How standards for integration will enable key business objectives. Jagdip Grewal Chief Technical...
29
How standards for How standards for integration will enable integration will enable key business objectives. key business objectives. Jagdip Grewal Jagdip Grewal Chief Technical Chief Technical Architect Architect
-
Upload
jewel-rogers -
Category
Documents
-
view
216 -
download
3
Transcript of How standards for integration will enable key business objectives. Jagdip Grewal Chief Technical...

How standards for How standards for integration will enable integration will enable key business objectives.key business objectives.
Jagdip Grewal Jagdip Grewal
Chief Technical ArchitectChief Technical Architect

Agenda
• CFH Update and Why are we here?• Enterprise Architecture – Integration Domain• CFH and HL7 CDA• The Future

Our Objectives
To deliver a 21st century health service through efficient use of technology to:
• Enable and improve Access and
Choice
• Enable care pathways and
patient focus
• Improve accuracy in treatment
• Create opportunities for
improved efficiency
• Create opportunities for real
NHS reform

……and the NHS in England and the NHS in England is BIGis BIG
In a typical week:• 6 million6 million people will visit their GPs• More than 800,000800,000 outpatients will be treated• Over 10,00010,000 babies will be delivered by the NHS • NHS ambulances will make over 50,00050,000 emergency journeys • Pharmacists will dispense approximately 8.5 million8.5 million items• NHS surgeons will perform around 1,2001,200 hip operations, 3,0003,000
heart operations and 1,0501,050 kidney operations• Labs and associated services will provide results on
millionsmillions of tests
Or another way, 3 million3 million critical transactions a day
There is no way to do this on a small scaleThere is no way to do this on a small scale

SupplySupply --sidesideReformsReforms
DemandDemand --side side ReformsReforms
Transactional Transactional
Reforms
System Management
Reforms
Better careBetter patient
experienceBetter value for
money
System Management
Standards, Accreditation & Inspection
Values, Brands & Codes
Planning, Performance & Assessment
Financial Strategy
Wider Review of Regulation
Payment by Results
Information Strategy & Systems
Payment & Settlement
Plurality in Primary Care
Foundation Trusts
Plurality / Contestability
Independent Sector
NHS Treatment Centres
Out of Hospital
18 Weeks
Workforce
Patient Choice
Commissioning
PCT Development
Patient Info
Long Term Conditions
Demand Management
Motivation: Why ?

Progress to date
• NHS Connecting for Health deployment statistics (to 3 October 2006) 276,899 users registered for access to the Spine 5,654,360 prescription messages transmitted using
the Electronic Prescription Service (EPS) 1,348,277 Choose and Book bookings 70,907,782 images stored using Picture Archiving and
Communications Systems (PACS) 15,686 National Network (N3) connections
• Thousands of systems exchanging information Over 9000 Accredited Systems connected

Why are we here?
• Enable the best integrated healthcare by the time these children grow up!

Agenda
• CFH Update and Why are we here?• Enterprise Architecture – Integration Domain• CFH and HL7 CDA• The Future

Enterprise Architecture – Integration is a key domain
Sec
uri
ty
Inte
gra
tio
n
Infrastructure
Enterprise Services
Channels
Local Services
Views

Infrastructure
Enterprise Services
Local Services
Channels and Presentation IntegrationSecurity
Information, Knowledge and
Research Services
Diagram file: Conceptual IS IT services v10.vsd
Profiling & personalisation
Session & context management
Scanning[116.6]
Reporting [385.7.17, 720.6.4, 600.5.5,
360.14.9]Deployment
Scheduling Services
Enquiry Support
Network ServicesPrint
managementMonitoring [360.6.8,
et al] Fault management
[600]Help desk Support
[600]
Reporting including Statutory Reports
Electronic Booking Service [109]
Terminology Data Services
[380]
E Booking [109]
Financial Services [117]
Operational reports
Clinical audit Data Sets
Ad Hoc Reports
Configurable reports [124.3]
Analytical tools [124.4]
Search & Lookup
Virtual Visiting[123.2]
Home monitoring[107.5.2 & 123.1]
Bed mgmt [107.7]
Diagnostic & Investigative
Services [114]
Patient Record Presentation
Requesting services [110]
Results Mgmt [111]
Decision Support [112]
Alerting
Clinical Noting [106.5]
Clinical Performance Management Information
Reporting
Connectivity
Audit: Local Capture & management
Audit record Consolidation
(Cluster)
Audit: View, Analyse, Search
SSOAuthentication
114.10.15
RBAC 730.12
Consent management [730.1]
Patient Record Access Control
[730.17]
Sealed envelopes [730.48]
Digital Signature[730.67]
Encryption [730.87.2, 975.6.3]
User Registration
User Directory
Central Audit
Audit record Consolidation
(National)
Local Application Integration
Social Care Integration
Legacy Departmental integration
Legacy Reporting integration
Data MigrationVideo Conferencing [123.3]
Order Management [110.11]
Dispensing[113.12]
Prescribing [113.6 – 11]
Medicines Administration
[113.13-15]
Enterprise Directory Services [350]
Service directory
Service registration maintenance
Workflow and Business Rules Services [370]
Validation
Transformation
Coordination, Reminder, Alert
Workflow management
Clinical Summary Access [311]
View Spine data
Update Spine data
Prescribing Alerts
Print prescription
Management Reports 311.19
Secondary Data Uses [385]
Pseudonymisation
Data storage
Data extract
Data transfer
Analysis
Demographics [211]
NHS No. Services
Patient trace & info
Registration & Maintenance
Reporting
External Interfaces
Screening
Service Hosting
Clinical Summary Records [200]
Update stored data types
Store, maintain, retrieve summary etc data
Duplicate Record mgmt
Create event, workflow or alert
Medications Management (EPS) [769]
Prescribing [113.6-11]
Dispensing 113.12
Medication mgmt recording
Update patient record
User interface services
Device and media repurposing
Disaster Recovery [720]
Data backup
Replacement IS and IT resources
Restore services
Devices
Peripherals
NHS Direct122
Patient Personal Health Information
(MyHealthSpace 311)
Document Management
[116]
Data Quality Services [736]
Workflow [101.7]
Workflow 101.7
Manage access
Create & manage Kbase
Patient & Identification Services
Patient Identification
[102]
In patient Tracking
Registration [102]
Duplicate Record mgmt
Address lookup & validation
Care management
Caseload mgmt
Waiting list mgmt
Referral mgmt
Major incident mgmt
Scheduling mgmt
[108, 114]
Assessment services [104]
Medicines Administration
[113.13-15]
Encounter mgmt
Resource mgmt
health issue mgmt
patient tracking
risk & warnings mgmt
professional care relationship
mgmt
Admission Transfer
Discharge
Patient incident and complaint
mgmt
Interventions mgmt
Mental health Act admin mgmt
Prevention, Screening,
Surveillance [103]
Demand & Access mgmt
[107.8]
Care management
Model Care pathways & plans 105.5
Care pathways 105.6
Care Planning 105.10 - 11
Correspondence mgmt [106.6]
NSF Support
Diabetes NSF 162
Cancer NSF [163]
Older People’s NSF [165]
Children’s NSF [166]
Coronary NSF [164]
Renal NSF [167]
Long Term Care NSF [168]
NSF Information Services [160]
Setting Specific Services
Ambulance [154]
Mental health [161]
Ambulatory Care Mgt
[107.6]
Emergency Services [122]
Maternity Services [118]
Domiciliary Care Mgt
[107.5]
Screening Mgmt
Dental[120]
Theatre management [125]
Digital Imaging [115]
Image Acquisition 115.5
Image Archive 115.6
Image Retrieval 115.7
Image Viewing 115.8
Hardcopy production 115.8.89
Enterprise Application Integration [360]
Data Transformation 360.4
Interface Mechanisms 360.3
Message validation 360.6
Message structure transformation & mapping
360.6
Business Rules and workflow 360.6
Routing 360.6
Error handling 360.6
Message Queue360.1
Translation (coding) 360.5, 380.3
EDI360.16.7
Certificate management
Demographic mgmt [102]

Integration Architecture Domain - Standards• CFH is committed to HL7
Use of V3 decision in 2003! Still needs development work and we will continue to
work within HL7 - e.g. HL7 Tooling Collaborative (
http://www.hl7toolingcollaborative.org/)
• Strategic alliance between HL7, ISO and Cen Agreed at joint meeting in Geneva, October 2006 Aim to co-ordinate work programme and joint
standards Plan to pull in others SDOs to join (e.g. SNOMED)

Allow Incremental Rollout
• All care settings will be upgrading systems for several years to come. A release from a supplier could take 1-2 years to rollout across a cluster.
• Need to enable a way of transferring information between systems which allows For different levels of SNOMED compliance of
systems And for those which are not compliant, to allow
the clinician to view the information

How do clinicians work?
• Need to be aware of information overload The right information is key
• Clinical coding teams Will be here for a while yet
• Business change in NHS will take a while

Need to enable increasing coding of clinical flows
Post-coordination
Full Pre-coord
Partial Pre-coord
Text
Provider of Care’sSystem
Primary Physician’sSystem
Post-coordination
Full Pre-coord
Partial Pre-coord
Text
SnomedCompliance
Benefits

Agenda
• CFH Update and Why are we here?• Enterprise Architecture – Integration Domain• CFH and HL7 CDA• The Future

CFH and HL7 CDA
• In Q2 06 a decision was made to adopt HL7 Clinical Document Architecture as the basis for all clinical messages.
• This supports the vision of allowing messages to flow between organisations and be processed at the capability of the receiving system. The minimum would be to view the message as a
document. GP summary message v1 (MIM 4.2) is not HL7 CDA. Other MIM domains (Emergency, Discharge etc) are
being amended to be HL7 CDA compliant to be published shortly.

About CDA – a reminder
• CDA documents carry a number of different pieces of information:
Metadata – information for document management e.g. type of document
Text – a textual representation of the clinical content which is rendered for human readability
Coded – a fully structured representation of the clinical content which is used for decision support

Components of CDA
• The clinical content in a CDA Release 2 document is stored in: Sections
- Allowing for classification and storage of narrative text- NHS CfH will define business headings and CRE Type
sections
Entries- The coded elements of the document- These will be constrained from the CDA CSP using templates

ED Care Provision Event

Templates
• Templates will allow constraints to be applied to the section, entries and roles of the CDA document
• The mechanism for templating is currently being developed by Comms and Messaging
• It will allow for greater extensibility of the messages using a modular approach as seen in MIM 4.1.04
• A library of templates will be maintained to meet changing requirements
• The following classes will have templates applied: Sections
- e.g. Business Headings, CRE Types etc Entries
- e.g. Clinical Statements Roles
- e.g. author

Template List Identifier
• The template list identifier lists the allowable templates in the same way a vocabulary lists the allowable codes
• It allows for greater extensibility of the messages as new templates can be added to the list removing the necessity to update the base model
• The format of the identifier will be:NPFIT-nnnnnn#<type>
• Examples:NPFIT-000001#RoleNPFIT-000002#ClinicalStatement

Section Template Example
The Template in ClinicalStatement is an abstract choice.
The template which will actually appear in it’s place in an instance is one from the template list identifier NPFiT-000005#Section
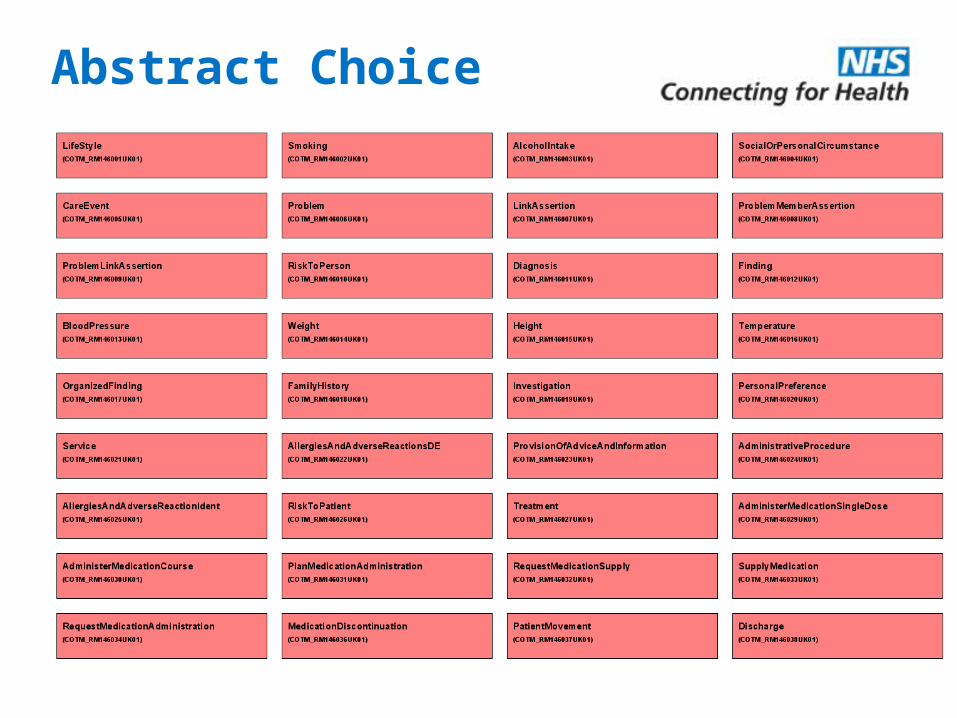
Abstract Choice

Clinical Statement Template Example
The Template in AuthorChoice is an abstract choice.
The template which will actually appear in it’s place in an instance is one from the template list identifier NPFiT-000001#Role

Validation
• The instances will carry the generic CDA class names and will be validated against the CDA schema
• The instances will be validated against the templates using a validation tool set which could include schema, schematron etc
CDA TemplatesInstance
validation validation

What will this achieve?
• Flows to and from different care settings e.g. Acute to GP Without all systems being
- HL7 v3 compliant- Fully SNOMED compliant
• Earlier benefits from information flows through CFH infrastructure (i.e. Spine)

Agenda
• CFH Update and Why are we here?• Enterprise Architecture – Integration Domain• CFH and HL7 CDA• The Future

The Future
• Devices (MRI etc.) Will collect more and more data
• Life sciences industry and genomics
• Personalised health care?
Standards - Long and interesting journey ahead….

Summary
• CFH committed to HL7 Key standard in its Enterprise Architecture
• CFH has decided to use HL7 CDA Release 2 for clinical information flows Using templates to constrain part of the
document