How to Maximize Resources, Optimize Quality and …...How to Maximize Resources, Optimize Quality...
129
How to Maximize Resources, Optimize Quality and Minimize Costs in the Coagulation Laboratory- by the Laboratory Whisperer Donna D Castellone, MS, MT(ASCP)SH QA Manager, Specialty Testing Supervisor, Special Coagulation [email protected]
Transcript of How to Maximize Resources, Optimize Quality and …...How to Maximize Resources, Optimize Quality...

How to Maximize Resources, Optimize Quality and Minimize Costs in the Coagulation Laboratory- by the Laboratory Whisperer
Donna D Castellone, MS, MT(ASCP)SHQA Manager, Specialty TestingSupervisor, Special [email protected]

Why a whisperer
• Excels at calming or training hard to manage animals/laboratories/people using non-coercive methods based especially on an understanding of the animals/laboratories/people natural instincts.

Objectives:
• Identify processes within the laboratory that can benefit from root cause analysis and corrective action plans
• Perform best coagulation practices that can help to maximize outcomes and minimize costs by understanding how reagent and interfering substances can impact testing.
• Determine testing algorithms that will identify and optimize test utilization providing the best outcome for patient care.

Case Study
• Sample is sent to the laboratory on an in-house patient
• aPTT is prolonged at 66.4 sec. ( 27-36sec)
• Ordered factor assays: VIII, IX, XI and XII
• Results:Factor 1:10 1:20 1:40
VIII 35 56 78
IX 20 55 82
XI 40 69 76
XII 44 55 66

Case Study
• How do you report these results?
• Looks like an inhibitor?
• Perform a mixing study?
• Do Lupus testing?
• Can you order a workup for a prolonged aPTT, and figure it out?
• Do you test what is ordered regardless?
• Cost/benefit
• Technical time??? Results to the patient???

Case Study
• Important clues: in-patient and inhibitor effect
• The most underused test in the coagulation laboratory-
• Before conducting expensive and time consuming assays
• Do the thrombin time-
• Result PNP= 15 sec (< 21 seconds)
Patient=52 sec

Case Study
• The thrombin time is the best test for residual heparin
• Most likely this sample is contaminated with heparin, or possibly a direct thrombin inhibitor
• If you perform the TT first, you could avoid unnecessary additional testing.
• Wasting reagents and technical time
• Check patient records, patient is on heparin
• Therefore no factor assays should have been done.

New shipment for lot of FVIII deficient plasma
• New lot of reagents have already been validated with this lot of plasma
• However, a new shipment of factor VIII is being used.
• New shipment is evaluated:
FVIII Old lot New Lot % difference acceptable
Abnormal control
42 % 41% 1% y
Normal control 98% 100% 2% y
Abnormal patient
35% 22% 37% n
Normal patient 123% 97% 21% n

Can I use these reagents?
• Controls are within range- patient samples are not within range-
• FVIII is heat labile, maybe the samples are bad?
• Tested another normal and abnormal patient sample
• still out of range-
• Check independent controls: FFP, kept at -70 degrees C

Results
FVIII Control result old
Control result new
% difference acceptable
Abnormalcontrol
34 21 38% n
Normal control 98 77 21% n

New lot of reagents, not a lot of historical data• Recalibrated, no change
• Could it be the reagents? All other aPTT based assays were working fine.
• However, did reconstitute new reagents, still no change
• Bad lot of deficient plasma- same as previously used-
• Possible shipment issue- got a new lot/shipment-
• All results were within acceptable levels
• MUST test both patient and controls-
• Should have independent controls on hand
• Also can test PT material- can be very helpful in troubleshooting

Case Study
• 16 year old male for a hernia operation
• Family has a positive history of bleeding
• Results: PT=12.9 (10.2-13.5)
APTT=33.0 (29.9-33.5)
Will this patient bleed?
Do we check for a factor deficiency?
What is the most important information when evaluating if a patient will bleed?

The Coagulation Cascade
XIIPrekallikreinHMWK
XI XIa Tissue FactorVIIa
IX IXaVIIIa
X Xa X
VaProthrombin Thrombin
Fibrinogen Fibrin
IntrinsicPathway
Extrinsic
Path
way
Common Pathway

In Vitro Cascade
• Allows logical effective lab based screening
• Can be evaluated through the PT & APTT
• Doesn’t reflect clotting physiologically
• Does play a role in laboratory evaluation of a potential clotting disorder

Results:
• Look at APTT factors: VIII, IX and XI
• VIII = 102% (50-150%)
• IX= 84%
• XI=21%
• Abnormal level of factor XI despite the normal APTT
• Patient is deficient in factor XI
• Shouldn’t the APTT have been abnormal

How are your reagents?
• Do your reagents truly reflect normal factor levels
• Normal PT & APTT levels indicate patient have a minimum of ~ 30-35% of factor levels present
• If your reagent is insensitive to a factor, you may get a normal PT or APTT
• The reagent may not be able to pick up a factor level below 30%
Test reagent sensitivity for factors
• Dilute normal plasma with factor deficient plasma at different levels
• Run either a PT or APTT on the sample
• Compare the results to the upper limit of the normal range
• You may get a normal PT or APTT with an abnormal % factor level

What to do?
• Factor XI Sensitivity: APTT= (29.5-33.5)
Normal + Deficient = % Activity APTT
plasma plasma
500ul 0ul 100% 29.0
250ul 250ul 50% 31.0
125ul 375ul 25% 32.0
62.5ul 437.5 12.5% 36.0
This reagent does not reflect an abnormality until 12.5%

Reagent sensitivity: point which APTT is outside normal range:
Reagent Sensitivity
Ppl
source
Contact % F VIII % F IX % F XI % F XII
RB Silica 50 20 50 40
BB Silica 60 20 60 60
RB Ellagic 40 30 50 40
Soy Ellagic 60 50 60 60
RB/Soy Ellagic 60 30 60 40
BB EA/Kao 50 10 60 30
Ruiz, JA., Limerick, KK, Utility of the APTT: Evaluation of ContactActivation and Other Clinical Conditions, Clinical Hemostasis Review,February 1994, pg12.

Factor Sensitivity
• It is important to understand how your reagents perform
• Small investment for a lot of information
• Should be performed even if you do not run factor assays
• Will this patient bleed? Should he have a further work up-
• FH is positive; FXI deficiency occurs in up to 8% of Ashkenazi Jews
• Incidence is estimated at 1 in 100,000 in the general population. In
• FXI deficiency is inherited in an autosomal recessive pattern,
• Men and women are affected equally.

FXI deficiency
• FXI deficiency can manifest first as a bleeding disorder or as an incidental laboratory abnormality.
• The bleeding manifestations can present at circumcision (rarely) or much later in life during elective surgery.
• An unexpected and incidental preoperative finding of a prolonged activated partial thromboplastin time (aPTT) can be quite disruptive and may prevent the scheduled surgery.
• Bleeding associated with FXI deficiency is predictable neither within a patient nor within a family. In contrast to hemophilias A and B, bleeding manifestations in hemophilia C do not correlate with the FXI level.

How do you use this information?
• 17 yr old male with traumatic injuries required surgery
• PT= 15.6 sec (12-14.5 sec) aPTT = 31.8 sec (27-35 sec)
Factor 100% 75% 50% 35% 20% 15% 5% 0%
II 13.1 11.8 11.9 12.7 14.4 18.3 26.8 112.6
Factor 100% 75% 50% 35% 20% 15% 5% 0%
V 13.2 13.5 14.3 16.2 18.3 18.5 24.2 54.6
Factor 100% 75% 50% 35% 20% 15% 5% 0%
VII 13.3 14.2 15.3 17.6 20.7 20.3 28 76
Factor 100% 75% 50% 35% 20% 15% 5% 0%
X 13.6 13.9 15.3 16.5 19 21.6 28.9v max

APTT based factors
Factor 100% 75% 50% 35% 20% 15% 5% 0%
VIII 30.2 31.5 32.6 34.5 37.1 38.4 46.2 82.3
Factor 100% 75% 50% 35% 20% 15% 5% 0%
IX 30.1 30.6 32.4 34.4 37.4 38.5 46.1 115.6
Factor 100% 75% 50% 35% 20% 15% 5% 0%
XI 29.9 30.9 33.2 35.7 39.5 41.9 50.2 79.3

Review of factor sensitivities
• Can give a ball park figure to show approximate levels of factor activities.
• In particular, if a mixing study can’t be done-
• But what if this is an inhibitor?
• Lupus is unlikely in a prolonged PT, also they tend to be thrombotic, not a bleed.
• Most factors are at least at 30% sufficient levels patient should not bleed.

Case Study :
• Pre-operative patient APTT 49.1 (25-36 seconds)
• No history of bleeding
• No medications
• What can prolong an APTT
• Pre-analytical variables- short draw
• Presence of heparin
• What factors deficiencies may prolong the APTT?
• Those in the Intrinsic pathway: VIII, IX, XI, XII
• An APTT may also be prolonged due to an inhibitor

Prolonged screening test:
• Next step is to perform a mixing study
• Correction: factor deficiency ( patient may bleed, unless FXII)
• No correction: inhibitor ( more likely a risk for thrombosis, unless specific factor inhibitor, then they can bleed)
• Do you use FFP for the mixing study, can I use a lyophilized standard human plasma?
• Do I incubate? How long?
• Do I incubate separately? Together? Both?
• Is this test cost effective? What information do I get from it?

Classical 1:1 Mixing Study
Step 1: Immediate Mix
Patient PNP
C
1:1 Mix
1. Test all.
2. Compare C to A & B.
Did C correct?
3. Incubate all.
A B
Step 2: Incubated Mix
1-2 hrs, 37C
Patient PNP
C
Incubated Tubes
A B D
Control
1. Test all.
2. Compare incubated C to D. Is it
prolonged? Yes, possible time
dependent inhibitor.
3. Interpret final results
Mix

Results:
• APTT = 42.1 seconds (25-36 seconds)
• Pooled Normal Plasma =31.5 seconds
• Mixing study 1:1 = 36.5
• Is this a correction?

Interpretation of a Mixing Study
• Based on PT or aPTT normal range
• Within limits @ 2SD or 3SD
• Within 5 seconds of the 2SD upper limit
• Rosner Index
• 1:1 mix
• Index = CT of 1:1 mix – CT of NPP x 100
CT of patient <15 = FD >15 = Inhibitor
• NPP tested with Mixing Study
• Within 5 seconds of NPP value
• 10% of NPP value
• Lack of correction @ >15% of NPP
• No recommendations or guidelines from ISTH Scientific & Standardization Committee CAP Coagulation Resource Committee

Variables affecting mixing studiesHeparin, OAC, DTI……..ideally do not perform
Pre-analytical variables the same as PT & APTT PPP critical for proper id of LA
Reagent Sensitivity Level where factor deficiency prolong assay LA sensitivity depends on concentration & type of phospholipid in
APTT reagent
Normal Pool Plasma Fresh/frozen human plasmaMinimum 20 normal individuals (not normal patients)Must by PPP (<5 x 109/L) Normal value within the normal range of PT or APTT

What do you do to standardize this test?
• Adhere to consistent policies in your laboratory- define your criteria and stick to it
• Eliminate the possibility of heparin being on board, perform a thrombin time
• Eliminate the test, many laboratories feel it is too confusing, and just proceed with additional testing

What do we have?
• A repeat APTT that is still prolonged 42.1 seconds (25-36 seconds)
• PNP =31.0 seconds, mixing study is 36.4 seconds 5.5 seconds from PNP
• > 5 seconds from PNP
• > normal range
• Not a correction
• Proceed with inhibitor testing
New Lot of quality control:
• Laboratory regulations: run control 20 times to demonstrate the ranges.
• Do I have to use these ranges?
• How do I run my 20 points?
• Over 20 days- or 5 times over 4 days
• Can I use the manufacturers range?

Results for FX normal control:Manufacturers range: 80-120 sec.FVIII DAY 1 DAY 2 DAY 3 DAY 4
95 93 95 96
94 94 96 95
95 95 95 95
94 93 96 96
94 94 95 96
Mean 95 % - range 85-105

Review of the first month:
• Mean 102%
• Out of 30 days- 10 days spent, re-running controls-
• Wasting time and reagents to get controls within range
• This was happening throughout all of the laboratories

What is the problem with this?
• We do fair amount of FX’s – probably due to order entry errors
• If you review the 20 control runs, looks like a precision run
• Not unique to coagulation- all disciplines
• If we would enter these ranges, we would spend a lot of time and money and effort in having techs re-run, re-calibrate and hold up the runs.
• Running 20 controls was not working.

Solution:
• We still run the 20 points, however we use this as a verification of the manufacturer’s ranges.
• The first month, we enter the manufacturers ranges.
• After a month of running in a real world setting, we re-evaluate the “true” ranges.
• Much less time wasted on trying to hit a “perfect target” which did not really reflect the testing environment- your analyzer, your reagents in your lab, with different operators.

Case Study
• A pediatric samples from a 3 month old sent to laboratory for testing
• Lupus work-up
• Issues with pediatric samples:
- small volume
- different ranges ( use published ranges)
- contaminated with heparin
• Transient? True LA?
• Little to no patient information

Results
• PT= 16.1 APTT=54.7
• 1:1 mix = 15.9 & 52.1
• Continue LAC work-up
• Drvvt screen= 114.0 sec (abn)
• Drvvt confirm= 128.0 ratio= 0.9; neg
• Hexagonal phase= positive (strongly 21.9 sec)
• Lupus, right?

Result Review
• Principle of DRVVT, is screen uses low concentration of ppl, prolongs result
• Confirm uses high concentration result should shorten
• Very prolonged results, confirm is longer than screen
• Different than APTT - suspicious.....

Factor Assays also performed
Factor 1:10 1:20 1:40
VIII 45% 65% 90%
IX 32% 46% 62%
XI 50% 71% 94%

Additional information
• Looked like an inhibitor, was heparin on board
• Thrombin time = 18.1 sec PNP=13.8 sec.
• Normal range for TT < 21 seconds
• Running out of sample
• Techs were running out of patience

Additional Information
• HIT testing
• Positive for HIT
• Patient not on Heparin
• Patient was on Argatroban
Baby had HIT, put on a DTI, laboratory not notified, caused abnormal results
Inhibitor seen-
No LAC
TT did not pick up the DTI?

Direct Thrombin Inhibitors (DTI's)
Alternative to heparin for the treatment of PCA
1. Directly bind to and inhibit thrombin’s interaction with its substrate
2. Action not mediated through antithrombin
3. Do not interact with other plasma proteins
4. Do not interact with PF4
5. Inactivate fibrin-bound thrombin and fluid-phase thrombin
6. Direct inhibitors
1. Argatroban
1. Bivalirudin
FDA approval for the treatment of HIT
44

ARGATROBAN - Novastan
• Synthetic small molecule, derived from arginine
• Direct thrombin inhibitor
• 1/2 life of 30-40 minutes
• Metabolized by the liver
• Approved for use in HIT

What do direct thrombin inhibitors do?• PT/INR, APTT prolonged, remain prolonged in
mix
• Acts like an inhibitor in clotting-time assays, under-estimating results
• Fibrinogen falsely low
• C & S, overestimated
• ATIII - has “anti-thrombin” activity, Increased-
• Heparin - anti-Xa, is okay, unless IIa
Walenga, J., (2006) Direct Thrombin Inhibitors & Laboratory Monitoring Issues,
Coagulation Symposium, Indianpolis, May 5.
Assay Insensitivity:
• Many reagents are insensitive to DTI’s
• The APTT reagent should be tested to determine where the insensitivity occurs
• For many reagent at 0,8mg/L the reagent is flat
• Leads to a potential to miss overdosing a patient
• Spike PNP with known concentrations of DTI and run the APTT
Jensen, R., (2003), Novel Anticoagulants used in the Therapy of Thrombotic
Disease, Clinical Hemostasis Review, 17 (8) 1-6.

APTT versus ARGATROBANArgatroban spike versus APTT
0
10
20
30
40
50
60
70
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8
Argatroban (ug/ml)
AP
TT
: (s
eco
nd
s)
Castellone, DD., Peerschke, EIB,(2006)A chromogenic method for quantitation of direct thrombin inhibitors: A case study, ISTH, abstract, Geneva,

Argatroban Laboratory Monitoring
• aPTT was recommended to be used:
• Baseline aPTT performed 2 hours after infusion is started
• aPTT range 1.5-3.0 times baseline
• Further studies have demonstrated that this is reagent dependent, APTT can flatten out and not reflect an increased dose, can have dangerous outcomes
• Ecarin clotting time
• Linear, may be substituted when APTT is not usable
• Activated clotting time (ACT)
• Used during very high levels of Argatroban during percutaneous cardiac intervention
• Maintain ACT 300-450 seconds
• We did not find this to be true, we also found a flattening of the results
• PT/INR cannot be used to monitor Argatroban therapy
• Thrombin time is not linear and can not be used to monitor Argatroban therapy
• When switching from Argatroban to Coumadin, the INR may not be reliable
• Therefore a chromogenic Factor X should be used until the patient of off of Argatroban
49
Not just heparin and coumadin anymore:
Large compendium of anticoagulation
Newest are anti-thrombin's
These direct inhibitors against IIa
Cannot be monitored by an APTT, or a thrombin time

History of anticoagulant therapy
1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Anticoagulant
in spoiled
Anticoagulant
in spoiled
sweet
clover
First clinical use of 4-
hydroxycoumarin
Warfarin
mechanism
elucidated ( Warfarin
dosing/INR
Warfarin
clinical trials
Direct thrombin and Xa
Heparin discovered
by medical student
(McLean)
Clinical use of
heparin
Clinical use of
heparin
Cont infusion of
heparin; aPTT
monitoringLMWH
(J. Hirsch)
LMWH trials
Fondaparinux
trials
HeparinDiscovered by McLean
2011

Anticoagulants:
• Used to prevent clotting by several different mechanisms
• Warfarin Sodium (coumadin): renders the Vitamin K factors non-functional (II, VII, IX and X)
• Heparins: Inhibits actions of IIa and Xa
• Direct Xa inhibitors- inhibits only Xa
• Direct IIa inhibitors – inhibits thrombin
• PT, APTT, TT and anti-Xa not optimum for all new agents

Indications for Anticoagulation
• Treatment and prevention of thrombosis
• Stroke prevention in high-risk patients with atrial fibrillation (AF).
• Long-term oral anticoagulation is also a mainstay in the management of patients with:
• Mechanical heart valves
• Deep venous thrombosis (DVT)
• Pulmonary embolism

The Ideal Oral Anticoagulant
Ideally, an oral anticoagulant would:
• Require no remote monitoring
• Have little interaction with food or other drugs
• Offer a good safety profile with regard to bleeding risk
• Have similar efficacy to warfarin in reducing thromboembolic events
• Reach therapeutic levels within several hours

STEPS IN
COAGULATION
COAGULATION
CASCADE
DRUG
INITIATION TF/VIIaTifacogi
n
NAPc2
FVIIai
PROPAGATION
TTP 889
Protein C
Drotrecogin
(activated)-
alpha
sTM
Fondaparinux
Idraparinux
Rivaroxaban
Apixaban
BAY59-7939
LY 517717
X IX
IXa
VIIIa
Va
Xa
II
IIa Ximelagatran
Dabigatran etexilate
FibrinFibrinogen
THROMBIN
ACTIVITY

Targeting Specific Coagulation Factors
• Newer oral anticoagulants target specific points in the coagulation cascade:
• Factor Xa inhibitors (eg, rivaroxaban, apixaban) target factor Xa, preventing the conversion of prothrombin to thrombin.
• Direct thrombin inhibitors (eg, dabigatran, ximelagatran) target thrombin (factor IIa), blocking the conversion of fibrinogen to fibrin.
• The goal of novel oral anticoagulants is, in part, to offer more specific targeting and to afford more predictable responses than current anticoagulant therapies, such as warfarin, can offer.

Case Study• A 75 year old woman enter the ED after an MVA, multiple trauma
requires surgery
• Patient is currently on dabigatran for AF
• An APTT and Thrombin Time are ordered on the patient. Results are as follows:
APTT= 37.5 seconds ( 26-37 sec)
Thrombin Time= 21 sec (<22 seconds)

What to do?
• Is the anticoagulant on board?
• Is the patient compliant with new OAC’s?
• Use on uncomplicated patients?
• Patient is bleeding, too much on board? Other issues?
• What can be used?

Dabigatran etexilate (Pradaxa)• Oral direct thrombin inhibitor
Prevention of stroke and systemic embolism – nonvalvular AF
• Prodrug – rapidly converted to an active metabolite in the liver
– Does NOT involve cytochrome p450 pathway
• Rapidly acting peak plasma concentration 1.5 hours
• ½ -life 14-17 hours – 2x/day dosing
• Predictable and consistent pharmacokinetic profile
• Not significantly affected by interactions with food
• Eliminated mainly via the kidneys
59

Dabigatran
• Generally does not require monitoring
• However, OAC, is patient compliant?
• Is medication on board?
• INRs should not be used as a measure of the anticoagulant effect
• Modest elevation of INR, variable and cannot be predicted
• aPTT can provide a qualitative indication of anticoagulant therapy
• Thrombin time can provide a qualitative indication of the presence of dabigatran
• Patient results are within normal levels, dabigatran is at trough level, patient risk of a bleed due to OAC is low
60

Emergency testing of :
• Dabigatran:
1. TT is normal can assume patients risk of bleeding is low.
2. PT/ INR is insensitive and not useful
3. POC INR shouldn’t be used
4. APTT: high levels, no clot, prolonged 2 fold at peak levels, and 1.5 fold at 12 hours.
Overdose: Since this drug the last enzymatic step of the coagulation cascade it is difficult to replace. May dialyze ( acute cases) since only 35% is bound to plasma proteins.
Idarucizumab: RE-VERSE AD, the study is an ongoing, international open-label trial with an expected enrollment of 250 to 300 patients.
Blood; Schulman, Crowther, published on line February 1, 2012
Thrombin Time
• Uses human or bovine thrombin
• Measures the conversion of fibrinogen into fibrin by thrombin.
• A qualitative assessment
• Will be very prolonged in the presence of DTI’s
• Over sensitive
• Demonstrate a DTI is on board quickly and easily
• Can tell if at peak (high) or trough ( low or normal) level
Hemoclot Thrombin Inhibitor
• A diluted Thrombin Time (dTT) using human thrombin 1:8 and 1:20
• measure off a curve calibrated with DTI (Dabigatran calibrator, controls, CE marked & Canada license)
• Uses human thrombin,
• Results of >200 ng/mL trough measure, eg, 10–16 hours after the previous dose) is associated with a higher risk of bleeding

The New Oral Anticoagulants:Similar Yet Different
• Thrombin Inhibitors:1. Dabigatran: pro-drug, renal clearance - twice daily
• FXa Inhibitors:1. Rivaroxaban: renal clearance - once daily2. Apixaban: hepatic clearance - twice daily3. Edoxaban: hepatic clearance - once daily
Circulation 2010;121:1523-1532
Apixaban
• Oral, direct, selective factor Xa inhibitor
• Produces concentration-dependent anticoagulation
• No formation of reactive intermediates
• No organ toxicity
• Low likelihood of drug interactions
• Good oral bioavailability
• No food effect
• Balanced elimination (~25% renal)
• Half-life ~12 hrs
65

Rivaroxaban (Xarelto®)
• Oral direct factor Xa inhibitor – both free and bound
• FDA approval for stroke prophylaxis in patients with nonvalvular AF
• Achieves maximum plasma levels ~3 hours
• Terminal plasma ½-life 4-9 hours(~12 hrs in patients >75 years)
• Few drug-drug and food-drug interactions
• Eliminated by kidneys (~60%)▫ Contraindicated when CCr <30 mL/min
66

Emergency testing of
• Rivaroxaban:
1. PT response is assay dependent, should be prolonged
3. anti-Xa levels using rivaroxban as a calibrator
2. Normal levels of PT, APTT and TT qualitative indicator of absence of drug
Overdose: due to a high degree of albumin binding in plasma; can not be dialyzed
Four factor prothrombin complex concentration showed promise

Monitoring: Xa inhibitors• Standard curve constructed using spiked PNP with the
Xa inhibitor
• From a syringe of the Xa inhibitor create a stock solution of 1mg/L in PNP
• Make a series of dilutions and run a standard curve using an anti-Xa assay
• Results are calculated off this curve and reported in mg/L
• Therapeutic Range
Peak 3 hours post dose 0.39-0.50 mg/L
Minimum steady state – 0.14-0.14 mg/L
Arixtra package insert, (2002) Organon sanofi-synthelabs, West Orange, NJ

Summary Table
Parameter Apixaban Dabigatran Rivaroxaban
Target Protein Factor Xa Thrombin (IIa) Factor Xa
Pro-Drug No Yes (etexilate) No
1˚ Elimination CYP3A4/P-gp Renal CYP3A4/P-gp
Renal Adjustment Avoid < 15 ml/min ↓ 15-29ml/minAvoid < 15 ml/min
Avoid < 30 ml/min
Drug-Drug Interact. CYP3A4/P-gp Rifampin (P-gp) CYP3A4/P-gp
Onset of activity 3-4 hrs 1-2 hrs 2-4 hrs
t½ 8-15 hrs 12-18 hrs 5-9 hrs
Dosing interval Twice daily Twice daily Daily
Monitoring tests Anti-factor Xa ECT, TT, +/- aPTT Anti-factor Xa
FDA Indications Stroke prevention Non-valvular Afib. Non-valvular Afib. Ortho VTE Proph.
Clinical Uses AfibOrtho VTE Proph
Afib, VTE Afib, Ortho VTE Proph, VTE

Case Study
• Patient presents with a DVT, placed on unfractionated heparin
• Given a bolus dose of heparin - monitored by the APTT
• First test taken 4 hours post dose
• APTT= 67.5 sec (25-35 sec)
• Develops a PE
• Was the patient properly anticoagulated?
Based on APTT result
• Prolonged aPTT
• What is the sensitivity of the aPTT reagent to heparin
• Not good enough to use 1.5-2.5 times the mean of the normal range
• Performed an anti-Xa assay = 0.25U/ml anti-Xa
• Patient under anticoagulated

Heparin
• Polysaccharide chain found in organs
• Binding site for ATIII
• Treats Venous Thromboembolism
• Prevention of Thromboembolism
• Analytical Variables
• Biological Disadvantages

Biological Disadvantages
• Liver Disease, increased response to heparin, can over anticoagulate
• Drugs interfere with heparin
• Level of ATIII < 75-80%, decreased response to heparin
• VIII & I are acute phase reactive proteins,levels increase-APTT decrease
• Depends on weight & not well absorbed by the GI tract

Fate of Heparin
• 20% excreted by the kidney
• 80% removed in circulation by the liver & RE system
• 1/2 life of 90 minutes
• Bolus dose 5-10,000 units
• 4-6 hrs later test to see if therapeutic

Laboratory Monitoring of UFH
• aPTT• 4-6 hours after bolus dosage and every 24 hours thereafter
• A dose adjustment requires monitoring 6 hours after the dose adjustment
• 1.5-2.5 x “normal”
• Therapeutic target—0.3-0.7 anti-Xa U/mL
• Monitor platelet count daily
75

UFH Therapeutic Range
• Problems with the 1.5-2.5 range
• Could lead to inadequate heparinization result in thrombosis
• aPTT response varies with different manufacturer’s reagents
• aPTT response varies with different instrumentation
• A patient’s baseline aPTT often is not a reliable measure for comparison
• Patients with recent thrombotic episode shortened aPTT
• Patients with undiagnosed LA high base-line aPTT
• Patients with factor deficiency high base-line aPTT
• ACCP and CAP suggested establishing a therapeutic range
• Based on the relationship of the local aPTT versus heparin levels in specimens collected from heparinized patients
76

CAP
• It is recommended that the first method be used initially to establish the therapeutic range before starting patient testing with a new instrument or new reagent, while the second method can be used for validation of the therapeutic range with subsequent reagent lot changes.
• It is not best practice to use plasma samples spiked with heparin in vitro to calculate the therapeutic range, as differences in heparin binding proteins in vitro may lead to overestimation of the therapeutic range.
77

Heparin Therapeutic Curve
• CAP recommends that each laboratory establishes its own heparin therapeutic range for each new lot of aPTT reagent based on reagent:instrument combination
• Heparin Anti-Xa Method• 50-60 plasma samples collected from patients treated with UFH• Mix of samples should span the therapeutic range• No more than two samples on the same patient • The PT/INR should normal (INR <1.3)• Assay aPTT, anti-factor Xa (UFH), and PT/INR• Plot the aPTT on the y-axis and the anti-Xa units on the X-axis• Draw a line through the middle of the points• The UFH therapeutic range is equivalent to
• 0.3-0.7 units/mL Anti-Xa Heparin assay
78

Chromogenic Anti-Factor Xa to Monitor UFH
• When Xa is present in excess along with AT the inactivation of Xa will be a function of the concentration of heparin
• The amount of Xa that remains after inactivation can be measured with a chromogenic substrate
• Chromogenic substrates are short amino acid sequences that contain PNA group
• Proteolysis of the chain occurs by the residual factor Xa liberating the PNA
• This liberation is measured as a change in OD/unit of time
• AT (excess) + Heparin [Heparin-AT] + AT• The inactivation of Xa is a function of the concentration of heparin
• [Heparin-AT] + Xa (excess) [Heparin-AT-Xa] + Xa• Xa that remains can be measured with a chromogenic substrate
• Chromogenic Substrate + Xa peptide + pNA• Short amino acid sequences that contain PNA group
• Proteolysis of the chain occurs by the residual factor Xa liberating the pNA
• Measure the released pNA
79

Brill-Edwards TechniqueTherapeutic Range= 0.3-0.7U/ml
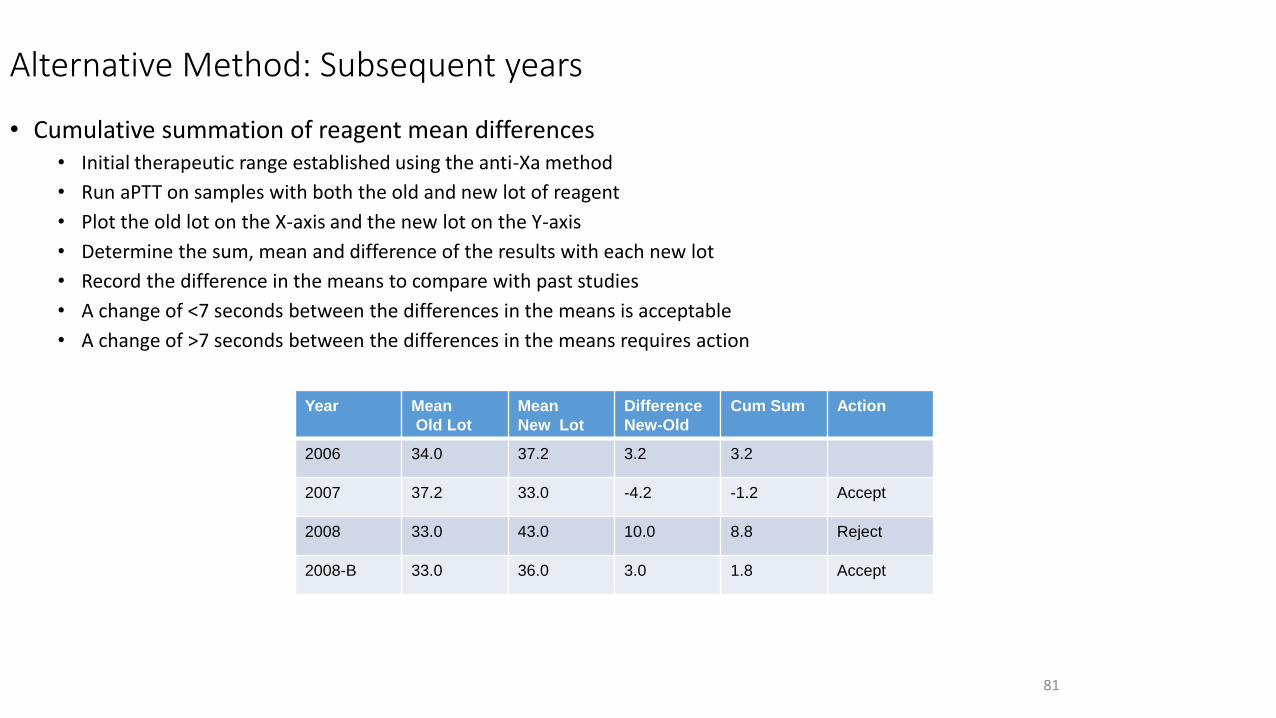
Alternative Method: Subsequent years
• Cumulative summation of reagent mean differences• Initial therapeutic range established using the anti-Xa method
• Run aPTT on samples with both the old and new lot of reagent
• Plot the old lot on the X-axis and the new lot on the Y-axis
• Determine the sum, mean and difference of the results with each new lot
• Record the difference in the means to compare with past studies
• A change of <7 seconds between the differences in the means is acceptable
• A change of >7 seconds between the differences in the means requires action
81
Year Mean
Old Lot
Mean
New Lot
Difference
New-Old
Cum Sum Action
2006 34.0 37.2 3.2 3.2
2007 37.2 33.0 -4.2 -1.2 Accept
2008 33.0 43.0 10.0 8.8 Reject
2008-B 33.0 36.0 3.0 1.8 Accept

Chromogenic Anti-Factor Xa
• Advantages
• Not affect by preanalytical variables
• Assess the true level of heparin present in the patient’s plasma
• Can be used to monitor UFH therapy in the following conditions
• Patients with a LA who present with prolonged aPTT’s
• Patients with an underlying defect in the contact factors that manifests as a prolonged aPTT
• Patients recently on Warfarin therapy with perhaps an unreliable aPTT
• The only assay available to measure the activity of LMWH
• Available on most automated analyzers today
• Not affected by short sample draws
• No need to establish a aPTT therapeutic range
82

Considerations:
• More expensive
• Maybe not available for 24/7
• Need prompt specimen processing to prevent PF4 neutralization of heparin.
• Clinicians may not like it
• We have implemented heparin in the core laboratory- 24/7 using liquid reagents, hybrid curve
• Improved patient management- our clinicians love it-

When faced with the option of treating bleeding or thrombosis, choose bleeding- it is easier to treatJack Hirsch- MD

Case Studies DVT/PE
• The precise number of people affected by DVT/PE is unknown,although as many as 900,000 people could be affected (1 to 2 per 1,000) each year in the United States.
• Estimates suggest that 60,000-100,000 Americans die of DVT/PE (also called venous thromboembolism).
• 10 to 30% of people will die within one month of diagnosis.• Sudden death is the first symptom in about one-quarter (25%) of people who have a
PE.
• Among people who have had a DVT, one-half will have long-term complications (post-thrombotic syndrome) such as swelling, pain, discoloration, and scaling in the affected limb.
• One-third (about 33%) of people with DVT/PE will have a recurrence within 10 years.

VTE causes a major burden of disease
• VTE associated with hospitalization was the leading cause of disability-adjusted life-years (DALYs) lost in low-income and middle-income countries
• Second most common cause in high-income countries, being responsible for more DALYs lost than nosocomial pneumonia, catheter-related bloodstream infections, and adverse drug events.
• In a study that looked at more than 6.7 million hospitalizations from 1,039 hospitals around the United States, findings included higher rates of VTE diagnosis were observed among patients:
80 years or older,
male,
Black,
hospitalized for seven days or longer, and
who had no operating room procedures.
Additionally, hospitalized adults with pre-existing conditions - such as AIDS, anemia, arthritis, congestive heart failure, clotting disorders, high blood pressure, cancers, obesity, paralysis among others - were almost three times more likely to be diagnosed with VTE.

ISTH- in May of 2015 to the World Health Assembly• We strongly recommend that VTE be included as a specific cause of
death to be assessed in the next Global Burden of Diseases study. We also call for a focused global effort on thrombosis prevention, beginning with patient safety improvements related to hospital associated VTE. Such an effort could save millions of lives and markedly reduce the death and disability caused by thrombosis

Clinical Utility of D-dimer
• Disseminated Intravascular Coagulation (DIC)
Simultaneous formation of thrombin and plasmin
Sensitive, but not specific marker for DIC
• Venous Thromboembolism (VTE)
High negative predictive value for exclusion
• Potential positive predictive value
Positive predictive of recurrent MI
Independent predictor of ischemic heart disease
Differentiate between a traumatic spinal tap or a subarachnoid bleed
Predictor of VTE recurrence, elevated levels following discontinuation of anticoagulant therapy associated with recurrence

Diagnostic Utility
• If you have a D-dimer test that has been cleared by the FDA for exclusion, that test can be used to rule out DVT and PE for non-high clinical pre-test probability assessment model to exclude DVT and PE.
• Outpatient setting
• To achieve this claim the FDA requires:
1. To establish the cutoff study of the assay (0.500 mg/L) by testing samples against a predicate to verify sensitivity
2. To prospectively collect and enroll patients suspected with PE and or DVT (first time event) and compared standard of care results (imaging) versus the D-dimer result.
3. Negative D-dimer patients receive a 90 day follow up call to evaluate potential development of a PE or DVT
4. Sufficient patients must be enrolled have a >99% NPV to be approved as an exclusionary claim by the FDA.

Clinical Model to aid in assessment & diagnosis:• Developed by Wells and colleagues
• Based on symptoms and signs for DVT and PE
• Presence or absence of an alternate diagnosis
• Presence and number of risk factors
• Patients are scored based on a series of criteria
Scoring for DVT Scoring for PE
High probability >/= 3 High probability >6
Moderate 1 or 2 Moderate 2-6
Low </=0 Low <2

Clinical Model for Predicting DVT
Pre-Test Probability Questionnaire Score
Active cancer 1
Paralysis, paresis or recent plaster immobilization of lower
extremities
1
Recently bedridden > 3d or major surgery w/in 4 wk 1
Localized tenderness along the distribution of deep venous
system
1
Entire leg swollen 1
Calf swelling 3 cm > asymptomatic side (measured 10 cm
below tibial tuberosity)
1
Pitting edema confined to the symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Alternative diagnosis as likely or greater than that of DVT -2
Wells, et al. Lancet, 1997;350:1795-1798

Case study
• A 52 year old male comes into the ED complaining of pain in the right calf
• Leg is slightly swollen, patient is concerned they may have a blood clot
• Otherwise healthy male, not on any medication, active
• Pain seems to have worsen through the night
• Wells scoring is a low PTP
• ED physician orders a D-dimer
• Result is negative (0.345 mg/L)
• Should this patient have imaging to rule out the possibility of a DVT?

Case Study
• Good subject to perform D-dimer for rule out claim.
• Healthy, not “older” population
• Low PTP
• D-dimer result not near the cutoff (result is .345 mg/L, cutoff 0.500 mg/L)
• Even knowing the CV of the test (<5% at this level) would not bring the result into the positive range of > 0.500
• May suggest follow up with physician- if pain worsens
• Most likely a strain due to sliding into the bases while playing softball!

Case Study:
• A 76 year old male patient has been admitted into the ED for an infection
• After performing an APACHE assessment, it is determined that he is critically ill, possibly septic
• He has a history of DVT so a D-dimer is ordered
• Has a high PTP with the Wells score
• D-dimer is positive 6.4 mg/L
• Does the patient have a blood clot?
Clues:
• Older patient, septic, previous history of DVT
• Wells scoring results in a high PTP
• What is the utility of an elevated D-dimer?
• What are you looking for?

Case study
• This patient has all the reasons to have a positive D-dimer
• Older, septic with previous history of DVT
• We don’t know specifically why it is increased
• There are many reasons
• Not the patient population to be using the D-dimer test to determine a DVT
• The patient may be in DIC

Case study
• 42 year old male enters the ED complaining of rapid onset, shortness of breath, pain in chest, numbness in arm
• Wells score is mod PTP
• Should this patient be imaged for a PE?
• D-dimer is normal 0.411mg/L
• Additionally testing included an elevated troponin and BNP
• Does this person have a PE?
Case study
• Patient test results appear to be more consistent with an MI, versus a PE
• Imaging doesn’t seem to be indicated at this time
• Patient is then admitted
• Follow up with imaging if symptoms still persist several days post admission
• D-dimer will most likely be elevated as an inpatient, and imaging would be the more diagnostic approach.

Case Study
• A 25 year old pregnant female in her second trimester comes into the ED
• She is complaining of pains in her leg, leg is slightly swollen
• No history of DVT, Wells scoring is low- moderate PTP
• Run a D-dimer
• The D-dimer test is 0.534 mg/dL (cut-off is 0.500 mg/dL)
• They perform imaging and the imaging is negative

Case Study
• Why did the clinician choose to perform imaging? Patient is an outpatient, has a low PTP
• Why was the D-dimer positive? Positive D-dimer during pregnancy
• However, pregnancy is a hypercoagulable state, and pregnant patients are usually excluded from studies
• Best to perform imaging on this patient

Case Study
• A 40 year old male comes into the ED complaining of sudden onset of shortness of breath
• He has had a cold for 2 days, but now feels a heaviness in his chest
• He does have a history of asthma
• The clinician suspects that he might have pneumonia, but wants to make sure he doesn’t have a PE
• Performs a D-dimer, which is negative
• Doesn’t order a VQ scan, treats the patient, gives him medication with orders to follow up with his family physician next week.
• Did he do the right thing?

Case study
• The laboratory used an automated immunoturbidimetric D-dimer assay
• This assay has been FDA approved for exclusion for PE
• A prospectively collected clinic trial looking at over 1000 patients suspected of DVT and or PE were tested and imaged and their imaging results were compared to the D-dimer
• A negative predictive value of >99% was determined
• This results in being able to have patients with a low-moderate pre test probability and a negative D-dimer not have to be imaged.
• This patient’s diagnosis was asthmatic bronchitis, did not have to have expensive imaging, D-dimer was able to provide a diagnosis

How do you use your tests for VTE
• D-dimer FDA cleared for exclusion?
• Do you test while on heparin? After an event?
• What tests: APCR? AT, Protein C, S? Lupus
• Molecular testing?
• May be positive for more than one test-
• Perform activity first, then antigen testing.
• Do it correctly-
• Treat the event

Who says iQCP
• CLIA/CMS – Review 493.1256-1269 – interpretive requirements for QC• CAP – new common core checklist• Individual State Requirements – (?)• No longer use EQC-Equivalent Quality Control
• You must follow the most strict guidelines of each directive- CLIA mandates 2 levels of controls every 24 hours, however CAP statesevery 8 hours for coagulation-
• In place by January 1, 2016

What is iQCP
• Plans that are constructed by the laboratory that involves 3 components:
• 1. Risk Assessment
• 2. Quality control plan
• 3. Ongoing review – Quality Assessment of the plan
• 493.1250: Each laboratory that performs non-waived testing must meet the applicable analytic systems requirements. The laboratory must monitor and evaluate the overall quality of the analytic systems and correct identifiable problems as specified in 493.1289 for each specialty and sub-specialty of testing performed.
WHY DO WE NEED iQCP
What is the purpose of QC as we know it:
• 1. to monitor the accuracy and precision of the complete analytical process
• 2. to detect immediate errors that occur due to test-system failure, adverse environmental conditions and operator performance
• 3. to monitor over time the accuracy and precision of test performance that may be influenced by changes in test system performance and environmental conditions, and variance in operator performance.
What is the purpose of iQCP:
• It is an all inclusive approach to assuring quality.
• Addresses the potential failures and errors in the entire testing process:
• Preanalytic, Analytic, and Postanalytic

NO iQCP – it is “voluntary”
• Minimum of 2 controls each day of patient testing- for EACH device and cartridge - CLIA requirement
• CAP may have different requirements in different areas ( check coagulation, micro, blood gases)
• If several tests are on one system can have 1 iQCP BUT all the risks for all the tests must be covered.
• If you have devices in different areas, (POC) you must cover the possible changes in environment, personnel etc. for that particular device.
Responsibility
• Laboratory director is responsible for determining if iQCPshould be used
• They must sign off on the plan
• Designate IN WRITING specific duties for the iQCPdevelopment (we will have a procedure in the QA manual)
• Laboratory must have data to support their control procedure decisions and all activities for iQCP must be documented per the CLIA regulations.

You are now QC’ing your QC
• No longer just bottles in the fridge; one size QC doesn’t work with a lot of the new technologies
• Looks at all activities that we do, not only the analytical phase
• Outcome is to minimize errors
• Provide optimum results from the laboratory
• By asking:
“What is the optimum QC for this test for my patients in my lab?

What test in coagulation may require iQCP
• Reptilase- runs 1 level of control
• Platelet aggregation- 1 level of control- some labs only run a control with a new lot of reagents.
• PFA-100
• Verify Now
• Any LDT
• Mass Spec?
• Any test that doesn’t have 2 levels of controls- fluids?
• Must at a minimum run what the manufacturer has in the PI

Considerations for iQCPAre there manufactures
instructions?
No QC requirements
Options
Frequency < 2 levels/day
Follow manufacturers instructions
NOYES
No
YES
Perform 2 levels of QC/day
Perform an iQCP:RA
QCPQA

Part 1: Risk Assessment
• Identifies and evaluated potential failures and sources of error in your testing process
• Evaluates the frequency and impact of potential failures
• Must look at all phases of testing- pre-analytical, analytical and post-analytical
• Uses in house data- which includes- demonstrates the stability of the test system in its own environment by its own personnel
• Supports the number and frequency of QC
• May be historical and/or new data
• Must cover 5 components
S-T-R-E-P• S- PECIMEN: patient prep, collection, label, storage,
processing• T-EST SYSTEM: sampling, interferences, calibration,
mechanical failures, software, hardware, transmission, reporting.
• R-EAGENT: shipping/receiving, storage, prep, expire• E-NVIRONMENT: temp, humid, ventilation, lighting,
water, space, utilities• P-ERSONNEL: training, competency, license,
education, staffing

CLSI: EP23-A
• Laboratory Quality Control Based on Risk Management: Approved guideline
• Manage risk: How good is good enough- set medical goals and acceptable risk level
• Evaluation of medically allowable error.
• Look at all known potential events that have a degree of likelihood for a level of severity of an adverse outcome- some are small, others are not
• Try to balance against all known beliefs, either perceived or real
• What are patients, physicians, institution and society are willing to risk as allowable errors and what are the consequences-
• NEED A SYSTEM IN WHICH ERRORS ARE DETECTED BY STATISTICAL QC THAT FINDS THE ERROR, AND LOWERS THE RISK OF ERRORS, SO THAT IT WILL BE MEDICALLY ACCEPTABLE.

RISK Management
• Risk identification- identifying potential errors
• Risk assessment- evaluating those error to determine their impact on patient test results
• Risk Mitigation- controlling the errors in such a way that residual risk is manageable.
• Essentially you are conducting an audit on tests that require iQCP

Information required to conduct the risk assessment:
1. Manufacturer’s current package insert
2. Owner’s manual for the test/ SOP
3. Graded results from the last three PT events for this test
4. Incident reports related to this test.
5. QA activities (and their conclusions) related to this test.
6. Customer or physician complaints related to this test/ corrective action logs/problem logs
7. Calibration logs, method comparison
8. Minimally, the last three months of storage temperature records, for the storage location (refrigerator, freezer, or room temperature) of the reagents and supplies for this test.
9. Minimally, the last three months of QC records for this test.
10. Data from any EQC qualifying study previously done for this test.
11. Written competency assessment procedures, for testing personnel as well as specimen collection personnel, for this test.
•

Evaluation of Risk
• Your IQCP Summary Report will include your overall risk score and the IQCP components that you have identified throughout your risk assessment. It will include a classification of risk, according to score from your scored answers.

You can use other methods:
• Risk assessment charts in EP23A
• CMS workbooks
• FISHBONE Diagrams
• Process Mapping
• However you must keep all documents (in one place) that you used to determine risks
• You need to then have specific information regarding how to mitigate those risks.

Now you can go to part 2: Your iQCP
• Your iQCP MUST:
• -detect immediate errors that occur due to test system failure, adverse environmental conditions, and operator performance.
• -monitor over time the accuracy and precision of test performance that may be influenced by changes in test system performance and environmental conditions and variance in operator performance.
• -meet ALL applicable regulatory requirements
• This plan will be your documented plan for mitigating risk by stating the mechanisms you select to detect and control each identified risk.

iQCP plan- EXAMPLE
• 1. List the manufacturer’s QC requirements:
• Run QC device daily
• Run external controls with each new lot #, shipment or at least every 30 days
• Internal controls are run automatically with each test device
• We are going to now look at the STREP requirements for a test:
• Specimen: Only NaCitrate used as per validated by manufacturer, keep at RT 4 hours, longer freeze at -20, to prevent serum from being used, only primary tube used for testing, etc.
• Test system: can only be used by personnel that have a user ID, if QC device fails will not run a test, no test if internal controls fail, no result on a new lot that wasn’t calibrated

Continue:
• Reagents: all stored at proper temperature and recorded, lot to lot validation will be performed, Any left over reagents will be discarded, etc
• Environment: humidity must be between 20-80%, must be on a level surface, must not be in direct sunlight, etc.
• Personnel: competency assessed, only those with user id’s can perform the test, etc.
• Post Analytical Phase: analyzer is interfaced to the LIS to eliminate transcription errors

OUTCOME OF RISK ASSESSMENT
• All relevant potential errors have been assessed in the pre, analytical and post analytical phase
• Most important is the outcome of the plan:
We have determined that the manufacturers recommendation of running:
Xxx levels of controls, xxx times/day
Correspond to the Low risk score for this test.
Acceptability levels of controls are within 2SD of the calculated/verified mean

Part 3: Quality Assurance
• This iQCP will be reviewed regularly (annually) for effectiveness and whenever any of these situations occur:
• 1. PT failure for this test
• 2. Errors not detected by this existing activity or in the risk assessment
• 3. Complaints or incidents reported with results from this test
• 4. Change in package inserts, operator manual, or supplies
• 5. Change in personnel, policies/procedure or test environment
• Approval by Laboratory Director, signed and dated!

Outcomes:
• If you determine that the most significant unmanageable risks falls within the pre-analytic and/or post-analytic phases, additional components should be included in your IQCP that will specifically mitigate the risks in these phases.
If you determine that the most significant unmanageable risk falls within the analytic phase, you should consider performing external QC at an increased frequency.
Monitor and review QC results per your normal procedure and review your IQCP for effectiveness as required by your regulatory agency. Re-evaluate your IQCP and revise if performance failures have been identified.

What happens if requirements call for more frequent QC than what found in the iQCP?• During the risk assessment, the lab must evaluate the potential
sources of errors, manufacturer’s instruction and historical test performance to ID appropriate control processes.
• The QC plan may define a frequency less than the minimum QC frequency defined in the CAP checklists and default CLIA requirements must be followed.
• In all cases, at a minimum manufacturer’s requirements for QC must be followed.

Regulatory requirements
• iQCP must be assessed annually for effectiveness and revised as necessary.
• All information used in conducting the Risk Assessment (QC data, PI, maintenance, PT data) and the QC plan must be maintained for the life of the iQCP plus 2 years, 5 years for Transfusion Medicine.
• It is important to file the specific PT information with the iQCP, since you can discard PT surveys after 2 years, however this will not be the case with the iQCP

How will it be inspected?
• 1. Risk assessment for 5 components (STREP); all phases of testing; all data used to develop the plan, all variations in testing (different sites, devices, type of personnel)
• 2. Written QC plan defining types of control processes, criteria for acceptable performance, and frequency determined (may NOT be less than manufacturers recommendations)
• 3. Approval of the written iQCP by laboratory director PRIOR to implementation
• 4. Ongoing assessment of errors, QC failures and complaints, including if the plan needs a new risk assessment and QC plan
• 5. Annual review of each plan
• 6. In addition to the optimizer iQCP : Use of CAP forms to maintain a list of iQCP and a summary of each iQCP, with the process used to control risks for EACH of the 5 components
• THE DECISION ON THE LEVEL OF RISK IS LEFT TO THE DISCRETION OF THE LABORATORY DIRECTOR!
How to plan: CAP FORMS
• 1. Review your laboratory testing and decide what needs an iQCP, or if you will decide to not have this plan and change how much you run QC make sure that you are compliant with the most stringent recommendations for that test.
•
• 2. Cap requires that you have a List of iQCP plans that will be used by your laboratory. This document will be to be given to the inspector upon inspection.
• 3. Additionally, CAP requires that you have a document that you can provide to them as a cover sheet that lists all of the relevant issues for that particular iQCP. It is called the
• “Individual Quality Control Plan Summary”

Thank you
• Thank you for your time
• Take away message:
Coagulation is complex
However
A glass of wine and a piece of dark chocolate is not only good for you, but may also decrease the complexity of coagulation and increase your willingness to learn





![The 4 Proven Marketing Systems Every [Insert Industry] Must Optimize to Maximize Revenue Growth [Insert Your Name/Logo]](https://static.fdocuments.us/doc/165x107/5697bfae1a28abf838c9c648/the-4-proven-marketing-systems-every-insert-industry-must-optimize-to-maximize.jpg)