Highlights of the annual meeting of the European Association of Nuclear Medicine, Lausanne 1993
11
European Journal of Nuclear Medicine Review article Highlights of the Annual Meeting of The European Association of Nuclear Medicine, Lausanne 1993 Keith Britton St. Bartholomew's Hospital and Medical College, West Smithfield, London EC1A 7BE, UK Introduction On arrival, the sun was shining, the white mountain visi- ble in the distance and the lake calm. A great conference progressed while the rain fell, confining the delegates to matters of nuclear medicine. The highlights were Profes- sor Bernard Delaloye and Dr. Mrs. Angelika Bischof- Delaloye, whose hospitality, discrete organisation and attention to detail made the conference so successful. On departure, the sun was shining, the white mountain visi- ble in the distance and the lake a little less calm. Perhaps one can judge the scientific contribution of a Congress under three headings: quantity, content and quality. The numbers were impressive: 312 oral presen- tations, 12 work in progress, 440 poster presentations, 27 technologist papers, 22 invited papers and 7 in the COST B2 symposium. As for content, the question to be answered is "Where is Nuclear Medicine going in the 1990s?" My answer is as follows: from function meas- urement to tissue characterisation and from sensitivity to specificity. I asked of this Congress to what extent were these goals supported and to what extent were there dis- tractions. The content ranged from excellent to average. The latter included "Let's try it out in ...", 'it' being indi- um-111 pentetreotide; "I have done five patients with..." linked to the me too, me too papers, and the pursuit of 'non-specificity'. I labelled the distractions: the 'stamp collectors' - the pretty pictures for 1993 -, the 'sweet talkers' - glucose and PET -, and the 'health care pur- chasers', of which the last are the most damaging. High- quality medicine has become too expensive for the health care purchaser and European nuclear medicine is primarily a high-quality service for the practice of high- quality medicine. As to scientific quality, I used three criteria: the iden- tification of an important clinical problem and its nucle- ar medicine solution, the development of objective measurements and the pursuit of specificity. If nuclear medicine is to progress it must find disease that is not clinically or radiologically evident, or it must demon- strate as specifically as possible the nature of a clinical or radiological abnormality. This tissue characterisation Correspondence to: K.E. Britton is the future. How did the scientific presentations live up to these ideals? Oncology Oncological papers provided the highest percentage con- tribution and they demonstrated a spectrum of tissue characterisation from the non-specific gallium-67 and fluorine-18 fluorodeoxyglucose (18F-FDG) to the highly specific use of certain radiolabelled monoclonal antibod- ies and receptor binding agents (Table 1). On what grounds is 18F-FDG uptake representative of tumour metabolism? On the answer to this question may rest the PET industry. From the days of Warburg [1] in- creased anaerobic glycolysis has been associated with tumour growth. But does this alteration of metabolism correlate with increased uptake or is there another expla- nation? Haberkorn (*5) and Kornrumpf (*3) start to pro- vide an answer. The uptake of ~SF-FDG depends on the activity of the glucose 1 transporter gene and the glucose transporter protein. Does this relate to tumour metabo- lism? The answer is rather negative. Kornrumpf et al. (*3) showed that increased 18F-FDG uptake is linked to the activation of this gene in pancreatic cancer, but that increase in glucose transport is independent of growth rate. They quoted Flier et al. [2], who, using the ras on- cogene, showed that increase in the glucose transporter gene is transformation specific. This means that it is likely to be a marker of malignancy, and it is dependent on relocation of the glucose transport protein in the cell membrane. Haberkorn (*5) also showed that 18F-FDG uptake is related not to differences in proliferation but to differences in transcription of the glucose carrier. These data make it unlikely that changes in ~SF-FDG uptake are going to be related to changes in growth rate or for it to be a reliable marker for the effects of chemotherapy. These matters have also been reviewed by Minn and Paul [31. This Congress abounded with papers on ~SF-FDG in tumours (*3, *4, *37, *38, *39, *40, *42, "133, *633, *634, *635, *636, *637, *638), including infec- tions (*4) and even fibromyalgia (*603) - sweet talk. Hence my observation that, like 67Ga, 18F-FDG has sen- sitivity but poor specificity. JSF-FDG is the 67Ga of PET. Eur J Nucl Med (1994) 21:159-169 Vol. 21, No. 2, February 1994 - © Springer-Verlag 1994
-
Upload
keith-britton -
Category
Documents
-
view
212 -
download
0
Transcript of Highlights of the annual meeting of the European Association of Nuclear Medicine, Lausanne 1993

European Journal of
Nuclear Medicine Review article
Highlights of the Annual Meeting of The European Association of Nuclear Medicine, Lausanne 1993 Keith Britton
St. Bartholomew's Hospital and Medical College, West Smithfield, London EC1A 7BE, UK
Introduction
On arrival, the sun was shining, the white mountain visi- ble in the distance and the lake calm. A great conference progressed while the rain fell, confining the delegates to matters of nuclear medicine. The highlights were Profes- sor Bernard Delaloye and Dr. Mrs. Angelika Bischof- Delaloye, whose hospitality, discrete organisation and attention to detail made the conference so successful. On departure, the sun was shining, the white mountain visi- ble in the distance and the lake a little less calm.
Perhaps one can judge the scientific contribution of a Congress under three headings: quantity, content and quality. The numbers were impressive: 312 oral presen- tations, 12 work in progress, 440 poster presentations, 27 technologist papers, 22 invited papers and 7 in the COST B2 symposium. As for content, the question to be answered is "Where is Nuclear Medicine going in the 1990s?" My answer is as follows: from function meas- urement to tissue characterisation and from sensitivity to specificity. I asked of this Congress to what extent were these goals supported and to what extent were there dis- tractions. The content ranged from excellent to average. The latter included "Let's try it out in ...", 'it' being indi- um-111 pentetreotide; "I have done five patients with..." linked to the me too, me too papers, and the pursuit of 'non-specificity'. I labelled the distractions: the 'stamp collectors' - the pretty pictures for 1993 -, the 'sweet talkers' - glucose and PET -, and the 'health care pur- chasers', of which the last are the most damaging. High- quality medicine has become too expensive for the health care purchaser and European nuclear medicine is primarily a high-quality service for the practice of high- quality medicine.
As to scientific quality, I used three criteria: the iden- tification of an important clinical problem and its nucle- ar medicine solution, the development of objective measurements and the pursuit of specificity. If nuclear medicine is to progress it must find disease that is not clinically or radiologically evident, or it must demon- strate as specifically as possible the nature of a clinical or radiological abnormality. This tissue characterisation
Correspondence to: K.E. Britton
is the future. How did the scientific presentations live up to these ideals?
Oncology
Oncological papers provided the highest percentage con- tribution and they demonstrated a spectrum of tissue characterisation from the non-specific gallium-67 and fluorine-18 fluorodeoxyglucose (18F-FDG) to the highly specific use of certain radiolabelled monoclonal antibod- ies and receptor binding agents (Table 1).
On what grounds is 18F-FDG uptake representative of tumour metabolism? On the answer to this question may rest the PET industry. From the days of Warburg [1] in- creased anaerobic glycolysis has been associated with tumour growth. But does this alteration of metabolism correlate with increased uptake or is there another expla- nation? Haberkorn (*5) and Kornrumpf (*3) start to pro- vide an answer. The uptake of ~SF-FDG depends on the activity of the glucose 1 transporter gene and the glucose transporter protein. Does this relate to tumour metabo- lism? The answer is rather negative. Kornrumpf et al. (*3) showed that increased 18F-FDG uptake is linked to the activation of this gene in pancreatic cancer, but that increase in glucose transport is independent of growth rate. They quoted Flier et al. [2], who, using the ras on- cogene, showed that increase in the glucose transporter gene is transformation specific. This means that it is likely to be a marker of malignancy, and it is dependent on relocation of the glucose transport protein in the cell membrane. Haberkorn (*5) also showed that 18F-FDG uptake is related not to differences in proliferation but to differences in transcription of the glucose carrier. These data make it unlikely that changes in ~SF-FDG uptake are going to be related to changes in growth rate or for it to be a reliable marker for the effects of chemotherapy. These matters have also been reviewed by Minn and Paul [31.
This Congress abounded with papers on ~SF-FDG in tumours (*3, *4, *37, *38, *39, *40, *42, "133, *633, *634, *635, *636, *637, *638), including infec- tions (*4) and even fibromyalgia (*603) - sweet talk. Hence my observation that, like 67Ga, 18F-FDG has sen- sitivity but poor specificity. JSF-FDG is the 67Ga of PET.
Eur J Nucl Med (1994) 21:159-169 Vol. 21, No. 2, February 1994 - © Springer-Verlag 1994

160
Table 1. Tissue characterisation in malignant disease Non- More Class Type
specific specific specific specific
Tumour or inflammation Tumour not Several tumours Few tumours infection
67Ga 2°IT1 Anti-tEA Anti-iymphoma ~SF-FDG 99mTc-MIBI A n t i - T A G 7 2 Anti-oestrogen 99mTc-glutathione 123I-/111 In I * MIB G Head/Neck
-octreotide C 174 123I-VIP Melanoma
123I_IBZM 225-28S Neuroblstoma chCE7
Fig. 1A, B. Pancreatic cancer. A Superimposition of ~SF-FDG up- take on Xray CT scan shows high uptake in the carcinoma in the head of the pancreas (Bares et al. *38). B Uptake of I*F-FDG in a pancreatic carcinoma. The nature and site of the lesion are less evident in the absence of the CT data (Grimmel et al. *37)
However, the sensitivity of 18F-FDG uptake has its uses provided that the competing diagnosis is not another cause of 18F-FDG uptake, such as infection. Thus 18F- FDG is a poor discriminator for lymph node involve- ment in head and neck tumours, where infective causes are common [4], but appears to be successful in combi- nation with radiology, although numbers are small, in
the staging of pancreatic cancer (*37, *38, *634) (Fig. 1) and urological cancers (*42, *638).
Many questions remain. How does one cope with tu- mour heterogeneity in measuring uptake? How does one choose and reproduce the region of interest? Do treat- ment changes in normal tissues affect tissue uptake ra- tios? Which lumped constant should be used and will it be the same before and after therapy? At what time in- terval after treatment should PET measurements be ma- de? What criteria are to be used to predict response to treatment successfully? Is tumour biopsy a valid indica- tor? :~
67Ga is the classical agent with overlap of uptake be- tween tumours and inflammation (*74, *77, "107, *480, *494, *495, *496, *504, *506, *649). The new techneti- um-99m glutathione is in this group ( '182, *573, '717). Therefore radiopharmaceuticals have been sought that bind to tumours but not to inflammatory processes (Ta- ble 1). 99mTc-(V)DMSA is one of these (*334, "641). Each of these agents binds to some tumours better than others because their mechanisms of uptake differ: active transport of thallium-201 (*1, *74, *77, *78, *293, *574, *627, *628, *642, *646, *657), cytosolic binding of 99mTc-methoxyisobutylisonitrile (MIBI) (* 107, * 116, "117, "136, *293, *294, *453, *572, *643, *644) and somatostatin receptor binding of mIn-pentetreotide (*97, *98, *99, *100, "106, *110, *111, "112, "113, "115, "157, *259, *260, "261, *262, *263, *264, *459, *477, *480, *574, "616, "618, "619, *620, "621, "715). Unfortunately from the diagnostic viewpoint only some examples of a particular tumour type bind these agents.
There are particular successes. These include 2°1TI in brain tumours ( '1, *574, *627, *628, *642), particularly in giving evidence of regrowth after therapy. 99mTc-MIBI may well become the standard agent for primary breast cancer diagnosis in association with mammography [5] (*643, *644) (Fig. 2). It appears able to demonstrate the presence and absence of tumour in those patients in whom mammography is difficult to interpret [6] as well as primary tumours generally. It appears to be better than estrogen receptors (*75), octreotide (*620) or 99mTc-ga- lactosyl neoglycoalbumin ('615). This is also an area
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

161
Fig. 2A-C. Breast cancer (Kao et al. *643). 99~Tc-MIBI scintigraphy. A Ante- rior view shows uptake in the left breast (arrowheaad), superior and lateral to the cardiac uptake. Thyroid, salivary and liver uptake is noted. B left oblique view: breast and left axillary nodes show uptake (arrowhead). C Left lateral, as B
Fig. 3. Bronchogenic cancer (Kirsch et al. *264) Imaging with ~In-pentreotide. Left: whole-body anterior view; right: posterior view. Focally increased uptake superior to the liver is evident in the small cell lung cancer. Liver, spleen, gut and urinary activity is evident
where radioimmunoscintigraphy (RIS) has not yet suc- ceeded. 99mTc-MIBI, however, is less reliable for axillary node evaluation, where RIS has more potential ( '150, *604). 99mTc-MIBI is the radiopharmaceutical of choice for imaging parathyroid adenoma (*456). The hope that a 3-h 99mTc-MIBI image would avoid the need for a thy- roid subtraction technique has not been confirmed (*457).
A particularly selective and beneficial form of tissue characterisation is that of specific receptor binding by a well-designed radiopharmaceutical. The somatostatin analogues iodine- 123 tyr-octreotide and ln In-pentetreot- ide are such agents. Yet their use highlights the conflict between the demand for a diagnostic catch-all and the demonstration of a specific aspect of tissue physiology with therapeutic potential. Somatostatin receptors do not occur on all tumours or, indeed, all examples of one tu- mour type. This in borne out by the large number of 'me too' papers, where almost every type of tumour-bearing
patient has been subjected to radiolabelled octreotide studies: bronchogenic cancer (*263, *264) (Fig. 3), lym- phoma ( '106, "261), breast tumours (*620), brain tu- mours ( '115, *260, *458, *574, "621), pancreatic tu- mours ( '715), and carcinoid (*97, *110, '113, *477), with diagnostic percentages as low as 50%. These 'stamp collections' are of interest but do not compare with the reviews by Krenning et al. [7] and Bihl and D6rr [8] and miss the point. The advantages of these re- ceptor binding agents are as follows: Firstly, they are of value in the localisation of the difficult tumour or its re- currence - the gastrinoma (*111, *477) or the medullary carcinoma of the thyroid (*100, '616, "618) even with the help of a peroperative probe (*295) - where a nega- tive is taken as a disadvantage and ignored but a positive is of real benefit to patient management. Secondly, and most importantly, scan positive predicts a therapeutic re- sponse to octreotide and scan negative, no response to this expensive drug. This is seen particularly in pituitary
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994
162
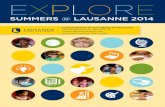
Fig. 4. Colorectal cancer (Douma et al. * 146). Radioimmunoscin- tigraphy with rain B72.3 (CYT-103). Anterior view of the abdo- men, showing an abdominal recurrence, not detected by other means but confirmed by surgery. The high liver uptake due to rain is also evident
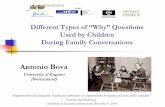
Fig. 5. Gastric cancer (Virgolini et al. * 114). Imaging with 123I-VIP. Anterior view of the chest showing extensive normal pul- monary uptake and a focal area of increased uptake in a Virchow node in the left supraclavicular region due to a metastasis. Note the absence of liver uptake
tumours, as Platz (*458) and others [9] have shown, and in some of the gastroendocrine tumours such as insulino- ma [10]. Thirdly, tissue receptor characterisation may be a prognostic indicator, as for oestrogen (*75) or epider- mal growth factor (*604) receptors in the breast and as shown by D6rr in neuroblastoma ( '157). Somatostatin receptor-positive children did better.
What is needed is a nice 99mTc somatostatin analogue. 99mTc-sandostatin was introduced by Martin-Comin (*262), as was another analogue, RC-160, but labelled with 123I or lllIn ( '109). The answer was given by Ma- ecke et al., who introduced a stable 99mTc-labelled octre- otide in the work in progress session. My concern for ra- diotherapeutically labelled octreotide, ytterbium-169, yt- trium-90 and samarium-153 (*247) is that the dose to the pituitary may be unacceptable.
Tumour-binding agents with a more selective range (Table 1) include tumour class-related monoclonal anti- bodies such as anti-CEA, which binds with virtually all tumours in its class, and anti-TAG 72, which binds with only about 80% of the tumours in its class. Ant i -CEA is
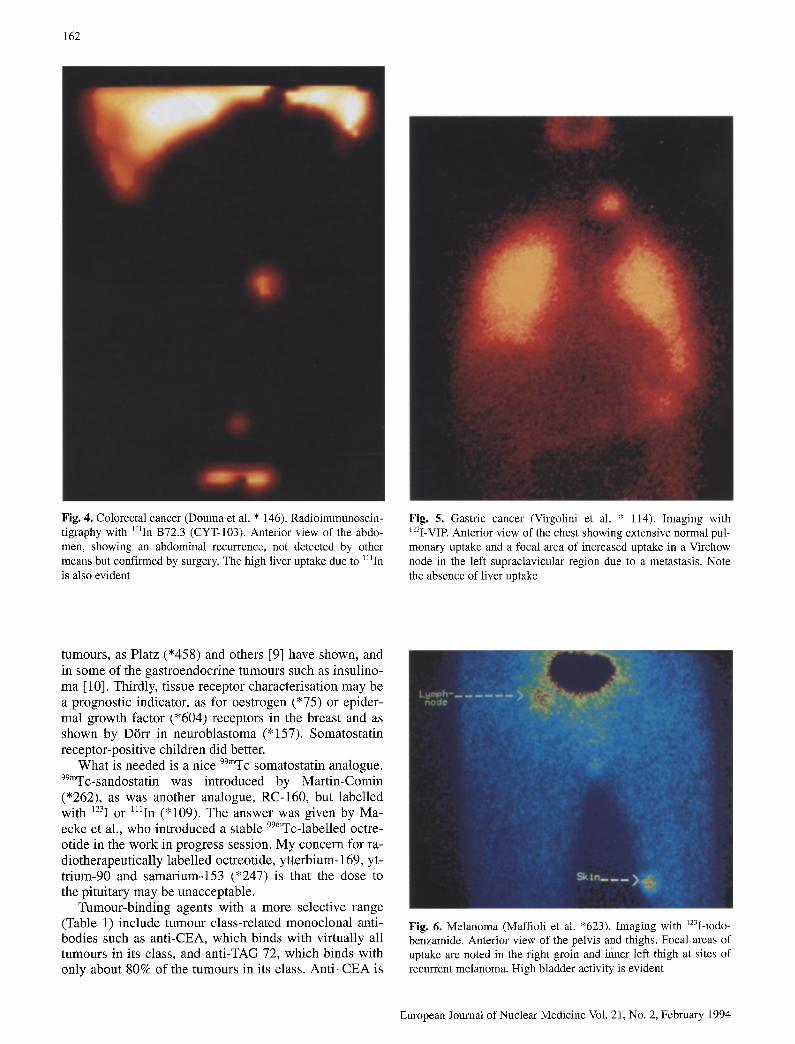
Fig. 6. Melanoma (Maffioli et al. *623). Imaging with ~23I-iodo- benzamide. Anterior view of the pelvis and thighs. Focal areas of uptake are noted in the right groin and inner left thigh at sites of recurrent melanoma. High bladder activity is evident
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

163
Fig. 7. Recurrent glioma (Langen et al. *2). Top row shows ~C-methionine uptake in tumour by PET. Bottom row shows ~23I-~x-methyl tyrosine uptake in the same tumour by SPET
Fig. 8. Epileptic focus (Todd-Pokropek and Oghabian *288). The significant abnormality on a 99mTc-HMPAO SPET study is super- imposed in orange on the equivalent MRI section of the brain
99mTc labelled (*609) or ra in labelled as with C46 stud- ied previously [11] and reintroduced as CY T 352 (*224). Ant i -TAG 72 (B72.3) is ~lIn labelled for colorectal can- cer ( ' 146 , *225, *608, "610). While the 99mTC label is
Fig. 9. Gastric motility (Urbain et al. * 463) is displayed as a colour spectrum
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

164
Fig. 11. T-cell activation, early diabetes (Signore et al. * 63). 123I-interleukin 2 imaging, posterior view at 1 h. The outline of the pancreas is from an X-ray CT scan and shows the concentration of 123I-interleukin 2 there. High uptake in the spleen and kidneys but not liver is also evident
Fig. 10. Imaging infection (Bomanji et al. *62). Above: High uptake is seen in an infected amputation stump; 6-h image with 99mTc-Infecton. Below: 11~In white cell scan the next day was nega- tive at 6 and 24 h, possibly due to prolonged antibiotic therapy
preferred, great credit is due to Cytogen for taking HIIn- CYT-103 (B72.3) as Oncoscint through the regulatory minefield to a commercial product for colorectal (Fig. 4) and also ovarian cancers (* 148).
More selective receptor-binding tumour agents in- clude the old friend MIBG (*73, "157, '160, "161, *300) and the new 123I vasoactive intestinal peptide (VIP) introduced by Virgolini et al., which is reactive with gastrointestinal cancers (Fig. 5) but only a few en- docrine and pituitary tumours ( '114). Osmanagaoglu (*73) showed the MIBG scan is better than bone marrow
sampling in evaluating neuroblastoma. The MIBG bone scan was normal in 91 instances with bone marrow sam- pling normal in 89, whereas the MIBG bone scan was positive in 24 instances while bone marrow sampling was positive in only eight. Ady ( '161) showed that the 123I-MIBG scan at the sixth week of chemotherapy pre- dicted outcome. Ricard ( '160) was able to use the per- operative probe with MIBG.
In the class of highly selective agents, radiolabelled monoclonal antibodies still excel. The Sorin 99mTc-label- led anti-melanoma antibody is specific for cutaneous ( '181) and ocular melanoma ( '184) and there is a new one, 99mTc-labelled BW 575 ( '183). There is competi- tion from the highly selective receptor agent 123I-iodo- benzamide (Maffioli *623 and Kirchner "185) (Fig. 6) but not from 99mTc-glutathione ( '182) or IgF-FDG (*637). A new specific chimeric monoclonal antibody was introduced for squamous head and neck cancer, 99mTc-labelled ch174 (Baum * 149). This is tumour se- lective, unlike 99mTc-glutathione (*573) or 1HIn-bleomy- cin (*76). Monoclonal antibodies were described for pancreatic cancer (AR-3: Mariani "226), B cell lympho- ma (99mTc-labelled LL2: Goldenberg "228), malignant lymphoma (99mTc-labelled antigranulocyte mAb BW 250/183: Castellani * 606) and neuroblastoma (a chi- meric agent chCE7: D/Srr "159). Colorectal cancer re- mains a major target, with a new human IgG3 99mTC- 88BV59 reported by Serafini (* 145).
Thus the key to nuclear medicine's success in oncolo- gy in the future is accurate tissue characterisation. This is essential if nuclear medicine is to progress. It is aided by superimposition of the positive findings with SPET on the corresponding radiological image.
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

165
The heart
The search for the ideal test or combination of tests for myocardial viability remains the major concern for the cardiologist. Let us marshall the protagonists: ~SF-FDG, PET, stress and reinjection 2°1T1 and 99mTc-MIBI, and 123I-labelled fatty acids. Is ~SF-FDG a gold standard for myocardial viability? This was called into question by Nishimura et al. at the Society of Nuclear Medicine meeting [12], who showed that tSF-FDG uptake was greater than normal at the site of acute myocardial in- farction and this finding was still present in six of ten cases 6 months after the infarct. This was attributed to inflammatory cell inflitration, for white cells can be used to image myocardial infarction [13]. The short-term ca- nine data of Wijns et al. [14] appear to contradict this, but as Gould (15) pointed out, long-term studies of in- farction had not until now [12] been carried out. Huitink ('129) found that myocardial infarction studied at 5 + 2 days showed, as expected, a 2°~T1 defect 78% + 16% of normal but an overlap of 18F-FDG uptake with normal (89% _+ 18%). Clearly ~SF-FDG cannot be considered a gold standard for myocardial viability during the months following an infarct, when uptake is present in 'dead' tissue which appears to be due to the inflammatory infil- trate. The high uptake of ~SF-FDG in pneumonia and lung abscess, shown by Grimmel (*4), confirms the lik- ing of leucocytes for this sugar. 18F-FDG is more reliable in hibernating myocardium. Yokoyama ('127) showed that for the most accurate result (93%), a formal 'myo- cardial glucose utilisation rate' in mg/min/100 g had to be calculated using the Patlak plot whereas percentage ~SF-FDG uptake alone had only a 67% accuracy with overlap between non-viable and viable myocardium. A1- teh6fer ( '132) showed that viable tissue had an tSF-FDG uptake of more than 70% while non-viable tissue had an uptake of less than 50%, and that 2°~T1 was as good as 18F-FDG except in the inferior wall due to attenuation (vide infra). In comparison, with a 99mTc-MIBI uptake of less than 30%, there was a less than 10% chance of vi- able tissue, whereas defects between 30% and 70% may well be viable on ~SF-FDG PET. PET agents other than 18F-FDG are available: potassium-38, copper-62 ('91), rubidium-82 (*94), nitrogen-13 ammonia (*95) and a new ~SF-thio fatty acid from Julich, reported by Swaiger in his review.
Pharmacological stress is being extensively studied not only for 2°lTI and 99mTc-MIBI but also because it en- ables stress echo studies to be performed. The safety of dipyridamole was emphasised by Lette (*380). In 64 000 studies, the death rate was 1:10 000 the rate for non-fatal myocardial infarction was 1:5000, for ventricular ar- rhythmia 1:10000, for transient ischaemic attacks 1:6000 and for severe bronchospasm 1:10000. Dondi (*382) showed that hand grip exercise was an unnecessary accompaniment to dipyridamole stress. Lekakis ( '381) showed that beta-blockers need not be stopped for dobu- tamine, previously one of its main disadvantages.
Dobutamine stress echo studies compared reasonably well with 2°1T1 studies but usually had a lower sensitivity and higher specificity ('201); they were better than single-day 99mTc-MIBI studies (*384). Combined with rest 99mTc-MIBI they were thought to be a fair predictor of myocardial viability (*378). An alternative was Amri- none-Echo, which correlated with dipyridamole 99~Tc- MIBI studies (*375). For 2°1T1, it is generally agreed that stress-reinjection is superior to stress-redistribution [16, 17]. A 33% increase in viability in 175 patients was shown by Rioja (*202). Reinjection 2°1T1 also correlated with MRI findings (*370) and could be enhanced by nitrates (*369). The question of the timing of imaging after rein- jection was addressed by Bourgeois (*203) and imaging at 4 h was found to be preferable to that at 20 rain. This, if confirmed, is a nuisance with regard to good patient throughput,
The main problem with 2roT1 is its weak gamma-ray energy. Roach (*393) showed that transmission attenua- tion correction reduces the problems of interpreting re- duced inferior wall perfusion. Why is not this a standard protocol from the instrument makers? Loboguerrero (*389) showed that imaging the patient prone caused in- ferior wall underperfusion to disappear, to be replaced by anterior wall underperfusion due to attenuation.
99mTc-MIBI is gradually taking over from 2°iT1, partly because it allows more sophisticated analysis. Gated MI- BI is better than non-gated MIBI (*354), and first-pass MIBI augments the interpretation of stress MIBI (*374, *397). 99mTc-MIBI studies predicted restenosis after an- gioplasty (*358), myocardial salvage after thrombolysis ( '361) and coronary artery disease in a 3-year follow-up (*344). Tc-99m MIBI uptake correlates with the rate- pressure product at 1 mm ST depression on peak exer- cise (*343). 99~Tc-MIBI rest defects in non-infarct pa- tients predict severe coronary arterial disease ('164). Pierre Rigo gave a superb review of the need and meth- ods for quantitative assessment of cardiac studies.
Fritsch (*395) used a knowledge-based system (KBS) approach with a library of 250 2°~T1 and 220 99mTc-MIBI studies to analyse a new study by making a comparison with the best ten from the library. For >50% stenosis, 2°1T1 was positive in 76% and 99mTc-MIBI in 80% by ROC analysis. Pretschner demonstrated the KBS ap- proach to cardiology in the COST B2 symposium. Lette ('391), using artificial intelligence with 200 dipyrida- mole 2°~T1 studies, found that the specificity of a neural network was 95% compared to 82% with multivariate analysis for predicting cardiac complications in patients after major non-cardiac surgery. 'Age', 'sex', 'angina', 'death' ran the neural network slide, summarising in four words better than any poet, life as it is.
New myocardial tracers were evaluated. 99mTc-tetro- fosmin (Myoview) was shown to be taken up by myocar- dial myocytes not by active transport but by passive dif- fusion ('216). A same-day protocol was successful (*346). Uccelli ( '215) introduced 99mTc-N-NOEt with studies in the rat. Rossetti et al. ( '167) showed that, us-
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

166
ing a same-day protocol their new agent, 99mTc-Q12, demonstrated angiographically confirmed coronary arte- rial disease with 98% sensitivity.
What, then, is the optimal procedure for the routine evaluation of reversible myocardial ischaemia and myo- cardial viability? Following Matzer et al. [18], Wein- mann ('163) found that rest 2mT1 (poor for counts, good for viability) followed by stress 99mTc-MIBI (good for counts, poor for viability) was successful in 177 patients. Egroizard (*373) found the same in 57 patients. This combination of rest 2°1T1 and a stress 99mTC agent could be used with any of the newer 99mTc myocardial perfu- sion agents. This appears to be a good compromise, al- though their differing energies may cause problems.
Those with ~23I-labelled fatty acids know they have some of the best agents for viability: beta-methyl io- dophenyl pentadecanoic acid (BMIPP) (*242, "377), iodophenylpentadecanoic acid (IPPA) (*243, *426) and methyl hexadecanoic acid (*244). It is the ~23I label that prevents their wider adoption, mIn-antimyosin continues to be of benefit in the evaluation of myocardial infarct size (*55, "57), cardiac transplant ('56), risk stratifica- tion with 99mTc-MIBI (*58) and doxorubicin cardiotoxic- ity (*59). But where is 99mTc-antimyosin? Only when this is available will this procedure be used as widely as it should be.
Cardiac risk stratification was studied by Lette (*304) in 737 patients. In order of importance were jeopardised myocardium, left ventricular hypertrophy on ECG, and transient dipyridimole-induced left ventricular cavity dil- atation. Adamec (*303) studied 184 patients over 70 and 2°~T1 studies predicted major cardiac events better than the exercise ECG. Marie (*302) evaluated 220 patients with exercise 2°~T1, rest radionuclide ventriculography and angiography. The extent of the 2mT1 defect predicted death (P<0.001), as did age (P<0.01). The number of >70% stenoses on angiography predicted myocardial in- farction (P<0.01), as did the extent of reversible 2°~T1 defects (P<0.01) and age (P<0.05).
123I-MIBG in cardiac disorders was less successful. Decrease of MIBG uptake relates to left ventricular dys- function in hypertrophic cardiomyopathy (*274). In the diabetic heart the MIBG inhomogeneity index cannot re- place heart frequency analysis ('271). In fact, studies in the rat heart show that MIBG is not an accurate indicator of adrenergic integrity ('716). Nevertheless, it has its clinical benefits. The perfused denervated heart is identi- fied by 2°1T1 and MIBG studies. Kuikka (*275) went fur- ther and showed that angina is associated with the per- fused denervated heart in patients with myocardial in- farction. After cardiac transplantation, MIBG shows the- re is renervation of the heart in the anterior basal region in 40% (*276). Doxorubicin toxicity may be assessed (*272, *273).
Atheroma continues to tempt nuclear medicine with its importance and its elusiveness to imaging. ~23I-label- led LDL and rain-labelled oxine platelets showed no colocalisation (*443). 99mTc-hexamethyl-propylene anti-
ne oxime (HMPAO) platelets (*444), 125I-LDL ('251), tzSI-endothelin ('251), mIn-IgG ('251), mIn-HDL (*245) and 99mTc-recombinant tissue plasminogen acti- vator ('441) have been tried with varying success.
The brain
There still appears to be a disproportionate effort on the part of nuclear medicine with regard to brain tumours. Perhaps this is a historical angst. 18F-FDG and 2°~T1 were compared (*1, *627, *628) or 18F-FDG was used alone (*575, *629, *630). Carbon-ll-l-D-glucose was evalu- ated in normal brains (*83). An I8F boron neutron cap- ture agent was introduced ('631) but the numbers are against it being a beneficial approach. HC-methionine is promising (*2, "41).
Single photon agents included: 2°lT1 (*78, *574, '642), 99mTc-MIBI ('116, "117, "572), 99mTc-(V)DMSA ('641), 99mTc-glutathione ('573), ~23I-methyl tyrosine ('2), mIn-octreotide ('115, *259, *260, *458, *574, • 621), 125I-labelled monoclonal antibodies ('186) and anti-EGF antibody (*574). Of these the ~23I-labelled ami- no acid cz-methyl tyrosine has potential as a marker of tumour viability, not through protein synthesis but through amino acid transport, Langen (*2) won the Ma- rie Curie prize for this work (Fig. 7).
The real benefit of PET from its earliest days is the development and demonstration of 'brain chemistry' through the use of receptor-specific neurotransmitter an- alogues. 11C-Iomezanil ('254), l~C-Flumazenil ('79), 11C-FCB457 ('172) and llC-raclopride ('154) follow this theme. Budinger reviewed the real benefits of PET versus MRI, which were through the application of high- ly specific tracers with high resolution and proper quan- titation in an academic environment. With the excellence of 99mTc-HMPAO SPET ('7), I8F-FDG PET is no longer needed for imaging regional grey matter. Superimposi- tion of results on MRI or CT sections sited the epileptic focus (*288) (Fig. 8).
The advent of 123I-Iomazenil as a benzodiazepine re- ceptor agent and ~23I-iodobenzamide (IBZM) as a D2 postsynaptic receptor agent transfers PET advances to SEPT in a traditional way. ~23I-Iomazenil was validated in epilepsy against ~C-Flumazenil ('79), and in volun- teers against the equivalent ~C-Iomazenil with superim- posable results (*254); furthermore its uptake was quan- titated ('701). A new mono amino oxidase beta inhibi- tor, 123I-Ro 43-0463 was introduced (*306).
123I-IBZM uptake was studied in parkinsonianism, when its uptake was similar to that of to 11C-raclopride (* 154). Its uptake had a poor relationship with treatment outcome ('152) and a poor correlation with 99mTc-HM- PAO studies ('155). Its uptake could be quantitated (*566). It was also evaluated in the movement and sleep syndrome (*153), in narcolepsy ('568), in depression ('567), in Alzheimer's disease (*569) and in therapy with flunarizine ('151) and clozapine (*570). New D2
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

167
receptor agents were described, 123I-IBF ('156) and 123I [3-CIT (*82).
Head injuries have been neglected for too long. Mas- deu (*43) studied patients with mild head injuries and found that 12/12 had abnormlities on 99mTc- HMPAO SPET but only 1/12 on X-ray CT. Acute (*546, *547) and subacute (*547) injuries and extradural haematoma (*545) were also studied.
Physics
One of the strengths of this Congress was its physics. There were advances in the quantitation of brain studies, both in recognising the problems and in seeking solu- tions. In PET, Meyer (*683) showed how to make Patlak easy. Hellwig (*258) demonstrated the benefits of com- bining Patlak and the maximum likelihood approach. Rota Kops (*709) tackled the problem of attenuation factors and Kaiser (*688) made image correlations be- tween PET and MRI. 3D brain quantitation is being studied in relation to MRI using 'phantom of the opera'- like masks (*583) and in focal cerebrovascular disease (*285). A PET brain atlas is in preparation (*559). 3D SPET cold lesion volume rendering was achieved by Su- rova (*687) and colour combinations in SPET are prov- ing valuable (*582).
Quite sophisticated analyses of the problems with SPET were presented. Naud6 (*679) showed that in the two-window solution to scatter, the scatter ratio varied with depth, thus invalidating some manufacturers' cor- rections for scatter. A multiwindow scatter correction improved quality and quantitation ('177). Bourguignon (*707) showed that 3D Fourier filtering improved reso- lution for quantitation. The advantages of the ring SPET were felt to be the lack of reconstruction artifacts (*703) and improved resolution over multiheaded SPET sys- tems by at least 1 mm (*704).
In instrumentation a new small size high-resolution gamma camera was introduced by Parmentier ('140) and a Jttrium aluminium perovskit multicrystal camera by Blazek ('139). Peroperative probes were discussed ( '18 "160 *295 "710).
A good emphasis was on standards for data exchange. There was a COST B2 [19] (Cooperation in Science and Technology, European Community Programme) sympo- sium led by Bergmann. Interfile is the medium for the universal exchange of patient study images developed and promoted by Todd-Pokropek and Cradduck [20]. Its philosophy is being accepted by DICOM, the new stan- dard replacing ACRNEMA, and MEDICOM, the Euro- pean standard in development by working group WG4 of the European standard organisation (CEN) technical committee TC251. All these approaches have become 'object orientated' to free them from the restrictions of hardware, to become context independent and multimod- ality (*286). Interfile conversion programmes for AD- AC, Elscint and GE were described by Maurel (*690)
and imaging mailbox by Jonsson (*689). PACS for nu- clear medicine (*284) and by a PC-LAN (*283) were al- so described. As a chairman of an EWOS technical com- mittee once said in an introductory speech: "If you don't know the initials you are not in the field!".
To move these processes into routine work, that is, to persuade manufacturers of their importance, it is impera- tive that, when new equipment is purchased, it is speci- fied that an INTERFILE conversion programme must be included. Interfile, through the COST B2 programme, allows the use of software phantoms for quality assu- rance and quality control of analysis programs for the kidneys, the heart and the brain. Jarritt ( '179) described a multicentre SPET reconstruction program with inter- file data transfer. Graham ('178) described performance testing of multihead SPET using AAPM guidelines. Quality assurance for nuclear medicine was stressed by Lottes ( '312) following IEC 789 and the German stan- dard DIN 6855, and Kugi and Bergmann (*680) de- scribed the quality control of the quality control pro- grammes !
The theme that low-level radiation is good for you is gaining momentum. A 32% decrease in DNA strand bre- aks in mononuclear cells after 131I therapy at 24 h, re- turning to 'normal' at 5 days, was shown by Hengstler (*297). The recognition that low-level radiation induced enhancement of free radical scavengers and their benefi- cial effects was not discussed formally here but is be- coming accepted. There was no increase in genetic risk to 167 children whose mothers received 4 - 26 GBq of t31I (*298). The effective dose equivalent from nuclear medicine studies has fallen from 21 to 6 mSv from 1972 to 1991 (*694). The radiobiology of nuclear medicine therapy should be recognised as different from that of external beam therapy [21].
Genitourinary studies
Two new renal agents were introduced: 99mTc-ethylene dicysteine (EC) and 99mTc-99m DACH, developed by Solanki [22,23]. 99mTc-EC was shown to have a better clearance than 99mTc-mercaptoacetyltriglycine (MAG3), i.e. 71% of ortho-iodohippurate clearance as compared to 58% (average of three papers, *49, *50, "51). Capto- pril test was better with 99mTc-EC than with 99mTc-diet- hylene triamine (DTPA) ('517). 99mTc-DACH, which is cationically transported [23], was shown in the baboon to have less uptake than MAG3, which is anionically transported (36% VS 59%), and to have some isomers that may reduce clearance (*731).
Captopril renal radionuclide studies have stood the test of time. They may be used to predict restenosis (*86) or bilateral renal artery stenosis (*88). Captopril renog- raphy is better than duplex doppler for diagnosing renal artery stenosis (87% VS 70%) (*89). The test with mean parenchymal transit time analysis is able to predict the benefit or detriment of angiotensin-converting enzyme
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

168
(ACE) inhibitors in patients with moderate to severe re- nal impairment (*530). The adverse effect of ibuprofen on glomerular filtration rate and renal plasma flow in chronic glomerulonephritis was demonstrated (*526). The use of doses of frusemide on a per kilogram basis was thought to be beneficial(*125). Factor analysis was shown to be the best way of extracting renal activity ti- me curves from serial renal images, i.e. better than man- ual or automated regions of interest (* 123), and was also tried out in 'predicting' the response to frusemide ('124).
99mTc-dimercaptosuccinic acid (DMSA) studies have good observer concordance ('194). 99mTc-DMSA SPET is better for visualising scars than planar or 3D imaging ('591) and better than ultrasonography, intravenous urography or micturating cystography for detecting acu- te pyelonephritis ('195). 99mTc-DMSA is good for the follow-up of pyelonephritis ('193, "195) and in predict- ing renal function outcome ('196). Gordon (*85) sho- wed its value with captopril in identifying renovascular causes of hypertension in children.
Gastroenterology
Time-dependent studies are being clinically applied. An- tral mobility measurements are becoming popular (*289, "291, *463), (Fig. 9). Small bowel transit is faster in pa- tients with diabetic autonomic neuropathy (*465). Co- lonic transit times bay be analysed using a geometric centre method (*470).
Liver transit is slowed in non-insulin-dependent dia- betes as assessed with ~z3I-labelled insulin ('461). Bay- ham showed that liver mean transit time measured by deconvolution analysis does not change after gallstone external shock wave lithotripsy but the hepatic extraction efficiency decreases, recovering by a week later (*208). Liver fractal analysis was of novelty interest (*222) and this approach was also applied to the lungs ('221).
Bones and joints
For bone scanning the emphasis was on SPET. Low back pain needs SPET ('13, "14, "313, "314), though no di- rect comparisons with conventional posterior oblique views were reported. The work-load of SPET for all chronic radiologically negative back pains appears daunting.
The scaphoid fracture on the bone scan (*323) was compared with MRI (*322) and the treatment of sca- phoid pseudoarthritis with shock wave therapy was as- sessed (*324). Three-phase imaging was reported to be of value in diagnosing reflex sympathetic dystrophy (*325) and in distinguishing malignant from benign tu- mours (*647).
Synovitis was treated by Dysprosium-165 ferric hy- droxide (*677) and haemophilic haemoarthritis by 90y
(*678). Bone metastases underwent therapy with Rheni- um-186 1-1-hydroxyethylene diphosphonate ('229, "231, *674), 153Sm-ethylene diamine tetramethylene- phosphonate (EDTMP) (*232, *675), Holmium-166 EDTMP (*675) or Strontium-89 (*232, *676).
Inflammation and infection
The studies on inflammation and infection also demon- strate the movement from non-specificity to specificity in the attempt to characterise the tissue or disease better. The general uptake of 67Ga was noted previously (*494, *495, *496, *506, *598) and the sensitivity but lack of specificity of the bone scan is well known ('17, *328, *331). Inflammation-specific agents include: 99mTc-HM- PAO-labelled white cells (*64, *65, *478) 99mTc-label- led anti-granulocyte antibodies (*25, *30, *327, *478, *486, *488) 99mTC human immune globulin (HIG) (*28, *330, *490) with some evidence for binding bacteria (*252), lllIn-HIG (*26, *27, *28, *29) with rain release at the site of infectious foci (*29), 99mTc-glutathione ('717) and lmIn-biotin (following streptavidin as the non-specific agent in two-stage imaging) ('61).
A more specific agent for infection is 99mTc-Infecton, a labelled antibiotic derivative which binds to living bac- teria (*62) (Fig. 10). Radiolabelled antibiotics with other uses were presented: 99mTc-erythromycin aerosol for lung macrophages (*32) and 99mTc-cephalosporanic de- rivatives (*732). Activated T cells were imaged in auto- immune disease by Signore using ~23I-interleukin 2 (*63) (Fig. 11), and 99mTc-interleukin 2 is about to undergo clincal trials [24]. 99mTc-anti CD 24 monoclonal antibod- y was shown to be more specific for rheumatoid arthritis after 4 h than a neutral monclonal antibody ('15), con- firming the principle that specific uptake of a monoclo- nal antibody increases with time whereas non-specific uptake after the initial distribution tends to decrease with time [25]. Amyloid specific imaging with 12~I-labelled serum amyloid protein was confirmed (* 103). Thus the principle of progressing from general inflammatory markers to more disease-specific tissue and bacterial characterisation was supported by these studies.
Conclusion
The organisers and scientific committee are to be con- gratulated on a successful Congress. The oral and poster presentations have demonstrated the themes and distrac- tions for nuclear medicine in the future. The objective measurement of organ function is taking on a role in the medical audit and outcome analysis of many medical and surgical procedures applied to the heart, brain, kid- neys, etc. The move to combine specificity with sensitiv- ity means more precise tissue characterisation as an aid to diagnosis, theraapy and prognosis, particularly for malignant disease and in inflammatory disorders. The
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994

169
quality service that nuclear medicine provides for the pa- tient and the medical practitioner requires a stable and secure health care environment.
References
N.B. * Numbers within parentheses are the abstract numbers of European Journal of Nuclear Medicine Abstract Congress Book 1993; 20: vol 10, 817-1013. They are not repeated here. They are not comprehensive.
1. Warburg O. Versuche an aberlebendem Carcinomgewebe. (Methoden). Biochem Z 1923; 142:317-333.
2. Flier JS, Mueckler MM, Usher R Lodish HE Elevated levels of glucose transport and transporter messenger RNA are in- duced by ras or sac oncogenes. Science 1987;235:1492-1495.
3. Minn H, Paul R. Cancer treatment monitoring with fluorine 18-2-flouro-2-deoxy-D-glucose and positron emission tomog- raphy: frustration and failure. Eur J Nucl Med 1992; 19:920-924.
4. Braams JW, Pruim J, Nikkels Pe t al. Detection of lymph node metastases in squamous head-neck cancer with MRI and FDG-PET. J Nucl Med 1993;34:55P-56R
5. Khalkhali L, Mena I, Jouanne E et al. Tc-99m-sesta MIBI pro- ne breast imaging in patients with suspicion of breast cancer. J Nucl Med 1993;34:140R
6. Khalkhali L. Presentation to the Middlesex Hospital, July 1993.
7. Krenning ER Kwekkeboom DJ, Bakker et al. Somatustin re- ceptor scintigraphy with I IIIn-DTPA-D-Phel and 123I-Tyr3-oc- treotide: the Rotterdam experience with more than 1000 pa- tients. Eur J Nucl Med 1993 ;20:716-731.
8. Bihl H, D6rr U. Somatoreceptor imaging. First German meet- ing Stuttgart 1992. Hormone and Metabolic Research Supple- ment Series vol 27. Stuttgart: Thieme, 1993.
9. Ur E, Mather SJ, Bomanji Je t al. Pituitary imaging using a la- belled analogue of somatostatin. Clin Endocrinol 1992;36:147-150.
t0. Ur E, Bomanji J, Mather SJ et al. Localisation of neuroendo- crine tumours and insulinomas using radiolabelled somatosta- tin analogues, ~23I-Tyr3 octreotide and mIn-pentatreotide. CIin Endocrinol 1993;38:501-506.
11. Granowska M, Jass JB, Britton KE, Northover JMA. A pros- pective study of the use of ~lIn-labelled monoclonal antibody against carcino-embryonic antigen in colorectal cancer and of
some biological factors affecting its uptake. Int J Colorectal Dis 1989;4:97-108.
12. Nishimura T, Uehara T, Ishida Yet al. Is ~SF-FDG a gold stan- dard for myocardial viability? Assessment by sequential myo- cardial PET scan following acute myocardial infarction. J Nucl Med 1993;34:24P-25R
13. Muir AJ, Bell D, Jackson Met al. The use of ~J~In-labelled au- tologous neutrophils in imaging myocardial infarction. Nucl Med Commun 1988;9:707-711.
14. Wijns W, Melin JA, Leners Ne t al. Accumulation of polymor- phonuclear leucocytes in reperfused ischaemic canine myocar- dium relation with tissue viability assessed by fluorine-18-2- deoxyglucose uptake. J Nucl Med 1988;29:1826-1832.
15. Gould KL. PET perfusion imaging and nuclear cardiology. J Nucl Med 1991;32:579-606.
16. Zaret BL, Wackers FJ. Nuclear cardiology, part I. N Engl J Med 1993;329:775-783.
17. Schoeder H, Friedrich M, Topp H. Myocardial viability: what do we need? Eur J Nucl Med 1993;20:792-803.
18. Matzer L, Kiat H, Freidman J e t al. Separate acquisition dual isotope myocardial perfusion SPECT using pharmacologic stress. J A m Coll Cardiol 1992;19 Suppl A:127A.
19. Britton KE, Vauramo E. COST B2: the quality assurance of nuclear medicine software. Eur J Nucl Med 1993;20:815-816.
20. Todd-Pokropek A, Cradduck TD, Deconinck E A file format for the exchange of nuclear medicine image data: a specifica- tion of Interfile Version 3.3. Nucl Med Commun 1992;13:673-699.
21. Britton KE. Radiobiology workshop: an elemental dose ap- proach to radioimmunotherapy. In: Epenetos AA, ed. Mono- clonaI antibodies 2. Applications in clinical oncology. Lon- don: Chapman & Hall; 1993:383-390.
22. Solanki KK, Theobald AE, Britton KE. Potential new renal imaging agent using the active tubular cationic mechanism. J. Nucl Med 1991 ;32:1102.
23. Padhy AK, Solanki KK, Bomanji Je t al. Clinical evaluation of 99mTc diaminocyclohexane, a renal tubular agent with cationic transport: results in healthy human volunteers. Nephron 1993;65:294-298.
24. Chianelli M, Signore A, Fritzberg AR, Mather SJ. 99mTcm-In- terleukin 2: a new radiopharmaceutical for use in autoimmune disease. Nucl Med Commun 1993; 14:280-281.
25. Britton KE, Granowska M, Mather SJ. Radiolabelled mono- clonal antibodies in oncology. I. Technical aspects. Nucl Med Commun 1991; 12:65-76.
European Journal of Nuclear Medicine Vol. 21, No. 2, February 1994