
HIV in Kidney Transplantation
57
HIV in Kidney Transplantation Wisit Cheungpasitporn May 22, 2015
-
Upload
aiem-wisit -
Category
Education
-
view
55 -
download
1
Transcript of HIV in Kidney Transplantation

HIV in Kidney Transplantation
Wisit Cheungpasitporn
May 22, 2015

Disclosure• None
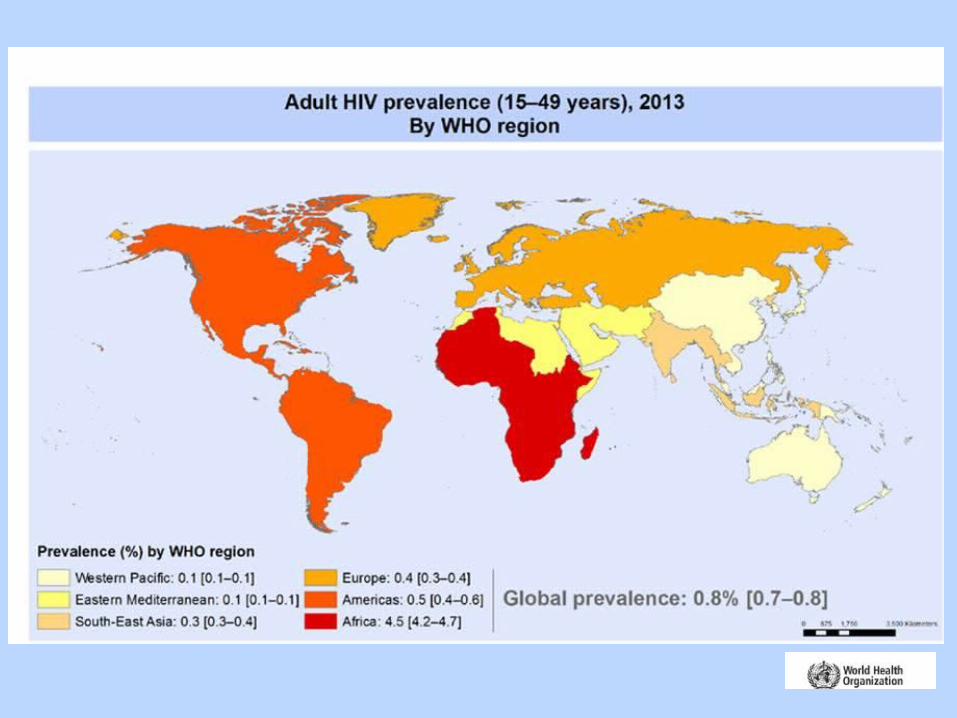

Adults Living with a Diagnosis of HIV Year-End 2008—United States

Classic pathologic features of HIVAN
Wyatt CM et al. Annu Rev Med. 2012;63:147-59.

Naicker S et al. Clin Nephrol. 2015;83(7 Suppl 1):32-8.

Age- and sex-standardized incidence of ESRD among HIV-infected adults
Abraham AG et al. Clin Infect Dis. 2015;60(6):941-9.

Trullas JC et al. Kidney Int. 2011 Apr;79(8):825-42

HIV and ESRD
• Nearly 90% of U.S. patients living with ESRD attributed to HIVAN are African-American.
• Nearly 900 patients with a presumptive diagnosis of HIVAN progress to ESRD each year.
• With improved survival of HIV-infected dialysis patients and increasing prevalence of HIV related ESRD.
United States Renal Data System 2010

HIV+ on dialysis vs. HIV- on dialysis
87%
54%
79%
41% HIV+
HIV-
Ahuja TS et al. J Am Soc Nephrol. 2002;13(7):1889-93.
USRDS data

Probability for kidney transplant
HIV-
HIV+
-National, multicenter, retrospective cohort study of HIV infectedpatients starting dialysis in Spain (1999–2006).
-66 HIV+ and 66 HIV- patients on dialysis
-Matching for dialysis center, year of startingdialysis, age, sex, and race.
Trullàs JC et al. J Acquir Immune Defic Syndr. 2011;57(4):276-83.

Factors Associated with Failure to List HIV+ Kidney Transplant Candidates
Sawinski D et al. Am J Transplant. 2009;9(6):1467-71.

Outcomes: HIV-Infected Recipients
Stock PG et al. N Engl J Med. 2010;363(21):2004-14.
150 patientsCD4+ >200Undetectable HIV RNA levelsTreated with a stable ARV regimen

Outcomes: HIV-Infected Recipients
Stock PG et al. N Engl J Med. 2010;363(21):2004-14.
31%
41%
12.3%

• SRTR; 2002–2011
• 510 adult kidney transplant recipients with HIV (median follow-up, 3.8 years) matched 1:10 to HIV-negative controls
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]

The number of kidney transplants
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]
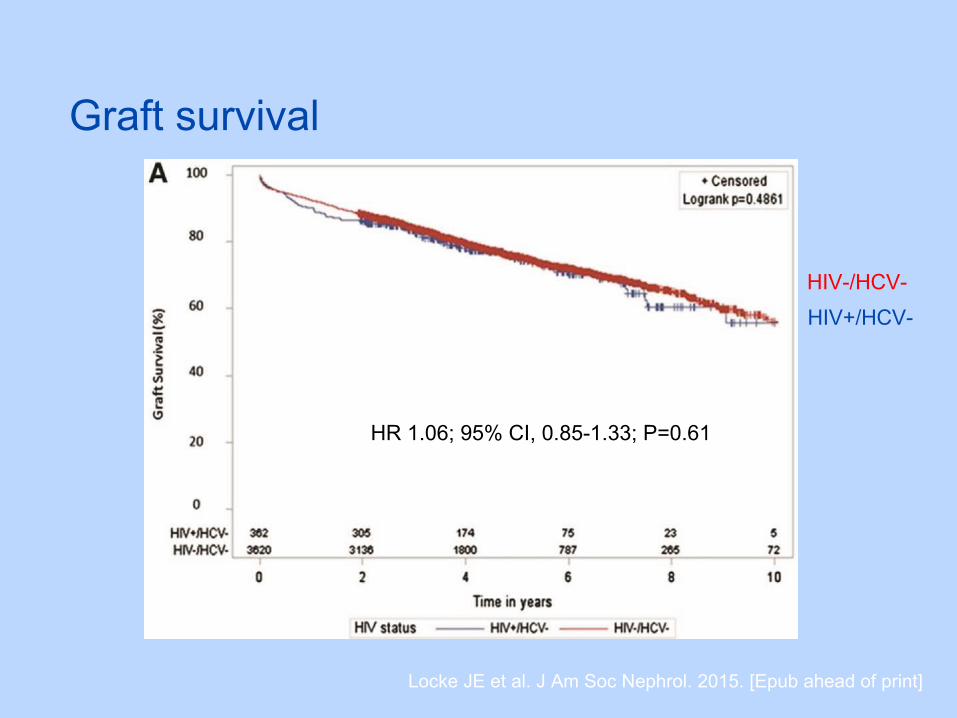
Graft survival
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]
HR 1.06; 95% CI, 0.85-1.33; P=0.61
HIV-/HCV-
HIV+/HCV-

Graft survival
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]
HR 1.38; 95% CI, 1.08-1.77; P=0.01
HIV-/HCV+
HIV+/HCV+

Patient survival
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]
HIV-/HCV-
HIV+/HCV-

Patient survival
Locke JE et al. J Am Soc Nephrol. 2015. [Epub ahead of print]
HIV-/HCV+
HIV+/HCV+

Wyatt CM et al. AIDS 2008, 22:1799–1807
Non-transplant HIV+ pts

Gonzalez VD et al. J Virol. 2009;83(21):11407-11.
T-cell activation in co-infected individuals
• CD38 is expressed selectively during the activation of a subset of mature T cells

Wyatt CM et al. AIDS 2008, 22:1799–1807

HIV-Positive–to–HIV-Positive Kidney Transplantation?

• November 2013: Organs infected with HIV may be transplanted only into individuals who are: (1) infected with such virus before receiving such an organ; and (2) participating in clinical research approved by an institutional review board.
HIV Organ Policy Equity (HOPE) Act approved by US Congress. 2013
HOPE

HIV-Infected Donor Eligibility and Selection in the USA
Richterman A et al. Curr Infect Dis Rep (2015) 17: 17

Moreno CN et al. Rev Assoc Med Bras. 2011;57(1):100-6

• Nationally, approximate 356 potential HIV+ deceased donors yielding 192 kidneys and 247 livers annually.
Richterman A et al. Am J Transplant. 2015 May 14. [Epub ahead of print]

Muller E et al. N Engl J Med. 2010;362(24):2336-7.
-In South Africa
-HIV+ recipients to HIV+ donors
-September to November 2008
-None had access to dialysis
-4 transplants from 2 deceased donors •not received ART•no opportunistic infection or cancer•had normal renal biopsies •without evidence of proteinuria
-ATG as induction therapy Maintenance: prednisone, mycophenolate mofetil, and tacrolimus.
7.7 6.6 19.4 8.2
1.3 1.3 2.01.2
1.11.0 1.2 1.0
-A patient receiving tacrolimus had calcineurin toxicity and was switched to sirolimus.
-At 12 months after transplantation, all patients had good renal function, did not have clinically significant graft rejection.

N Engl J Med. 2015 Feb 12;372(7):613-20.

Method
• Prospective nonrandomized study
• Groote Schuur Hospital, Cape town, South Africa• 50-70 KTx/year• Donor: living (30%) vs deceased (70%)
• All HIV-positive patients with stage 5 CKD who underwent KTx from HIV-positive donors
• September 2008 – February 2014

Donor selectionInclusion
• HIV-infected deceased donors
• Not on ART or received first-line treatment
• Undetectable plasma HIV RNA viral load (<50 copies/mL)
Exclusion
• Severe sepsis
• Active tuberculosis
• WHO stage 4 HIV disease (AIDS)
• Abnormal renal function
• Proteinuria on urine dipstick
• Alb:Cr ratio ≥ 300 µg/g

RecipientInclusion
• HIV-infected
• Receiving ART for ≥ 3 Mo
• CD4 T-cell ≥ 200 /mm3
• Undetectable plasma HIV RNA viral load
Exclusion
• History of opportunistic infection (AIDS)

Immunosuppression
• Induction: rabbit antithymocyte globulin• Thymoglobuline (1.5 mg/kg/d for 5-7 days) or
• ATG (2 mg/kg/d for 5 – 7 days)
• Maintenance: start on day 0• Prednisone (30 5 mg/d over the first 3 Mo after KTx)
• MMF (1 g q 12 hr)
• Tacrolimus (0.2 mg/kg adjusted for trough level 6-8 ng/mL)

Antiretroviral therapy
• Initially, NNRTI-based ART were switched to a boosted PI-based regimen at the time of KTx
• To increase the suppression of donor-virus replication • To lower the costs of immunosuppressive Tx by the inhibitory
effect of ritonavir on calcineurin-inhibitor metabolism
• Due to concern regarding calcineurin-inhibitor toxicity, recipients continued to receive their pre-KTx regimen
• Prophylaxis for opportunistic infection• TMP 80 mg and SMX 400 mg daily for PCP• Isoniazid 300 mg/d for TB • Valganciclovir 900 mg/d for the first 3 Mo for CMV

Clinical protocol
• Follow-up: weekly for 1st month and monthly thereafter
• Lab• Monthly: Urea .Cr• Every 6 Mo: CD4 T-cell count, plasma HIV RNA viral load
• Allograft biopsy• Performed yearly • When clinical suspicion of acute rejection
• Acute rejection: biopsy proven using Banff classification

Statistical analysis
• Kaplan Meier method was used to estimate patient survival, graft survival and allograft rejection
• Data regarding graft survival were censored at the time of patient’s death

Result - Donor
• 15 eligible donors
• Median age 30 (IQR 23-36) years
• Cause of death• 13 trauma• 1 overdose• 1 subarachnoid hemorrhage
• ART therapy before death• 1 NNRTI-based first-line therapy• 14 no ART

Result - Recipient
• 27 recipients
• Survivors were followed for a median of 2.4 yr

RESULTS – Patient and graft survival
• 2 had delayed graft function and required dialysis during the 1st week after KTx
• 1 graft failure due to venous thrombosis on day 1• 1 acute severe Ab-mediated rejection , refractory to
plamapheresis, which necessitated graft removal after 2 weeks
• 25 well-functioning graft at the end of 1st year
• Median Cr at 1 year 1.3 (1.2-1.3 mg/dL)

RESULTS – Patient survival
Time (Yr)
HIV +ve HIV -ve
1 84 91
3 84 -
5 74 85

RESULTS – Patient survival
• 5 patients died after KTx• 1 Sepsis (E.coli and pseudomonas) and acute pancreatitis• 1 MI• 1 recurrent klebsiella pneumoniae septicemia due to UTI• 1 rapidly progressive, invasive pulmonary aspergillosis • 1 pulmonary squamous cell carcinoma
1 month
6 months1st year
1st year
5 years

RESULTS – Graft survival
Time (Yr)
HIV +ve HIV -ve
1 93 88
3 84 -
5 84 75

RESULTS – Allograft rejection
• 8 episodes of biopsy-confirmed acute rejection• 6 were successfully reversed using steroid, ATG, or
plasmapheresis• 2 graft failure
• 1st week: acute severe Ab-mediated rejection• 2 years: chronic scarring and fibrosis
• Rejection rate; 8% at 1 year and 22% at 3 years


RESULTS – Pharmacologic interactions
• Type of ART regimen had a consierable effect of the tacrolimus dosing
• The median tacrolimus dose was 0.5 mg q 7 – 10 days in PI-based regimen vs 8.5 mg q 12 hours in NNRTI-based regimen
• Side effect of tacrolimus were more pronounced in PI-based regimen
• 5 renal biopsy of calcineurin-inhibitor toxicity

RESULTS – Progression of HIV disease
• CD4 T-cell count• Median was 179 (IQR 141-310) in 1st year and 386 (IQR 307-
484) at 3 years
• Viral load• All had undetectable viral load (<50 copies/mL) during F/U
• Histologic finding• 3 routine renal biopsy revealed typical change of early HIV-
associated nephropathy; none had clinically significant renal impairment, proteinuria or required dialysis

Discussion
• Outcomes in HIV+ patient who received kidneys from HIV+ donors were comparable with those who received from HIV- donor
• Concerns• The risk of transmission of a new and possibly
resistant strain of HIV from donor to recipient• The appearance in the postoperative biopsy
specimens of early changes related to HIV-associated nephropathy that were not present in the baseline biopsy specimens
• Interaction between medications

Discussion
• The patients in this study did not have any increase in plasma viral load, and viral levels remained undetectable after transplantation.
• All the donors in this study had not received ART previously or had received first-line treatment with no known virologic evidence that would suggest resistance, although genotyping was not performed.

• Protocol renal transplant biopsies performed at 3 months from 19 recipients with HIV-1
• Undetectable levels of plasma HIV-1 RNA at transplantation
• HIV-1 infected the kidney allograft in 68% of these patients
• Podocyte infection associated with a faster decline in allograft function compared with tubular cell infection.
Canaud G et al. J Am Soc Nephrol 2014;25:407-19
in situ hybridization of HIV-1 RNA

Discussion
• The interaction between ART and immunosuppressants• Ritonavir and TAC
• Decreases the metabolism of TAC, resulting in a decrease of more than 80% in the clearance of TAC
• Required minimal doses of TAC every 7 to 10 days to maintain adequate levels.
• A higher incidence of CNI nephrotoxicity
• The NNRTIs and TAC• Induce the cytochrome P450 enzyme system• Increases the metabolism of tacrolimus, necessitating
higher doses (median, 8.5 mg twice daily) to maintain adequate levels.

Discussion
• Rejection rates among HIV-positive recipients have been reported to be approximately 3 times as high as those among HIV-negative recipients: unclear reasons
• Immune dysregulation• Challenge of managing the drug interactions
Stock PG et al. N Engl J Med. 2010;363(21):2004-14.

Conclusions
• Kidney transplantation from an HIV-positive donor appears to be an additional treatment option for HIV-infected patients requiring renal-replacement therapy.

Questions & Discussion

Apply to the United States?
• Lack of access to dialysis severely limits options for HIV-infected individuals with ESRD in South Africa, altering the risk–benefit dynamic.
• South African donors have been untreated for HIV; given the homogeneity of HIV infection in South Africa, it is unlikely that there will be resistance issues complicating management of the recipients.

Apply to the United States?
• The population of HIV-infected individuals in U.S.- higher rates of antiretroviral exposure and resistance:
• making it less likely that a single empiric choice of antiretrovirals will be sufficient to treat both donor and recipient.
Ethics of HIV-Infected Donation
• Attitudes of HIV-Infected Patients on waiting list- No data available
• Beneficence- strive to expand access to transplant in novel ways because of the discrepancy between the need for transplant and organ shortage.
• Non-maleficence-requires a cautious process forward because of limited outcomes data from HIV-infected donors.
• Informed consent















![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://static.fdocuments.us/doc/165x107/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)


