Holland Bloorview BLOOM Summer 2011
36
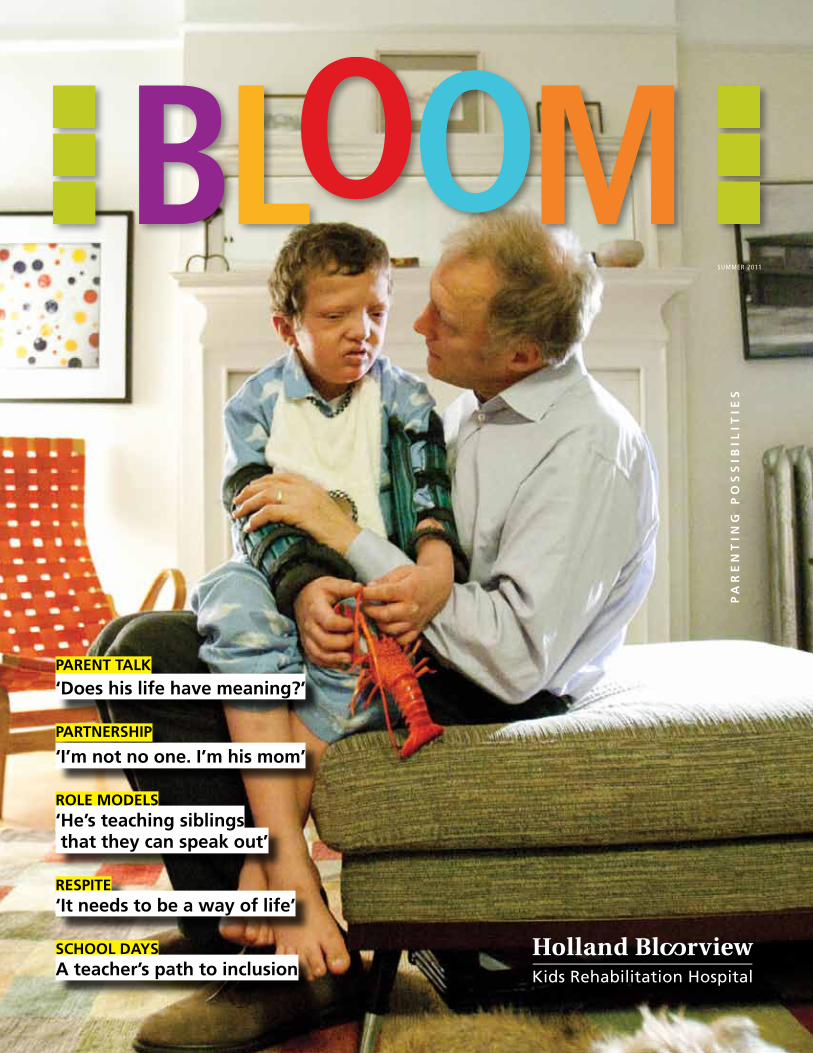
BLOOM ~ summer ~ 2011 ~ 1 SUMMER 2011 PARENTING POSSIBILITIES PARENT TALK ‘Does his life have meaning?’ PARTNERSHIP ‘I’m not no one. I’m his mom’ ROLE MODELS ‘He’s teaching siblings that they can speak out’ RESPITE ‘It needs to be a way of life’ SCHOOL DAYS A teacher’s path to inclusion
-
Upload
holland-bloorview-kids-rehabilitation-hospital -
Category
Documents
-
view
215 -
download
1
description
BLOOM is a how-to magazine on parentingchildren with disabilities. BLOOM gives voiceto the joys and challenges of special-needsparenting by combining firsthand familyinsights and the best professional advice.We believe that every child bloomsin his or her own unique way.
Transcript of Holland Bloorview BLOOM Summer 2011
BLOOM ~ summer ~ 2011 ~ 1
SUMMER 2011
PA
RE
NT
ING
PO
SS
IBIL
ITIE
S
PARENT TALK
‘Does his life have meaning?’
PARTNERSHIP
‘I’m not no one. I’m his mom’
ROLE MODELS‘He’s teaching siblings that they can speak out’
RESPITE‘It needs to be a way of life’
SCHOOL DAYSA teacher’s path to inclusion
2 ~ BLOOM ~ summer ~ 2011
Visit the Family Resource Centre
Want information and support on parenting kids with disabilities? Visit Holland Bloorview’s new online Family Resource Centre at http://www.hollandbloorview.ca/resourcecentre/. Topics include Parenting, Fun, Growing up, School, Respite, In hospital, Money and ‘My child has…’ Or drop by the Family Resource Centre on the main floor of Holland Bloorview where our family support specialists, social worker and parent mentors share resources on child disability and Holland Bloorview programs. For more information, call our Warmline at 1-877-463-0365.
BLOOM named one of best non-profit blogs
BLOOM was named one of nine top non-profit blogs in the world by Mark W. Schaefer, a well-known blogger at http://www.businessesgrow.com/blog, author and social media educator at Rutgers University.
BLOOM family
Keep sending digital photos of your child “in bloom.”E-mail to [email protected].
BLOOM blog & e-letter
http://bloom-parentingkidswithdisabilities.blogspot.com
Patient Declaration of Values
Read Holland Bloorview’s new Patient Declaration of Values, developed by our clients and families, at: http://www.hollandbloorview.ca/about/accountability/patient_values.php.
Connect with us through social media
Facebook: http://www.facebook.com/pages/Holland-Bloorview-
Kids-Rehabilitation-Hospital/107274595987209
Twitter: http://twitter.com/BloorviewPR
YouTube: http://www.youtube.com/user/PRBloorview
Issuu: http://www.issuu.com/hollandbloorview
Blog: http://bloom-parentingkidswithdisabilities.blogspot.com
Contest: http://www.filmpossible.ca
BLOOM is a how-to magazine on parenting children with disabilities. BLOOM gives voice to the joys and challenges of special-needs parenting by combining firsthand family insights and the best professional advice.
We believe that every child blooms in his or her own unique way.
BLOOM is published two times annually and mailed to Holland Bloorview families and parents and professionals who ask to be on our list.
CONTRIBUTORSPUBLISHED BY: Holland Bloorview Kids Rehabilitation HospitalWRITER AND EDITOR: Louise KinrossCREATIVE DIRECTOR & DESIGNER: Sara PurvesPRINTER: Continental Press
HOLLAND BLOORVIEW KIDS REHABILITATION HOSPITALHolland Bloorview is Canada’s largest children’s rehabilitation hospital. Our vision is to create a world of possibility for kids with disability. We pioneer treatments, technologies, therapies and real-world programs that give children with disabilities the tools to participate fully in life.
DISCLAIMERArticles in BLOOM are not a substitute for professional medical advice. Resources listed in BLOOM do not signify endorsement by Holland Bloorview. Where appropriate, please consult your physician.
CONTACT USEMAIL: [email protected]: 416.424.3866 or 800.363.2440FAX: 416.425.9332WARMLINE: 1-877-463-0365MAIL: Holland Bloorview Kids Rehabilitation Hospital150 Kilgour Road, Toronto, ON M4G 1R8
SUMMER 2011
BLOOM ~ summer ~ 2011 ~ 3
features
inthisissue
departments
PARENT TALK
06 The absence of normal ‘frees us’
10 One mother’s lesson: ‘He is just my son’
ROLE MODELS
14 ‘ He’s teaching siblings that they can speak out’
PARENT HEALTH
16 Respite needs to be ‘a way of life’
20 Real-world tips
PARTNERSHIP
22 ‘I’m not no one. I’m his mom.’
SCHOOL DAYS
24 Inclusion: One teacher’s experiment
GROWING UP
26 Tips for making friends
RESEARCH HITS
28 Game to boost fitness, friendship
30 Science roundup
TRAIL BLAZER
32 A good life, despite adversity
FROM THE EDITOR
04 Human worth: Are we looking in the wrong places?
FEEDBACK
05 Your letters
RESOURCES
31 Online and book shelf
YOUR KIDS IN BLOOM
35 Photo gallery
On the cover
The lack of normal expectations “frees us to be ourselves with each other,” writes The Boy in the Moon author Ian Brown of relationship with son Walker (p. 6).
4 ~ BLOOM ~ summer ~ 2011
fromtheeditor
Author Ian Brown has contributed a piece this issue addressing a central
question for parents of children with complex disabilities: What
is the value of my child’s life when he or she will not achieve conventional success (The absence of normal ‘frees us,’ page 6)?
I have struggled with this puzzle as my own son Ben becomes a young adult but does not follow the traditional path of university, independence and career.
Brown reminds us that human worth depends on perspective, and encourages us to “look in the right places.”
For him, that includes his son Walker’s ability to intensify a moment, making Brown examine it more closely, in essence slowing life down. Or Walker’s ability to express pure delight; as when, despite his father’s watchful eye, he succeeds in swiping whatever is on the table in front of them to the floor. “It’s as if he’s saying, really, how important is that newspaper/glass of wine/Blackberry?”
In a boy saddled by all that he can’t do, Brown writes, tricking his dad with the table clearings is liberation. “…If only for a moment, we are suddenly equals…We can relate to each
other not as we are supposed to, not as others insist we should, but as we can, in a way that makes that moment ours and ours alone.”Because he has no choice but to love Walker “as he is,” they are both freed to be “who we are, weary dad and broken boy, without alteration or apology.”
University of Houston social worker Brené Brown (not related) says her research into shame shows that people who feel worthy of love and belonging—as opposed to those who never feel good enough—embrace their vulnerabilities. This allows them to let go of who they ‘think’ they should be in order to be who they are.
Disability is a visible form of vulnerability. Typical bodies and minds mask a person’s inner world, which can be rife with feelings of fear, ambiguity and inadequacy. Children with complex disabilities can’t walk around like the rest of us, projecting an ‘I’ve got it all together’ image and pretending to be something they’re not. Perhaps that’s why they have much to teach us about acceptance, honesty and life in the moment.
Health professionals need to heed Brown’s admonition to “teach parents how to measure success in less obvious, less quantifiable, but equally important ways.”
Human worth: Are we looking in the wrong places?

BLOOM ~ summer ~ 2011 ~ 5
Although often well-intentioned
and enthusiastic, our support
services can forget they are not the
only ones (Repetitive strain, May
10)! Many parents of kids with
multiple disabilities visit several
clinics a year and it’s just not
reasonable to do everything. So it’s
up to parents to prioritize. A much
bigger, more philosophical issue:
the behemoth that is the healthcare
system must be accountable and
transparent. Fair enough. But the
very nature of it requires a level of
surveillance and reporting that I
think comes at a direct cost to the
family. The instruments and tools
that are used to create and measure
goals for each child are, I think,
primarily there for organizational
and administrative purposes. Some
(not all, I’m sure) being products
of the ‘fake work’ phenomenon I
wrote about.
Jennifer Johannessen, Toronto, online
Thank you for this quote today
(Day 1 at family-centred care
training, May 3) It is very thought
provoking. We do compare and we
shouldn’t. Each child is different
and brings with them their own
special gift. I remember when
Savannah started to lose her
abilities one by one and we had
a visit from friends that had a
‘normal’ child the same age...her
BFF (best friend forever). It was so
painful to look at her and compare
and see what Savannah couldn’t
do anymore. It is still a demon of
mine today as I see other children
that are the age she would’ve been
today. Next time, I will remember
your quote. Savannah taught me
so much about life and selflessness
through her special needs and
health issues...and I wouldn’t see
the beauty in the world now if it
wasn’t for her and that gift. I know
you probably feel the same way
about your son.
Diana Doyle, Los Angeles, online
Louise this is such a lovely piece
of writing (In each other’s eyes, we
are enough, May 2). Thank you
for sharing. I remember sitting
in the NICU reading Julia’s chart
hoping for some clarity about our
future. I will never forget the list of
dysmorphic features, a seemingly
random collection of critiques
of her appearance. I laughed at
‘depressed nasal bridge’ because
she’s half Chinese! Now I look back
and understand that these were
clues the doctors were using to seek
a diagnosis but I still feel that there
was a ‘disconnect’ between the
notes and the attitude towards this
person. My daughter is more than
a collection of features or a genetic
diagnosis.
Lisa, online
Thank you Barb for taking up the
call to change the way our medical
system views our children (For the
love of Annie, letter received Feb. 27,
2011). Your story is heartbreaking
and hits close to home. Our story
is vastly different, but the ethics
and values are much the same. My
son was a 25-week preemie, born
in Western Canada. His life was
endangered when the Neonatal
Unit viewed him as “not viable”
and determined that there was a
“90% certainty that, even if he did
survive, he would be so severely
handicapped that it would be
cruel to allow him to live.” (What
parent doesn’t read that as a 10%
chance of survival?) Thank God we
had one very determined doctor
who found him a bed, so that
he survived his neonatal period!
During his four months in hospital
I had to continually defend his
right to live, as did other parents
on the ward. One mother was so
tired of being told to “discontinue
treatment” that she pretended
she couldn’t speak English! Sadly,
others began to believe the doctor-
speak, and let their babies go. Now,
when I see my son smile, hear him
laugh, I think of those mothers, and
my heart breaks. I wonder what
it will take to remind the medical
community that life is precious.
Period. No imperfect babies. No
accidents.
Anonymous, online
Online
I love reading the magazine
(December 2010). The issues get
passed around here until they’re
dog-eared. I have used several
articles for training sessions for the
assistants here in the community.
Thanks for the incredible work
you are doing in transforming our
attitudes towards disability!
Jenn Power, L’Arche Cape Breton
I love the BLOOM issue from
December! It is fantastic, and I
take it everywhere I go for therapy,
appointments or other meetings
related to special needs. Everyone
that has looked through the copy
was impressed!
Sara Pot, Waterloo, Ont.
FROM THE MAGAZINE, E-LETTER & BLOG
feedback
Comment on these letters or send your own to [email protected]

6 ~ BLOOM ~ summer ~ 2011
The absence of normal ‘frees us’

BLOOM ~ summer ~ 2011 ~ 7
parenttalk
By Ian Brown
Without question the most common reaction people have, when they find out I have a seriously disabled son, is “I don’t know how you do it.”
It’s an interesting reaction, because in many ways, the act of physically caring for a boy like Walker (photo left) is the easy part. Walker is 14, looks about 10, and has the mental function of someone who is about two or three. It looks like he always will. He can’t speak, and because he can’t speak, I don’t know how well he sees or hears, or why he hits his head again and again if I let him, or where he’s in pain. He can’t swallow, so he has to be fed with a tube, and he can’t figure out the routine of going to the bathroom, so he has to wear a diaper. But those are easy problems to fix, albeit time consuming and sometimes a little dreary: a diaper is a diaper, and sometimes it is full and needs to be changed.
What I found more upsetting, practically from the day Walker was born, was a bigger and more unknowable question: did he have an inner life? Did he have any intentions, and therefore did his life have any purpose, any meaning?
That’s a hard question for any of us to answer, but it’s especially hard to answer for a boy who cannot speak or reason, and whose care consumes countless resources and many, many hours of human effort. Because I did that calculation too, when Walkie was an infant: if he lives at 10 per cent of human
capacity, and if the care of him reduces my wife and I to 30 per cent of our human capacity, and if my daughter Hayley is set back 30 per cent, because of him—well, add those up, and you have two and a half lives spent to sustain the so-called life of one broken boy.Is that worth it? I couldn’t tell, and so I spent a lot of time looking for some way of justifying his life, lived as it is in semi-darkness. I found proof again and again, if only I remembered to look in the right places. Walker’s life is not a success measured on any conventional scale of human success: he is never going to earn his living, never mind an income big enough to buy a fancy retirement home for his Mum and Dad; he is not going to go to Harvard or anywhere else that will make his parents proud; he is never going to invent a faster, easier way for people to spend money on the internet. The value of his life, if it has a value, will have to reside in his life, per se, in the sheer fact of his existence.
Gradually, I have begun to realize that he has a way of intensifying a moment, a way of making me take the time to look at it again, more closely, without an interfering agenda. He slows things down, and in the technology-mad world most of us scurry through, that is a valuable talent, even if it is not intentional. When his sister deigns to read to him (she has a busy life of her own) and his face lights up like a beacon, he forces me to pay attention to what is making him engage so intensely: his gorgeous sister, holding this weird contraption we call a book, chanting a story in the ancient rhythms human beings
Phot
ogra
phy
by P
eter
Pow
er/G
lobe
and
Mai
l

8 ~ BLOOM ~ summer ~ 2011
have used to make each other feel things since we first started telling stories. I don’t think he understands a single word, but he understands the importance of that hallowed ritual, and his pleasure is so intense and unfiltered and therefore contagious that I have no choice but to remember how important the act of sharing a story is—fundamental, you might say, to human existence. When I walk down the street with him, pushing his chair with my elbows so I can lean forward and talk into his ear, out loud, about the sights we behold on the boulevard before us—the return of the white miniskirt, for instance, or the popularity of the clunky Dutch bike in Toronto these days—he goes into thrills of glee. He can’t contribute to the conversation, but he apparently loves to be on the receiving end of one, to be thought of as someone who can listen and appreciate the fact that two people are talking about the world around them. I often forget how important that transaction is. But not when I am with him, because he will not let me forget it.
One of the things Walker likes to do when he’s with me is sweep anything on the table in front of me onto the floor. He knows I’m always watching for this act of subversion, and he waits and waits and waits until I am distracted for even a fraction of a second, and then he makes his move. It’s as if he’s saying, really, how important is that newspaper/glass of wine/BlackBerry? Then he throws his head back and laughs.
For a long time I worried this was evidence that he was a sociopath, that I’d end up one day nattering to him through the Plexiglas of the visiting room at Kingston penitentiary. I must have watched him do it 1,000 times, to my great dismay, before I stopped worrying about why he wasn’t behaving like a normal boy, and began to try to understand him as he was, a boy with an unusual and persistent habit. Eventually I figured out that Walker knows he is less capable than others (it makes him feel lonely and sad), and that the table clearings are a way for him to show me, once in a while, that he can trick me.
At those moments, if only for a moment, we are suddenly equals. I imagine this is a bit of a thrill for him, and even a liberation. But it is an especially great liberation for me, because it allows me to be his equal, in a context of our own making. Yes, smarty pants, I can say in all honesty: you got me that time. And I can be happy for his achievement. We can relate to each other not as we are supposed to, not as others insist we should, but as we can, in a way that makes that moment ours and ours alone. That is freedom—not only of the mind, but of the heart. It is one of the deepest and most unalloyed freedoms I have ever felt.
Walker gives me the opportunity to observe another human being, without self-consciousness: that is worth his weight in gold. (About 95 pounds worth, these days.) I get to love him as he is, because he gives me no choice, and so we can be who we are, weary dad and broken boy, without alteration or apology, in the here and now. He is the antidote to the stark emptiness of the survival of the fittest. He may not be much on the evolutionary scale—“a deleterious effect of nature,” a geneticist once called him—but in my experience he has few peers as a route to developing what Darwin himself in The Descent of Man called the evolutionary advantages of “the social instincts . . . love, and the distinct emotion of sympathy.”
parenttalk
BLOOM ~ summer ~ 2011 ~ 9
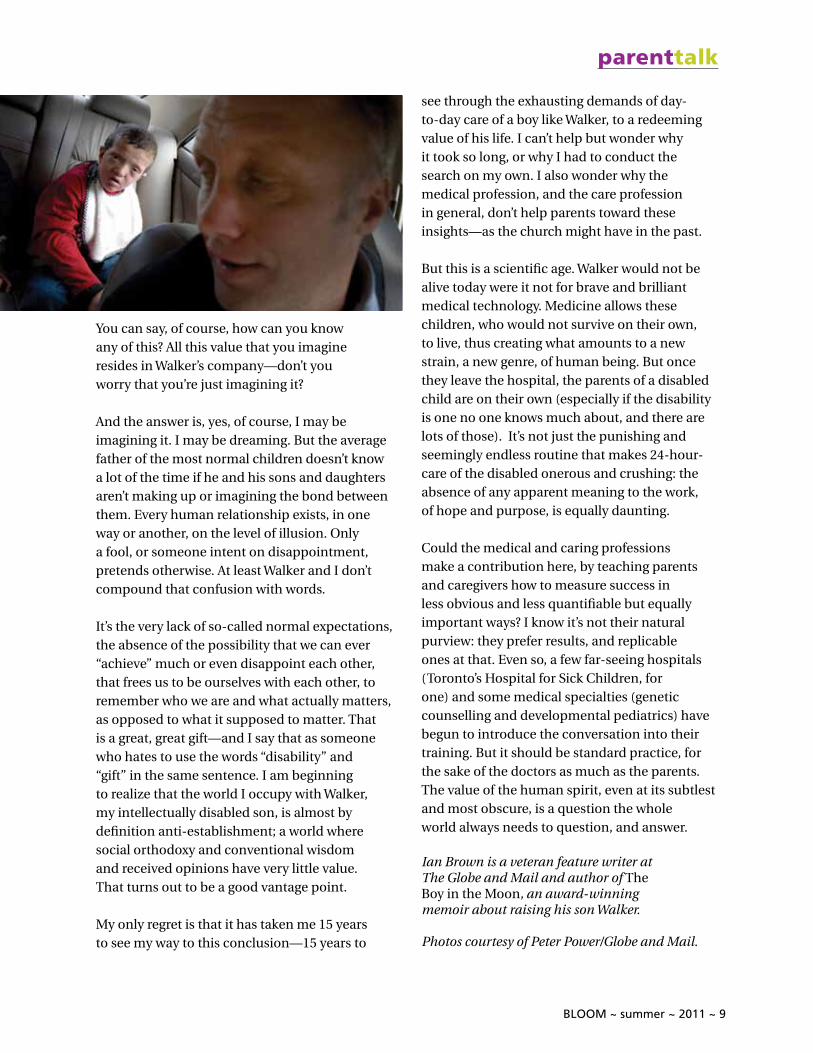
You can say, of course, how can you know any of this? All this value that you imagine resides in Walker’s company—don’t you worry that you’re just imagining it?
And the answer is, yes, of course, I may be imagining it. I may be dreaming. But the average father of the most normal children doesn’t know a lot of the time if he and his sons and daughters aren’t making up or imagining the bond between them. Every human relationship exists, in one way or another, on the level of illusion. Only a fool, or someone intent on disappointment, pretends otherwise. At least Walker and I don’t compound that confusion with words.
It’s the very lack of so-called normal expectations, the absence of the possibility that we can ever “achieve” much or even disappoint each other, that frees us to be ourselves with each other, to remember who we are and what actually matters, as opposed to what it supposed to matter. That is a great, great gift—and I say that as someone who hates to use the words “disability” and “gift” in the same sentence. I am beginning to realize that the world I occupy with Walker, my intellectually disabled son, is almost by definition anti-establishment; a world where social orthodoxy and conventional wisdom and received opinions have very little value. That turns out to be a good vantage point.
My only regret is that it has taken me 15 years to see my way to this conclusion—15 years to
see through the exhausting demands of day-to-day care of a boy like Walker, to a redeeming value of his life. I can’t help but wonder why it took so long, or why I had to conduct the search on my own. I also wonder why the medical profession, and the care profession in general, don’t help parents toward these insights—as the church might have in the past.
But this is a scientific age. Walker would not be alive today were it not for brave and brilliant medical technology. Medicine allows these children, who would not survive on their own, to live, thus creating what amounts to a new strain, a new genre, of human being. But once they leave the hospital, the parents of a disabled child are on their own (especially if the disability is one no one knows much about, and there are lots of those). It’s not just the punishing and seemingly endless routine that makes 24-hour-care of the disabled onerous and crushing: the absence of any apparent meaning to the work, of hope and purpose, is equally daunting.
Could the medical and caring professions make a contribution here, by teaching parents and caregivers how to measure success in less obvious and less quantifiable but equally important ways? I know it’s not their natural purview: they prefer results, and replicable ones at that. Even so, a few far-seeing hospitals (Toronto’s Hospital for Sick Children, for one) and some medical specialties (genetic counselling and developmental pediatrics) have begun to introduce the conversation into their training. But it should be standard practice, for the sake of the doctors as much as the parents. The value of the human spirit, even at its subtlest and most obscure, is a question the whole world always needs to question, and answer.
Ian Brown is a veteran feature writer at The Globe and Mail and author of The Boy in the Moon, an award-winning memoir about raising his son Walker.
Photos courtesy of Peter Power/Globe and Mail.
parenttalk
10 ~ BLOOM ~ summer ~ 2011
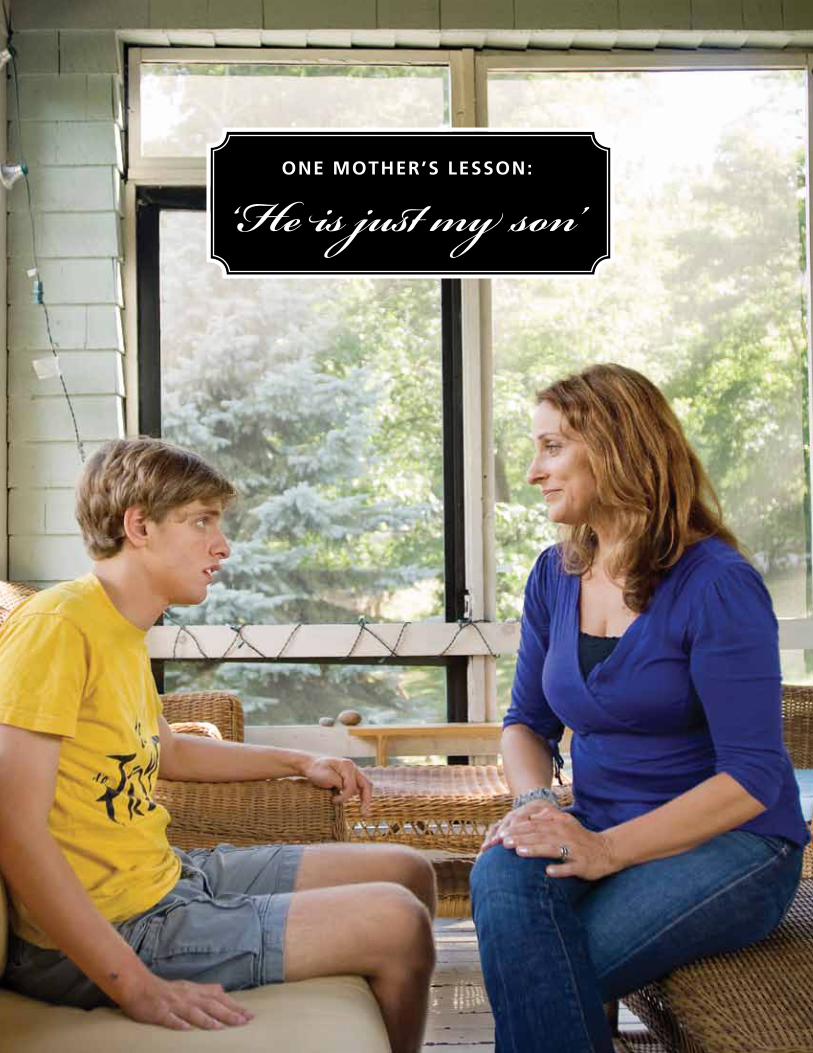
ONE MOTHER’S LESSON:
‘He is just my son’
BLOOM ~ summer ~ 2011 ~ 11
parenttalk
Nothing is ever what you think it’s going to be. Even if my firstborn son had not been autistic, motherhood was crazy different from anything I had ever experienced or been prepared for. From the moment that my ‘birth plan’ of soft lights, music and foot massage was scrapped in favour of a strong epidural, life with Nat (photo left) was a wild ride. When I think about myself in those early days, 21 years ago, I feel maternal and protective. I was so scared, before I even knew about the autism; a gauzy gray fear was wrapped around everything I experienced as a new mom. I think I was sensing autism, almost from the very beginning. I felt it when I looked at Nat, and it just kind of seemed like he would be content without me, like he didn’t need me. His smile was always inward. And very quickly, as the developmental phases unfolded mostly normally over the months, I learned what it was like to be plagued with self-doubt. I felt something was wrong, but nobody else did. No one believed me. Nat’s diagnosis marked a huge change in our lives, a huge change in me. It wasn’t just the focus it gave me, of needing to learn and learn fast; it was also the awareness that I had been right. Little scared new mother me, imagine that! It turned out I had a mother’s instinct par excellence! If I were to give the young me any pearls of wisdom gleaned along the way, I would start
with this lesson about intuition. I would say, “Trust your gut; you know your child best.” The sooner I realized that I did know about Nat, the better I felt. The stronger I felt. I think that we need to feel strong as a first step towards dealing with autism. Strength breeds clarity, and from clarity comes vision, perspective. Getting clear about what is around you marks the early days post-diagnosis, but there will always be the need to focus and understand, even when your child is older. The important thing is to know your kid, and then figure out what’s important—to you and your family. Early on, I knew that I wanted to be able to take family vacations the way I had with my family growing up. I did not want autism to stop that. And yet, it was so hard taking Nat to new places that I almost did give up the desire. Until one night, just before Thanksgiving, when I grumbled that there were no books that could help someone like Nat get through the holiday. “Why don’t you make it yourself?” my husband Ned asked, making it seem simple and obvious. Making me feel like I could do it. And so I did, cutting up family pictures and sticking them together to flimsy pages, telling the story of what Nat’s Thanksgiving would be like, and showing him the familiar faces he would see. And Nat was delighted with it. This type of “Nat Book” became our first strategy for taking Nat to new events. It was a successful strategy both for Nat and for me, because it strengthened
By Susan Senator
Phot
ogra
phy
by Ja
red
Leed
s
12 ~ BLOOM ~ summer ~ 2011
my conviction that I did know what to do. Over the years Ned and I developed this kind of pattern, where we would talk together (grumble and grouse) about a problem we needed to solve, and together we would come up with some kind of solution. And later on, we would look back on the problem and it would be part of our “couple culture,” a phrase I coined for our history together. There are so many old Nat stories we laugh about now, simply because we survived them. Like the time I caught him carrying poop from one toilet to another, simply because the first toilet was not working. “Ah, good times,” my husband will say sarcastically, and we’ll laugh. Laughing makes the event into something contained, shared and safe. It also makes you feel like you have a good life, after all. And who is to say you don’t? I did not learn the most important lesson about being Nat’s mom until he was in his early teens. We were sitting on the living room couch together and he was being horrible. He was loudly and hysterically fake-laughing. He had been doing this for months. We could not ever get him to stop. But in that moment, that late afternoon, I kind of gave up trying. I just started poking him and tickling him, saying, “What’s so funny, you? Huh?” And suddenly we were laughing together. Real laughter. This struck me to my core. I think that any remaining shreds of old fear fell away then, as I realized the most important thing of all: Nat is just a kid. Not a creature, not a disorder, not a freak of nature. He is just my son and that is that. Knowing that, feeling that, is the secret of making peace with autism.
Susan Senator is the author of Making Peace with Autism and The Autism Mom’s Survival Guide. Follow her at http://susansenator.com/blog.
Photos by Jared Leeds.
How to make peace with autism
1) When trying something new, set realistic goals and have fairly low expectations. Then you can define your own victories.
2) If no one can tell you what to do, find your own solution. There’s no right or wrong, only what works.
3) Give yourself a break. There are terrible times in every family’s life. Know that it will pass. Lay low until it does.
4) Never say never. You just don’t know what your kid may be capable of when he’s little. Keep an open mind and try failed things again later. Developmental delay means all bets are off. A lot happens later than the books say.
5) Don’t compare your family’s insides to another family’s outsides. You never know what life is really like for anyone else.
6) Assume your child understands more than he appears to. Autism is often about communication difficulties, not about being anti-social. Assume the best and that’s what you’ll get.
7) Fall in love with your child. Let yourself glory in his cute face, his small gains, his moments of beauty. Be on the lookout for them and you’ll see them more and more.
parenttalk
BLOOM ~ summer ~ 2011 ~ 13
‘He is just my son and that is that. Knowing that, feeling that, is the secret of making peace with autism.’
14 ~ BLOOM ~ summer ~ 2011
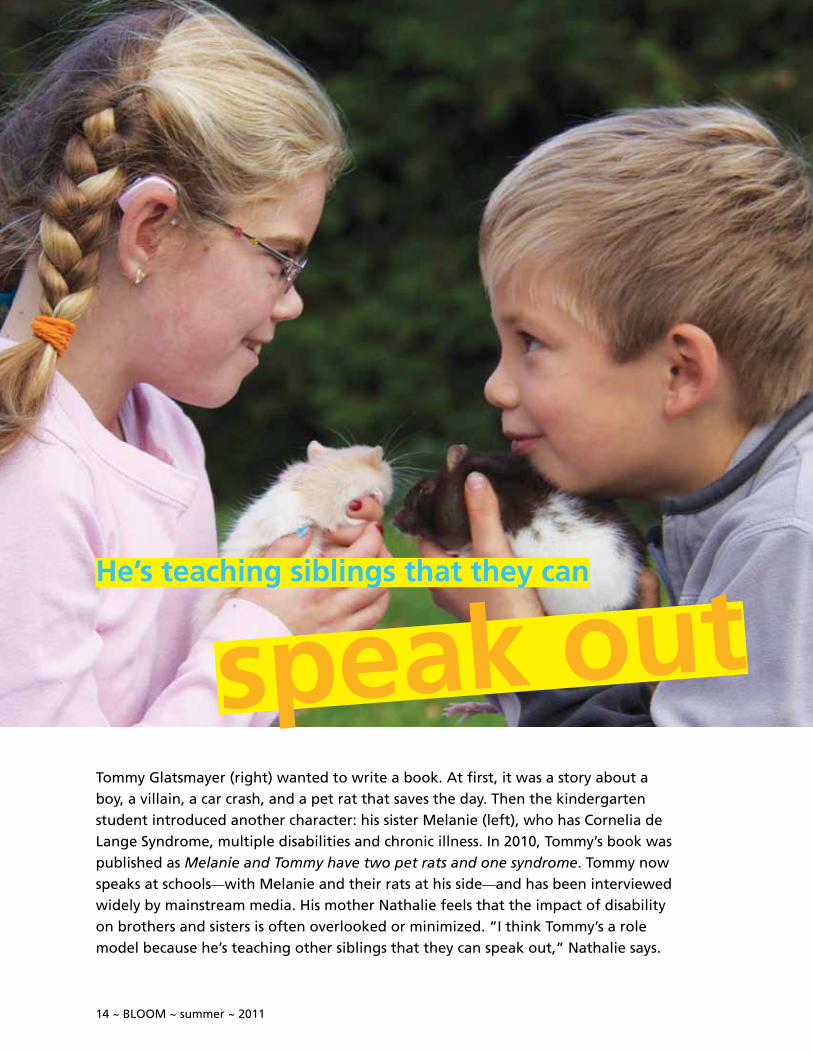
Tommy Glatsmayer (right) wanted to write a book. At first, it was a story about a boy, a villain, a car crash, and a pet rat that saves the day. Then the kindergarten student introduced another character: his sister Melanie (left), who has Cornelia de Lange Syndrome, multiple disabilities and chronic illness. In 2010, Tommy’s book was published as Melanie and Tommy have two pet rats and one syndrome. Tommy now speaks at schools—with Melanie and their rats at his side—and has been interviewed widely by mainstream media. His mother Nathalie feels that the impact of disability on brothers and sisters is often overlooked or minimized. “I think Tommy’s a role model because he’s teaching other siblings that they can speak out,” Nathalie says.
He’s teaching siblings that they can
speak out

BLOOM ~ summer ~ 2011 ~ 15
rolemodels
BLOOM: Describe Tommy.
Nathalie Wendling: Everyday is Christmas for Tommy. He wakes up super excited every morning. He loves to help people and is very social. He’s easy going and doesn’t get upset often. He loves his pet rat. He loves to create things—like taking all the recycling in and building something. He loves people and having friends over. He likes sports and adventure.
BLOOM: How has Tommy been affected by Melanie’s syndrome?
Nathalie Wendling: I don’t think we understand, as parents, the extent of how siblings feel. I think they have a lot of stress socially. They can be embarrassed about their sibling in social situations. I think at home Tommy feels my stress as a parent. By the time I get to Friday I’m exhausted trying to get Melanie out of bed on time and he’ll have a five-course breakfast laid out for me. If Melanie’s having a bad day and I’m almost in tears, he’ll do something to lighten the moment.
BLOOM: So Tommy compensates by being helpful?
Nathalie Wendling: Yes. At age five, he was cleaning the bathrooms and vacuuming. At age six he was making scrambled eggs and French toast. At seven he shovelled our driveway, the neighour’s driveway and the whole court. At other times he might act up if he feels Melanie’s getting too much attention. It takes me about 45 minutes every morning and night to get Melanie out of bed or to put her to bed. She needs ear drops, nose spray, hearing aids, her teeth brushed, to be dressed, and her medication. I started to notice that Tommy would misbehave then. It was his hardest time of the day. It’s almost like he wants his own 45 minutes of intense time with me.
BLOOM: Has Tommy ever said he wants more attention?
Nathalie Wendling: No, he hasn’t articulated that. But last Christmas, when they saw their cousins, who are the same ages, I think it hit him how behind Melanie is in everything. “It’s so weird, if Melanie was normal she’d have an iPod and be doing this and that,” he said. But by the end of the conversation, he’d found a positive: “We’re lucky that Melanie has a syndrome because we never fight,” he said. He had noticed that all of the other siblings fought at this age and took the positive over the negative.
BLOOM: It’s obvious in the book that Tommy loves Melanie.
Nathalie Wendling: He always wants to participate in helping her achieve things. For example, recently he taught her about the planets. But he did it for three hours, five days in a row! It took three years for Melanie to learn the letter P and
Tommy worked at it with her for almost three years. Melanie tends to want to play in her own world, and Tommy does everything he can to get into that world to play with her.
BLOOM: How did the book come about?
Nathalie Wendling: We wrote the book together. Tommy was in charge of the story. He wanted to make it funny enough to entertain his friends while still educating them about Melanie’s syndrome. In Grade 1, Tommy came home devastated because his friends were making fun of Melanie. We had never seen him cry so hard. He loved his sister and couldn’t understand why they were being so mean. As
speak out
Continued on page 34
16 ~ BLOOM ~ summer ~ 2011
Respite‘It needs to be a way of life’
BLOOM ~ summer ~ 2011 ~ 17
parenthealthRespite Tim and Gina Gort of Grand Rapids, Mich. have three children: Gwendolyn, 8, Violet, 2, and Eliza, 1 (photo left). Gwen and Eliza have cerebral palsy and use g-tubes and Gwen has a tracheotomy for breathing problems. This year Tim and Gina each took a week long respite or ‘retreat,’ on their own, while the other parent held the fort at home. The family has nursing care during the day, but supports the children alone at night. “As Gwen got older, and then Eliza came along, I realized respite needed to be more than a break—it needed to be a way of life,” says Gina. The Gorts share how they’re making ‘time away’ an essential part of their lives.
BLOOM: Why is respite critical?
Tim Gort: The most important thing is to acknowledge that you can’t handle things anymore and you need a break. The alternative is to become burned out or inoperable or to take out your stress and sleep deprivation on your spouse. For me, it was a lot of things. I had been running on auto-pilot and then Eliza’s diagnosis pushed me over the edge. By removing yourself from the situation you clear your head and have a deeper appreciation for your family and children and what they’ve taught you. You come back refreshed and re-energized.
Gina Gort: I have to go away to not only get a break and get rejuvenated, but to come back with tools and ways to be in my situation and be okay with it. Now everyday I make time to write and I make time to meditate. Respite is now something we implement on a weekly basis. We have date nights. On Tuesday night we separate and Tim may go to a support group or go golfing and I may go to a writers’ group. On Friday we do something together that’s romantic, if possible. This is new for us and it’s taken us a long time to get to this point.
BLOOM: What supports do you have for date nights?
Gina Gort: Nurses and a babysitter. It’s extremely hard letting go and getting to a trust point. Especially with Gwen, who has respiratory issues. You have to accept that these people are caretakers, they’re not you and they won’t do things exactly the way you do them. But you give them the best tools and a ‘dos and don’ts’ list and you trust in them. You need to be able to walk out the door, mentally and physically.
BLOOM: Describe the 10-day retreat you went on Gina.
Gina Gort: I chose to go to a convent. I wanted to make a drastic change in my life. I felt that by going away to a place where I could be silent, in retreat, I could re-examine myself and look at who I am and how I’m defining myself. Every day I met with a spiritual guide who is a sister. I’m not religious at all and she was very open to that. She would prompt me with questions and I’d spend the day reflecting on my answers. One question was: “If you could go back and change your life, what would it look like and how would things have to be for you to be happy?” Initially I saw
By Louise Kinross

18 ~ BLOOM ~ summer ~ 2011
myself at our cabin on the lake and I saw Gwen walking on the beach and I saw Eliza sitting up. And then it shifted and I thought “I don’t need my children to be normal to be happy.” I’m already happy and I need to accept what I have and go forward and stop looking back and saying “What if, what if?” I did meditation in the morning and yoga, reading, writing and reflection.
BLOOM: What impact did the retreat have on you and your family?
Gina Gort: It was huge. I have patience. I’m more honest with myself and therefore I can be honest with Tim. I’m not thinking three steps ahead. I’m really focused on being in the now and loving it. My relationship with Gwen has always been difficult, but since I’ve been back it’s been
totally different. It’s like we’re on the same page. There was a time I would get angry and resentful towards her because I was strung out. Now I’m patient with her and she can feel the difference.
BLOOM: Tim, what activity did you choose for respite?
Tim Gort: I chose to go to the Smoky Mountains to do a backpacking trip. I needed to do something physical because I felt like there was a lot of grieving that I had to do—not only about the acceptance of Eliza but with other issues and with Gwen. I needed to break my body down physically before I could work on the mental stuff. I hadn’t had a physical outlet for a couple of years. I was able to be gone long enough to really miss my family and really want to come back. I
BLOOM ~ summer ~ 2011 ~ 19
feel like my physical self is ready to go forward, but my mental self is still lagging behind. I’m working on getting another therapist that can help me with both. And I’m thinking about a second, seven-day retreat, maybe at a monastery.
BLOOM: How can you afford these longer respites?
Gina Gort: At the convent I paid $80 dollars a day and that included three square meals, a place to sleep and a spiritual director. When I hear people say they can’t afford respite, I say look at your tax returns. When someone asks you what you want for Christmas, say you want to go on a respite. Have a garage sale and put the proceeds to a respite. It’s necessary.
BLOOM: How did you manage your children’s care on longer respites?
Gina Gort: We have nurses during the day and on the night shift, each of us is on our own. Tim was the major caretaker when I was gone. Violet was able to spend some time with relatives. We know that as part of our relationship we have to support the other person and that our workload will double. For people who are single parents, you have to lean on whatever support group you have.
BLOOM: I haven’t heard of many parents taking these retreats.
Gina Gort: Parents in our community have been astounded and shocked. We’re teaching them and they’re excited and ready to try this for themselves.
Tim Gort: The breaking point for us was Eliza’s diagnosis. We were going through life with an older child with CP and had a second child. When we decided to have Eliza, we assumed everything would be fine, just like Violet. When it wasn’t, it was a complete shock to our system. We had already been through eight years with Gwen and we were starting over with another child with special needs. It brought up all the issues we thought we had covered—the emotions, the
grieving. We were even seeing some of Gwen’s old therapists! Being able to see Eliza’s future in Gwen was very difficult and it’s still very difficult for us to separate them and not compare them. Then there’s the grieving for Violet, who is the 2-year-old sandwiched between two kids with CP. The reason we wanted to have a third was so that Violet would have a playmate.
BLOOM: What other advice would you give to parents in similar situations?
Gina Gort: We’ve solved a lot of our issues just by talking to a therapist and then coming up with our own solutions. Having a third party to observe and help you along has been critical for me. We’re both writers so we do a lot of self-discovery through writing. You don’t have to be a writer to keep a journal. Journaling doesn’t cost any money and if you just write down what happens that day, it often transforms into how you’re feeling, and then ‘why’ you’re feeling that way.
BLOOM: Do you rely on extended family for care?
Gina Gort: Other than with our middle child, it’s very minimal. They have to work through their own grief. Everything relies heavily on Tim and I working as a team and thank God we have nursing staff now.
Tim Gort: We’ve also built our own support system by finding the right friends and thinning ourselves from people who don’t support us. We have a lot of friends we can count on for meal support or for emotional support.
BLOOM: How often do you plan to take a longer retreat?
Gina Gort: I plan to do it once a year.
Learn more about the Gorts on their blog at The Gort Family (http://thegortfamily.blogspot.com/).
20 ~ BLOOM ~ summer ~ 2011
What is respite?
It’s an opportunity for your child to enjoy activities with others at home or in the community while you get a much-needed break and re-energize.
Respite is not one place or thing. It can be a worker taking your child to the park, pizza place, exercise club or zoo. It can be a worker, family member or friend cooking with your child at home or shooting hoops in the driveway.
It can be an arts program you drop your child off at in the community, a day program or an overnight stay in a hospital.
Respite works best when you build strong relationships between your child and family and the respite worker or community program.
How do you find respite workers?
Be on the lookout for people who naturally connect with your child. It could be an assistant at school, a swim instructor, a camp counsellor,
a retired teacher or a university student who wants to learn a skill like sign language.When you visit your child’s rehab hospital or attend a workshop, network with other parents. Find out who they use.
Visit your local community centre, coffee shop, college, place of worship or library and talk to people. You never know where you may find a caring person with skills who can connect with your child.
Post an ad at high schools and universities for students who may want experience. Register with www.respiteservices.com to take advantage of their worker database. Ask your children’s treatment centre for a list of formal respite programs. Some parents have found excellent workers through Craigslist. Remember, you have to interview and screen people no matter where you source them.
Respite workers don’t stay forever, so keep networking to ensure you have the support you need over time.
Real-world tips:Respite careThese tips were developed with input from parents of children who have physical and developmental disabilities, as well as complex medical problems and autism.
BLOOM ~ summer ~ 2011 ~ 21
parenthealth
What do you look for in respite workers?
There is no ‘perfect’ respite worker. Look for someone who connects well with your child and has interests or skills that can benefit your child. Parents recruit workers for different roles. Perhaps you want a male worker who can play basketball with your teenage son. Maybe your child enjoys nature and you find someone who loves to garden. Look for people who are motivated to learn skills in areas that meet your child’s needs. For example, a student who wants to learn sign language or someone who’s a whiz at technology and enjoys programming your child’s voice device.
How do you keep respite workers?
Invest time in your worker. Initially be present so that you can model what works best with your child. Be open to questions. Make working with your family fun, rewarding and convenient. Create learning opportunities that fit with your worker’s interests (e.g. a student who wants to be a physiotherapist attends therapy with your child).
When it’s convenient, offer to pick your worker up or drive them home. Recognize your worker and remember little things, like birthdays. Make sure your worker is comfortable with the hourly rate you pay and feels valued.
Some respite arrangements may not involve money. For example, one dad pays gas money for a friend to visit and read with his daughter in hospital. Another provides workers with a laptop or Blackberry during visits. The child and worker have fun with the technology and send photos of their activities to the parent. One mom takes advantage of a Sunday morning respite program run by students from a Jewish high school.
Never take your respite worker for granted!
How do you get funding for respite?
Ask the social worker at your children’s treatment centre to help you fill out government forms such as Special Services at Home (http://www.children.gov.on.ca/htdocs/English/topics/specialneeds/specialservices/index.aspx). Your social worker can also tell you about charitable foundations that fund respite.
Where can I learn more?
Visit www.respiteservices.com or the Family Resource Centre at Holland Bloorview. Or ask the social worker at your children’s rehab centre.
What parents say:
“Respite is about my boys having fun, getting to go out and explore and be happy and do things with other people.”
“I look at respite as a day off for a parent to do the things they couldn’t do before. I may attend an appointment. It could be having a coffee and reading the paper. You’re able to relax your mind and re-energize. It takes away the constant worry.”
“It can be hard to trust someone else. You think no one can take care of your child the way you do. But it’s important to let go. You want to be healthy for your child over the long term. If you don’t take respite, you burn out.”
“You have to invest time in your workers. It’s not ‘here you are, take my kid.’ You spend time building a relationship and giving them the tools to be successful.”
“I want my child to be visible in the community, not isolated, and respite workers get her out there.”
By Louise Kinross

22 ~ BLOOM ~ summer ~ 2011
I’m hismom’‘I’m not no one.

BLOOM ~ summer ~ 2011 ~ 23
partnership
I think the most engaging presentation at the patient- and family-centred care conference in St. Louis in May was by Jim Conway, a lecturer at the Harvard School of Public Health.
Jim talked about an experience in the 1970s that woke him up to the essential role of parents in the care of hospitalized children.
He was an administrator in radiology at Children’s Hospital Boston and explained to a mom that she couldn’t accompany her child into the x-ray room. “I don’t care who you are, I’m staying with my kid,” she said. When he pointed out the sign that said “no one” was allowed through the door, the mom said: “I’m not no one. I’m his mom.”
During his 27 years at Children’s Hospital he learned that if there was a discrepancy between a child’s hospital health record and the mother’s account, they were to go with what the mother said, because “we were only taking care of a piece of that child and she was taking care of the whole child.”
Since that time, hospitals that are committed to partnering
with families have stopped viewing parents as ‘visitors’ and allow 24/7 access.
Jim said family-centred care occurs when patients and families are treated as partners in care at every level: from their participation on key hospital decision-making bodies to their input at the bedside. “Patient- and family-centred care isn’t an advisory council,” he said. “That’s just one piece.”
Leaders play a critical role, he said, communicating in words and actions that the patient’s safety and wellbeing guide all decision-making. The entire system is organized around the choices and needs of patients and families.
Jim shared research that shows that patient- and family-centred care reduces length of stay; lowers cost per case; reduces adverse events; improves employee retention; reduces operating costs; decreases malpractice claims; and increases market share.
A recent study in the International Journal of Health Care Quality showed that hospitalized patients who participated in their care cut adverse events in half.
The team of Holland Bloorview staff who just attended the Institute for Patient- and Family-Centred Care training
came back with two plans to improve the practice here. The first is to include clients and families in bedside rounds, and the second is to incorporate family storytelling into meetings throughout the organization to illustrate client- and family-centred behaviours.
Through Holland Bloorview’s new family leadership program, parents sit as advisors on key hospital decision-making committees; mentor other families; and share their firsthand stories with staff to improve how we deliver care.
Jim said patient- and family-advisory councils are mandatory in Massachusetts hospitals and 93 per cent of health leaders surveyed in 2010 said the patient experience was one of five top priorities.
He concluded by saying that patients and families are the only people who know the ins and outs of your hospital and that if healthcare is on the table, patients and families have to be there too.
The Institute for Patient- and Family-Centred Care has excellent materials on their website: http://www.ipfcc.org.
By Louise Kinross
mom’
Phot
ogra
phy
by W
illia
m S
uare
z
24 ~ BLOOM ~ summer ~ 2011
schooldays
Sheila Dobson (above with son Ben) teaches a class for students with developmental disabilities at Sutton District High School in Ontario. She and colleague Andy Hagerman designed a three-week unit called Inclusive Recreation to bring together four classes for students with disabilities with a regular Grade 11/12 Recreational Leadership class. She shares the challenges and rewards of her first experiment with inclusion.
I started teaching special education two years ago, after being a guidance counsellor for most of my career. I knew very little about inclusion, other than being the parent of a child with autism and the joy and heartache that seem to be part of that territory.
I was looking for ways for my students to get to know students in the mainstream and for the mainstream to get to know my students. It’s not that anyone is unkind to my students, but there’s a barrier: it’s like being on different sides of the glass and not being able to communicate. I was searching for a way to make the glass disappear; for our kids to know each other as peers.
Andy and I designed the unit on Inclusive Recreation with ordinary high school kids in mind. The Grade 11/12 class we partnered with is not remarkable. They’re not gifted or
elite athletes. They’re just ordinary kids texting at the back of the class and wondering what they’re doing on the weekend. When we began the unit we talked first about the necessity for honesty—that if they couldn’t ask me the questions they were thinking, or if they felt constrained by using correct language or being ‘nice,’ we probably wouldn’t get far. We did some exercises to help them identify how they felt about disability and inclusion. I asked what words came to mind when they thought of a person with a disability. They wrote about being sad and afraid. They talked about the randomness of a person’s movements, verbalizations that were unclear and a general lack of understanding. This allowed us to have the honest discussions we needed to have before the students could begin interacting together. We used a few articles
By Sheila Dobson
Inclusion: One teacher’s experiment
BLOOM ~ summer ~ 2011 ~ 25
schooldays
from BLOOM to create some context for them, and we had some discussion about the ‘why’ of inclusion, with the emphasis on everybody benefitting. We did a disability simulation where they had a chance to use wheelchairs or experience certain types of disability, such as navigating the school wearing a blindfold.
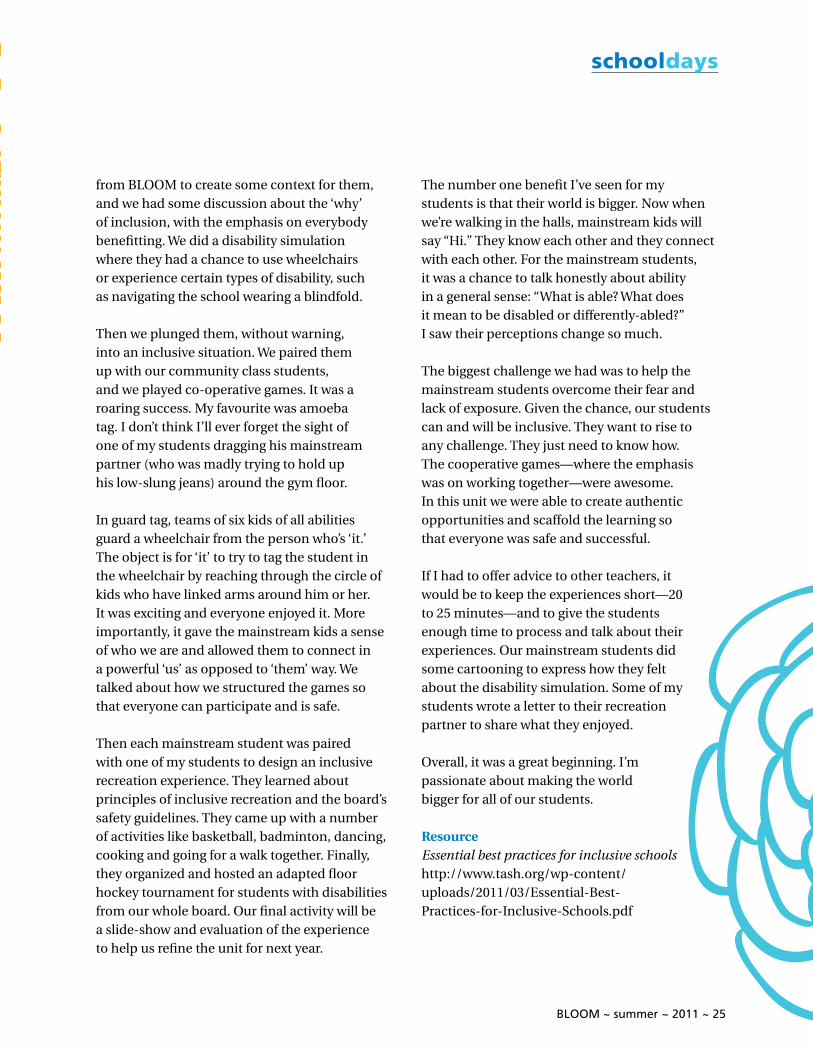
Then we plunged them, without warning, into an inclusive situation. We paired them up with our community class students, and we played co-operative games. It was a roaring success. My favourite was amoeba tag. I don’t think I’ll ever forget the sight of one of my students dragging his mainstream partner (who was madly trying to hold up his low-slung jeans) around the gym floor.
In guard tag, teams of six kids of all abilities guard a wheelchair from the person who’s ‘it.’ The object is for ‘it’ to try to tag the student in the wheelchair by reaching through the circle of kids who have linked arms around him or her. It was exciting and everyone enjoyed it. More importantly, it gave the mainstream kids a sense of who we are and allowed them to connect in a powerful ‘us’ as opposed to ‘them’ way. We talked about how we structured the games so that everyone can participate and is safe. Then each mainstream student was paired with one of my students to design an inclusive recreation experience. They learned about principles of inclusive recreation and the board’s safety guidelines. They came up with a number of activities like basketball, badminton, dancing, cooking and going for a walk together. Finally, they organized and hosted an adapted floor hockey tournament for students with disabilities from our whole board. Our final activity will be a slide-show and evaluation of the experience to help us refine the unit for next year.
The number one benefit I’ve seen for my students is that their world is bigger. Now when we’re walking in the halls, mainstream kids will say “Hi.” They know each other and they connect with each other. For the mainstream students, it was a chance to talk honestly about ability in a general sense: “What is able? What does it mean to be disabled or differently-abled?” I saw their perceptions change so much. The biggest challenge we had was to help the mainstream students overcome their fear and lack of exposure. Given the chance, our students can and will be inclusive. They want to rise to any challenge. They just need to know how. The cooperative games—where the emphasis was on working together—were awesome. In this unit we were able to create authentic opportunities and scaffold the learning so that everyone was safe and successful.
If I had to offer advice to other teachers, it would be to keep the experiences short—20 to 25 minutes—and to give the students enough time to process and talk about their experiences. Our mainstream students did some cartooning to express how they felt about the disability simulation. Some of my students wrote a letter to their recreation partner to share what they enjoyed.
Overall, it was a great beginning. I’m passionate about making the world bigger for all of our students.
ResourceEssential best practices for inclusive schoolshttp://www.tash.org/wp-content/uploads/2011/03/Essential-Best-Practices-for-Inclusive-Schools.pdf
26 ~ BLOOM ~ summer ~ 2011
friendship
BLOOM ~ summer ~ 2011 ~ 27
growingup
Friendships are at the heart of a good life. But they may not come naturally for some children with disabilities. Perhaps the child isn’t able to speak, doesn’t understand social cues or is so busy in therapy she doesn’t have time to “hang out.”
Holland Bloorview life-skills coaches Natalie Timbrell and Sarah Keenan say it’s important for kids with disabilities to know that it’s hard for many people to make friends. They offer these tips to parents:
k Get your child involved in fun activities early on. Find out what they like and don’t like. Help them develop interests, because common interests foster friendships. Be active in your community. Ask your child what qualities they look for in a friend. Emphasize that friendship is reciprocal and takes work (some children with disabilities have developed a learned passiveness).
k Teach and role-play social rules. Practise an opener to a conversation and how to keep a conversation going (answering “yes” and “no” isn’t sufficient.). For example: “Do you like movies?” “Yes. I like
action movies. What about you?” Role-play awkward social situations and how your child can respond. Have your child practise social skills when out in the community. Practise what to say on the phone.
k Teach your child to use technology. “The number one way teens communicate today is through texting,” Natalie says. “Everything is electronic. If your child is not a part of that, they’re missing out. Educate your child on how to use e-mail and Facebook and how to use it safely.” Check out Ability Online, an online community where youth with disabilities can connect. Ability Online is monitored by volunteers and mentors: http://www.abilityonline.org.
Support networks
A support network—or friendship circle—is a group of people who intentionally come together to support the wellbeing, safety and health of a child or adult with disability. “We all need people we can connect with, who inspire us, support us and share common interests,” says Susan Beayni of Plan Toronto, which helps families
plan for their child’s future. Support networks, which can include peers, family, friends and acquaintances, identify a child’s gifts and passions and work as a team to brainstorm ideas for how the child can contribute in the community. They improve a child’s life in the present and lay the groundwork for continuing friendships, support and connections when family members have died. Safe and Secure, by Al Etmanski, 2010, has a great chapter on creating support networks. Go to www.plantoronto.ca and click on the picture of the book to download worksheets.
Other resources
Circle of friends, Robert Perske, 1992
Friendships and inclusion: Five steps to approaching friendships, Peggy Hutchison and John and Karen Lord, 2011
Friendly facts: A fun, practical, interactive resource to help children explore the complexities of friends, Margaret-Anne Carter, 2010
It’s okay to be different, Todd Parr, 2009
We come bearing gifts, Janet Klees, 1996
By Louise Kinross
Phot
ogra
phy
by W
illia
m S
uare
z
Tips for making friends

28 ~ BLOOM ~ summer ~ 2011
researchhits
Game to boost fitness, friendship
Scientists at Holland Bloorview and Queen’s University
are developing a virtual-reality game that promotes
fitness and social networking for teens with cerebral
palsy. BLOOM interviewed Dr. Darcy Fehlings, co-principal
investigator, to learn more about this two-year project.
BLOOM ~ summer ~ 2011 ~ 29
researchhits
BLOOM: What is the goal of this research?
Darcy Fehlings: To develop a fun, virtual-reality game that youth with cerebral palsy can use to improve their fitness and interact with other kids through a social-networking platform.
BLOOM: Why is exercise important for teens with cerebral palsy?
Darcy Fehlings: We find that they grow a lot in their teenage years, but their muscle strength doesn’t increase, so they become more tired when moving and that leads to a decrease in fitness. Their body is bigger, so there’s more mass to move, but they don’t have an increase in muscle strength. Our study is focused on kids who are using a walker and who might typically have moved to a wheelchair for longer distances. We want to develop a game that’s fun and keeps their muscles strong so they can continue walking with a walker.
BLOOM: What would the game look like?
Darcy Fehlings: The teen will hold a playstation controller that moves an avatar. They will sit on a recumbent bike in front of a computer or TV at home, and the faster they pedal, the more they control the game. Queen’s University has a lot of expertise in modifying games so that if two students have different fitness levels or physical disabilities, they will be perceived as equal. Their effort will result in the same impact. So no one will be discouraged because they’re playing with someone at a different ability level. Dr. Nicholas Graham is the co-principal investigator at Queen’s.
BLOOM: How does the game improve a person’s fitness?
Darcy Fehlings: The bike gives them a cardiovascular workout and builds leg strength.
But we’re not only interested in improving physical fitness. We want to engage teens in the social networking aspect of the game. They will participate in the design of the game so it’s something they’re interested in.
BLOOM: Is there anything like this on the market?
Darcy Fehlings: Nothing that’s geared to youth with cerebral palsy and physical mobility issues. We’re taking advantage of the explosion of virtual-reality exercise programs on the market. What’s also unique about our project is the idea that we can use networking to decrease social isolation.
BLOOM: How will the game be developed?
Darcy Fehlings: We have a collaborative team of experts in cerebral palsy, virtual-reality exercise, programmers and our youth with cerebral palsy. They will work together in focus groups to develop the game concept. The virtual platform is already in place so we need to develop the game more from the storyline perspective.
BLOOM: How will the game be tested?
Darcy Fehlings: We will do baseline testing of fitness level, whether they’re still able to use their walker, how much they walk each day and social quality of life.
BLOOM: Who is funding the project?
Darcy Fehlings: It’s being funded by NeuroDevNet, a Canadian Network of Centres of Excellence. NeuroDevNet’s focus is to bring together basic scientists and clinicians working with children with cerebral palsy, autism and fetal alcohol syndrome. For more information, call 416-425-6220, ext. 3613.
By Louise Kinross

30 ~ BLOOM ~ summer ~ 2011
researchhits
Chronically ill children 88 per cent more likely to suffer physical abuse
Children with chronic health conditions are 88 per cent more likely to suffer physical abuse than healthy children, according to Swedish research published in Acta Paediatrica. They are also 154 per cent more likely to suffer a combination of physical abuse and exposure to intimate partner violence than their healthy school friends.
Scienceroundup
Autism takes toll on dads
Over 30 per cent of fathers of grown children with autism experience symptoms of depression that warrant clinical attention, according to a study presented at the International Meeting for Autism Research in San Diego. Researchers found fathers of young adults with autism experience high levels of depression and are pessimistic about what the future holds, much more so than fathers of kids with Down syndrome or Fragile X.
Osteopathy ‘of no benefit’ to children with cerebral palsy
Researchers found no statistically significant difference between a group of children who received osteopathy for six months and one that didn’t, according to a British randomized control study published in the Archives of Disease in Childhood. No differences were identified in terms of the child’s movement, quality of life, sleeping patterns or pain level.
Short antibiotic use safer for children who use ventilators
Short courses of antibiotics appear just as effective as longer ones—and a great deal safer—in treating respiratory infections that might cause pneumonia in children who use ventilators, according to a Johns Hopkins Children’s Center study published online May 3 in Clinical Infectious Diseases.

BLOOM ~ summer ~ 2011 ~ 31
resources
online
Coping with pain
Anesthesia and pain management: A kid’s illustrated guidehttp://www.rch.org.au/anaes/health-info/index.cfm?doc_id=780
Comfort kids program: Coping with health procedureshttp://www.rch.org.au/comfortkids/parents.cfm?doc_id=10137
Kid language
A children’s dictionary of medical wordshttp://kidshealth.org/kid/word/#cat20190
Online teens
Teens with serious illness connecthttp://www.starbrightworld.org/default_login.aspx?ReturnURL=%2fhome.aspx
Disability History Museum
http://www.disabilitymuseum.org/dhm/index.html
Stephen Hawking on disability
New York Times: “My advice to other disabled people would be, concentrate on things your disability doesn’t prevent you doing well, and don’t regret the things it interferes with. Don’t be disabled in spirit, as well as physically.”
bookshelf
Bad animals: A father’s accidental education in autism, Joel Yanofsky, 2011
The everyday advocate: Standing up for your child with autism or other special needs, Areva Martin, 2011
The story of beautiful girl, Rachel Simon, 2011
For kids!
Out of my mind, Sharon Draper, 2010. Ages 9-12.What happens when 11-year-old Melody—who can’t talk or control her body—moves from a contained special-ed class to a regular class?
Online video and photo contestbringing visibility to disability!Enter June 20th - August 12th, 2011.
P R E S E N T S
filmpossible
f
lif bi lbpmlif bisso elb
www.filmpossible.caContest rules apply, see website for details.
1st Priz
e Video $5000
Send us your videos and photos with thetheme of bringing visibility to disability. Be bold, creative, and inspiring! You could:
• Capture life experiences • Demonstrate inclusion • Tell a story • Show changes we can make.
Spread the word to earn votes.
Winners will be determined by a panel oftop-notch judges and by public voting.
1st Priz
e Photo $1000
Filmpossible_TorontoKids_ad_5.125x5.44:Layout 1 18/07/11 10:25 AM Page 1

32 ~ BLOOM ~ summer ~ 2011
In The Four Walls of My Freedom, Donna Thomson (left photo
centre) recounts life raising her son Nicholas, 22 (front left), who
has cerebral palsy and requires 24-hour care. Donna is married
to James Wright (back left), the High Commissioner for Canada
in the UK, and has a daughter, Natalie (right). Donna shares her
thoughts on how people can find freedom, choice and wellbeing
within any set of life circumstances, including severe disability.
BLOOM: It struck me how you moved from one medical crisis to another with Nicholas early on. How did you stay afloat?
Donna Thomson: As women I think we’re socialized to expect that any capable person should be able to cope with any circumstances their baby presents with. I was so exhausted but I thought I should be able to cope. It took me a long time to put up my hand and say ‘I am seriously not able to do this.’ When my daughter was born I knew I needed practical help, and I realized that the only way I was going to access help through government programs was to be dramatic in the language I used. I realized words like ‘family breakdown’ and ‘drowning in my son’s needs’ got attention. I think using that language strategically to get funding helped me understand my own limitations.
BLOOM: In your book you talk about how parents are judged.
Donna Thomson: The moment your child is diagnosed with a disability, they become public property. It’s not the same with an able-bodied child at all. Professionals have a say in how you feed your child, how you hold your child, the kinds of activities you do with your child, and what you allow your child to do or not do. You’re judged on these things absolutely.
BLOOM: I identified with this quote: ‘I remember thinking that modern medicine and the power of love could beat the effects of cerebral palsy. How wrong I was.’ What is it about our culture that leads to the perception that people can ‘overcome’ disability?
trailblazer
A good life, despite adversity
BLOOM ~ summer ~ 2011 ~ 33
trailblazer
Donna Thomson: I think it has to do with the notion of independence as being the core value of our society. There is a great aversion to dependence. I think when you put the individual at the heart of society, as opposed to the family or community, then it’s a natural outcome that you think you will be able to manipulate nature. I would never advocate not doing therapy with our children because we want to enable their potential. However, I think because we define a successful life by independent function we never talk about the children who can’t aspire to that. The question at the heart of Western society that worries me is that people who will never be independent or employable are not worth supporting. Why would you support someone who could never give back to society what they consume? They’re abandoned.
BLOOM: Why as parents of children with disabilities must we redefine happiness and achievement?
Donna Thomson: I think a lot of people are beginning to realize that having wealth and position in society doesn’t make you happy if you can’t convert your wealth into good living. And what is good living? Good living can be quantified by your loving relationships. I think there are many people who are realizing that loneliness and isolation are a contemporary scourge. What our children need in terms of support is company, and to be with other people. And what our children need is what society needs. When I talk to people who have cared for Nicholas or been friends with him they say they have been transformed in a very positive way by their relationship with Nick. I think that to a large extent we in contemporary society have lost the knack of neighbourliness that we used to have in more rural communities.
BLOOM: What is the Capability Approach?Donna Thomson: The Capability Approach is an idea about how people can function well within
circumstances of adversity. It’s to do with the factors that allow a person the freedom to make choices to have a life that they value. Economist Amartya Sen wrote about it in the context of extreme poverty in India, talking about the types of freedoms people need to have the basic level of functioning that allows a person to have human dignity. He was interested in minimum levels, but because I’m a very middle-class person, I want to use the Capability Approach to look at maximum levels of flourishing. I want to know what are the supports and services and policies that will enable Nick to have the freedom to make daily choices to have a life that he values. Rather than to be spoon-fed programs he doesn’t want.
BLOOM: You note that Nick spends most of his time in bed, yet experiences the world richly. Can you explain?
Donna Thomson: Nicholas has a big screen TV in his room connected to a computer in Canada that enables him to watch Canadian TV. He watches the CBC News and Hockey Night in Canada. He’s very interested in hockey and can watch all of the NHL games if he wants. He writes a hockey blog. He does all of this with a lot of assistance. He uses a communication program on an iPad with his helpers. He also has facebook and hotmail and he’s a seller on eBay. He has great friendships with his carers and remains friends with them when they leave.
BLOOM: Many parents of children with complex medical needs struggle to get the supports they need at home.
Donna Thomson: I think the issue of 24-hour care is an urgent concern for governments. Part of the public discussion we need to have is about a global or national ethic of care that we believe supports human dignity. How many baths does a person need per week, and is it okay to leave a person alone in a room in a facility for two, three, four hours? What’s the cut
34 ~ BLOOM ~ summer ~ 2011
off? We need to actually make those decisions about what is the kind of care we expect for someone we love if we drop dead tomorrow and they become the responsibility of the state. Then we need to figure out what’s the responsibility of the government, national and provincial, and what is the responsibility of the community, the family and the individual. When making these decisions, I argue we should always think about how we can maximize human freedom to have choice and wellbeing. My guiding principle for policy making and funding is that it be ‘most supportive and least restrictive.’ That, of course, is most expensive.
BLOOM: How can we financially support these services?
Donna Thomson: Given this is the first generation of people with severe disabilities who will outlive their parents, we have to look at how we can mobilize communities to work together to enable a good life for all. This is an international phenomenon and an international concern. In Japan they’re doing a system where if you volunteer to help the elderly or disabled, you get ‘time credits’ you can claim when you need care yourself later in life.
BLOOM: You mention a time when Nick rates himself low in the area of meaningful work. How can parents maintain their children’s self-esteem when they’re not able to do paid work?
Donna Thomson: That’s a really tough one. It’s very natural and deeply human to want meaningful work in your life. And it’s also deeply human for Nicholas to want a girlfriend. And some of these things may not happen for him. So the job of the people who love him is to help him understand what his reality is, to help him make peace with his limitations, and to help him aspire to his dreams.
BLOOM: How can parents of children with complex difficulties assess whether they’re leading the life they choose?
Donna Thomson: It’s very difficult to do. But the people closest to that person will have a strong gut feeling and a deep, fundamental knowledge of that person and if they’re happy. Sometimes comfort is happiness, and things that are very humanly basic, like touch and intimacy in terms of singing and sound. That’s why Snoezelen is so good. We know when our children are enjoying those kinds of physical and spiritual comforts and that is happiness.
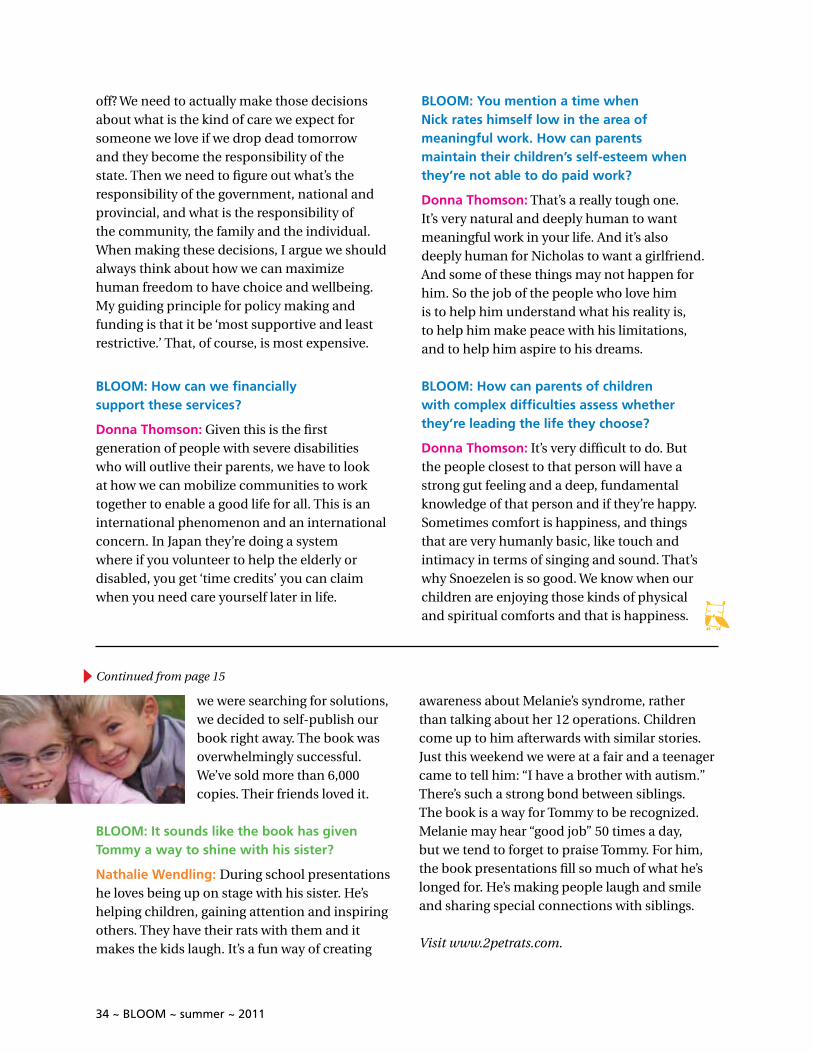
we were searching for solutions, we decided to self-publish our book right away. The book was overwhelmingly successful. We’ve sold more than 6,000 copies. Their friends loved it.
BLOOM: It sounds like the book has given Tommy a way to shine with his sister?
Nathalie Wendling: During school presentations he loves being up on stage with his sister. He’s helping children, gaining attention and inspiring others. They have their rats with them and it makes the kids laugh. It’s a fun way of creating
awareness about Melanie’s syndrome, rather than talking about her 12 operations. Children come up to him afterwards with similar stories. Just this weekend we were at a fair and a teenager came to tell him: “I have a brother with autism.” There’s such a strong bond between siblings. The book is a way for Tommy to be recognized. Melanie may hear “good job” 50 times a day, but we tend to forget to praise Tommy. For him, the book presentations fill so much of what he’s longed for. He’s making people laugh and smile and sharing special connections with siblings.
Visit www.2petrats.com.
Continued from page 15
BLOOM ~ summer ~ 2011 ~ 35
your kids ‘in bloom’If you would like to see your child here, please email a high-resolution phototo [email protected]. We will try to feature as many as possible.
36 ~ BLOOM ~ summer ~ 2011
The unlimitedJoey.We’re creating a world withoutlimits for children with disabilities.
You can help a child discover a world of possibility. Donate today:hollandbloorviewfoundation.ca
HBF half pg horiz ads:Layout 1 02/02/11 2:37 PM Page 2
Holland Bloorview Kids Rehabilitation Hospital: 150 Kilgour Road, Toronto, ON M4G 1R8 | Tel: 416-425-6220 | www.hollandbloorview.ca