Histologic and electron microscopic periapical tissue examination
6
642 http://www.journal-imab-bg.org / J of IMAB. 2014, vol. 20, issue 5/ ABSTRACT Introduction: Key stages in the treatment of chronic apical periodontitis (CAP) are the assessment of the status of periapical zone, effective decontamination and subse- quent sealing of the root canal space. Purpose: The aim of this article is to analyze histo- logic and electron microscopic results from periapical tis- sue examination in teeth with chronic apical periodontitis. Material and Methods: The apices of 43 teeth (n = 43) were examined, allocated in two groups. The teeth were stored in saline solution (9% NaCl) supplemented with thy- mol, at 4°C. The apical portions of the roots were resected at 5 mm coronary. After resection, the apices were fixed to stands for SEM-examination. The periapical lesions (n = 24) were carefully removed with a curette from the root or the apical portion of the alveolar socket and were kept in 10% formalin solution to the preparation of histological samples. Results and Discussion: The results of the per- formed SEM-examinations of the apical zones showed that in 97.6% of the teeth with radiographically diagnosed CAP, there were external resorption around the apical foramen and associated apertures of varying degrees – from the ini- tial to the advanced stage of apical resorption. Despite the limited number of examined cases, the results obtained con- firm the histology and the inaccuracy of diagnostic assump- tions in some of the cases, resultant from the radiographic examination only Conclusion: Based on the analysis of results, the fol- lowing conclusions can be drawn: that external resorption around the apical foramen is established in 97.6% of cases in the teeth with radiographically diagnosed CAP. Key words: apical zone, chronic apical periodonti- tis, external apical resorption. INTRODUCTION Apical resorption is a biological phenomenon, char- acterized by processes of cement and/or dentine depletion, resulting from the physiological or pathological activity of resorptive cells, called dentoclasts (a subclass of the osteoclasts) [1, 2]. Studies have suggested that the perma- nent dentition is protected against physiological resorptive processes, but pathological resorption has been found in cases of trauma, orthodontic treatment, expansion of tumor or cystic formations, or has been largely the result of in- flammatory processes in the pulp tissue, etc. [3]. In inter- HISTOLOGIC AND ELECTRON MICROSCOPIC PERIAPICAL TISSUE EXAMINATION RESULTS IN TEETH WITH CHRONIC APICAL PERIODONTITIS Angela Gusiyska Department of Conservative Dentistry, Faculty of Dental Medicine, Medical University, Sofia, Bulgaria. Journal of IMAB - Annual Proceeding (Scientific Papers) 2014, vol. 20, issue 5 Journal of IMAB ISSN: 1312-773X http://www.journal-imab-bg.org nal root resorption, normal or necrotic pulp tissue, trans- formed into granulation tissue with giant multinuclear cells resorbing the dentinal wall in the absence of the odontob- last layer and predentine, has been histologically demon- strated [4, 5]. Stopping the internal resorptive processes is likely to occur through removal of the pulp and granula- tion tissue, as well as interruption of the blood supply to these tissues, necessary for the development of resorbing cells. Key stages in the treatment of chronic apical peri- odontitis (CAP) are the assessment of the status of periapi- cal zone, effective decontamination and subsequent sealing of the root canal space. MATERIAL AND METHODS Our objective was to clarify some aspects of the find- ings in the apical zone of teeth with chronic apical periodon- titis by applying ex vivo scanning electron microscopy (SEM) of the apical zone to detect the presence of resorption and by histological examination of the periapi- cal lesions. To clarify the available apical resorption, the peculiarities in the apical zone in teeth with CAP and the difficulties for the treatment, a comparative ex vivo SEM- examination was performed between the apical zones of teeth extracted for CAP and intact teeth with completed root development extracted on the basis of orthodontic consid- erations. For this purpose, the apices of 43 teeth (n = 43) were examined, allocated in two groups: group I (n = 24) – apices with radiographically diagnosed CAP and group II (n = 19) – apices with normal radiographic periapical structures, extracted on the basis of orthodontic considera- tions. The teeth were stored in saline solution (9% NaCl) supplemented with thymol, at 4°C. The apical portions of the roots were resected at 5 mm coronary. After resection, the apices were fixed to stands for SEM-examination. The prepared samples were vacuum coated with gold dust in an argon medium by using JEOL JFC- 1200 fine coater and examined with a scanning electron microscope (JEOL JSM- 5510 SEM) at the corresponding magnifications (x 50, x 200, x 1000, x 5000). The periapical lesions (n = 24) of group I were care- fully removed with a curette from the root or the apical por- tion of the alveolar socket and were kept in 10% formalin solution to the preparation of histological samples. The his- tological samples were prepared in 4-5 µ thickness and stained with hematoxylin-eosin (HE). http://dx.doi.org/10.5272/jimab.2014205.642
Transcript of Histologic and electron microscopic periapical tissue examination

642 http://www.journal-imab-bg.org / J of IMAB. 2014, vol. 20, issue 5/
ABSTRACTIntroduction: Key stages in the treatment of chronic
apical periodontitis (CAP) are the assessment of the statusof periapical zone, effective decontamination and subse-quent sealing of the root canal space.
Purpose: The aim of this article is to analyze histo-logic and electron microscopic results from periapical tis-sue examination in teeth with chronic apical periodontitis.
Material and Methods: The apices of 43 teeth (n =43) were examined, allocated in two groups. The teeth werestored in saline solution (9% NaCl) supplemented with thy-mol, at 4°C. The apical portions of the roots were resectedat 5 mm coronary. After resection, the apices were fixed tostands for SEM-examination. The periapical lesions (n = 24)were carefully removed with a curette from the root or theapical portion of the alveolar socket and were kept in 10%formalin solution to the preparation of histological samples.
Results and Discussion: The results of the per-formed SEM-examinations of the apical zones showed thatin 97.6% of the teeth with radiographically diagnosed CAP,there were external resorption around the apical foramenand associated apertures of varying degrees – from the ini-tial to the advanced stage of apical resorption. Despite thelimited number of examined cases, the results obtained con-firm the histology and the inaccuracy of diagnostic assump-tions in some of the cases, resultant from the radiographicexamination only
Conclusion: Based on the analysis of results, the fol-lowing conclusions can be drawn: that external resorptionaround the apical foramen is established in 97.6% of casesin the teeth with radiographically diagnosed CAP.
Key words: apical zone, chronic apical periodonti-tis, external apical resorption.
INTRODUCTIONApical resorption is a biological phenomenon, char-
acterized by processes of cement and/or dentine depletion,resulting from the physiological or pathological activity ofresorptive cells, called dentoclasts (a subclass of theosteoclasts) [1, 2]. Studies have suggested that the perma-nent dentition is protected against physiological resorptiveprocesses, but pathological resorption has been found incases of trauma, orthodontic treatment, expansion of tumoror cystic formations, or has been largely the result of in-flammatory processes in the pulp tissue, etc. [3]. In inter-
HISTOLOGIC AND ELECTRON MICROSCOPICPERIAPICAL TISSUE EXAMINATION RESULTS INTEETH WITH CHRONIC APICAL PERIODONTITIS
Angela GusiyskaDepartment of Conservative Dentistry, Faculty of Dental Medicine, MedicalUniversity, Sofia, Bulgaria.
Journal of IMAB - Annual Proceeding (Scientific Papers) 2014, vol. 20, issue 5Journal of IMABISSN: 1312-773Xhttp://www.journal-imab-bg.org
nal root resorption, normal or necrotic pulp tissue, trans-formed into granulation tissue with giant multinuclear cellsresorbing the dentinal wall in the absence of the odontob-last layer and predentine, has been histologically demon-strated [4, 5]. Stopping the internal resorptive processes islikely to occur through removal of the pulp and granula-tion tissue, as well as interruption of the blood supply tothese tissues, necessary for the development of resorbingcells.
Key stages in the treatment of chronic apical peri-odontitis (CAP) are the assessment of the status of periapi-cal zone, effective decontamination and subsequent sealingof the root canal space.
MATERIAL AND METHODSOur objective was to clarify some aspects of the find-
ings in the apical zone of teeth with chronic apical periodon-titis by applying ex vivo scanning electron microscopy(SEM) of the apical zone to detect the presence ofresorption and by histological examination of the periapi-cal lesions. To clarify the available apical resorption, thepeculiarities in the apical zone in teeth with CAP and thedifficulties for the treatment, a comparative ex vivo SEM-examination was performed between the apical zones ofteeth extracted for CAP and intact teeth with completed rootdevelopment extracted on the basis of orthodontic consid-erations. For this purpose, the apices of 43 teeth (n = 43)were examined, allocated in two groups: group I (n = 24)– apices with radiographically diagnosed CAP and groupII (n = 19) – apices with normal radiographic periapicalstructures, extracted on the basis of orthodontic considera-tions. The teeth were stored in saline solution (9% NaCl)supplemented with thymol, at 4°C. The apical portions ofthe roots were resected at 5 mm coronary. After resection,the apices were fixed to stands for SEM-examination. Theprepared samples were vacuum coated with gold dust in anargon medium by using JEOL JFC- 1200 fine coater andexamined with a scanning electron microscope (JEOL JSM-5510 SEM) at the corresponding magnifications (x 50, x200, x 1000, x 5000).
The periapical lesions (n = 24) of group I were care-fully removed with a curette from the root or the apical por-tion of the alveolar socket and were kept in 10% formalinsolution to the preparation of histological samples. The his-tological samples were prepared in 4-5 µ thickness andstained with hematoxylin-eosin (HE).
http://dx.doi.org/10.5272/jimab.2014205.642
/ J of IMAB. 2014, vol. 20, issue 5/ http://www.journal-imab-bg.org 643
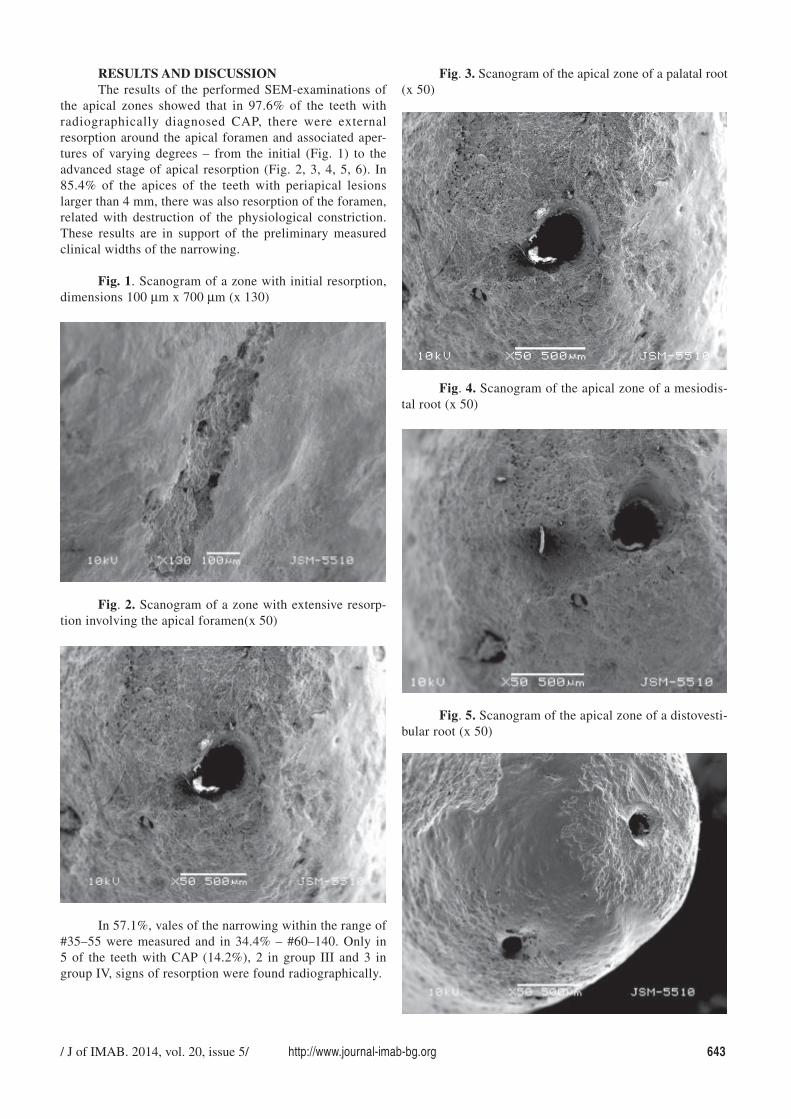
RESULTS AND DISCUSSIONThe results of the performed SEM-examinations of
the apical zones showed that in 97.6% of the teeth withradiographically diagnosed CAP, there were externalresorption around the apical foramen and associated aper-tures of varying degrees – from the initial (Fig. 1) to theadvanced stage of apical resorption (Fig. 2, 3, 4, 5, 6). In85.4% of the apices of the teeth with periapical lesionslarger than 4 mm, there was also resorption of the foramen,related with destruction of the physiological constriction.These results are in support of the preliminary measuredclinical widths of the narrowing.
Fig. 1. Scanogram of a zone with initial resorption,dimensions 100 µm x 700 µm (x 130)
Fig. 3. Scanogram of the apical zone of a palatal root(x 50)
Fig. 2. Scanogram of a zone with extensive resorp-tion involving the apical foramen(x 50)
In 57.1%, vales of the narrowing within the range of#35–55 were measured and in 34.4% – #60–140. Only in5 of the teeth with CAP (14.2%), 2 in group III and 3 ingroup IV, signs of resorption were found radiographically.
Fig. 4. Scanogram of the apical zone of a mesiodis-tal root (x 50)
Fig. 5. Scanogram of the apical zone of a distovesti-bular root (x 50)
644 http://www.journal-imab-bg.org / J of IMAB. 2014, vol. 20, issue 5/
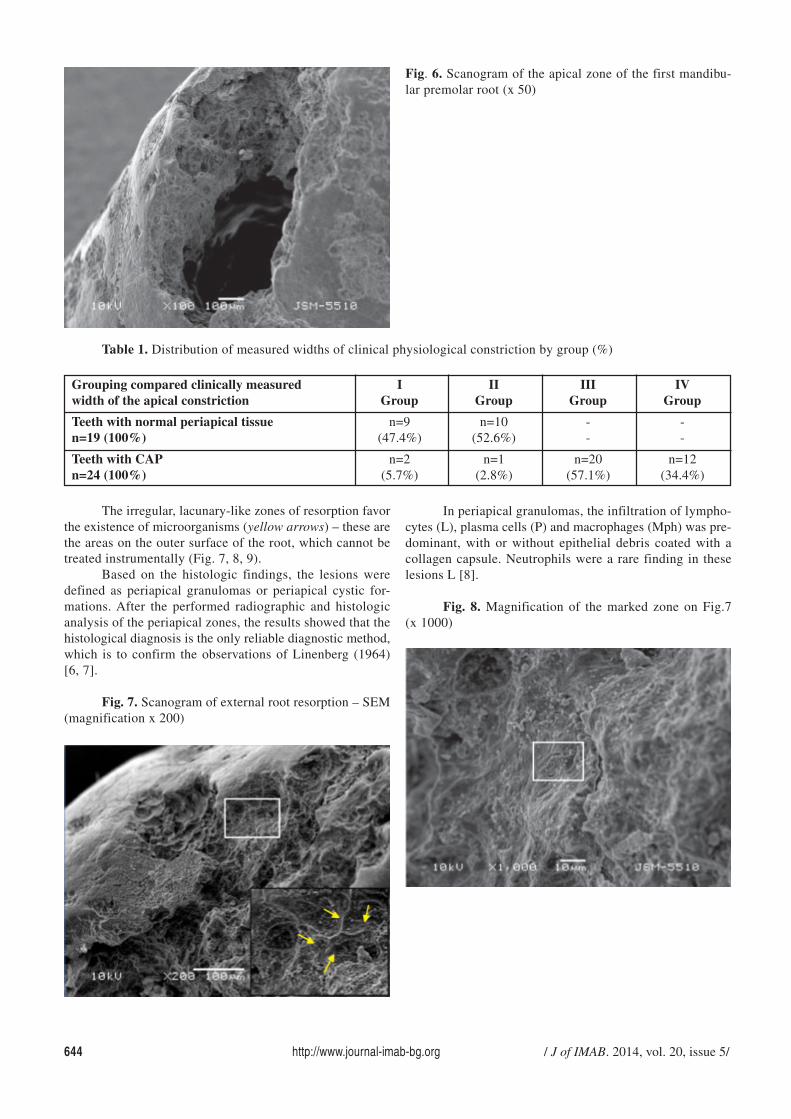
Fig. 6. Scanogram of the apical zone of the first mandibu-lar premolar root (x 50)
In periapical granulomas, the infiltration of lympho-cytes (L), plasma cells (P) and macrophages (Mph) was pre-dominant, with or without epithelial debris coated with acollagen capsule. Neutrophils were a rare finding in theselesions L [8].
Fig. 8. Magnification of the marked zone on Fig.7(x 1000)
Table 1. Distribution of measured widths of clinical physiological constriction by group (%)
The irregular, lacunary-like zones of resorption favorthe existence of microorganisms (yellow arrows) – these arethe areas on the outer surface of the root, which cannot betreated instrumentally (Fig. 7, 8, 9).
Based on the histologic findings, the lesions weredefined as periapical granulomas or periapical cystic for-mations. After the performed radiographic and histologicanalysis of the periapical zones, the results showed that thehistological diagnosis is the only reliable diagnostic method,which is to confirm the observations of Linenberg (1964)[6, 7].
Fig. 7. Scanogram of external root resorption – SEM(magnification x 200)
Grouping compared clinically measured I II III IVwidth of the apical constriction Group Group Group Group
Teeth with normal periapical tissue n=9 n=10 - -n=19 (100%) (47.4%) (52.6%) - -
Teeth with CAP n=2 n=1 n=20 n=12n=24 (100%) (5.7%) (2.8%) (57.1%) (34.4%)

/ J of IMAB. 2014, vol. 20, issue 5/ http://www.journal-imab-bg.org 645
Fig. 9. Magnification of the marked zone on Fig. 8(x 5000) (the arrows indicate E. faecalis)
Histological sections were analyzed under magnifi-cations x 4, x 10 and x 40 (Zeiss microscope, Germany).The results of the histological examination are presented inTable 2.
Table 2. Distribution of samples by periapical find-ing
Fig. 11. Histological sample of periapical granuloma-tous lesion (stained with HE)
Fig. 12. Clinical case 2 – tooth23, periapical lesion
Fig. 13. Histological sample of periapical cystic lesion(stained with HE)
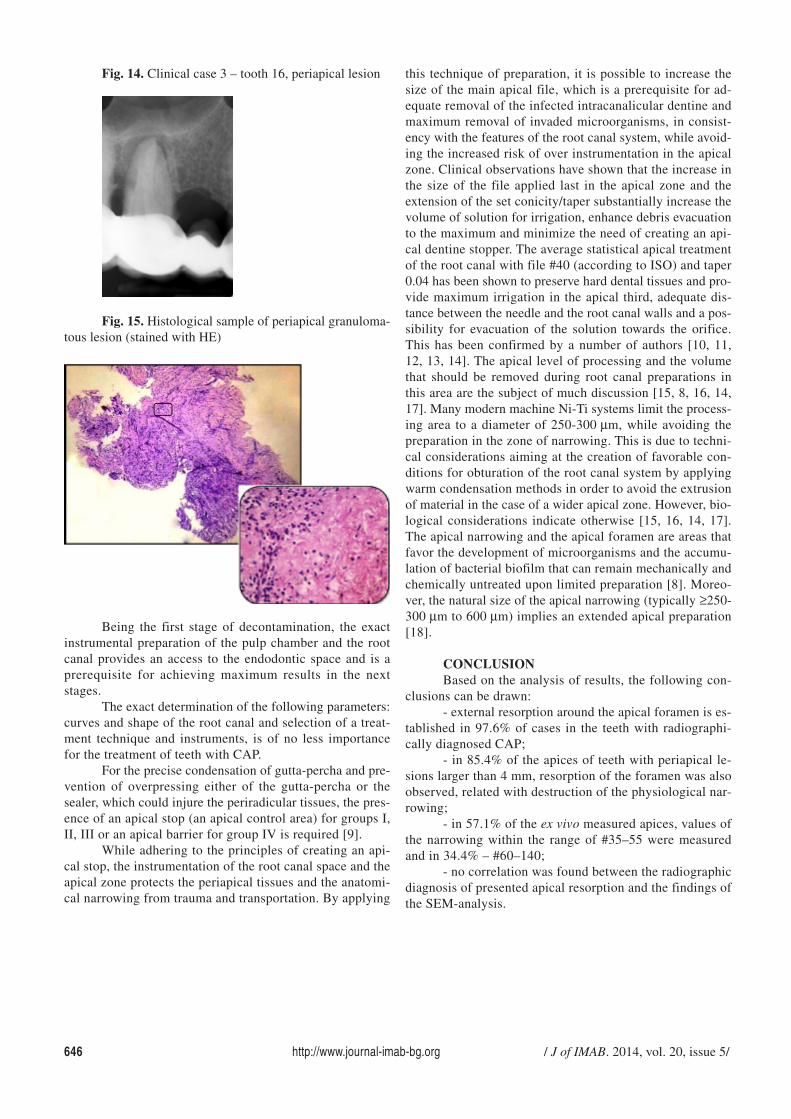
Despite the limited number of examined cases, the re-sults obtained confirm the histology and the inaccuracy ofdiagnostic assumptions in some of the cases, resultant fromthe radiographic examination only (cases 1 and 2). Both clini-cal cases were radiographically diagnosed as periapicalgranuloma. Because of the coronary loss of hard dental tis-sues, the teeth (n = 24) were planned for extraction. Afterthe microscopic analysis of the histological samples, the di-agnosis of clinical cases 1 and 3 was confirmed (Fig. 10,11, 14 and 15), while this of clinical case 2 was rejected,where the histology was indicative for periapical cystic le-sion (Fig. 12 and 13).
Fig. 10. Clinical case 1 – tooth 26 – lesion around MBroot
Teeth with CAP Histological Radiographicn=24 (42) samples examination
Periapical granuloma n= 33 n= 27
Periapical cyst n= 9 n= 15
646 http://www.journal-imab-bg.org / J of IMAB. 2014, vol. 20, issue 5/
Fig. 14. Clinical case 3 – tooth 16, periapical lesion
Fig. 15. Histological sample of periapical granuloma-tous lesion (stained with HE)
this technique of preparation, it is possible to increase thesize of the main apical file, which is a prerequisite for ad-equate removal of the infected intracanalicular dentine andmaximum removal of invaded microorganisms, in consist-ency with the features of the root canal system, while avoid-ing the increased risk of over instrumentation in the apicalzone. Clinical observations have shown that the increase inthe size of the file applied last in the apical zone and theextension of the set conicity/taper substantially increase thevolume of solution for irrigation, enhance debris evacuationto the maximum and minimize the need of creating an api-cal dentine stopper. The average statistical apical treatmentof the root canal with file #40 (according to ISO) and taper0.04 has been shown to preserve hard dental tissues and pro-vide maximum irrigation in the apical third, adequate dis-tance between the needle and the root canal walls and a pos-sibility for evacuation of the solution towards the orifice.This has been confirmed by a number of authors [10, 11,12, 13, 14]. The apical level of processing and the volumethat should be removed during root canal preparations inthis area are the subject of much discussion [15, 8, 16, 14,17]. Many modern machine Ni-Ti systems limit the process-ing area to a diameter of 250-300 µm, while avoiding thepreparation in the zone of narrowing. This is due to techni-cal considerations aiming at the creation of favorable con-ditions for obturation of the root canal system by applyingwarm condensation methods in order to avoid the extrusionof material in the case of a wider apical zone. However, bio-logical considerations indicate otherwise [15, 16, 14, 17].The apical narrowing and the apical foramen are areas thatfavor the development of microorganisms and the accumu-lation of bacterial biofilm that can remain mechanically andchemically untreated upon limited preparation [8]. Moreo-ver, the natural size of the apical narrowing (typically ≥250-300 µm to 600 µm) implies an extended apical preparation[18].
CONCLUSIONBased on the analysis of results, the following con-
clusions can be drawn:- external resorption around the apical foramen is es-
tablished in 97.6% of cases in the teeth with radiographi-cally diagnosed CAP;
- in 85.4% of the apices of teeth with periapical le-sions larger than 4 mm, resorption of the foramen was alsoobserved, related with destruction of the physiological nar-rowing;
- in 57.1% of the ex vivo measured apices, values ofthe narrowing within the range of #35–55 were measuredand in 34.4% – #60–140;
- no correlation was found between the radiographicdiagnosis of presented apical resorption and the findings ofthe SEM-analysis.
Being the first stage of decontamination, the exactinstrumental preparation of the pulp chamber and the rootcanal provides an access to the endodontic space and is aprerequisite for achieving maximum results in the nextstages.
The exact determination of the following parameters:curves and shape of the root canal and selection of a treat-ment technique and instruments, is of no less importancefor the treatment of teeth with CAP.
For the precise condensation of gutta-percha and pre-vention of overpressing either of the gutta-percha or thesealer, which could injure the periradicular tissues, the pres-ence of an apical stop (an apical control area) for groups I,II, III or an apical barrier for group IV is required [9].
While adhering to the principles of creating an api-cal stop, the instrumentation of the root canal space and theapical zone protects the periapical tissues and the anatomi-cal narrowing from trauma and transportation. By applying

/ J of IMAB. 2014, vol. 20, issue 5/ http://www.journal-imab-bg.org 647
1. Gulabivala K, Patel B, Evans G,Ng YL. Effects of mechanical andchemical procedures on root canal sur-faces. Endod Topics. 2005 Mar;10(1):103-122. [CrossRef]
2. Kabak Y, Abbott PV. Prevalenceof apical periodontitis and the qualityof endodontic treatment in an adultBelarusian population. Int Endod J.2005 Apr;38(4):238-45. [PubMed][CrossRef]
3. Lana MA, Ribeiro-Sobrinho AP,Stehling R, Garcia GD, Silva BK,Hamdan JS, et al. Microorganisms iso-lated from root canals presentingnecrotic pulp and their drug suscepti-bility in vitro. Oral MicrobiolImmunol. 2001 Apr;16(2):100-105.[PubMed] [CrossRef]
4. Pierce A, Berg JO, Lindskog S.Calcitonin as an alternative therapy inthe treatment for root resorption. JEndod. 1988 Sep;14(9):259-64.[CrossRef]
5. Katebzadeh N, Sigurdsson A,Trope M. Radiographic evaluation ofperiapical healing after obturation ofinfected root canals: an in vivo study.Int Endod J. 2000 Jan;33(1):60-66.[PubMed] [CrossRef]
6. Spatafore CM, Griffin JA Jr,Keyes GG, Wearden S, Skidmore AE.Periapical biopsy report: An analysisover a 10-year period. J Endod. 1990May;16(5):239-241. [PubMed]
7. Vianna ME, Horz HP, Gomes BP,Conrads G. In vivo evaluation of mi-crobial reduction after chemo-me-
REFERENCES:chanical preparation of human root ca-nals containing necrotic pulp tissue. IntEndod J. 2006 Jun;39(6):484-492.[PubMed] [CrossRef]
8. Nair PN, Sjögren U, Krey G,Kahnberg KE, Sundqvist G. Intraradi-cular bacteria and fungi in root filledasymptomatic human teeth with the-rapy resistant periapical lesions: a longterm light and electron microscope fol-low-up study. J Endod. 1990 Dec;16(12):580-588. [PubMed] [CrossRef]
9. Murugan R, Ramakrishna S. De-velopment of cell-responsive nano-phase hydroxyapatite for tissue engi-neering. Am J Biochem Biotech. 2007;3(3):118-124. [CrossRef]
10. Boutsioukis C, Verhaagen B,Versluis M, Kastrinakis E, Wesselink P,Van der Sluis LW. The effect of apicalpreparation size on irrigant flow in rootcanals evaluated using an unsteadyComputational Fluid Dynamics model.Int Endod J. 2010 Oct;43(10):874-81.[PubMed] [CrossRef]
11. Brunson M, Heilborn C,Johnson DJ, Cohenca N. Effect of api-cal preparation size and preparation ta-per on irrigant volume delivered by us-ing negative pressure irrigation system.J Endod. 2010 Apr;36(4):721-4.[PubMed] [CrossRef]
12. Dalton BC, Ørstavik D, PhillipsC, Pettiette M, Trope M. Bacterial re-duction with nickel-titanium rotary in-strumentation. J Endod. 1998 Nov;24(11):763-767. [PubMed] [CrossRef]
13. Ørstavik D, Kerekes K, EriksenHM. The periapical index: a scoringsystem for radiographic assessment ofapical periodontitis. Endod DentTraumatol. 1986 Feb;2(1):20-34.[PubMed] [CrossRef]
14. de Souza-Filho FJ, Soares AdeJ, Vianna ME, Zaia AA, Ferraz CC,Gomes BP. Antimicrobial effect andpH of chlorhexidine gel and calciumhydroxide alone and associated withother materials. Braz Dent J. 2008;19(1):28-33. [PubMed] [CrossRef]
15. Card SJ, Sigurdsson A, ØrstavikD, Trope M. The effectiveness of in-creased apical enlargement in reducingintracanal bacteria. J Endod. 2002Nov;28(11):779-783. [PubMed][CrossRef
16. Peters LB, Wesselink PR, vanWinkelhoff AJ. Combinations of bac-terial species in endodontic infections.Int Endod J. 2002 Aug;35(8):698-702.[PubMed] [CrossRef]
17. Vier F, Figueiredo J. Prevalenceof different periapical lesions associ-ated with human teeth and their corre-lation with the presence and extensionof apical external root resorption. IntEndod J. 2002 Aug;35(8):710-719.[PubMed] [CrossRef]
18. Marroquin BB, El-Syed MA,Willershausen-Zonnchen B. Morphol-ogy of the physiological foramen: I.Maxillary and mandibular molars. JEndod. 2004 May;30(5):321-8.[PubMed] [CrossRef]
Address for correspondence:Dr Angela Gusiyska, PhDDepartment of Conservative Dentistry, Faculty of Dental Medicine1, St. George Sofiiski Str., 1431 Sofia, BulgariaE-mail: [email protected]
Please cite this article as: Gusiyska A. Histologic and electron microscopic periapical tissue examination results inteeth with chronic apical periodontitis. J of IMAB. 2014 Oct-Dec;20(5):642-647.doi: http://dx.doi.org/10.5272/jimab.2014205.642
Received: 15/07/2014; Published online: 06/11/2014