Homograft Aortic Valve Replacement—The Experience of One Unit
7
ORIGINAL ARTICLE Original Article Homograft Aortic Valve Replacement—The Experience of One Unit Gautam Ganguly, MS, Zakir A. Akhunji, FRCS(I), William M.L. Neethling, PhD(Cardiothoracic) 1 and Andrew J. Hodge, FRACS(Cardiothoracic) ∗ Department of Cardiothoracic Surgery, Fremantle Heart Institute, Fremantle Hospital, P.O. Box 480, Fremantle, WA 6959, Australia Background. Homograft valves offer advantages including avoidance of anticoagulation and less susceptibility to in- fection especially in the setting of endocarditis. However, there is concern about their durability and possible accelerated degeneration particularly in cases of second time replacement with homografts. Aim. This study aimed to evaluate the pattern of homograft failure and the quality of life in patients after homograft implantation. Methods. Between 1990 and 1998, 58 patients underwent aortic valve replacement with a homograft (aortic homograft = 47, pulmonary homograft = 11). Evaluation was based on clinical and echocardiographic examination, patient ques- tionnaires and explanted valve pathology. Survival and freedom from cardiac related death were expressed by actuarial methods. Results. Follow up ranged from 1 to 10 years (mean 5.5 years). Analysis of questionnaires revealed 60% of respondents to be in good performance status and 20% in moderate and 20% in poor performance status groups. Eleven patients (18.9%) required subsequent redo valve replacement after initial homograft insertion (pulmonary = 6, aortic = 5) due to either valve dehiscence (n = 4) or valve degeneration (n = 7). The mean interval of re-replacement was 5.4 years. Conclusions. Pulmonary homografts have a high failure rate in the aortic position. Overall subjective and clinical im- provement after surgery is less than expected for a “physiological” device. In the setting of low availability of homografts the use of off-the-shelf devices such as stentless xenografts may be preferable in most cardiac surgical units in the current era. (Heart Lung and Circulation 2004;13:161–167) © 2004 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New Zealand. Published by Elsevier Inc. All rights reserved. Keywords. Homograft; Valve replacement; Quality of life Introduction A ortic valve replacement (AVR) with cryopreserved hu- man aortic or pulmonary valves (homografts) is an attractive alternative to the implantation of mechanical or bioprosthetic valves as anticoagulation can be avoided and durability is said to be at least as good as, or better than, xenograft bioprostheses. 1–4,30 The first orthotopic insertion of a homograft was performed by Donald Ross in 1962. Brian Barrett-Boyes performed a similar procedure in London the same year, reported in 1964. 5 At first the homografts were harvested aseptically and implanted within a few days. This was soon replaced by unsterile collection with subsequent sterilisation by ethy- lene oxide, betapropiolactone or irradiation. The homo- graft was then stored in Hank’s solution at 4 ◦ C or by freeze drying. This technique had a high incidence of cusp ∗ Corresponding author. Present address: Cardiothoracic Surgical Unit, Ward B8N, Fremantle Hospital, Alma Street, Fremantle, WA 6160, Australia. Tel.: +61-8-9431-3337; fax: +61-8-9431-2915. E-mail address: [email protected] (A.J. Hodge). #1 Co-corresponding author. rupture. 6 In 1968 antibiotic sterilisation was introduced at Green Lane Hospital, New Zealand by Barratt-Boyes. 7 Cryopreservation was introduced in 1975 by O’Brien. 8 The use of the homograft was expanded by Yacoub and by Ross for use in combined aortic valve and ascending aortic replacement. 5 Donald Ross performed the first AVR using the autograft pulmonary valve in 1967. 5,9,10 This study aimed to evaluate the pattern of homograft failure and the quality of life in patients after homo- graft implantation in a small Unit largely typical of the Units in Australasia. Evaluation was based on clinical and echocardiographic examination, analysis of data from pa- tient questionnaires and explanted valve histopathology. Materials and Methods Patients Between 1990 and 1998, 58 patients underwent aortic valve replacement with a homograft largely by one surgeon (A.J.H.). Patients were selected on the basis of general suitability for bioprosthetic replacement and none were excluded on the grounds of risk or co-morbidity. A fre- © 2004 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New Zealand. Published by Elsevier Inc. All rights reserved. 1443-9506/04/$30.00 doi:10.1016/j.hlc.2004.02.004
-
Upload
gautam-ganguly -
Category
Documents
-
view
213 -
download
1
Transcript of Homograft Aortic Valve Replacement—The Experience of One Unit

ORIG
INALARTICLE
Original Article
Homograft Aortic Valve Replacement—TheExperience of One Unit
Gautam Ganguly, MS, Zakir A. Akhunji, FRCS(I), William M.L. Neethling,PhD(Cardiothoracic)1 and Andrew J. Hodge, FRACS(Cardiothoracic)∗
Department of Cardiothoracic Surgery, Fremantle Heart Institute, Fremantle Hospital, P.O. Box 480, Fremantle, WA 6959, Australia
Background. Homograft valves offer advantages including avoidance of anticoagulation and less susceptibility to in-fection especially in the setting of endocarditis. However, there is concern about their durability and possible accelerateddegeneration particularly in cases of second time replacement with homografts.
Aim. This study aimed to evaluate the pattern of homograft failure and the quality of life in patients after homograftimplantation.
Methods. Between 1990 and 1998, 58 patients underwent aortic valve replacement with a homograft (aortic homograft= 47, pulmonary homograft = 11). Evaluation was based on clinical and echocardiographic examination, patient ques-tionnaires and explanted valve pathology. Survival and freedom from cardiac related death were expressed by actuarialmethods.
Results. Follow up ranged from 1 to 10 years (mean 5.5 years). Analysis of questionnaires revealed 60% of respondentsto be in good performance status and 20% in moderate and 20% in poor performance status groups. Eleven patients(18.9%) required subsequent redo valve replacement after initial homograft insertion (pulmonary = 6, aortic = 5) due toeither valve dehiscence (n = 4) or valve degeneration (n = 7). The mean interval of re-replacement was 5.4 years.
Conclusions. Pulmonary homografts have a high failure rate in the aortic position. Overall subjective and clinical im-provement after surgery is less than expected for a “physiological” device. In the setting of low availability of homograftsthe use of off-the-shelf devices such as stentless xenograftsmay be preferable inmost cardiac surgical units in the currentera.
(Heart Lung and Circulation 2004;13:161–167)© 2004 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New
Zealand. Published by Elsevier Inc. All rights reserved.
Keywords. Homograft; Valve replacement; Quality of life
Introduction
Aorticvalve replacement (AVR)with cryopreservedhu-man aortic or pulmonary valves (homografts) is an
attractive alternative to the implantation of mechanical orbioprosthetic valves as anticoagulation canbeavoidedanddurability is said to be at least as good as, or better than,xenograft bioprostheses.1–4,30
The first orthotopic insertion of a homograft wasperformed by Donald Ross in 1962. Brian Barrett-Boyesperformed a similar procedure in London the same year,reported in 1964.5
At first the homografts were harvested aseptically andimplanted within a few days. This was soon replaced byunsterile collection with subsequent sterilisation by ethy-lene oxide, betapropiolactone or irradiation. The homo-graft was then stored in Hank’s solution at 4 ◦C or byfreeze drying. This technique had a high incidence of cusp
∗Correspondingauthor.Present address:CardiothoracicSurgicalUnit,WardB8N, FremantleHospital, AlmaStreet, Fremantle,WA6160, Australia. Tel.: +61-8-9431-3337; fax: +61-8-9431-2915.E-mail address: [email protected] (A.J. Hodge).# 1 Co-corresponding author.
rupture.6 In 1968 antibiotic sterilisation was introducedat Green Lane Hospital, New Zealand by Barratt-Boyes.7
Cryopreservationwas introduced in 1975 byO’Brien.8 Theuse of the homograft was expanded by Yacoub and byRoss for use in combined aortic valve and ascending aorticreplacement.5 Donald Ross performed the first AVR usingthe autograft pulmonary valve in 1967.5,9,10
This study aimed to evaluate the pattern of homograftfailure and the quality of life in patients after homo-graft implantation in a small Unit largely typical of theUnits in Australasia. Evaluation was based on clinical andechocardiographic examination, analysis of data from pa-tient questionnaires and explanted valve histopathology.
Materials and Methods
PatientsBetween 1990 and 1998, 58 patients underwent aortic valvereplacement with a homograft largely by one surgeon(A.J.H.). Patients were selected on the basis of generalsuitability for bioprosthetic replacement and none wereexcluded on the grounds of risk or co-morbidity. A fre-
© 2004 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society ofAustralia and New Zealand. Published by Elsevier Inc. All rights reserved.
1443-9506/04/$30.00doi:10.1016/j.hlc.2004.02.004

ORIG
INALARTICLE
162 Ganguly et al. Heart Lung and CirculationHomograft aortic valve replacement—the experience of one unit 2004;13:161–167
Table 1. Pre-operative Valvular Pathology in Patients(n = 44) for Primary Replacement
Valvular Pathology Number (% of total)
Calcified aortic stenosis (AS) 24 (41.3)Aortic regurgitation (AR) 5 (8.6)AS + AR 11 (18.9)Endocarditis 4 (6.8)
Table 2. Valvular Pathology in Patients (n = 14) for RedoAVR with Homograft (Previous Bioprosthesis)
Prosthetic Pathology Number (% of total)
Endocarditis 4 (6.8)Calcific degeneration 6 (10.3)Valve dehiscence withtransprosthetic orperiprosthetic leak
5 (8.6)
quent cause of exclusion was unavailability of a suitablysized homograft. Forty were male and 18 were female.They ranged in age from 22 to 88 years with a mean of63 years. Twenty-seven patients (46.5%) were older than65 years at the time of surgery. Forty-four patients under-went primary homograft replacement (75.8%). The indi-cation for this replacement is shown in Table 1. Fourteenpatients (24.1%) underwent redo AVR with a homograftafter a previous AVR with a tissue valve. The indicationfor redo AVR is shown in Table 2. Forty-seven patientsreceived an aortic homograft and 11 patients received apulmonary homograft into the aortic position. Eleven pa-tients (18.9%) in this series required subsequent redoAVRafter homograft insertion due to either valve dehiscence(4 cases) or valve degeneration (7 cases). Of these 11 pa-tients, 6 had received a pulmonary homograft and 5 hadreceived an aortic homograft at the initial operation. Themean interval of re-replacement after the first homograftreplacementwas 5.4 years and the types of valve used dur-ing this re-replacement are shown in Table 3.Homograftswere inserted freehand in thesub-coronary
position in 48 patients (82.7%) and aortic root replace-ment was done in 10 patients (17.3%). Concomitant pro-cedures were performed in 14 patients (24.1%), 12 under-going coronary artery bypass procedures and 2 undergo-ing mitral valve annuloplasty. Pre-operative left ventric-ular function was assessed by echocardiography and/orLV angiogram. Fifteen (25.8%) patients had mild to mod-erate impairment of left ventricular function and 3 (5.2%)patients had severe systolic dysfunction. The remainder(69%) had normal LV function.
Table 3. Types of Valves (n = 11) Used for Re-replacementAfter Homograft AVR
Types of Valve Number of Patients
Mechanical (St Jude) 5Stented pericardial 2Stentless porcine (Toronto) 2Homograft (aortic) 2
Surgical TechniqueAll patients were operated on using cardiopulmonarybypass (CPB) with core cooling to 28–32 ◦C. Myocardialpreservation was achieved by using intermittent coldblood cardioplegia at 4 ◦C infused antegrade throughthe aortic root, retrograde through the coronary sinus,or directly into the coronary ostia because of aorticregurgitation or when the root was open. The myocardialtemperature was reduced to less than 12 ◦C in all coro-nary territories. Cardioplegic infusion was repeated every20–30min. The left ventricle was vented through the rightsuperior pulmonary vein and across the mitral valve in allcases.For sub-coronary implantation, the native aortic valve
was exposed through a curved aortotomy beginning justabove the shoulder of the right ventricle, extended trans-versely to the left, and towards the centre of the non-coronary sinus without transgressing the sino-tubularjunction, on the right. This gavegoodexposureof theaorticvalve to allow thorough excision/explantation of the valveand annular debridementwithout disturbing the integrityof the aortic root. The homograft valves were inserted ei-ther in the sub-coronary position or as an aortic root re-placement with re-implantation of the coronary buttons.The decision as to whether to perform root replacementdepended on the configuration of the root, size of the aor-tic sinuses, donor/recipient configuration mismatch, andthe need to debride abscess cavities in patients with en-docarditis.
Homograft PreparationHomografts were collected, antibiotic sterilised, cryopre-served and thawed according to the protocol initiated byO’Brien and co-workers.26,27
Follow UpThe duration of follow up ranged from 1 to 10 years with amean of 5.5 years and a cumulative follow up time of 442patient years. All patients were followed up at 1 month, 3months, 6 months and then annually. At follow-up apartfromclinical examination, a chestX-ray, ECGandechocar-diogram were done for all patients. A questionnaire con-cerning physical status and life style was sent in April 2000and resulted in a 93% response rate (40 of 43 survivors).The study was censored in May 2000. Evaluation of thequality of life and physical activity was made on the basisof clinical examination and data from the questionnaire.Thequestionnaireswereprepared inaccordance to theSF-36 Health Survey Scoring Manual of Medical OutcomesTrust, Boston.11 The questionnaire, apart from personaldata, also contained questions concerning quality of lifebefore and after surgery and level of exercise tolerance.Based on their score the patients were divided into threegroups: poor, moderate and good performance status.
Statistical MethodsThe estimated probability of survival and freedomfrom cardiac related death were expressed by actuarialmethods.12 Outcome after surgery was calculated accord-

ORIG
INALARTICLE
Heart Lung and Circulation Ganguly et al. 1632004;13:161–167 Homograft aortic valve replacement—the experience of one unit
ing to a standard exponential model based on the averagecomplication rate and survival time.
Results
MortalityThere were a total of nine (15.5%) cardiac deaths and six(10.3%) non-cardiac deaths over the study period of 10years. Of the cardiac related deaths, five (8.6% of the to-tal group) were early (within 60 days). Two patients couldnot be weaned from CPB and died on the table. Anotherpatient was weaned off CPB with the help of a right ven-tricular assist device (RVAD) but died in ICU after 2 dayson RVAD support. The fourth patient died after 12 days inthe ward following ventricular arrhythmia. The fifth pa-tient died after 4 weeks due to continuing endocarditisand interstitial pneumonia. The risk factors found to bepredictors of early death are shown in Table 6. Risk strat-ification analysis was done on the basis of the Parsonnetscoring system.13 The average Parsonnet score in this pa-tient group was 14 resulting in a predicted operative mor-tality of approximately 14%.Theoperativemortality in thisseries was 8.6% at 60 days.During the period of followup therewere 10 late deaths.
The causes of these late deaths are shown in Table 4. Over-all actuarial survival was 70% at 2 years, 55% at 5 years and50% at 10 years (Fig. 1).
Homograft FailureHomograft failure was defined as need for re-operationdue to either degenerative valve failure, valve dehiscenceor endocarditis. Degenerative valve failure was definedas moderate or severe valve malfunction due to calcifica-tion or cusp perforation diagnosed at echocardiography.Valve dehiscence was defined as actual anatomical sep-
Figure 1. Postoperative survival for cardiac related (�) and all (�) deaths, represented as an actuarial curve.
Table 4. Causes of Late Deaths in Homograft AVR Recipients
Cause of Death Interval AfterAVR (Years)
Non cardiac1. Seizure 92. Brain tumour 63. Carcinoma colon 54. Cerebrovascular accident 55. Brain tumour 46. Carcinoma prostate 3
Cardiac1. Valve dysfunction andcongestive heart failure
6
2. Congestive heart failure 23. Congestive heart failureand arrhythmia
2
4. Unknown 5
aration of the homograft tissue from the native annulusor native aortic wall causing periprosthetic leak. Elevenpatients (18.9%) required reoperation due to homograftfailure. The linearised failure rate for homograft valvesin this series was 2.48% per year. Expressed as an actu-arial curve (Fig. 2), at 10 years no valve had escaped avalve-related complication. The interval between initialhomograft AVR and re-operation ranged from 1 to 9 yearswith a mean of 5.4 years. Valve degeneration occurred in7 of the 53 patients discharged from hospital (13.2%) andvalve dehiscence occurred in 4 of the 53 patients (7.5%).Six pulmonary homografts needed re-operation for de-generation (n = 4) or dehiscence (n = 2) and five aortichomografts needed re-operation for degeneration (n = 3)or dehiscence (n = 2). There were no reoperations for en-docarditis. One patient required heart transplantation 8years after homograft replacement. In this case when ex-amined histologically after explant, both the homograft

ORIG
INALARTICLE
164 Ganguly et al. Heart Lung and CirculationHomograft aortic valve replacement—the experience of one unit 2004;13:161–167
Figure 2. Ten year prosthetic failure free rate (includes all cardiac-related deaths and complications), expressed as a percentage and represented asan actuarial curve after homograft aortic valve replacement.
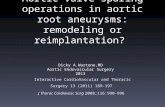
aortic wall (Fig. 3) and the valve leaflets (Fig. 4) had exten-sive areas of acellular non-viable tissue. The results of his-tology on the remaining explanted valves were not readilyavailable.
MorbidityFourteenpatients (24.1%)hadvariouspost-operative com-plications including low cardiac output, resternotomy forbleeding, permanent neurological deficit, renal failure,etc. as shown in Table 5. The patient who required RVADalso required intra-aortic balloon counter-pulsation anddialysis.
Figure 3. Representative electron micrograph of an aortic wall section of an explanted aortic homograft, showing non-viable acellular material(black arrows) in the media (magnification 6000×).
Quality of LifeAnalysis of questionnaires revealed 60% (24patients) to bein goodperformance status and 20% (8 patients) inmoder-ate and 20% in poor performance status groups. Three pa-tients in themoderate performance group and one patientin the poor performance group attributed their physicallimitations to causes other than cardiac-knee replacement(2 patients), rheumatoid arthritis (1 patient) and demen-tia (1 patient). Clinical assessment of NYHA functionalclass preoperatively and at the longest postoperative re-view recorded NYHA I 6.6% versus 30%, NYHA II 33.3%versus 45%, NYHA III 50% versus 25% and NYHA IV 10%versus 0%.

ORIG
INALARTICLE
Heart Lung and Circulation Ganguly et al. 1652004;13:161–167 Homograft aortic valve replacement—the experience of one unit
Figure 4. Representative electron micrograph of the aortic valve leaflet of an explanted aortic homograft, showing damaged collagen fibers (blackarrows) in the spongiosa. The tissue is acellular (magnification 6000×).
Table 5. Post-operative Complications Following HomograftAVR
Complication Number (% of total)
IABP 3 (5)RVAD 1 (1.6)Dialysis 2 (3.3)Resternotomy 3 (5)Septicaemia 2 (3.3)Stroke 2 (3.3)Complete heart block 1 (1.6)
Discussion
Aortic valve replacement with cryopreserved homograftshas well established advantages in avoiding anticoagula-tion and has less susceptibility to infection.1 Various au-thors in the past have indicated good surgical outcomeand good early and long term survival.14–16 Podolec etal. compared quality of life after homograft and mechan-ical prosthetic valve implantation and did not find anysignificant difference in outcome.17 Analysis of the pa-tient questionnaire in our series suggests only 74% ofpatients improved their quality of life and only 70% ofpatients actually had improvement in NYHA class aftersurgery.The findings of 18.9% incidence of homograft failure
within amean interval of 5.4 years remains amatter of con-cern regarding the durability of these prostheses. The dif-ference in re-operation rate for aortic and pulmonary ho-mografts was statistically significant as 5 out of 47 (10.6%)patients with aortic homograft and 6 out of 11 (54.5%) pa-tients with pulmonary homograft needed subsequent re-operation (P = 0.002, estimated at 95% confidence limits)and we would agree with previous work18–22 that the pul-monary homograft is not a suitable replacement in theaortic position Poor alignment of the prosthetic inflow
and of the spatial separation of the commissural postshas been cited as a reason for early prosthetic failure. Al-though there is of necessity a learning curve for the correctinsertion of these prostheses, immediate post-operativeechocardiography in this series did not detect any func-tional problem.It is attractive to think that once inside a patient, the
purpose-designed collagen/elastin matrix of the homo-graft, if devitalised prior to insertion by the processes ofcollection, preservation and storage, would repopulate it-self with autologous cells, resulting in a completely viablestructure. It is very disappointing that this had not oc-curred in our removed degenerate homografts, but hasbeen reported previously.28,29
The 8.6% incidence of early mortality was consideredhigher than other published results from high volumeUnits.23–25,30 The operative group was moderately highrisk according to the Parsonnet score and in concert withthe usual patient population that we see (average Par-sonnet score for all patients in our Unit having a pro-cedure which includes aortic valve replacement is 17).Comparison of results between groups is difficult with-out appropriate risk stratification, although available riskstratification scores for coronary artery surgery (e.g. Par-sonnet, Tu, Higgins, Tremblay) are no more than 70%predictive.Analysis of risk factors for early death indicates that age
beyond 70 years, female gender, endocarditis and asso-ciated procedures increase the risk of death significantly(Table 6).The overall mortality of 15.5% over 10 years is high, but
comparable with other published series,25 and is what wehave come to expect from these prostheses. Seven yearsago on abandoning the homograft as the prosthesis ofchoice, our groupmoved to the use of commercially avail-able stentless porcine bioprostheses and have found the

ORIG
INALARTICLE
166 Ganguly et al. Heart Lung and CirculationHomograft aortic valve replacement—the experience of one unit 2004;13:161–167
Table 6. Risk Factors Examined for Early Death
Factor Risk Odds Ratio P-values
Age ≥70 years:<70 years 3:1 0.147Sex Female:male 8:1 0.019LV dysfunction Moderate:severe 1:2 0.024Re operation 1:1 0.949Endocarditis 10:1 0.002
Type of procedureRoot replacement 1:1 0.865Subcoronary 1:1 0.503Associated procedures 9:1 0.002
clinical outcomes to be at least as good and with lowermortality and morbidity rates. There is the added benefitof easy procurement and storage.In conclusion it can be said that:
(i) Pulmonary homografts have a high failure rate in theaortic position.
(ii) The performance of aortic homografts in the aorticposition is disappointing in our hands.
(iii) Overall subjective and clinical improvement aftersurgery is less than expected for a “physiological” de-vice.
The authors would like to thank Drs. Peter Bissaker, Mark New-man and Ian Gilfillan for their contribution to this study, andSharyn Baker for her collection and collation of the patient data.
References
1. Staab ME, Nishimura RA, Dearani JA, Orszulak TA. Aorticvalve homografts in adults: a clinical perspective. Mayo ClinProc 1998;73(3):231–8.
2. DotyDB. Replacement of aortic valvewith cryopreserved aor-tic allograft: the procedure of choice for young patients. J CardSurg 1994;9(2 Suppl.):192–5.
3. Angell WW, Oury JH, Lamberti JJ, Koziol J. Durability ofthe viable aortic allograft. J Thorac Cardiovasc Surg 1989;98:48–55.
4. Kon ND, Cordell AR, Adair SM, Kitzman DW. Comparisionof results using “Freestyle” stentless porcine aortic root bio-prosthesis with cryopreserved aortic allograft. Semin ThoracCardiovasc Surg 1999;11(4 Suppl. 1):69–73.
5. Kirklin JW, Barratt-Boyes BG. Aortic valve disease. In: KirklinJW, Barratt Boyes BG, editors. Cardiac surgery, 2nd ed. NewYork, NY: Churchill-Livingstone; 1992. p. 491–557.
6. Christie GW, Barratt-Boyes BG. Identification of a failuremode of the antibiotic sterilized aortic allograft after 10years: implications for their long-term survival. J Card Surg1991;6(4):462–7.
7. Barratt-BoyesBG,RocheAHG,WhitlockRML.Sixyear reviewof the results of freehand aortic valve replacement using anantibiotic sterilized homograft valve. Circulation 1977;55:353–61.
8. O’BrienMF, Stafford EG,GardenerMA, Pohlner PG, Tesar PJ,Cochrane AD, et al. Allograft aortic valve replacement: long-term follow up. Ann Thorac Surg 1995;60(2 Suppl.):S65–70.
9. O’Brien MF. Homograft and autograft. In: Baue AE, edi-tor. Glenn’s thoracic and cardiovascular surgery. New York, NY:Churchill-Livingstone; 1996. p. 2005–42.
10. Chambers JC, Somerville J, Stone S, Ross DN. Pulmonaryautograft procedure for aortic valve disease. Circulation1997;96:2206–14.
11. Ware JE, SnowKK,KosinskiM,GendekB.SF-36Health Survey:manual and interpretation guide. Boston: The Health Institute,New England Medical Centre; 1993.
12. Lefrak EA, Starr A, editors. Cardiac valve prosthesis. New York:Appleton-Centuary-Crofts; 1979.
13. Parsonnet V, DeanD, BernsteinAD.Method of uniform strati-fication of risk for evaluating the results of surgery in acquiredadult heart disease. Circulation 1989;79(Suppl. I):3–12.
14. Bodnar E, Wain W, Martelli V, Ross DN. Long term perfor-mance of 580 homograft and autograft valves used for aor-tic valve replacement. J Thorac Cardiovasc Surg 1979;27:51–65.
15. YacoubMH,RasmiNR, Sundt TM, et al. Fourteen year experi-ence with homovital homografts for aortic valve replacement.J Thorac Cardiovasc Surg 1995;110:186–94.
16. Lund O, Chandrasekaran V, Grocott-Mason R, et al. Primaryaortic valve replacementwithallografts over twentyfiveyears:valve related andprocedure relateddeterminants of outcome.J Thorac Cardiovasc Surg 1999;117:77–90.
17. Podolec P, Pfitzner R, Wierzbicki K, et al. The quality of lifeafter aortic valve replacement with homografts or prostheticvalves. J Heart Valve Dis 1999;8(3):270–6.
18. Livi U, Abdulla AK, Parker R,Olsen EJ, RossDN. Viability andmorphology of aortic and pulmonary homografts. A compar-ative study. J Thorac Cardiovasc Surg 1987;93(5):755–60.
19. Naegele H, BohlmannM, Doring V, Kalmar P, RodigerW. Re-sults of aortic valve replacement with pulmonary and aortichomografts. J Heart Valve Dis 2000;9(2):215–20.
20. Mair R, Peschl F, Gross C, Klima U, Hinterreiter H, Brucke P.The pulmonary homograft as aortic valve substitute: 7 years’follow up. Eur J Cardiothorac Surg 1997;11:910–6.
21. Choudhary SK, Saxena A, Dubey B, Sampath AK. Pulmonaryhomograft: should it be used in the aortic position?. J ThoracCardiovasc Surg 2000;120:148–55.
22. Gerosa G, Ross DN, Brucke PE, et al. Aortic valve replace-ment with pulmonary homografts: early experience. J ThoracCardiovasc Surg 1994;107:424–37.
23. HasnatK, BirksEJ, Liddicoat J, et al. Patient outcomeandvalveperformance following a second aortic valve homograft re-placement. Circulation 1999;100(19 Suppl.):II42–7.
24. Grocott-Mason RM, Lund O, Elwida H, et al. Long term re-sults after aortic valve replacement in patients with conges-tive heart failure. Homograft vs. prosthetic valves. Eur Heart J2000;21(20):1698–707.
25. Langley SM,McGuirk SP, ChaudhryMA, Livesey SA, Ross JK,Monro JL. Twenty year follow up of aortic valve replacementwith antibiotic sterilized homografts in 200 patients. SeminThorac Cardiovasc Surg 1999;11(4 Suppl. 1):28–34.
26. O’Brien MF. Personal communication. 1989.

ORIG
INALARTICLE
Heart Lung and Circulation Ganguly et al. 1672004;13:161–167 Homograft aortic valve replacement—the experience of one unit
27. McGiffin DC, O’BrienMF, Stafford EG, GardnerMA, PohlnerPG. Long-term results of the viable cryopreserved allograftaortic valve: continuing evidence for superior valve durability.J Card Surg 1988;3(3 Suppl.):289–96.
28. Koolbergen DR, Hazekamp MG, de Heer E, Bruggemans EF,Huys HA, Dion RA, et al. The pathology of fresh and cryopre-served homograft heart valves: an analysis of forty explantedhomograft valves. J Thorac Cardiovasc Surg 2002;124(4):689–97.
29. Sadowski J, Kapelak B, Bartus K, Podolec P, Rudzinski P,Myrdko T, et al. Reoperation after fresh homograft replace-ment: 23 years experience with 655 patients. Eur J CardiothoracSurg 2003;23(6):996–1000; discussion 1000–1.
30. O’Brien MF, Harrocks S, Stafford EG, Gardner MA, PohlnerPG, Tesar PJ, et al. The homograft aortic valve: a 29-year,99.3% follow up of 1022 valve replacements. J Heart Valve Dis2001;10(3):334–44; discussion 345.