
Hosmac Pulse - Innovations in Healthcare Infrastructure
36
Copper connects life Pg. 5 Saving energy and lives Pg. 5 Vol. 1 December 2010 No. 4 Innovations in healthcare infrastructure
-
Upload
oneclickdrive -
Category
Documents
-
view
224 -
download
4
description
Hosmac Pulse - December 2010 issue
Transcript of Hosmac Pulse - Innovations in Healthcare Infrastructure
Copper connects lifePg. 5
Saving energy and livesPg. 5
Vol. 1 December 2010No. 4
Innovations in healthcare infrastructure

HOSMAC Pulse is an initiative of HOSMAC Foundation. High-quality standards have been maintained while preparing and presenting the information
in this periodical. However, no legal responsibility will be accepted by HOSMAC Foundation or HOSMAC India Pvt Ltd for any loss or damage resultant
from its contents. The views expressed are solely that of the authors or writers, and do not necessarily represent the views of HOSMAC Foundation
or its consultants in relation to any particular projects. No part of this periodical may be reproduced in any form without the written permission of
HOSMAC Fooundation — the publisher.
Sustainable healthcare design in the Middle East 3
Copper connects life 5
Saving energy and more lives
A pipe dream made real 15
More with less 17
Penetrating radiation 7
11
Pathway to glory 19
Engaging expertise externally 21
Distilling costs alike 23
Be a radiologist! 25
Healthcare made affordable 27
Money matters 31
Editorial Board Table Of Content
Advisory Panel
Creative Consultant
Chief Editor
Printed by
Narendra Karkera
Isha Khanolkar
Smita Sridharan
Kaustubh Sardesai
Amit Pandya
Vinay Pagarani
Kothari Printers, Bangalore

Indian healthcare is on an ascent, and the healthcare infrastructure across the country is on the upswing. India
currently holds 0.9 beds per thousand populations as against the recommended WHO standard of 3 beds per thousand
populations. To bridge the gap would mean adding a whopping 80,000 beds every year for the next 10 years.
Hospital buildings need a large capex for both building engineering and medical equipment. Public-private
partnerships will be a key to growth of healthcare services and that would mean — one would have to network hospitals
across the country and develop a referral chain mechanism. This will mean intelligent use of information technology
and tele-communication systems leading to larger role for telemedicine based clinical services.
Considering 24x7 operations of hospitals and the fact that most future hospitals will be centrally air-conditioned, there
is a dire need to adopt building automation systems and other engineering solutions like high performance glass, gas
based air-conditioning systems, solar energy, heat recovery systems, sewage treatment plants etc. to make hospitals
more green and energy efficient.
Proper use of information technology can also help us reduce paper usage, and data can be shared across the hospital.
Access control systems, CCTV networks, and advanced fire fighting systems are also becoming essential in hospitals,
especially after the terror strike in Mumbai. Pneumatic tube systems which carry blood samples and other small items
help reduce manpower traffic to deliver the samples.
Thanks to the galloping growth of health costs and demand, even if the Indian government doubles spending on health
to around 2% of GDP till 2020, it may not maintain the current 1:4 ratio of public to private spending on health. The
government, corporates, private doctors, NGOs and think-tanks must help create a common vision of affordable,
accessible healthcare for all and devise a broad framework to achieve global standards with a local touch.
Executive's note
Dr. Vivek DesaiManaging Director, Hosmac India Pvt. Ltd.
There is a dire need to adopt building automation systems and
other engineering solutions like high performance glass, gas based
air-conditioning systems, solar energy, heat recovery systems,
sewage treatment plants etc. to make hospitals more green and
energy efficient.


Sustainable healthcare design in the Middle East
Erik Hokanson, Leed Healthcare Designer — Burt Hill, gives a rundown of the integrated planning and designing
phase of the Al Mafraq Hospital, UAE.
A state-of-the-art healthcare facility that promotessustainability and wellness as an integral part of the healingenvironment is ideal — such as theAl Mafraq Hospital, UAE.
Located in the central region of Abu Dhabi, the newly designedhospital is carefully situated on a prominent site directlyadjacent to the existing Al Mafraq Hospital. The site offers anopportunity to express the client's desire to have visible andtimeless architectural presence set in the midst of theAl Mafraqcommunity. The new hospital complex boasts a strikingcontemporary architecture defined by four distinctive patienttowers and a glass enclosed podium representing ultramodernmedical facilities.
The 272,000 square meter 750-bed replacement hospital andoutpatient clinic will offer an enhanced and comprehensivepatient care program extending excellent urgent care andgeneral medical services. Patients and visitors to the hospitalwill be greeted with a welcoming approach and invited into thenaturally lit lobby concourse which offers hotel-like loungingspaces, beside a private and dignified patient reception area.Wayfinding is incorporated into the design fabric of the buildingthrough elegant sculptural elements and water features thatorient visitors to the patient towers' elevator lobbies. Easyaccess to the outpatient clinic is offered from the main hospitallobby through an enclosed pedestrian bridge.
Located to support the privacy and comfort of women andchildren, a pavilion with a separate entrance was intrinsicallyplanned. A separate tower dedicated for specialist service tomothers and children was also instituted.
Each patient tower will contain no more than 30 single roomsper floor, with each floor having functional nursing stations andpatient control centres. Spacious corridors will lead to privateand appropriately sized rooms designed for the comfort of thepatient and visitors. All rooms will have large windows and
ample natural light. Special VIP floors will provide dignifiedsuites for patients and families requiring special privacy andattention.
The new hospital facility will provide urgent care services withan expanded emergency department and critical care services.Flexibility is the key component of the facility, allowing forexpansion of departments with minimum disruption. In additionto rooftop gardens and the latest energy conservation devices,the entire facility will provide enhanced patient environmentsand longterm efficiency. The entire medical center complex isdesigned for sustainability and maximum energy savings.
Most of the healthcare design programs in the Middle East areled by American standards as they are recognized — the best inthe world. It is important so designers can define the spaces andproper environments within a facility, and coordinate with thehealthcare staff to best meet their working needs. The aim is toadapt to the culture in this part of the world while integratinginnovation and improved practices from other parts of theworld.
Family-centred care has been a tradition of the region forcenturies and the design of Al Mafraq allows this tradition tocontinue in a new international setting. The planning and designof healthcare projects in the Middle East must recognize theneed to provide appropriate and dignified spaces for thepurpose of prayers by both the patient and staff. Further, theseparation of males and females must be considered in allaspects of the design including waiting areas, hospital wardsand recovery rooms. It is common for large families toaccompany patients, which has a direct impact on the kinds ofspaces and furniture to be considered in the waiting areas.
The patient room, which is the heart of any healthcare
Culture
3

institution, needs to be generous in size and to allowappropriate caregiver zones unobstructed by the family zones.The patient room design must recognize numerous users of theroom: family, medical staff, and not the least the patient.Architects and medical planners need to consider thesecultural requirements in the early stages of programming andconceptual design.
Al Mafraq Hospital has been designed utilizing sustainableguidelines established in the Estidama and the Pearl RatingSystem. This system as part of the Abu Dhabi 2030 plan is achecklist of sustainable requirements similar to the Leed ratingsystem. The design process has been a collaborative effortbetween architects, engineers, the client and Abu Dhabistakeholders.
Weekly scheduled integrated workshops resulted inestablishing key sustainable strategies. These include buildingorientation, storm water management, water conservation,reduction of annual energy consumption and high-qualityindoor air environment to name a few. The building alsoincorporates sustainable materials and will be sited in alandscape with a substantial component of indigenous desertplantings.
The project has been designed in parallel with the Al Mafraqcommunity master plan and will incorporate publictransportation and other amenities to hospital visitors andemployees via future connectivity to the new capital district ofAbu Dhabi.
The master plan design successfully integrates new urbanistprinciples, and carefully considers the placement of thehospital, while accommodating complex patterns of circulationnecessary for the facility. Moreover, the plan's land use programincludes space for a variety of related medical programs. Themaster plan provides appropriate facilities and pathways tothose staff and employees who wish to ride their bicycles towork to reduce the single-occupancy vehicle traffic to thebuilding.
Extreme temperatures exceeding 50 degrees centigrade insummer months result in challenges when designing efficientmechanical cooling systems. Smart decisions can be made earlyin the design process by understanding a site's prevalentenvironmental attributes as well as utilization of energymodeling. For the hospital, energy modeling assisted indetermining the ideal building orientation, the appropriatebuilding envelope, sun-screening strategy and engineering forefficient MEP systems.
In parallel with the energy modeling, life cycle cost analysiswas performed during the design process to evaluate go-no-gowith systems vis-à-vis the client. The hospital incorporatesmany energy savings items including roof mounted solar panels,which provide 75% of the total power requirement for heatinghot water.
Mechanical cooling systems for the project to utilize a flexibleand zoned VAV system where appropriate (90% of building HVACsystem) to reduce volume of air supply and fan energy. Further,a heat pipe system for infection control was designed toseparate supply and exhaust air streams, which results in 50%energy recovery of exhaust air stream.
Computational Fluid Dynamic (CFD) modeling was utilized inthe design process for studying appropriate air flow in burnsunit and operating theatres, envelope wind pressure, andsmoke management systems.
Evidence based design was utilized during the design process asa means to measure the impact of all design and materialsolutions. Every element, from the use of anti-microbial paintto bathroom placement related to slip and fall injuries wasstudied and analyzed to best arrive at the optimal solution.
The use of rapidly renewable and sustainable materialsincluding certified wood products for casework and wood wallpaneling, linoleum flooring for corridors, patient rooms andcarpet tiles in administrative areas are used throughout theproject. Paint systems, sealants and adhesives have beenspecified to reduce or eliminate volatile organic compoundemissions in occupied spaces .
The site and landscape strategy for the project incorporates asustainable planting and design approach through createdwadi-scapes which have both ecological and economicaladvantages. Existing wetlands on site have been retained andnew ones created with native marsh grasses. These wadilandforms collect and deliver seasonal drainage water to
locations where it can filter back into the water table.
The wadi-scape and preserved wetland areas also help tosupport and nourish natural habitat for local wildlife to live.The extensive planting areas which will have significant areasof sand and wadi gravel help to reduce the overall heat islandeffect. They also reduce the overall water demand whileproviding an indigenous landscape for the project.
The planting layout and species selection has been designed intandem with the irrigation system to maximize the availablewater resource by using technologies such as flow and weathersensors, soil moisture sensors, soil additive to increase waterretention in the soil and drip irrigation to ensure maximumwater efficiency.
Over 350 cubic meters of treated sewage effluent (TSE) andgrey water, which is separated from sewage produced dailyfrom the hospital, will be used to irrigate the landscape andprovide all of the required water needs. No potable water isused for irrigation. The site landscape strategy alsoincorporates the planting of many existing mature native,exotic trees and date palms which will be relocated from theexisting hospital site.
The new medical center reflects the future of healthcare. Theintegration of outpatient and inpatient services provides thehighest level of care and achieves economies of operations. AlMafraq Hospital will offer a new experience to medical staffand patients, as it will set the standard for sustainable modernhealing environments in the Middle East.
Sustainable strategies
Energy
Products and materials
Landscape and water usage
, where possible
The author has led the design and management of severalaward winning healthcare, corporate and higher educationprojects in the Middle East and United States. He can becontacted at [email protected]
4
Time for a new approach
Antimicrobial Copper
EPAregistration
Historic evidence
In the 1850s, some 50 years before scientists discoveredmicrobes, Florence Nightingale — a pioneer of modern nursing,discovered that her patients recovered much better when thehospital environment was kept clean. She instituted a laundryservice, rigorously cleaned all medical and hospital equipment,and had the floors scrubbed for the first time. The results wereunbelievable: the death rate of patients suffering from cholera,typhus and dysentery came down from 42% to a mere 2%.
More than 150 years later, however, despite enormous advancesin the field of microbiology and infection control, hospital-acquired infections still continue to plague the patients andhospitals at alarming levels.
Scientific research and historic facts confirm that copper andits alloys, brass and bronze, are naturally antimicrobialmaterials. They work as dinfectants restraining the growth ofharmful bacteria, which has also been recognized by the U.S.Environmental ProtectionAgency (EPA).
275 copper alloys, including brass and bronze, have beenregistered with the EPA as antimicrobial materials that killbacteria. The registration acknowledges claims that copper,brass and bronze are capable of killing harmful, potentiallydeadly bacteria. Copper is the first solid surface material to
receive this type of EPA registration, which is supported byextensive antimicrobial efficacy testing.
The laboratory research performed under EPA-approvedprotocols demonstrated that copper alloy surfaces kill morethan 99.9% of several bacteria known to be human pathogenswithin two hours. The organisms tested were:
• StaphylococcusAureus
• EnterobacterAerogenes
• Escherichia Coli O157:H7
• PseudomonasAeruginosa and
• Methicillin-resistant StaphylococcusAureus (MRSA)
MRSA is one of the most virulent strains of antibiotic-resistantbacteria and a common cause of hospital-acquired infections.
Before anyone recognized that microorganisms existed, theEgyptians, Greeks, Romans and Aztecs used copper compoundsfor good hygiene and to treat disease. Egyptians used copper tosterilize drinking water and wounds. Hippocrates treated openwounds and skin irritations with copper. The Romans cataloguednumerous medicinal uses of copper for various diseases. TheAztecs treated sore throats with copper, while people in Persiaand India applied copper to treat boils, eye infections andvenereal ulcers.
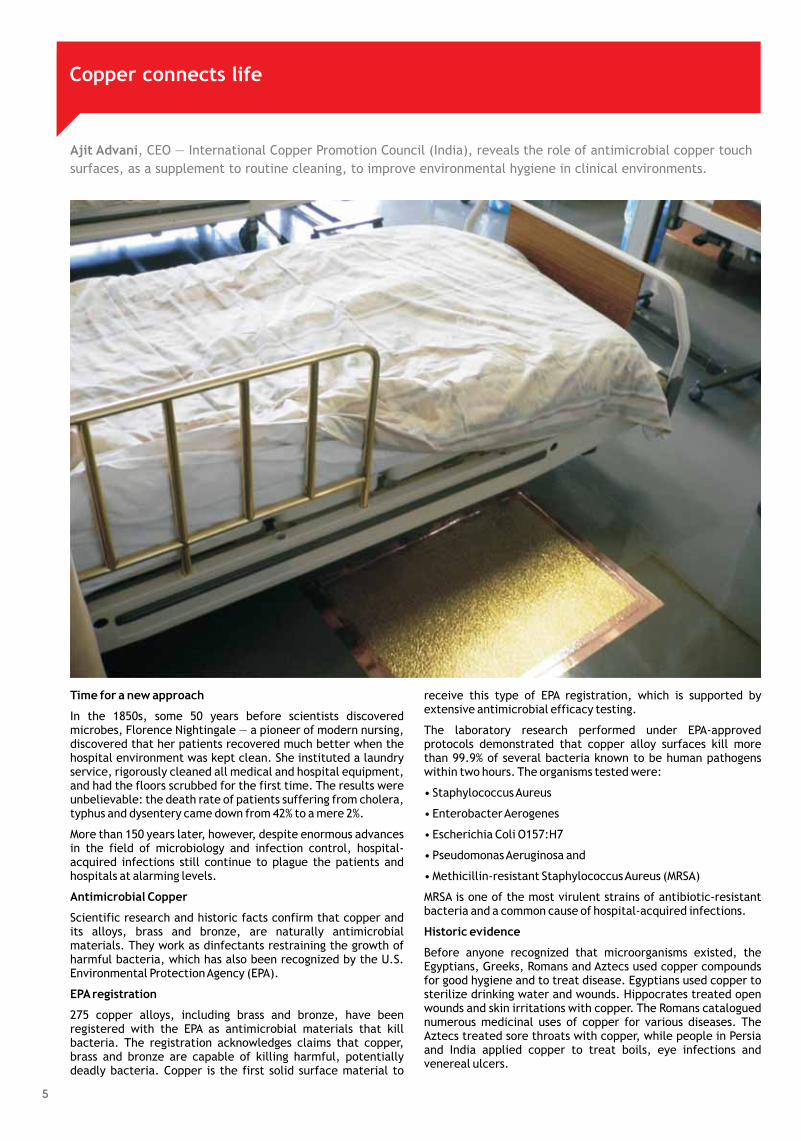
Ajit Advani, CEO — International Copper Promotion Council (India), reveals the role of antimicrobial copper touch
surfaces, as a supplement to routine cleaning, to improve environmental hygiene in clinical environments.
Copper connects life
5
Touch surfaces: Source of infections
Copper touch surfaces
Conclusion
In healthcare facilities, surfaces in proximity to patients are ofthe most concern. 80% of infectious diseases are spread bytouch. A hand contaminated with the influenza ‘A’ virus willcontaminate the next seven surfaces that are touched.
Not all hospital-acquired infections are preventable. However,in the UK, infection control teams recognize that a 15%reduction could be achieved through a series of infectioncontrol measures, including improved hygiene. This could alsolead to savings of approximately 150 million pounds a year.
Many of the commonly used materials in healthcare facilitiessuch as stainless steel have proven to have comparatively littleor no adverse effect on harmful bacteria.
Replacing frequently touched surfaces with copper or high-copper alloys such as brass and bronze, which are naturallyantimicrobial, can be an effective infection control measure.Such a measure can complement other infection controlpractices such as frequent hand washing, patient screening andisolation, and improved cleaning.
Frequently touched surfaces in hospitals that can be madefrom copper or copper alloys include:
Door handles
Push plates
Light switches
Bed rails
Grab rails
Intravenous (IV) stands
Dressing trolleys
Dispensers (alcohol gel, paper towel, soap)
Faucets
Sinks
Counter and table tops
These touch surfaces are all potential reservoirs of harmfulmicrobes. Reducing the number of live germs on these surfacescan possibly control the spread of MRSA and other sources ofhospital-acquired infections.
The use of copper alloys for frequently touched surfaces as asupplement to existing standard infection preventionmeasures, such as hand-washing and disinfection regimens,have far-reaching implications. Potential applications with thefrquently touched surfaces in hospitals can help reduce thepresence of disease-causing bacteria in hospitals.
•
•
•
•
•
•
•
•
•
•
•
The International Copper Promotion Council India (ICPCI) isthe Indian centre of the International Copper AssociationLimited that promotes the beneficial usage of copper forsafety, health, environment and energy savings by guidingpolicies, strategies and funding of international initiativesand promotional activities. To know more, please visit
and .www.copperindia.org www.antimicrobialcopper.com
6
Given the large capital expenditures required to run radiologydepartments, it is surprising to note that more effort andthought have not gone into figuring out how to run these moreefficiently in our country. It is best to start by differentiatingbetween standalone and hospital based centres.
Their main aim is to provide exceptional service to existingclinical facilities. They have to be well-equipped with state-of-the-equipment within reason and above average radiologists,capable of working in sync with clinical colleagues.
Agood radiology department functions as an integral part of thehospital, providing a “value add” that goes beyond the profitand loss account (P & L), by empowering the physician orsurgeon to improve clinical deliverables and thus increasepatient flow to the hospital. It stands to reason therefore that ahospital radiology department should have all the modalities tobegin with, and not follow the step-wise, graded growth thatmany mid-sized hospitals do.
Outsourcing of radiology departments to private entities whoseonly focus will be the P & L is also an extremely debatable issue,not just for private hospitals but also for government ones.
Their primary objective is to provide service while also making aprofit for the promoters.
The aims of the two groups are therefore completely differentand while they share some commonalities; they also presentdifferent challenges. Where not mentioned below, the issuesdiscussed will be common to both types of setup.
a. Procurement
b. Capital expenditure (Capex) management
c. Information technology (IT)
d. Tracking a good monthly income statement (MIS)
e. Sales and marketing
f. Referrals and revenue sharing
g. Material cost control
h. Human resources (HR) challenges
i. Managing repairs and annual maintenance contracts (AMCs)and comprehensive maintenance contracts (CMCs)
Hospital based
Standalone and outsourced hospital based departments
Issues
Dr. Bhavin Jankharia, Director — Radiology Services — Piramal Diagnostics, suggests how operational efficiencies
in radiology management systems can be effectuated.
Penetrating radiation
Dr. Narottam Puri (centre) with Dr. Abdul Kalam Azad (left)
7

j. Regulatory compliance
k. Quality monitoring and audits
The choice of machine in more ways than one impacts futureoperations. If the machine is not up to the mark, it will not dowell and this will impact the top line. If it is too expensive,while sales may be good, the return on investment (ROI) andprofit before tax (PBT) will be affected. In both situations,eventually there will be a tendency to cut corners. Hence, it isimperative that the pre-purchase technical and financialanalyses be perfect.
i. It is best to go with one single vendor to get a great “package”deal.
ii.Aradiologist is not required in the decision-making process.
During procurement, some issues that are often left out andimpact future operational efficiencies include:
i. Laser printers
ii. Workstations
iii. Pressure injectors
iv. Training for radiologists and technologists
v. Proper understanding of CMCs/AMCs and warranties
vi. Optional packages
Among other issues, the way CMCs are handled can affectoperations. If a CMC is capitalized at the time of purchase, itwill enhance the P & L and PBT, but reduce the ROI. Moreimportantly, there is a sales tax savings of 12.4% per year at thispoint in time that directly goes to the bottom line.
i. Radiology Information Systems (RIS)
These should capture patient information, provide proper
billing facilities, allow recovery of outstandings, integrate withthe inventory so that material usage can be captured and bepart of a CRM system that allows patient tracking, especiallyfor screening tests (mammography and bone density) andrepeat studies such as for multiple sclerosis, oncology, etc.
ii. Workstations and advanced processing
An understanding of workstation needs can reduce capital andoperational costs without compromising on quality. Forinstance, using Osirix based IMAC workstations instead ofvendor-based products.
iii. PACS and teleradiology
These should allow image transfer to all locations within theradiology departments, outside the department within allrelevant hospital facilities and to a central server forteleradiology and similar applications, depending on need.
Robust IT systems allow all revenues and expenses to betracked meticulously, thus helping track costs. There should bea strong focus on tracking gross sales, net sales (gross sales -patient discounts) and all other expenses as percentages of netsales. This will give an estimate of EBITDA before corporate orcentral allocations and then net profit as well.
For standalone centres, each modality should be treated as aseparate profit-centre to understand what works and whatdoesn't.
This can be done with the help of various methods:
i. Brochures and pamphlets
ii. Newsletters
iii. Loyalty cards and a robust CRM
iv. Sales and marketing personnel
v. Advertising
vi. GoogleAdWords
A. Procurement
Myths
B. Capex Management
C. IT Systems
D. Tracking a good MIS
E. Sales and marketing
8
vii. Generation of publicity
Depending on the circumstances, all or some of these may help.A robust team can add value by enhancing patient throughput.Ultimately though, it must be understood that the radiologistand his/her report are the cornerstone of a good radiologydepartment/centre, interaction with patients and referring
doctors on a daily, ongoing basis is the best marketing tool. Theuse of short messaging service (SMS) and emails helps reportsget out faster, allowing more robust communication and betterefficiency.
While the ethics of this can be debated endlessly, it is a reality.To maintain a reasonable ROI and PBT, it is necessary to restrictreferrals and revenue sharing to less than 20% of net sales. In ahospital department, this should be 0%. It is up to the hospitaladministration to crack the whip and ensure that no radiologywork leaves the hospital premises, whether it be OPD or in-door.
If work has to go out due to non-availability of certain machinesand modalities, then it should only be to those centres ordepartments that are accredited by the hospital. All suchappointments should be routed through the hospital's radiologydepartment to ensure quality and accountability.
Material cost tracking and control should be obsessive. Forexample, in a full-service department, exclusive of a PET/CT(positron emission tomography/computed tomography), thematerial cost inclusive of stationery, CDs, films and contrastshould not exceed 12% of net sales.
A part of this involves auditing waste. In the pre-digital era,film wastage as a result of improper technique was quitesignificant. In the digital era, this has been virtuallyeliminated.
These involve recruitment, retention, training andcompensation. Good HR strategies go a long way in maintainingan efficient department/centre.
i. Training
This involves front-desk training, behavioral training for therest of the staff as well as technical training. Just ensuring thateveryone is properly attired can make a big difference.
ii. Retention
This is important. Though the adage “no one is indispensable”is an oft-quoted “corporate mantra”, it is just not true. Goodhuman assets, from ward-boys to radiologists, make asignificant difference. Figuring out ways to motivate and retainkey talent is a must.
iii. Recruitment
This is obvious. Good people make all the difference.
iv. Compensation
This should follow reasonable standards such as the totalcompensation of the entire radiology team should not exceed18% of net sales, assuming a reasonable flow of patients. Similarstandards exist for the rest of the staff. Compensation shouldinclude performance and statutory incentives to motivate staffacross all levels.
These can be significant costs (up to 20% of net sales) and shouldbe adequately managed. CMCs are the best option for busycentres, since the onus of uptime delivery is entirely on thevendor company.
These are a must, both from the perspective of following the“law of the land” and for obtaining accreditations such as NABHfor radiology. These include:
i. Shop and establishment licenses
ii. Atomic Energy Regulatory Board (AERB) clearance for all x-ray based and radiation based equipment
iii. PC-PNDT (Pre-conception and prenatal sex determinationact) compliance, which is both a one-time and an ongoingprocess, for all USG machines
There should be an in-house, automatic method of tracking thequality of reports, the turnaround time for reports, theavailability of emergency services and the quality of emergencyand teleradiology based reports, etc.
There are many ways to do this. Example, one parameter thatcan be tracked is turnaround time (TAT), which can vary from 30minutes in emergency situations to 24 hours for non-emergencycases. One method of speeding up TAT is to use automatedtranscription software, such as ‘Dragon Naturally Speaking’from that allows instantaneous transcription on thecomputer.
Having a multi-functional facility manager to oversee eachfacet of the centre/department in conjunction with otherfunctional heads (biomedical, finance, supply chain) makes asignificant difference and allows radiologists and technologiststo focus on their clinical work, without having to worry aboutother day-to-day administrative issues. This facility managermay be a receptionist with extensive experience, a nurse or atechnologist, who is willing to shoulder additional responsibilityand is given adequate gap training.
F. Referrals and revenue sharing
G. Material Control
H. HR Challenges
I. Repairs, CMCs andAMCs
J. Regulatory Compliance
H. Quality audits and compliance
Final words
Nuance
The author is also the Editor-in-Chief of the ‘Indian Journal ofRadiology and Imaging’. He can be contacted at
.
As shown above, a radiology department, whether standaloneor within a hospital, is a complex animal that needs a significantamount of attention if it has to be run efficiently.
9
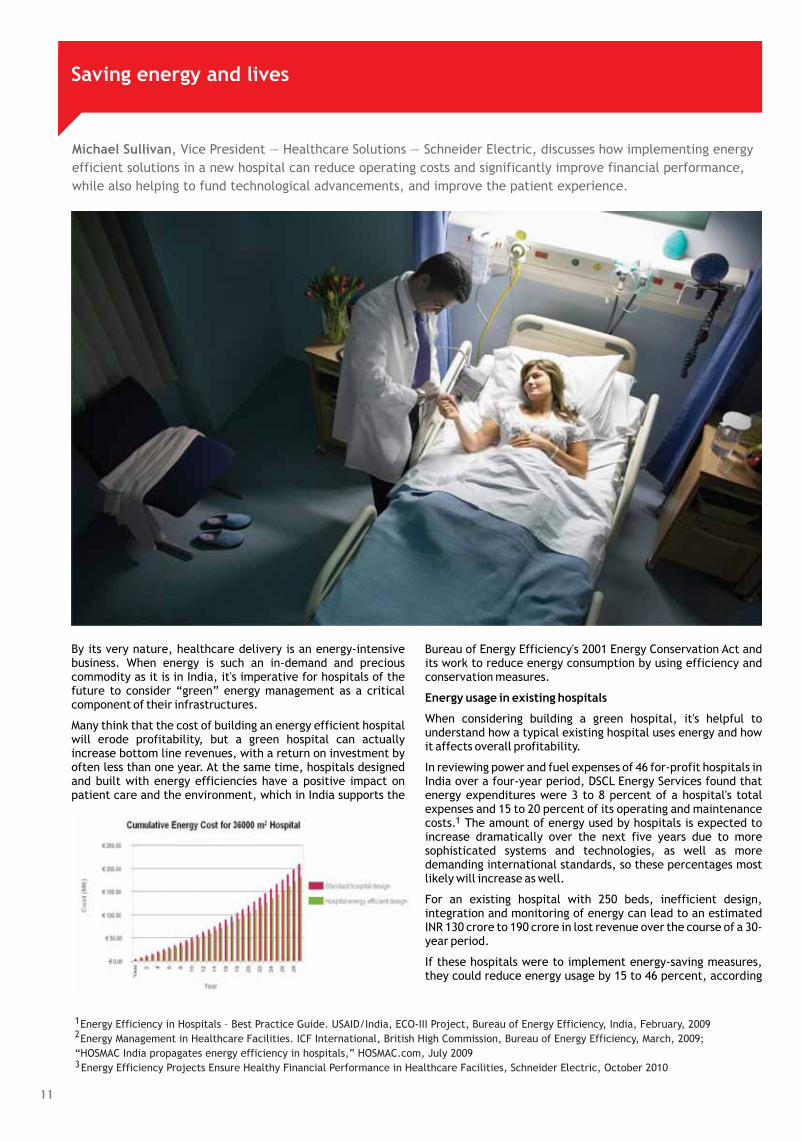
Michael Sullivan, Vice President — Healthcare Solutions — Schneider Electric, discusses how implementing energy
efficient solutions in a new hospital can reduce operating costs and significantly improve financial performance,
while also helping to fund technological advancements, and improve the patient experience.
11
Saving energy and lives
By its very nature, healthcare delivery is an energy-intensivebusiness. When energy is such an in-demand and preciouscommodity as it is in India, it's imperative for hospitals of thefuture to consider “green” energy management as a criticalcomponent of their infrastructures.
Many think that the cost of building an energy efficient hospitalwill erode profitability, but a green hospital can actuallyincrease bottom line revenues, with a return on investment byoften less than one year. At the same time, hospitals designedand built with energy efficiencies have a positive impact onpatient care and the environment, which in India supports the
Bureau of Energy Efficiency's 2001 Energy Conservation Act andits work to reduce energy consumption by using efficiency andconservation measures.
When considering building a green hospital, it's helpful tounderstand how a typical existing hospital uses energy and howit affects overall profitability.
In reviewing power and fuel expenses of 46 for-profit hospitals inIndia over a four-year period, DSCL Energy Services found thatenergy expenditures were 3 to 8 percent of a hospital's totalexpenses and 15 to 20 percent of its operating and maintenancecosts. The amount of energy used by hospitals is expected toincrease dramatically over the next five years due to moresophisticated systems and technologies, as well as moredemanding international standards, so these percentages mostlikely will increase as well.
For an existing hospital with 250 beds, inefficient design,integration and monitoring of energy can lead to an estimatedINR 130 crore to 190 crore in lost revenue over the course of a 30-year period.
If these hospitals were to implement energy-saving measures,they could reduce energy usage by 15 to 46 percent, according
Energy usage in existing hospitals
1
1
2
3
Energy Efficiency in Hospitals – Best Practice Guide. USAID/India, ECO-III Project, Bureau of Energy Efficiency, India, February, 2009
Energy Management in Healthcare Facilities. ICF International, British High Commission, Bureau of Energy Efficiency, March, 2009;
“HOSMAC India propagates energy efficiency in hospitals,” HOSMAC.com, July 2009
Energy Efficiency Projects Ensure Healthy Financial Performance in Healthcare Facilities, Schneider Electric, October 2010
to energy audits by India's Bureau of Energy Efficiency andHOSMAC research.
A 30-percent savings in energy costs has the potential toimprove profitability by up to 1 percent, with savings of nearlyINR 6.4 crore.
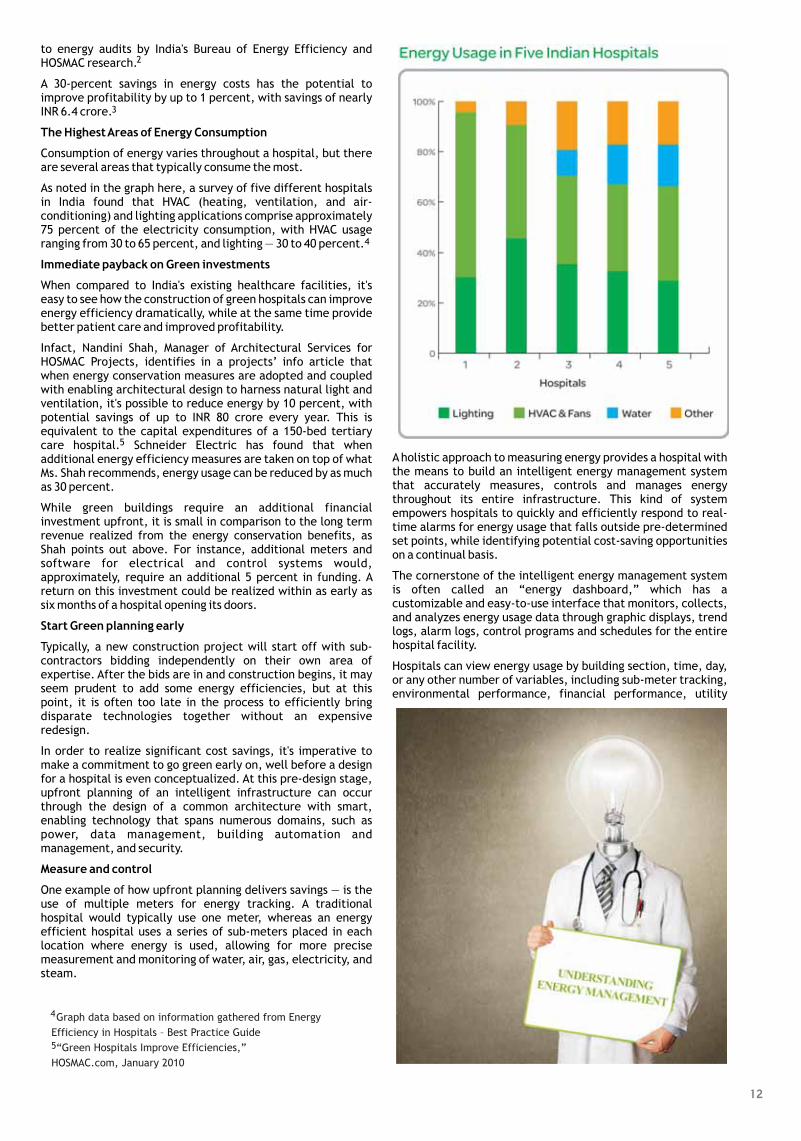
Consumption of energy varies throughout a hospital, but thereare several areas that typically consume the most.
As noted in the graph here, a survey of five different hospitalsin India found that HVAC (heating, ventilation, and air-conditioning) and lighting applications comprise approximately75 percent of the electricity consumption, with HVAC usageranging from 30 to 65 percent, and lighting — 30 to 40 percent.
When compared to India's existing healthcare facilities, it'seasy to see how the construction of green hospitals can improveenergy efficiency dramatically, while at the same time providebetter patient care and improved profitability.
Infact, Nandini Shah, Manager of Architectural Services forHOSMAC Projects, identifies in a projects’ info article thatwhen energy conservation measures are adopted and coupledwith enabling architectural design to harness natural light andventilation, it's possible to reduce energy by 10 percent, withpotential savings of up to INR 80 crore every year. This isequivalent to the capital expenditures of a 150-bed tertiarycare hospital. Schneider Electric has found that whenadditional energy efficiency measures are taken on top of whatMs. Shah recommends, energy usage can be reduced by as muchas 30 percent.
While green buildings require an additional financialinvestment upfront, it is small in comparison to the long termrevenue realized from the energy conservation benefits, asShah points out above. For instance, additional meters andsoftware for electrical and control systems would,approximately, require an additional 5 percent in funding. Areturn on this investment could be realized within as early assix months of a hospital opening its doors.
Typically, a new construction project will start off with sub-contractors bidding independently on their own area ofexpertise. After the bids are in and construction begins, it mayseem prudent to add some energy efficiencies, but at thispoint, it is often too late in the process to efficiently bringdisparate technologies together without an expensiveredesign.
In order to realize significant cost savings, it's imperative tomake a commitment to go green early on, well before a designfor a hospital is even conceptualized. At this pre-design stage,upfront planning of an intelligent infrastructure can occurthrough the design of a common architecture with smart,enabling technology that spans numerous domains, such aspower, data management, building automation andmanagement, and security.
One example of how upfront planning delivers savings — is theuse of multiple meters for energy tracking. A traditionalhospital would typically use one meter, whereas an energyefficient hospital uses a series of sub-meters placed in eachlocation where energy is used, allowing for more precisemeasurement and monitoring of water, air, gas, electricity, andsteam.
Aholistic approach to measuring energy provides a hospital withthe means to build an intelligent energy management systemthat accurately measures, controls and manages energythroughout its entire infrastructure. This kind of systemempowers hospitals to quickly and efficiently respond to real-time alarms for energy usage that falls outside pre-determinedset points, while identifying potential cost-saving opportunitieson a continual basis.
The cornerstone of the intelligent energy management systemis often called an “energy dashboard,” which has acustomizable and easy-to-use interface that monitors, collects,and analyzes energy usage data through graphic displays, trendlogs, alarm logs, control programs and schedules for the entirehospital facility.
Hospitals can view energy usage by building section, time, day,or any other number of variables, including sub-meter tracking,environmental performance, financial performance, utility
2
3
4
5
The HighestAreas of Energy Consumption
Immediate payback on Green investments
Start Green planning early
Measure and control
Graph data based on information gathered from Energy
Efficiency in Hospitals – Best Practice Guide
“Green Hospitals Improve Efficiencies,”
HOSMAC.com, January 2010
4
5
12

performance, maintenance scheduling and asset optimization.
Intelligent decisions can be made as to how to improve energyefficiency on a real-time, ongoing basis. In addition, built-inalgorithms identify potential areas of waste and present energysavings opportunities, allowing for quick alterations of usage,with results that are low-risk to patient care, while creating thegreatest financial return on the hospital's investment.
Energy efficiency solutions provide hospitals with built-incontrols to help them regulate the highest areas of energy use,such as HVAC and lighting.
For instance, hospitals pay usage charges for electricity, as wellas a demand fee on top of that, which is established by peaklevels of energy usage. A maximum demand report generatedfrom an energy dashboard identifies the peak periods, allowingfor adjustments that can reduce the demand fees and generatesignificant savings over time.
Other opportunities for energy efficiency that can beconsidered include:
Advanced and integrated control techniques that regulate allbuilding systems can help a hospital save 5 to 20 percentannually on HVAC and lighting costs.
By installing variable speed drives for air-conditioning pumpsand fans, a hospital can reduce motor speeds and optimize fanand pump runtime. A 20-percent motor speed reduction coulddeliver a 50 percent energy savings.
Integrated lighting control systems with low-consumptionlighting can offer up to a 30-percent savings on energy.
Energy efficiency measures for operating theatre can reducethe air change rate based on operating theatre occupancy, withpotential for as much as 25 percent savings.
In a hospital datacenter, in-row cooling devices for serverscould save 30 percent on energy.
The savings noted above are based on measures taken byexisting hospitals. When these steps are integrated early intothe design of a new hospital, the savings potential is evengreater, as new hospitals continually meter, monitor, and controltheir usage through an intelligent energy management solution.
As a global leader in energy management, Schneider Electric hashelped both existing and new hospitals around the worldimprove their bottom line by reducing energy costs, as describedin this paper.
Schneider Electric is currently delivering solutions to a hospitalinAustralia, which hopes to be the country's first Five-Star Greenhospital. Due to open in 2011, this hospital will minimize waterand energy consumption as well as greenhouse gas emissions.Schneider Electric's solutions for the hospital include buildingautomation and security, medium and low voltage electricaldistribution, metering, lighting systems and powermanagement.
Hospitals like this are improving the overall patient journey,with reductions in patient recovery time, reduced risk ofinfection, and overall improved patient satisfaction. And it'sthese kinds of hospitals that India needs today — ones that useenergy intelligently and efficiently, while still providingprofitable bottom line results and better healthcare.
Identifying areas of high potential savings
Amodel Green hospital
•
•
•
•
•
The author offers 23 years of experience including, helpinghospitals and healthcare facilities improve their financialperformance, patient safety, and environment of care. Hebegan his career in the IT and automation businesses and can bereached at [email protected].
13

A pipe dream made real
With inputs from Jitendar Sharma, , Head — Department of Hospital Administration & Medical
Superintendent — All India Institute of Medical Sciences, Delhi, delineates the increasing applicability of Pneumatic
Chute Systems in hospitals.
Dr. Shakti Gupta
The meaning of the word ‘chute’ is as dynamic as is its growingapplication. Chute means to convey, deposit, go, send, or todescend. In most common applications, it is a long tube or slidein which things are dropped or slid down to a lower place.Pneumatic, on the other hand, means driven by air pressure.
Thus a Pneumatic Chute System essentially is a system oftransport which is driven by air pressure. Though engineeringtechniques could be applied to fix various regulators to themovement, an ideal chute system is one which can operate withleast number of resources or consumables.
The main advantages of a Pneumatic chute transport systeminclude:
i. Rapidity of movement — as nothing disrupts the flow
ii. Safety in transport — as interaction with external agents isimpossible
iii. Reliability of movement direction — as movement is towardsa fixed location
iv. Saving on manpower needed for carrying items
v. Reduction in turnaround time
It is interesting to see that the three characteristics mentionedabove, have special relevance to the items most commonlytransported within a hospital setting. Pneumatic Chute Systemsthus enjoy being one of the technologies capable of harnessingthe heavy load of transport of sensitive items within a hospitalfacility.
Laboratory samples, blood samples, drugs, injection vials,saline bags, disposables, reports etc. can be safely and speedilymoved from one station to another. For instance in the transportof samples from Emergency department to the Laboratory, fromOperation Theatre to Emergency, from hospital stores to OT andviseversa.
There is practically no limit on the number of stations that canbe connected or the distance that it may need to cover. With thePCS system installed in the hospital, critical patients andattending staff shall no more wait for staff to run over fromplace to place to perform errands and carry supplies.
The System is driven by an air compressor, which is installed in a
central place and generates air pressure to transport items. Thecontrol station is equipped with a computer system in which thechute system software is loaded. This system contains thedigital control with records and data of all transfers.
The other unit of PCS is the “diverter” units. This unit receivesthe items, takes the air pressure from the compressor andsignals from the computer as inputs, and ‘diverts’ the items intothe desired location. Thus, when the sending station i.e. theplace from which an item has been dispatched comes to thediverter, depending upon the destination station numberpunched at the sending station, appropriate signals are sent tothe diverter, which in turn shoots the items in the desiredlocation. The receiving station is equipped with a similar shootand items are received on a platform.
It is important to note that though the system gives “to & fro”service, every receiving station or sending station has only onechute panel. The items are sent in fibre jar with corks inside tokeep the items safe and intact. Thus transfer takes place withina matter of seconds.
The running cost of the chute system is considerably low, andconsists of mainly the electrical consumption and themaintenance contract charges for the system. Though theinitial investment could be high, it justifies the savings incurredon the salaries of staff used for transport of items and also theopportunity cost of the time saved in the item transport.
Chutes are grouped as per their design under the followingheads:
i. Single entry chutes which have a single entry point.
ii. Multi-entry chutes are those that are modular single chutes.
When an assembly of chute lines is planned in different floors,the height of each chute equals to the height of the floordifference connecting the two chutes.
Chutes could be placed either inside or outside the buildingdepending upon the area being covered and the number ofservice stations attached.
Pneumatic Chute Systems could be used at a number of places ina hospital setting, more so when the set-up caters to a largernumber of beds, and when the hospital building has a
How PCS works?
Design based classification
15

perceivable vertical height and the human resource is limited.
Functionally, the PCS can be used in a hospital for followingpurposes:
Pneumatic Chute for Laboratory samples: This transportslaboratory samples from the phlebotomist cabin to adesignated place in the laboratory. The results arecommunicated usually using a computerized hospitalinformation system which brings the values online attached tothe patient’s unique bar-coded identification number. In theabsence of such a system, reports in hard copies could be senteither conventionally or via the chute system.
Transportation of blood and blood components: It is a commonperception that the staff of blood banks remain occupied withthe blood banking activities, whereas that of the clinicaldepartments with patient treatment activities. Though in theabsence of a pneumatic chute system, the onus of collectingthe blood units from the blood bank remain with the clinicalstaff, pneumatic chute system does this transactionaloperation without a continuous human resource attachmentand yet, the delivery is made in a protective way at a pre-decided recipient area.
The linen and laundry system demands heavy workforce due toits sheer quantum of work. Here, instead of precision infunction like in the laboratory or blood bank, the PCS works likea heavy transporter of goods. Thus, need for mobile transportmachinery and manpower is reduced, hazards of handlingsoiled linen are minimized, and timeliness and work efficiencyis maximized.
Transport of medical and surgical stores from the central drugstores to the substores at consumption centres like the wards,emergency units, OTs and ICUs. The main advantages being —safety during the transport of items and promptness in deliverywithout any potential chances of en-route thefts.
Centralized Sterile Supply Department (CSSD) finds theapplication of PCS for transporting the sterile as well asreceiving the unsterile items from the theatres. It is importantto note that a PCS does not alter the status of sterile items, thusmaking it a safe pathway for transfer of items.
Bio-medical waste transport using PCS has gained goodpopularity. The challenges of training all the staff towards safehandling of bio-medical waste are well-recognized. Further,the reliability of materials used for packing waste and thechances of potential spillage during transport hover around theplanning of waste disposal pathways. Even the disposal zone ordirty utility corridor of Operation Theatres is being speedilyreplaced with PCS which comes up as a space saving andrelatively risk-free methodology.
Technology has brought the integration of alarm systems withthe PCS which makes it more prompt. Alarms can be used toinitiate the process of transfer by placing a call reminder to thesender and/or recipient. The receiving of any new item at areceiving station also triggers an alarm to the receiver.
Ambience and internal environment control is an essentialfeature which enables the preservation of blood samples,medications and sterility of packs and instrument kits. Thetemperature and humidity inside the chute is controlled so thatitems due not get altered in quality, physical and/or chemicalproperties when in transit.
PCS can also be deployed as an emergency evacuation strategyin case of disasters or accidents. The design of such humanevacuation specific chutes is different in terms of protectivelayers and landing. Some companies in the western countriesare installing chute systems that can evacuate at the rate of 25persons per minute. This provides solution for rapid evacuationof patient and healthcare staff in the quickest possible time.
Knowing the excellent features of the PCS technology, it isimportant to have the following considerations:
It is necessary to have appropriate cleaning and disinfection ofthe Pneumatic Chute Systems. Use of mild disinfecting agentsandAir Scavenging Systems can be extended for this purpose.
Popularity of this technology should be increased by exhibitionson hospital technology and by providing training to the hospitalstaff.
In India, there is no formal certification of the PCS by anystandardizing agency. However, being a product with highpotential of use in public sensitive places like hospitals, itwould be appropriate to get the available productsstandardized for quality, specifications and design.
Making the chute systems fire resistant would make it safer andmore acceptable for use in patient and staff evacuationscenarios.
Using robotics to clean chute system would be another areaneeding exploration.
The Pneumatic Chute Technology needs to be explored,
examined and extended for use in healthcare institutions toprompt uninterrupted, faster and accurate care delivery, andreducing the overstretched workload on healthcare workers.
Some improvisations
Challenges and ways to harness PCS technology
The author has over 25 years of distinguished academic andhealthcare management experience, and has authored fivebooks in the specialty of Hospital Administration. He can bereached at [email protected].
16
Anil Joseph, Country Director — Ortho Clinical Diagnostics — Johnson & Johnson, unravels Lean thinking and
designing for a slick hospital laboratory and more.
Take a look around your lab. You'll see countless opportunities tobetter organize your supplies and put equipment within easierreach. But which changes would be cosmetic and which wouldmake a meaningful difference? Other situations seem to defysolution, such as orders piling up in your receiving area, anendless stream of STAT requests, and a constant reliance onovertime.
The good news is that there is a proven methodology toeffectively address these issues — systematic ways to determinewhich changes are readily achievable and will streamline yourworkflow, eliminate waste, and let you deliver better value.That proven methodology is Lean. Lean is doing more and morewith less and less. It is a methodical approach to eliminatingwasted effort and lost revenue in your lab.
At any size, at any level, clinical laboratories can reduceexpenses and enhance revenue with ValuMetrix® Services. Toachieve permanent solutions, we work closely with bothmanagement and laboratory staff to maintain andinstitutionalize improvements and redesign. These efforts alsoinclude training, mentoring and certification of personnel. Moreimportantly, Lean implementation produces improvements inthe quality and operational efficacy of clinical laboratories andtransfusion services and blood donor centers.
The underlying Lean principle — to create flow and terminatewaste in all its forms — is logical and readily understandable.The ValuMetrix process sets out to eradicate waste, to simplifyand to standardize. Laboratory layouts have often evolvedinstead of being designed for purpose. A laboratory mightmaintain the highest standards of clinical excellence, but aprocess can be verifiable yet still flawed from a Leanperspective. If there is over-reliance on memory and vigilanceto do the work right, then the work required to maintain thosehigh standards will be more stressful — and probably more costlythan it need be.
Every change made as part of the ValuMetrix process issupported by data from your own laboratory. The variousProcess Excellence tools that are routinely employed include:
Lean review of processes, products and information flow
Voice of the Customer (VOC)
Visual Control Management
Process Mapping
Value Stream Mapping
Workcell Utilization Maps
Review and analysis of value added and non-value added
•
•
•
•
•
•
More with less
17

activities from the data collected can help identifyimprovement opportunities. Most of the recommendationshave a significant financial impact. Others, while not assigned adollar amount, offered substantial value in terms of quality ofpatient care.
For 14 weeks — from July to early October 2006 — a Lean teamdevoted 100% of its time to a lean implementation process. Thiswas an in-depth redesign of lab processes. After initial leantraining, the team's analysis of the current situation found theexisting lab layout and processes drove wasted motion anddelayed turnaround times. The team designed a new lab layout,focused on reducing systemic waste. The team also introducedstandard work, 5S, and visual management in multiple areas,and implemented a visual system for organizing andreordering supplies.
Most hospital laboratories are designed in a departmentallayout, even if the lab is a single open room. This is an historicalartifact, which dates from the time when academic specialtiessuch as chemistry and urinalysis were located in different
rooms or floors. As hospitals created unified clinicallaboratories, managers continued to organize the layout bydepartments, even though most technologists weregeneralists. As testing became more automated, manylaboratories still adhered to the “one machine, one tech”approach. Even with “walkaway” instruments, techniciansoften stood and watched an instrument, “just in case.” Physicalseparation of departments made it difficult for lab employeesto communicate or assist each other when workloads in onedepartment were high.
The lab layout didn't consider the flow of specimens, such astubes of blood. Chemistry, a high-volume testing area, was inthe back, far from the point where specimens arrived. Astraight path from receiving to testing was blocked by a largesupply storage cabinet. The newly created lean “core lab”
layout considered the flow of products (specimens), operators(technicians and lab assistants), information, and material(replenishment of test reagents and other consumablesupplies). Department boundaries were broken down, creatinga single U-shaped cell with different automated instrumentsnext to the specimen receiving department to encouragesingle-piece flow of specimens.
With the new layout, specimen travel distance for chemistrytests was reduced by 54%, from 146 to 67' (44.5-20.4 m). Withthe lean system, hematology techs' walking distance per hourwas estimated to decrease by more than half. As in amanufacturing implementation, the lab's lean efforts and newlayout set free significant space. When lean was firstimplemented in October 2006, the percentage of lab testresults available on doctors' charts by 7 am was 62%. BetweenNovember 2006 and January 2007, that amount increased to85% and was sustained at 82% for March 2007.
Lean is not a “project” that ends after an initial timeframe. Itrequires long term commitment and management support. Thehospital's leadership is now looking at bringing the leanapproach to other areas, such as the lab's Microbiology area,and other departments, such as the pharmacy and surgicalinstrument sterilization. They join a growing number ofhospitals that are implementing lean, and understand that it ismore than just a toolkit, a cost-cutting method or a project.
Case Study — Hospital Lab
kanban
The author has had over a decade of professional experience,including exposure to some of the best systems & practices inthe world. He can be reached at [email protected].
18

Pathway to glory
Hussain Varawalla, Mentor — Design Services — Hosmac, lights up yet another vital aspect of hospital
infrastructure — the circulation routes.
‘Circulation’ is defined by the Merriam-Webster's Collegiatedictionary as “orderly movement through a circuit; especiallythe movement of blood through the vessels of the bodyinfluenced by the pumping action of the heart.”
So we have our medical analogy, though a hospital is oftencompared to a small city, I've never heard or read a comparisonto the human body. We do, however speak of the ‘pulse’ of acity, and it's ‘major arteries’. But we are wandering; let us getback on track.
In the above definition, ‘orderly movement through a circuit,’the word we should pick up and focus on is ‘orderly’. It impliespurpose, and purpose implies design. We are going to talk aboutthe importance of the design of circulation in a healthcarefacility.
Hospitals, like the small cities they are likened to, contain maincirculation routes often described as hospital streets. The wayin which — different parts of the hospital are assembled, as acoherent whole but with the parts differentiated, make foranalogies with urban design; the way in which traffic moves,and the routes that are taken by mechanical and electricalservices are fundamental generators of the plan.
In a vertically stacked hospital, which could also be called afunctionally stratified hospital, almost always the inpatientareas are placed on the upper floors, to allow for a morepleasant, naturally lit environment. The planning grid for thehospital is determined by the layout of these inpatient floors.Another important planning feature, the vertical circulationcore, is also to some extent located within the building by thelayout of the inpatient floors. Usually, in vertically organizedhospitals we design “from the top down”, that is, we design theinpatient floors first. What we actually do is during the layout ofthe inpatient floors, we provisionally decide on a position forthe vertical circulation core and other staircases that may berequired, many a times by the local building codes. Thislocation, however, is to be checked for its design impact on thelower floors containing the diagnostic/therapeutic/interventional departments.
The pattern of circulation conceptualized for the hospitalunder design will be considerably impacted by the location(s) ofthe vertical circulation core(s).
It's something like all roads leading to Rome(s). The verticalcirculation core is the centre, the focus of all the majorcirculation paths of the hospital. An attempt can be madethrough design to minimize vertical transportation by siting (forexample) all surgical beds, operating theatres and the intensivecare unit on the same floor. This design approach may be usedas a justification to reduce the number of elevators, or thewidth of the staircases, but in no way does this mean that thecore can be located more casually by the designer.
Avoidance of dependence on lifts is particularly important inplaces where maintenance and availability of spare parts isunreliable; long waits for lifts are a major cause of inefficiencyand frustration to hospital users — more of a problem, the tallerthe building is.
It is important that patients, visitors and staff are enabled toorient themselves while moving through the hospital byproviding windows in corridors to enable them to look out andto allow natural light in, important in alleviating the tedium oflong corridors. If the site enables them, courtyards are also anexcellent means to this end.
As such there is no easily available prescription for the way thecirculation pattern of a healthcare facility should be. Thequalities it should possess, however, I will try to enumerate:
It should have conceptual clarity. By this I mean it should bedesigned with purpose, and should not be the leftover space orsqueezed into the gaps between other areas. Geometry can bea recourse, but it should work with other planningimperatives. Junctions should be uniquely treated to avoidconfusion over which corner of the hexagon (for example) youhave reached.
It should not be boring. Try to make walking from one place toanother interesting, modulate those corridors, color them
19

differently, and hang artwork along the way. Niches, outsideviews, courtyards, all these will help.
It should enable wayfinding. In combination with well-designedsignage and maybe supergraphics, people should be able to findtheir way to their destination with ease. Color-coding for floorsor departments is sometimes used.
They should be wide enough to handle anticipated traffic.Stretcher traffic needs 8'-0” width of corridor for easymovement (turning). 7'-0” will work, but use 8'-0” if you can.Corridors between Operation Theatres make sense even with10'-0” width.
There may be a lot of stuff parked along the sides, despiteinstructions to OT staff on the contrary.They should beindirectly lit. Patients on stretchers get to look at the ceilings.The sign put up by the traffic police at the end of Marine Drivein Mumbai says, “Drive carefully. Hospital ceilings are boring.”While not advocating rash driving, we would advocate makingthe ceilings interesting.
Some of the hospitals currently existing in India have beenprovided with ramps in addition to the usual elevators andstairs. Power cuts are realities that have to be considered. Butconsider putting some (two) of the elevators on a generator, ifthis helps in avoiding the ramp, which is wasteful of space anddifficult to use, as the gradient is often excessive. With anacceptable gradient, the length becomes excessive,considering that the lower floors of hospitals are considerablyhigher than those of the usual non-hospital building.
When planning for the area occupied by this circulation space(corridors) in the architectural space plan, it can be providedfor as a percentage of the department area (usable, built-uparea). This percentage will vary depending on the departmentand may also vary if the architect has any special feature inmind for that department, which is not explicitly provided forin the room-by-room area statement (such as semi-covered,landscaped waiting). The percentage can vary from 35% for anOperation Theatre Suite (with 8'-0” corridors) to 20-25% for theadministration department.
On the inpatient floors or even in the outpatient department,these corridors can be modulated by recessing pairs of doorsthat occur at regular intervals, and using an accent color in theniche so created. This helps relieve the boredom of walkingthrough long, uninteresting corridors.
Very frequently, the major circulation paths through thehospital are laid out even before the tentative space allocationfor the hospital departments is done. Thus, the importance ofconceptualizing these paths in a way that they contribute tothe concept and functional layout of the hospital is not to beunderestimated, the exercise should not be done casually.
The manner in which the healthcare architect conceptualizesthe working (and therefore layout) of certain hospitaldepartments, notably the Operation Theater Suite and theRadiology & Imaging Sciences Department will determine thecirculation pattern through that department, and hence affectthe layout of circulation paths in contiguous areas of thehospital.
Habitually, we healthcare architects find that in the areasbelow the footprint of the inpatient tower in the podium, weend up using the same corridors that we used in the inpatientfloors. (At least I find myself doing this quite often. There mustbe a good reason for this, I hope there is!)
Defining major circulation paths through the proposed andfuture buildings is a design decision that will considerablyimpact the form, layout and thus the eventual functioning ofthe healthcare facility being designed. Do it thoughtfully andwith conceptual clarity.
The author has had 20 years of rich experience in healthcaredesign building, and has worked with Reliance HealthcareVentures Ltd. He can be reached [email protected].
20

Dr. Sujit Chatterjee, CEO - Dr. L.H. Hiranandani Hospital, unveils organized outsourcing models in corporate hospitals.
One of the major reasons for, the most powerful man in theworld, President Barack Obama of the United States to visitIndia was the issue about outsourcing! It is a reality and is a USD60 billion industry in India, and from all counts it seems to begrowing. According to Dunn & Bradstreet, outsourcing hasbecome USD 4 trillion a year business, world wide.
While we keep speaking and writing about the US, the truism isthat outsourcing in healthcare too is a reality in India. This 60billion dollar pie has affected businesses across industry andhealthcare is no exception. Outsourcing potentially enablesbusinesses to reduce costs, and concentrate on corecompetencies. Thereby, essentially, transferring non-corebusiness processes to others, allowing those who are competentin their fields to ensure services are provided, effectively andprofessionally.
Outsourcing is basically classified into strategic outsourcing,where a number of functions are outsourced, such as security,catering, insurance, housekeeping, laundry, so on and so forth.Whereas functional outsource involves a single function. Thereis also departmental outsourcing such as a particulardepartment of radiology or engineering.
Pursuant to the foregoing, organizations that are interested inoutsourcing are often curious to know about the advantages anddisadvantages of such a process. It is but natural thatoutsourcing some of the functions which had to be traditionallyin-house within the hospital could be an area of concern, and tillthe organization is fully aware of the pros and cons, woulddesist from jumping headlong to outsource a particular
function, department or a making policy for strategicoutsourcing.
Our hospital after having extensively studied outsourcing fromthe hospitality sector took it on itself to lead in the field ofoutsourcing strategically in healthcare. The departments thatwere outsourced at the outset at Dr. L.H. Hiranandani Hospitalwere security, housekeeping, patients' services (in transportingpatients from one department to another), catering andlaundry.
Having learnt from the above, this hospital is now even engagedin functional and departmental outsourcing. The benefits ofstrategic outsourcing include:
i. A non-core activity is given to another, and this gives theorganization more time to concentrate on core business.
ii. It increases the efficiency and also the productivity in thenon-core business areas as professionals were hired to dothat work without hospital staff having to understand thenitty-gritty and put the processes in place.
iii. It helps to streamline operations, manpower issues areoffset as the outsourced organization is wholly responsibleto provide the same.
iv. It gives the organization the flexibility to increasemanpower in short notice if it is required.
v. The outsourced organization invests in latest technology forcarrying out their professional tasks which also saves timefor the hospital as no further research is needed to perform
Engaging experts externally
21
these tasks to perfection.
vi. The hospital processes for cleaning or housekeeping, etcare run efficiently and the turnover time is also less.
vii. It has helped the organization to understand the cash flowas well as plan in advance the cash flow required for all thesefunctions.
viii. It is my perception that the hospital got a competitive edgeand was able to maintain standards of cleanliness.
While the above is the sunny side up, there is a sunny side downand that is:
i. The outsourced partners must share the ethos of theorganization and that requires multiple levels of meetingsand also the hospital's participation in their trainingprogramme.
ii. There may bee discrepancy in salary & benefits between thefull-time employees paid by the organization and theoutsourced organizations.
iii. As a principal employer it is also the hospital's responsibilityto ensure that the outsourced organizations have met allthe statutory requirements of their employees.
iv. The hospital has to depend on the outsourced organization'sprobity that it has screened all the employees beforeemploying them within the hospital.
v. It is a challenging task to keep the outsourced organizationfocused on the customer and ensure that the ultimateexperience is not blemished by the outsourced employeesperformance and behavior.
vi. There can be several disadvantages in outsourcing, such asrenewing of contracts, lack of communication,misunderstanding of the contract, delay in services thatimpact customer decisions and poor quality of service oreven worse and inconsistent quality which would create animpression that the hospital is either very good or very bad.
The experience in departmental outsourcing in this hospital hasbeen with the engineering department and before it wasoutsourced the organizations were explained the hospital'senergy utilization policy, energy discipline, concept of daylightharvesting and the organization's desire to support theGovernment and return power to the national grid or utilize lesspower that the allotted quota. For this the hospital has beenvery successful and has utilized 25% less power than the allottedquota. The hospital continues today with the departmentaloutsource.
Healthcare today in this country is cost intensive and thesecomes from the facts that there are newer diagnostic tools aswell as therapeutic that come at a phenomenal cost. Also inhealthcare there is the obsolescence which is rapid and
depreciation which impacts healthcare costs and these aretransmitted to the patients. Rising costs have impacted healthinsurances in particular and everybody in healthcare is aware ofthe stand off between the insurance sector and the healthcaresector.
To offset some costs this hospital had thought in terms ofanother departmental outsource and that was radiology. Asuitable partner was identified and taken on board and thishelped the hospital reduce the cost of high ticket items as CTScanners, MRI machines, so on and so forth and at the same timethe partner's land and infrastructure costs were reduced. Thecosts to the patients were competitive and the cost advantagewas transmitted to the patient. Thus it was a winning situation
for both the providers as well as the patient.
The future if outsourcing is bright. It is a industry that is here tostay. In a highly competitive business environment companiesneed to stick to their core competencies and go for strategic,departmental or functional outsourcing to reduce their costsand become very effective in their services to their customers.Outsourcing requires an essential business skill. Thus thesuccess of the business will depend on managing outsourcingrelationships.
While newer business models in healthcare need to be exploredto contain healthcare costs, outsourcing may be a effectivemodality to be considered for all future projects, be itstrategic, departmental or even functional.
The author had led the Hiranandani Group to be the firstPublic Private Partnership in healthcare with the NaviMumbai Municipal Corporation. He can be reached [email protected].
22

Narendra Karkera, Director — Hosmac, explains the changing paradigms of healthcare and how cost can be revised
in the current scenario.
The competitive market
Market
Health insurance
Quality
Overheads
Need of the hour
Today, the world is fiercely competitive, and India is noexception to it. For a healthcare facility, there is an immensepressure to reduce tariffs to attract more customers.Healthcare organizations are beginning to relook at theirexpense structure and reduce costs wherever possible. A lot ofemphasis is put on finding out the underutilizations andinefficiencies within the organization.
The health industry views itself as the “Seller's Market” with anability to command over price. However, this is no longer thecase today. With competition mushrooming in the form of newfacilities opening up every other day, the customer has easyaccess to healthcare to both — ultra-modern facilities andexisting facilities at increased service levels. Each new facilitywants to prove itself unique and patient-friendly to attractmore customers. It has to invest in marketing to make itselfvisible in the face of existing brand names. Hence to controlexpenditures and recover investment, every new facility is costconscious.
Easy availability of affordable health insurance has helped theIndian population to move towards getting health cover andeven cashless hospitalization. This has also created demand formore healthcare facilities but this advantage comes with a rider— the medical insurance companies demand high quality servicefrom the healthcare facilities at lower tariffs.
Essentially, all insurance companies should categorizehealthcare facilities into categories A, B and C with respect totariff, location and quality. If a healthcare provider wants toqualify for grade A, then it should qualify as per the standardslaid down by the insurance companies. This should help makeimprove insurance companies profitable. Also if hospitals arecategorized, a healthcare service provider categorized as B or C
is incentivized to upgrade his facility to Category A for higherpotential revenues.
The measures of Quality are based on objective criteria likematerials used, service levels, patient satisfaction etc. It is acommon belief that high quality comes at a high cost. This beliefis erroneous. Skillful purchase negotiation can reduce costs ofprocuring even the highest quality materials. Better qualitymeans faster recovery and less length of stay, more turnover,and hence more revenue, more utilization, more efficiency andless cost. Improvement in process and service delivery alwaysleads to a low cost as a result of avoiding unwanted processesand better utilization of man, machine and materials.Increasing patient satisfaction increases demand and reducesoverheads. Hence quality does not cost, the lack of qualitydoes.
The need of the hour is to sensitize the employees about thewastage of material and identification of unnecessaryprocesses. This leads to better utilization and efficiency ofmanpower. Multitasking and regular training of personnel, bothclinical and non-clinical should be an organizational practice.An important observation is that much effort is spent inmonitoring the overheads of the revenue generatingdepartments while the non-revenue generating processes areignored. Equal focus should be given to support-servicedepartments as they also tend to increase cost due tounderutilization and inefficiency. It is observed that if the costgoes up in certain cost centres, it is pushed onto the patient byway of an increase in tariff rather than relooking into thecosting, and finding reasons for the increase and takingcorrective actions thereof.
Healthcare providers must relook at their costing and find out
Distilling costs alike
23

areas where cost reduction is possible to maintain theirprofitability without increasing tariff. This can be done byprocess re-engineering and accepting the most modern methodof costing i.e.Activity Based Costing (ABC).
One of the benefits of adopting ABC is that non-revenuegenerating departments are given equal importance, whileperforming the costing exercise.
ABC can be used under following situations;
i. When the overheads are high
ii. When services are diverse and complex
iii. When cost of errors is high
iv. When competition is stiff
The above points are acutely relevant today. A set-up needs tocontrol its overheads and not pass it on to the patients.Inefficiency and underutilization on the part of the institutionare not the patients' problems, and passing this cost to thepatients is unethical.
ABC could help in finding the true cost of the service, hence itresults in accurate costing, focused approach to hospitaloverheads, caters to both internal and external customers:external customers by the way of tariff rates and internalcustomers by the way of interdepartmental charges. Usually inconventional costing, the service centre overheads are eitherapportioned or allotted to the revenue centres, and revenuecentres add their cost and margin to arrive at a tariff rate.
Under ABC no overheads are passed on but actual billing is doneby service centre to the revenue centre for the service taken,hence there is an internal tariff of service centres. The tariff ofservice centre charges can be compared with the market andshould be competitive. This process would make all cost of therevenue centre direct except its own departmental cost.
a) Equal importance to service centres as the revenue centre
Today, we give more importance to only the revenue centre.But under ABC, even a service centre would get equalimportance since it too would generate billing.
b)Activities of the service centre are monitored continuously
Under ABC, service centre charges would be compared with themarket prices. Hence, service centres would have to keep theircost under control.
c) Underutilization and inefficiency of both — revenue andservice centre are highlighted
Due to continuous cost monitoring, all costs due toincompetencies are automatically checked and correctivemeasures can be immediately taken.
d) Self-discipline in both revenue and service centres
Monitoring would also bring in self-discipline since accountingresponsibility would be in place.
In short, each cost centre shall work like a strategic businessunit and would be seen as a profit centre, whereby reducing theburden of the hospital administrator in monitoring the day-to-day operations.
Whenever a costing exercise is conducted, one encountersresistance from the department heads because such exercisecan reveal their department’s fallacies. Besides, no employeein the operational area would like to volunteer for this exercisesince it may only bring out the deficiencies of a department. Agood deal of convincing needs to be done to make them feelthat it is in their own interest to make this exercise successful.
On the other hand, the accounting staff in the organization maynot like to take up ABC because they may view it as additional
work. In some cases, the existent accounting staff may not beexperienced to conduct ABC, and may require some externalspecialist to undertake it. It is difficult to get trained staff orexperts for doing such an exercise. This operation can best beundertaken by only a hospital that is fully computerized.Manually,ABC is an onerous task.
Activity based costing has become a priority for all hospitals:for their survival and future growth. Before starting thisexercise, business process re-engineering must be instituted,and all kinds of incompetencies from the organization must beexpelled. Thereafter, the various cost centres in theorganization must be spell out in utmost detail; a cost centrecan be a single man or a single machine. Once havingdetermined the cost centre, the activities of these costcentres: manpower cost, material cost and other overhead costfor each activity charged to the revenue centre must bedetected.
A defined margin is added to the cost and a tariff rate is arrivedat. The difference between the conventional method of costingand theABC method is that under conventional method, servicecentre costs are apportioned or allocated to the revenue centreirrespective of usage of service, whereas inABC, cost is chargedto the revenue centre based on the usage of the service. Hiddenunderutilization, inefficiency, wastage etc of service isuncovered and curtailed — making all service centres morerealistic in charging the revenue centre. Charges of servicecentre can be compared with the market rates and madecompetitive.
In activity based costing, the cost is charged to the revenuecentre based on the type and time of service availed from theservice centres. Therefore, these charges by service centresbecome variable costs since they are fees for the respectiveservices. This would result in making all costs variable exceptthe revenue centre's own departmental expenses.
What is further suggested is to add a defined margin on the costof the service centre and arrive at a tariff for all the services ofthe service centre, this would then result in making all servicecentres generating their own notional revenue, and would beseen as a revenue centre. By this method, all the centres wouldbecome profit centres. Above all, a cost conscious cultureshould be developed by the top management to implement andenforce the paradigm shift in costing.
Activity Based Costing
Further advantages ofABC
Hindrances
ABC simplified
Derivation
The author has served the finance and administrationdepartments in various leading healthcare organizations forover 37 years. He can be reached [email protected].
24

Be a radiologist!
Rajeev Pradhan guides healthcare aspirants and professionals to play a more intrinsic role in the
healthcare industry.
Ever wanted to get your hands on one of those spy glasses withvision that could penetrate the human skin and see rightthrough to the bones, the kind we see in the movies?
Well, even if you don't exactly get them at a neighbourhoodstore, the idea of expanding the number of things we can seewith our eyes with the help of technology has long been apursuit of scientists. Once W.C. Roentgen discovered themysterious phenomena of X-rays in 1895, it became possible forus to look beyond the naked eye and make an accurate diagnosisof a plethora of medical conditions.
Over the years as technology progressed, so did the need fortrained professionals who could properly utilize this technologyand aid in the diagnosis and treatment of the patient.
Most of us at some point of time have either broken a bone orhad a surgical procedure performed. The first step in anymedical consultation after studying the background history is toaccurately diagnose the underlying condition. There are varioustools which help us in this step, principal of these being theimages taken using different medical equipment. From simpleX-rays, imaging tools have today been extended to CT scans,MRI and PET which use the principles of physics for penetratingthe human skin by applying low levels of radiation such that
they do not harm the human body.
But what do we do once we obtain this image? To a layman, a CTscan might seem like just a blurred black and white photo. It isthe job of the radiologist to effectively interpret this image anddetect the abnormality in it, thus paving the way for asuccessful treatment regime. There are two roles a person canplay in this event — that of a radiologist or of a radiologytechnician who carries out the actual procedure using theappropriate equipment.
The first step to becoming a radiologist is to acquire a degree inmedicine (MBBS) — which takes approximately five and a halfyears. After which a student needs to take an entranceexamination for post-graduation. There are entrance testsconducted at the state-level such as PGM-CET for admission tomedical postgraduate courses such as MD/MS/Diploma (inMaharashtra); at the national-level such as the All India PGMedical and Dental (AIPGMEE); or those conducted separatelyby deemed universities. Depending on the rank thus obtained, astudent can then choose the further course of action.
An MD in Radiodiagnosis is the preferred option for thoseobtaining a good rank, the duration of which is three years.During these three years of resident-ship, students receive astipend as per their post. Another path taken by many is to get adiploma, either a DMRD (Diploma in Medical Radiodiagnosis) orDMRE (Diploma in Radiology and Electrology), both of which areof a two-year duration and can be pursued simultaneously withan MD.
A diplomate of National Board Degree in Radiology is also anoption that students can pursue. Sneha Zanje, a DNB student,currently doing her residentship with Lilavati Hospital explains,“Post MBBS, one can work as a resident in a hospital with the X-ray, CT scan or other department for three years. At the end ofwhich, they have to submit a thesis, upon which a degree is
Academically speaking
25

awarded to them. This degree like an MD allows them topractice anywhere in India.”
Dr. Arjun Kalyanpur, MD — CEO — Teleradiology Solutions, adds,“While one may practice radiology with a DMRD, careerprospects can be improved by obtaining a DNB or a MD degree.Also, for academic (teaching) positions, a DNB or MD is typicallya mandatory requirement.”
Dr. Girish Burde, MD, DMRD while explaining about the variousavenues in radiology states that, “Radiology is a diverse field,as apart from reading X-rays, CT scans, MRI, PET scans;interventional radiology plays a huge role too. In interventionalradiology, using sophisticated equipment for image guidance,minimally invasive surgical procedures are carried out. Forexample, the introduction of stents to treat embolisms (orblockages) in an artery, in any part of the body or even in thecase of tumors and aneurysms, a radiologist plays the definingrole. The noninvasive nature of most of these procedurescontributes to its cost effectiveness, ultimately benefiting thepatient.”
Another avenue for aspiring radiology students to explore is theDiploma in Medical X-Ray Technician (DMXT) or a Bachelor ofScience in Medical Imaging Technology — both of which can betaken up after passing class 12 examinations with physics,chemistry and biology as the principle subjects. These coursesessentially help a student take up work as a technician whohandles the actual process of X-Rays or CT scans. Admission tosuch courses is subject to individual college requirements.
Apart from these, radiology professionals can also branch outinto teleradiology — a field fast gaining popularity. It is a form ofoutsourcing, where X-ray images or such are sent from differentcountries (such as underdeveloped regions of our own country)to radiologists elsewhere that can analyze them.
“This is the future of radiology, given that it allows images to betransported to the radiologist and interpreted from anywhere.It allows high quality diagnostics to be delivered to theunderprivileged in remote parts of the country,” elaborates Dr.Kalyanpur. With experience, one can even run their own setup
for medical imaging services or work in large hospitals.
Radiology is considered as an elite option for post-graduationafter a medical degree. Stable working hours and relatively lessstressful conditions coupled with attractive remuneration,even for freshers, makes radiology a much sought after careerchoice.
Dr. Kalyanpur further emphasizes this fact, “There is a seriousshortage of radiologists in the country and hence radiologistsare in great demand to meet the growing healthcare needs ofthe country today. It is a rapidly evolving, dynamic and excitingbranch of medicine on which all other clinical specialtiesdepend.”
Dr. Burde seconds this opinion as he states, “Radiology is achallenging field as you are not restricted to any one certainpart of the body.”
Thus, if you are looking for a dynamic career which combinesmedicine and technology and tests your knowledge andanalytical skills to the fullest, radiology is definitely right foryou.
Abundant avenues
Radiology rewards
The author can be reached at [email protected].
26

Healthcare made affordable
Dr. S.K. Saran, Director — Medical Services — Yashoda Medicare & Research, puts together an interesting analysis
of the present-day healthcare industry with suggestions to develop affordable healthcare for all.
Healthcare systems across the world are constantly workingtowards providing equal access to healthcare facilities at lowcosts without compromising on quality. The challenges areenormous and the remedies — limited, coupled with economic,social and political implications. One way to reduce healthcarecosts is to reduce higher spends on medication and treatment,which calls for emphasis on preventive healthcare mechanisms.
People's ability to pay for healthcare is not determined only bytreatment costs, but by a series of other socio-economicfactors. One of these is the role of payment modalities. Thecurrent pricing policies may need to be relooked at foralternative methods.
Hospital pricing policies often leave patients confused andexasperated. Industry analysts say pricing justification isgaining importance as consumers become more involved inpaying for their own healthcare. With the number of healthinsurance providers growing, hospitals are being called uponmore frequently to explain and defend their pricingmethodologies.
The Constitution of India incorporates provisions guaranteeingeveryone's right to the highest attainable standard of physicaland mental health. Article 21 of the Constitution guaranteesprotection of life and personal liberty to every citizen. TheSupreme Court has held that the right to live with humandignity, enshrined in Article 21, derives from the directiveprinciples of state policy and therefore includes protection ofhealth. Further, it has also been held that the right to health isintegral to the right to life and the government has aconstitutional obligation to provide health facilities.
While the Government has laid the policies and planned theconstitutional rights judiciously, it has failed to execute itsuitably. The socio-economic determinant of the currentscenario has resulted in the inclusion of the “aam admi” asinitiated by our Honourable Prime Minister of India Dr.Manmohan Singh in the form of financial inclusion. However, it isinclusion and provision of basic infrastructure, sanitation,education, and potable water, which can result in “affordablehealthcare for all.”
India's healthcare expenditure is around 6 per cent of its GDP(USD 13 per capita) which in comparison to developed countriesis way behind in terms of absolute numbers. The abysmal stateof availability of qualified resources and healthcareinfrastructure can be judged by that current data which showsthe doctor and nurse patient ratio is 0.6 and .08 per 1000people, respectively; while the bed ratio is 1.5 per 1000 people.
A comparison with the world ratio where averages are 1.2doctors and 2.6 nurses and 4 beds per 1000 people shows a needfor improvement. There are more than 15000 hospitals of whichtwo-thirds are public owned. Of 1.1 Million hospital bedsavailable, 40 per cent are privately owned. The private sectoraccounts for approximately 80 per cent of healthcareexpenditure. Of the remaining 20 per cent, more than three-fourth is funded by respective state governments. Today, theIndian Healthcare Sector is valued at approximately USD 34billion.
Unequal power relationships interact across four maindimensions — economic, political, social and cultural, and atdifferent levels including individual, household, group,
27
community, country and global. It results in a continuum ofinclusion/exclusion characterized by unequal access toresources, capabilities and rights, which leads to healthinequities. Factors that can help in “affordable healthcare forall” could be such as the following.
The Government has set up limited tertiary hospitals such asAIIMS, which hasn't had the desired geographical reach. ThePPP model (Public Private Partnership) initiated by the StateGovernment with help from few financial institutions isgenerating a positive response and could give a boost to theaffordability of healthcare services.
The foundation of India's health policy was laid by the BhoreCommission Report in 1946. The report established primaryhealthcare as the foundation for the national healthcaresystem, and developed the first patterns for primaryhealthcare facilities and health personnel in the public sector.Therefore, a hospital system that accounts for a quarter of themarket must do more than manage the care of the patients, “itmust guarantee an adequate supply of primary healthcarecentres everywhere in the community and ensure appropriateaccess to emergency care.”
Minimal access surgery not only helps in making the duration ofthe surgery shorter but also in early recovery of the patient;thus resulting in a shorter stay and cost reduction. Similarly,day care treatment reduces cost. Nursing, pharmacy andtherapies with potential for home based treatment likephototherapy can be provided to reduce cost by deliveringtreatment at home.
Medical insurance could play a big role in reducing healthcarespends among the urban populace and sustainable schemesusing public-private partnership can bring smiles to the ruralpoor.
Private health insurance has played a major role in reviving thehealth industry after globalization, yet it covers a little morethan 1 per cent of the total population. Private healthcareproviders have already made substantial inroads in this areaand set up facilities both in India and abroad.
In terms of market penetration and affordability, mostdiagnostic centres and healthcare providers are restricted to afew cities and urban areas at a cost which only a few can afford.Cost is an important factor to consider especially for lowincome families and health insurance companies can play a
vital role in this regard.
One can reduce the risk of low cost health insurance plans bytaking only the right coverage that you will need and willprotect you when emergencies arise. State-level insuranceschemes have been launched and gained well-deservedpopularity among economically deprived classes. The initiativeby the Karnataka government to bring in ‘Yashaswini’ andAndhra Pradesh for ‘Arogyashree’ are perfect examples ofPublic-Private partnership. It has benefitted millions of peopleat a minimal annual cost (Rs. 30-60) who were earlier deprivedof world-class healthcare due to non-availability of insurance.
Due to the unceasing increase of health insurance costs, morefamilies are finding it difficult to find low cost health insuranceplans. Considering the huge positive externality from a healthysociety, it definitely calls for government intervention. TheGovernment should ensure that the benefits of its interventionshould largely flow to the patients through reduced pricesrather than to the hospital owners alone. The government canhelp through targeted incentives that can reduce the cost ofinsurance of such facilities by up to 30%.
Research and Development has aided the development of
Need for primary healthcare centres
Minimal access surgery, day care and home care treatment
Insurance Schemes
R&D
28

innovative devices, diagnostics, medicines and vaccines tobring in safe and effective healthcare delivery mechanisms ataffordable costs. This could be furthered by bringing togetherresearchers from both public and private sectors, largelyworking in India. Integrating and streamlining primary,secondary and tertiary services could make healthcareaffordable to a large section of people.
Hospitals strive to provide an optimum healthcare experienceand a more sustainable environment, especially one thatcontributes to quality patient care, revenue generation andregulatory compliance.As a result, hospitals are adopting GreenHealthcare Practices by creating conducive environments forpatient well-being, delivery of energy saving programmes,technology innovation and preventive services maintenance foroptimum hospital performance.
India has emerged as a destination for quality healthcare ataffordable costs to patients traveling from the west. Longwaiting lists, non-availability of expert medical care and highcost of treatment in their home country have forced many totravel to India for medical treatment giving impetus to ‘MedicalTourism’. Every year, millions of patients from around the globeflock to some of the finest medical tourism destinations in orderto receive five-star treatment at unbelievable prices. Indianmedical tourism was estimated at USD 350 million in 2006 andhas the potential to grow into a USD 2 billion industry by 2012.The private healthcare sector caters to this niche segment andrenders world-class affordable healthcare to patients usingstate-of-the-art technologies at a fee which is 10-15 times lowerthan anywhere in the world. These hospitals could help fill thegap by volunteering or regulatory methods to provide treatmentto the needy in emergencies.
Affordable and qualitative healthcare can be brought byintegrating technology, and innovations in healthcare policiesand infrastructure. Though the Government has takeninitiatives such as creating a framework of IT infrastructure forhealth in collaboration with private healthcare providers,establishing National Knowledge Commission (NKC),liberalization of insurance sector and so on, the desired resultsare yet to be realized. Electronic Medical Records Systems inevery doctor's office and clinic will ensure inter-operability ofsystems and facility, aiding the use of clinical decision aids.Telemedicine has proven itself as an excellent tool to help inprovision of affordable healthcare and all healthcareorganizations should be encouraged to use it.
The time is right for India to learn from the best practicesavailable across the world to customize, adopt and implementfor its own betterment before it fails to deliver the fundamentalpublic right of good health. Dr. Kalam envisages a strong anddeveloped India by year 2020 and so do I.
“The country's 'vision 2020' should include delivery of affordablehealthcare system even to the rural poor, apart from makingavailable the best healthcare system.”
–Former President Dr.A.P.J.Abdul Kalam
Green healthcare
Medical Tourism
IT for health
Conclusion
The author is a retired Group Captain, an MBBS, CIBM (IIMA) anda certified Lead Auditor ISO 9001:2000. He can be reached [email protected].
References:
· Indian journal of Medical Ethics (Health & Law) Issues Med Ethics.2003 Oct-Dec;11(4)
· Centre for Development & Human Rights (c) 2003 CDHR
· Statistics source:Asian Hospital & Healthcare Management
· The Next Wave of Corporate medicine- How we all might benefit: David MCutler PhD: NEJMAug 5th 2009
29


Financial modeling is the process of estimating and predictingthe performance of a project, venture or any other investment.It allows one to evaluate an investment in terms of its capacity,scalability, feasibility and viability. It helps in analyzingbusiness risks and challenges, and ultimately helps inevaluating the correctness of an investment vis-à-vis otheropportunities that may be available.
The healthcare industry is peculiar due to its critical socialimpact, heavy initial capital infusion, high operating costs andlong gestation period. Hence, it is critical for all stakeholdersto evaluate the potential risks and ensure its mitigation. Abusiness model to identify the future prospects on theinvestment and eventually understand the appropriateness ofthe investment is imperative for this industry. Hence, afinancial model helps to arrive at the estimated costs of theproject and analyze the stake holder's capacity to fund theproject or helps in arriving at various funding mechanismsother than the promoter's contribution.
The financial model for a healthcare venture throws light onvarious pertinent issues, some of which are mentioned below.
Although not a financial indicator, this forms the very basis ofany healthcare financial model/venture. The speciality mixincluding the facility, service and bed mix portrays, in anutshell, the whole gamut of services that the healthcareventure will provide. It is important to understand the mix wellbecause the nature of speciality drives the capex and revenuestreams.
For instance, oncology as a speciality is a high capitalinvestment and results show in a longer gestation period,whereas ophthalmology is easy on the initial capex with higherreturns vis-à-vis its initial capex. Hence based on a thoroughmarket survey, epidemiology and socio-economic condition of agiven area, the speciality mix is derived, which drives thefinancial model and the investment.
It is observed that the capital expenditure in ahospital/healthcare venture is considerably high. Theallocation towards building infrastructure costs and medicaltechnology is the highest, when compared to other cost heads.The total built-up area allocated per bed, in essence, drivesthe building infrastructure costs, and the speciality mix drives
Speciality mix
Capital expenditure
the medical technology estimates, since speciality specificequipment are estimated.
The revenues and expenditures are estimated based on thespeciality mix, area and technology specific volume, tariffs andcost assumptions. For example, income productivities,manpower estimations, salary patterns, overhead expenses suchas power, water, utilities, etc. It helps in understanding thecapacity of the venture to generate returns over a period of time.
Once the above parameters are estimated, the financial model isthen subjected to various scenarios, risks and case-basedsensitivities to understand the volatility and vulnerability of themodel to real-time changes and factors. These sensitivities canbe changes in the speciality mix or level of technology ordifferent revenue streams or differential schemes on expenses,etc. Similar to a simulation exercise, the financial model thenhelps in carrying out the analysis of the complexities of theproject, evaluate capacity utilizations to find out the optimalcapacity under varying industry demand-supply scenarios andsimilar other cases.
The financial model presents a fair idea to a potential investor onthe investment performance in a set period of time in the future.Considering the complexities of the healthcare industry,financial modeling helps in making informed decisions oninvestments, gauging the industry performance given aparticular set of assumptions and gives a view on the effect thatthe internal and external environment would have on a proposedproject/venture.
In conclusion, it is safe to say that financial modeling is the onlyway in assessing the feasibility and viability of a healthcareproject. At a later stage, it aids to compare the real operationalparameters with those estimated in the model to understanddeviations and find out the causes/reasons. In turn, it enablesthe organization to be better equipped to handle and do awaywith inconsistencies. In the long run, it sustains the provision ofan effective and efficient healthcare delivery system for all.
Operational Parameters
The author has worked on more than 100 healthcare projectsin the last six years. She can be reached [email protected].
Money matters
Smita Sridharan, Principal Consultant — Consultancy Services — Hosmac, exemplifies the essence of financial
modeling in healthcare analysis.
31

Head Office
120, Udyog Bhavan, Sonawala Lane,
Goregaon East, Mumbai - 400 063, Maharashtra
Tel: +91 22 6723 7000, Fax: +91 22 2686 3465
Middle East Region
#
HOSMAC Middle East FZ LLC
PO Box 505064, DHCC, Dubai, UAE
Tel: +9714 4298345
North Region
,
1016, Galleria Tower, DLF City, Phase IV,
Gurgaon - 122 002 Haryana
Tel: +91 124 3240 677
South Region
95, Sai Dham, 4th Main HAL (2nd Stage),
Kodihalli, Bengaluru - 560 008, Karnataka
Tel: +91 80 2521 3486
East Region
,
,
5B, BB-99, VIP Park, Prafulla Kanan
Kolkatta - 700 101 West Bengal
Tel: +91 33 6455 1246
North East Region
,
Eureka Tower, 1st Floor, Near Chandmari Flyover,
Uturn, Guwahati - 781003 Assam
Tel: +91 755 2420331
HOSMAC FOUNDATION w w w . h o s m a c f o u n d a t i o n . o r g

















![Hosmac Pulse December 2010[1]](https://static.fdocuments.us/doc/165x107/577d27181a28ab4e1ea30a82/hosmac-pulse-december-20101.jpg)
