

How Health Plans, Employers, and Providers Improve Care ...€¦ · How Health Plans, Employers,...
24
How Health Plans, Employers, and Providers Improve Care, Efficiency and Revenue with Value-Based Care Rodrigo Giacinti, MHA Market Manager West Operations
Transcript of How Health Plans, Employers, and Providers Improve Care ...€¦ · How Health Plans, Employers,...

How Health Plans, Employers, and Providers Improve Care, Efficiency and
Revenue with Value-Based Care
Rodrigo Giacinti, MHAMarket Manager West Operations

Rodrigo Giacinti, MHAMarket Manager West Operations
2

OutlineThe Evolution of Bundled Payment Programs
Episodic Management Tools and Interventions
BPCI Advanced• Pricing• Trumping• Advanced APM •New Bundles• Timeline• Application deadline
3
1
2
3
4

BPCI Advanced Enhancements
The Evolution of Bundled Payment Programs BPCI Advanced aims to build upon knowledge gained under the legacy BPCI program to further improve the efficiency and quality of care for patients.
Legacy BPCI Program Carryover
Advanced APM status under MACRA
Continued voluntary participation
Simplified precedence rules
Hospital setting triggered
Increased ACH/PGP engagement with specialists
DRGs collapsed into clinical bundles
New bundles including 3 outpatient episodes
Risk-adjusted prospective pricing
$
Quality-based performance measures
Single payment linking services in
a 90-day period
1
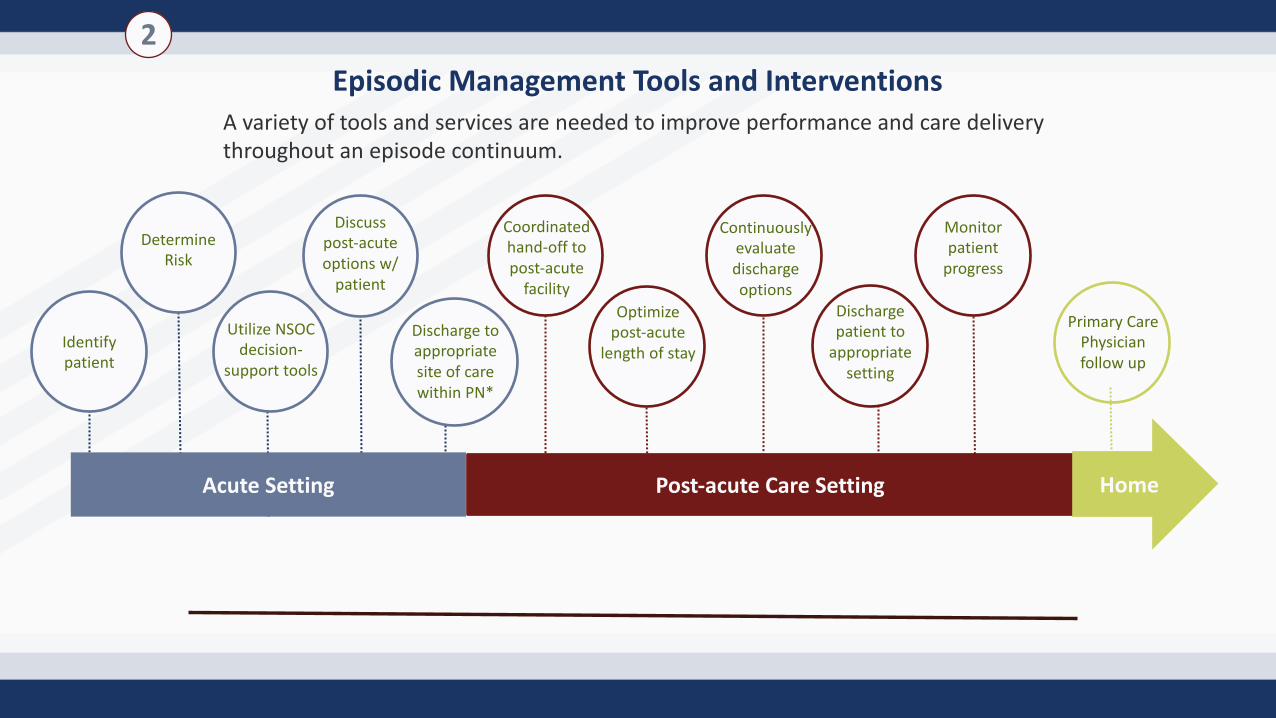
Episodic Management Tools and Interventions
Identify patient
Determine Risk
Utilize NSOC decision-
support tools
Discuss post-acute options w/
patient
Coordinated hand-off to post-acute
facilityOptimize
post-acute length of stay
Continuously evaluate discharge options
Post-acute Care Setting
Discharge patient to
appropriate setting
Monitor patient
progress
Primary Care Physician follow up
Home
Discharge to appropriate site of care within PN*
Acute Setting
A variety of tools and services are needed to improve performance and care delivery throughout an episode continuum.
2
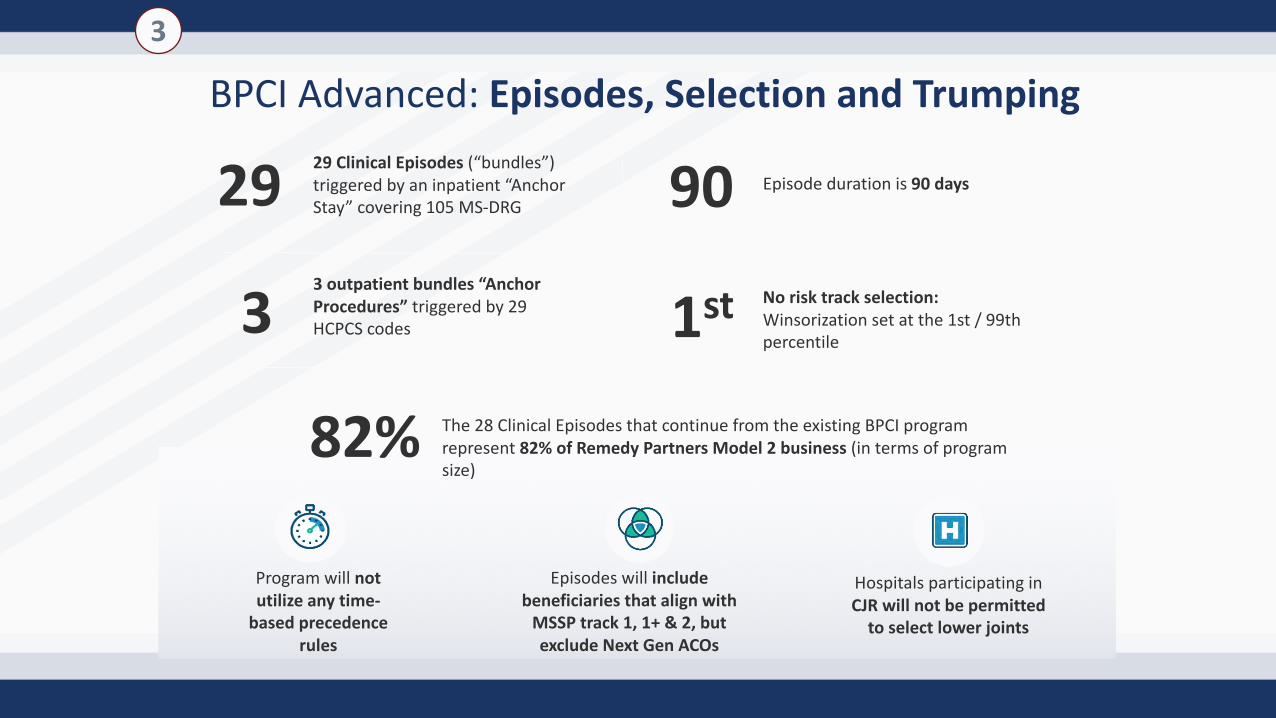
BPCI Advanced: Episodes, Selection and Trumping
29
3
82%
9029 Clinical Episodes (“bundles”) triggered by an inpatient “Anchor Stay” covering 105 MS-DRG
3 outpatient bundles “Anchor Procedures” triggered by 29 HCPCS codes
The 28 Clinical Episodes that continue from the existing BPCI program represent 82% of Remedy Partners Model 2 business (in terms of program size)
Episode duration is 90 days
1st No risk track selection: Winsorization set at the 1st / 99th percentile
Program will not utilize any time-
based precedence rules
Hospitals participating in CJR will not be permitted
to select lower joints
Episodes will include beneficiaries that align with
MSSP track 1, 1+ & 2, but exclude Next Gen ACOs
3

Bundles29 Inpatient Clinical Episodes 3 Outpatient Clinical EpisodesDisorders of the liver excluding malignancy, cirrhosis, alcoholic hepatitis - NEW Gastrointestinal obstruction Percutaneous coronary intervention (PCI)
Acute myocardial infarction Hip & femur procedures except major joint Cardiac defibrillator
Back & neck except spinal fusion Lower extremity/humerus procedure except hip, foot, femur Back & neck except spinal fusion
Cardiac arrhythmia Major bowel procedure
Cardiac defibrillator Major joint replacement of the lower extremity
Cardiac valve Major joint replacement of the upper extremity
Cellulitis Pacemaker
Cervical spinal fusion Percutaneous coronary intervention (PCI)
COPD, bronchitis, asthma Renal failure
Combined anterior posterior spinal fusion Sepsis
Congestive heart failure Simple pneumonia and respiratory infections
Coronary artery bypass graft Spinal fusion (non-cervical)
Double joint replacement of the lower extremity Stroke
Fractures of the femur and hip or pelvis Urinary tract infection
Gastrointestinal hemorrhage

BPCI Advanced: Reconciliation, Financial Arrangements & Pricing
8
Reconciliation• Semi-annual reconciliation• Payments can be reduced by 10%
based on adherence to quality measures• Quality data mined by CMS for first
two years, reporting requirements for participants begin in 2020
Financial Arrangements• 50% cap will apply to NPRA Sharing partners
(“gainsharers”)• NPRA sharing partners must participate in
activities specified by CMS
ØPricing based on four year historical period from 2013-2016.
ØThe price for each bundle will be set prior to the beginning of each performance year.
ØCMS will build in a 3% discount into the pricing model.
Ø The price will be specific to the facility participant or the facility in which the Participant treats patients.
Pricing
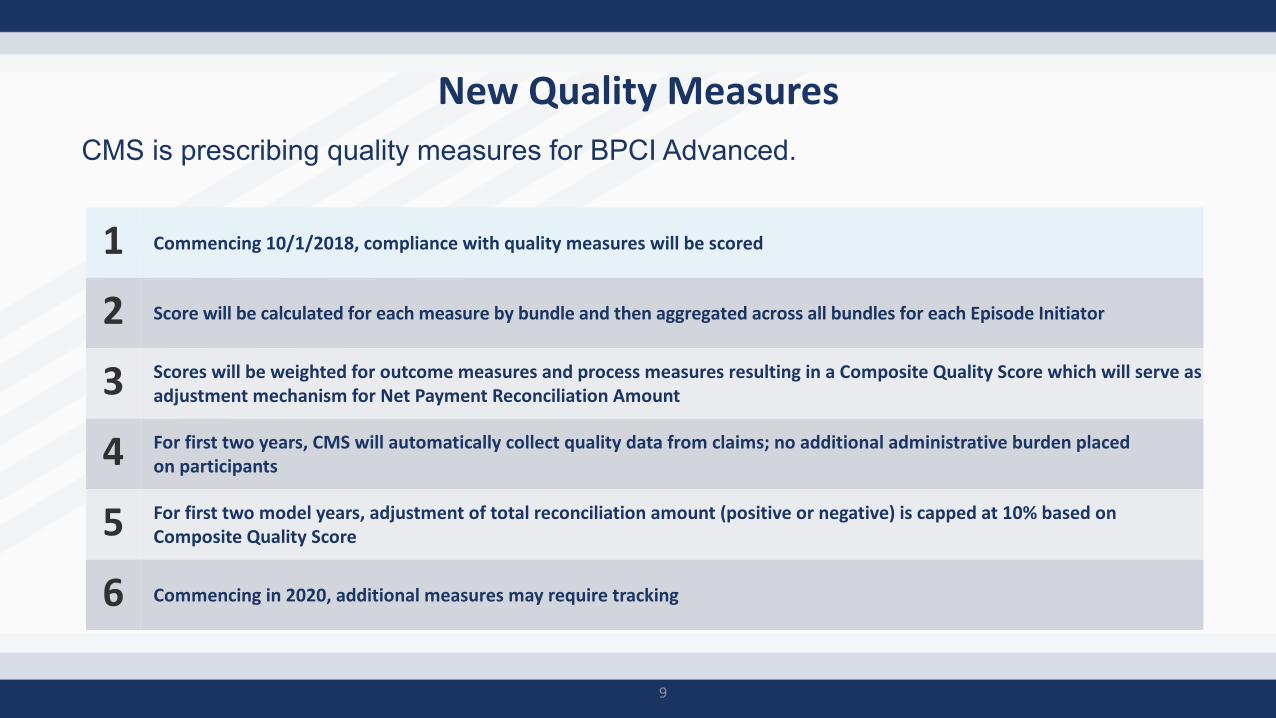
New Quality MeasuresCMS is prescribing quality measures for BPCI Advanced.
9
1 Commencing 10/1/2018, compliance with quality measures will be scored
2 Score will be calculated for each measure by bundle and then aggregated across all bundles for each Episode Initiator
3 Scores will be weighted for outcome measures and process measures resulting in a Composite Quality Score which will serve as adjustment mechanism for Net Payment Reconciliation Amount
4 For first two years, CMS will automatically collect quality data from claims; no additional administrative burden placed on participants
5 For first two model years, adjustment of total reconciliation amount (positive or negative) is capped at 10% based on Composite Quality Score
6 Commencing in 2020, additional measures may require tracking
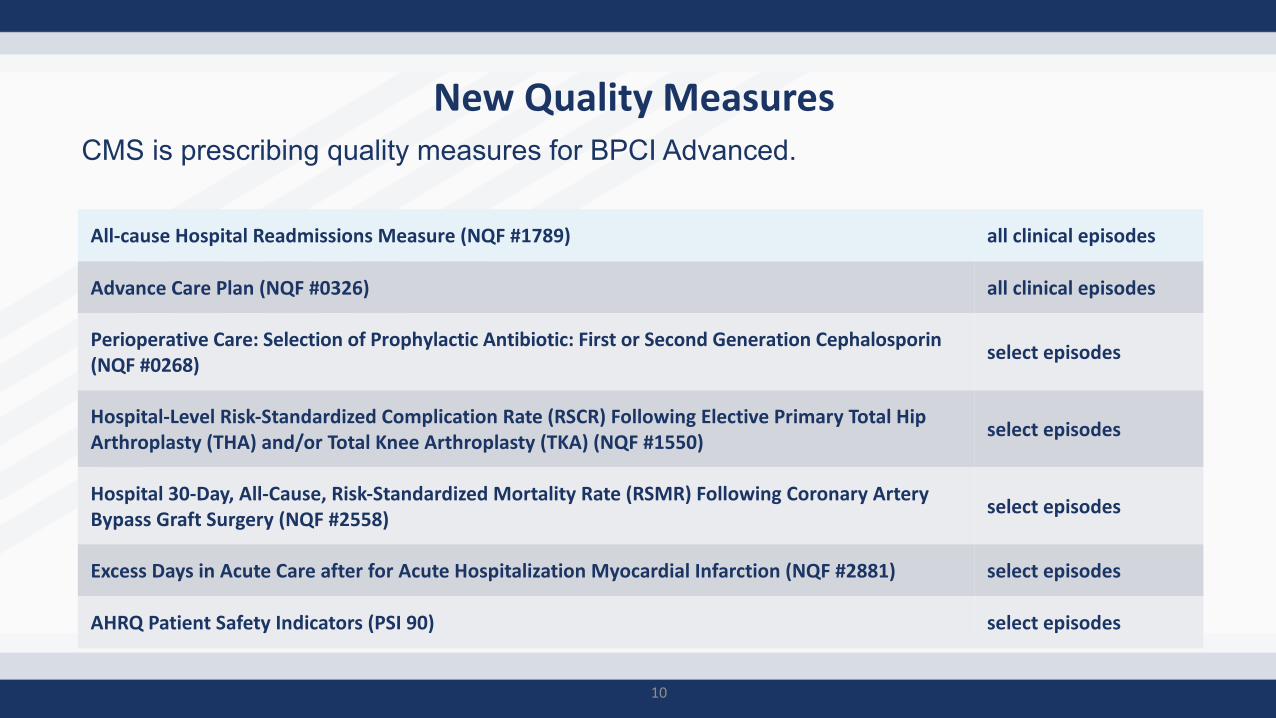
New Quality MeasuresCMS is prescribing quality measures for BPCI Advanced.
10
All-cause Hospital Readmissions Measure (NQF #1789) all clinical episodes
Advance Care Plan (NQF #0326) all clinical episodes
Perioperative Care: Selection of Prophylactic Antibiotic: First or Second Generation Cephalosporin (NQF #0268)
select episodes
Hospital-Level Risk-Standardized Complication Rate (RSCR) Following Elective Primary Total Hip Arthroplasty (THA) and/or Total Knee Arthroplasty (TKA) (NQF #1550)
select episodes
Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate (RSMR) Following Coronary Artery Bypass Graft Surgery (NQF #2558)
select episodes
Excess Days in Acute Care after for Acute Hospitalization Myocardial Infarction (NQF #2881) select episodes
AHRQ Patient Safety Indicators (PSI 90) select episodes

What is an Advanced Alternative Payment Model?Alternative payment model (APM): a payment approach that rewards providers for delivering high-quality and cost-efficient care.
Advanced APMs: a subset of APMs that let practices earn more rewards in exchange for taking on risk related to patient outcomes.
Exempt from MIPS penalties and quality reporting if meet volume thresholds
11
To Qualify, You Must:Use Certified EHR TechnologyBear > nominal risk (8% revenue)Base payment on quality measures comp. to MIPS
Examples of Advanced APMs:BPCI AdvancedMSSP Track 2 or 3 ACOCPC+OCM 2-sided riskComprehensive ESRDNextGen ACOCJR CEHRT Track
© 2018 Remedy Partners, Inc. All Rights Reserved.
What is a Qualifying APM Participant (QP)?
12
Must achieve threshold for Patients or Spending in an Advanced APM
Must exceed revenue or patient count thresholds
For 2019: 50% Medicare Part B payments or 35% Medicare Part B patients in AAPM
For 2023: 75% payments or 50% patients
© 2018 Remedy Partners, Inc. All Rights Reserved.
13
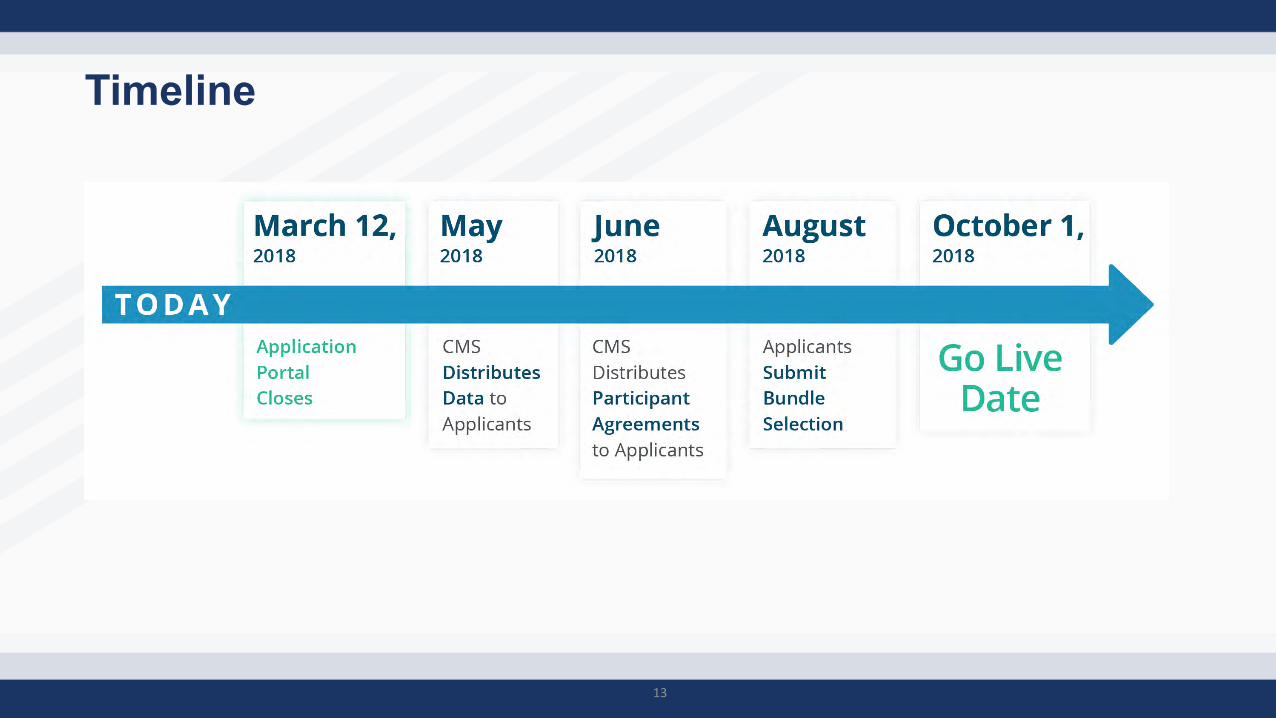
Timeline

BPCI Advanced: First Quality Payment Program Impact in 2019
14
Data Submission Deadlines
March 2020
Performance Period EndsDec 2019
QPP Performance Period
Jan 2019
Payment Adjustments
Jan 2021

Thank you!
Rodrigo Giacinti, MHA
Email: [email protected]
Phone: (573) 310-1485
www.remedypartners.com

BPCIRemedy’s Experience in Arizona
Rodrigo GiacintiMarket Manager, West Operations
Remedy Partners

Our History in Arizona
• Remedy Partners was founded in 2011 by Steve Wiggins. In 2013 our first partner goes live
• In 2015 Remedy becomes the Convener for one of the largest PGP company in the nation
• In 2017 Remedy’s Partner Services division begins the development/execution of the Post Acute Strategy in AZ

Arizona by the BPCI numbers• Our primary partner in AZ is a PGP with 5 Episode Initiators• 1,551 Episodes Initiated over the last year• 17 Bundles or 53 MS-DRG (2 ortho bundles)
AMI ATHEROSCLEROSIS CABG CELLULITIS
COPD DIABETES EGODD GI HEMM
GI OBSTRUCT HIP AND FEMUR E/MJ LEHP MPVD
RED BLOOD CELL DISORDERS RENAL FALURE SEPSIS SIMPLE PNEUMONIA
TRANSIENT ISCHEMIA

Key Lever Management• Post Acute Care Performance Management Networks
– SNF and HHA networks created for each site– Networks are intended for all patient population (not just BPCI)– Qualitative and Quantitative selection process (Bi-annual revision) using our analytic
shop and tools• Appropriate NSOC
– Select the appropriate setting with our CARL (Care at the Right Location) decision support mechanism
– Interdisciplinary approach• Readmission Reduction
– Leverage our Episode Connect technology to track VBC patients for the duration of the episode
– Partner with strong downstream providers to maximize patient care experience

Leverage Technology…. Episode Connect• Episode Connect connects administrators, nurses, physicians,
nurses, patients and families

Challenges
• Cooperation between stakeholders (Hospital, SNF, HHA, other)• Technology Adoption (Episode Connect) for
downstream providers• Downstream provider education and buy in on the BPCI
program• Homeless and Behavioral patients

Successes over the last year
• Increased Home Health Utilization from 4% (Adj Hist) to 13.7%
• Decreased readmission from 60.7% (Adj Hist) to 36%
• Decreased SNF LOS from 37 days (Adj Hist) to 25 days
• Created 5 High Quality SNF and HHA networks
• Developed great partnerships with Downstream providers
Adjusted Historic – Claims occurring between July 2009 and June 2012Current Period – Claims occurring between 2016Q4 and 2017Q3
Lessons to Share • As an awardee Convener, we are able to bring the combined
experience of 800+ providers nation wide and share best practices across all partners. Healthcare is local, and we must tailor the plan according to the market needs
• Partner Services is composed of hundreds of professionals that can use Big Data to generate next steps and insights.
• Program Design and Administration is key. Having a dependable back office that can take care of the program while you can focus on the #1 priority, the patient!
• BPCI is the beginning of payment reform. Payers, employers, and patients will soon follow


















