
HOMECARE CLIENT HANDBOOK - Sibley Medical Center...
45
HOMECARE CLIENT HANDBOOK
Transcript of HOMECARE CLIENT HANDBOOK - Sibley Medical Center...

HOMECARE CLIENT HANDBOOK

601 West Chandler Street, Arlington, MN 55307-2127 507-964-2271 www.sibleymedical.org
Arlington Location 601 W. Chandler Street Arlington, MN 55307-2127 PH: 507-964-2271 FAX: 507-964-5898 Gaylord Location 660 3rd Street P.O. Box 388 Gaylord, MN 55334-0388 PH: 507-237-5523 FAX: 507-237-3145 Winthrop Location 223 North Carver P.O. Box 427 Winthrop, MN 55396-0427 PH: 507-647-5318 FAX: 507-647-2118 Henderson Location 550 Main Street P.O. Box 97 Henderson, MN 56044-0097 PH: 507-248-3433 FAX: 507-248-3455
Welcome to Sibley Medical Center Home Care! Thank you for choosing Sibley Medical Center Home Care for your home health care needs. We appreciate the opportunity to be of service to you. Enclosed is your client packet containing information regarding the services provided through Sibley Medical Center and the Home Care Department. The patient bill of rights, our privacy policy, and information regarding the billing is available for your information at the end of the packet. If you have any questions on this information please ask for assistance. We look forward to a long relationship with you. For additional information, please feel free to visit our website at www.sibleymedical.org. or call our toll free number at 888-974-2539. Sincerely, SMC Home Care Staff


SIBLEY MEDICAL CENTER HOME CARE 601 WEST CHANDLER STREET
ARLINGTON, MN 55307 507-964-2271
ON-CALL INFORMATION & GUIDELINES
As a part of our services, Sibley Medical Center Home Care offers on-call nursing. In the event a problem occurs after normal office hours, on holidays or on weekends, an on-call nurse is available for assistance with problem solving. Changes in your condition may occur suddenly. Our on-call nurse is available to answer questions and provides assistance when these unforeseen changes occur. When calling our office, please refer to "Emergency Procedures" given during your first home visit. Please note:
For medical emergencies, call 911
Our on-call nurse will assist callers with their concerns and attempt to resolve the situation over the phone. In the event that the problem is not resolved, our nurse will make a home visit.
The on-call systems works as follows: Call into our office (507-964-2271) and identify the type of services you are receiving to the hospital personnel. In turn, the hospital personnel will take the information and contact the on-call nurse. This process may take up to 20 minutes. If you have not received a call within 20 minutes, please call again. After the nurse on-call assists you, they will also alert your case manager the next working day for any further appropriate follow-up.


HOME CARE
DEPARTMENT
Explanation of Home Health Aide Service
For Home Health Aide services to be covered by your insurance, the services must be ordered by your physician, be reasonable and necessary to the treatment of your illness, you must be confined to your home and you must have an ongoing need for the skilled professional services of the case manager. The Home Health Aide services must be for the purpose of providing hands-on personal care necessary to maintain your health and to facilitate the treatment of your illness. When a Home Health Aide visits you to provide a health related service, the Home Health Aide may also perform some incidental light housekeeping services that do no substantially increase the time spent on the visit. The Home Health Aide visit duration is as long as it takes to provide personal care, not to exceed 2 hours. Visit duration, time and day may vary according to you and other patient needs. Personal Care Means:
Bathing, dressing, grooming, caring for hair, nail and oral hygiene which are needed to facilitate treatment or to prevent deterioration of the patient's health.
Changing the bed linens of an incontinent patient. Shaving Skin care with lotions and/or powder deodorant application Foot Care Ear Care
Light Housekeeping Means: Changing bed linens Picking up and cleaning client's personal care area
Explanation of Home Health Aide Service For client's living alone whose medical condition prevents them from providing housekeeping for themselves, and if time allows in the visit, the following services may be provided by the aide:
Light vacuuming, light dusting, light floor mopping Reasonable amount of dishwashing Assistance with laundry Meal preparation
The Aides can not move furniture, do heavy lifting or do outdoor chores. If at any time you have questions about Home Health Aide Services you are eligible for, please discuss them with your Home Care Case Manager, or phone the Home Care Office at (507) 964-2271.


PROFESSIONAL EXTENDED SERVICES BY HOUR
Nursing Services Week Day Weekend ** R.N. $56.00/hour $59.00/hour L.P.N. $42.50/hour $45.50/hour
One (1) hour minimum charges for these services Clinical Nursing Visit $33.50/visit $35.00/visit** (Medication set up, blood draw, vital check etc)
Support Services Week Day Weekend** Home Health Aide $32.00/hour $34.00/hour
One (1) hour minimum charges for these services Homemaker $21.50
Two (2) hour minimum for Homemaker Services
** Please Note : Weekends begin at 5:00 p.m. on Friday and end at 7:00 a.m. on Monday Holidays: The following holidays will be observed only upon staff availability and billed at time and a half. Christmas Eve, New Years Eve (3:00p.m.-midnight) New Years Days, Easter day, Memorial Day, July 4th, Labor Day, Thanksgiving Day and Christmas Day.
601 West Chandler Street, Arlington, MN 553087 PH: 507-964-2271 FAX: 507-964-2941

HOME HEALTH CARE
601 W Chandler StreetArlington, MN 55307
507-964-2271888-974-2539
www.sibleymedical.org
Helping you get the care you need . . .When you want it at home.
Who will be coming to my home?You will be visited by one of the professionals on our Home Health Care Team. The team includes:
•Registered Nurses •Licensed Practical Nurses •Physical Therapists •Occupational Therapists •Home Health Aides •Homemakers •Speech Therapists
Your specific needs, as identified by your physician, will determine who comes to your home. A registered nurse will plan and supervise your Home Health Care program and will report your progress to your physician.
Back Row: Pam Fitterer, PT; Tim Theisen, PTA; Missy Weber, RN; Janice Larson, LPN; Jane Scharpe, Patient Account Services ManagerFront Row: Tamara Balder, CNA; Andrea Brinkman, Aide; Teresa Messner, RN, Home Care Director; Donna Schiro, RN; Not Pictured: Sandy Bergs, RN
Home Health Care Office Hours
7:30 a.m. - 4:00 p.m. Monday-Friday
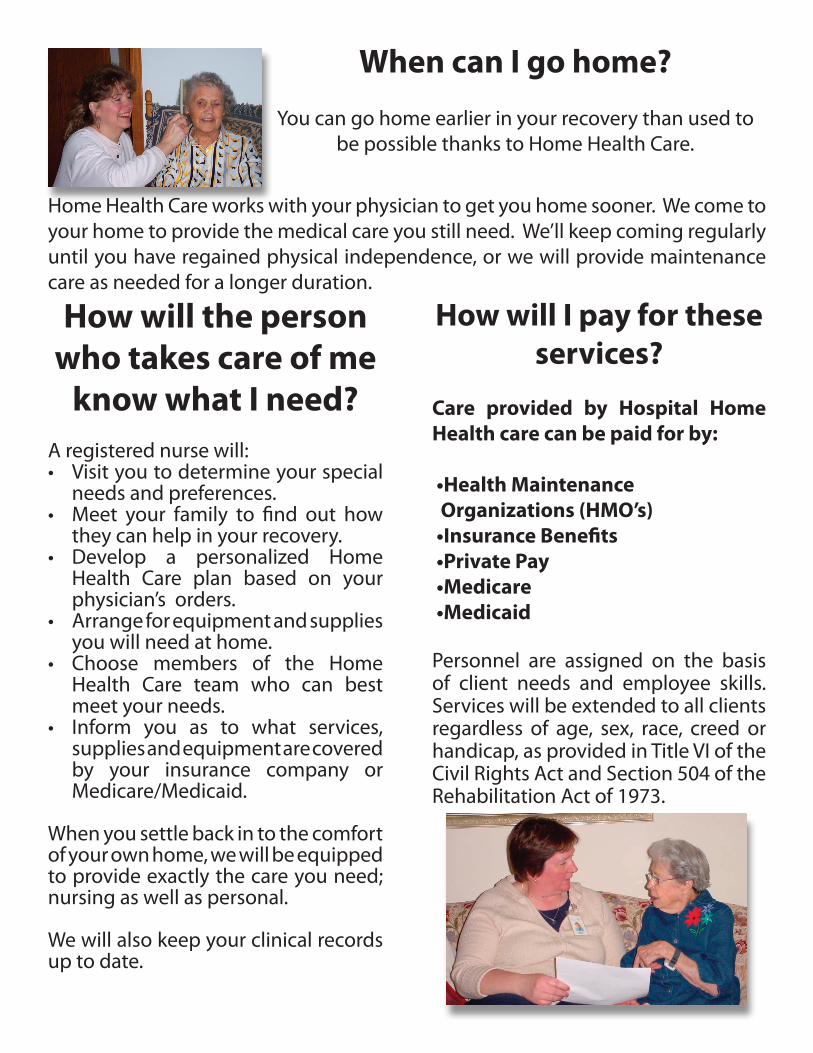
When can I go home?
You can go home earlier in your recovery than used to be possible thanks to Home Health Care.
Home Health Care works with your physician to get you home sooner. We come to your home to provide the medical care you still need. We’ll keep coming regularly until you have regained physical independence, or we will provide maintenance care as needed for a longer duration.
How will the person who takes care of me
know what I need?A registered nurse will:• Visit you to determine your special
needs and preferences.• Meet your family to find out how
they can help in your recovery.• Develop a personalized Home
Health Care plan based on your physician’s orders.
• Arrange for equipment and supplies you will need at home.
• Choose members of the Home Health Care team who can best meet your needs.
• Inform you as to what services, supplies and equipment are covered by your insurance company or Medicare/Medicaid.
When you settle back in to the comfort of your own home, we will be equipped to provide exactly the care you need; nursing as well as personal.
We will also keep your clinical records up to date.
How will I pay for these services?
Care provided by Hospital Home Health care can be paid for by:
•Health Maintenance Organizations (HMO’s) •Insurance Benefits •Private Pay •Medicare •Medicaid
Personnel are assigned on the basis of client needs and employee skills. Services will be extended to all clients regardless of age, sex, race, creed or handicap, as provided in Title VI of the Civil Rights Act and Section 504 of the Rehabilitation Act of 1973.

Meet Our Health Care Team
Troy Hanson, MDFamily Medicine
Cheryl Lindgren, CNP Family Medicine
Melanee Buckentin, CNP Family Medicine
Dean Bergersen, MDFamily Medicine
John Vener, MDFamily Medicine
Primary Care Providers
Katie Phillips, PA-CFamily Medicine
Muhamed Durakovic, MDFamily Medicine
Ehtaisham Mohammed, MDFamily Medicine
Serving the health care needs of Sibley County and
the surrounding areas.
Sibley Medical Center & Clinic601 West Chandler Street
Arlington, MN 55307-2127Ph. 507-964-2271 888-974-2539Fax 507-964-8490
Henderson Clinic505 Main Street
Henderson, MN 56044Ph. 507-248-3433Fax 507-248-3455
Gaylord Clinic315 Fourth Street
P.O. Box 388Gaylord, MN 55334Ph. 507-237-5523Fax 507-237-3145
Winthrop Clinic223 North Carver Street
P.O. Box 427Winthrop, MN 55396
Ph. 507-647-5318507-647-2118
Azra Durakovic, MDFamily Medicine
Jeannine Phillips, PA-CFamily Medicine


Meet Our Specialists
Chad Robbins, DO, FACOSGeneral Surgery
John Mark Johnson, DOOB/GYN
John Bernhardson, MDCardiology
John Bergseng, DO, FACOS
General Surgery
Special Services Available:• BoneDensityAnalysis• CardiacRehab• CardiacStressTesting• CataractSurgery• Colonoscopy• CTScans• DiabetesEducation• DietitianConsultation• DigitalMammography• DOTPhysicals• Echocardiograms• EEG-EKG-EMG• FAAPhysicals• HomeHealthCare• Hospice• Laboratory• MagneticResonanceImaging(MRI)• MastectomyOutreach• MealsonWheels• NuclearMedicine• Physical,OccupationalTherapy• SpeechTherapy• PulmonaryFunction• RespiteCare• SleepStudies• Surgery• SwingBed• Tele-Radiology• TransitionalCare• Ultrasound• VenousDoppler
Jeffrey Mair, DOOrthopedics
Michael T. Hopfenspirger, MD
Otolaryngology
Andrew Lundquist, MDPodiatry
Ravi Vaela, MDPulmonology



PRACTICING SAFETY AT HOME
Dear Patient: Each year accidents kill or disable thousands of people in their own homes. Some accidents can be avoided by adopting a few safety practices. Here is a guide to help you review home safety practices. Avoid burns and fires
Turn cooking utensil handles inward (away from the stove’s outer edge). Wear short or tight sleeves while cooking to prevent burning your clothes. Use pot holders to remove covers from hot cookware. Vent the steam away from you. Ventilate gas cooking units properly. Keep vents and burners grease-free. Use long-handled tools when barbequing. And never squirt lighter fluid directly onto charcoal
fires. Set your water heater temperature no higher than 120 degrees F (48.9 degrees C). Install smoke alarms throughout your home. Replace inefficient batteries. If you have a fireplace, use a fire screen. Clean your chimney regularly. Turn off appliances (coffee pot, iron, oven, and TV) when you go out. Store flammable chemicals (paints, gasoline, and solvents) in a cool well-ventilated area. Discard
old rags and empty cans. Keep a working fire extinguisher handy, and learn how to use it. Head off electrical accidents
Never use a knife or fork to retrieve toast from a plugged in toaster. Never use appliances (such as hair dryers, shavers, curling irons, and TV’s) while bathing. Install portable or permanent ground fault circuit interrupters into electrical outlets, especially in
the kitchen and bathrooms. Don’t overload outlets. Plug unused outlets with safety caps. Secure electrical cords away from children or pets. Turn off appliances during thunderstorms. Avoid using an electric lawn mower on wet grass or in the rain.
Prevent Poisoning
Store household cleaners, disinfectants, garden products, and pesticides in their original containers. Follow label instructions to safely dispose of old or unwanted substances.
Label all medicines, and keep prescriptions in their original bottles. Note expiration dates and discard any unused or outdated medication.
Falls Prevention: Falling can have bad effects on your health. Injury from a fall can lead to losing your independence. About 75 percent of all falls occur at home. Tripping and health problems cause most of these falls. A fall can be very serious, especially if you have just had surgery or you have an illness. This sheet tells you how to reduce your risk for falls and what to do if you fall. Tips to prevent tripping • Lighting. Walking in the dark is dangerous. You can trip over objects that you can’t see. Have bright lighting in your home. Be sure the stairs are well lit. Locate light switches at the top and bottom of each stairway. Put night lights in the bedroom, hallways, and bathroom. Place a bedroom lamp where you can reach it in the dark. • Vision. If you don’t see well, your risk of falling is greater. Blurred vision is a side effect of some medicines. Cataracts and other eye diseases can limit your vision. Be sure to wear your glasses or contact lenses. • Rugs and cords. Fasten rugs firmly to the floor, or use rugs with non-skid backing. Tack down all loose ends on rugs. Move electrical cords from areas of the floor where you walk. • Spills. Wipe up spills immediately. • Bathroom Area. Install grab bars in the bathroom. Put them in the bath and shower and next to the toilet. Do not hold onto towel bars or soap dishes when you move in the bathroom. These items may not be strong enough to support you. Place a nonskid mat in the tub or shower. • Hand rails. Avoid using stairs without hand rails. Install sturdy hand rails on all stairs. • Kitchen items. Place kitchen items within easy reach. Do not store things too high or too low. When things are easy to reach, you will not need to use a step ladder or a stool. Remember to close cabinet and closet doors and drawers. • Mattress. Place a “rug grabber” between the mattress and the box spring to prevent the mattress from sliding. • Footwear. When you wear stockings or socks without shoes, you have a greater risk of falling. Wear shoes and slippers that fit well and have firm, non-skid soles. Do not wear loose-fitting shoes or slippers. Take good care of yourself When you stay healthy, you reduce your chance of falling. Follow these guidelines: • Foot problems. See your doctor if you have pain or loss of feeling in your feet. You also should see your doctor if you have large, thick toenails and corns. When you have pain or discomfort in your feet, you make small changes in the way you walk. These changes can lead you to stumble and fall. • Medicines. Talk to your doctor about possible side effects of all the medicines you take. The side effects of medicine are a common cause of falls. The more medicines you take, the more side effects you may have. • Dizziness. If you have dizzy spells, see your doctor. Dizziness can make you lose your balance and fall. When you get up from lying down, sit for a few minutes. Then stand and get your bearings before you walk. Your blood pressure takes some time to adjust when you get up. If you stand up quickly, your blood pressure may be too low. You could then get dizzy, lose your balance, and fall. • Canes and walkers. If your doctor suggests that you use a cane or a walker, use it. These devices provide extra stability for walking and can help you avoid falls. • Vision. See your eye doctor once a year. Cataracts and other eye diseases can limit your vision. You have more risk of falling when you don’t see well.

What to do if you fall If you fall at home, remember: Step 1. Stay quiet for a moment —don’t panic. Step 2. Decide whether or not to try to get up. If you decide to try to get up: Step 1. Use strong, stable furniture for support as you try to get up. Step 2. Take some time to recover from your fall after you get up. Step 3. Tell someone that you had a fall. Step 4. Get medical advice if necessary. If you cannot get up, or if you decide not to try: Step 1. Slide or crawl to get help if you can. You might be able to reach one of the following:
a. Telephone b. Door to the Outside c. Personal Alarm Device d. Something to make a loud noise.
Step 2. Tell someone you have fallen and need help. Step 3. After calling for help, lie quietly until help arrives. Keep as warm and comfortable as you can. Step 4. Get medical advice if necessary. If you have questions If you have any questions about this information, please talk with your nurse, therapist, or doctor.


Preventing Falls Falls are the leading cause of injury for older people and more than half of all falls occur in the home. Discuss fall prevention with your physician and take the necessary steps to make your home safe. Take the following quiz to help assess the risk of falling in your home, the more “true” answers you have, the chance of falling is lessened: T F I do not have throw rugs; area rugs are secured with non-slip pads or double-sided tape
T F I do not store or stack items on the floor or steps
T F I have a night light in the bedroom, hallway and bathroom
T F I have a lamp close to my bed so I can turn it on before rising
T F I always turn on the light before entering a dark room
T F My shower/tub has a non-slip surface
T F My bathroom towel rack is sturdy
T F All stairways inside and outside my home have sturdy handrails
T F I am careful when taking medications that may cause me to become dizzy or drowsy
T F I wear my glasses when moving about my home
T F I do not rush to answer the phone or door
T F I never use a step stool or ladder that is not sturdy
T F I am careful not to block my vision when carrying packages
T F There are no electrical cords on the floor that may be a tripping hazard
T F Spills are wiped up immediately
Important Information If you or someone in your home uses oxygen, be sure to know exactly where the tubing before you stand up and move about in your home. Gather tubing in your hand as you walk always keeping it behind you. For children Make sure all stairways are gated and all screens are secured on the windows. For additional information Administration on Aging www.aoa.gove American Association of Retired Persons www.aarp.org US Consumer Product Safety Commission www.cpsc.gov


Questions and Answers about Health Care Directives
Minnesota Law Minnesota law allows you to inform others of your health care wishes. You have the right to state your wishes or appoint an agent in writing so that others will know what you want if you can't tell them because of illness or injury. The information that follows tells about health care directives and how to prepare them. It does not give every detail of the law. What is a Health Care Directive? A health care directive is a written document that informs other of your wishes about your health care. It allows you to name a person ("agent") to decide for you if you are unable to decide. It also allows you to name an agent if you want someone else to decide for you. You must be at least 18 years old to make a health care directive. Why Have a Health Care Directive? A health care directive is important if your attending physician determines you can't communicate your health care choices (because of physical or mental incapacity). It is also important if you wish to have someone else make your health care decisions. In some circumstances, your directive may state that you want someone other than an attending physician to decide when you cannot make your own decisions. Must I Have a Health Care Directive? What Happens if I Don't Have One? You don't have to have a health care directive. But, writing one helps to make sure your wishes are followed. You will still receive medical treatment if you don't have a written directive. Health care providers will listen to what people close to you say about your treatment preferences, but the best way to be sure your wishes are followed is to have a health care directive. How Do I Make a Health Care Directive? There are forms for health care directives. You don't have to use a form, but your health care directive must meet the following requirements to be legal:
Be in writing and dated. State your name. Be signed by you or someone you authorize to sign for you, when you can understand and
communicate your health care wishes. Have your signature verified by a notary public or two witnesses. Include the appointment of an agent to make health care decisions for you and/or instructions about
the health care choices you wish to make. Before you prepare or revise your directive, you should discuss your health care wishes with your doctor or other health care provider. Information about how to obtain forms for preparation of your health care directive can be found in the this document. I Prepared My Directive in Another State. Is It Still Good? Health care directives prepared in other states are legal if they meet the requirements of the other state's laws or the Minnesota requirements. But requests for assisted suicide will not be followed.
What Can I Put in a Health Care Directive? You have many choices of what to put in your health care directive. For example, you may include:
The person you trust as your agent to make health care decisions for you. You can name alternative agents in case the first agent is unavailable, or joint agents.
Your goals, values and preferences about health care. The types of medical treatment you would want (or not want). How you want your agent or agents to decide. Where you want to receive care. Instructions about artificial nutrition and hydration. Mental health treatments that use electroshock therapy or neuroleptic medications. Instructions if you are pregnant. Donation of organs, tissues and eyes. Funeral arrangements. Who you would like as your guardian or conservator if there is a court action.
You may be as specific or as general as you wish. You can choose which issues or treatments to deal with in your health care directive. Are There Any Limits to What I Can Put in My Health Care Directive? There are some limits about what you can put in your health care directive. For instance:
Your agent must be at least 18 years of age. Your agent cannot be your health care provider, unless the health care provider is a family member or
you give reasons for the naming of the agent in your directive. You cannot request health care treatment that is outside of reasonable medical practice. You cannot request assisted suicide.
How Long Does a Health Care Directive Last? Can I Change It? Your health care directive lasts until you change or cancel it. As long as the changes meet the health care directive requirements listed above, you may cancel your directive by any of the following:
A written statement saying you want to cancel it. Destroying it. Telling at least two other people you want to cancel it. Writing a new health care directive.
What If My Health Care Provider Refuses to Follow My Health Care Directive? Your health care provider generally will follow your health care directive, or any instructions from your agent, as long as the health care follows reasonable medical practice. But, you or your agent cannot request treatment that will not help you or which the provider cannot provide. If the provider cannot follow your agent's directions about life-sustaining treatment, the provider must inform the agent. The provider must also document the notice in your medical record. The provider must allow the agency to arrange to transfer you to another provider who will follow the agent's directions. What If I've Already Prepared a Health Care Document? Is It Still Good? Before August 1, 1998, Minnesota law provided for several other types of directives, including living wills, durable health care powers of attorney and mental health declarations. The law changed so people can use one form for all their health care instructions. Forms created before August 1, 1998, are still legal if they followed the law in effect when written. They are also legal if they meet the requirements of the new law (described above). You may want to review any existing documents to make sure they say what you want and meet all requirements.
What Should I Do With My Health Care Directive After I Have Signed It? You should inform others of your health care directive and give people copies of it. You may wish to inform family members, your health care agent or agents, and your health care providers that you have a health care directive. You should give them a copy. It's a good idea to review and update your directive as your needs change. Keep it in a safe place where it is easily found. What if I believe a Health Care Provider Has Not Followed Health Care Directive Requirements? Complaints of this type can be filed with the Office of Health Facility Complaints at 651-201-4200 (Metro Area) or Toll-free at 1-800-369-7994. What if I Believe a Health Plan Has Not Followed Health Care Directive Requirements? Complaints of this type can be filed with the Minnesota Health Information Clearinghouse at 651-201-5178 or Toll-free at 1-800-657-3793. How To Obtain Additional Information If you want more information about health care directives, please contact your health care provider, your attorney, or: Minnesota Board on Aging's Senior LinkAge Line® 1-800-333-2433. A suggested health care directive form is available on the internet at: http://www.mnaging.org/.


PATIENT BILLING AND
FINANCIAL ASSISTANCE INFORMATION
Sibley Medical Center is grateful for your commitment to our facility for your healthcare services. We are dedicated to providing healthcare services of outstanding quality, caring for our patients with respect and compassion, and improving the health of the individuals we serve.
Our charitable mission is to remove the barriers in accessing healthcare services.
If you do not have health care coverage please ask the receptionist to talk to a patient account representative for assistance.
PATIENT BILLING INFORMATION : Sibley Medical Center will process claims on your behalf to all health insurance carriers. All necessary and required information must be provided for each visit at the time of service, as well as any required assignments or authorizations. Please bring your insurance card and any co-payments required on your policy to each visit. Insurance billing specialists are available to work with you on any insurance billing questions you may have. Sibley Medical Center will send you a monthly statement showing any balances remaining after your insurance company has responded to us with either a payment or a denial of payment for your visit. Payment in full is due upon receipt of your first statement after insurance has paid.
PAYMENT ARRANGEMENTS: If you are unable to pay your balance in full please contact the patient account representative immediately to make payment arrangements. You may call 888-974-2539 to set up payment arrangements. These payments will be based on a schedule which is determined by the size of your account. Interest will be charged on all accounts not paid in full with your statement.
CLINIC LAB AND X-RAY SERVICES: Due to our status as a provider-based rural health clinic all the lab and x-ray services you receive as a clinic patient will be billed as hospital outpatient services. Please check with your insurance on how outpatient services are paid under your policy.
UNINSURED DISCOUNT: A ten percent (10%) uninsured discount will be offered for medically necessary services to any uninsured patient that has an income level of $125,000 or less if the patient does not have health care coverage. The discount will also apply to any charges that an insured patient incurs for medically necessary services that are not covered by their health insurance.
PROMPT PAY DISCOUNT: A five percent (5%) prompt pay discount will be offered to any uninsured patient that pays the entire portion of their account if paid at the time of the service or within 10 days of receiving notification of the amount of the medical service bill.
FINANCIAL AID/CHARITY CARE: Financial aid will be offered to insured and uninsured patients that meet the criteria set forth in our financial assistance policy. An application may be picked up in the business office or can be mailed to the patient. Proof of income and assets will be required to determine if a patient can qualify. The income guidelines follow the federal poverty income guidelines. A portion or the entire amount of your charges may qualify for this write off.
Please stop by the Business Office with any questions at 601 West Chandler, Arlington, MN. 55037
or call our toll free line at: 888-974-2539 to request any additional information or applications for these programs.
Business Office Hours: Monday-Friday 8:00-4:00
This information applies only to the services billed by Sibley Medical Center. Services such as outpatient specialty physician charges, radiology reads, and pathology services are not billed by our facility.


NON-DISCRIMINATION POLICY
It is the policy of Sibley Medical Center to provide services to all persons without regard to race, color, sex, national origin, handicap or age. The same requirements are applied to all and there is no distinction in eligibility for, or in the manner of providing services. All services are available without distinction to all participants regardless of race, color, sex, national origin, handicap or age. All persons and organizations having occasion either to refer persons for services or to recommend our services are advised to do so without regard to the person’s of race, color, sex, national origin, handicap or age. The person designated to coordinate compliance with this policy is the Compliance officer who can be reached at (507) 964-8420


1
OVERVIEW OF PATIENT PRIVACY RIGHTS
(7/2012)
The attached Notice of Privacy Practices describes in detail how we manage your health information. This page summarizes these rules and your rights. How We Use Your Information We use your health information to treat you, to facilitate payment for services, and to inform you of helpful services. This can include sharing information with people involved in your care. It may include sharing limited information for development and to conduct research to better serve you. We also may give information to law enforcement and certain government offices if there is a threat to public health or safety. Your Rights We fully support your right to manage your health information. The attached document (Notice of Privacy Practices) explains these rights in detail. Here is a summary of your rights.
1) In general, you can see your health information upon request.
2) You can request restrictions on who sees your health information.
3) You can request corrections to your health information.
4) You can request a list of certain disclosures we have made of your health information.
5) We must get your written permission to share health information for any purpose other than those described in the Notice of Privacy Practices. If you give us permission, you may revoke it at any time.
6) You can ask questions about our privacy practices and you can disagree with any decision we make about your rights. You may do so by contacting us directly or contacting the U.S. government.
You may call us at any time with general questions about your privacy rights. When making specific requests, please write to us at the address listed on the last page. Fulfilling some requests may incur a charge. We will let you know which of these requests will be charged and the approximate amount of such charges before we respond to your request. We are glad to have you as a patient, and we will work hard to protect your health information.


2
NOTICE OF PRIVACY PRACTICES
THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
PLEASE REVIEW IT CAREFULLY.
Our Health Information Duties We have a legal duty to protect the privacy of your health information and to give you this Notice. We have a legal duty to abide by the Notice of Privacy Practices that is current. We may change the terms of this Notice and to make the new terms effective for all health
information we have. This includes health information we created or received before we made the changes.
We will make any revised Notice available in hard copy, and by displaying it in our facilities and on our Web site. Also, you can request the revised Notice in-person or by mail.
“Health information” means, generally, information about your past or present health status, condition, diagnosis, treatment, prognosis, or payment for health care. Who will Follow this Notice This notice describes our facility’s practices and that of: Any health care worker authorized to enter information into your medical and billing records. All departments and programs of the facility. All students, and other trainees affiliated with this facility. All employees, volunteers, and others working for this facility. Your Health Information Rights
Restrictions on Use or Disclosure. This Notice describes some restrictions on how we can use and give out your health information. You may ask us for extra limits on how we use or to whom we give the information. You need to make your request in writing. We are not required to agree to your request. If we do agree, we will follow our agreement, except: in an emergency where the information is needed for your treatment if you give us written permission to use or give out your information if you or we end the restriction, or as otherwise required by law.
Alternative Communication. Normally, we will communicate with you at the address and phone you give us. You may ask us to communicate with you by other ways or at another location. Your request needs to explain how you want the information communicated and where. We will agree to your request if it is reasonable. If you restrict us from providing information to your insurer, you also need to explain how you will pay for your treatments. Patient Access. You may look at or get copies of your health information. (There are some exceptions.) You need to make your request in writing. If you ask for copies in a format other than paper copies, we will give you that other format if practical. If you ask for copies, we may charge fees as allowed for by law. If you ask for your records in a format we can provide, we will charge a reasonable fee based on our

3
costs.If your request is denied, we will send the denial in writing. This will include the reason and describe any right you may have to a review of the denial. Amendment. You may ask us to change certain health information. You need to make your request in writing. You must explain why the information should be changed. If we accept your change, we will try to inform others (including people you list in writing) of the change. We will include the changes in future disclosures of your health information. If your request is denied, we will send the denial in writing. This denial will include the reason and describe any steps you may take in response. Disclosure List. You may receive a free list of disclosures - with some exceptions – made by us or our business associates of your health information. The list does not include: disclosures made for treatment, payment or health care operations disclosures made before April 14, 2003 disclosures you have authorized certain other disclosures. You need to make your request in writing. If you ask for a list more than once in a 12-month period, we may charge you a fee for each extra list. You may withdraw or change your request to reduce or eliminate the charge. Paper Copy of Notice. You may receive a paper copy of our current Notice of Privacy Practices. How to Use These Rights. Please contact our Health Information Management Department listed on the last page to use any of these rights or receive more information about any related fees. Uses and Disclosures of Health Information To provide you care, we have certain reasons we use and disclose health information. We make all uses and disclosures according to our privacy policies and the law. We may use and give your health information as follows: Treatment, Payment and Health Care Operations. We may use and give your health information for: treatment (includes working with another provider) payment (such as billing for services provided) our health care operations. These are non-treatment and non-payment activities that let us run our
business or provide services. These include, for example, quality assessment and conducting training programs.
Medical Emergency. We may use or give your health information to help you in a medical emergency. Appointment Reminders; Treatment Alternatives. We may send you appointment reminders, or tell you about treatments and health-related benefits or services that you may find helpful. Patient Information Directory. We may give the following information to people who ask about you by name: your name location in the facility general condition religious affiliation (given only to clergy). You may choose not to have us give out some or all of this information. (There are some exceptions, such as medical emergencies, if you cannot talk to us until the emergency is over.) For example, if you do not want us to tell people you are in the facility or give out your general condition or location, we will agree to your instructions.

4
People Involved in Your Care. We may give limited health information to people involved in your care or to help plan your care (such as a family member or emergency contact). If you do not want this information given out, it will not be given. If appropriate, we may allow another person to pick up your prescriptions, medical supplies or X-rays. Foundations/Fundraising. We may contact you or have our foundations contact you about health system activities, including fundraising programs and events. We will use or give only your name, how to contact you, other demographic information, and the dates we served you. We may give this information to a business associate to help us with our programs. Research. We may use or share your health information for research purposes as allowed by law or if you have given permission. Death; Organ Donation. We may give certain health information about a deceased person to the next of kin. We may also give this information to a funeral director, coroner, medical examiner, law enforcement official, or organ donation groups. Health Care Workplace Medical Surveillance/Injury/Illness. If your employer is a health care provider, we may share health information required by state or federal law:
about work-related illness or injury, or for workplace medical surveillance activities.
Law Enforcement. We may give certain health information to law enforcement. This could be:
about a missing child, or when there may have been crime at the facility, or when there is a serious threat to the health or safety of another person or people.
Correctional Facility. We may give the health information of an inmate or other person in custody to law enforcement or a correctional institution. Abuse or Neglect. We may give health information to the proper authorities about possible abuse or neglect of a child or a vulnerable adult. Food and Drug Administration (FDA) Regulation. We may give health information to people regulated by the FDA to measure the quality, safety and effectiveness of their products. Military Authorities/National Security. We may give health information to authorized people from the U.S. military, foreign military, and U.S. national security or protective services. Public Health Risks. We may give health information about you for public health purposes. These purposes include the following: reporting and controlling disease (such as cancer or tuberculosis), injury or disability reporting vital events such as births and deaths reporting adverse events or surveillance related to food, medications, or problems with health
products notifying persons of recalls, repairs or replacements of products they may be using notifying a person who may have been exposed to a disease or be at risk for catching or spreading a
disease or condition. Health Oversight Activities. We may give health information to government, licensing, auditing and accrediting agencies for actions allowed or required by law.

5
Required by Other Laws. We may use or give health information as required by other laws. For example:
We may give health information to the U.S. Department of Health and Human Services during an investigation.
We may give health information under workers’ compensation or similar laws. We may give health information:
- To social services and other agencies or people allowed to receive information about certain injuries or health conditions for social service, health or law enforcement reasons. - About an unemancipated minor or a person who has a legal guardian or conservator about a pending abortion. - About an emancipated minor or a minor receiving confidential services to prevent a serious threat to the health of the minor.
Legal Process. We may give health information in response to a state or federal court order, legal orders, subpoenas, or other legal documents. Health Records under State Law. Release of health records (such as medical charts or X-rays) by licensed Minnesota providers usually requires the signed permission of a patient or the patient’s legal representative. Exceptions include you having a medical emergency, you seeing a related provider for current treatment, and other releases required or allowed by law. With Your Authorization Your Authorization. Except for what is listed above, we may use or give health information only with your written permission. If you give written permission, you may revoke it at any time by notifying us in writing. This form is available from the Health Information Management Department listed below. Your permission will end when we receive the signed form, or when we have acted on your request. Questions and Complaints If you have questions about our privacy practices, please contact the Health Information Management Department listed below. If you think your privacy rights have been violated, or if you disagree with a decision about any of your rights, you may file a complaint with us at the office listed below. You also may send a written complaint to the U.S. Department of Health and Human Services. We will give you the address to file a complaint if you ask for it. We will not punish you or retaliate if you choose to file a complaint. Organizations Covered by this Notice
This Notice applies to the privacy practices of Sibley Medical Center. These businesses are part of an organized health care system. We may share health information within the system for treatment, payment or health care operations. This Notice takes effect April 14, 2003. It will remain in effect until we replace it.
Sibley Medical Center Health Information Mangement Dept
601 West Chandler Street Arlington, MN 55307-2127
July 1, 2007 Page 1
Home Care Bill of Rights
Per Minnesota Statutes, Section 144A.44, except language in bold print which represents additional consumer rights under federal law. To be used by Medicare certified agencies. 144A.44 Home Care Bill of Rights. Subdivision 1. Statement of rights. A person who receives home care services has these rights: 1. The right to receive written information about rights in advance of receiving care or during the initial evaluation visit before the initiation of treatment, including what to do if rights are violated. 2. The right to receive care and services according to a suitable and up-to-date plan, and subject to accepted medical or nursing standards, to take an active part in creating and changing the plan and evaluating care and services. The provider must advise the recipient in advance of the right to participate in planning the care or treatment. 3. The right to be told in advance of receiving care about the services that will be provided, the disciplines that will furnish care, the frequency of visits proposed to be furnished, other choices that are available, and the consequences of these choices, including the consequences of refusing these services. 4. The right to be told in advance, of any changes in the plan of care and to take an active part in any changes; and the planning before any change is made. 5. The right to refuse services or treatment. 6. The right to know, in advance, any limits to the services available from a provider, and the provider’s grounds for a termination of services. 7. The right to know, and to be advised, both orally and in writing, in advance of receiving care whether the services are covered by health insurance, medical assistance, or other health programs, the charges for services that will not be covered by Medicare, and the charges that the individual may have to pay. The provider must advise the recipient of home care services, both orally and in writing, of any changes in such coverage and the recipient’s liability for charges as soon as possible, but no later than 30 calendar days after the provider becomes aware of the change. 8. The right to know what the charges are for services, no matter who will be paying the bill.

July 1, 2007 Page 2
9. The right to know that there may be other services available in the community, including other home care services and providers, and to know where to go for information about these services. 10. The right to choose freely among available providers and to change providers after services have begun, within limits of health insurance, medical assistance, or other health programs. 11. The right to have personal, financial, and medical information kept private, and to be advised of the provider’s policies and procedures regarding disclosure of such information. 12. The right to be allowed access to records and written information from records in accordance with section 144.335. 13. The right to be served by people who are properly trained and competent to perform their duties. 14. The right to be treated with courtesy and respect, and to have the patient’s property treated with respect. 15. The right to be free from physical and verbal abuse. 16. The right to reasonable, advance notice of changes in services or charges, including at least ten days’ advance notice of the termination of a service by a provider, except in cases where:
(i) the recipient of services engages in conduct that alters the conditions of employment as specified in the employment contract between the home care provider and the individual providing home care services, or creates an abusive or unsafe work environment for the individual providing home care services; or (ii) an emergency for the informal caregiver or a significant change in the recipient’s condition has resulted in service needs that exceed the current service provider agreement and that cannot be safely met by the home care provider.
17. The right to a coordinated transfer when there will be a change in the provider of services. 18. The right to voice grievances regarding treatment or care that is, or fails to be, furnished, or regarding the lack of courtesy or respect to the patient or the patient’s property. 19. The right to know how to contact an individual associated with the provider who is responsible for handling problems and to have the provider investigate and attempt to

July 1, 2007 Page 3
resolve the grievance or complaint. The provider shall document in writing all complaints, as well as document, in writing, any resolution of the complaint against anyone furnishing services on behalf of the provider. 20. The right to know the name and address of the state or county agency to contact for additional information or assistance. 21. The right to assert these rights personally, or have them asserted by the patient’s family or guardian when the patient has been judged incompetent, without retaliation. A home care provider may not require a person to surrender these rights as a condition of receiving services. A guardian or conservator or, when there is not a guardian or conservator, a designated person may seek to enforce these rights. A provider must protect and promote these rights. IF YOU HAVE A COMPLAINT ABOUT THE AGENCY OR PERSON PROVIDING YOU HOME CARE SERVICES, YOU MAY CALL, WRITE, OR VISIT THE OFFICE OF HEALTH FACILITY COMPLAINTS, MINNESOTA DEPARTMENT OF HEALTH. YOU MAY ALSO CONTACT THE OMBUDSMAN FOR LONG-TERM CARE. Office of Health Facility Complaints (651) 201-4201 1-800- 369-7994 Fax: (651) 281-9796 Mailing Address Minnesota Department of Health Office of Health Facility Complaints 85 East Seventh Place, Suite 300 P.O. Box 64970 St. Paul, Minnesota 55164-0970 Ombudsman for Long-Term Care (651) 431-2555 1-800-657-3591 Fax: (651) 431-7452 Mailing Address Home Care Ombudsman Ombudsman for Long-Term Care PO Box 64971 St. Paul, MN 55164-0971 ________________________________________________________________________

July 1, 2007 Page 4
Licensee Name: ________________________________________________________________________ Telephone Number: ________________________________________________________________________ Address: ________________________________________________________________________ Name/Title of Person to Whom Problems or Complaints May be Directed: For informational purposes only and is not required in the Home Care Bill of Rights text: MN Statutes, section 144A.44 Subd. 2. Interpretation and enforcement of rights. These rights are established for the benefit of persons who receive home care services. "Home care services" means home care services as defined in section 144A.43, subdivision 3. A home care provider may not require a person to surrender these rights as a condition of receiving services. A guardian or conservator or, when there is no guardian or conservator, a designated person, may seek to enforce these rights. This statement of rights does not replace or diminish other rights and liberties that may exist relative to persons receiving home care services, persons providing home care services, or providers licensed under Laws 1987, chapter 378. A copy of these rights must be provided to an individual at the time home care services are initiated. The copy shall also contain the address and phone number of the Office of Health Facility Complaints and the Office of the Ombudsman for Older Minnesotans and a brief statement describing how to file a complaint with these offices. Information about how to contact the Office of the Ombudsman for Older Minnesotans shall be included in notices of change in client fees and in notices where home care providers initiate transfer or discontinuation of services.
jenniferf
Typewritten Text
Sibley Medical Center Home Care
jenniferf
Typewritten Text
507-964-2271
jenniferf
Typewritten Text
601 West Chandler St Arlington MN 55307
jenniferf
Typewritten Text
Teresa Messner RN, Home Care Coordinator
jenniferf
Text Box
_________________________________ Signature and date received
jenniferf
Text Box
jjj
jjj
jjj
jjj
Home Health AgencyOutcome and Assessment Information Set(OASIS)
STATEMENT OF PATIENT PRIVACY RIGHTSAs a home health patient, you have the privacy rights listed below.
j You have the right to know why we need to ask you questions.
We are required by law to collect health information to make sure: 1) you get quality health care, and 2) payment for Medicare and Medicaid patients is correct.
j You have the right to have your personal health care informationkept confidential.
You may be asked to tell us information about yourself so thatwe will know which home health services will be best for you. We keep anything we learn about you confidential.This means, only those who are legally authorized to know, or whohave a medical need to know, will see your personal health information.
j You have the right to refuse to answer questions.
We may need your help in collecting your health information. If you choose not to answer, we will fill in the information as best we can. You do not have to answer every question to get services.
j You have the right to look at your personal health information.
I We know how important it is that the information we collect about you is correct. If you think we made a mistake, ask us to correct it.
I If you are not satisfied with our response, you can ask the Health Care FinancingAdministration, the federal Medicare and Medicaid agency, to correct your information.
You can ask the Health Care Financing Administration to see, review, copy, or correct your personal healthinformation which that Federal agency maintains in its HHA OASIS System of Records. See the back of this Notice for CONTACT INFORMATION. If you want a more detailed description of your privacy rights, see theback of this Notice: PRIVACY ACT STATEMENT - HEALTH CARE RECORDS.
This is a Medicare & Medicaid Approved Notice.

PRIVACY ACT STATEMENT - HEALTH CARE RECORDS
THIS STATEMENT GIVES YOU ADVICE REQUIRED BY LAW (the Privacy Act of 1974). THIS STATEMENT IS NOT A CONSENT FORM. IT WILL NOT BE USED TO RELEASE OR TO USE YOUR HEALTH CARE INFORMATION.
I. AUTHORITY FOR COLLECTION OF YOUR INFORMATION, INCLUDING YOUR SOCIAL SECURITY NUMBER, AND WHETHER OR NOT YOU ARE REQUIRED TO PROVIDE INFORMATION FOR THIS ASSESSMENT. Sections 1102(a), 1154, 1861(o), 1861(z), 1863, 1864, 1865, 1866, 1871, 1891(b) of the Social Security Act.
Medicare and Medicaid participating home health agencies must do a complete assessment that accurately reflects your current health and includes information that can be used to show your progress toward your health goals. The home health agency must use the ^Outcome and Assessment Information Set] (OASIS)
assessment, it is protected under the federal Privacy Act of 1974 and the ^Home Health Agency Outcome and Assessment Information Set] (HHA OASIS) System of Records. You have the right to see, copy, review, and request correction of your information in the HHA OASIS System of Records.
II. PRINCIPAL PURPOSES FOR WHICH YOUR INFORMATION IS INTENDED TO BE USED
The information collected will be entered into the Home Health Agency Outcome and Assessment Information Set (HHA OASIS) System No. 09-70-9002. Your health care information in the HHA OASIS System of Records will be used for the following purposes: A support litigation involving the Centers for Medicare & Medicaid Services; A support regulatory, reimbursement, and policy functions performed within the Centers for Medicare & Medicaid Services or by a contractor or consultant; A study the effectiveness and quality of care provided by those home health agencies; A survey and certification of Medicare and Medicaid home health agencies; A provide for development, validation, and refinement of a Medicare prospective payment system; A enable regulators to provide home health agencies with data for their internal quality improvement activities; A support research, evaluation, or epidemiological projects related to the prevention of disease or disability, or the restoration or maintenance of health,
and for health care payment related projects; and A support constituent requests made to a Congressional representative.
III. ROUTINE USES
These ^routine uses ] specify the circumstances when the Centers for Medicare & Medicaid Services may release your information from the HHA OASIS System of Records without your consent. Each prospective recipient must agree in writing to ensure the continuing confidentiality and security of your information.Disclosures of the information may be to:
2. contractors or consultants working for the Centers for Medicare & Medicaid Services to assist in the performance of a service related to thissystem of records and who need to access these records to perform the activity;
3. an agency of a State government for purposes of determining, evaluating, and/or assessing cost, effectiveness, and/or quality of health care servicesprovided in the State; for developing and operating Medicaid reimbursement systems; or for the administration of Federal/State home health agency programs within the State;
4. another Federal or State agency to contribute to the accuracy of the Centers for Medicare & Medicaid Services' health insurance operations (payment,treatment and coverage) and/or to support State agencies in the evaluations and monitoring of care provided by HHAs;
6. an individual or organization for a research, evaluation, or epidemiological project related to the prevention of disease or disability, the restoration or maintenance of health, or payment related projects;
7. a congressional office in response to a constituent inquiry made at the written request of the constituent about whom the record is maintained.
IV. EFFECT ON YOU, IF YOU DO NOT PROVIDE INFORMATION
The home health agency needs the information contained in the Outcome and Assessment Information Set in order to give you quality care. It is important thatthe information be correct. Incorrect information could result in payment errors. Incorrect information also could make it hard to be sure that the agency is givingyou quality services. If you choose not to provide information, there is no federal requirement for the home health agency to refuse you services.
N OTE: This statement may be included in the admission packet for all new home health agency admissions. Home health agencies may request you or your representative to sign this statement to document that this statement was given to you. Your signature is NOT required. If you or yourrepresentative sign the statement, the signature merely indicates that you received this statement. You or your representative must be supplied with a copy of this statement.
CONTACT INFORMATION
that the Federal agency maintains in its HHA OASIS System of Records: Call 1-800-MEDICARE, toll free, for assistance in contacting the HHA OASIS System Manager.
TTY for the hearing and speech impaired: 1-877-486-2048.
care to its patients. You have the right to refuse to provide information for the assessment to the home health agency. If your information is included in an
when evaluating your health. To do this, the agency must get information from every patient. This information is used by the Centers for Medicare & MedicaidServices (CMS, the federal Medicare & Medicaid agency) to be sure that the home health agency meets quality standards and gives appropriate health
Improvement Organizations, to perform Title XI or Title XVIII functions relating to assessing and improving home health agency quality of care;5. ualityQ
1. the federal Department of Justice for litigation involving the Centers for Medicare & Medicaid Services;
If you want to ask the Centers for Medicare & Medicaid Services to see, review, copy, or correct your personal health information


















