Home based KMC practices – feasibility and acceptability ... · Home based KMC practices –...
18
Home based KMC practices – feasibility and acceptability in deprived section of community in rural, tribal and urban slums in India- a pilot study Dr. Reeta Rasaily, Scientist E Div. Of Reproductive & Child Health ICMR, N. Delhi
Transcript of Home based KMC practices – feasibility and acceptability ... · Home based KMC practices –...
Home based KMC practices – feasibility and acceptability in deprived section of community in rural, tribal and urban
slums in India- a pilot study
Dr. Reeta Rasaily, Scientist EDiv. Of Reproductive & Child Health
ICMR, N. Delhi
feasibility and acceptability in deprived section of
Background
• LBW contributes to 28% of newborn death• KMC method (STS contact) reduces morbidity,
promote thermal regulation, improves breast feeding rates and early discharge in hospital born LBW babies
• Studies have shown this method could be adopted in the community(Q. Iftekhar, J. Perinatology 2003, Shivgarh study)
• Limited evidence available on impact on mortality of community KMC (Joy Lawn 2010, Cochrane review)
• Feasibility and acceptability of the method in different setting needs to be tested
Objective
• To test feasibility and acceptability of KMC by the mother / family members
• Compliance of the method
Participating centers:• PMC Anand, Gujrat, Anand municipality area: Urban
and periurban• NIAHRD, Cuttack, Orissa: Rural area• NIRRH Mumbai, Maharashtra: Rural tribal area
Study design & methodology
Study design: community based intervention (pilot) study
Study size: 100 newbornsInclusion criteria
– Home deliveries as well as hospital deliveries returning home within one wk of delivery
– B.wt. 1500-2000 grams Exclusion criteria:
– Sick mothers– Significant bleeding in mothers– Features suggestive of chorioamnioitis– Psychiatric illness– Post partum convulsions– Do not agree to participate in the study
Intervention:• Existing health care infrastructure of anganwadi
center were utilized for IEC session• KMC messages promoted as part of essential
newborn care during antenatal period by ANM, AWWs, ASHAs
• Counseled pregnant women and family members• At delivery, by TBA / ANM• Post partum period by ANM, TBA, AWW,
Reinforce other messages of health education, Feeding advise, Explain danger signs, distribute pictorial education material
• Apparel: KMC bag/ KMC blouse
Study design & methodology
Methodology (contd.)
Quantitative:• Demographic data• Delivery details• Newborn care practices• Time of initiation of KMC• No of hours of practice• Duration• Morbidity, Discomfort in mother
• Follow up -1 wk every day, alternate day 2 wk, 2nd month
• Weight: at birth and follow up
Qualitative: FGD before and after intervention, IDI
Quality assurance:
• Tools & SOP developed centrally• Centralised training for trainers at AIIMS for 3 days• Trainers trained project
staff, Mos, ANM, LHVs, AWWs, ASHAs at respective sites
• IEC of pregnant women and family members by health workers,
• Counseling sessions supervised by project staff• Data collection by separate staff
• Percentages of women accepting KMC method, • Percentages of women continuing KMC• Duration of KMC/day, • total number of days continuing KMC
Acceptability was defined as practicing skin to skin contact by mother/ care giver for any duration.
Acceptability was also assessed on day 7 after initiation of kangaroo mother care using a questionnaire incorporating Likert scale
Outcome measure

Results
• Study period: Jan 2010-Dec 2011• Enrollment: 12 months period (all 4 seasons)• Live birth =2567• LBW(upto 2000gms)= 129• Excluded =13
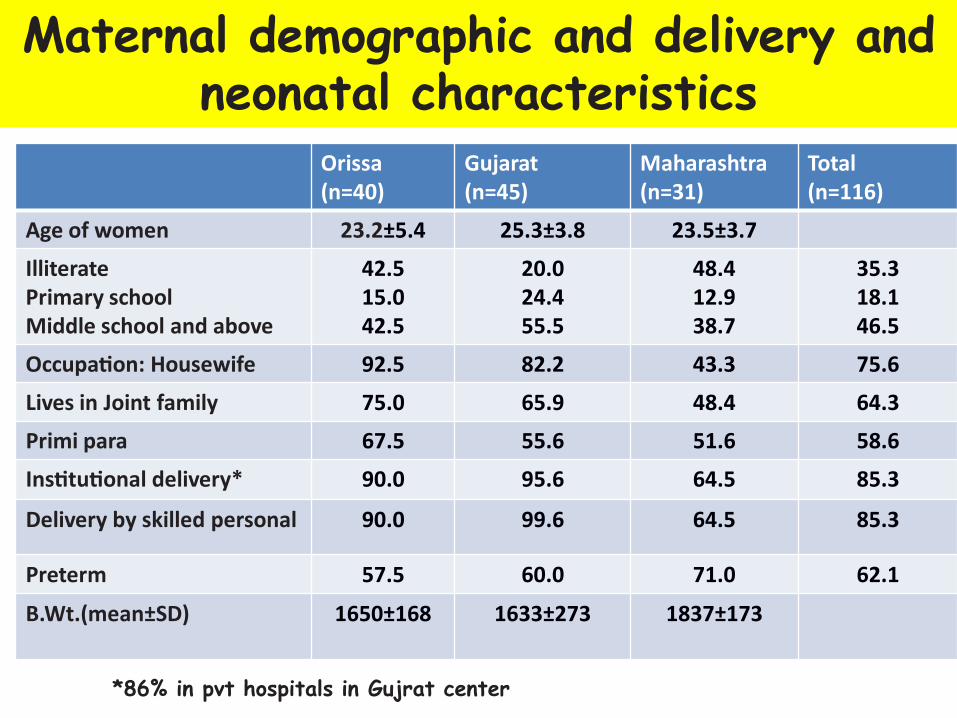
Maternal demographic and delivery and neonatal characteristics
Orissa(n=40)
Gujarat(n=45)
Maharashtra(n=31)
Total (n=116)
Age of women 23.2±5.4 25.3±3.8 23.5±3.7
IlliteratePrimary schoolMiddle school and above
42.515.042.5
20.024.455.5
48.412.938.7
35.318.146.5
Occupation: Housewife 92.5 82.2 43.3 75.6
Lives in Joint family 75.0 65.9 48.4 64.3
Primi para 67.5 55.6 51.6 58.6
Institutional delivery* 90.0 95.6 64.5 85.3
Delivery by skilled personal 90.0 99.6 64.5 85.3
Preterm 57.5 60.0 71.0 62.1
B.Wt.(mean±SD) 1650±168 1633±273 1837±173
*86% in pvt hospitals in Gujrat center
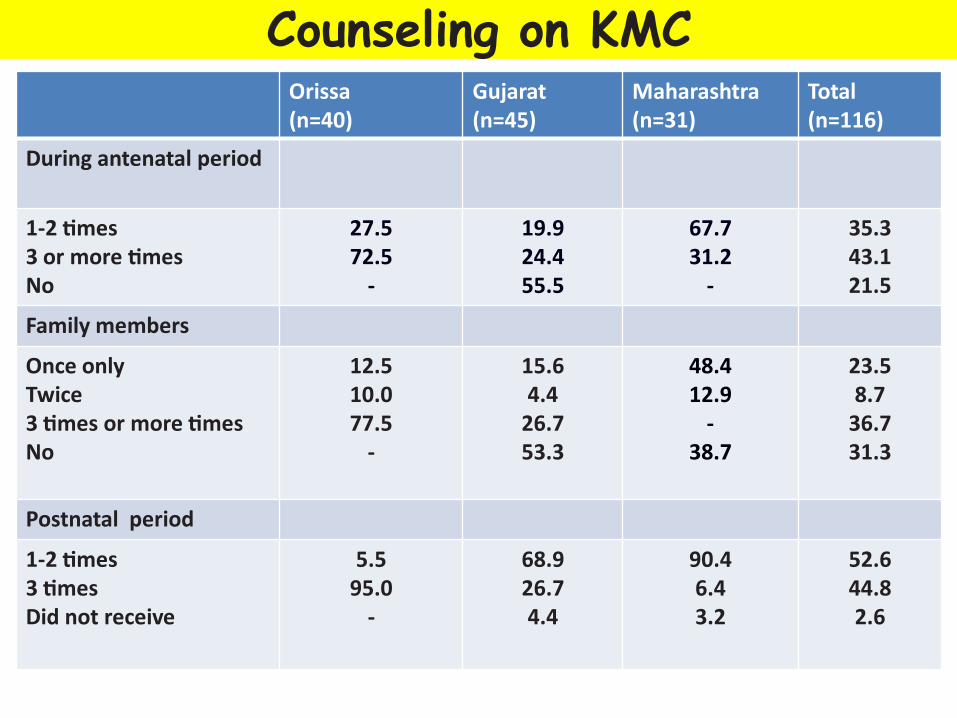
Maternal demographic and delivery and Counseling on KMCOrissa(n=40)
Gujarat(n=45)
Maharashtra(n=31)
Total(n=116)
During antenatal period
1-2 times3 or more timesNo
27.572.5
-
19.924.455.5
67.731.2
-
35.343.121.5
Family members
Once onlyTwice3 times or more timesNo
12.510.077.5
-
15.64.4
26.753.3
48.412.9
-38.7
23.58.7
36.731.3
Postnatal period
1-2 times3 times Did not receive
5.595.0
-
68.926.74.4
90.46.43.2
52.644.82.6

AcceptabilityOrissa(n=40)
Gujarat(n=45)
Maharashtra(n=31)
Total(n=116)
Time of initiation of KMC
Within 24 hrs24-<72 hrs72 hrs-<1wk>1 wk
37.550.012.5
-
8.913.326.751.1
12.932.354.8
-
19.831.029.319.8
Mode of providing KMC
Once in a whileAlmost always/intermittentlyNot given
-100.0
-
9.390.7
-
16.177.46.5
7.990.31.8
No. of hrs of KMC 8 4 3 5
Total no. days KMC given(median) 35 45 25
Family member provided KMC 37.5 16.7 22.6 25.7
Suggest KMC to others 100.0 86.7 90.3 92.2
66.7% Practiced KMC while sleeping in Gujrat, 37.9% in Mumbai
Was there any problems
Problems stated (10%)• Mothers: back pain during KMC for sitting in one
place for long time, body pain, knee pain
• Newborn: fast breathing, poor sucking, fever, cold to touch, yellow skin, vomiting after breast feeding, sticky eyes)
8(7%) deaths, not related to practice of KMC
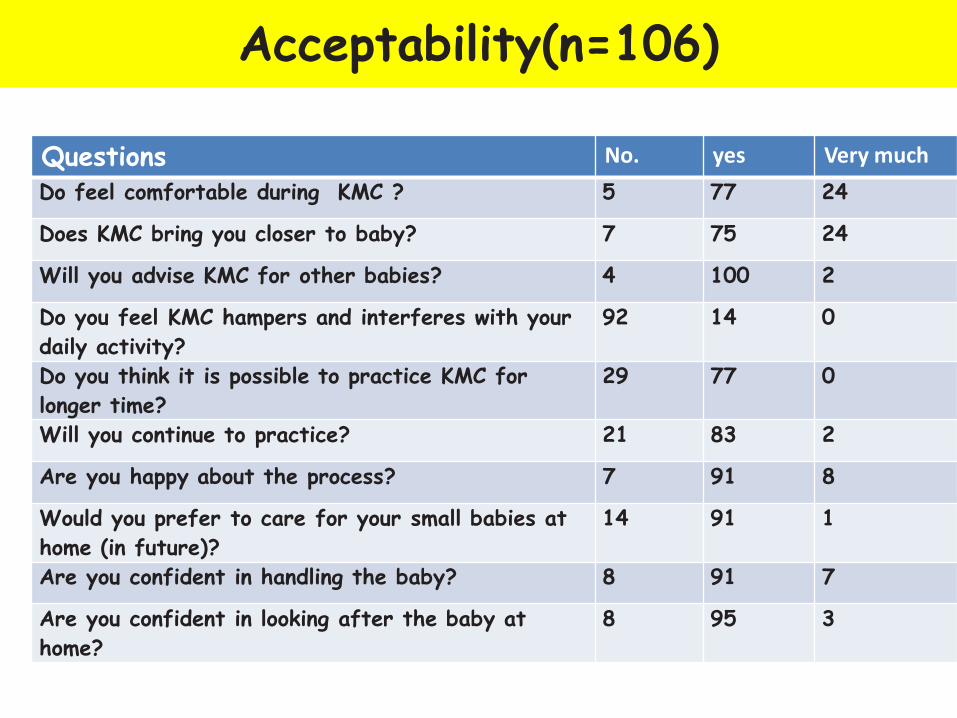
Acceptability(n=106)
Questions No. yes Very muchDo feel comfortable during KMC ? 5 77 24
Does KMC bring you closer to baby? 7 75 24
Will you advise KMC for other babies? 4 100 2
Do you feel KMC hampers and interferes with your daily activity?
92 14 0
Do you think it is possible to practice KMC for longer time?
29 77 0
Will you continue to practice? 21 83 2
Are you happy about the process? 7 91 8
Would you prefer to care for your small babies at home (in future)?
14 91 1
Are you confident in handling the baby? 8 91 7
Are you confident in looking after the baby at home?
8 95 3
Conclusion• Community level initiation• Utilized AWW infrastructure• Counseling by health workers• Feasible to introduce through health system• Acceptance by mothers and family members :80%
initiated within 1 wk, provided KMC average 5 hrs/ day, median no. days 25-35
• Other family members, mother-in-law, husband also provided KMC (25%)
Further research needed to assess impact on mortality
Challenges:
• Skill building of health workers• Follow up strategy• Referral linkage • Strengthening referral facility• Enabling environment at home• Educational material for family members
Further health system research to identify barriers to and finding solutions
Acknowledgement:
• Site PIs:• NIRRH Mumbai:
– Dr. R. Kulkarni– Dr. S. Chauhan
• NIAHRD:– Dr. S. Swain– Ms. L. Kanugo
• Gujrat:– Dr. S.N. Vani– Dr. N. Kharood,
Health officials, health workers,community
Members of Steering Group:• Dr. H.P.S. Sachdev, N. Delhi• Dr. V.K. Paul, AIIMS• Dr. A.K. Deorari, AIIMS• Dr. R. Nanavati, KEM Mumbai• Dr. V. Kumar, Lucknow• Late Dr. G.K. Malik, Lucknow• Dr. R. Agarwal, AIIMS
Centralised Training:• AIIMS team• Shivgarh team
Data analysis: Mrs Garima

THANK YOU