
HLTEN504A - INCP Swallowing Difficulties. Dysphagia Is a problem or difficulty with swallowing.
13
HLTEN504A - INCP Swallowing Difficulties
-
Upload
leticia-vink -
Category
Documents
-
view
219 -
download
0
Transcript of HLTEN504A - INCP Swallowing Difficulties. Dysphagia Is a problem or difficulty with swallowing.
HLTEN504A - INCP
Swallowing Difficulties
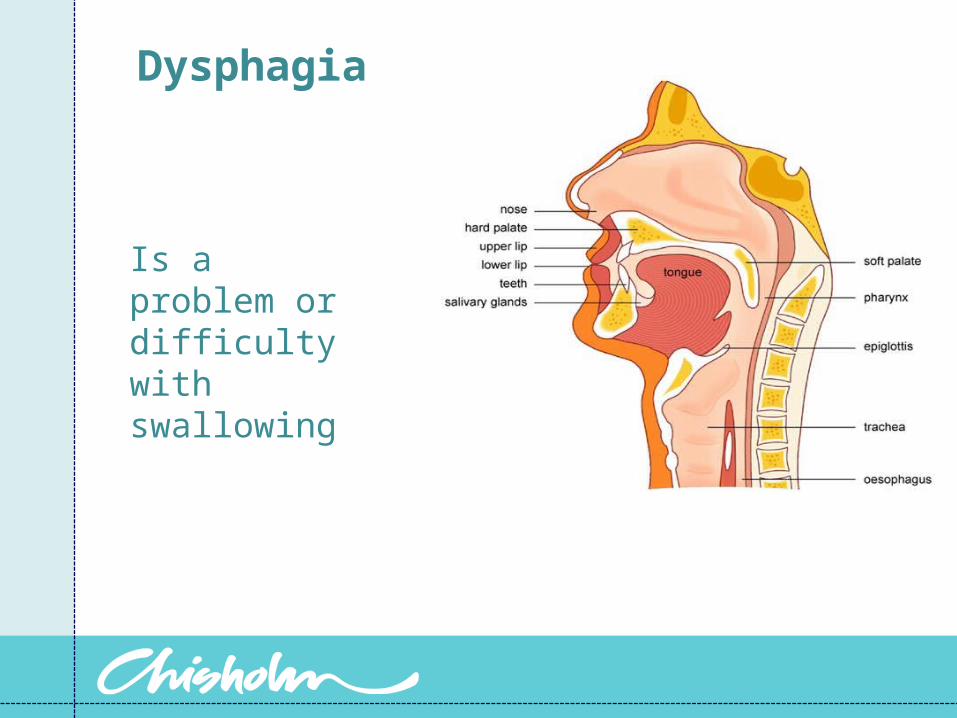
Dysphagia
Is a problem or difficulty with swallowing
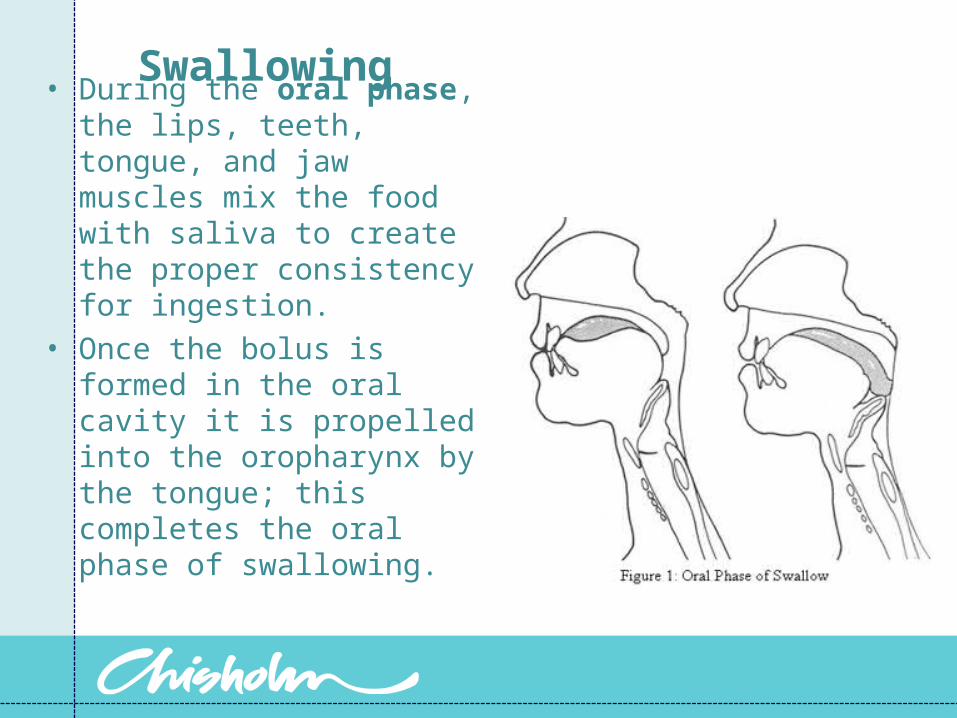
Swallowing • During the oral phase, the
lips, teeth, tongue, and jaw muscles mix the food with saliva to create the proper consistency for ingestion.
• Once the bolus is formed in the oral cavity it is propelled into the oropharynx by the tongue; this completes the oral phase of swallowing.
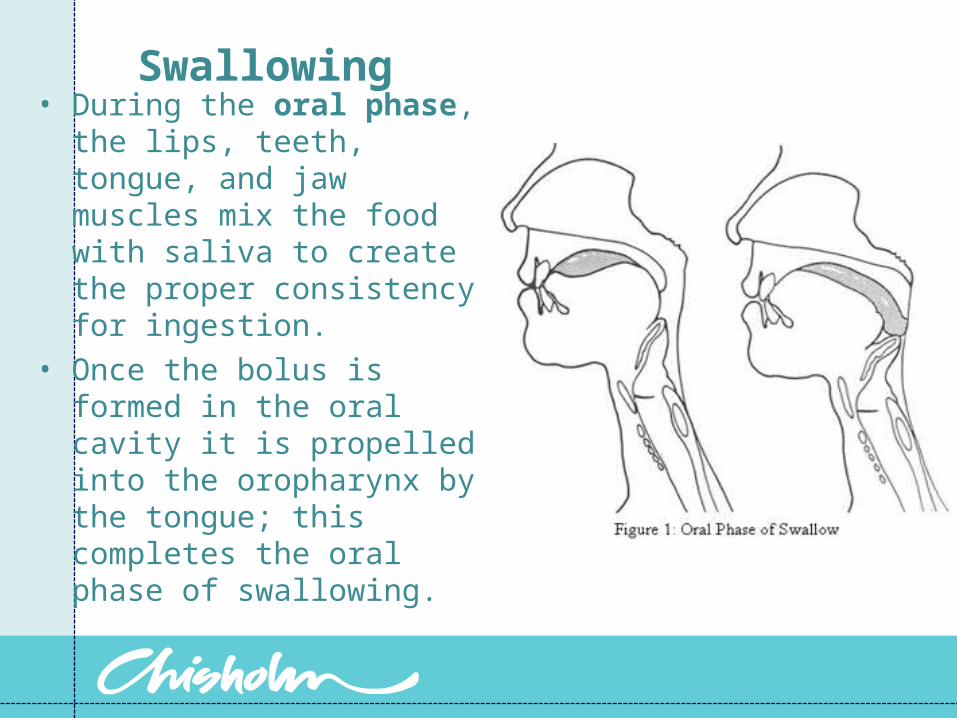
Swallowing• During the oral phase, the
lips, teeth, tongue, and jaw muscles mix the food with saliva to create the proper consistency for ingestion.
• Once the bolus is formed in the oral cavity it is propelled into the oropharynx by the tongue; this completes the oral phase of swallowing.
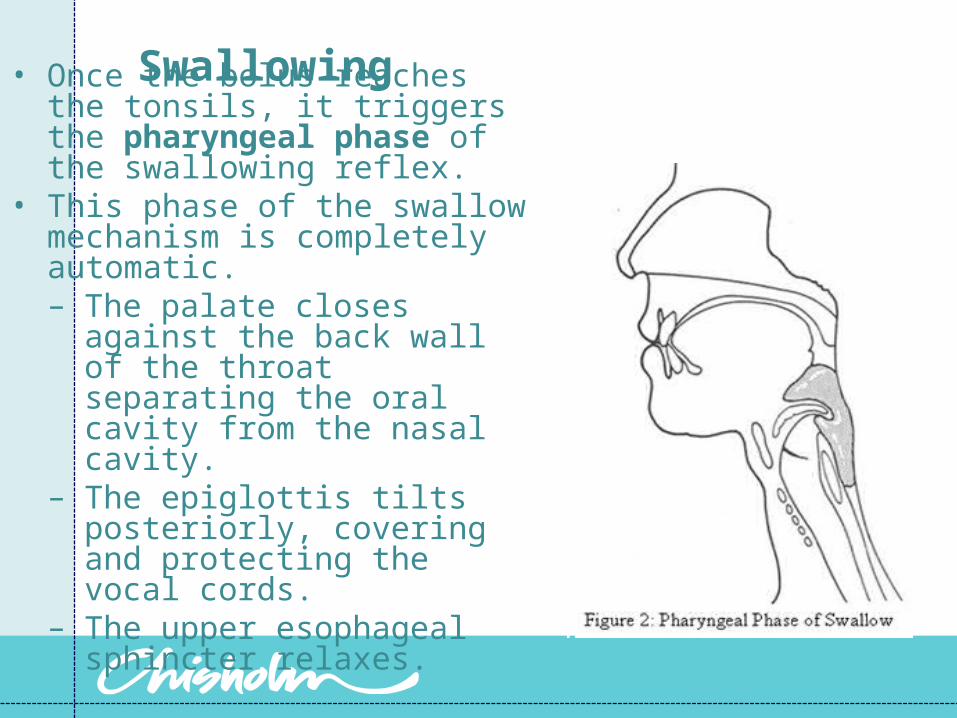
Swallowing • Once the bolus reaches the tonsils, it triggers the pharyngeal phase of the swallowing reflex.
• This phase of the swallow mechanism is completely automatic.– The palate closes against the
back wall of the throat separating the oral cavity from the nasal cavity.
– The epiglottis tilts posteriorly, covering and protecting the vocal cords.
– The upper esophageal sphincter relaxes.
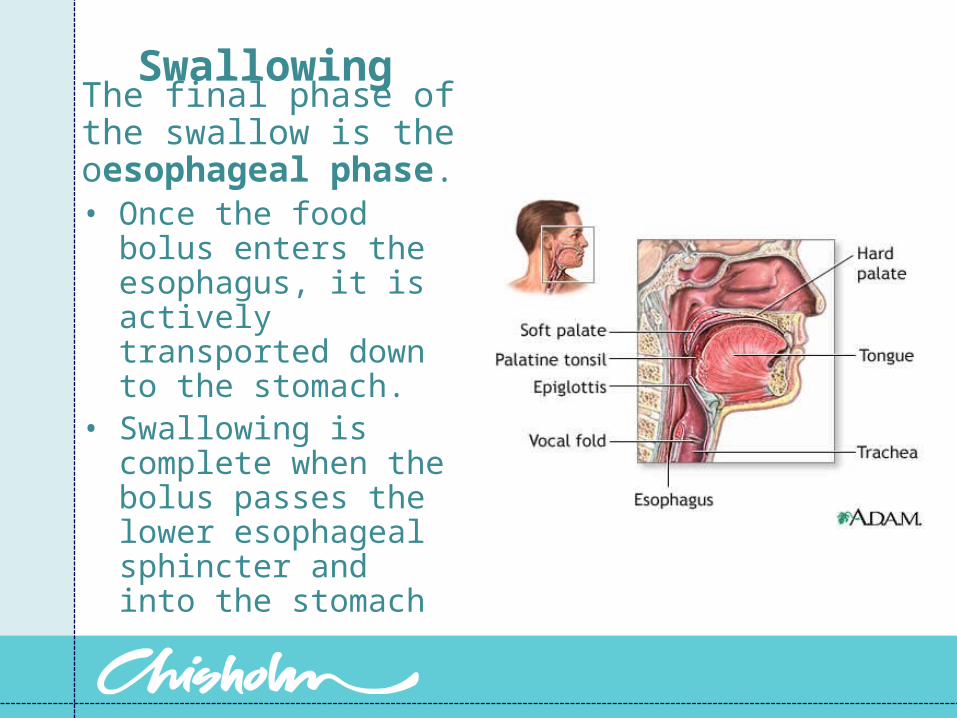
Swallowing The final phase of the swallow is the oesophageal phase.• Once the food bolus
enters the esophagus, it is actively transported down to the stomach.
• Swallowing is complete when the bolus passes the lower esophageal sphincter and into the stomach
Causes of dysphagia
These may develop suddenly or develop slowly over an extended period of timeSevere pain • Trauma/accident• Surgery• RadiationObstruction • Structural defects • Radiation
Causes of dysphagia (cont)
Abnormal peristalsis • Neuromuscular • Degenerative diseases • Metabolic/toxic
Impaired gag reflex • Neurological• Degenerative diseases • Unconscious states• Metabolic/toxic
Excessive, scant, or thick oral secretions
Some conditions that cause dysphagia
Stroke
Closed head injury
Parkinson’s disease
Motor neuron disease
Huntington’s disease
Clinical manifestations of impaired swallowing
Patient reports difficulty
Coughing with food or liquid intake
Longer time taken with meals than other people
Drooling, constantly open mouth, constantly mopping mouth
"Gurgly" voice
Food remaining in mouth after meals
Choking or asphyxiation with oral intake
Clinical manifestations of impaired swallowing
Diminished or absent coughDiminished or absent gag reflexWeight lossPneumoniaX-Ray evidence of aspirationFluctuating levels of consciousnessTracheostomyNaso-gastric feeding tube
To prevent aspiration/choking
Sit person upright to assist gravity. Sometimes the person needs to sit out of bed for all meals.• Maintain slight neck flexion• Ensure that patient is awake and alertModifications to the consistency of the food and fluid may be required: • Soft/pureed diet, thickened fluids (nectar or honey
consistency)Initiation of the swallowing reflex may be required – press on the tongue
To prevent aspiration /choking
Offer food and fluid at a rate that the person can cope with – prevents aspiration• One mouthful at a time• Effective swallow before next mouthful• Examine mouth at end of meal• Unhurried mealtime
If facial paralysis is present offer the food to the non-affected side. • Check that they have swallowed each mouthful
offered. • Ensure that there is no food left in the mouth
before you leave the person unattended.
Maintain upright position 1/2 hour post meal


















