How to diagnose prostate cancer better in 2017 - IDF presentation
36
Prostate Cancer: Men at risk & diagnosis Marc Laniado
-
Upload
marc-laniado -
Category
Health & Medicine
-
view
192 -
download
4
Transcript of How to diagnose prostate cancer better in 2017 - IDF presentation
Prostate Cancer:
Men at risk & diagnosis
Marc Laniado
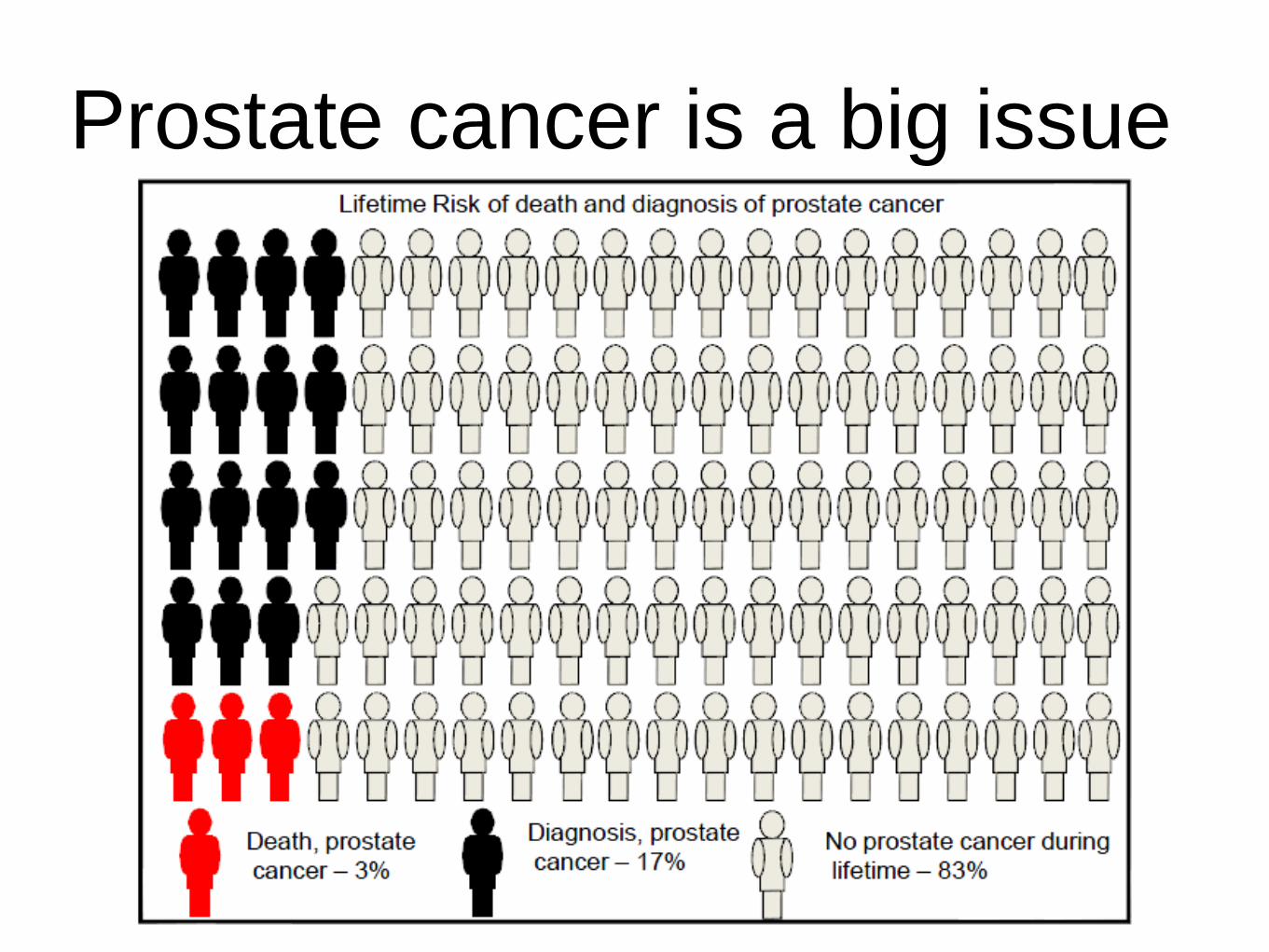
Prostate cancer is a big issue
Q: Which ethnic group is at the HIGHEST
risk of developing prostate cancer?
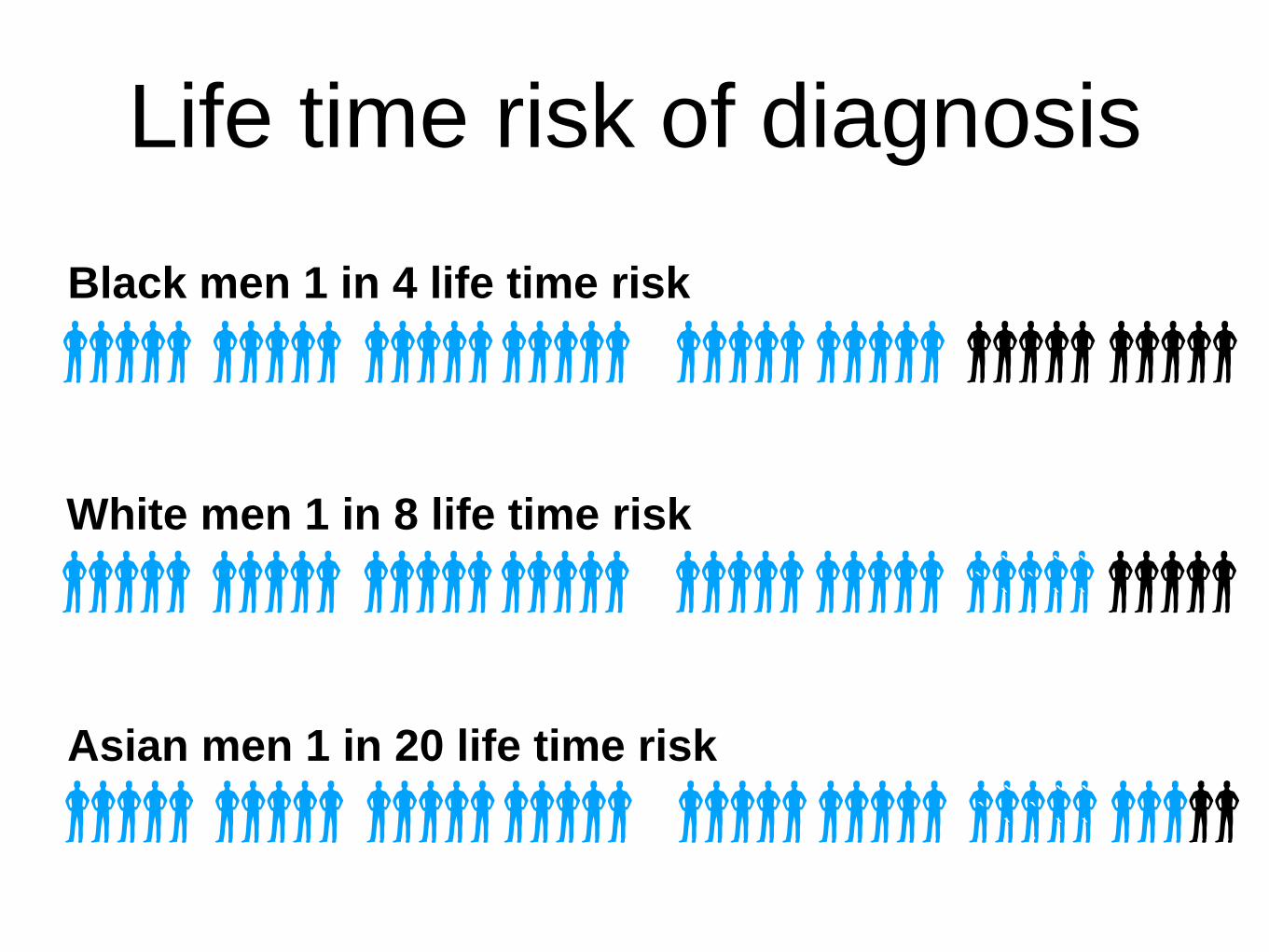
Life time risk of diagnosis
Black men 1 in 4 life time risk
Asian men 1 in 20 life time risk
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
White men 1 in 8 life time risk
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
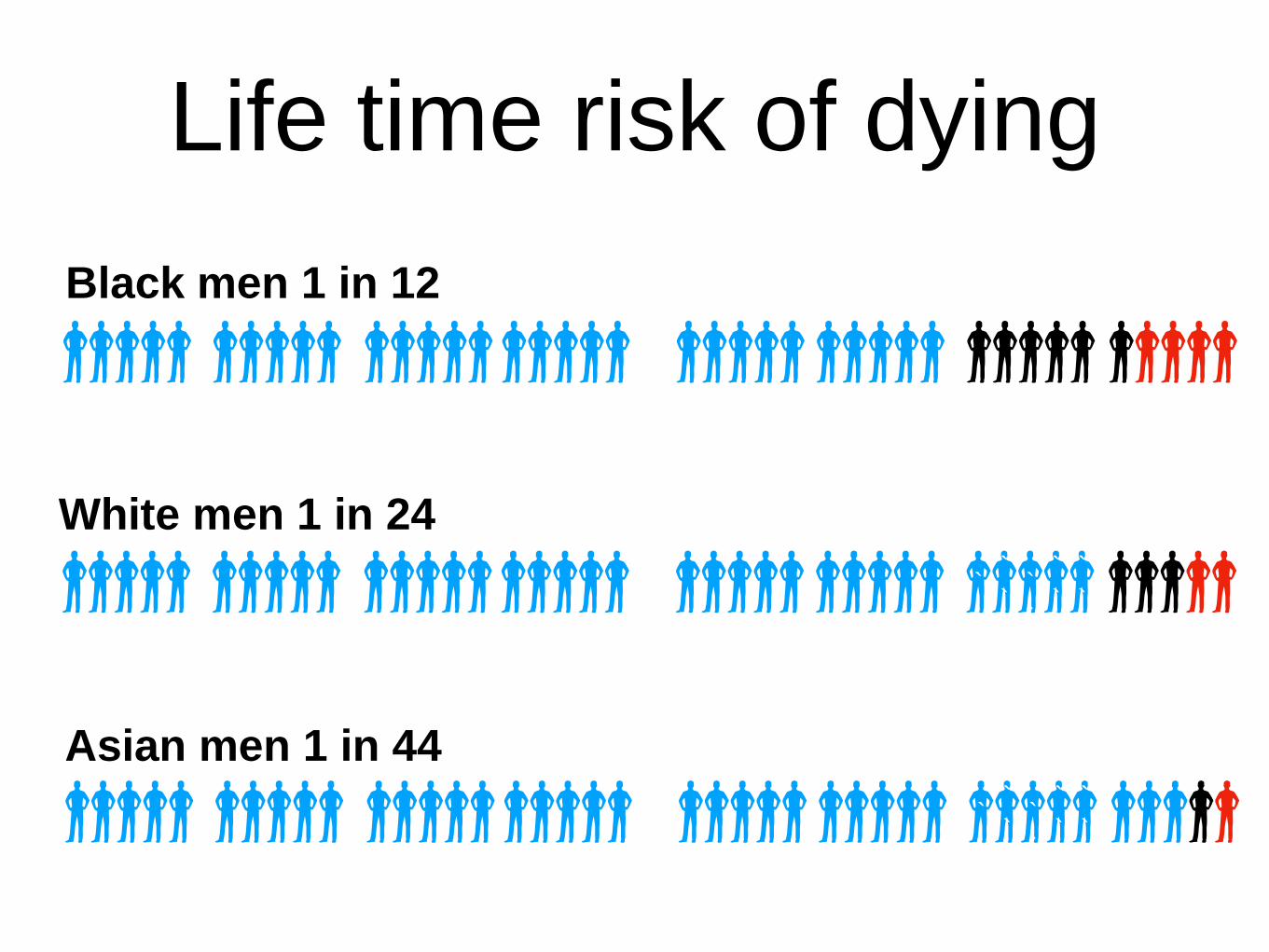
Life time risk of dying
Black men 1 in 12
Asian men 1 in 44
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
White men 1 in 24
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
`
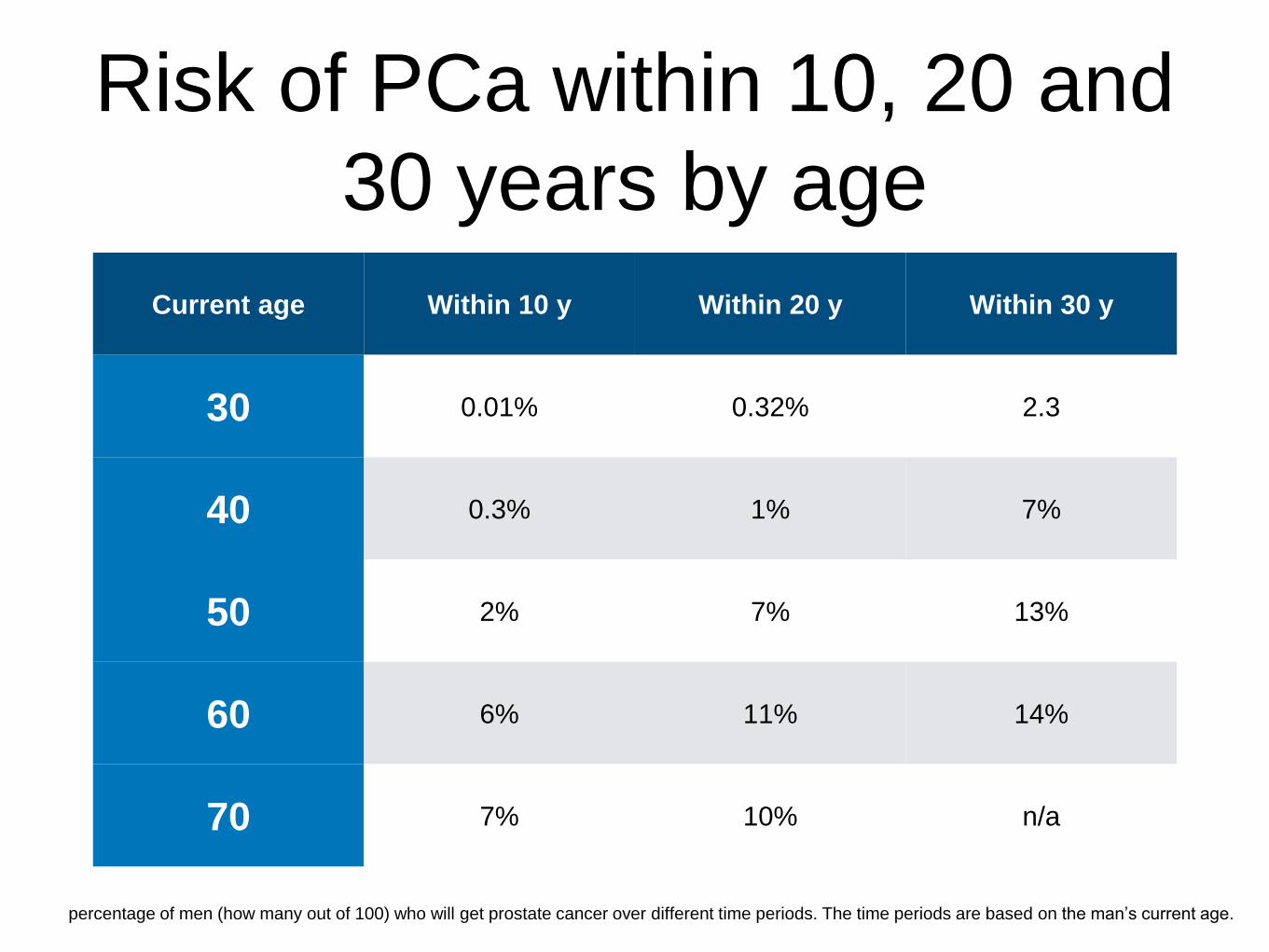
Risk of PCa within 10, 20 and
30 years by age
percentage of men (how many out of 100) who will get prostate cancer over different time periods. The time periods are based on the man’s current age.
Current age Within 10 y Within 20 y Within 30 y
30 0.01% 0.32% 2.3
40 0.3% 1% 7%
50 2% 7% 13%
60 6% 11% 14%
70 7% 10% n/a

(A) Prostate cancer is more likely than benign disease
(B) Benign disease is more likely than cancer
Q: In a 50 year old white man
with moderate lower urinary
tract symptoms (LUTS) & PSA
4 mcg/L,
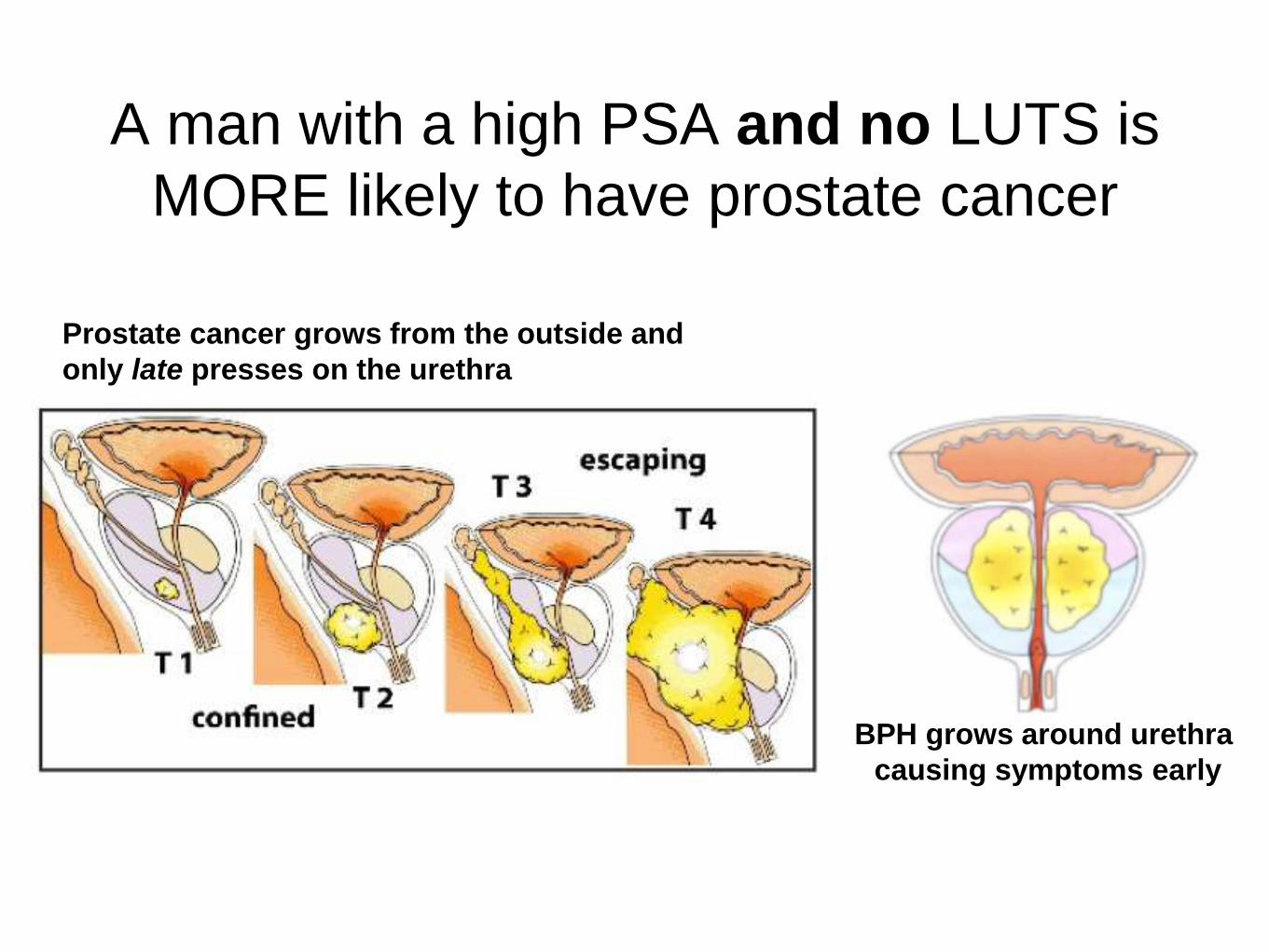
A man with a high PSA and no LUTS is
MORE likely to have prostate cancer
Prostate cancer grows from the outside and
only late presses on the urethra
BPH grows around urethra
causing symptoms early

• Test for PSA & do prostate examination for [1.6.2]
• Lower urinary tract symptoms OR urinary retention
• Erectile dysfunction
• Haematuria -
• DVT - test for urological cancers
• 2WW suspected cancer referral [new 2015]
• PSA > age specific reference range PSA
• Abnormal DRE
NICE Guideline 12
prostate cancer
testing & referral

Q: A 50 y.o. man is concerned: his prostate feels
benign & you test his PSA. On follow up, you advise
him that his PSA is 4 mcg/L Do you refer now
A) yes, even though he remembers he
ejaculated 2 nights before the blood was taken
B) No, because urine culture suggests a UTI
C) Yes, as his prostate felt small
D) Yes, as his prostate felt enormous
E) No, because he exercised vigorously the
day before the blood was taken
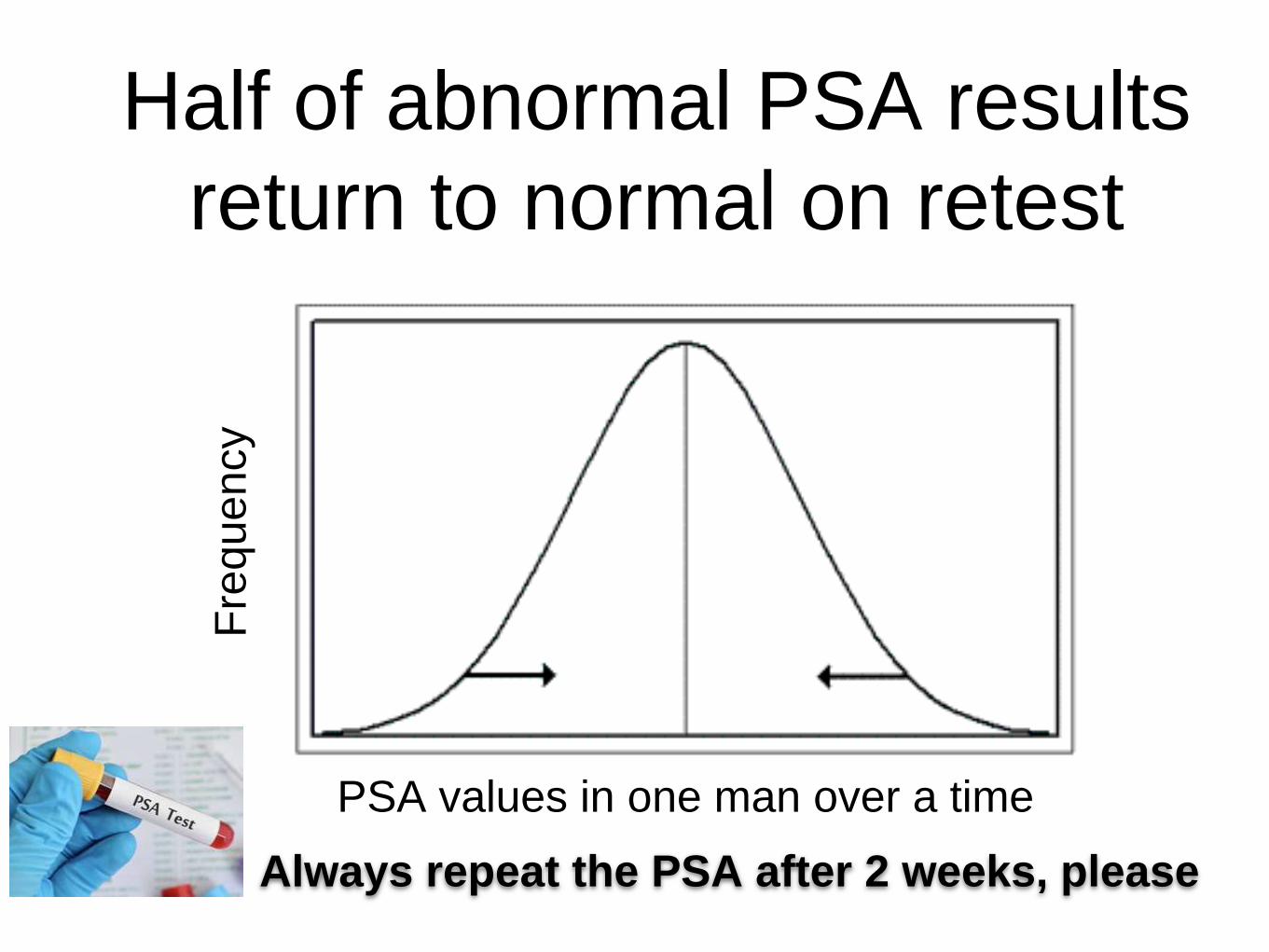
Half of abnormal PSA results
return to normal on retest
PSA values in one man over a time
Fre
quency
Always repeat the PSA after 2 weeks, please
Avoid exercise and ejaculation
for 2 days before PSA
If PSA high with UTI, give quinolone for 2
weeks, wait 2 weeks or more before retest
But don’t routinely give antibiotics
just repeat after 2 weeks

Prostate examination▪ Prostate
▪ Size
▪ Normal – golf ball
▪ > 50 cc – tennis ball
– Consistency
▪ Nodule/asymmetric? Cancer
– Anatomical limits
▪ Should be able to feel median sulcus, lateral
and cranial borders
▪ Seminal vesicles impalpable
– Normal anal tone and sensation
T1: feels benign
T2: hard but mobile
T3: hard, not mobile
T4: fixed
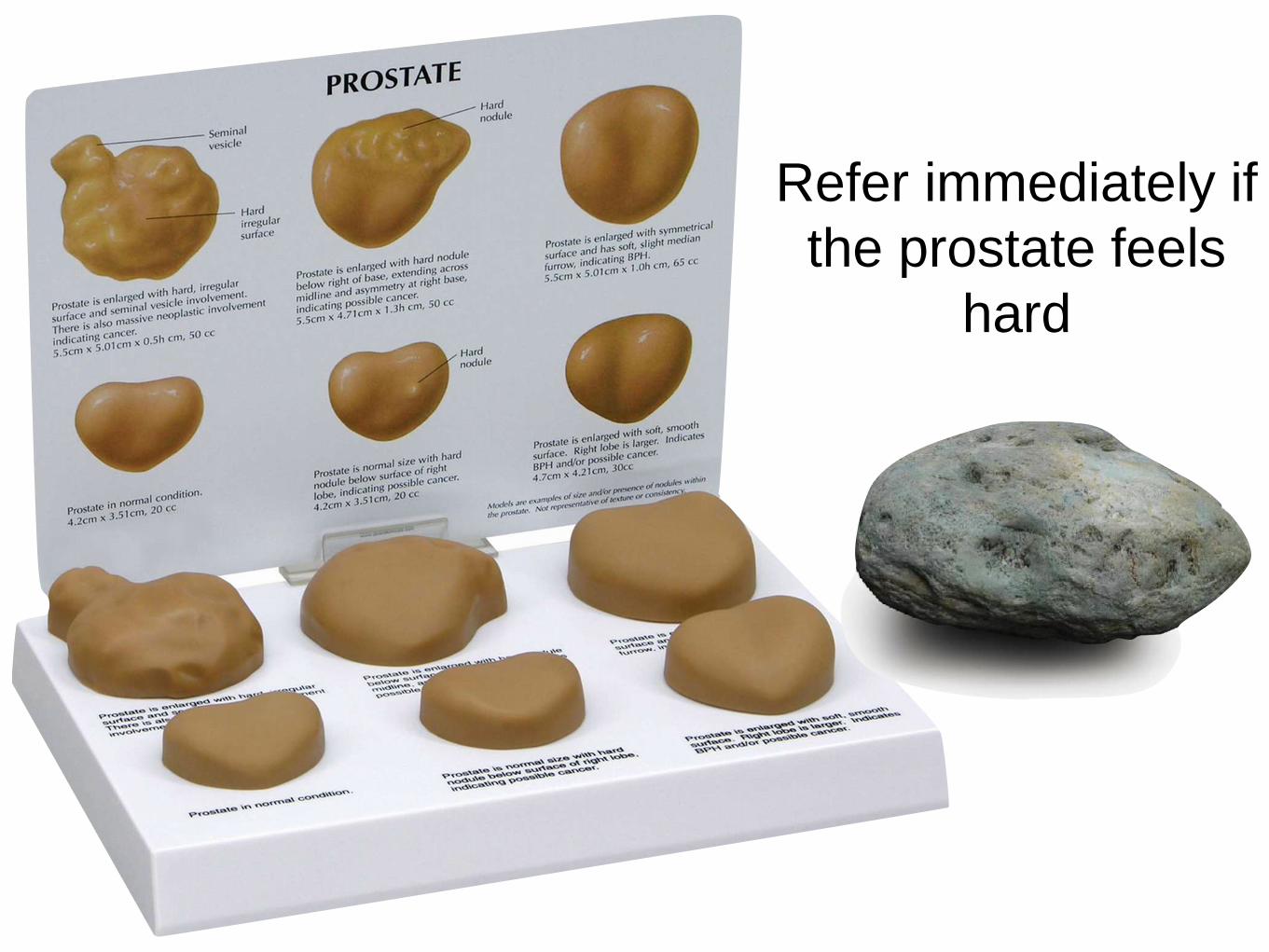
Refer immediately if
the prostate feels
hard
Q Your patient: 63 year-old, white man, PSA
6.5 & 7 mcg/L, benign-feeling prostate
What should you NOT tell him next?
A) His chance of any prostate cancer is
70% & significant prostate cancer 40%
B) a multiparametric MRI is the next test
and can avoid the need for prostate
biopsies in 25% of men
C) His chance of urosepsis after a
transrectal biopsy is <1%
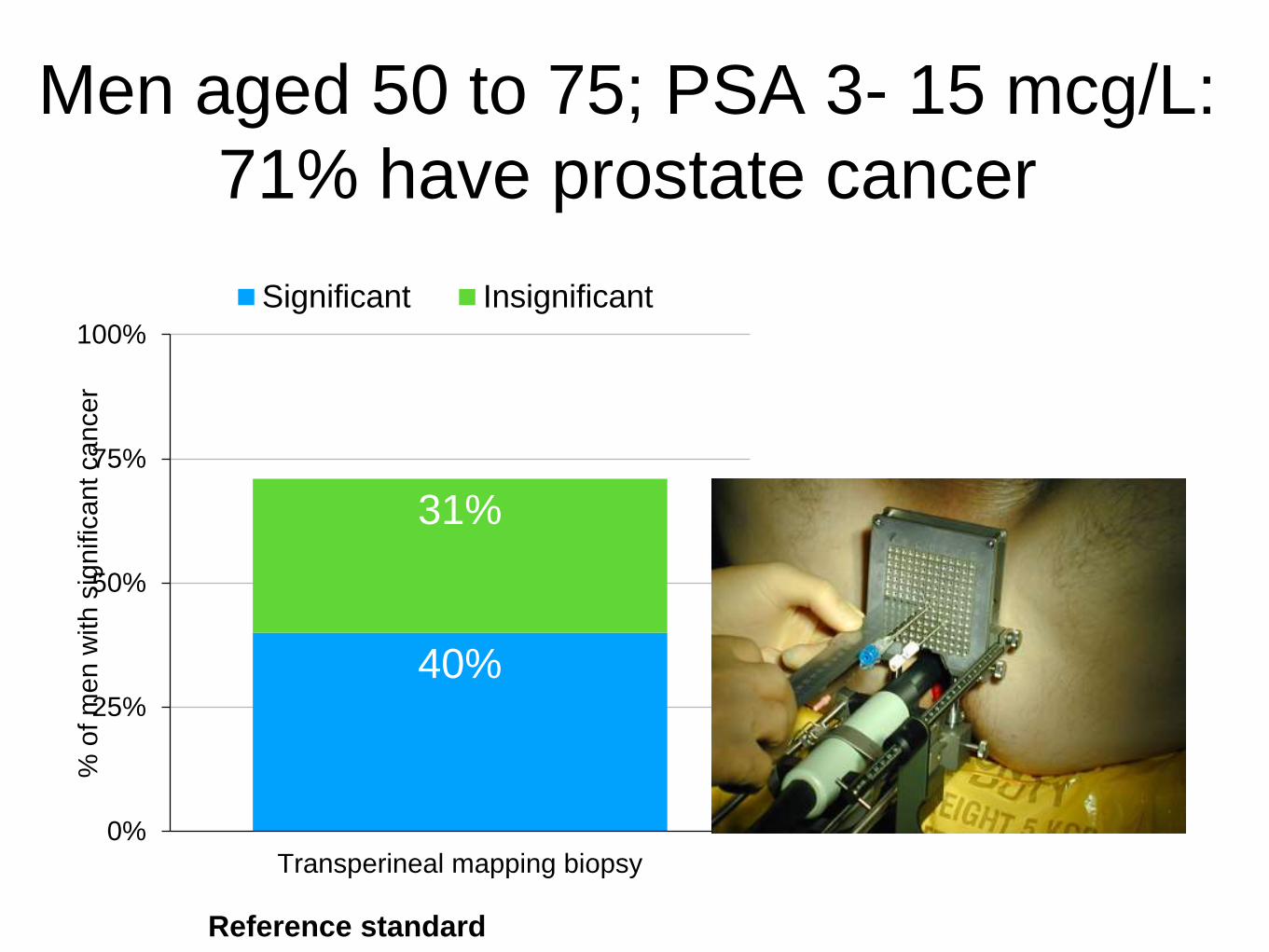
Men aged 50 to 75; PSA 3- 15 mcg/L:
71% have prostate cancer
Reference standard
40%
31%
0%
25%
50%
75%
100%
Transperineal mapping biopsy
% o
f m
en w
ith s
ignific
ant ca
ncer
Significant Insignificant
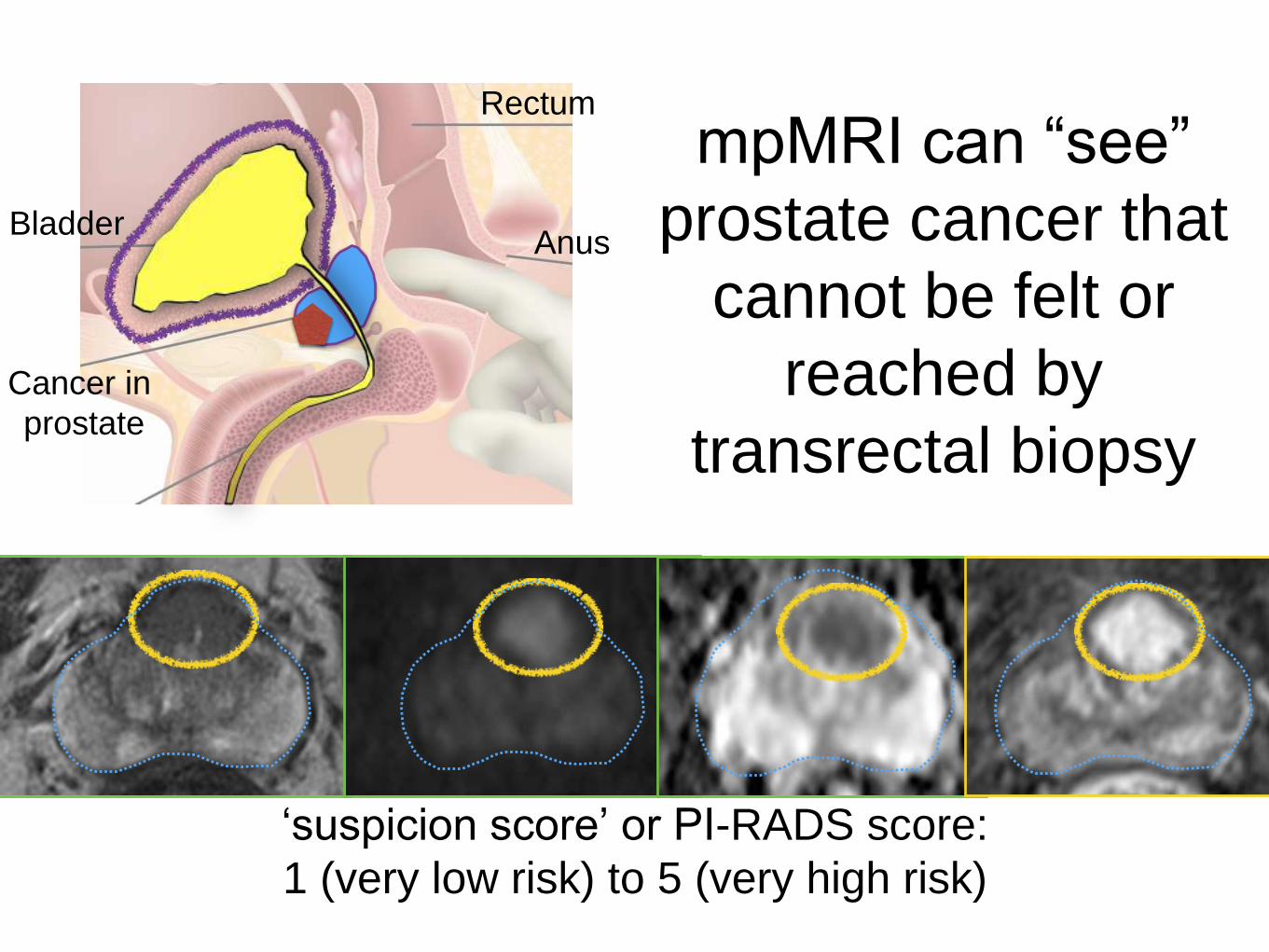
mpMRI can “see”
prostate cancer that
cannot be felt or
reached by
transrectal biopsy
‘suspicion score’ or PI-RADS score:
1 (very low risk) to 5 (very high risk)
Cancer in
prostate
Bladder
Rectum
Anus
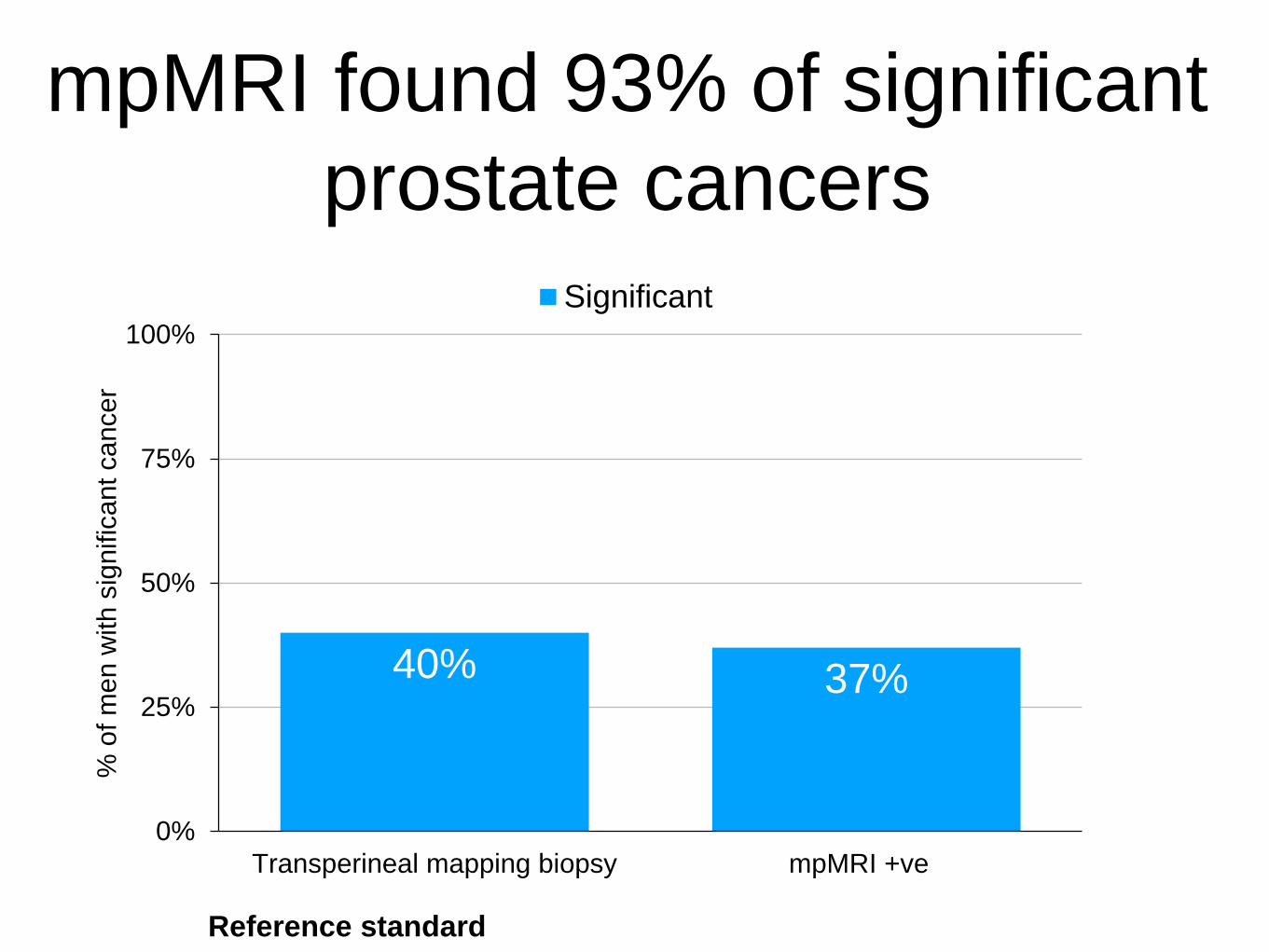
mpMRI found 93% of significant
prostate cancers
Reference standard
40% 37%
0%
25%
50%
75%
100%
Transperineal mapping biopsy mpMRI +ve
% o
f m
en w
ith s
ignific
ant ca
ncer
Significant
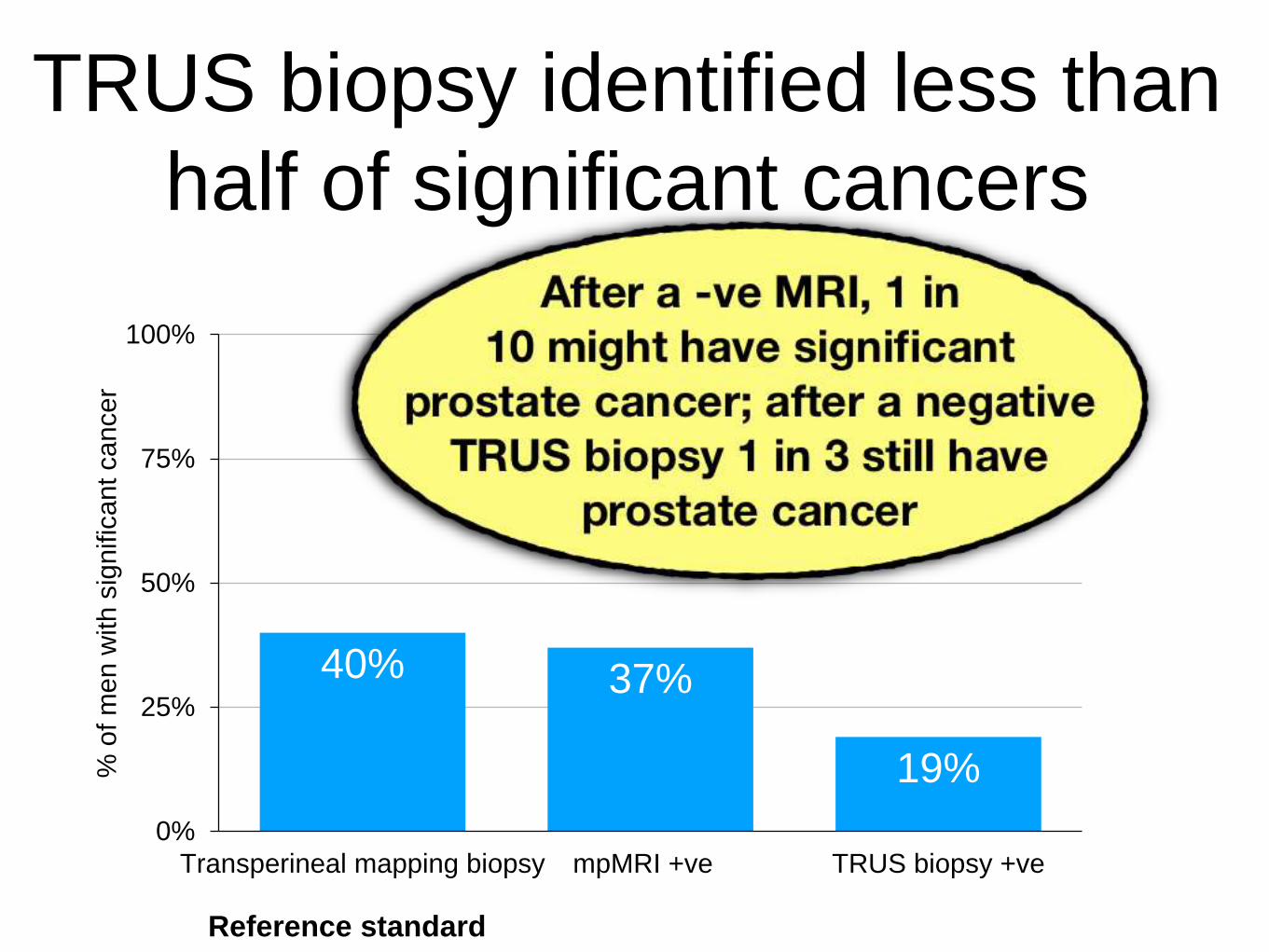
TRUS biopsy identified less than
half of significant cancers
Reference standard
40% 37%
19%
0%
25%
50%
75%
100%
Transperineal mapping biopsy mpMRI +ve TRUS biopsy +ve
% o
f m
en w
ith s
ignific
ant ca
ncer
Significant
1 in 4 men have low suspicion score
MRI (i.e. 1 or 2) & can avoid biopsy
Ahmed 2017 Lancet
But even low suspicion score MRI scan
may require biopsies if other high risk factors
e.g. PSA density, FH of PCa, Afro-Caribbean origin, low free/total PSA ratio
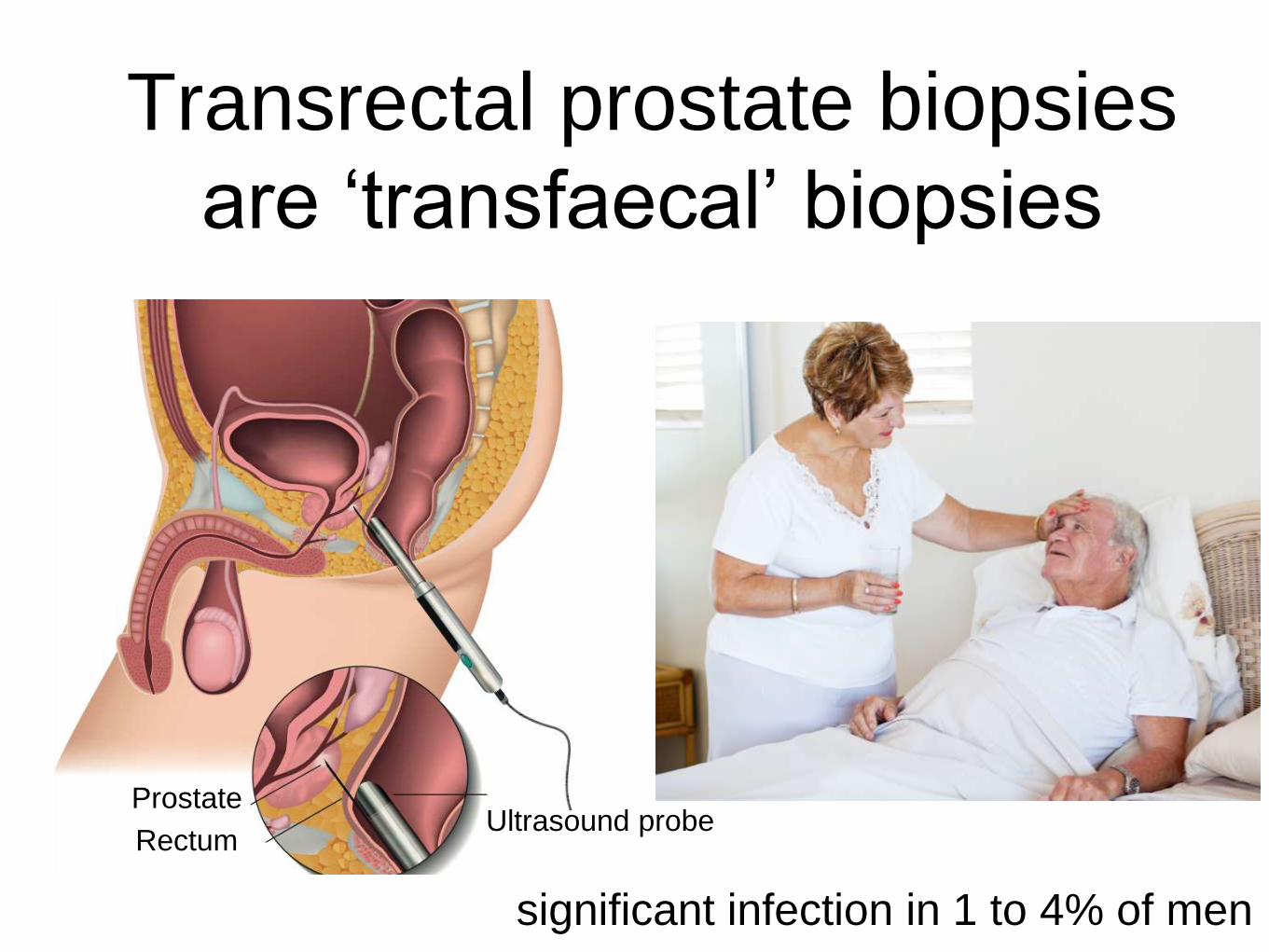
Transrectal prostate biopsies
are ‘transfaecal’ biopsies
Prostate
RectumUltrasound probe
significant infection in 1 to 4% of men
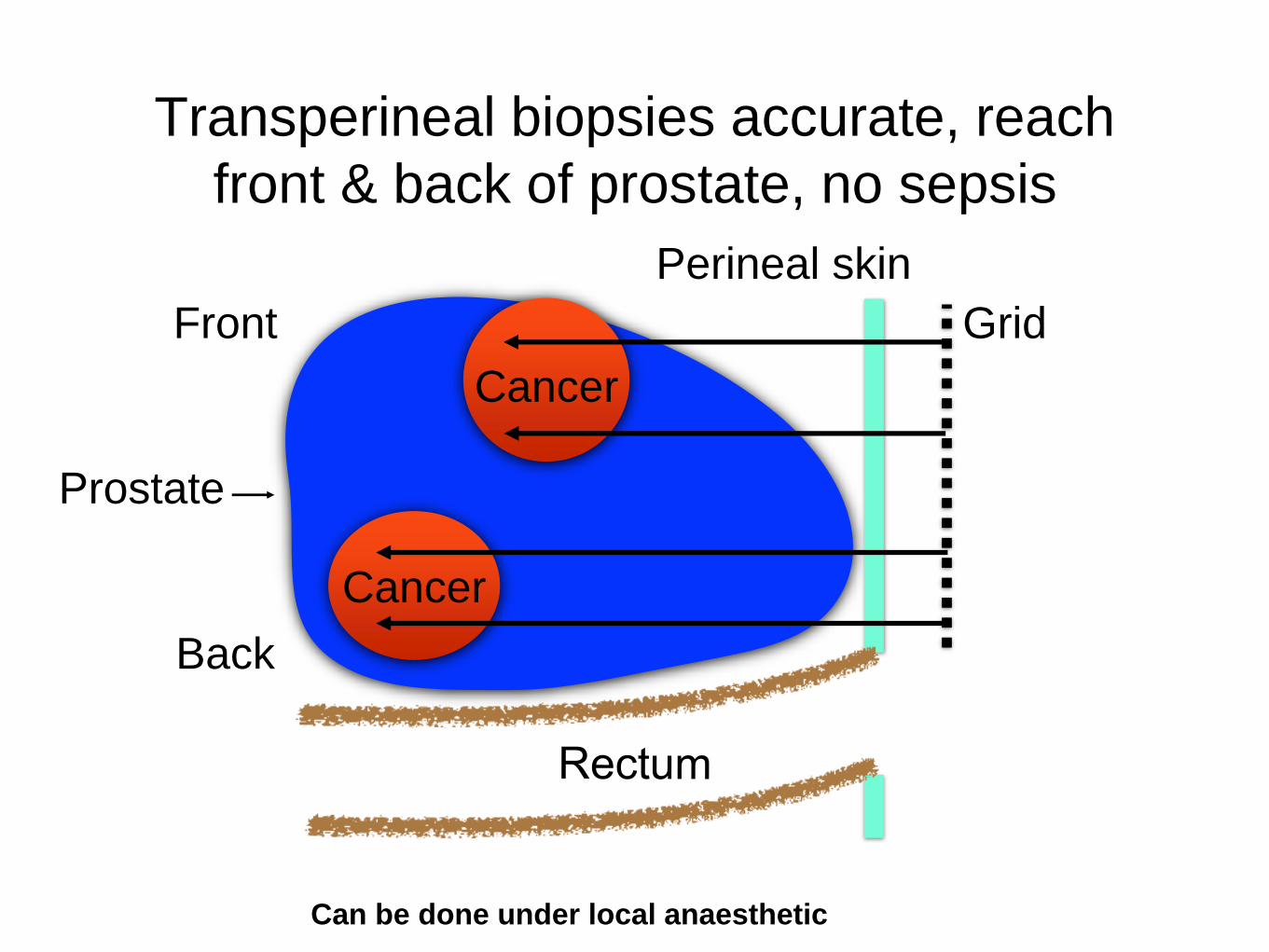
Transperineal biopsies accurate, reach
front & back of prostate, no sepsis
Front
Cancer
Prostate
Perineal skin
Grid
Back
Cancer
Can be done under local anaesthetic
Q: 47 y.o. man, father had prostate cancer,
benign-feeling prostate, PSA 2.7 mcg/L
A. You admonish him for having had his PSA test and
tell him never to do it again
B. you advise him that his PSA is normal, and to
forget about
C. you tell him to repeat his PSA & will make a
Suspected Cancer Referral only if the PSA is the
same or more
D. You give him two weeks of an antibiotic
(ciprofloxacin/trimethoprim) & repeat his PSA in
another 2 weeks
E. You tell him that randomised studies have shown
no benefit in PSA testing and treatment makes no
difference anyway
PCRMP guidance states that
"The PSA test is available free to any
man aged 50 or over who requests
it, after careful consideration of the
implications".
https://www.gov.uk/guidance/prostate-cancer-risk-management-programme-overview

PSA testing in asymptomatic men
Prostate Cancer Risk Management Programme,
Public Health England 2016
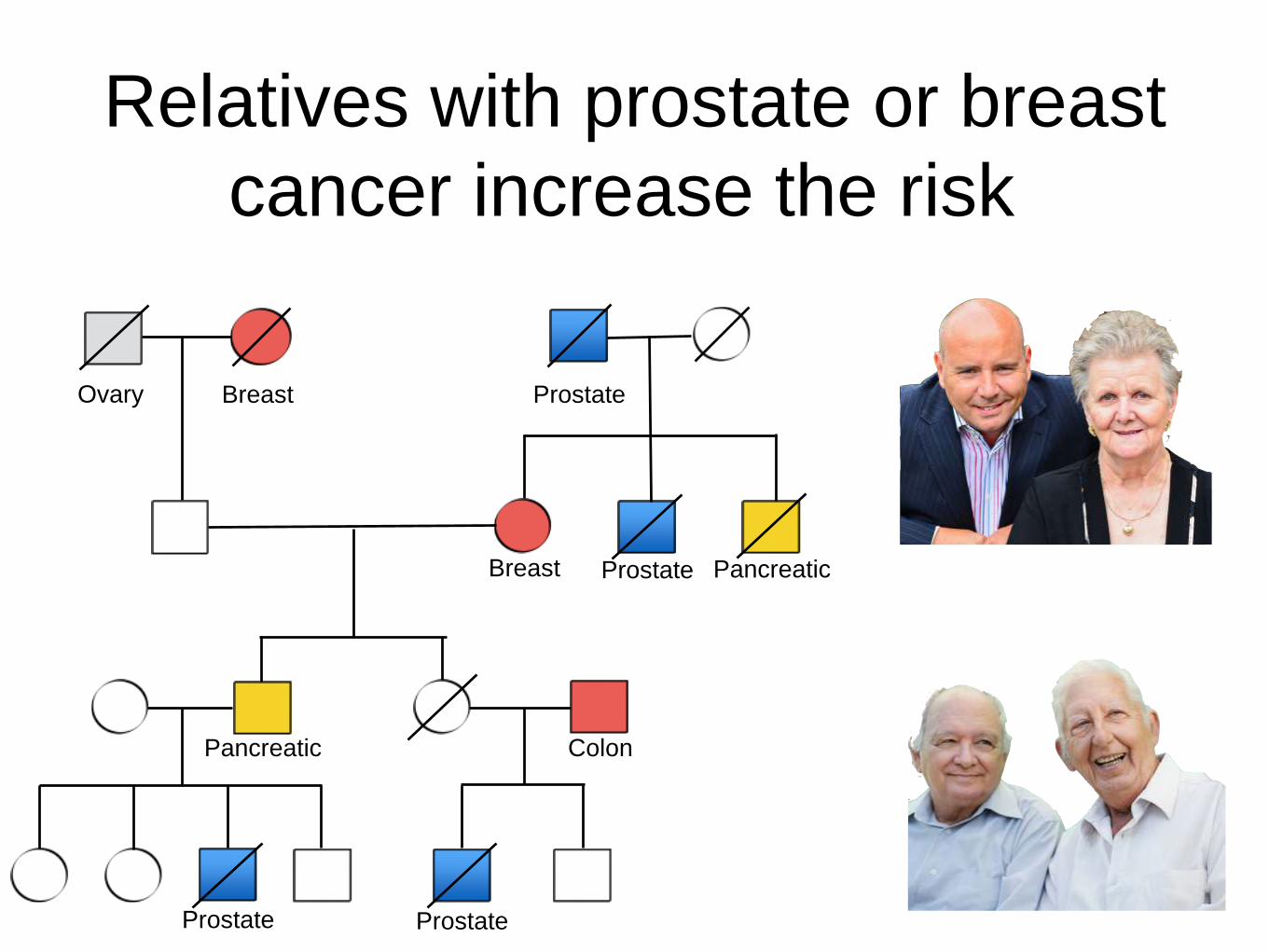
Relatives with prostate or breast
cancer increase the risk
Pancreatic
Prostate
Prostate PancreaticBreast
Breast
ProstateProstate
Ovary
Colon
https://prostatecanceruk.org/for-health-professionals/our-
projects/psa-consensus-for-health-professionals

Prostate Cancer Diagnostic Pathway with mpMRI and transperineal biopsies
31
PSA > 3 or > 2.5 with risk
factorsmpMRI
Suspicion score 3, 4 ,5
Suspicion score 1, 2
Targeted transperineal
prostate biopsies
transperineal systematic biopsies
PSA surveillance & repeat mpMRI
Biomarker?
No mpMRI
PSAD = PSA density (PSA/prostate volume)
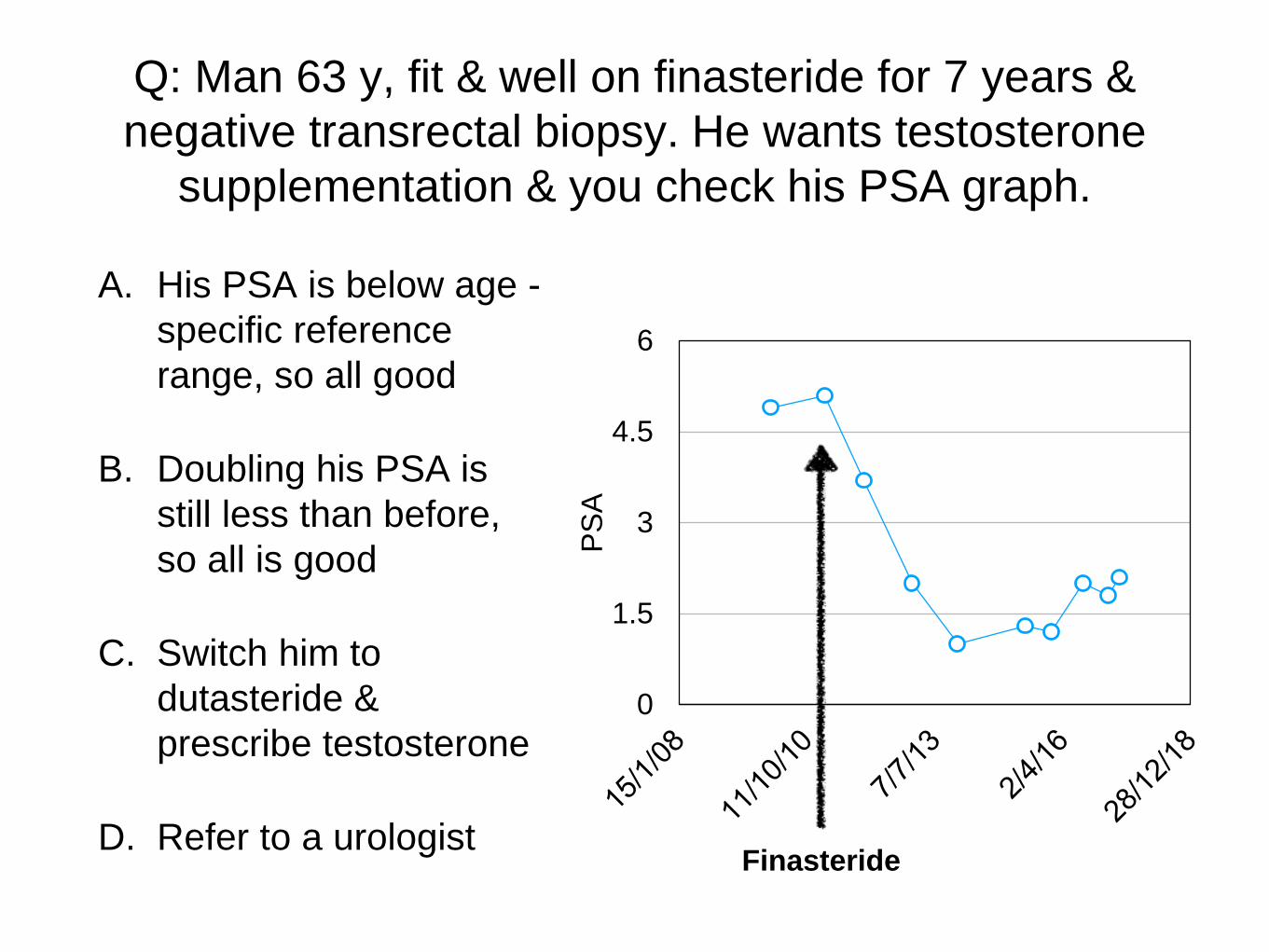
Q: Man 63 y, fit & well on finasteride for 7 years &
negative transrectal biopsy. He wants testosterone
supplementation & you check his PSA graph.
A. His PSA is below age -
specific reference
range, so all good
B. Doubling his PSA is
still less than before,
so all is good
C. Switch him to
dutasteride &
prescribe testosterone
D. Refer to a urologist
0
1.5
3
4.5
6
PS
A
Finasteride

Finasteride shrinks benign prostate tissue;
significant cancer continues to still grow
Low risk tumour
High-risk tumour
Proportion occupied by the tumour
increased after background prostate shrinks
Proportion occupied by the growing tumour
increases even more after background prostate shrinks
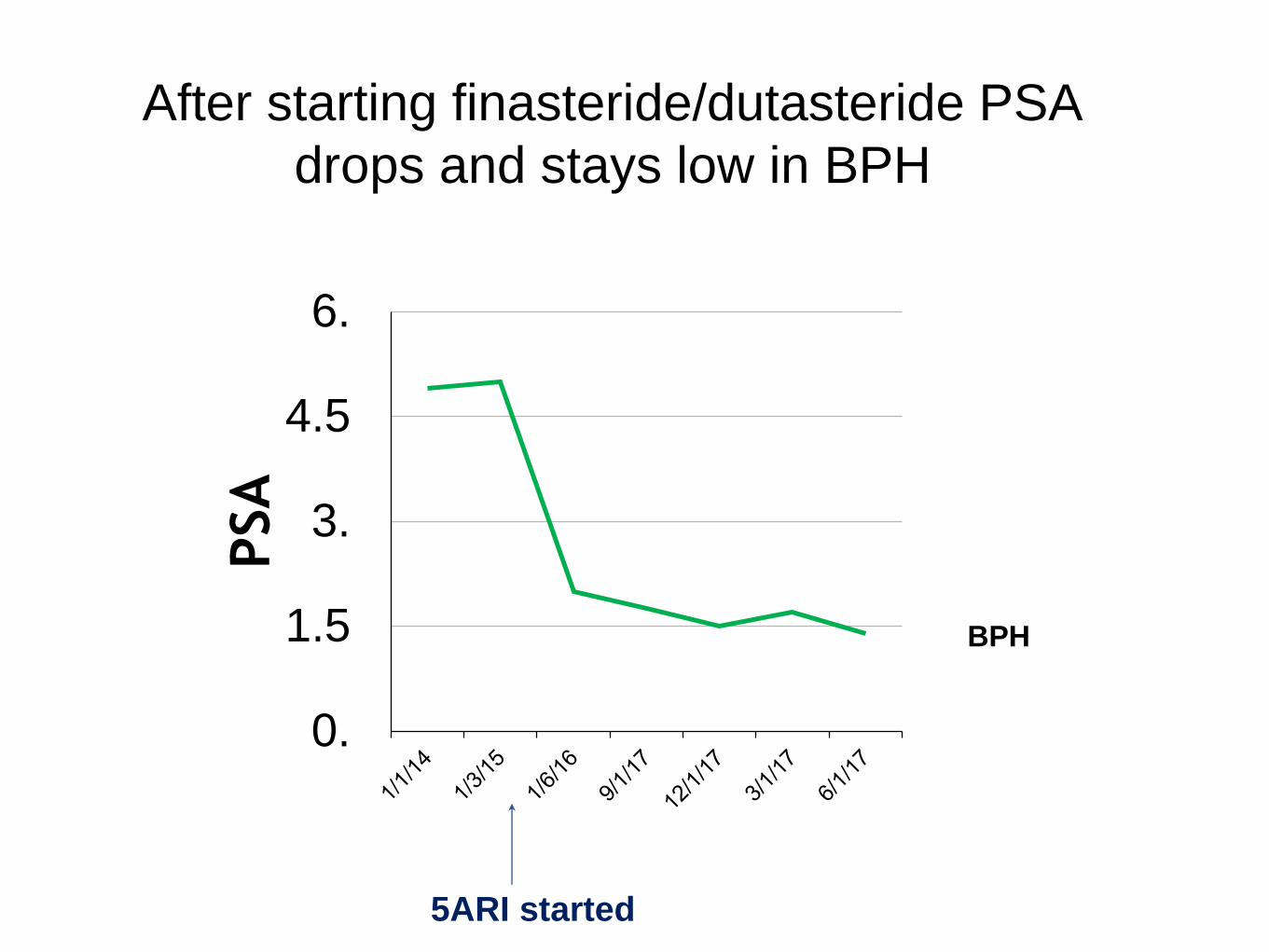
After starting finasteride/dutasteride PSA
drops and stays low in BPH
0.
1.5
3.
4.5
6.
PSA
5ARI started
BPH
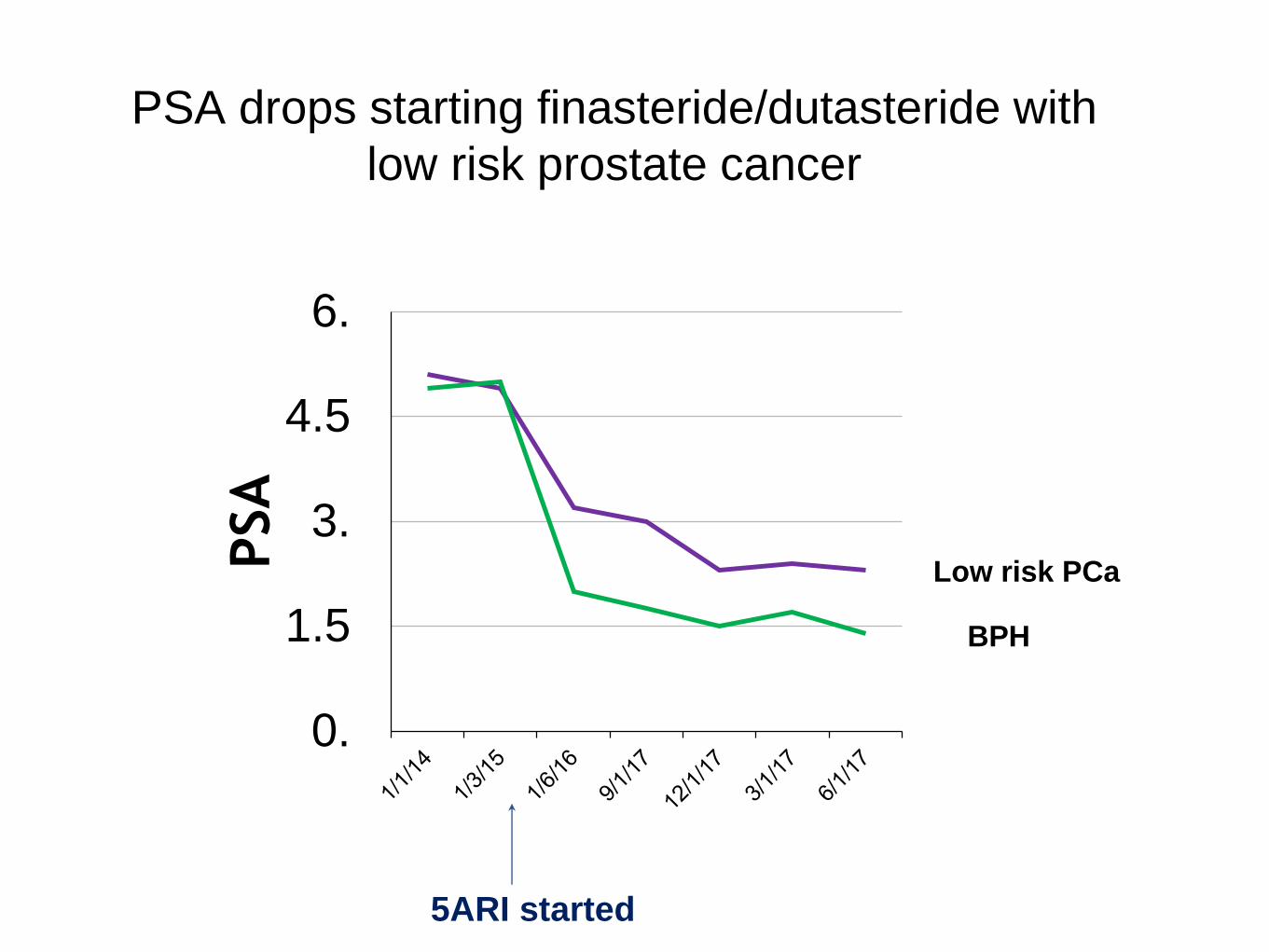
PSA drops starting finasteride/dutasteride with
low risk prostate cancer
0.
1.5
3.
4.5
6.
PSA
5ARI started
Low risk PCa
BPH
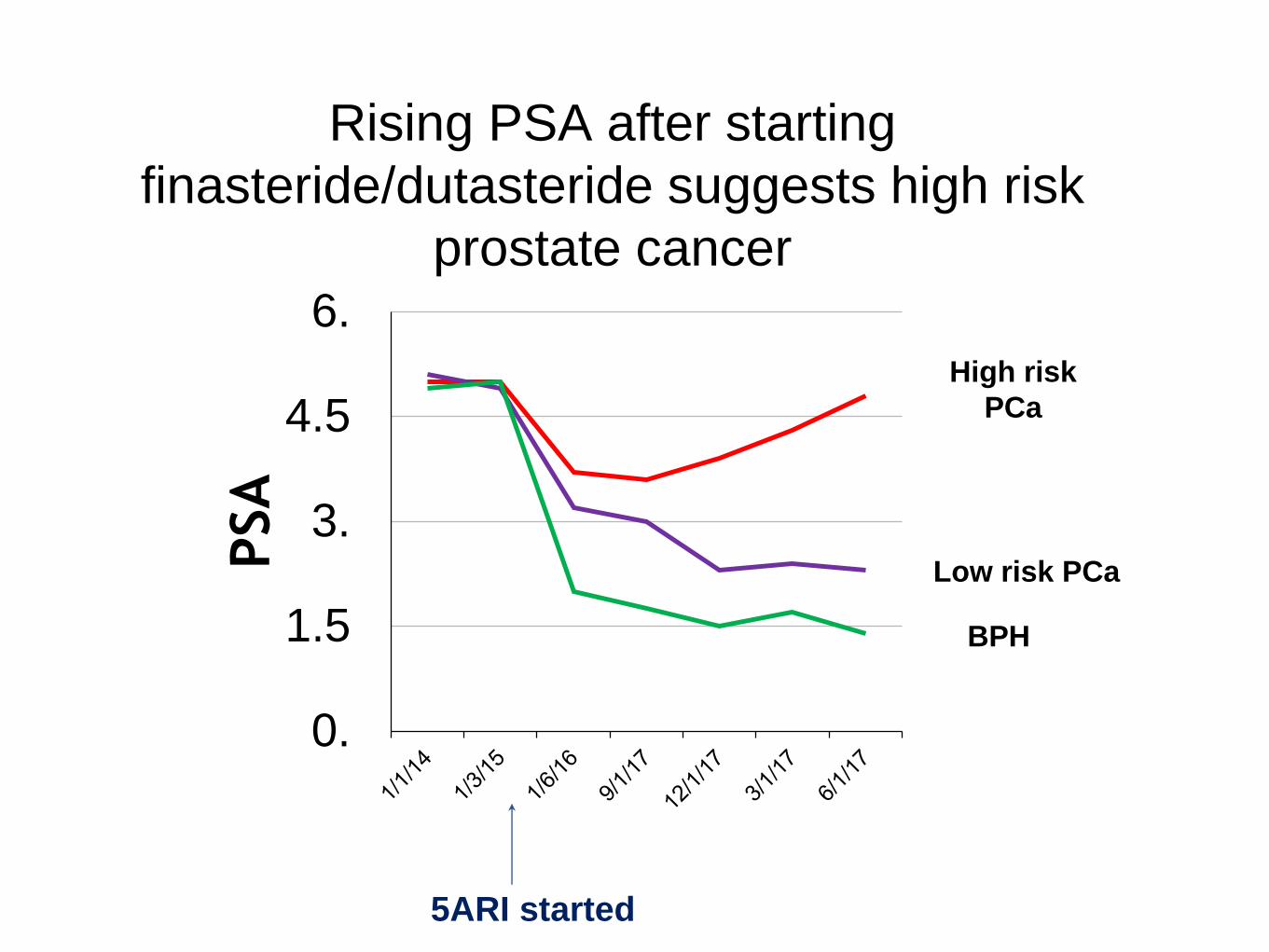
Rising PSA after starting
finasteride/dutasteride suggests high risk
prostate cancer
0.
1.5
3.
4.5
6.
PSA
5ARI started
High risk
PCa
Low risk PCa
BPH
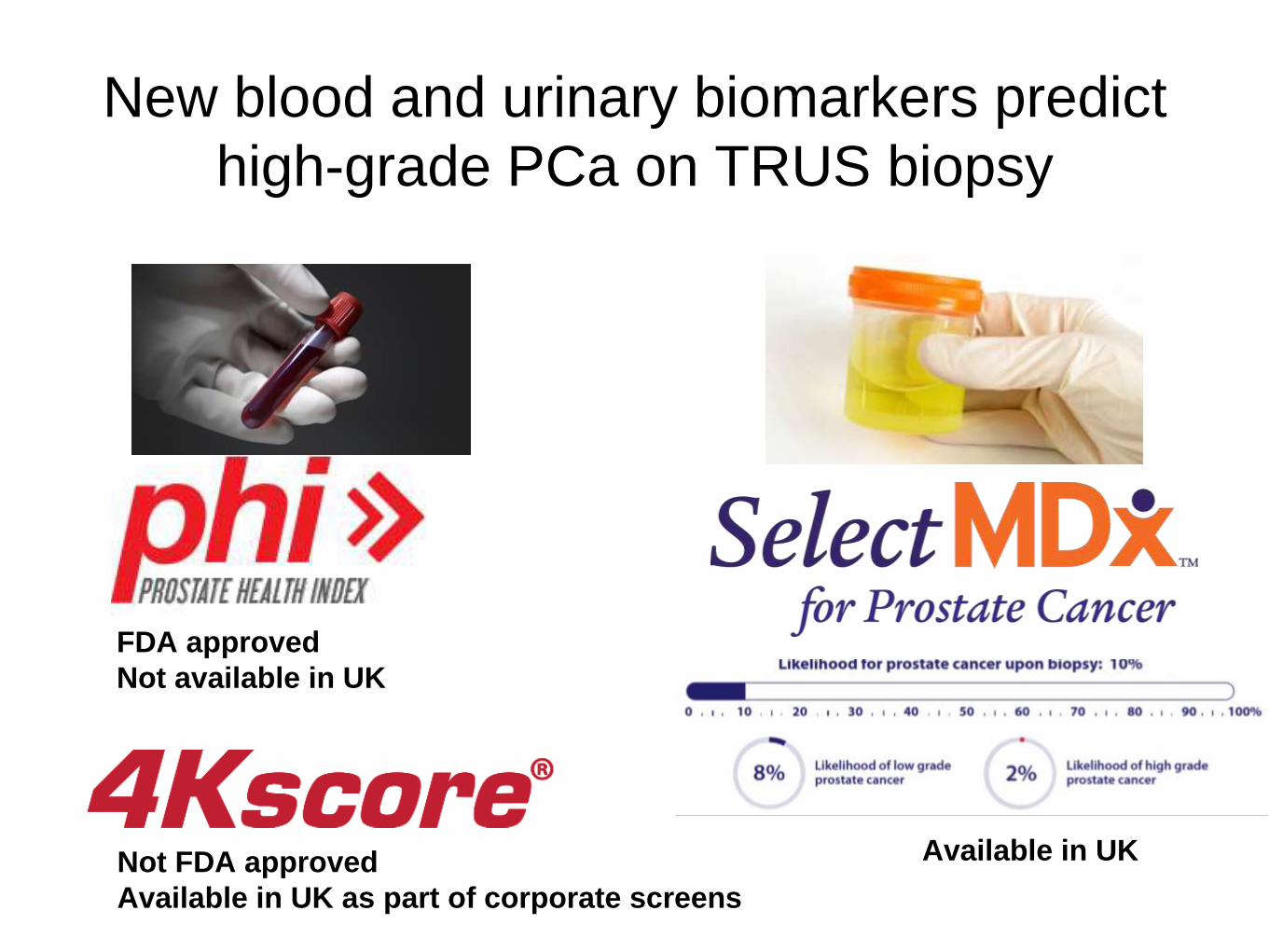
New blood and urinary biomarkers predict
high-grade PCa on TRUS biopsy
•
FDA approved
Not available in UK
Not FDA approved
Available in UK as part of corporate screens
Available in UK
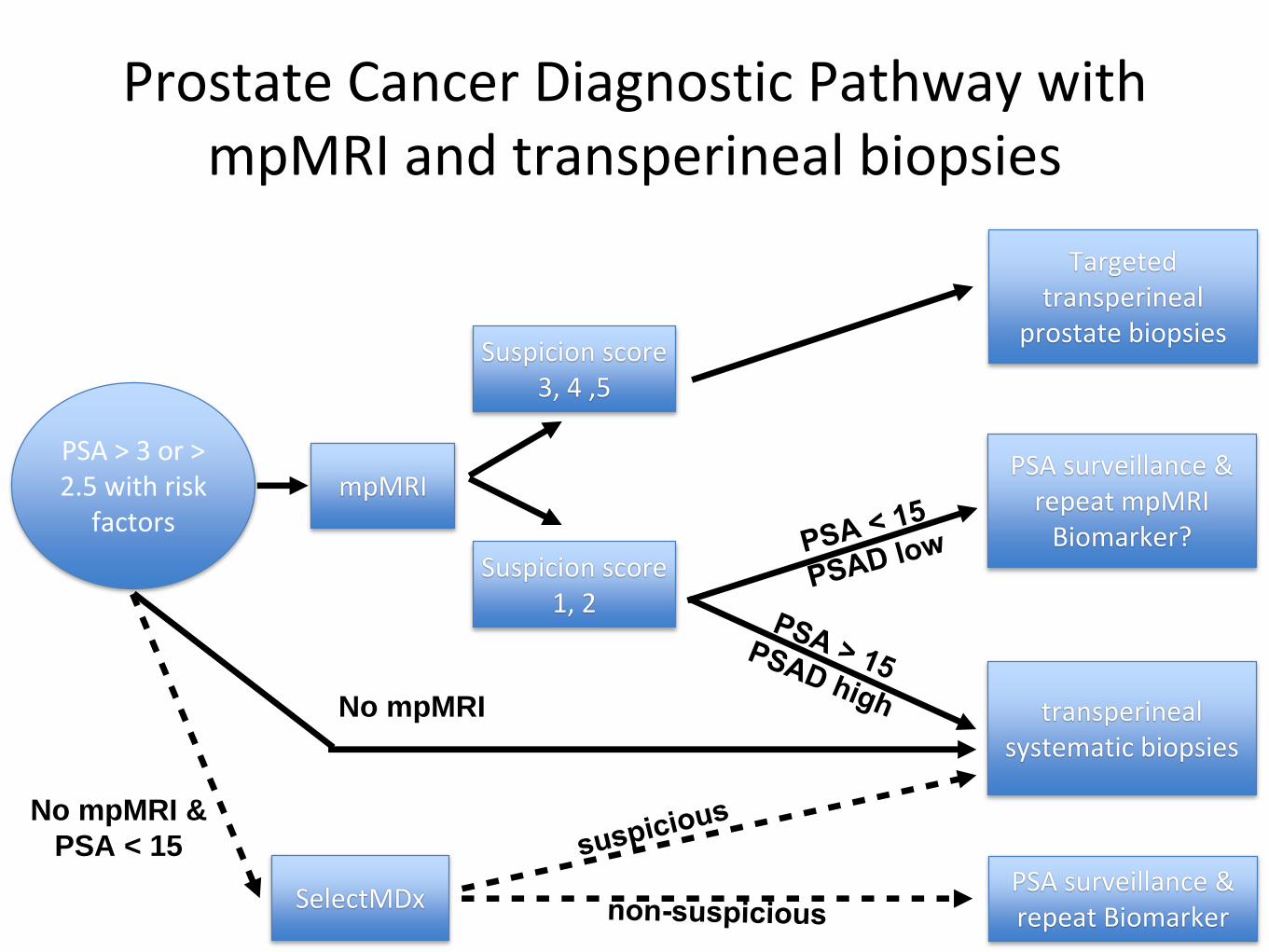
Prostate Cancer Diagnostic Pathway with mpMRI and transperineal biopsies
38
PSA > 3 or > 2.5 with risk
factorsmpMRI
Suspicion score 3, 4 ,5
Suspicion score 1, 2
Targeted transperineal
prostate biopsies
transperineal systematic biopsies
PSA surveillance & repeat mpMRI
Biomarker?
No mpMRI &
PSA < 15
SelectMDxPSA surveillance & repeat Biomarker
No mpMRI


















