
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, … · I have the following potential...
19
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan
Transcript of Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, … · I have the following potential...
Hiroshi Ando, MDKasukabe Chuo General Hospital
Saitama, Japan

I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest
Disclosure
Hiroshi Ando, MD
Kasukabe Chuo General Hospital
✓

Difficult to Avoid Restenosis
after Balloon Angioplasty
3M-Restenosis = 73%Iida O, Soga Y, et al. EJVES 2012
3M-Restenosis = 69%Schmidt A, et al. CCI 2010;76:1047–1054
J-BEAT Angio
Multicenter prospective registry
101 infrapopliteal lesions (63 CLI patients)
Courtesy of Dr. Soga
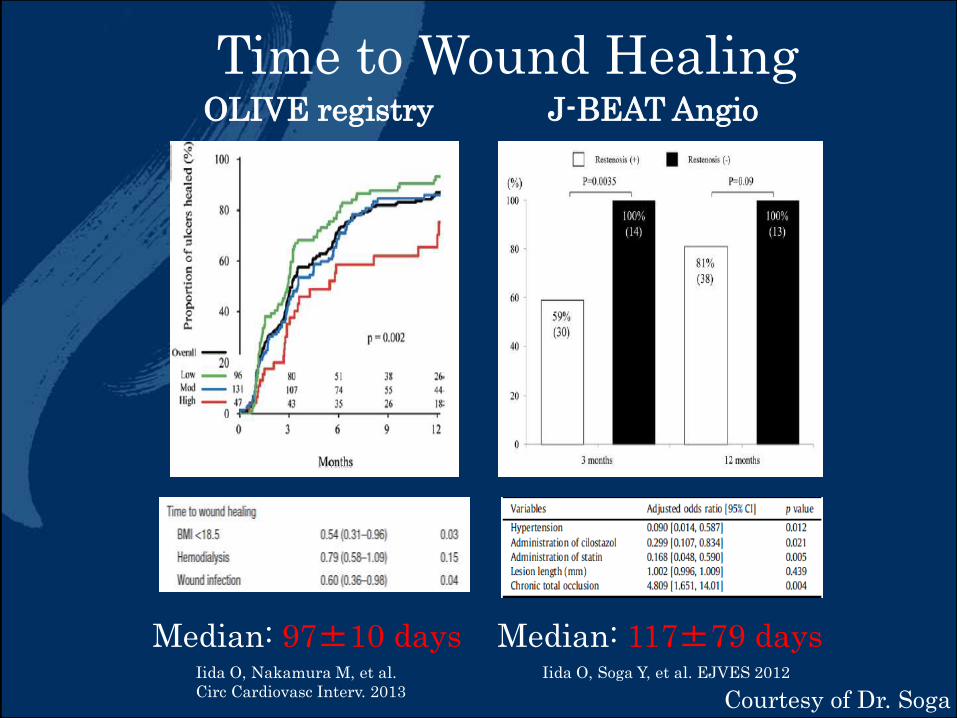
Time to Wound Healing
Courtesy of Dr. Soga
Median: 97±10 days
OLIVE registry J-BEAT Angio
Median: 117±79 daysIida O, Soga Y, et al. EJVES 2012Iida O, Nakamura M, et al.
Circ Cardiovasc Interv. 2013

Time to Wound Healing
N. Azuma et al. Eur J Vasc Endovasc Surg. 2012
Median
9M!!
To complete wound healing for dialysis pts,
we spend too much time!!
Courtesy of Dr. Soga

Time to Wound Healing is
longer than Time to Restenosis
Wound healing 3-4M > restenosis 3M
(dialysis 9M !)
Courtesy of Dr. Soga
Repeat balloon angioplasty is
often needed to achieve complete
wound healing.

6 and 12 month follow up data DES trials
P.P: primary patency
ACHILLES
SES/PTA
YUKON-BTK
SES/BMS
DESTINY
EES/BMS
DESTINY II
EES
PES BTK-70self-expanding
BVSeverolimus-eluting
Patients(n) 99 82 78 60 70 22
Rutherford(CLI)
3 to 5 2 to 5(51.2%)
4 to 5 4 to 5(96.7%)
4 to 5 3 to 6(60%)
LL(mm)MLL±SD(mm) 26.9±20.
931±9 15.9±910.
2
30-10047.4 19.7
5-5020.2
CTO(%) 81.3 15 53.3 14.3
P.P(%) 75 80.6 85.2 75.4 72.6 94.4
TLR(%) 10.0 9.2 8.7 15.1 20.9 5.6
Death(%) 10.1 22.4 18.1 10.7 10.6 4.6
Limb salvage(%) 86.2 97.4 94.8 96.6 100
DES > BMS > PTA
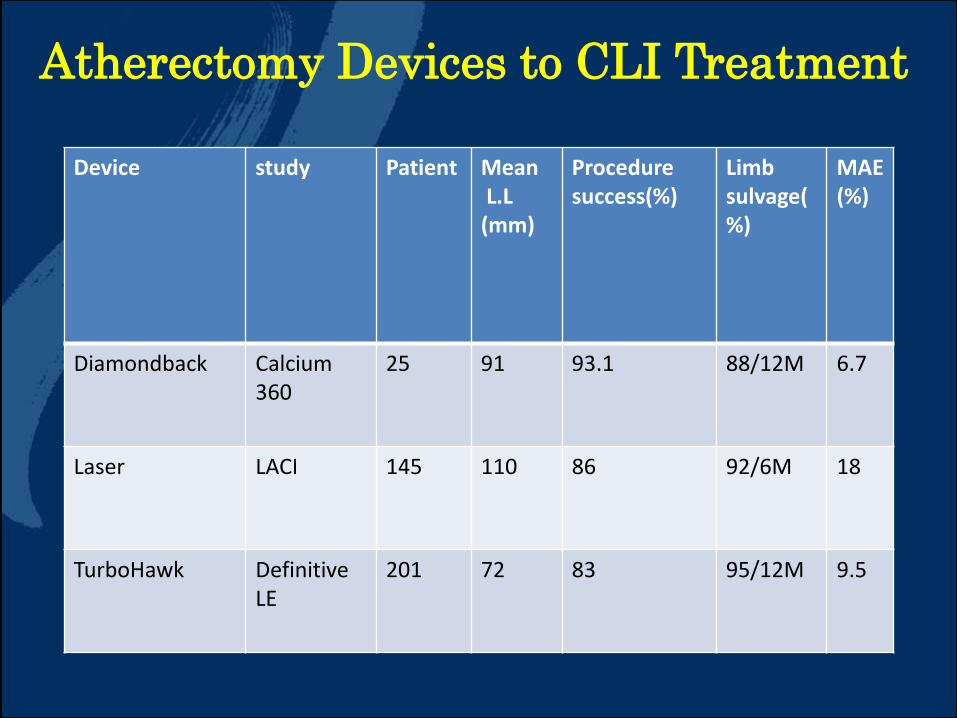
Atherectomy Devices to CLI Treatment
Device study Patient MeanL.L
(mm)
Procedure success(%)
Limb sulvage(%)
MAE(%)
Diamondback Calcium360
25 91 93.1 88/12M 6.7
Laser LACI 145 110 86 92/6M 18
TurboHawk DefinitiveLE
201 72 83 95/12M 9.5

Study Design
Study Design
Study Design
Study Design Prospective, Multicenter, Single Arm, Real-world Registry
Objective
To demonstrate safety and assess the clinical use and outcomes of the Lutonix DCB for treatment of stenosis or occlusion of native below-the-knee arteries in a heterogeneous patient population in real world clinical practice
Number of patients/sites
371 subjects enrolled from 26 international sites
Inclusion CriteriaRutherford Class: 3-5, ≥ 70% stenosis lesion, target vessel(s) reconstitute(s) at or above the ankle with inline flow to at least one patent (<50% residual stenosis) inframalleolar outflow vessel
Exclusion CriteriaNeurotrophic ulcer or heel pressure ulcer or ulcer potentially involving calcaneus (index limb)
Primary EndpointsSafety: Freedom from BTK MALE+POD at 30-daysEfficacy: Freedom from TLR at 6 months
Follow-up 1, 6, 12 and 24 Months
The Global Lutonix DCB BTK Registry
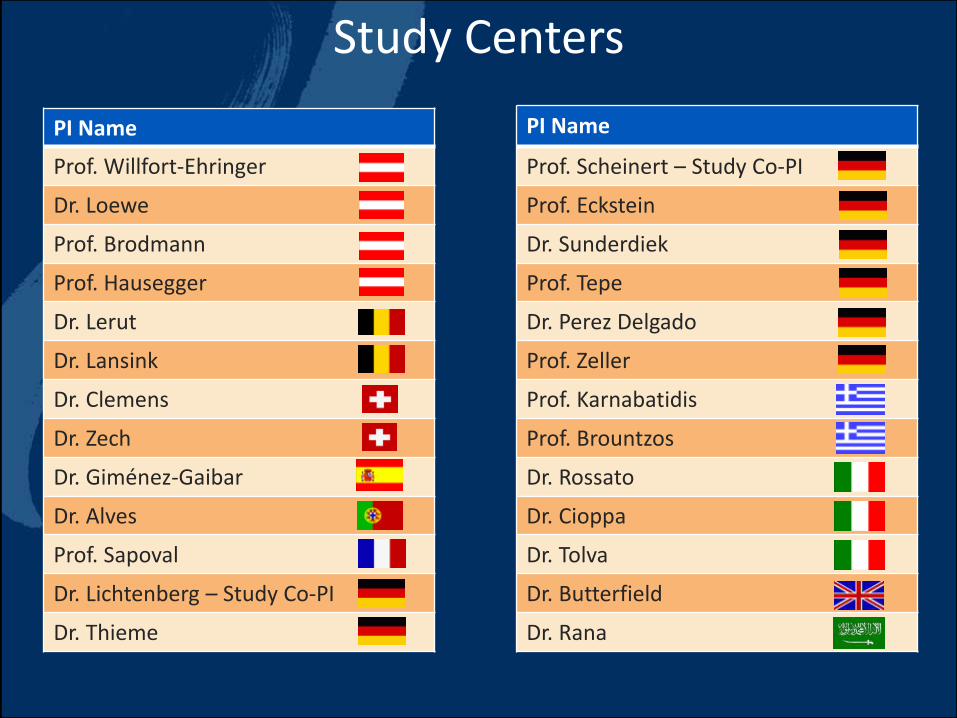
PI Name
Prof. Willfort-Ehringer
Dr. Loewe
Prof. Brodmann
Prof. Hausegger
Dr. Lerut
Dr. Lansink
Dr. Clemens
Dr. Zech
Dr. Giménez-Gaibar
Dr. Alves
Prof. Sapoval
Dr. Lichtenberg – Study Co-PI
Dr. Thieme
Study Centers
PI Name
Prof. Scheinert – Study Co-PI
Prof. Eckstein
Dr. Sunderdiek
Prof. Tepe
Dr. Perez Delgado
Prof. Zeller
Prof. Karnabatidis
Prof. Brountzos
Dr. Rossato
Dr. Cioppa
Dr. Tolva
Dr. Butterfield
Dr. Rana
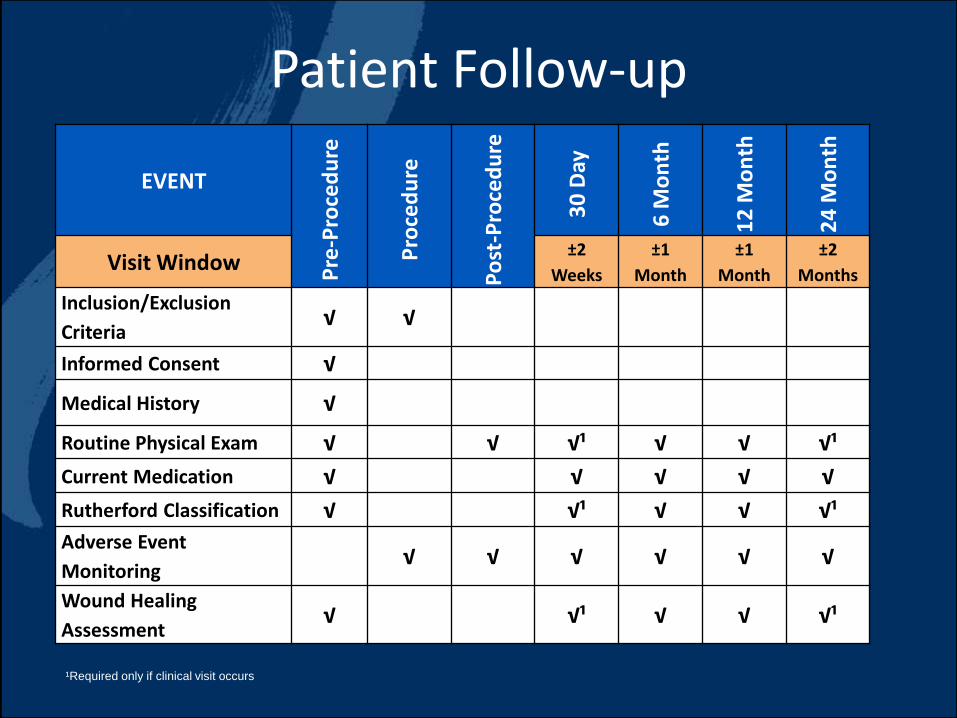
EVENT
Pre
-Pro
ced
ure
Pro
ced
ure
Po
st-P
roce
du
re
30
Day
6 M
on
th
12
Mo
nth
24
Mo
nth
Visit Window±2
Weeks
±1
Month
±1
Month
±2
Months
Inclusion/Exclusion
Criteria√ √
Informed Consent √
Medical History √
Routine Physical Exam √ √ √¹ √ √ √¹
Current Medication √ √ √ √ √
Rutherford Classification √ √¹ √ √ √¹
Adverse Event
Monitoring√ √ √ √ √ √
Wound Healing
Assessment√ √¹ √ √ √¹
Patient Follow-up
¹Required only if clinical visit occurs

DescriptionBTK Study Registry
(N=364)
Age (Years), Mean ± SD (n) 73.6 ± 9.5 (364)
Gender, % (n/N)
Female
Male
28.0% (102/364)
72.0% (262/364)
BMI ≥30 kg/m², % (n/N) 23.7% (85/358)
Hypertension, % (n/N) 86.8% (316/364)
Dyslipidemia, % (n/N) 62.4% (227/364)
Diabetes 64.0% (233/364)
Current/Previous Smoker, % (n/N) 50.5% (184/364)
Rutherford Category
3
4
5
23.7% (86/363)
10.5% (38/363)
65.8% (239/363)
Demographics / Baseline Characteristics
RCC 5
65.8%
(239/363)
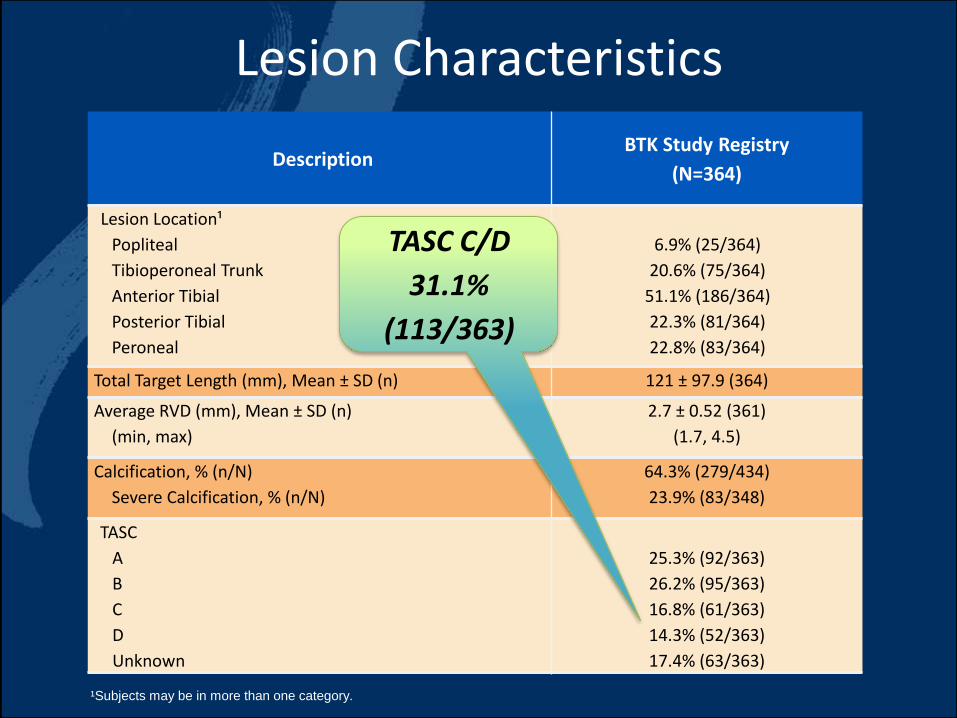
DescriptionBTK Study Registry
(N=364)
Lesion Location¹
Popliteal
Tibioperoneal Trunk
Anterior Tibial
Posterior Tibial
Peroneal
6.9% (25/364)
20.6% (75/364)
51.1% (186/364)
22.3% (81/364)
22.8% (83/364)
Total Target Length (mm), Mean ± SD (n) 121 ± 97.9 (364)
Average RVD (mm), Mean ± SD (n)
(min, max)
2.7 ± 0.52 (361)
(1.7, 4.5)
Calcification, % (n/N)
Severe Calcification, % (n/N)
64.3% (279/434)
23.9% (83/348)
TASC
A
B
C
D
Unknown
25.3% (92/363)
26.2% (95/363)
16.8% (61/363)
14.3% (52/363)
17.4% (63/363)
Lesion Characteristics
¹Subjects may be in more than one category.
TASC C/D
31.1%
(113/363)
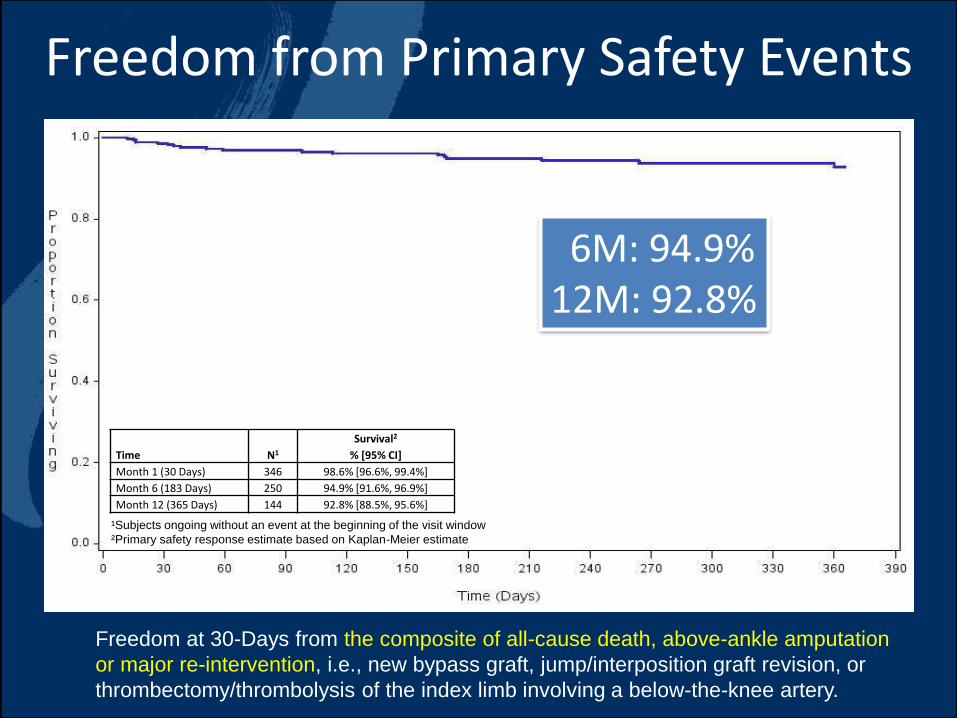
Freedom from Primary Safety Events
Freedom at 30-Days from the composite of all-cause death, above-ankle amputation
or major re-intervention, i.e., new bypass graft, jump/interposition graft revision, or
thrombectomy/thrombolysis of the index limb involving a below-the-knee artery.
Time N1
Survival2
% [95% CI]
Month 1 (30 Days) 346 98.6% [96.6%, 99.4%]
Month 6 (183 Days) 250 94.9% [91.6%, 96.9%]
Month 12 (365 Days) 144 92.8% [88.5%, 95.6%]
¹Subjects ongoing without an event at the beginning of the visit window
²Primary safety response estimate based on Kaplan-Meier estimate
6M: 94.9%12M: 92.8%
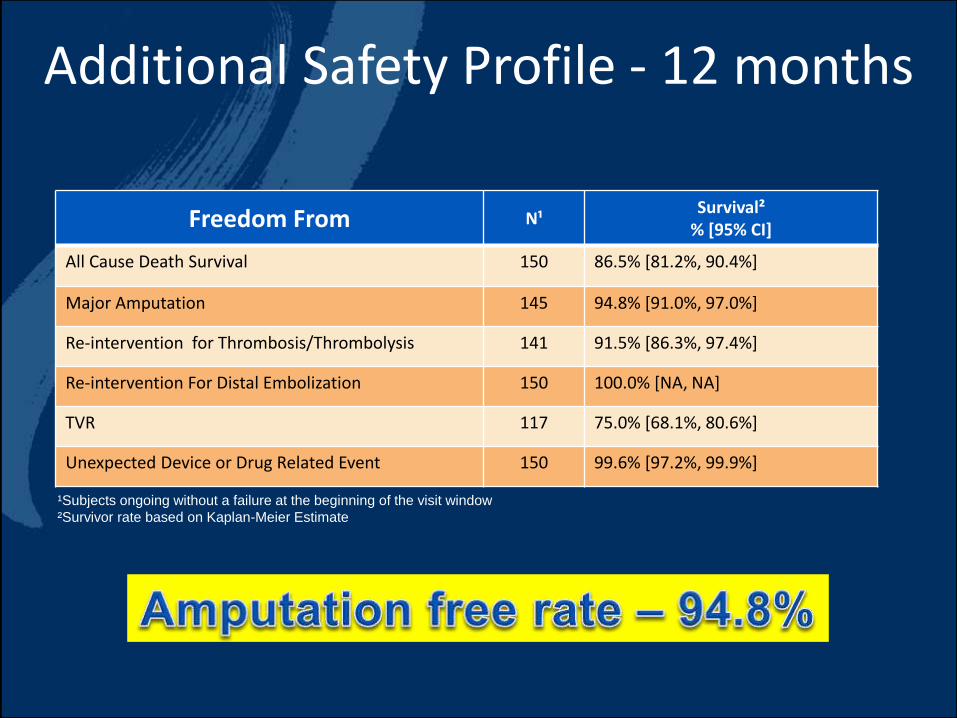
Freedom From N¹Survival²
% [95% CI]
All Cause Death Survival 150 86.5% [81.2%, 90.4%]
Major Amputation 145 94.8% [91.0%, 97.0%]
Re-intervention for Thrombosis/Thrombolysis 141 91.5% [86.3%, 97.4%]
Re-intervention For Distal Embolization 150 100.0% [NA, NA]
TVR 117 75.0% [68.1%, 80.6%]
Unexpected Device or Drug Related Event 150 99.6% [97.2%, 99.9%]
Additional Safety Profile - 12 months
¹Subjects ongoing without a failure at the beginning of the visit window
²Survivor rate based on Kaplan-Meier Estimate
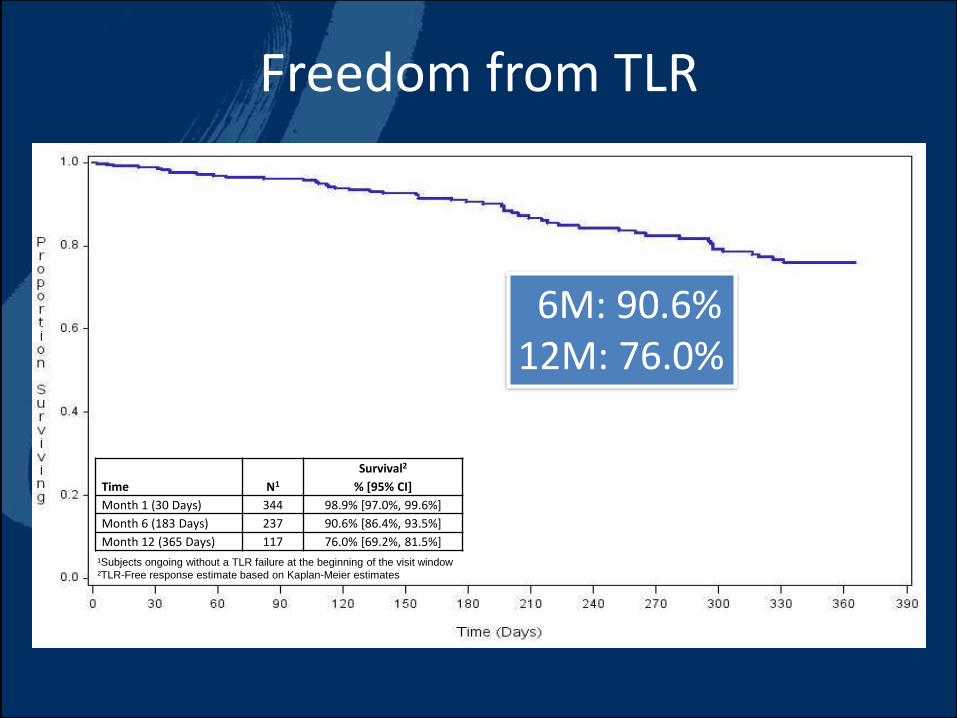
Freedom from TLR
¹Subjects ongoing without a TLR failure at the beginning of the visit window
²TLR-Free response estimate based on Kaplan-Meier estimates
Time N1
Survival2
% [95% CI]
Month 1 (30 Days) 344 98.9% [97.0%, 99.6%]
Month 6 (183 Days) 237 90.6% [86.4%, 93.5%]
Month 12 (365 Days) 117 76.0% [69.2%, 81.5%]
6M: 90.6%12M: 76.0%
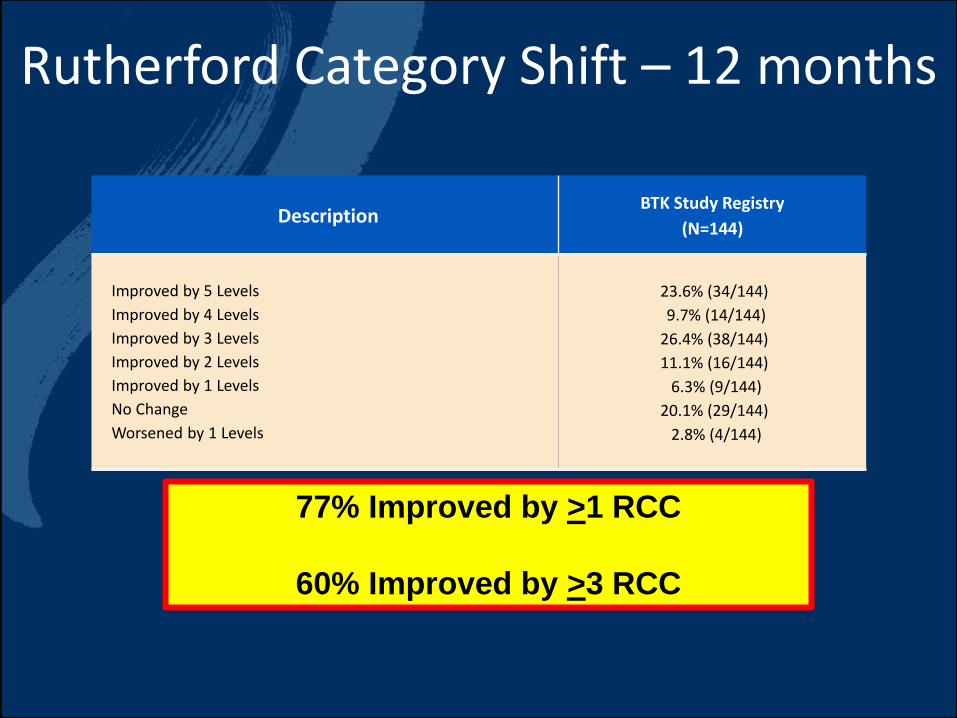
Rutherford Category Shift – 12 months
DescriptionBTK Study Registry
(N=144)
Improved by 5 Levels
Improved by 4 Levels
Improved by 3 Levels
Improved by 2 Levels
Improved by 1 Levels
No Change
Worsened by 1 Levels
23.6% (34/144)
9.7% (14/144)
26.4% (38/144)
11.1% (16/144)
6.3% (9/144)
20.1% (29/144)
2.8% (4/144)
77% Improved by >1 RCC
60% Improved by >3 RCC

• Only BTK Multi-Center On-going Registry Study
• Freedom from TLR 76.0% at 12 months
• Low Amputation Rate – 5.2% at 12 months
• ~60% Improvement by >3 Rutherford Classifications at 12 months
• ZERO Re-interventions for Distal Embolization at 12 months
• Promising Treatment Effect in Below-the–Knee Arteries
• Safety Outcomes Consistent with the Strong Safety Profile of the
Lutonix DCB in PAD
12 Month Conclusions

Hiroshi Ando, MDKasukabe Chuo General Hospital
Saitama, Japan


















