HIV/HPV
21
HIV AND HPV
-
Upload
thuphan95 -
Category
Health & Medicine
-
view
205 -
download
3
description
HIV Aids HPV STDs
Transcript of HIV/HPV
HIV AND HPV
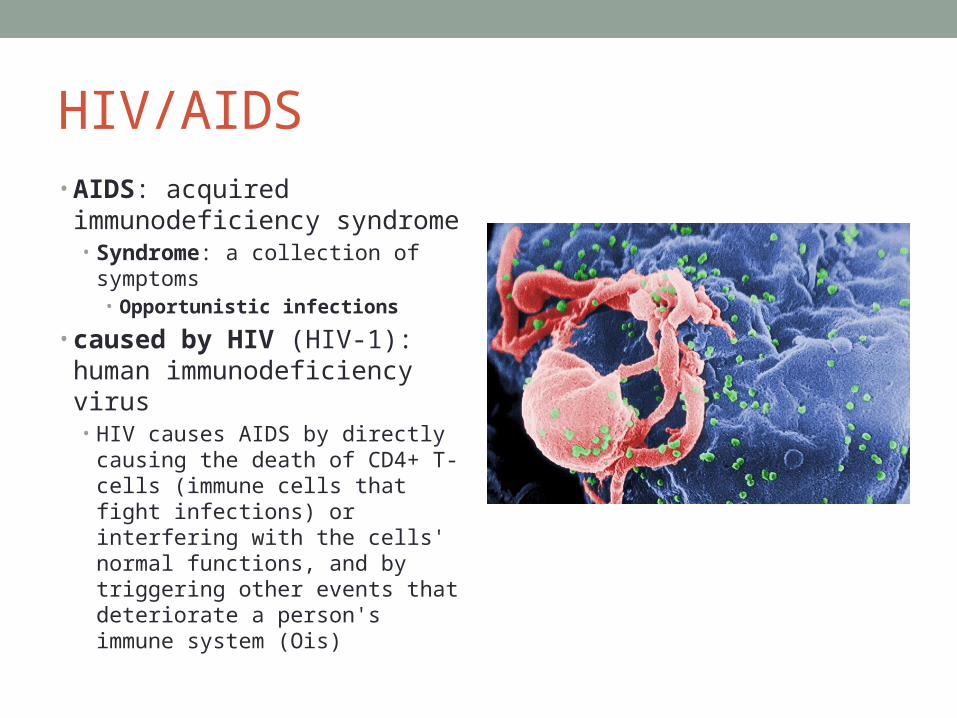
HIV/AIDS• AIDS: acquired
immunodeficiency syndrome• Syndrome: a collection of
symptoms• Opportunistic infections
• caused by HIV (HIV-1): human immunodeficiency virus• HIV causes AIDS by directly
causing the death of CD4+ T-cells (immune cells that fight infections) or interfering with the cells' normal functions, and by triggering other events that deteriorate a person's immune system (Ois)

AIDS considered an “emerging disease”
• HIV mutated in 1930s from a form exclusive to apes to one that could live in humans.
• Such diseases that move from one species to another are known as zoonoses. Ebola and tuberculosis are both examples of other zoonoses.
Where did HIV come from?• http://youtu.be/UF3JGrt9Zvo

HIV/AIDS• HIV is a virus
• All viruses unable to multiply outside a host cell, and therefore, are classified as intracellular, obligate parasites• Most often causes some type of cell damage or death• Many viruses exist within host at a low enough level that the host is not aware of this
• Since viruses’ survival depends entirely on host, most viruses tend to cause mild infections• Death in host = death of virus • this is not the usual mode of action for most viruses because their existence would
cease to be• Exceptions human immunodeficiency virus, ebola virus, pandemic influenza
• HIV is lentivirus, a class of retroviruses• Unlike other retroviruses, which typically bud from infected cell for a long period
of time, HIV can lyze cell or lie dormant for many years, especially in resting T4 (CD4) lymphocytes;• while HIV may disappear from cells of circulation, viral replication and budding
continues to occur in other tissues.
• recrudescence of viral production occurs that ultimately destroys the cell.

Short hx• AIDS 1st described in 1981 by physicians in U.S.- saw healthy
patients become sickly and develop opportunistic infections and cancers • described AIDS in the medical literature.
• Public health officials (PHOs) started with this information and amassed additional data about the patients, hoping to identify a cause for the new disease.
• By mid-1982, epidemiologists had data demonstrating that AIDS was transmissible. A virus was suspect.
• 1983, a candidate retrovirus isolated and in 1984, it was demonstrated to be causative pathogen.• This retrovirus destroyed helper T-cells, the master cells of the body’s
immune response.

1984-95• Intensive research period to learn how HIV
worked• HIV found to mutate 1,000 times faster than
influenza virus, thus dashing hopes for making a traditional vaccine
• Antiviral drugs tested; AZT rapidly approved as 1st anti-AIDS drug1987
• Public fear of AIDS and hostility towards people with AIDS reached their zenith • PHOs had to deal with epidemic of fear as well as
biological epidemic.
• 1988-95 • Congress increased funding for AIDS research
across U.S.• Surgeon General C. Everett Koop mailed a
brochure, “Understanding AIDS,” to every household in the U.S. so that citizens would know facts about AIDS instead of believing rumors.
• World Health Organization’s AIDS Programme began functioning
1995-2006• With introduction of first protease inhibitor drug in 1995, Highly Active Anti-Retroviral Therapy (HAART) transformed AIDS into a chronic disease.
• epidemiological focus of epidemic shifted to developing countries and marginalized populations in U.S.
• 2006, universal screening guidelines for HIV infection aimed to make AIDS a routinely reported disease in U.S.
• 2013 UN agency reports ‘dramatic’ progress on reducing new HIV infections

8
HIV/AIDS Key driver of change in public health
• Enormous impact because• no biological control mechanism• enormous cost• many are vulnerable
• Effect on other infectious disease programs• TB surveillance and control programs were successful public health
interventions, until HIV/AIDS epidemic reversed this achievement• rise in active cases
• Effect on maternal child health programs and reproductive health programs• Changes to program planning and infrastructure due to:
• use of antiretroviral drugs for treatment• prophylactic treatment for exposed babies• breast feeding

HIV/AIDS epidemiology• 2.3 million adults and children newly
infected with HIV in 2012,• represents 33 % reduction in annual new cases
compared to 2001.• new HIV infections among children fell 52 % to
260,000 in 2012.• greater access to antiretroviral TX led to a 30 per
cent drop in AIDS-related deaths from the peak in 2005.
• In the U.S., deaths typically through Pneumocystis carinii
• In other parts of the world, it is TB• > 90% of new HIV infections are in
developing countries. • In Africa (mostly sub Saharan), > 24 million people
with HIV infection and about 1 million new cases of AIDS per year
• .
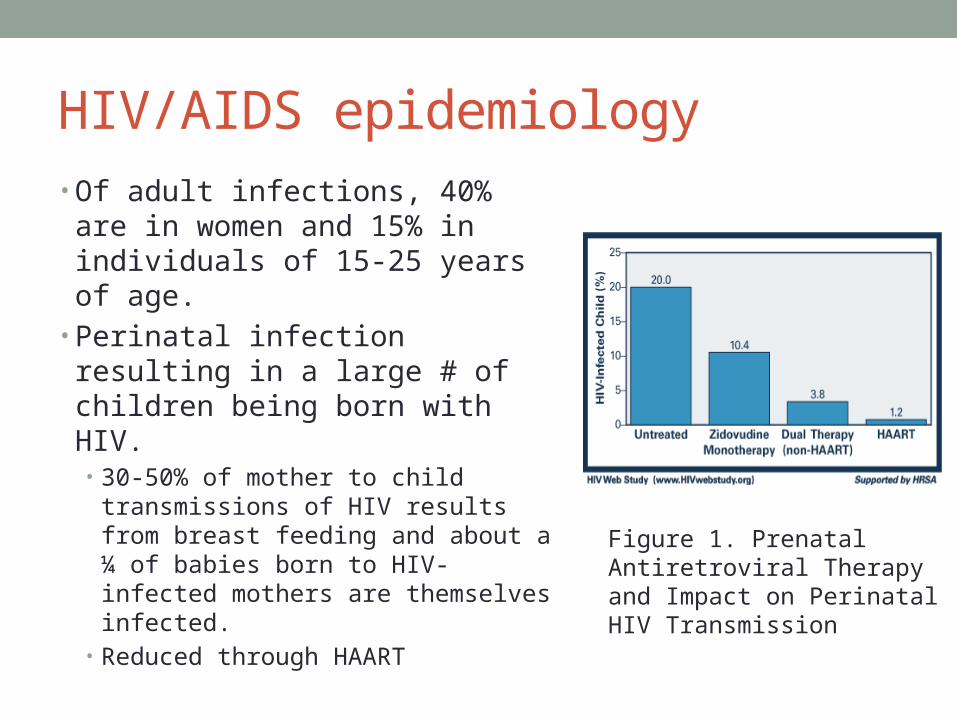
HIV/AIDS epidemiology• Of adult infections, 40% are in
women and 15% in individuals of 15-25 years of age.
• Perinatal infection resulting in a large # of children being born with HIV. • 30-50% of mother to child
transmissions of HIV results from breast feeding and about a ¼ of babies born to HIV-infected mothers are themselves infected.
• Reduced through HAART
Figure 1. Prenatal Antiretroviral Therapy and Impact on Perinatal HIV Transmission


HIV Transmission• Sexual Transmission
• Blood Transmission
• Mother to Child
HIV/AIDS Risk Groups• Paid/commercial sex workers (CSWs)• Men who have sex with men (MSM)• Injecting drug users (IDUs)• Prisoners• Any sexually active person who does not assume she/he is
at risk and take preventive measures• Women
• HIV/AIDS Mother-to-child transmission • Risk of
• acquiring HIV during delivery without intervention: 15% to 30%• HIV transmission during delivery if the mother is taking ARVs: <2%• acquiring HIV from breastfeeding without intervention: 25% to 45%• HIV transmission during breastfeeding if the mother is taking ARVs: much
lower

Testing for HIV• Antibody tests: Once infected, takes 3-6 months for
enough antibodies to be formed for screening tests to be positive
• If test negative, person should be retested in 6 months
• ELISA (also called EIA) • Western blot or indirect immunofluorescence assay (IFA).• Rapid assessment tests
• PCR tests. • Once positive additional tests may be done for
• CD4 count. Important because healthy person's CD4 count can vary from 500 to more than 1,000. Even if a person has no symptoms, HIV infection progresses to AIDS when CD4 count becomes < 200.
• Viral load. measures amount of virus in blood; people with higher viral loads generally fare more poorly than do those with a lower viral load.
• Drug resistance. determines whether strain of HIV will be resistant to certain anti-HIV medications and which ones work better
The Course of the diseaseFrom HIV Infection to AIDS
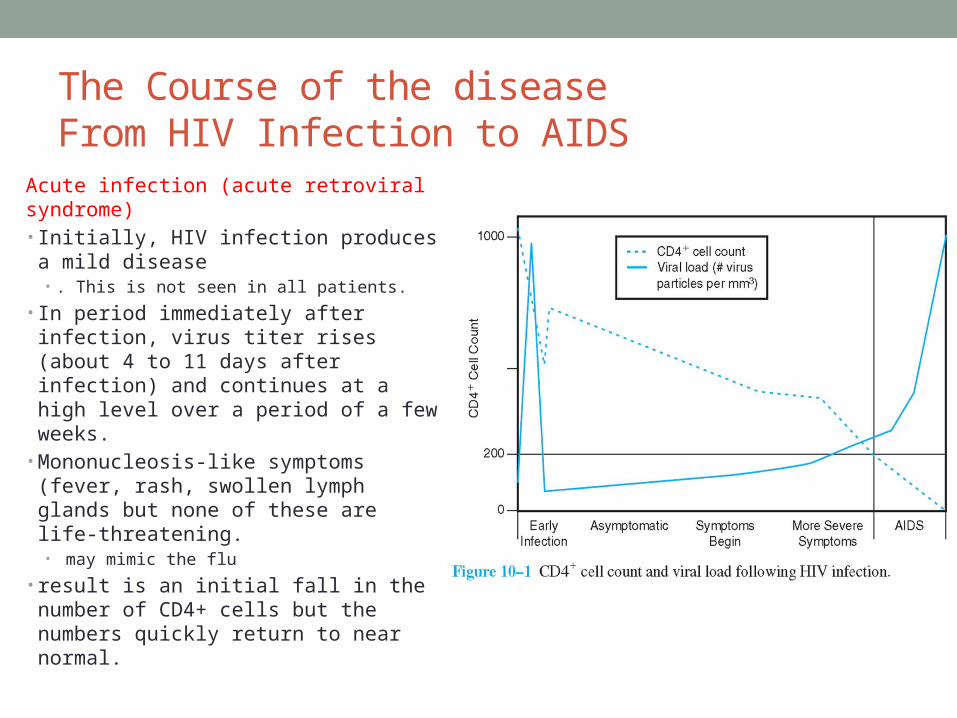
Acute infection (acute retroviral syndrome)• Initially, HIV infection produces a
mild disease • . This is not seen in all patients.
• In period immediately after infection, virus titer rises (about 4 to 11 days after infection) and continues at a high level over a period of a few weeks.
• Mononucleosis-like symptoms (fever, rash, swollen lymph glands but none of these are life-threatening.• may mimic the flu
• result is an initial fall in the number of CD4+ cells but the numbers quickly return to near normal.
The Course of the diseaseFrom HIV Infection to AIDS
• No other symptoms may occur until enough CD4 cells have been destroyed by HIV • With loss of CD4 cells, the immune system cannot protect• When CD4 count reaches 200 – person considered to have AIDS• Without therapy, time from infection to AIDS = approximately 8-10
years• Despite possible co-factors associated with lifestyle, HIV infected
persons progress to AIDS at a remarkably similar rate
• Antiretroviral therapy can prolong this time span• Some people naturally have not progressed from HIV
infection to AIDS• Referred to as long-term nonprogressors

Preventive interventions for HIV/AIDS• Safe sex, including condom use• Unused needles for drug users• Male circumcision• Treatment of other sexually transmitted infections (STIs)• Safe, screened blood supplies• Antiretrovirals (ARVs) in pregnancy to prevent mother-to-
child transmission (MTCT) and after occupational exposure

Treatment Interventions for HIV/AIDS• Antitretroviral drugs (ARVs)
• Highly active antiretroviral therapy (HAART): combination of antiretroviral drugs that are used as medications to control retroviruses
• Extend years between infection and onset of clinical AIDS• Extend years between onset of AIDS and death
• works against HIV by using drugs in combination to suppress HIV replication as many times as possible. • problems for HIV replication, keeps HIV offspring low, and reduces the possibility of
HIV mutating.
• must be used in combination to suppress HIV for long periods of time
• Treatment of opportunistic infections (OIs)• Palliative care (pain management)

High Costs of HIV Medication Cause 'Terrible Dilemma' in Mozambique
• http://www.youtube.com/watch?v=sETtnySexxy• 10:30• In Mozambique, where 1 in 8 adults is living with HIV, the
number of patients on antiretroviral drugs has expanded thanks to international AIDS funding, but a debate is emerging over whether foreign donors can continue to fund an ever-expanding pool of patients.

20
Role of Advocacy and Activism
• International response to epidemic• U.S. PEPFAR program• Global Fund to treat AIDS, TB, and Malaria• Bill and Melinda Gates Foundation• World Bank

HIV/AIDS Critical Challenges • Developing a vaccine to prevent the 2.6 million new
infections per year• Cost-effective approaches to prevention in different
settings• Universal treatment for all those who are eligible• Management of TB and HIV coinfection