Hormone Actions and Insulin Receptors By: Netee Papneja, PGY5
55
Hormone Actions and Insulin Receptors By: Netee Papneja, PGY5 Netee Papneja PGY 5, Endocrinology
-
Upload
quamar-barker -
Category
Documents
-
view
30 -
download
0
description
Hormone Actions and Insulin Receptors By: Netee Papneja, PGY5. Netee Papneja PGY 5, Endocrinology. Objectives:. Introduction to hormones: Definition Classification Structure Synthesis and release Function Hormone receptors: Classification Brief overview of each class - PowerPoint PPT Presentation
Transcript of Hormone Actions and Insulin Receptors By: Netee Papneja, PGY5

Hormone Actions and Insulin Receptors
By: Netee Papneja, PGY5
Netee PapnejaPGY 5, Endocrinology

Objectives:• Introduction to hormones:
– Definition– Classification– Structure– Synthesis and release– Function
• Hormone receptors:– Classification– Brief overview of each class
• Insulin and insulin receptors:– General information– Mechanism of action
04/20/23 2
• What is a hormone?
– A hormone (from Greek ''ὁρμή'' - "impetus") is a chemical released by one or more cells that affects cells in other parts of the organism.
• a chemical messenger that transports a signal from one cell to another
– Only a small amount of hormone is required to alter cell metabolism
04/20/23 3

• Endocrine hormones - secreted (released) directly into the bloodstream
• Exocrine hormones - secreted directly into a duct, and from the duct they either flow into the bloodstream or they flow from cell to cell by diffusion in a process known as paracrine signalling.

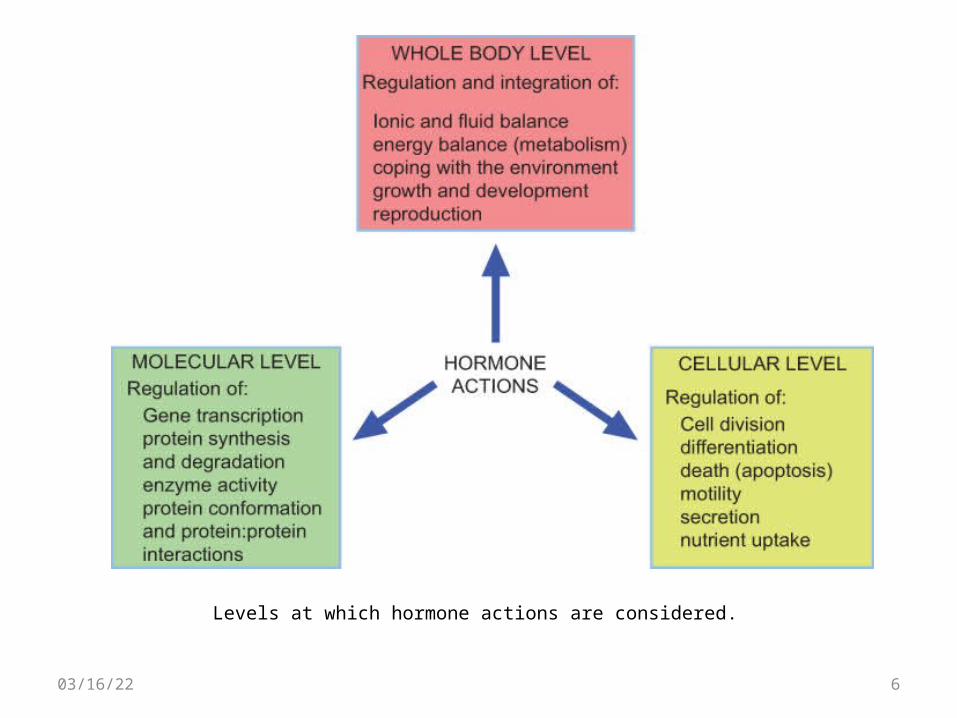
Levels at which hormone actions are considered.
04/20/23 6

Classification by Structure
04/20/23 7

04/20/23 8

04/20/23 9

04/20/23 10

• The physiologic functions of hormones can be divided into three general areas:
1. Growth and differentiation:• Multiple hormones and nutritional factors
2. Reproduction:• The stages of reproduction include:
1. Sex determination during fetal development
2. Sexual maturation during puberty
3. Conception, pregnancy, lactation, and child-rearing
4. Cessation of reproductive capability at menopause
04/20/23 11

3. Maintenance of homeostasis• T4 controls about 25% of basal metabolism in most
tissues
• Cortisol exerts a permissive action for many hormones in addition to its own direct effects
• PTH regulates calcium and phosphorus levels
• Vasopressin regulates serum osmolality by controlling renal free water clearance
• Mineralocorticoids control vascular volume and serum electrolyte (Na+, K+) concentrations
• Insulin maintains euglycemia in the fed and fasted states
04/20/23 12
Communication system
• Optimal coordination and communication between organ systems is required to sustain homeostasis
• A complete communication system needs: – A cell that produces the signaling molecule (the
hormone, which is sometimes called the ligand)– A target cell with a specific receptor that can bind
the signal with high affinity and produce a desired effect.
04/20/23 13
• Receptors:– molecules that hormones bind to in order to exert
their effects
• Characteristics of receptors:– Proteins or glycoproteins– Able to distinguish their hormone from other
molecules that may have very similar structures
Characteristics of receptors:
– Bind to the hormone, or ligand, even at exceedingly low concentrations
– Undergo a conformational change when bound to the hormone
– Catalyze biochemical events or transmit changes in molecular conformation to adjacent molecules that produce a biochemical change
04/20/23 15

General Classification:
• Membrane receptors
• Nuclear receptors
04/20/23 16
Nuclear Receptors • Change the degree of gene expression• Can be located in the cytoplasm or in the nucleus
• Steroid receptors– In the cytoplasm– steroid diffuses through the membrane and binds to its receptor – It then dissociates from proteins and translocates to the nucleus, where
another steroid-receptor complex binds to it to form a dimer of steroid-receptor complexes, which exposes the DNA-binding site and, at this point, becomes active.
• Thyroid hormone receptors– Are already in the nucleus and bound to the target genes– There are inactivating thyroid binding proteins that dissociate once the
hormone has bound, allowing the hormone-receptor complexes to cause changes in gene expression

Membrane Receptors
• Activated through the binding of peptide hormones and catecholamines
• The ligand (hormone), or first messenger, binds to its receptor and causes activation of a second messenger system, which is mediated with intracellular signalling molecules (through phosphorylation reactions)

• Membrane receptors can be classified according to the molecular mechanisms by which they accomplish their signaling function:
1. Ligand-gated ion channels (e.g., nicotinic acetylcholine receptor)
2. Receptor tyrosine kinases (e.g., receptors for insulin and insulin-like growth factor I [IGF-I])
3. Receptor serine/threonine kinases (e.g., receptors for activins and inhibins)
1. G protein–coupled receptors (e.g., receptors for adrenergic agents, muscarinic cholinergic agents, glycoprotein hormones, glucagon, and parathyroid hormone)
2. Cytokine receptors (e.g., receptors for growth hormone, prolactin, and leptin)
04/20/23 19

04/20/23 20

• Ligand-gated ion channels
• Receptor tyrosine kinases
• Receptor serine/threonine kinases
• Receptor guanylate cyclase
➙ Bifunctional molecules that can bind hormone as well as serve as effectors by functioning either as ion channels or as enzymes.
04/20/23 21

• G protein–coupled receptors
• Cytokine receptors
➙Have the ability to bind the hormone but must recruit a separate molecule to catalyze the effector function.
04/20/23 22

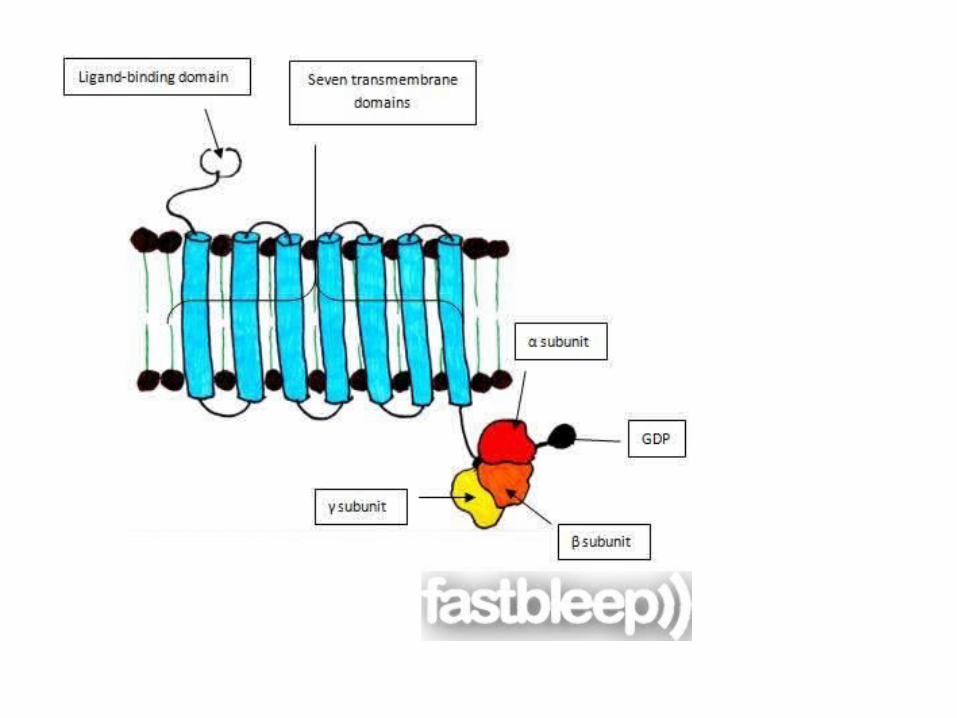
G protein-coupled receptors • Span the membrane seven times, with the receptor
extracellularly and regions that activate a G protein intracellularly
• Three components: α, β and γ subunits • Ligand binding to the receptor results in a conformational
change that causes the α subunit to exchange a GDP molecule for that of a GTP molecule
• This causes the GTP-bound α subunit to dissociate from the βγ complex and act at an effector (usually an enzyme, but sometimes an ion channel or other protein).
• The α subunit hydrolyses GTP back to GDP to terminate the process.

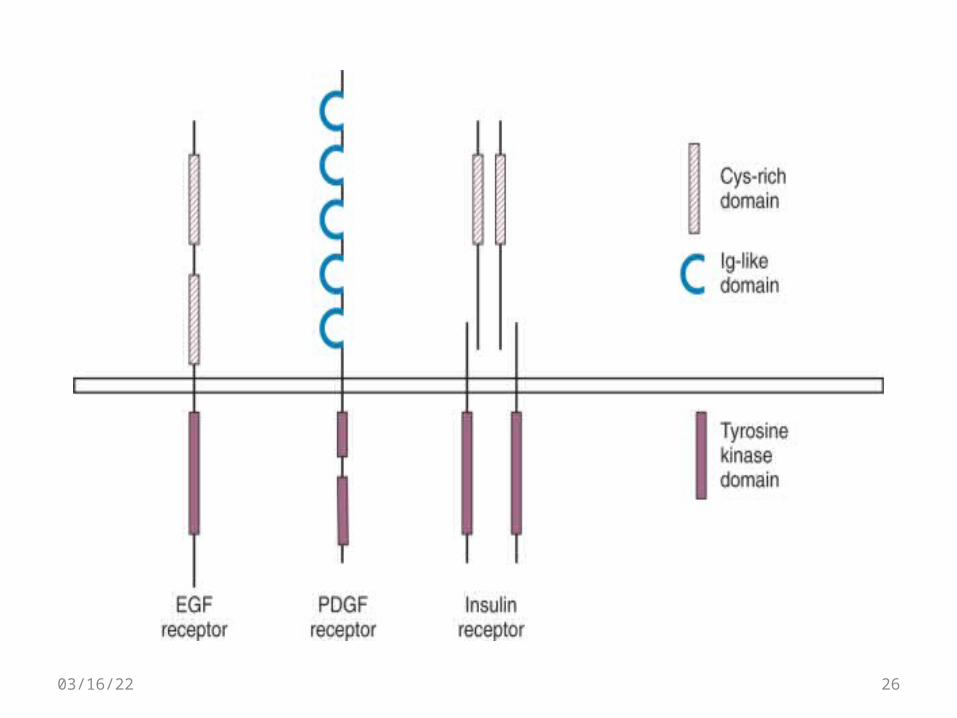
Receptor Tyrosine Kinases:
• Have several structural features in common:
– an extracellular domain containing the ligand-binding site
– a single transmembrane domain
– an intracellular portion that includes the tyrosine kinase catalytic domain
04/20/23 25
04/20/23 26
• 100 receptor tyrosine kinases sequenced in the human genome
• Classified into 16 subfamilies based on the extracellular domain
• Mediate the actions of many ligands:– insulin,
– epidermal growth factor (EGF),
– platelet-derived growth factor (PDGF)
– vascular endothelial cell–derived growth factor.
04/20/23 27

Receptor activation: Role of Dimerization:
• Plays a central role in the activation of most receptor tyrosine kinases.
• The molecular mechanisms differ from receptor to receptor
04/20/23 28

• Examples of mechanisms of dimerization:
– Ligand has two subunits, each binds to a receptor (dimeric ligand)
– Two receptor-binding sites on a single molecule of ligand
– Pre-existing receptor dimers, undergo conformational change and become activated when bound to ligand
04/20/23 29
• After dimerization, receptor tyrosine kinases undergo conformational change in the kinase domain
• Mainly due to autophosphorylation of the “activation loop”
• Ultimately leads to activation of the receptor to phosphorylate other proteins
04/20/23 30

Termination of signal:
– Receptor-Mediated Endocytosis:
– Protein Tyrosine Phosphatases:
– Serine/Threonine Kinases
04/20/23 31

Receptors that Signal through Associated Tyrosine Kinases
• Members of the cytokine family of receptors resemble receptor tyrosine kinases in their mechanism of action
• Instead of the tyrosine kinase being intrinsic to the receptor, enzymatic activity resides in a protein that associates with the cytokine receptor.
• Ligand binding to the cytokine receptor activates the associated kinase.
04/20/23 32

Insulin: Receptors and action

Insulin Physiology
• Insulin – key regulator of glucose, protein, fat homeostasis
• 51-amio acid anabolic hormone made of 2 peptide chains connected by 2 disulfide chains

• Pre-proinsulin(PPI) synthesized from the Insulin gene
•The signal sequence is removedand proinsulin is further processed in the Golgi apparatus, where the C-peptide is removed and packaged with insulin for secretion
• PPI into the endoplasmic reticulum by the signal sequence, where it folds into a proper conformation that is stabilized by three disulfide bonds (SS)
Insulin Biosynthesis

Proinsulin• A single chain of 86 amino acids
• Small amount escapes from pancreas uncleaved and circulates in serum
• Metabolized in kidney instead of liver therefore 3 to 4-times the half life of insulin
• 12-20% of circulating “insulin” that we measure in the fasting state
• Has 7-8% of insulin’s biologic activity
C-Peptide
• 31 amino acid peptide• No known biologic activity• Excreted by kidney• Half-life 3-4-times that of insulin

Insulin• Processed and secreted by pancreatic B cells
of the islets of Langerhans
• Transported via portal circulation to hepatic vein to the liver– 50% of insulin is removed by a single pass through
the liver, remainder of it by kidneys
• Circulatory half-life of 3-5 minutes
Insulin Secretion
• Pancreas secretes about 30 units per day
• Release of insulin occurs at a basal rate and in short lived large bursts with glucose load
• Basal insulin secretion occurs during fasting/resting states to inhibit hepatic glycogenolysis, ketogenesis, and gluconeogenesis– 40% of total insulin output/24h
Insulin Secretion
• Bolus insulin occurs when plasma glucose levels are >4.4-5.6mmol/L after meals
• Bolus insulin released in 2 phases– First phase: initial transient surge– Second phase: prolonged steady increase
• Increased levels start 8-10 minutes after eating and peaks in 30-45 minutes
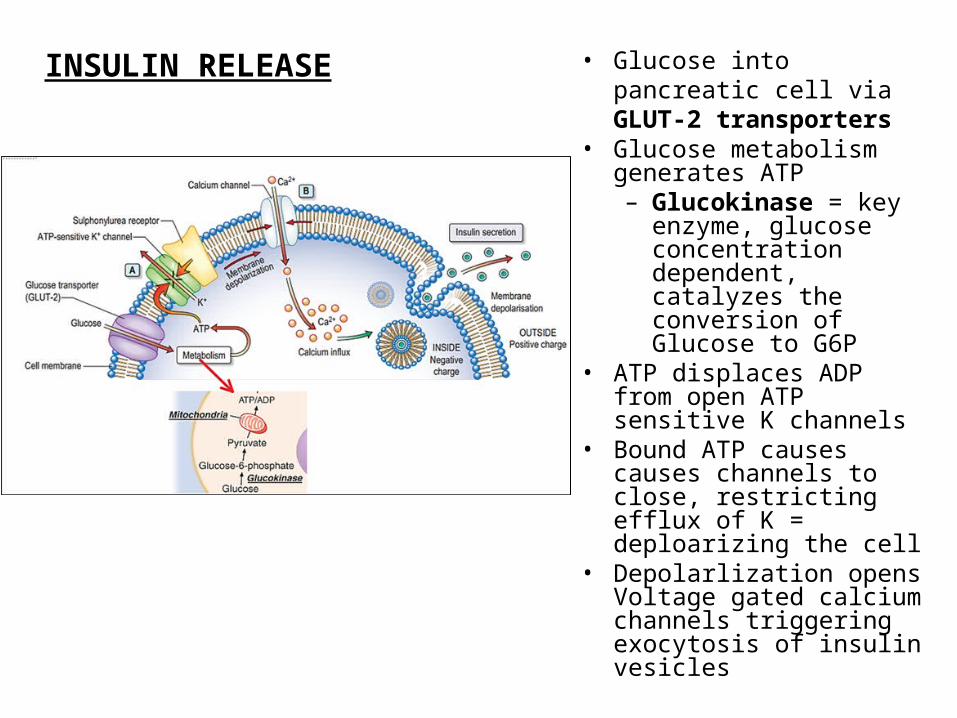
• Glucose into pancreatic cell via GLUT-2 transporters
• Glucose metabolism generates ATP– Glucokinase = key
enzyme, glucose concentration dependent, catalyzes the conversion of Glucose to G6P
• ATP displaces ADP from open ATP sensitive K channels
• Bound ATP causes causes channels to close, restricting efflux of K = deploarizing the cell
• Depolarlization opens Voltage gated calcium channels triggering exocytosis of insulin vesicles
INSULIN RELEASE

Insulin action on a target cell

Insulin receptor • Most body cells (hepatocytes, fat, muscle
cells) have insulin receptors
• Composed of:– Two alpha subunits and two beta
subunits linked by disulfide bonds
• It is a transmembrane receptor that is activated by insulin, IGF-1, IGF-II, and belongs to class of tyrosin kinase receptors
– a kinase is a type of enzyme that transfers phosphate groups from high-energy donor molecules, such as ATP to specific target molecules phosphorylation.
– Kinase enzymes that specifically phosphorylate tyrosine amino acids are termed tyrosine kinases.

• Mitogenic functions: mediated via the mitogen-activated protein kinase (MAP kinase) pathway.
• Metabolic actions: mediatedby phosphatidylinositol-3-kinase (PI-3K) pathway

• PI-3K-signaling pathway is responsible for:
– Translocation of GLUT-4 containing vesicles to the surface
– Increasing GLUT-4 density on the membrane and rate of glucose influx
– Promoting glycogen synthesis via activation of glycogen synthase
– Promoting protein synthesis and lipogenesis, while inhibiting lipolysis

Insulin Receptors • Insulin binds to α subunits of insulin
receptor tyrosine kinase and causes shape changes communicated to the intracellular β subunits and cause it to bind ATP and autophosphorylate
• This then allows other intracellular proteins to bind to the intracellular domain of the receptor, and become phosphorylated and generate their actions.– A cascade of phosphorylations and
shape/activity changes START

• Signal transduction pathways:– IRS (insulin receptor
substrates) binding sites for PI3K (phosphatidylinositol-3-kinase) activates Akt/PKB (Protein Kinase B) and the aPKC (Protein Kinase C) cascades
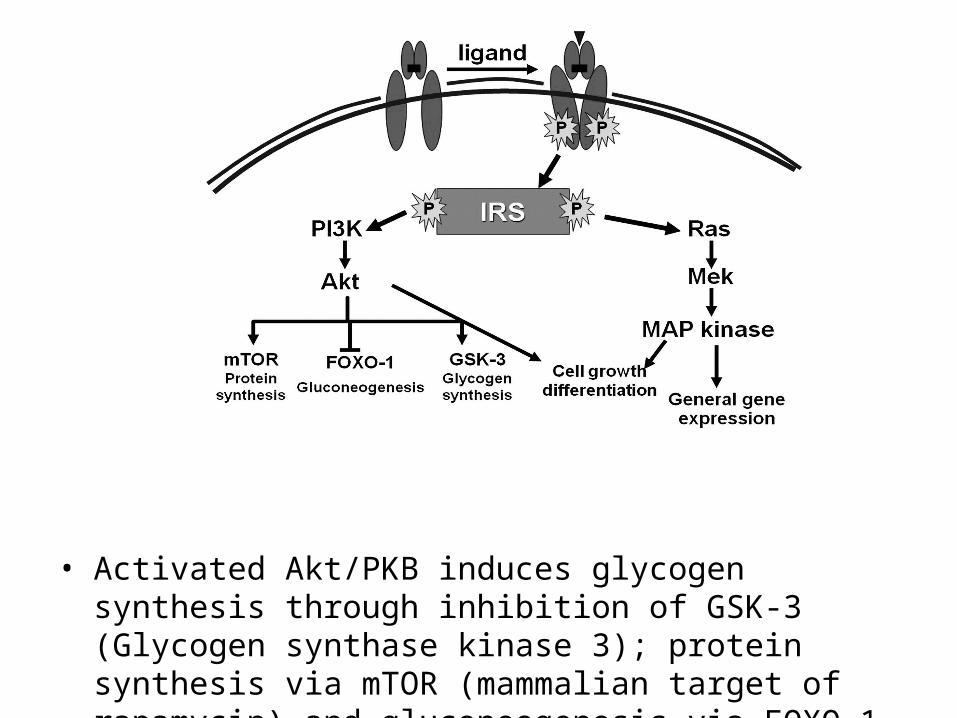
• Activated Akt/PKB induces glycogen synthesis through inhibition of GSK-3 (Glycogen synthase kinase 3); protein synthesis via mTOR (mammalian target of rapamycin) and gluconeogenesis via FOXO-1 (Forkhead box protein O1)

Glucose uptake… • Insulin stimulates glucose
uptake via translocation of GLUT4 vesicles to the plasma membrane
• Activation of PKB and PKC-λ lead to translocation of GLUT4 molecules to the cell surface resulting in increased glucose uptake

• Insulin signaling also has growth and mitogenic effects, which are mostly mediated by the Akt cascade as well as by activation of the Ras/ MAPK pathway
Other actions of Insulin …
• insulin signaling inhibits gluconeogenesis in the liver, through disruption of CREB/CBP/Torc2 binding
• promotes fatty acid synthesis through activation of SREBP-1C, USF1, and LXR
• A negative feedback signal from Akt/PKB, PKCζ, p70 S6K, and the MAPK cascades results in serine phosphorylation and inactivation of IRS signaling
Regulators of Insulin Release • Stimulates release:
– glucose, vagal stimulation, sulfoylureas, meglitinides
• Amplifies release:– GLP-1, GIP, cholecystokinin, gastrin, secretin,
beta-adrenergic, arginine, GLP-1 agonists• Inhibits release:
– Catecholamines, somatostatin, diazoxide, phenytoin, vinblastine, colchicine

Insulin receptor• Down-regulation
– obesity, high carb intake, too much exogenous insulin
• Up-regulation– exercise, fasting
• Cortisol– decreased insulin binding– exact mechanism of insulin resistance unknown
• Post-receptor defects– cause of most clinically relevant insulin resistance
References:
• Companion site for Basic Medical Endocrinology, 4th Edition, by Dr. Goodman
• Basic Medical Endocrinology, Dr Goodman• Williams Textbook of Endocrinology • Harrison’s Textbook of Medicine
• Henderson, J. J Endocrinol 2005;184: 5-10
• Nussey SS & Whitehead SA. Endocrinology An Integrated Approach 2001
• Melmed S & Conn PM (eds) Endocrinology: Basic & Clinical Principles 2nd Edition 2005
04/20/23 67
THANK YOU