
History and policy a typology of approaches and its uses2
16
This paper is part of the proceedings of the 2 nd Annual conference on Qualitative Research for Policy Making, 26 & 27 May 2011, Belfast History and Policy A Typology of Approaches and Its Uses Ellen van Reuler 1 Centre for the History of Science, Technology and Medicine The University of Manchester United Kingdom Abstract The relevance of historical studies for policy is a topic that has become increasingly debated over the past few years. In this paper, I develop a typology of modes of policy relevant history that helps us classify and apply historical scholarship in the policy environment. This typology is based on distinctions along two dimensions. The first dimension is the concept of history applied, because history can be ‘the past’ or a method to study developments over time. The second dimension is the primary aim of the study, which can be either problem-oriented or understanding-oriented. These two dimensions are combined into a typology of four modes of history for policy. Central to this model is that each of the four modes requires specific ‘translational devices’ if we want to transfer the results of the historical analyses to the policy process. Several elements of this typology are illustrated drawing from my research on the contemporary history of cancer care and palliative care in England and the Netherlands. 1. Introduction Why should the policy community pay attention to history? The following two quotes provide suggestions. The first is from a noted historian of medicine, the second from a physician who was the English Chief Medical Officer from 1998 to 2010. Policy is always history. Events in the past define the possible and the desirable, set tasks, and define rewards, viable choices, and thus the range of possible outcomes. As we move through time those choices reconfigure themselves and trends may establish 1 I would like to thank John Pickstone from the Centre for the History of Science, Technology and Medicine in Manchester for the stimulating discussions that shaped the typology presented in this paper. The research reported in this paper is funded by a Wellcome Trust Doctoral Studentship.
-
Upload
merlien-institute -
Category
Education
-
view
1.445 -
download
1
description
Presented at the 2nd European Conference on Qualitative Research for Policy Making, 26-27 May 2011, Belfast, UKOrganised by Merlien Institute
Transcript of History and policy a typology of approaches and its uses2

This paper is part of the proceedings of the 2nd
Annual
conference on Qualitative Research for Policy
Making, 26 & 27 May 2011, Belfast
History and Policy
A Typology of Approaches and Its Uses
Ellen van Reuler
1
Centre for the History of Science, Technology and Medicine
The University of Manchester
United Kingdom
Abstract
The relevance of historical studies for policy is a topic that has become increasingly
debated over the past few years. In this paper, I develop a typology of modes of policy
relevant history that helps us classify and apply historical scholarship in the policy
environment.
This typology is based on distinctions along two dimensions. The first dimension is
the concept of history applied, because history can be ‘the past’ or a method to study
developments over time. The second dimension is the primary aim of the study, which
can be either problem-oriented or understanding-oriented. These two dimensions are
combined into a typology of four modes of history for policy. Central to this model is that
each of the four modes requires specific ‘translational devices’ if we want to transfer the
results of the historical analyses to the policy process. Several elements of this typology
are illustrated drawing from my research on the contemporary history of cancer care and
palliative care in England and the Netherlands.
1. Introduction
Why should the policy community pay attention to history? The following two quotes
provide suggestions. The first is from a noted historian of medicine, the second from a
physician who was the English Chief Medical Officer from 1998 to 2010.
Policy is always history. Events in the past define the possible and the desirable, set
tasks, and define rewards, viable choices, and thus the range of possible outcomes. As we
move through time those choices reconfigure themselves and trends may establish
1 I would like to thank John Pickstone from the Centre for the History of Science, Technology and
Medicine in Manchester for the stimulating discussions that shaped the typology presented in this paper.
The research reported in this paper is funded by a Wellcome Trust Doctoral Studentship.

themselves - but at any given point the ‘actionable’ options are highly structured. It is the
historian’s disciplinary task to define those likelihoods. Most important, what history can
and should contribute to the world of policy and politics is its fundamental sense of
context and complexity, of the determined and the negotiated. Rosenberg (2006, p.28)
I never ever heard a discussion during my twelve years in post - although I tried many
times to raise it - where people would sit down and say: Now, have we ever done
anything like this before? What tools did we use? What worked well? What didn’t work
well and how are we going to take that learning into the change programme that we are
now going to introduce?’ People reached for the tools almost absent-mindedly. Say,
we’ve got to have a few regional road shows, we’ve got to do some legislation, we’ve got
to do this, we’ve got to do that, but not thinking fundamentally about change the way that
I believe is done in many of the most innovative organisations in other sectors.
Donaldson (2011, 37:43 - 38:30).
Rosenberg and Donaldson both maintain that history can be useful for policy, but their
concepts of history and their aims for the use of history differ. These differences and their
consequences for the transfer of insights from historical studies to policy making are
discussed in this paper.2
2. Literature review
Although not a main focus in social sciences, history-conscious approaches are certainly
not unknown. But most of the effort relates history to fields like sociology and
anthropology, rather than to ‘applied’ social sciences such as policy studies (for example,
Hodgson, 2001; Mahoney & Rueschemeyer, 2003; McDonald, 1996; Monkkonen, 1994).
Nevertheless, the case for the use of historical evidence to inform policy making has been
made convincingly (Berridge, 2008; The British Academy, 2008). Examples of
arguments for the value of historical perspectives for policy are:
1. Long-term perspective allows for a sense of chronology and the identification of
continuity as well as change;
2. Diachronic attitude supports the identification of slowly developing and temporally
distant causes of current problems;
3. Historical analyses allow for combinations of various types of source material, levels
of interpretation, and theoretical perspectives;
4. Contextualisation of issues under investigation provides insight into a wide range of
influences lying behind the immediate issue (See Berridge & Strong, 1991; Berridge,
1994, 2000, 2001, 2008, 2010; Hacker, 2005; Pollitt, 2008; Stevens, Rosenberg &
Burns, 2006; Tilly, 2006; Zelizer, 2000).
2 An important distinction can be made between policy history and histories that are of use for policy. On
the one hand, accounts of the first type describe and analyse, for instance, the decisions that led to a
particular policy document or governmental intervention. This does not imply that that these histories
are always relevant for current policy. On the other hand, policy relevant histories need not be
concerned with policy as such, but provide insights of use to policy makers. This paper deals with these
policy relevant histories.

At a time in which publications in public policy ‘remain present and future oriented,
and history-lite’, historical studies emphasise aspects that differ from mainstream policy
analyses (Pollitt, 2008, p.13; also Raadschelders, 1998; Zelizer, 2000)..
Given the development of the British History & Policy website from 2002 onwards
and the publication of books and articles, such as, Pierson (2004; 2005), Pollitt (2008),
Stevens et al. (2006), and Zelizer (2005), it might seem that the value of history for
policy is an issue that has emerged only recently.3 However, concepts like dynamics of
policy and inheritance in policy appeared in earlier studies (Rose, 1976; Rose & Davies,
1994). Worth mentioning are also the books on the uses of history by decision makers
and social history and social policy by May (1973), Neustadt & May (1986), and
Rothman & Wheeler (1981).
Some of these authors, most notably Rothman and Wheeler, mention that the
translation of historical studies for policy audiences is a complex endeavour. Insight into
the different modes of history for policy and the strategies that can be used to maximise
their potential to inform policy is crucial, but this is an issue hardly addressed in the
literature.
3. Research Method
The primary aim of this paper is to present a simple typology of forms of historical
analysis which are useful for policy and the strategies for translation of these analyses to
a useful input for policy making. In subsection 4.1, I sketch the typology, while the
subsequent subsection discusses the relationship between the modes of history and policy
issues. Subsection 4.3 contains a note on the presentation of the outcomes of historical
studies for policy. I give some examples to illustrate the typology and the ‘translational
devices’ that can be used to transfer the results of the historical analysis to the policy
process in subsections 4.4 and 4.5. These examples are based on my ongoing research on
the histories of palliative care4 and cancer care in England and the Netherlands during the
3 See http://www.historyandpolicy.org.
4 Notions of palliative care have changed over time and several closely related terms, such as hospice
care, palliative medicine and terminal care, are in use. The term currently dominating English
governmental policy is end of life care (see Department of Health, 2008). A well-known definition of
palliative care is provided by the World Health Organisation:
‘Palliative care improves the quality of life of patients and families who face life-threatening illness, by
providing pain and symptom relief, spiritual and psychosocial support from diagnosis to the end of life
and bereavement. Palliative care:
- provides relief from pain and other distressing symptoms;
- affirms life and regards dying as a normal process;
- intends neither to hasten or postpone death;
- integrates the psychological and spiritual aspects of patient care;
- offers a support system to help patients live as actively as possible until death;
- offers a support system to help the family cope during the patients illness and in their own
bereavement;
- uses a team approach to address the needs of patients and their families, including bereavement
counselling, if indicated;
- will enhance quality of life, and may also positively influence the course of illness;
post war era. These histories are grounded in a variety of primary and secondary written
sources, such as policy reports and parliamentary proceedings, as well as (oral history)
interviews.5
4. Discussion
4.1 A typology of modes of policy relevant history
The quotes in the introduction stress the importance of history for policy, but they present
dissimilar modes of history. It is helpful to conceptualise these differences by
distinguishing the approaches on two dimensions:
A. The concept of history applied:
a. History as ‘the past’;
b. History as a method to study the social world and its development over time.
B. The focus of the study:
a. Problem-oriented studies, which start with a particular problem in mind and aim
to contribute to a solution for this issue;
b. Understanding-oriented studies, which increase our comprehension of policy
and its contexts.
Illustration 1 shows the typology of modes of history for policy that emerges if we
combine the two dimensions discussed in the previous paragraph. In this typology,
investigations following Donaldson’s suggestions would result in a mode 1 analysis,
while Rosenberg’s ideas match with mode 4 histories for policy.
- is applicable early in the course of illness, in conjunction with other therapies that are intended to
prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to
better understand and manage distressing clinical complications’ (World Health Organisation,
2006). 5 For reasons of readability, I decided to exclude references from these examples to avoid densely
referenced accounts. Further references are available from the author upon request. For a discussion of
the debates about the regional concentration of cancer care, see also Van Reuler (2008). For a brief
analysis of the position of hospices in the health care system in England and the Netherlands, see Van
Reuler (2010).
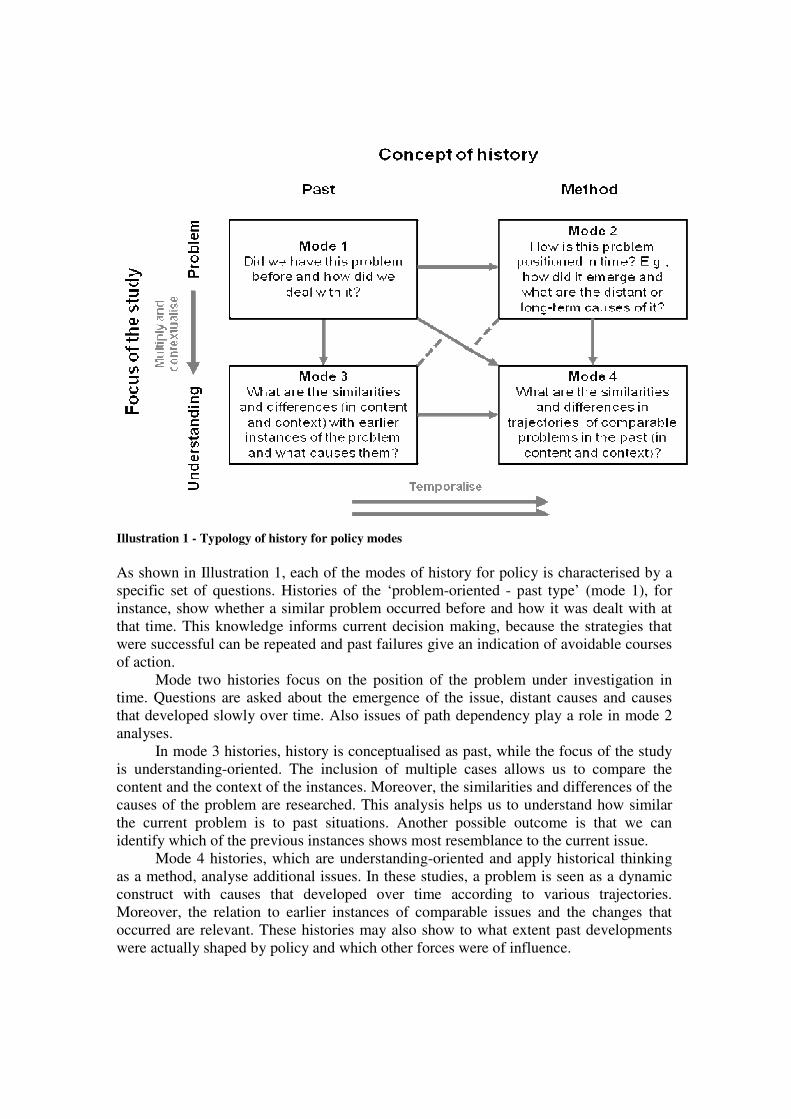
Illustration 1 - Typology of history for policy modes
As shown in Illustration 1, each of the modes of history for policy is characterised by a
specific set of questions. Histories of the ‘problem-oriented - past type’ (mode 1), for
instance, show whether a similar problem occurred before and how it was dealt with at
that time. This knowledge informs current decision making, because the strategies that
were successful can be repeated and past failures give an indication of avoidable courses
of action.
Mode two histories focus on the position of the problem under investigation in
time. Questions are asked about the emergence of the issue, distant causes and causes
that developed slowly over time. Also issues of path dependency play a role in mode 2
analyses.
In mode 3 histories, history is conceptualised as past, while the focus of the study
is understanding-oriented. The inclusion of multiple cases allows us to compare the
content and the context of the instances. Moreover, the similarities and differences of the
causes of the problem are researched. This analysis helps us to understand how similar
the current problem is to past situations. Another possible outcome is that we can
identify which of the previous instances shows most resemblance to the current issue.
Mode 4 histories, which are understanding-oriented and apply historical thinking
as a method, analyse additional issues. In these studies, a problem is seen as a dynamic
construct with causes that developed over time according to various trajectories.
Moreover, the relation to earlier instances of comparable issues and the changes that
occurred are relevant. These histories may also show to what extent past developments
were actually shaped by policy and which other forces were of influence.

Illustration 1 also shows possible moves from mode 1 studies to more complex
modes of policy relevant history. If we want to progress vertically from problem-oriented
to understanding-oriented studies, we multiply the number of cases analysed and we
contextualise them. By contrast, the horizontal move from history as past to history as
method entails a temporalisation of the phenomenon under investigation. In other words,
we move from a static view of the subject to a dynamic conceptualisation of the issue and
its causes.
The arrows in Illustration 1 do not imply that every history for policy study has to
start with a mode 1 analysis and add layers of complexity to move to mode 4. It is
possible to develop a mode 2, 3 or 4 historical analysis immediately. Moving from mode
1 or mode 2 to mode 4 has the benefit that the problem around which the questions in
mode 1 and 2 studies are centred remains present in understanding-oriented modes of
history for policy. This implies that a link to a current policy debate will exist. By
contrast, many historians start their studies for other reasons than its direct policy
relevance and will carry out a mode 4 analysis. Nevertheless, these analyses may hold
lessons that can inform current or future policy making. The moves from the four modes
of history to policy are elaborated on in the following subsection.
4.2 Translational devices
The intellectual projects of historians and policy makers do not align naturally. Policy
makers focus on knowledge to inform actions, whereas historians develop their analyses
mainly as knowledge for understanding. Therefore, we need strategies, which I call
‘translational devices’, to ensure that the insights from policy relevant histories are
framed in a way that enables their transfer to the policy process.
Illustration 2 shows the same typology as Illustration 1, but now the policy issue
for which the histories are relevant is placed in the centre. We can see that the policy
issue is closer related to the problem-oriented modes of history than to the understanding-
oriented modes. Each of the four modes of history for policy sketched in the previous
subsection has its own specificities. Consequentially, the transfer from insights from each
of the modes of history to inform policy has its own characteristics. These relationships
are indicated with the arrows A to D in Illustration 2. I sketch the ‘translational devices’
that can help us to maximise the potential of each of the modes of history to inform
policy in the following paragraphs.

Illustration 2 - The modes of policy relevant history and their relation to policy issues
Mode 1 histories are closely linked to Donaldson’s suggestion to consider whether we did
something comparable in the past and to what extent the outcomes were favourable
before opting for a policy tool. The reasoning strategy behind the identification of these
‘good guides from the past’ for current practice is based on the analogy. The answers to
the questions for this mode of history for policy often result in clear suggestions for
policy makers (See Rose, 2005, p.42-47 for a discussion of learning policy lessons from
analogies).
In mode 2 history for policy analyses we place an issue in the flow of time and then
come back to the specific issue. Which insights for the policy process can we gain from
this work? Examples are an understanding of sequences of developments, insight in the
duration of episodes, identification of temporally distant causes and influences
developing gradually over time, and knowledge of differences in the pace of various
developments. Some of these outcomes of mode 2 histories for policy analyses, transfer
to policy relatively easily. Temporally distant causes, for instance, can be treated
similarly to causes that developed recently in the sense that policy makers can try to
develop strategies to deal with them to reduce the problem. An understanding of the
sequence of developments provides insight into cause and effect relationships beyond the
level of statistical correlation. Duration and pace of developments are particularly

relevant for policy makers to develop a feeling for the time scale that might be needed to
implement a solution to the problem.
Arrow C represents the move from mode 3 histories to policy. As mentioned
before, the lessons from understanding-oriented histories for policy are harder to
determine. In this case, we have to make an adaptation for the differences in context of
the instances studied. A possible outcome can be that we can say that the contexts of two
situations are relatively comparable, while differences with the third and the fourth case
are substantial. In drawing lessons from mode 3 histories for a policy issue, it is
important to assess the consequences - either favourable or unfavourable - of differences
in context. However, significant contextual differences need not imply that the past
instance has nothing to offer to the current policy issue. Even if the context differs, a past
instance may, for example, help policy makers to generate alternative solutions.
Mode 4 histories have to be adapted for time as well as context if the outcomes are
to feed into policy (Arrow D in Illustration 2). Since these two operations enabled the
move from mode 2 and 3 histories to policy, most ideas presented in the previous
paragraphs can be of use to mode 4 histories. However, the combination of characteristics
in mode 4 histories lends itself to three further uses in a policy context.
- Reasoning about continuity and change in contexts: This translational device
combines an analogy with a force field analysis (see Lewin, 1951; Daft, 2003). The
application of this ‘extended analogy’ means that you search for historical
antecedents of current problem. For each of the instances, you plot the major factors
stimulating and restraining change in a force field diagram. A comparison of these
force fields provides an indication of the feasibility of the implementation of a
proposal and will hold clues about the main barriers for change.
- Policy evaluation: Mode 4 histories are particularly suitable for the evaluation of
policies with a focus on context, long time spans, and unintended consequences. The
average evaluation of policy interventions by mainstream policy analysts takes place
within a few years after implementation. Consequentially, long-term influences
cannot be taken into account. Another strength of history is contextualisation. For
long-term policy evaluation this means that external factors that interfered with the
implementation of the policy and the outcomes that were achieved can be identified.
- Search light: Offering mode 4 histories to policy makers can help them to
incorporate a feeling for developments over time and context in their future problem
solving.
In addition to the Arrows A to D, Illustration 2 also includes four dotted arrows.
They indicate that relatively complex histories can be reduced to simpler, policy relevant
histories by stripping away layers of complexity. Is it worth the effort to develop complex
modes of history if we might want to reduce them to simpler forms to increase their
potential to inform policy making? My answer would be affirmative. Mode 1 studies, for
example, can be enriched if a mode 3 study is carried out, because this allows you to
select not just a case in the past, but the ‘best case’ - i.e. the case with the most similar
context.

4.3 A note on presentation
In addition to the dissimilarities of the intellectual projects of policy makers and
historians, the standards for presenting research differ as well. Historians generally prefer
detailed narratives, whereas policy makers favour a list with recommendations for action.
Therefore, historians who want to present their work to the policy community, should
think carefully about the language and format they use. The further one moves away from
mode 1 histories, the more pressing this issue becomes.
Historians might not want to position themselves as advisors who advocate a certain
action. In that case, the transfer of mode 2, 3 and 4 histories to policy making can be
supported by reducing the histories to a summary of the main changes, stabilities, causes,
trajectories and contextual influences. An overview of these issues is likely to be a more
usable input for policy than a (long) historical narrative.
Not only the presentation of the research results, but also the way in which they are
framed matters. For mode 2, 3 and 4 studies, it can be useful to frame the histories in
concepts and theories policy makers are familiar with. This approach helps to make the
outcomes of historical studies more accessible to policy makers. Moreover, these models,
such as Kingdon’s model of policy streams, can help historians to articulate clearer
whether actual practice converged on or diverged from what policy makers would have
expected on the basis of these models (Kingdon, 1984).6
4.4 Example 1: The regional organisation of Dutch cancer care In this subsection, I illustrate the typology using the case of the current debates on the
regional organisation of cancer care in the Netherlands. I will first give an overview of
the current Dutch health care system to provide the context for this debate. Since the
example in subsection 4.5 relates to developments in English health care, I now describe
the two health care systems briefly from a comparative perspective.
Four main areas of differences between the English and the Dutch health care
system can be identified.
1. Funding arrangements. The English National Health Service (NHS) is funded by the
government from tax revenues. In the Netherlands, however, inhabitants are obliged
to insure themselves against health care costs.
2. Ownership. Whereas the British state is - in the end - responsible for NHS premises,
the Dutch health care infrastructure is owned privately. Most health care providers
in the Netherlands operate on a not-for-profit basis.
3. Governmental influence. In comparison to the situation in the Netherlands, the
influence of the British government on the NHS is relatively direct and far-reaching.
4. Reform and stability. Many observers perceive the English NHS to be in a
continuous flux since the reforms of the early 1990s. The Dutch health care system
is comparatively stable and changes are implemented more gradually (for example,
Boot & Knapen, 2005; Ham, 2004; Rivett, 1997; Schäfer, Kroneman, Boerma, van
6 In this way, histories for policy can not only influence policy making, but they might also have an
impact on the academic study of policy.

den Berg, Westert, Devillé & van Ginneken, 2010; Schrijvers & Droyan Kodner,
1997).
One of the workshops during the concluding conference of the Dutch National Cancer
Control Programme (NCCP)7 in November 2010 focussed on the regional coordination of
oncological care. The attendees agreed that the implementation of a structure in which
specific cancer treatments are concentrated in a limited number of hospitals would be
desirable for reasons related to the quality and efficiency of care.
A typical mode 1 history for policy question would be whether a regional structure
for cancer care was implemented in the Dutch health care system before. The short
answer is that this has not been the case. A somewhat longer response is that the
governmental planning of centres for radiotherapy on the basis of the law on specialised
medical interventions (WBMV)8 from the 1980s onwards was an earlier instance of the
centralisation of cancer care. The implementation of this law was successful from the
perspective of the central government. If we apply an analogy without giving the
situation much further thought, we could say that the introduction of a law on the regional
organisation of cancer care would be an option. However, the inclusion of radiotherapy in
the WBMV is a topic on the political agenda, because the government wants to increase
competition in the health care system and the central control of the availability of medical
equipment does not fit this context. The general trend in health care policy is toward
delegation of power from the government to health insurers. Therefore, legal codification
of the regional concentration of cancer care is unlikely to be a feasible option. These
reasons show that a simple analogy is not always the best lesson history has to offer to
policy. The following paragraphs illustrate what mode 2, 3 and 4 histories might add.
A mode 2 history for policy analysis would stress how the current problem
developed over time. Among the drivers for the recent emergence of the debate on the
centralisation of cancer care are the increased availability of data on hospital performance
and the fact that the breast cancer patients association in cooperation with the consumers
association published a ranking of the best hospitals for breast surgery in 2005. In
addition, insurers obtained the power to contract with hospitals on the basis of quality and
price for a governmentally defined segment of medical treatments during the recent
health reforms. The first publicly known instance in which a health insurer used this
power to influence the place of treatment of their customers occurred in October 2010.
More indirect causes for the debate on the regional structure of cancer care that a
historian would identify are, for instance, the increasing complexity of cancer treatments
and the availability of international, comparative statistics on cancer survival rates.
A limited form of a mode 3 historical analysis took place when one of the attendees
of the NCCP conference mentioned that the regional organisation of cancer care had been
discussed during the mid 1990s and 2000s. Her fairly short conclusion was that ‘the time
was not yet ripe for it’ in those days, but that the proverb ‘three times lucky’ would hold
this time. A historian could contextualise these developments further as part as a mode 3
analysis. In that case, we would come across influences like changes in the health care
system and treatments available for cancer. A likely conclusion of a comparison of the
7 In Dutch this programme is known as the ´Nationaal Programma Kanker (NPK 2005-2010)´.
8 In Dutch: ´Wet Bijzondere Medische Verrichtingen
´.

three instances of attempts to concentrate oncological care would be that the context of
this issue had indeed changed substantially. To a historian, however, the implications of
this finding for the feasibility of the introduction of concentrated cancer care would not
be as obvious as for the workshop participant.
As became clear from the discussion of history for policy in Subsection 4.1, mode
4 analyses are the most complex form of the four. This means that a mode 4 historical
analysis of the regional structure of cancer care would incorporate most of the issues
elaborated on for the modes 1, 2 and 3. On top of that, attention would be paid to the
trajectories followed by the variables influencing the concentration of oncological care.
The dynamic context of the three attempts to organise Dutch cancer care at a regional
level would also be studied. These investigations indicate, among others, that the
implementation of the first advisory report that suggested to centralise cancer care was
hampered by the interests of hospitals and medical specialists who were afraid to loose
part of their work.9 Moreover, this analysis would include the fact that the centralisation
of oncological care dropped from the political agenda during the second half of the
1990s, because parliament had to deal with more pressing issues in health care. One of
the conclusions about the second debate on centralisation of cancer care, which took
place in 2004, could be that the role of the only independent, specialist cancer hospital in
the Netherlands did not contribute to building support for this idea. Although the debate
first emerged in the context of the start of the NCCP, the publications on the
centralisation of cancer care by the directors of the cancer hospital that appeared shortly
afterwards polarised the debate.
The main question for the current debate on the concentration of oncological care
is: Would a renewed attempt to implement it succeed? In my view, an extended analogy
is a particularly suitable translational device to help us answer this question. The force
field analyses show that the situation remained relatively stable between the first and the
second attempt to centralise cancer care, but that the changes between the second attempt
and the current situation are significant. The shifts of the balance in the governance
structure of health care, with an increasingly central position for the health insurers,
makes successful implementation of centralisation in the current circumstances more
plausible than in the past. Additionally, an extended analogy holds information that
health insurers who aim to concentrate oncological care could interpret as the main
factors constraining change. For example, the enumeration structure for medical
specialists has not changed significantly and hospitals would still be afraid of loosing
work and income.
9 Under the health care payment system in place at that time, loosing work meant a reduction of income
for hospitals and for consultants who worked in hospitals that were not part of a university.

4.5 Example 2: The comparative histories of English and Dutch voluntary
palliative care As described in the methods section of this paper, my project focuses on comparative
histories of palliative and cancer care. In this section, I will briefly explain the reasons for
comparative histories for policy and then related this to the typology presented in this
paper.
What is to be won by including a geographical comparison in policy relevant
histories? Comparative histories can be used to develop extra analogies or compare
trajectories of similar developments at different places. More extensive use of
understanding-oriented modes of history for policy can be made if the issue under
investigation is explicitly framed comparatively. These questions can relate, for instance,
to the reasons why a phenomenon is present in one country, but absent at another place.
Another example of a comparative history for policy question is why the first hospice that
was similar to the English hospices was established in the Netherlands nearly 25 years
after St. Christopher’s hospice was founded in London in 1967.
In the following paragraphs, I explore a comparative historical question of which the
answer can be of use to policy making. I will present the backgrounds to voluntary
palliative care by developing a mode 2 history for policy analysis.
In a report published by the think-tank Demos in Autumn 2010, it was argued that
the establishment of voluntary palliative care, especially in the form of home care
services, in Britain would be desirable (Leadbeater & Garber, 2010). A related,
interesting comparative question is how England developed a relatively medically
oriented system of palliative care provision, whereas a differentiated structure, including
medically oriented palliative care as well as voluntary palliative care by home care teams
and in low-care hospices, evolved in the Netherlands.
A mode 2 analysis indicates that the changing balance between voluntary and NHS
driven provision of palliative care is an important theme in the history of palliative care
in England. Cicely Saunders wrote about the decision to establish St. Christopher’s
Hospice, the first modern hospice in England and indeed in the world, outside the NHS:
‘We want to be independent because we need freedom of thought and action; we want to
be an interdenominational but a religious foundation, and we want freedom to develop
and expand as we are led to do so’ (quoted in du Boulay & Rankin, 2007, p.64).
An arrangement with the Regional Hospital Board was, however, negotiated for St.
Christopher’s. Moreover, the NHS participated in the foundation of hospices during the
mid 1970s. The governmental influence on providers of palliative care increased by the
late 1980s, because the government expected District Health Authorities to cooperate
with the voluntary sector to ensure that the needs of their population were met. These
requirements were soon accompanied by ring-fenced funds for hospices. By the mid
1990s, NHS managed hospices accounted for circa a quarter of the total number of
hospices. Other hospices relied on the NHS for at least a substantial part of their income.
Under New Labour, governmental control of palliative care continued to increase. While
levels of public funding rose, the same was true for control measures, such as the
application of targets. The most recent major policy document on palliative care in
England is the End of Life Strategy that was published in 2008. My evaluation of this

plan is that the implementation would result in a further integration of palliative care into
the NHS. Thus we can see that, the introduction of voluntary palliative care would imply
a significant move away from the past trends in England.
The first initiatives to establish palliative care in the Netherlands were volunteer
led. These services support people dying at home and their relatives. Additionally, these
volunteers created a form of palliative care, which appears to be unique for the
Netherlands. In these so-called low-care hospices, volunteers provide care for a few
terminally ill persons at a time.
In terms of governmental policy for palliative care in the Netherlands, it is
noteworthy that the Secretary of State for Health decided in the mid 1990s that palliative
care had to be integrated into the health care system as a whole. Therefore, she stimulated
care homes and nursing homes to establish palliative care units, while low-care hospices
would not be reimbursed for their housing costs. This policy was an impetus for the
creation of palliative care units in care and nursing homes, but the proliferation of low-
care hospices continued. Though hardly formally debated, a new chapter in palliative care
policy seems to have started in 2007. The Minister of State for health received a report
which stated that low-care hospices experienced problems with funding their housing
costs. Her response was to grant them additional resources. Currently, around 80% of the
costs of the low-care hospices are on average covered by public funds. Most of the people
in charge of low-care hospices are keen to continue to rely on private funds for the
remainder of their income, because this gives them the freedom to run their low-care
hospice as they want. Currently, the extent to which the voluntary sector palliative care
providers can and should be accountable for the public money they receive is being
debated.
Applying the translational device of the identification of developments over time,
these mode 2 accounts show, among others, that the current structure of the provision of
palliative care in both countries is firmly rooted in its development over time. Therefore,
it is questionable whether the implementation of voluntary palliative care will be
successful in England. It is, for instance, unsure whether potential English volunteers will
perceive a deficiency in the provision of care for the dying that they want to create a
service for. Moreover, it can be expected that tensions will emerge between the current
providers of palliative care and the new entrants. The comparative dimension of this
example reveals that voluntary palliative care has also disadvantages from a
governmental perspective. The Dutch experiences indicate, for example, that it is hard to
ensure that sufficient levels of voluntary palliative care are available around the country.
Additionally, quality criteria and output targets are difficult to impose on voluntary
providers of palliative care.
5. Conclusion
In this paper, I sketched a typology of four modes of history for policy based on the
distinctions between 1) history as past and as method and 2) the focus of the study, which
is either problem-oriented or understanding-oriented. Moreover, several translational
devices to move from histories to policy were discussed. Mode 4 and mode 2
translational devices were illustrated by discussions of the debates on the regional

organisation of cancer care in the Netherlands and the suggestion to introduce voluntary
palliative care services in England.
The typology of modes of history for policy is a stylised model. It is certainly
possible to imagine investigations that combine aspects of two or more modes of history
for policy. Moreover, additional translational devices to move from history to policy can
be developed. Nevertheless, the examples presented in this paper show that the typology
is a useful tool to think through the various modes of policy relevant history and the
translational devices that are needed to derive a lesson from these histories that is of
practical use to the policy community.
If history attracts interest from a policy perspective, history is often conceptualised
as the past. So, a legitimate question is: ‘Why should we move beyond these relatively
simple accounts that might hold clear lessons and apply history as method approaches?’
A short answer is that the temporalisation of an issue has several benefits. A multilayered
account of the emergence of a problem enables us to identify, for example, temporally
distant causes or developments that unroll slowly over time. Additionally, mode 4
histories for policy allow us to look at a fairly complex picture of how a topic evolved
and how it compares to earlier developments. As illustrated in the example about the
regional organisation of cancer care in the Netherlands (Subsection 4.4), this enhances
our understanding of the present options open to various stakeholders. Not all issues
require these extensive analyses and it is the task of the historian to judge which mode
and translational device are most suitable and feasible in a particular situation.
References
Berridge, V. (1994). Researching Contemporary History: Aids. History Workshop
Journal (38), 228-234. Berridge, V. (2000). History in Public Health: A New Development for History? Hygiea
Internationalis, 1 (1), 23-36. Berridge, V. (2001). History in the Public Health Tool Kit. Journal of Epidemiology and
Community Health, 55, 611-612. Berridge, V. (2008). History Matters? History's Role in Health Policy Making. Medical
History, 52, 311-326. Berridge, V. (2010). The Art of Medicine. Thinking in Time: Does Health Policy Need
History as Evidence? The Lancet, 375 (March 6), 798-799. Berridge, V. & Strong, P. (1991). Aids and the Relevance of History. Journal for the
Social History of Medicine, 129-138.
Boot, J. M. & Knapen, M. H. J. M. (2005). De Nederlandse Gezondheidszorg. [Dutch
Health Care]. Houten: Bohn Stafleu van Loghum.
Daft, R. L. (2003). Management (6 ed.). Mason: Thomson.
Department of Health. (2008). End of Life Care Strategy. Promoting High Quality Care
for All Adults at the End of Life. London: Department of Health. Donaldson, L. (2011). Presentation ‘Leadership in the NHS: Reflections of a Chief
Medical Officer’ During ‘Leadership in the NHS Lecture Series’ at the King's Fund (London, 4 April). Available at http://www.kingsfund.org.uk/events/past_events_catch_up/leadership_in_the_1.html

du Boulay, S. & Rankin, M. (2007). Cicely Saunders. The Founder of the Modern
Hospice Movement. London: SPCK.
Hacker, J. S. (2005). Bringing the Welfare State Back In: The Promise (and Perils) of the
New Social Welfare History. The Journal of Policy History, 17(1), 125-154.
Ham, C. (2004). Health Policy in Britain. The Politics and Organisation of the National
Health Service (5 ed.). Basingstoke: Palgrave Macmillan.
Hodgson, G. M. (2001). How Economics Forgot History. The Problem of Historical
Specificity in Social Science. London: Routledge.
Kingdon, J. W. (1984). Agendas, Alternatives, and Public Policies. Michigan: Harper
Collins Publishers.
Leadbeater, C. & Garber, J. (2010). Dying for Change. London: Demos.
Lewin, K. (1951). Field Theory in Social Science. New York: Harper & Brothers.
Mahoney, J. & Rueschemeyer, D. (Eds.). (2003). Comparative Historical Analysis in the
Social Sciences. Cambridge: Cambridge University Press.
May, E. R. (1973). “Lessons” of the Past: Use and Misuse of History in American
Foreign Policy. London: Oxford University Press.
McDonald, T. J. (1996). The Historic Turn in the Human Sciences Michigan: University
of Michigan Press
Monkkonen, E. H. (Ed.). (1994). Engaging the Past: The Uses of History across the
Social Sciences. Durham: Duke University Press.
Neustadt, R. E. & May, E. R. (1986). Thinking in Time - the Uses of History for Decision
Makers. New York: The Free Press.
Pierson, P. (2004). Politics in Time. History, Institutions, and Social Analysis. Princeton:
Princeton University Press. Pierson, P. (2005). The Study of Policy Development. The Journal of Policy History,
17(1), 34-51. Pollitt, C. (2008). Time, Policy, Management. Oxford: Oxford University Press.
Raadschelders, J. C. N. (1998). Handbook of Administrative History. New Brunswick:
Transaction Publishers.
Rivett, G. (1997). From Cradle to Grave: Fifty Years of the NHS. London: King's Fund.
Rose, R. (2005). Learning from Comparative Public Policy. A Practical Guide. London:
Routledge.
Rose, R. (Ed.). (1976). The Dynamics of Public Policy. A Comparative Analysis. London:
Sage Publications.
Rose, R. & Davies, P. (1994). Inheritance in Public Policy: Change without Choice in
Britain. New Haven: Yale University Press.
Rosenberg, C. E. (2006). Anticipated Consequences. Historians, History, and Health
Policy. In R. A. Stevens, C. E. Rosenberg & L. R. Burns (Eds.), History & Health
Policy in the United States. Putting the Past Back In (pp. 13-31). New Brunswick:
Rutgers University Press.
Rothman, D. J. & Wheeler, S. (Eds.). (1981). Social History and Social Policy. New
York: Academic Press.
Schäfer, W., Kroneman, M., Boerma, W., van den Berg, M., Westert, G., Devillé, W. &
van Ginneken, E. (2010). The Netherlands. Health System Review. Health systems in
Transition, 12(1), 1-229.

Schrijvers, A. J. P. & Droyan Kodner, L. (1997). Health and Health Care in the
Netherlands. A Critical Self-Assessment by Dutch Experts in the Medical and Health
Sciences. Utrecht De Tijdstroom.
Stevens, R. A., Rosenberg, C. E. & Burns, L. R. (Eds.). (2006). History & Health Policy
in the United States. Putting the Past Back In. New Brunswick: Rutgers University
Press.
The British Academy. (2008). Punching Our Weight: The Humanities and Social
Sciences in Public Policy Making - a British Academy Report. London: The British
Academy.
Tilly, C. (2006). Why and How History Matters. In R. E. Goodin & C. Tilly (Eds.), The
Oxford Handbook of Contextual Political Analysis (pp. 417-437). Oxford: Oxford
University Press.
van Reuler, A. A. H. E. (2008). On Specialist Cancer Hospitals, Cancer Policies and
Health Care Systems - a Comparative History of the Developments in England and
the Netherlands in the Period 1980-2007 (M.Sc. Thesis). University of Manchester,
Manchester.
van Reuler, A. A. H. E. (2010). EAPC Abstracts: The Position of Hospices within the
Health Care System. A Comparative Contemporary History of the Developments in
England and the Netherlands. Palliative Medicine, 24(4), S206-S207.
World Health Organisation. (2006). Palliative Care. Retrieved 20 April 2010, 2010,
from http://www.who.int/cancer/palliative/en/
Zelizer, J. E. (2000). Clio's Lost Tribe: Public Policy History since 1978. Journal of
Policy History, 12(3), 369-394.
Zelizer, J. E. (Ed.). (2005). New Directions in Policy History. Pennsylvania: The
Pennsylvania State University Press.


















