Hiv – Aids in Neurology
25
HIV – AIDS IN NERVOUS SYSTEMS DIAH MUSTIKA HW, SpS,KIC Intensive Care Unit of Emergency Department Navy Hospital Dr Ramelan Surabaya
-
Upload
dessy-missa -
Category
Documents
-
view
12 -
download
3
description
xyz
Transcript of Hiv – Aids in Neurology
-
HIV AIDS IN NERVOUS SYSTEMS
DIAH MUSTIKA HW, SpS,KIC
Intensive Care Unit of Emergency Department
Navy Hospital Dr Ramelan Surabaya
-
Multiple areas of the nervous system may be
involved simultaneously or sequentially.
Without anti-retroviral treatment, up to 80% of
patients are symptomatic and for 30%,
neurologic symptoms are the initial clinical
problem.
Neurologic syndromes may be the sole clinical
problem or cause of death.
-
All levels of the neuraxis are potential sites of
involvement:
Meninges
Brain
Spinal cord
Cranial and peripheral nerves
Autonomic nervous system
Muscle
-
CLINICAL SYNDROMES
BRAIN SYNDROMES
Meningitis
Dementia
Stroke
Seizures
Degenerative Disorders
-
SPINAL CORD SYNDROMES
Transverse myelitis
Progressive myelopathy
-
NERVE AND MUSCLE
Bells palsy
Hearing loss
Peripheral neuropathies
Autonomic neuropathy
Myopathy
-
HOW DOES HIV AFFECT THE NERVOUS SYSTEM?
HIV easily crosses the blood-brain barrier
Dave R, Pomerantz RJ. (2005). HIV neuropathogenesis: persistent
infection, persistent questions. Science & Medicine.
-
HOW DOES HIV AFFECT THE NERVOUS SYSTEM?
General immunosuppression can lead to:
Opportunistic Infections
Fungal (Cryptococcal Meningitis)
Parasitic (Toxoplasmosis)
Viral (Progressive Multifocal
Leukoencephalopathy)
HIV-Related Tumors
-
HOW DOES HIV AFFECT THE NERVOUS SYSTEM?
Primary HIV Disease can lead to:
AIDS Dementia Complex (brain)
Vacuolar Myelopathy (spinal cord)
Peripheral Neuropathy (nerve)
Meningitis (acute and chronic)
-
HOW DOES HIV AFFECT THE NERVOUS SYSTEM?
HIV indirectly destroys cells in the nervous system
Kaul, Garden & Lipton (2001). Pathways to neuronal injury and apoptosis in HIV-
associated dementia. Nature 410, 988-994.
-
HOW DOES HIV AFFECT THE NERVOUS SYSTEM?
10-15% of AIDS patients present with neurologic
symptoms only
35-50% of AIDS patients have neurologic
symptoms during life1,2
75-90% have neuropathologic abnormalities at
death3
1) Brouwman et al, Neurology. 1998 ; 50:1814-20.
2) McArthur J Neuroimmunol 2004; 157 : 3-10
3) Vago et al., AIDS. 2002;16:1925-8.
-
Primary or HIV-Related Syndromes of Acute
Infection
Meningitis or encephalitis
Seizures, generalized or focal
Transverse myelitis
Cranial or peripheral neuropathy ( Bells palsy or
Guillain-Barre-type neuropathy )
Polymyositis +/- myoglobinuria
-
Primary or HIV-related Syndromes of Chronic Infection: common disorders
Meningeal pleocytosis +/- symptoms
Dementia and / or psychiatric disturbances (AIDS dementia complex, ADC )
Strokes
Seizures
Progressive myelopathy
Neuropathy or myopathy
-
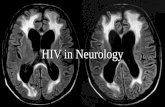
HIV AND
CNS INVOLVEMENT
-
CEREBRAL TOXOPLASMOSIS
Most common CNS impairment seen in HIV
Is a reactivation of a latent protozoal infection
Can also affect myocardium, lung skeletal muscle
Generally presents as multiple enhancing lesions with perifocal oedema in the basal ganglia and grey-white matter interface of the cerebral hemispheres, although can be in any part of brain
-
TOXOPLASMOSIS
-
TOXOPLASMOSIS
Common signs and symptoms
Headache, fever
Confusion
Lethargy
Seizure (may be initial clinical manifestation)
Focal neurologic signs (50%-60% of HIV-infected cases)
Usually hemiparesis or visual field defects
Treatment
Antio-toxo drugs: Sulfadiazine, pyrimethamine, clindamycin, pyrimethamine, folinic acid
-
TOXOPLASMOSIS
Usually responds well to treatment
Usually the worse the initial presentation, the
longer the recovery; may have some long term
residual deficits
Can sometimes have multiple small lesions
which present with quite specific / unusual
sensory / motor / cognitive symptoms
-
CRYPTOCOCCYL MENINGITIS, TB
MENINGITIS
Both quite common presentations
Crypto caused by fungal infection
TB may also cause focal lesions as well as the
menigitis
Both may or may not have other systemic
illness associated e.g. Cryptococcosis, TB lung,
spine, miliary TB
-
CMV ENCEPHALITIS (AND OTHERS)
CMV= cytomegalovirus
Quite common; CMV encephalitis is a reactivation of latent CMV infection - features cell death in meninges and peri-ventricular area
Often associated with a CMV retinitis
Rapidly progressing; responds well to treatment if caught in time otherwise responds poorly
-
CMV ENCEPHALITIS (AND OTHERS)
Treatment is usually IV ganciclovir,
valganciclovir, foscarnet, cidofovir these
drugs can be quite toxic
Presentations vary, however usually involve
confusion, headache, delirium
Can have focal neurology, cranial nerve deficits
-
CMV ENCEPHALITIS (AND OTHERS)
Therapy approach again is treat what presents;
often complicated by permanent visual field
loss
Other encephalitis presentations include HSV
(Herpes Simplex Virus) and VZV (Varicellar
Zoster Virus)
-
HIV AND PNS INVOLVEMENT
-
INFLAMMATORY DEMYELINATING
POLYNEUROPATHY (IDP)
IDP, and its more severe cousin Gullain- Barre
Syndrome sometimes occur acutely in
otherwise well HIV+ patients, or in HIV+
patients with advanced disease.
Seems to be some sort of auto-immune
response that attacks the myelins sheath
mechanism is poorly understood
Treated with IVIg