

HIGH DOSE INSULIN IN BETA BLOCKER AND … 5C High-Dose Insulin Therapy (T...high dose insulin in...
67
HIGH DOSE INSULIN IN BETA BLOCKER AND CALCIUM CHANNEL BLOCKER OVERDOSE
Transcript of HIGH DOSE INSULIN IN BETA BLOCKER AND … 5C High-Dose Insulin Therapy (T...high dose insulin in...

HIGH DOSE INSULIN IN BETA BLOCKER AND CALCIUM CHANNEL BLOCKER OVERDOSE


TOM SCULLARD RN MSN CCRN CLINICAL CARE SUPERVISOR
MEDICAL INTENSIVE CARE UNIT HENNEPIN COUNTY MEDICAL
CENTER MINNEAPOLIS MINNESOTA


OBJECTIVES
1. Identify the cardiovascular effects of beta blocker
and calcium channel blocker overdoses
2. Describe the proposed mechanism of high dose
insulin use in beta blocker and calcium channel
blocker overdose
3. Describe the role of the nurse when caring for the
patient receiving high dose insulin therapy.

OVERDOSE
• Intentional ingestion
• Unintentional ingestion
• Patient error
• Medication interaction
• Children

BETA BLOCKER & CALCIUM CHANNEL BLOCKER OVERDOSE
• Overdose is associated with a high incidence of
morbidity and mortality due to cardiovascular
toxicity including profound hypotension and
conduction disturbances

AMERICAN ASSOCIATION OF POISON CONTROL CENTERS’ NATIONAL POISON
DATA SYSTEM
• 2012
• 10691 beta blocker overdoses
• 5076 calcium channel blocker overdoses
• Fatalities
• beta blocker 13
• calcium channel blocker 24

BETA BLOCKERS & CALCIUM CHANNEL BLOCKERS
• Beta Blockers
• 128 million prescriptions for β-blockers filled in 2009
• 5th most commonly prescribed medication class
• Calcium channel blockers
• 98 million prescriptions filled in 2010

BETA BLOCKER USES
• Beta blockers are used for treating:
Abnormal heart rhythm
High blood pressure
Heart failure
Angina (heart pain)
Tremor
Pheochromocytoma
Prevention of migraines

CALCIUM CHANNEL BLOCKERS
Amlodipine (Norvasc)
Diltiazem (Cardizem LA, Tiazac)
Felodipine (Plendil)
Isradipine (Dynacirc)
Nifedipine (Adalat, Procardia)
Nicardipine (Cardene)
Nimodipine (Nimotop)
Nisoldipine (Sular)
Verapamil (Covera-hs, Verelan PM, Calan)
Diltiazem
Nicardipine

CALCIUM CHANNEL BLOCKER USES
Calcium channel blockers are approved for treating:
High blood pressure
Angina
Abnormal heart rhythms (for example, atrial fibrillation,
paroxysmal supraventricular tachycardia)
Subarachnoid hemorrhage
Raynaud's phenomenon
Cardiomyopathy
Migraine headaches

CARDIAC MYOCTES
• Myocte: Type of cell found in muscle tissue
• Cardiac myoctes responsible for:
• Electrical impulses
• Contractility
• Exchange ions

BETA AND CALCIUM CHANNEL RECEPTORS
What do they do?

BETA RECEPTORS
• Beta 1
• Primarily regulate myocardial tissue and affect
the rate of contraction via impulse conduction
• Beta 2
• smooth muscle tone and influence vascular and
bronchiolar relaxation
• Beta 3
• thought to primarily affect lypolysis and may have
effects on cardiac inotropy

BETA RECEPTORS ACTION
• Beta receptors coupled with Gs protiens
• Activate adenylate cyclase
• Form cAMP from ATP
activates cAMP dependent protein kinase
(PK-A)
• Causes increase calcium into the cell
• Leads to increased release calcium by
sarcoplasmic reticulum in the heart
• Increased contractility heart rate

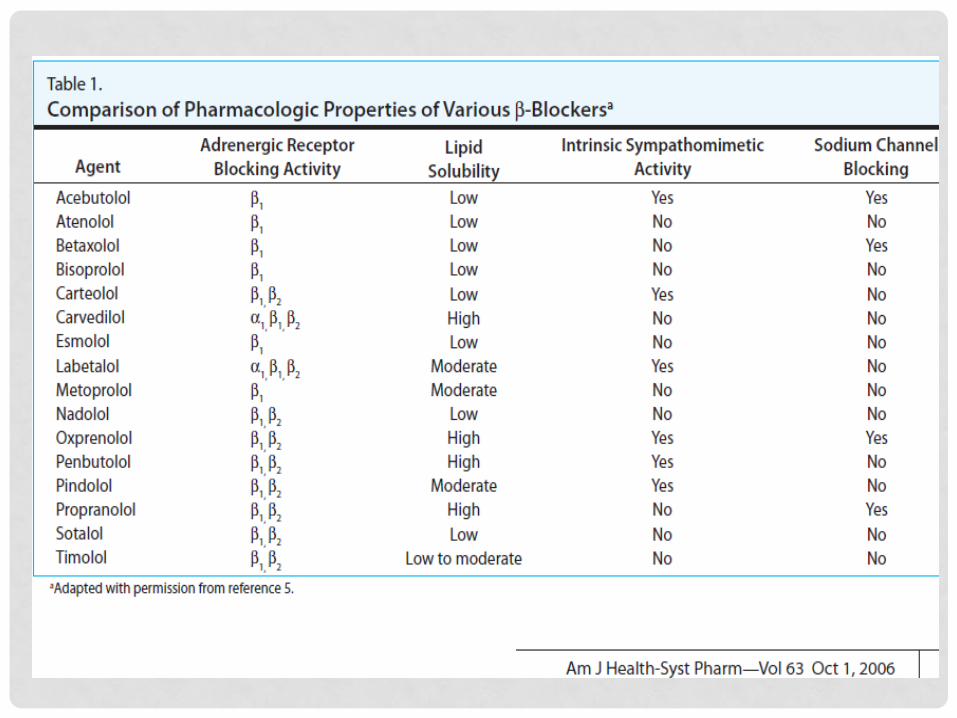
BETA- BLOCKERS
• Beta-blockers selectively antagonize the effects of
catecholamines at the beta-adrenergic receptor
that are linked to G proteins

BETA BLOCKERS
• Beta-adrenergic antagonists competitively
antagonize the effects of catecholamines at the
beta-adrenergic receptor and blunt the
chronotropic and inotropic response to
catecholamines

BETA BLOCKER OVERDOSE SYMPTOMS
• Hypotension
• Bradycardia
• Bronchospasms
• Cool extremities r/t vasoconstriction
• Beta 2 blockade and alpha -1 activity
• Low blood sugars ?
• Inhibition of release of glucagon in the pancreas

L-TYPE CALCIUM CHANNELS
• Found on myocardial cells
• contractility
• Vascular smooth muscle cells
• Contractility
• Conducting cells
• Pacemaker cells
• β-islet cells of the pancreas

CALCIUM CHANNELS
• Calcium enters open voltage-sensitive calcium
channels to promote the release of calcium from
the sarcoplasmic reticulum. The released calcium
combines with troponin to cause muscle
contraction via actin and myosin fibers

CALCIUM CHANNEL BLOCKER OVERDOSE
• Calcium channel blockers prevent the opening of
the voltage-gated calcium channels and reduce
calcium entry into cells during phase 2 of an action
potential.

CALCIUM CHANNEL BLOCKERS
• Dihydropyridines
• Preferentially block L-type calcium channels in the
vasculature (vasodilators)
• Nondihydropyridines
• Selectively block L-type calcium channels in the
myocardium (depressive effect on conduction and
contractility).

CALCIUM CHANNEL BLOCKER OVERDOSE SYMPTOMS
Hypotension
Bradycardia
Hyperglycemia
Hypoinsulinemia
Warm extremities (vasodilation)
Conduction delays
Metabolic Acidosis (poor perfusion)
BETA BLOCKER/ CALCIUM CHANNEL BLOCKER DRUG INDUCED SHOCK
• Heart preferred energy source
• Free Fatty Acids
• Stress
• Carbohydrate
• Increased glucose (glycogenolysis)
• Decreased insulin (pancreatic b-islet cell blockage)
• Lack of fuel for energy production
• Aerobic Anaerobic metabolism

BETA BLOCKER AND CALCIUM CHANNEL OVERDOSE
• In overdose, β-blockers and CCBs often have similar
presentation and there is much overlap in
treatment.
• Cardiotoxicity characterized by hypotension and
bradycardia is the common clinical feature

TREATMENT
• Airway
• Breathing
• Circulation
• Decontamination (Gastrointestinal)
• Gastric lavage
• Activated charcoal
• Whole bowel irrigation

TREATMENT
• Fluids
• Atropine
• Calcium
• Glucagon
• Pacing
• Adrenergic drugs
• dopamine, norepinephrine, epinephrine
• Insulin


INSULIN
• Case series
• Animal models

INSULIN
• When to use
• Conventional therapies fail
• Fluids
• Atropine
• Calcium
• Glucagon
• Pacing
• Adrenergic drugs
• dopamine, norepinephrine, epinephrine

INSULIN
• Strong positive inotropic effect
• Increases uptake of carbohydrates
• The preferred fuel substrate of the heart under stressed
conditions
• Inhibits free fatty acid metabolism
• Vasodilation
• Improves local microcirculation
• Accelerates oxidation of myocardial lactate and
reversal of metabolic acidosis

INSULIN DOSING
• 1 unit/kg bolus dose ( regular insulin)
• 10 units/kg/ bolus
• continuous infusion 0.5-1 unit/kg /hr
• 10 - 20 units/kg/hr
• Titrate to response (20-30 minutes)
• Heart rate 50
• Systolic blood Pressure 100

INSULIN DOSING
• Onset of action = 15-45 minutes ? 2 hours
• Continue until hemodynamically stable
• Duration – hemodynamic status
• 9-72 hours

DEXTROSE
• Dextrose bolus 0.5g/kg with initial insulin bolus if
blood sugar < 400 mg/dl
• Infusion 125-250 ml/Hr of 10% solution
• Goal glucose- 100-200 mg/dl

COMPLICATIONS OF HIGH DOSE INSULIN
• Hypoglycemia
• Supplemental glucose
• Hypokalemia
• Extracellular intracellular shift
• Monitor every hour while insulin titration
• Every 6 hours once stable
• Target 2.8-3.2

NURSING CARE
• General nursing care
• Frequent glucose monitoring
• 20-30 minutes for the 1st hour then hourly
• Insulin/dextrose titration
• Frequent labs

WEANING INSULIN
• Slow taper
• Do not stop abruptly
• Continue to monitor blood glucose for 24 hour after
insulin discontinued

CASE STUDY

ED
• BP 88/54
• Pulse 57
• Temp(Src) 37 °C
• 98.6 °F
• Resp 15
• Wt 47.9 kg

MEDICATIONS

MEDICATIONS

ED
• ED
• Hypotensive and Bradycardic
• HR 55, BP 60/30
• Norepinephrine drip started .01
• 50 Units Regular insulin IV
• Central line
• D50 drip
• Calcium

ED
• Insulin drip started at 1 unit/kg/hr
• Norepinephrine weaned off
• Transferred to MICU

CASE STUDY
• Transferred to MICU
• Hypotensive SBP ( 60-70s)
• Insulin 2 units/kg/hr 8 units kg/hr - MAP of 65
• q15 minute glucose checks with D50 infusion
• Norepinephrine up to 0.4 mcg/kg/min
• Start dopamine as needed with goal MAP of 65
• Hourly potassium checks with replacement as needed
• Calcium and ionized calcium

ARRIVAL TO MICU 1600

6/23

6/23
• D5 @ 75
• D50 @ 80

6/23

6/23

6/24
• D5 @ 75
• D50 @80
• MAP-68-72


6/24




• D50 = 60
• D5 =100


• D50 = 40 cc/hr
• D5 = 100 cc/hr
• Levophed 0.17 mcg/kg/min

CALCIUM




REFERENCES
• Doepker, B., Healy, W., Cortez, E., & Adkins, E. J. (2014). High-dose insulin and intravenous lipid emulsion therapy for cardiogenic shock induced by intentional calcium-channel blocker and beta-blocker overdose: A case series. The Journal of Emergency Medicine, 46(4), 486–490. doi: http://dx.doi.org/10.1016/j.jemermed.2013.08.135
• Engebretsen, K. M., Kaczmarek, K. M., Morgan, J., & Holger, J. S. (2011). High-dose insulin therapy in beta-blocker and calcium channel-blocker poisoning . Clinical Toxicology, 49, 277-283. doi: 10.3109/15563650.2011.582471
• Kerns, W. (2007). Management of b-adrenergic blocker and calcium channel antagonist toxicity. Emergency Medicine Clinics of North America, 25, 309-339. doi: 10.1016/j.emc.2007.02.001
• Lheureux, P., Zahir, S., Gris, M., Derrey, N., & Penaloza, A. (2006). Bench-to-bedside review: Hyperinsulinaemia/euglycaemia. Critical Care, 10(3). Retrieved March 4, 2014, from http://ccforum.com/content/10/3/212
• Lyden AE, Cooper C, Park E (2014) Beta-Blocker Overdose Treated with Extended Duration High Dose Insulin Therapy. J Pharmacol Clin Toxicol 2(1):1015.
• Mowry, J., Spyker, D., Cantilena, L., Bailey, E., Ford, M., (2013). 2012 annual report of the american association of poisoncontrol centers ’ national poison data system (npds): 30th annual report . Clinical Toxicology, doi: 10.3109/15563650.2013.863906
• Shepard, G. (2006). Treatment of poisoning caused by β-adrenergic. American Journal of Health-System Pharmacy , 63, 1828-35. doi: 10.2146/ajhp060041

REFERENCES
• Woodward, C., Pourmand, A., & Mazer-Amirshahi, M. (2014). High dose insulin therapy, an evidence
based approach to beta blocker/calcium channel blocker toxicity . DARU Journal of
Pharmaceutical Sciences , 22, 36. doi: 10.1186/2008-2231-22-36













![Efficacy and Safety of Fast-Acting Insulin Aspart in ... · The manner in which the bolus insulin dose is adjusted is an important aspect of diabetes self-management [4, 5]. Dose](https://static.fdocuments.us/doc/165x107/5f069ec27e708231d418e5ea/efficacy-and-safety-of-fast-acting-insulin-aspart-in-the-manner-in-which-the.jpg)




