayed on either a strip chart recorder or a digital computer. The graphical representation of this electrical activity is called an electrocardiogram (ECG) (Fig. 6.1). Three deflection waves are visible on an electrocardiogram. The first wave, called the P wave, represents the depolarization of atrial conduction system fibers just before the atria contract. The second set of waves, the QRS complex, represents depolarization of the ventricles just prior to ventricular contraction. Finally, the T wave represents repolarization of the ventricles. Atrial repolarization occurs during ventricular depolarization and is thus obscured by the QRS complex.
The ECG is a diagnostic tool used to detect myocardial infarcts (tissue death) and problems with the intrinsic conduction system. The P-R interval represents the time between atrial depolarization and ventricular depolarization. An abnormally long P-R interval may indicate a partial AV (first-degree) block caused by damage to the AV node or weak SA impulses. An abnormally long QRS interval may indicate a right or left bundle branch block where one ventricle is contracting later than the other.
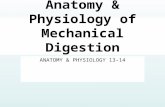
The normal anatomical axis of the heart, measured from the middle of the base to the apex, is approximately 55o (with the apex pointing toward the left). The electrical axis of the heart, normally ranging between 0 and 100o and averaging around 59o, closely approximates the anatomical axis (Fig.6.2). Measuring the electrical axis, therefore, can help to diagnose anatomical abnormalities of the heart. Electrical axis deviation can be caused by changes in heart position, ventricular hypertrophy, or ventricular destruction. When one ventricle hypertrophies (enlarges), the electrical axis shifts toward the hypertrophied side because of the greater time required for depolarization of the increased muscle mass. Subsequently, right ventricular hypertrophy results in right electrical axis deviation and left ventricular hypertrophy results in left axis deviation. Tall, lanky people, whose anatomical heart axis typically is more vertical, have an electrical axis shifted to the right. Conversely, short, obese people, whose diaphragms push upward on the heart, have both anatomical and electrical axes shifted toward the left.
1 Refer to pages 457-466 in Marieb’s Human A&P Lab Manual

17
Figure 6.1. A normal electrocardiogram (ECG).
Figure 6.2. The Electrical and Anatomical Axes of the Heart

18
Procedure - The Electrocardiogram and Mean Electrical Axis of the Heart
In this exercise, you will record the electrical activity of the heart using body surface electrodes and Cardiocomp® technology coupled to the Dell Wireless Notebook computers. The most reliable ECG recordings made with the subject fully reclined and completely relaxed to minimize contributions from skeletal muscles. Begin by having the subject remove their wristwatch and any jewelry then expose both wrists and ankles. Clean the inside of each wrist, ankle, and anterior shoulder with rubbing alcohol. The electrode pads we will be using are pre-treated with electrode gel, and are affixed to the skin with the pre-applied adhesive. The ECG wires are attached to the electrode pads with snaps. 1. Connect the Cardiocomp ECG probe to the data acquisition module. 2. Click on the Intelitool Cardiocomp icon on the desktop. 3. Follow the instructions in the handout for recording, analyzing, and printing your results. Electrical axis _________________o Normal Axis Range – 0-100o; Average – 59o PR Interval ____________sec Normal PR Interval – 0.16-0.18 sec QRS Interval __________sec Normal QRS Interval – 0.06-0.010 sec QT Interval __________sec Normal QT Interval – 0.31-0.41 sec

19
THE ROLE OF THE RESPIRATORY SYSTEM IN ACID/BASE BALANCE
The respiratory system is intimately involved in regulating the blood pH. The respiratory (physiological) buffer system can be two times more powerful than chemical buffer systems. Alveolar ventilation rate can be increased approximately 15 times to compensate for changes in blood pH. Respiratory system control of hydrogen ion concentration is a quick response system (approximately one minute) that functions in accordance with the following chemical reaction:
Carbonic Anhydrase
CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3-
An increase in [H+] shifts reaction to the left, more CO2 is formed & voided via increased respiratory rate.
Normally, the rate of ventilation is matched to the rate of CO2 production by the tissues, so that the carbonic acid, bicarbonate, and H+ concentrations in the blood remain in the normal range. If hypoventilation occurs, however, the carbonic acid levels will rise above normal and the pH will fall below 7.35. This condition is called respiratory acidosis. Hyperventilation, conversely, causes an abnormal decrease in carbonic acid and a corresponding rise in blood pH. This condition is called respiratory alkalosis. Respiratory acidosis or alkalosis thus occurs when the blood CO2 level (measured as the partial pressure, PCO2, in mm of mercury [Hg]) is different from the normal value (40 mm Hg) as a result of abnormal breathing patterns. Procedure 1. Fill a beaker with 400 ml of distilled water, and add 1.0 ml of 0.10 N NaOH and a few drops of
phenol red (or 10 mg phenolphthalein) indicator. This indicator is red (or pink) in alkaline solutions (range 8-10; PKA = 9.4) and yellow (or clear) in neutral or acidic solutions. Divide this solution into four beakers.
2. While sitting quietly, exhale through a glass tube or straw into the solution in the first beaker.
Using a stopwatch, note the time it takes to turn the solution from red to yellow and record this time in the table below.
3. Exercise vigorously for 5 minutes on the Harvard step. Exhale through a glass tube or straw into
the second beaker, and again note the time it takes to make indicator change color. 4. Hyperventilate for 10-20 seconds by taking short inhalations and rapid, forceful exhalations (be
careful, as you may begin to feel light-headed if you hyperventilate correctly), then exhale through a glass tube or straw into the third beaker, and again note the time it takes to make indicator change color.
5. Breath into a paper bag for 1-3 minutes, then exhale through a glass tube or straw into the fourth
beaker, and again note the time it takes to make indicator change color.
20
ACTIVITY
TIME TO COLOR CHANGE (sec)
Resting
Post-Exercise
Hyperventilation
Breathing into paper bag

21
KIDNEY REGULATION OF FLUID AND ELECTROLYTE BALANCE2 MATERIALS Distilled water or bottled spring water 0.9% and 2.0% saline (NaCl) solutions 0.2% NaHCO3 solution or club soda or lemonade Wide-range pH paper or pH meter Refractometer Wax marking pencils Colored pencils 20% potassium chromate in dropper bottle 2.9% AgNO3 in dropper bottle (made fresh daily) 500 ml beakers 1000 ml beakers 100 ml graduated cylinders (meticulously cleaned) 500 ml graduated cylinders (meticulously cleaned) Test tubes Test tube racks Test tube holders Stoppered flasks Laboratory bucket with 10% bleach solution
2 Modified from Marieb, Human Anatomy and Physiology Laboratory Manual, Benjamin Cummings, CA.
22
REGULATORY MECHANISMS A major role of the kidney is to keep the solute concentration, or osmolarity, of the body fluids at a relatively constant level (approximately 300 milliosmol/liter), thus maintaining adequate body hydration and avoiding both dehydration and water intoxication. Hormones regulate the reabsorption into the blood stream of water and electrolytes by the kidney. Water reabsorption is influenced primarily by antidiuretic hormone (ADH a.k.a. vasopressin), which is released by the posterior lobe of the pituitary gland (or neurohypophysis). Sodium reabsorption is influenced primarily by aldosterone (a mineralocorticoid), which is produced by the adrenal cortex.
ADH enters the blood when specialized neurons (osmoreceptors) in the hypothalamus are stimulated by an increase in the osmotic pressure of the blood (that is, increased solute concentration and decreased water concentration) as might occur in dehydration. In the kidney, ADH increases reabsorption of water primarily by acting on the collecting tubules to increase their permeability to water. The net result of this mechanism is that the water content of the blood (and pressure) increases, osmotic pressure decreases, and a small volume of highly concentrated or hypertonic urine is excreted. ADH is released continually except when inhibited by a decrease in blood osmotic pressure. In the absence of ADH release, for example in the hormonal imbalance known as diabetes insipidus, large volumes (up to 25 liters) of very dilute urine are lost daily.
A decrease in blood volume or blood pressure, an increase in K+ in the plasma, or a decrease in blood sodium may initiate the release of aldosterone from the adrenal cortex. Any or all of these factors cause specialized cells in the kidney's juxtaglomerular apparatus to release the enzyme called renin. Once released, renin catalyzes a series of reactions leading to the formation of a molecule called angiotensin II in the blood. Angiotensin II has two major functions: it acts directly on vascular smooth muscle to cause vasoconstriction, producing an increase in systemic blood pressure, and it stimulates the release of aldosterone from the adrenal cortex.
Sodium is the most important plasma ion that has to be regulated; normally, it is reabsorbed actively along the entire length of the nephron tubules. In the presence of aldosterone, the renal reabsorption of sodium increases even more, especially in the distal convoluted tubule. This mechanism helps to prevent a deficit of sodium in the blood, which would result in the dilution of body fluids and a loss in plasma volume to the body tissues, leading to edema and possible circulatory collapse. For each sodium ion that is reabsorbed, another cation, often a potassium ion is secreted into the filtrate. Thus, as the Na+ concentration in the blood increases, the K+ concentration decreases, bringing these two ions back into their normal electrolyte balance in the blood. If ADH is present in high concentration along with aldosterone, sodium is reabsorbed in response to aldosterone and water follows sodium. The net effect is an increase in blood volume, which automatically causes an increase in blood pressure. This mechanism is used, for example, during massive hemorrhaging when blood volume and pressure drop substantially. The combined effect of the ADH/aldosterone system is to elevate blood pressure to compensate for blood loss.
The volume and specific gravity of urinary output are important indications of a person's state of hydration. In individuals with excessively low fluid intake, the urine is much reduced in volume and its specific gravity is high. Conversely, if the fluid intake is excessive, a large volume of low-specific gravity urine is excreted.
23
Procedure - Effect of Fluid and Salt Load on Urinary Output and Characteristics As you investigate the alterations in volume and urine composition the kidneys make under conditions of known fluid and salt load, you should work in pairs but handle only your own urine sample and use latex gloves. Dispose of all specimen cups in the orange autoclave bag. Ideally, a minimum of three students will conduct each of the four procedures. The results should be recorded on the data sheet provided below. When you have completed the experiments, graph the results in Microsoft EXCEL. 1. Each student should void into a clean 500-ml plastic specimen cup before beginning the
experiment. Save this urine, label it with your name, the word "control", and the time of collection. You should use the sample labeled control from the urinalysis portion of this exercise. You will need this sample for tests to be performed in the time intervals between experimental sample collections and testing.
2. Consult the list that follows, which indicates the experimental conditions (treatment) for each
group member. There should be at least 3 students (replicates) for each treatment. Each student is to drink the designated amount of one of the solutions in as short a time as is comfortable. Do not attempt to drink the solution too rapidly, as this may cause emesis or vomiting.) After drinking the solution, record the time, and then void at 30-minute intervals for a period of 90 minutes after obtaining the control sample. Collect each voiding in a pre-marked specimen cup (labeled with your name, time of collection, solution drunk) and record the volume. If you are unable to void at any predetermined collection time, retain the urine in your bladder until the next half-hour collection interval.
Treatment #
Solution & Volume to be Drunk
1
700 ml distilled water (or bottled spring water)
2
500 ml 0.9% saline solution
3
150 ml 2.0% saline solution*
4
500 ml 0.2% sodium bicarbonate solution (or lemonade)
* The 2.0% saline solution is difficult to ingest. If any nausea, vomiting, or abnormal cramping occurs, discontinue the experiment. 3. Make the following observations or tests on each sample collected and on the control sample.
Record the results on the appropriate column of the data sheet. Transparency: Record as clear or cloudy Color: Record as pale, medium, or deep yellow Volume: Measure the volume of the urine sample collected and calculate the rate of urine
formation. Divide the total volume collected in the 30-minute interval by 30 to determine ml/min excreted.

24
pH: Use wide-range pH paper or a pH meter to determine pH. Be sure to rinse the pH meter thoroughly with distilled water when finished.
Specific Gravity: Place a drop of the sample in a refractometer and read the specific gravity
through the viewing window of the apparatus. Be sure to rinse the refractometer thoroughly with distilled water when finished.
Chloride: Knudsen Procedure: Using a medicine dropper, put 10 drops of urine into a test
tube, add 1 drop of potassium chromate, and then add AgNO3, 1 drop at a time. Count the number of drops necessary to change the solution from bright yellow to brown. Each drop of the 2.9% AgNO3 solution required to bring about this color change corresponds to 1 g/L of NaCl in the urine (or 1000 mg/1000 ml). For example, if 5 drops were required to titrate the sample, then the NaCl concentration of your urine is 5 g/L (or 5000 mg/1000 ml). Calculate the total number of mg of NaCl per ml in the sample and enter the information on the data sheet.
Urea a) Put two drops of urine on a clean microscope slide and carefully add two drops of concentrated
nitric acid to the urine. b) Slowly warm the mixtures on a slide warmer tray until it begins to dry at the edges, but do not
allow it to boil or to evaporate to dryness.
c) When the slide has cooled, examine the edges of the preparation under low power to identify the rhombic or hexagonal crystals of urea nitrate, which form when urea and nitric acid react chemically. Keep the light low for best contrast. Record your results.
4. When all the information has been collected, complete your data sheet with information from other
students in the group, and make a graphic analysis of the group results. Make four separate plots as indicated below for the averages from each set of test results using Microsoft EXCEL.
• Specific Gravity vs. Time
• ml/min vs. Time
• mg NaCl/ml vs. Time
• pH vs. Time
5. Rinse the glassware used to collect or measure urine samples and place it in the bleach-
containing bucket. Wash the laboratory bench with bleach solution before leaving the laboratory.