Development of a Stable Latanoprost Solution for Use as Eye Drops
Upload
jose-moralesCategory
view
213download
1
Rarely, angle-closure glaucoma occurs with full resolutionupon discontinuation of the sulfa medication.2 The under-lying mechanism by which this occurs has been bettercharacterized with ultrasound technology. Ciliary bodyedema causes relaxation of zonules, which allows lensthickening. Anterolateral rotation of the ciliary bodyabout its attachment to the scleral spur leads to anteriordisplacement of the iris–lens complex and concomitantshallowing of the anterior chamber. Choroidal detach-ments and supraciliary effusions are frequently present.Glaucoma occurs without pupillary block; thereby periph-eral iridotomies are ineffective.
Topiramate is a sulfamate-substituted monosaccharidewith a labeled use for partial-onset seizures. Given theonset within 2 weeks of initiating therapy and rapidimprovement after cessation of therapy, it is implicated asthe causative agent in our patient. Other sulfa-derivativedrugs, including acetazolamide,3 hydrochlorothiazide,4 andsulfamethoxazole5 have been noted to cause similar com-plications. Although acetazolamide has been reported tocause bilateral acute angle-closure glaucoma by the samemechanism, several factors lead us to believe that this wasnot the case in our patient. First, the symptoms and signsof bilateral acute angle-closure glaucoma clearly precededthe administration of the single dose of acetazolamide.Second, this reaction has not been reported after a singledose of acetazolamide, but only after a sensitizing dose inthe past or repeated dosing. Increased awareness of thisrare, idiosyncratic reaction is essential for ophthalmolo-gists to avoid visual loss and institute appropriate, timelyintervention.
REFERENCES
1. Grinbaum A, Ashkenazi I, Gutman I, Blumenthal M. Sug-gested mechanism for acute transient myopia after sulfon-amide treatment. Ann Ophthalmol 1993;25:224–226.
2. Maddalena MA. Transient myopia associated with acuteglaucoma and retinal edema, Arch Ophthalmol 1968;80:186–188.
3. Fan JT, Johnson DH, Burk RR. Transient myopia, angle-closure glaucoma, and choroidal detachment after oral acet-azolamide. Am J Ophthalmol 1993;115:813–814.
4. Geanon JD, Perkins TW. Bilateral acute angle-closure glau-coma associated with drug sensitivity to hydrochlorothiazide.Arch Ophthalmol 1995;113:1231–1232.
5. Postel EA, Assalian A, Epstein DL. Drug-induced transientmyopia and angle-closure glaucoma associated with supra-ciliary choroidal effusions. Am J Ophthalmol 1996;122:110 –112.
Herpes Simplex Virus Dermatitis inPatients Using LatanoprostJose Morales, MD, Zuhair M. Shihab, MD,Sandra M. Brown, MD, andMichael R. Hodges, MD
PURPOSE: To describe the possible association of latano-prost with herpetic dermatitis of the periocular skin.METHOD: Interventional case reports. A 79-year-oldwoman with open-angle glaucoma developed a vesiculardermatitis of the left lower eyelid 14 months afterstarting latanoprost therapy. An 84-year-old man withpigmentary glaucoma developed a vesicular dermatitis ofthe right upper lid after 2 months of treatment withlatanoprost and 8 days of treatment with tobramycin/dexamethasone for presumed bacterial conjunctivitis. Inboth cases, the dermatitis was characteristic of a herpeticinfection.RESULTS: Latanoprost was discontinued in both cases.The woman was treated with vidarabine 3% ointment,and the man was not treated with antiviral agents. Inboth patients, the dermatitis healed uneventfully. Thelesions of the man were cultured, and a biopsy wasperformed; herpes simplex virus type 1 was recoveredfrom the culture and confirmed by immunofluorescencetesting.CONCLUSION: Latanoprost, which has been associatedwith reactivation of herpetic keratitis, may also causereactivation of herpetic dermatitis of the periocular skin.(Am J Ophthalmol 2001;132:114–116. © 2001 byElsevier Science Inc. All rights reserved.)
LATANOPROST (XALATAN; PHARMACIA AND UPJOHN,
Kalamazoo, Michigan) was approved for treatment ofglaucoma in 1996. In 1999, Wand and associates1 reporteda possible association between latanoprost and the reacti-vation of herpes simplex virus keratitis. Herein, we de-scribe two cases of herpetic dermatitis of the eyelids,possibly associated with the use of latanoprost.
● CASE 1: A 79-year-old white woman was treated for 22years for open-angle glaucoma. During that time, noepisodes of herpetic dermatitis or keratitis were recorded.Latanoprost in both eyes was added to her medicationregimen of timolol and dorzolamide on December 10,1998. On February 4, 2000, the patient presented with a3-day history of redness, itching, and “blisters” of the leftlower eyelid. Examination revealed numerous open andcrusted vesicles of the left lower eyelid (Figure 1). Noassociated conjunctivitis, keratitis, or uveitis was found.Latanoprost was discontinued, and vidarabine 3% ophthal-mic ointment was prescribed. The vesicles healed unevent-fully without scarring. The patient was not rechallengedwith latanoprost.
Accepted for publication Mar 27, 2001.From the Department of Ophthalmology and Visual Sciences, Texas
Tech University Health Sciences Center, Lubbock, Texas (J.M., S.M.B.,M.R.H.) and Lubbock, Texas (Z.M.H.).
Inquiries to Sandra M. Brown, MD, 3601 Fourth St, STOP 7217,Lubbock, TX 79430-7217; fax: (806) 743-2471; e-mail [email protected]
AMERICAN JOURNAL OF OPHTHALMOLOGY114 JULY 2001

● CASE 2: An 84-year-old white man was treated for 26years for pigmentary glaucoma. During that time, noepisodes of herpetic dermatitis or keratitis were recorded.Latanoprost in the left eye was added to his medicationregimen of timolol, pilocarpine, brimonidine, and dorzol-amide in April, 1999. Latanoprost in the right eye wasadded to timolol, pilocarpine, and brimonidine on Febru-ary 28, 2000. On April 26, 2000, the patient presentedwith a 3-day history of redness of the eyelids and conjunc-tiva of both eyes, with matting and a foreign bodysensation. Symptoms initially began in the left eye. Onexternal examination, moderate swelling of all four eyelidswas present. Slit-lamp examination showed moderate(12) injection of the conjunctiva with palpebral folliclesand mild watery discharge; the corneas were clear, and nouveitis was found. A diagnosis of probable bilateral bacte-rial conjunctivitis was made, and a combination tobramy-cin/dexamethasone eyedrop was prescribed in both eyes.The patient returned on May 4, 2000, with multiple openand crusted vesicular lesions on the right upper eyelid
(Figure 2). A diagnosis of probable herpes simplex virusdermatitis was made; viral cultures and biopsies of severallesions were performed. Latanoprost and tobramycin/dexa-methasone were discontinued. The lesions healed un-eventfully without antiviral treatment.
Herpes simplex virus type I was isolated from the viralcultures of Patient 2 and confirmed by direct fluorescenceantibody testing. Pathology reported the presence of squa-mous cells with recognizable nuclei, nuclear molding,amorphous nucleoplasm, and salt and pepper nuclearmembranes characteristic of the herpes virus cytopathiceffect.
Cutaneous herpes simplex infection can be primary(direct inoculation of virus into skin), or secondary (reac-tivation of quiescent virus in nerve ganglia). Both formspresent as a focal cluster of vesicles, initially weeping andthen crusted, which resolve over 5 to 7 days. A symptomprodrome of itching or nonspecific discomfort, followed byredness and then vesicle development, is typical. In reac-tivated infections, the vesicles may follow a dermatomal
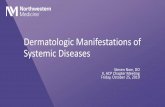
FIGURE 2. Patient 2. (Left) Right upper lid with erythema and slight edema. (Right) Higher magnification shows discrete openand crusted vesicles.
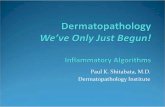
FIGURE 1. Patient 1. (Left) Left lower lid with focal erythema and slight edema. (Right) Higher magnification shows discrete openand crusted vesicles.
BRIEF REPORTSVOL. 132, NO. 1 115

distribution. In a patient with no previous episodes ofvesicular eyelid rash, the first attack of dermatitis may stillbe caused by reactivation of quiescent herpes virus; in thiscase, labial cold sores are a common primary infection,which leads to virus migration and proliferation in theGasserian ganglion. The virus then reactivates in the V1or V2 branches of the Trigeminal nerve to cause oculardisease.
Latanoprost is a prostaglandin analog. Increased prosta-glandin levels have been implicated in many origins ofcutaneous herpetic recurrence, and they may represent animportant final common pathway in reactivation of viralreplication.2 We believe that both of our patients sufferedattacks of recurrent herpes simplex virus dermatitis. In thefirst case, latanoprost was started 14 months before theonset of symptoms, whereas in the second case, it wasstarted in the affected eye 2 months before onset. It isinteresting to speculate whether the use of a topicalcorticosteroid in Patient 2 further increased his risk forherpetic reactivation.
Wand and associates1 described three patients withherpes simplex virus keratitis recurrence that was tempo-rally associated with the use of latanoprost. One patientdeveloped symptoms 5 months after starting treatment;when the patient was inadvertently rechallenged, thekeratitis recurred in a few days. Two other patients in thisreport developed herpes simplex virus keratitis manifesta-tions between 1 week and 1 month of initiating latano-prost use. A recent laboratory study in rabbits confirmed arelationship between latanoprost and the recurrence andseverity of herpes simplex virus keratitis.3 Based on thereport of Wand and associates1 and on our cases, it appearsthat the time to reactivation after starting latanoprost isidiosyncratic, and it may be influenced by other factorsmediating immune competence.
The possibility exists that the herpetic dermatitis inboth our patients was primary, or it recurred coinciden-tally. Proving a direct causal relationship is difficult; we didnot feel that a rechallenge with latanoprost was in thepatients’ best interests. We know that latanoprost isabsorbed into the eyelid, as evidenced by hypertrichiasisand increased pigmentation of the eyelid skin.4,5 There-fore, it seems plausible to postulate that over time, anadequate level of the medication could develop in eyelidtissues to reactivate latent herpes virus. Clinicians shouldconsider the diagnosis of herpetic dermatitis when apatient recently prescribed latanoprost presents with com-plaints of nonspecific periorbital discomfort, itching, orredness, before the development of characteristic vesicles.
REFERENCES
1. Wand M, Gilbert CM, Liesegang TJ. Latanoprost and herpessimplex keratitis. Am J Ophthalmol 1999;127:602–604.
2. Pereira FA. Herpes simplex: evolving concepts. J Am AcadDermatol 1996;35:503–520.
3. Kaufman HE, Varnell ED, Thompson HW. Latanoprost in-
creases the severity and recurrence of herpetic keratitis in therabbit [comment]. Am J Ophthalmol 1999;127:531–536.
4. Johnstone MA. Hypertrichosis and increased pigmentation ofeyelashes and adjacent hair in the region of the ipsilateraleyelids of patients treated with unilateral topical latanoprost.Am J Ophthalmol 1997;124:544–547.
5. Kook MS, Lee K. Increased eyelid pigmentation associatedwith use of latanoprost. Am J Ophthalmol 2000;129:804–806.
Post-traumatic EndophthalmitisInvolving Clostridium tetani andBacillus sppMohan N. Iyer, MD, George Kranias, MD, andMichael E. Daun, MD
PURPOSE: To report a case of post-traumatic infectiousendophthalmitis caused by Clostridium tetani and Bacil-lus spp.METHODS: Case report.RESULTS: A 25-year-old man developed endophthalmitisafter a traumatic corneoscleral laceration of his right eyeby a concrete reinforcement bar. He underwent parsplana lensectomy and vitrectomy with aspiration of vit-reous fluid and a conjunctival swab for cultures. Culturesfrom the conjunctival swab were negative for organisms.Cultures of the vitreous aspirate were positive for Bacil-lus species and C. tetani. He had received a tetanustoxoid booster at the emergency department. By the timethe culture results became available, he had developedsevere eye pain associated with marked orbital conges-tion, increased swelling and erythema of the lids, markedinjection and chemosis of the conjunctiva, and subse-quently underwent evisceration. The inflammation re-solved after evisceration of the right eye, and he wasdischarged to home on doxycycline 100 mg orally twotimes daily for 10 days.CONCLUSION: We are unaware of previous reports ofendophthalmitis involving C tetani and could find nonein a computerized MEDLINE search. Patients withpenetrating eye injury should be assessed for tetanusimmunization status, and early intervention with tetanustoxoid booster and/or tetanus immune globulin should beconsidered if cultures are positive. (Am J Ophthalmol2001;132:116–117. © 2001 by Elsevier Science Inc.All rights reserved.)
Accepted for publication Dec 6, 2000.From the Departments of Internal Medicine (Dr Iyer) and Ophthal-
mology (Drs Kranias and Daun, The Christ Hospital, Cincinnati, Ohio.Inquiries to Michael E. Daun, MD, Department of Ophthalmology,
The Christ Hospital, 2139 Auburn Ave, Cincinnati, OH 45219; fax:(513) 287-6403.
AMERICAN JOURNAL OF OPHTHALMOLOGY116 JULY 2001