
HIV and Hepatitis C Co-infection Amy Kindrick, M.D., M.P.H. San Francisco AIDS ETC National HIV/AIDS...
49
HIV and Hepatitis C Co- infection Amy Kindrick, M.D., M.P.H. San Francisco AIDS ETC National HIV/AIDS Clinical Consultation Center February 12, 2002
-
Upload
agnes-foster -
Category
Documents
-
view
214 -
download
0
Transcript of HIV and Hepatitis C Co-infection Amy Kindrick, M.D., M.P.H. San Francisco AIDS ETC National HIV/AIDS...

HIV and Hepatitis C Co-infection
Amy Kindrick, M.D., M.P.H.San Francisco AIDS ETC
National HIV/AIDS Clinical Consultation Center
February 12, 2002

The Hepatitis C Virus
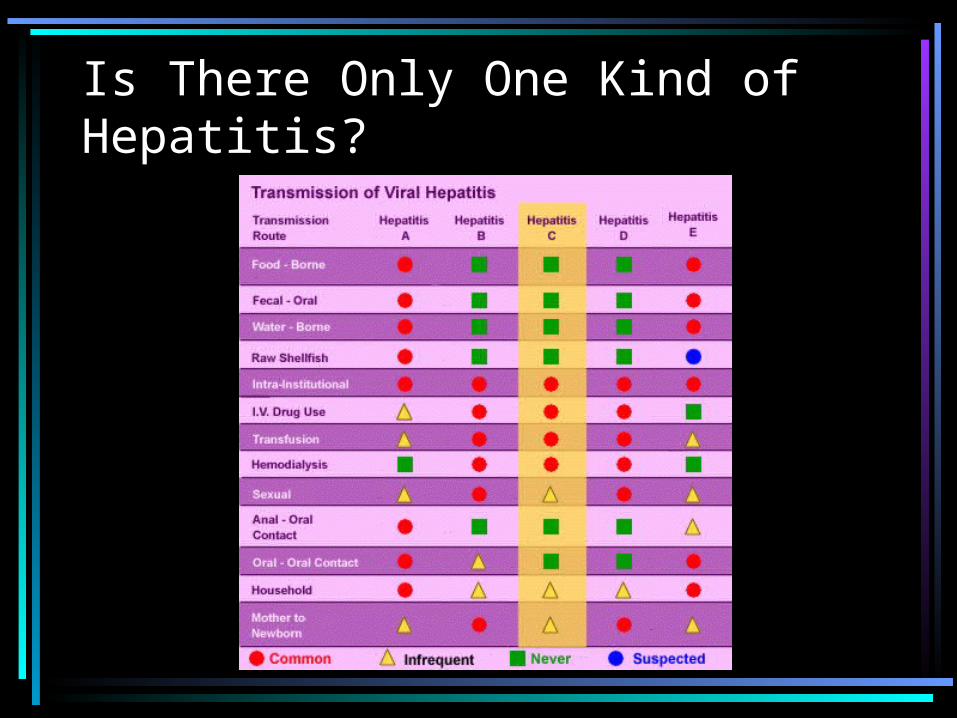
Is There Only One Kind of Hepatitis?

HCV Infection: Epidemiology
• Major healthcare problem worldwide• 70%–90% of HCV-infected patients
develop chronic disease• ~50 million infected worldwide
– ~5 million in Europe– ~4 million in USA
•Contributes to ~12,000 deaths/yr

<1 %
1–2.4 %
2.5–4.9 %
5–10 %
> 10 %
No data available
HCV Has Broad Global PrevalenceHCV Has Broad Global Prevalence

Hepatitis C Virus Infection• U.S. Overall antibody prevalence
1.8%– 64% positive for HCV RNA– Estimated 2.7 million persons
chronically infected
• Parenteral transmission route– Current risk of transfusion about 1 in
1,000,000

How Is HCV Transmitted?
• Infected blood– Needlestick– Needle sharing– Transfusion
• ?Infected body fluids– Amniotic fluid– Breast milk

Who Should Be Tested?• Drug users• Recipients of blood products or organ
transplant before 1992• Long-term partners of infected
individuals• Persons with occupational exposures• Children born to HCV-infected
mothers• HIV-infected individuals

Consider Testing For
• Persons with tattoos or body piercing
• Persons with multiple sexual partners
• Tissue transplant recipients

HCV Diagnosis• Enzyme immunoassays (EIA)
– Initial screening test for patients with liver disease
– False positives in low risk patients– Occasional false negatives, esp. With HIV+
• Recombinant immunoblot assays (RIBA)– Confirmatory test if EIA positive in low risk pt
• HCV RNA by PCR– Confirmatory if RIBA is “indeterminant”

Hepatitis C Virus Infection: Diagnosis• HCV antibody• HCV viral load• HCV genotype• Liver function tests• Liver biopsy is gold standard for
assessing disease status– ALT and AST do not predict liver histology– HCV RNA does not predict liver histology or
outcomes
Hepatitis C Virus Infection• Incubation period 2-26 weeks• Acute infection may be asymptomatic• Natural history variable
– Chronic infection in 70-75%– Cirrhosis in 10% to 20% of chronically infected
• Develops in 15-25 years
– Hepatocelluar carcinoma in 1% to 5% after 20 years• 1% to 4% per year once cirrhosis is established
– Extrahepatic manifectations• Arthritis• Glomerulonephritis• Mixed cryoglobulinemia



Vaccinate, Vaccinate, Vaccinate


Acute Hepatitis C

Chronic HCV Infection With Cirrhosis

Stigmata of Chronic Liver Disease

Mixed Cryoglobulinemia

Esophageal Varices

Hepatocellular Carcinoma

Hepatocellular Carcinoma

HCV/HIV Co-infection:General Issues
• U.S. Prevalence 40% to 60%– Varies geographically– Varies by HIV risk behavior
• Major transmission routes are transfusion and IDU
• Sexual and vertical transmission are rare• Coinfection may enhance
– Sexual transmission of HIV– Vertical transmission of HCV

Diagnosis of HCV in HIV-infected Patients
• Co-infection may reduce sensitivity of HCV antibody test (EIA or RIBA)– Measure HCV RNA by PCR or bDNA if
history or clinical symptoms are suggestive

Patients With HCV and HIV: Key Points
• 30% of patients with HIV also have HCV
Mortality from HCV proportional to mortality from HIV
• Natural history more fibrotic in coinfected patients

Impact of HIV on HCV
• HIV infection worsens HCV-related liver disease (in pre-HAART era)– ALT levels higher – Fibrosis more severe – Cirrhosis, liver failure, and HCC more
common– Death rates higher– Vertical HCV transmission enhanced
Impact of HCV on HIV
• Impaired Th1 function in HIV infection affects appropriate immune response to HCV
• Conflicting clinical results• More rapid progression to AIDS or
death for HCV genotype 1• Increasing HIV RNA and decreasing
CD4 more likely in co-infected pts

AIDS Incidence by HCV Genotype inGreek Hemophiliacs With HCV/HIV
0.250.25
0.50.5
0.750.75
PP=0.002=0.002
Genotype 1Genotype 1Other genotypesOther genotypes
00
1.01.0
44 88 1212 161600After HIV seroconversion (yr)After HIV seroconversion (yr)
Pro
babi
lity
ofP
roba
bilit
y of
deve
lopi
ng A
IDS
deve
lopi
ng A
IDS Conclusion:Conclusion:
Genotype 1 is Genotype 1 is associated associated with faster with faster progression to progression to AIDSAIDS

Are There Any Treatments for Hepatitis C?

HCV Treatment Rationale
• Treatment may improve HCV outcomes– Decrease fibrosis– Increase T-cell responsiveness to HCV
antigens– Decrease rate of fatal hepatocellular
carcinomas
• Treatment may improve HIV outcomes– Reduce hepatic toxicity of ARVs

HCV Treatment Options
• Interferon monotherapy– Sustained response rates similar to HCV-
infected alone• 8% - 44%
– Minimal correlation with CD4 counts
• Interferon-ribavirin combination therapy– Trials ongoing– Preliminary findings encouraging


0
5
10
15
20
25
30
35
Treatment of HCV in HIV+ Patients
Soriano et al. Clin Infect Dis 1996;23:585Soriano et al. Clin Infect Dis 1996;23:585
Pat
ient
s (%
)P
atie
nts
(%)
n=80n=80
5 MU TIW 3 mo, Responder 3 MU 9 mo5 MU TIW 3 mo, Responder 3 MU 9 mo
Complete responseComplete response Sustained responseSustained response
32.5%32.5%
22.5%22.5%

Interferon-Ribavirin Therapy
• Cohort study with 37 pts• 84% of patients on HAART with
stable HIV disease– Median baseline CD4 343– Median baseline HIV RNA < 400 c/mL
• 59% on combination therapy• 41% on IFN monotherapy
Interferon-Ribavirin Therapy: Interim Results
• Analysis of 27 patients at 12 weeks of treatment– 50% of combo arm had undetectable
HCV RNA vs 9% on mono arm– No significant change in HIV RNA
• Similar results in NYC cohort on HAART– Absolute CD4 count drop (529 to 277)
without change in CD4 %
Interferon-Ribavirin Toxicity
• Flu-like symptoms• Depression• Leukopenia• Anemia• ? Reduced effectiveness of ARV
therapy with ribavirin– May inhibit intracellular AZT and d4T
phosphorylation
What About OTC Medications?

Conclusions
• Natural course of chronic HCV accelerated by concurrent HIV infection
• Coinfected patients with stable HIV and good clinical, functional status should be considered for treatment
• New treatment options for chronic HCV should be urgently explored

HCV Future Treatment Options
• HCV-specific viral enzyme inhibitors– Helicase– Protease– RNA polymerase
• Internal ribosomal entry site inhibitors• Antisense nucleotides• Vaccination
Case 1
• 39 y/o HIV-infected man– HIV+ in 5/98– PCP in 12/98– Elevated LFTs and HCV antibody + in 12/98– Began HAART in 1/99
• d4T, 3TC, NVP• Labs
– ALT 100-200 u/l (2-4x ULN)– CD4 300 (from 80), HIV RNA <400

Case 1: Antiretroviral Treatment
• d4T, 3TC, NVP (transaminitis)• d4T, 3TC, ABC (worsening
transaminitis)• ARVs stopped (transaminitis
resolved)• d4T, 3TC, NLF (transaminitis)

Case 1:Management Challenge
• Stop ARVs and treat HCV• Continue ARVs and treat HCV• Continue ARVs and biopsy liver
Case 2
• 34 y/o HIV-infected man– HIV+ in 1991– H/O IDU and alcohol use– Persistent transaminitis (ALT 160-280)– Negative HBV and HCV serologies– HCV RNA > 1,000,000 c/mL

Case 2: Diagnosis
• Liver biopsy– Fibrous expansion of portal areas,
portal inflammation, piecemeal necrosis, activity in >2/3 of lobules

Case 2: HIV Therapy
• Initial CD4 50, HIV RNA 100,000• 6/98 d4T, 3TC, ADF (renal toxicity)• 8/98 ABC, 3TC, NLF, EFV• 11/98 NLF stopped for rash• 12/98 transaminitis• 3/99 all ARVs stopped (despite
VL>1 mil)• 6/99 d4T, 3TC, ABC, NLF (jaundice)

Case 2: Management Challenge
• Hold ARVs until LFTs normalize, then restart with different agents
• Stop ARVs and treat HCV• Continue ARVs and treat HCV

Consultation Services for Clinicians Caring for Patients with HIV/AIDS
• Local expert clinicians• Regional and local AIDS Education and
Training Centers• National HIV Telephone Consultation
Service (Warmline)– (800) 933-3413
• National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline)– (888) HIV-4911

National HIV/AIDS Clinicians’ Consultation Center
A Joint Program of UCSF and San Francisco General
HospitalSupported by HRSA and
CDC
http://www.ucsf.edu/hivcntr
PEPLine (888) 448-4911
Warmline (800) 933-3413


















