How the Interventionist can Get It Right First Time-...How the Interventionist can Get It Right...
23
How the Interventionist can Get It Right First Time- Optimising quality, reducing unwarranted variation and delivering cost effectiveness in UK (interventional) cardiology practice Dr Sarah Clarke Immediate Past President British Cardiovascular Society Consultant Cardiologist and Clinical Director Strategic Development Royal Papworth Hospital Joint National Lead for GIRFT Cardiology
Transcript of How the Interventionist can Get It Right First Time-...How the Interventionist can Get It Right...

How the Interventionist can Get It Right First Time-
Optimising quality, reducing unwarranted variation and delivering cost effectiveness in UK
(interventional) cardiology practice
Dr Sarah ClarkeImmediate Past President British Cardiovascular Society
Consultant Cardiologist and Clinical Director Strategic DevelopmentRoyal Papworth Hospital
Joint National Lead for GIRFT Cardiology
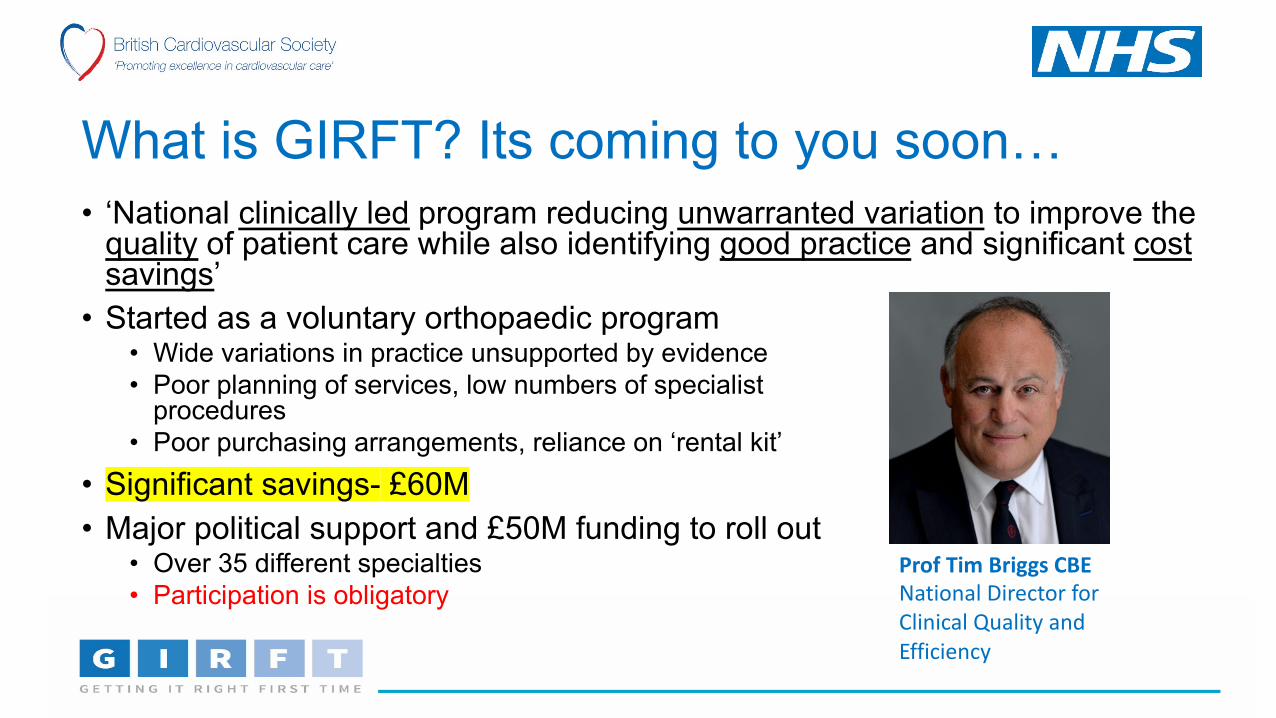
What is GIRFT? Its coming to you soon…• ‘National clinically led program reducing unwarranted variation to improve the
quality of patient care while also identifying good practice and significant costsavings’
• Started as a voluntary orthopaedic program• Wide variations in practice unsupported by evidence• Poor planning of services, low numbers of specialist
procedures• Poor purchasing arrangements, reliance on ‘rental kit’
• Significant savings- £60M
• Major political support and £50M funding to roll out• Over 35 different specialties• Participation is obligatory
Prof Tim Briggs CBENational Director for Clinical Quality and Efficiency

Appointed GIRFT Clinical Leads for Cardiology
Clinical Leads usually senior representatives of professional societyEngagement with subspecialty groups in preparatory work

How it Works….Data packs sent to each Trust• Data packs assembled for each Trust –benchmarked against
others• About 150 in England- all will be visited
• Multiple clinical data sources• Hospital episode statistics (HES)- coding, OP, elective, emergency spells• National clinical audit datasets, NICOR- outcome data (PCI, TAVI)• Questionnaire to hospitals- staffing, clinical pathways and NCBC data
• Non clinical datasets• Purchasing data• Litigation data

GIRFT cross-cutting themes:clinical service lines
ED & Acute Admissions
Outpatients Pathology services
Diagnostic services
Critical & Intensive
Care
Anaesthetics Perioperative

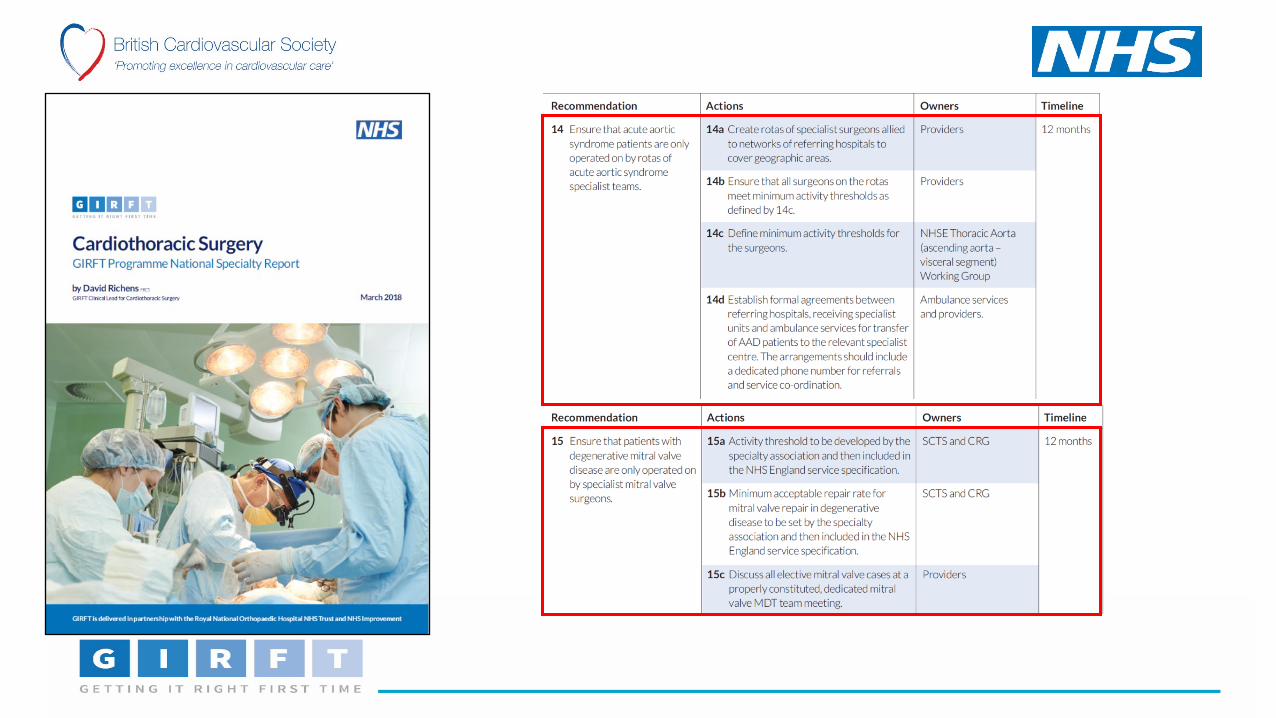
How it works….peer to peer ‘deep dives’
• Clinical leads• ‘Deep dive’ visits to every Trust providing cardiology• Review key elements of data packs with senior clinical
and management teams• Seek examples of good practice• Make recommendations• Individual report• Later meeting with Trusts at STP level
• National specialty report summarising main themes

Implementation after ‘deep dive’
• Each Trust has a ‘responsible officer’
• Usually the Medical Director
• Responsible for delivering on recommendations
• Seven regional hubs
• Clinical Ambassadors for GiRFT
• GIRFT implementation team
• Support for hospitals in implementation and
breaking down barriers to change
• Revisit from clinical leads at 6 months
• Ensure implementation in progress
• Further input from national team, STP level

What are we looking at in cardiology?• Overall service and staffing• Access to specialist opinion / treatment
• 7/7 – ward rounds to review admitted / unwell patients• 24/7 – oncall access to specialist advice/review• 7 day access to key diagnostics – echocardiography• Out patients
• New:FU ratio• Advice and guidance for primary care• Virtual clinics
• Appropriate pathways in specific areas (guidelines- NICE, ESC)• Stable chest pain NICE guidelines• NSTEMI- NICE, ESC guidelines• Heart failure• TAVI(R)• Pacing- out of hours
• Procedural access and activity• Cath lab and utilisation• Imaging eg CT. MR
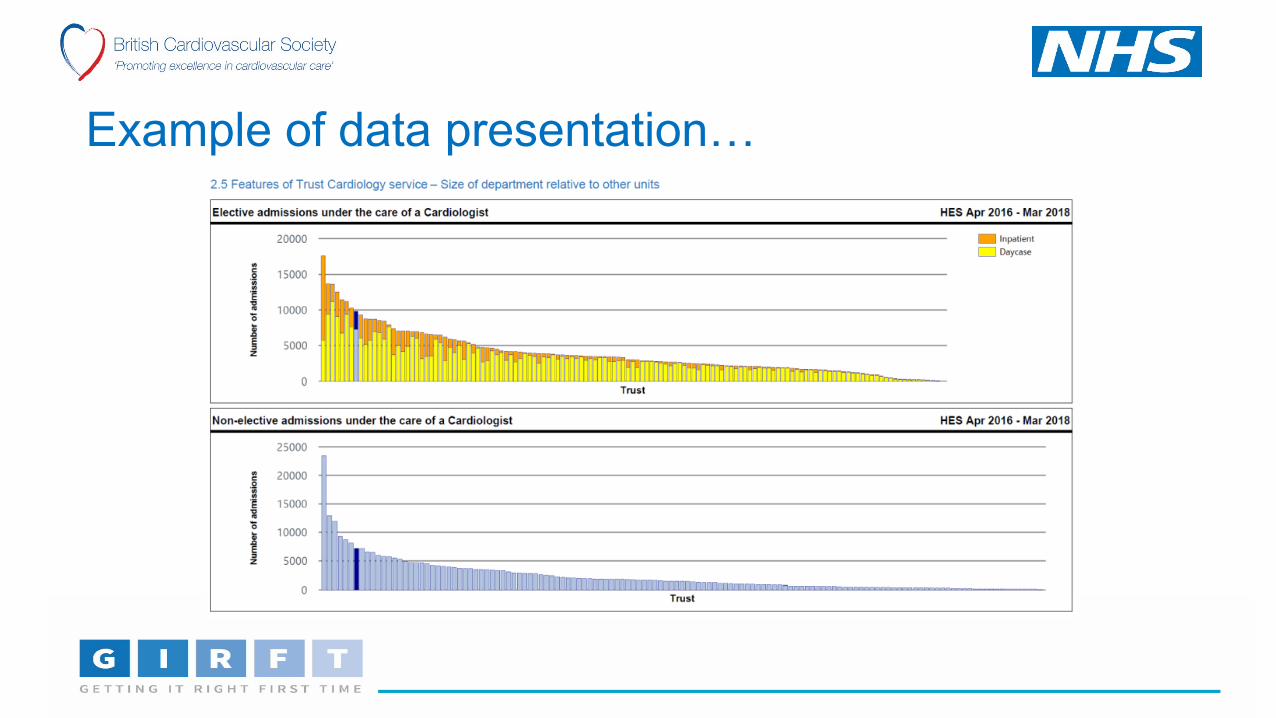
Example of data presentation…
ID: GB-13673 (Prepared September 2018)
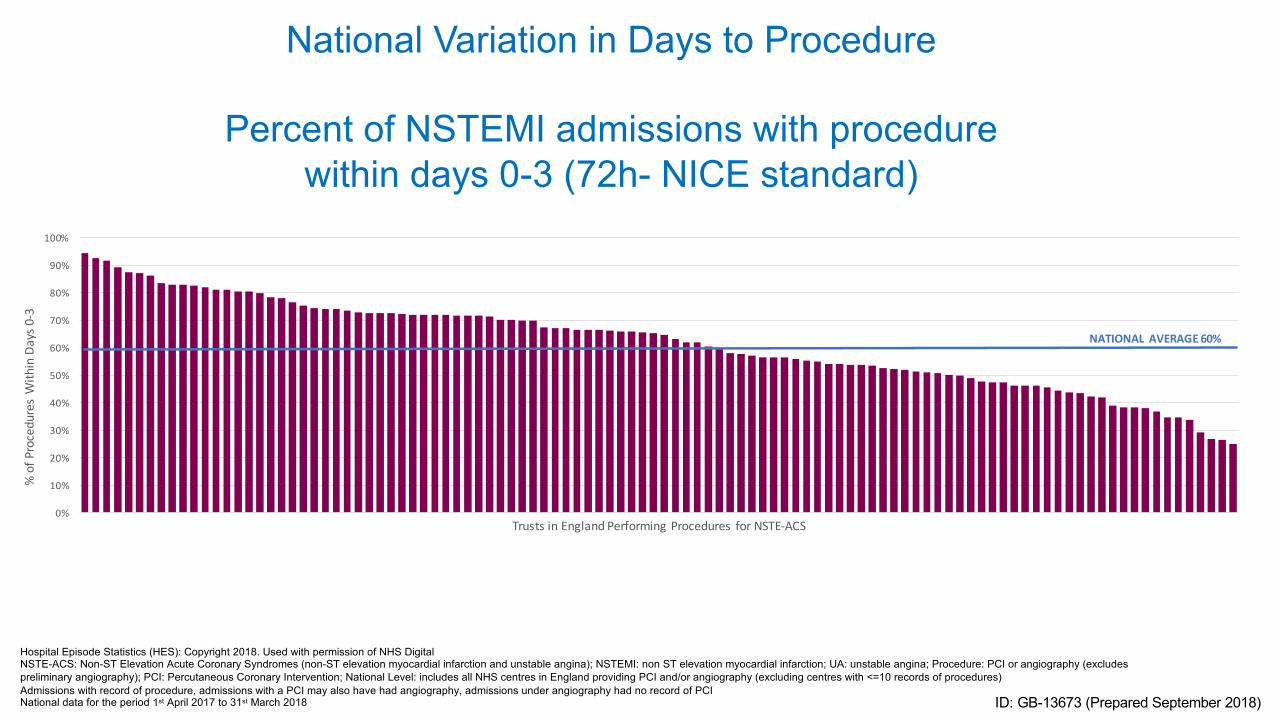
Hospital Episode Statistics (HES): Copyright 2018. Used with permission of NHS Digital NSTE-ACS: Non-ST Elevation Acute Coronary Syndromes (non-ST elevation myocardial infarction and unstable angina); NSTEMI: non ST elevation myocardial infarction; UA: unstable angina; Procedure: PCI or angiography (excludes preliminary angiography); PCI: Percutaneous Coronary Intervention; National Level: includes all NHS centres in England providing PCI and/or angiography (excluding centres with <=10 records of procedures)Admissions with record of procedure, admissions with a PCI may also have had angiography, admissions under angiography had no record of PCINational data for the period 1st April 2017 to 31st March 2018
National Variation in Days to Procedure
Percent of NSTEMI admissions with procedurewithin days 0-3 (72h- NICE standard)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% o
f Pro
cedu
res
With
in D
ays 0
-3
Trusts in England Performing Procedures for NSTE-ACS
NATIONAL AVERAGE 60%

ID: GB-13673 (Prepared September 2018)
Hospital Episode Statistics (HES): Copyright 2018. Used with permission of NHS Digital NSTE-ACS Admissions without CABG. The Average Bed Days includes bed days from first admission to end of procedural admission i.e. a “super spell” (data excludes repatriation admissions involving Trust transfers)CABG: Coronary Artery Bypass Graft; NSTE-ACS: Non-ST Elevation Acute Coronary Syndromes (non-ST elevation myocardial infarction and unstable angina); NSTEMI: non ST elevation myocardial infarction; UA: unstable angina; Procedure: PCI or angiography (excludes preliminary angiography); PCI: Percutaneous Coronary Intervention; National Level: includes all NHS centres in England providing PCI and/or angiography (excluding centres with <=10 records of procedures)Admissions with record of procedure, admissions with a PCI may also have had angiography, admissions under angiography had no record of PCINational data for the period 1st April 2017 to 31st March 2018
National Variation in Bed Days
Average Bed Days for NSTE-ACSAdmissions with a Procedure
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
Aver
age
Bed
Days
Trusts in England Performing Procedures for NSTE-ACS
NATIONAL AVERAGE 6.2 BED DAYS



Radial access…identifying centres
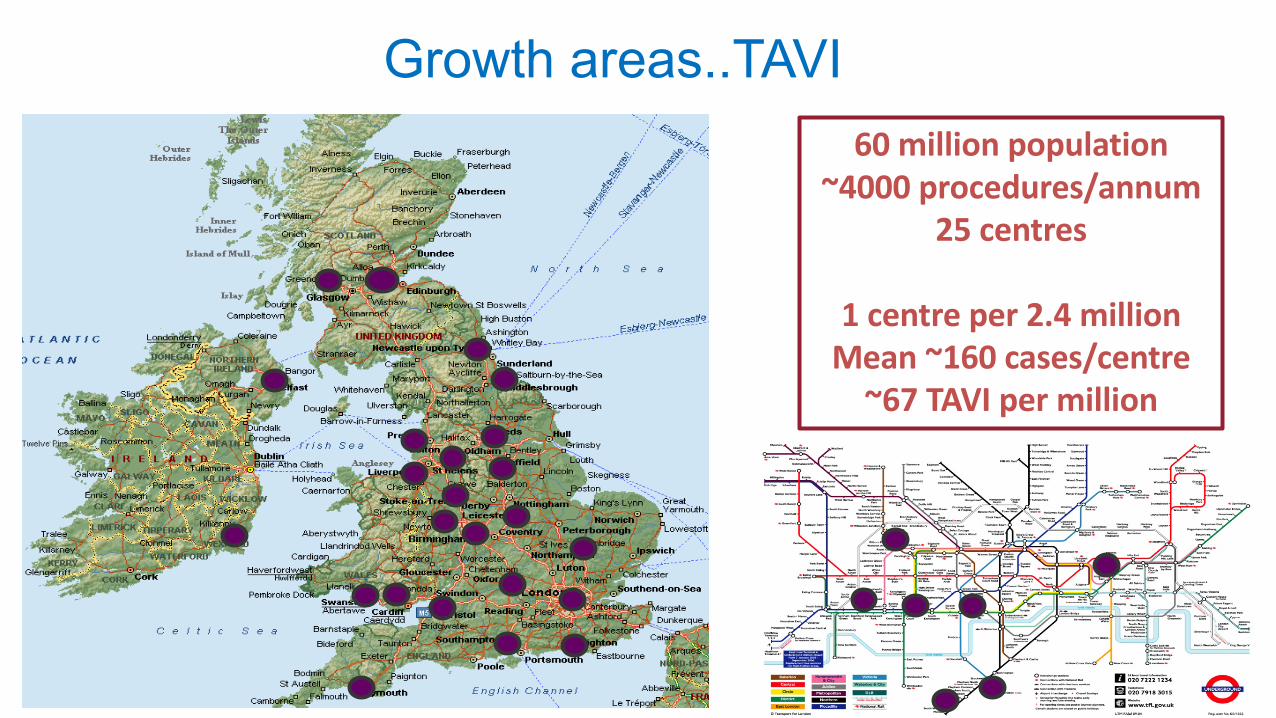
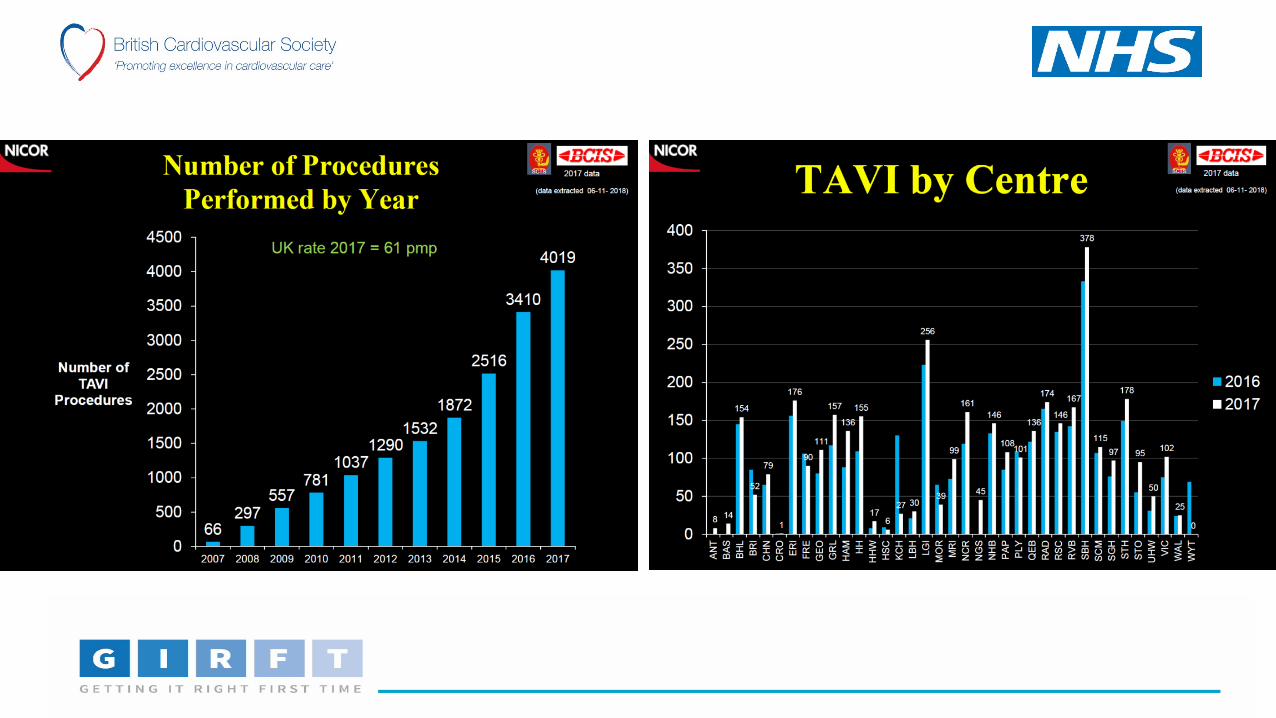
Growth areas..TAVI60 million population
~4000 procedures/annum25 centres
1 centre per 2.4 millionMean ~160 cases/centre
~67 TAVI per million

TAVI- quality metrics HES vs NICOR

Non-clinical data- device costs
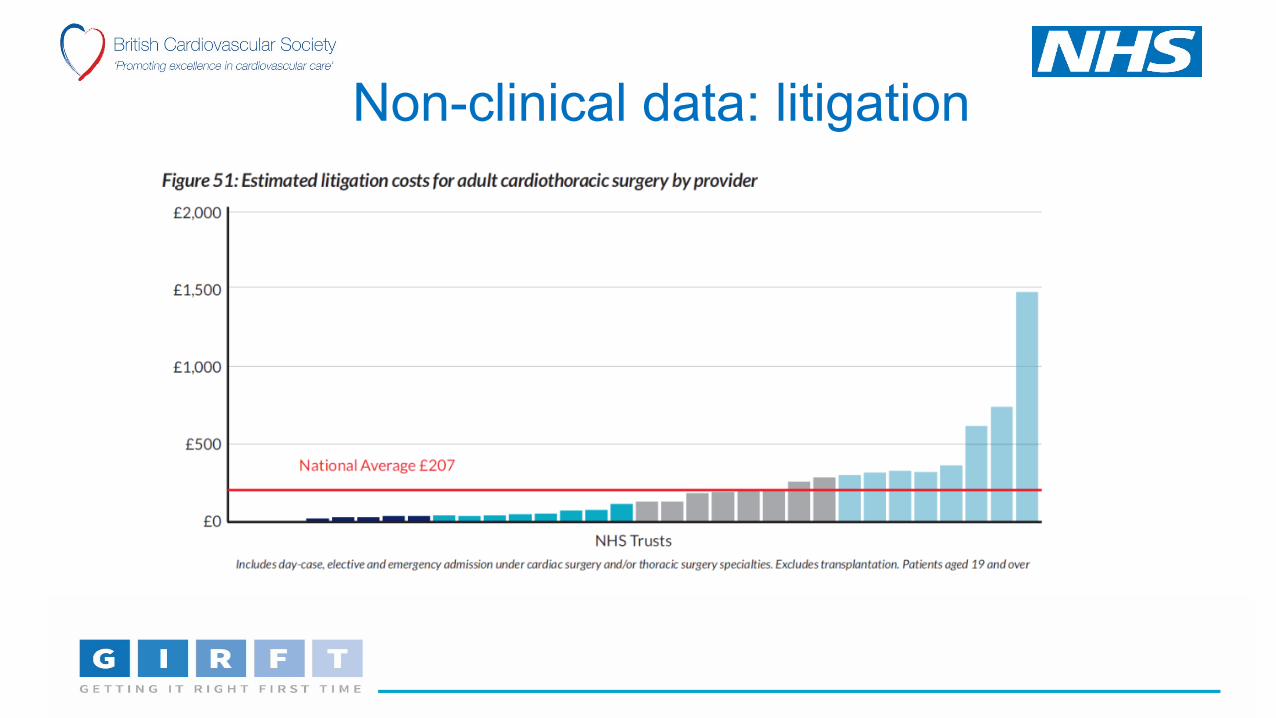
Non-clinical data: litigation

What is different about GIRFT?• Clinically led• Engagement with national professional societies and affiliated
societies• High level political buy in• Dynamic national leadership• Empowered to deliver change• Major financial investment to deliver

The Future…Upsides and downsides• Upsides
• Best chance we have got of making significant change in service delivery• Recognition of the importance of data collection• Focus on ‘global’ quality and cost effectiveness NOT budget reduction• Co-operation between clinicians and management
• Downsides• Limitation of ‘clinical freedom’• Risk of GIRFT fatigue