Herpes simplex type-1 virus infection
15
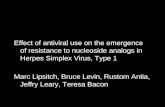
Clinical Practice Guidelines The scope ot oral medicine practice and practitioner competencies is evoijtiorary in nature. This section ol Quintessence International is cnmrnitted to presenting evidenced-based olinical practice guidelines in collaboration with oral and nonoral health care providers. Herpes simplex type-1 virus infection Michaeli A. Huber, Oral infection caused by the herpes simplex virus represents one ot the more oommon conditions the den- tal practitioner will be oalied upon to manage. Unique in its ability to eslablish iatency and undergo subse- quent recurrence, it is an ubiquitous intectious agent for which a cure does not exist. For the immunocom- petent patient, herpes virus simplex infection typicaiiy represents nothing more than a nuisance. However, for the immunooompromised patient, this infection is associated with increased morbidity and mortality. Recentiy introduced antiviral drug regimens may reduce the morbidity and potential mortality of the herpes simplex virus, especiaiiy in immunocompromised patients. The value of antivirai therapy in the manage- ment of recurrent herpes simplex virus infection in the immunocompetent patient remains an area of con- tentious debate. (Quintessence Int 2003:34:453-467) ETIOLOGY AND EPIDEMIOLOGY Of the more than 80 berpes viruses, at least eigbt are known to infect man.' An important feature common to all tbe buman berpes viruses is tbeir ability to estab- lisb latency in tbe bost.--" Both herpes simplex type-1 (HSV-l) and herpes simplex type-2 (HSV-2) are re- sponsible for primary oral herpes simplex infections, with HSV-l accounting for 75% to 90% of cases."" Transmission occurs via direct contact with contami- nated secretions from an infected individual.'^'^' Of the half million new cases per year in the United States,'* most occur in children between tbe ages of two and tbree years of age. While prevalence rates as high as W/o have been reported, age-specific preva- lence rates appear to be decreasing in industrialized countries. In one survey, 40'>/o of those studied be- tween the ages of 25 and 29 years had positive serol- ogy to HSV, and antibody prevalence rates increased 'Assistant Professor, University ot Texas Health Science Center at San Antonio, Dental School, Division of Oral Medicine, Sari Antonio, Tenas. Reprint requests; Dr Michaeii A. Huber, University of Texas Health Science Center at San Antonio, Dental Sctiool, Division of Oral Medicine, Mail code 7919, 7703 Floyd Curl Drive, San Antonio, TX 78239-3900. E-rnail:[email protected] 1.5% per year up to tbe age of 50.-' Witb sucb bigb prevalence rates, it is clear tbat the vast majority (over 90%) of primary exposures result in either asympto- matic or mildly symptomafic illness.= ' *>^^ CLINICAL MANIFESTATIONS Primary herpetic gingivostomatitis Tbe most commonly observed clinical manifestation of primary HSV infection is primary acute herpetic gingivostomatitis. After an incubation period of 1 to 26 days, initial nonspecific signs and symptoms of moderate to high fever, malaise, irritability, headache, and cervical lymphadenopatby occur.-'i'''^^" Witbin 1 to 3 days, tbe cbaracteristic findings of widespread vesicular eruptions and gingival inflammation are evi- dent. The vesicles affect any intraoral mucosal surface {buccal mucosa, bard/soft palate, floor of the mouth, tongue, gingiva, tonsillar pillars, pharynx) and rupture within a few days to produce painful, small, round, shallow ulcers (Figs 1 to 6). Often, lesions coalesce to fortn larger ¡rregular-shaped ulcérations. New vesicles may erupt and break down for 3 to 5 days, but gradual healing, without scarring, occurs within 1 to 2 weeks. Quintessence International 453
Transcript of Herpes simplex type-1 virus infection

Clinical Practice Guidelines
The scope ot oral medicine practice and practitioner competencies isevoi j t iorary in nature. This section ol Quintessence International iscnmrnitted to presenting evidenced-based olinical practice guidelines incollaboration with oral and nonoral health care providers.
Herpes simplex type-1 virus infectionMichaeli A. Huber,
Oral infection caused by the herpes simplex virus represents one ot the more oommon conditions the den-tal practitioner will be oalied upon to manage. Unique in its ability to eslablish iatency and undergo subse-quent recurrence, it is an ubiquitous intectious agent for which a cure does not exist. For the immunocom-petent patient, herpes virus simplex infection typicaiiy represents nothing more than a nuisance. However,for the immunooompromised patient, this infection is associated with increased morbidity and mortality.Recentiy introduced antiviral drug regimens may reduce the morbidity and potential mortality of the herpessimplex virus, especiaiiy in immunocompromised patients. The value of antivirai therapy in the manage-ment of recurrent herpes simplex virus infection in the immunocompetent patient remains an area of con-tentious debate. (Quintessence Int 2003:34:453-467)
ETIOLOGY AND EPIDEMIOLOGY
Of the more than 80 berpes viruses, at least eigbt areknown to infect man.' An important feature commonto all tbe buman berpes viruses is tbeir ability to estab-lisb latency in tbe bost.--" Both herpes simplex type-1(HSV-l) and herpes simplex type-2 (HSV-2) are re-sponsible for primary oral herpes simplex infections,with HSV-l accounting for 75% to 90% of cases.""Transmission occurs via direct contact with contami-nated secretions from an infected individual.'^'^' Ofthe half million new cases per year in the UnitedStates,'* most occur in children between tbe ages oftwo and tbree years of age. While prevalence rates ashigh as W/o have been reported, age-specific preva-lence rates appear to be decreasing in industrializedcountries. In one survey, 40'>/o of those studied be-tween the ages of 25 and 29 years had positive serol-ogy to HSV, and antibody prevalence rates increased
'Assistant Professor, University ot Texas Health Science Center at SanAntonio, Dental School, Division of Oral Medicine, Sari Antonio, Tenas.
Reprint requests; Dr Michaeii A. Huber, University of Texas HealthScience Center at San Antonio, Dental Sctiool, Division of Oral Medicine,Mail code 7919, 7703 Floyd Curl Drive, San Antonio, TX 78239-3900.E-rnail:[email protected]
1.5% per year up to tbe age of 50.-' Witb sucb bigbprevalence rates, it is clear tbat the vast majority (over90%) of primary exposures result in either asympto-matic or mildly symptomafic illness.= '*>^
CLINICAL MANIFESTATIONS
Primary herpetic gingivostomatitis
Tbe most commonly observed clinical manifestationof primary HSV infection is primary acute herpeticgingivostomatitis. After an incubation period of 1 to26 days, initial nonspecific signs and symptoms ofmoderate to high fever, malaise, irritability, headache,and cervical lymphadenopatby occur.-'i'''^^" Witbin 1to 3 days, tbe cbaracteristic findings of widespreadvesicular eruptions and gingival inflammation are evi-dent. The vesicles affect any intraoral mucosal surface{buccal mucosa, bard/soft palate, floor of the mouth,tongue, gingiva, tonsillar pillars, pharynx) and rupturewithin a few days to produce painful, small, round,shallow ulcers (Figs 1 to 6). Often, lesions coalesce tofortn larger ¡rregular-shaped ulcérations. New vesiclesmay erupt and break down for 3 to 5 days, but gradualhealing, without scarring, occurs within 1 to 2 weeks.
Quintessence International 453

Huber
The pain associated with primary herpetic gingivo-sfomatitis may adversely affect the patient's ability toeat, swallow, and speak,^"''"' In the immunocompro-mised patient, a primary HSV infection may be moresevere and persistent, and death due to aggressivelocal spread or dissemination to the lungs or brainmay occur,™' Conditions that predispose to dissemi-nation include immunologie immaturity, malignancy,malnutrifion, pregnancy, organ transplantation, burns,corticosteroid therapy, and autoimmune deficiencysyndrome (AIDS), «^«- '- '
Recurrent iierpes
One of the more perplexing hallmarks of HSV is itsability to establish latency and undergo future reacfi-vation. During primary oral infection, the virus istransported via retrograde axonal transport to regionalsensory ganglia where it establishes latency in neu-ronal cell bodies. While laicnt, the virus exists in anonreplicating immunologically shielded state in theneuron,^'' The most frequent site of latency for HSV-1is the trigeminai ganglion,^^ but other potential sitesinclude the nodosa ganglia of the vagus nerve, dorsalroot ganglia, sympathetic ganglia, and brain,** Viral re-activation does not always result in clinical recur-rence, as evidenced by the fact that asymptomafic viralshedding has been observed in 2% to 9% of the at-riskpopulation. The impact of asymptomatic viral oralshedding on disease transmission remains unclear,^'*-'
Numerous well-documented trigger factors are as-sociated with HSV recurrence. They include sunlight,trauma, menstruation, fever, immunosuppression, de-compression of the trigeminai nerve, and irritation bydental instruments.'^^''^^"''' While it has been postu-lated that individuals who respond to stress with moreemofion arc more prone to recurrence, the commonlyheld belief that stress predisposes the pafient to recur-rence has not been confirmed through controlledstudies,^"-^''""" Ciearly, much remains to be deter-mined concerning the understanding of the homeosta-tic dynamic of primary infection, latency, and reactiva-tion of HSV.
Recurrent infecfions are esfimated to occur in 15%to 40% of individuals harboring latent HSV'^*''' Threeclinical forms of recurrence are recognized: recurrentherpes labialis (RHL), intraoral recurrence, and recur-rence mimicking a primary infection. RHL is clearlythe most predominant form, with an estimated 100 mil-fion cases occurring each year,'' ^^ RHL typically pre-sents as a focal clustering of vesicles affecting the lipvermilion or some other perioral site such as the skinor ala of the nose (Figs 7 and 8). The vesicles quicklyrupture and coalesce to form the characteristic crustingulcer. Patients usually relate a prodrome of pain, hum-
ing, tingling, or itching prior to tbe clinical appearanceof the recurrence, Intraorai recurrence follows a pat-fern of presentafion similar to that of RHL except thelesions arc intraorai, occur on keratinized mucosa(palate or gingiva), and crusting does not occur (Fig 9),The pain associated with intraorai herpes may interferewith eafing and speaking. In the immunocompetent pa-fient, recurrent lesions resolve uneventfully within twoweeks. Rarely, a recurrent infection affecting the im-munocompetent patient may mimic a primary infec-fion,^^ In the immunocompromised pafient, recurrencetends to be more severe, widespread, and prolonged.For such a patient the clinical appearance often mimicsa primary infection.'' '**''"'*
DIAGNOSIS
Differentiai diagnosis
The diagnosis of both primary and recurrent HSV in-fections is typically derived from the history and clini-cal presentation. However, other stomatologie muco-cutaneous diseases should be considered in thedifferential diagnosis (Table 1), Recurrent aphthousstomatitis (RAS) is often misdiagnosed as a HSV infec-fion. This is most likely to occur with the uncommonherpetiform variant of RAS. However, RAS typicallydoes not have a prodrome of fever and malaise, thereis no associated gingival erythema, and the ulcérationsalmost universally occur on movcablc oral mucosa.
Varicella zoster virus (VZV) infection (chiciien pox)may manifest oral ulcérations similar to an HSV infec-fion. However, the presence of the characteristic pru-rific crusfing skin erupfions establishes the correct di-agnosis. Infrequently, an infraoral recurrent VZVinfecfion (zoster) may occur, but the dramafic unilat-eral distribution and intense pain help distinguish itfrom an HSV recurrence. Hand-foot-and-mouth dis-ease is disfinguished by the characteristic presence oflesions affecting the oral cavity, feet and hands.Likewise, herpangina is characterized by oral ulcéra-tions limited to the soft palate, uvula, tonsils, and pos-terior pharyngeal wall.
Laboratory testing
Tzanck smear. The Tzanck smear is a rapid and inex-pensive diagnostic aid. A sterile scalpel blade is usedto unroof a vesicle, and the base of the vesicle is gen-tly scraped to obtain the specimen. The specimen issmeared on a glass slide, allowed to air dry, andstained with Giemsa or Wright's stain in preparationfor histologie interpretafion,=* Characteristic multinu-cleated epithefial cells with intranuclear inclusions
454 Voiume 34, Number 6, 2003

• Huber
Figs 1 to 6 Primary herpefic gmgivcstomatitis affecting a 29-yeai-old *hife man
Quintessence International 455

Huber
Fig 7 ;ñ,-c,..ri..-;-itwoman (day 1).
aîïccting a 32-year-old white Fig 8 Recurrent herpes labiaüs affecting a 32-year-oio' whitewoman (day 4).
Fig 9 intraorai recurrent herpes simpiex, secondary to anes-thetic injection into the greater palatine foramen.
TABLE 1 Differential diagnosis of oral HSVInfection
Dtfterentjal diagnosis
Herpetiform recurrentapthous stomatitis
Ha nd-loot-and-mouthdiseaseHerpangina
Pemphigus
Erythema muitiforme
Intraoral zoster
Necrotising uicerativegingivitis
Pertinent findings
Clustered, small, shaliow ulcérationsaffecting free orai mucosa, recurrent, nofeverAphthouslike oral ulcérations or lesionson hands and feefBandlike oral ulcération atfecting softpaiate, uvula, tonsils, and posteriorpharyngeal wallEpitheliai sloughing aftecting any oraltissue, fetor oris, positive Nikolsky's sign.possible skin lesionsPolymorphous oral lesions ranging fromvesicles or bullae, charaoterislic targetlesions on skinVesicular eruption to the midline, severepain, skin lesions possibiePiery red gingiva, interproximai necrosiswith crater formation, hypersalivation.halitosis, malaise, low grade fever
Fig 10 Tzanck smear demonstrating cytopatholcgic effect cfHSV.
signify a positive result (Fig 10). Cytology cannot dis-tinguish between HSV-1 and HSV-2, and interpreta-tion is highly variable with positive results noted inonly 50% of cases.5' '''5'í- s
Serology. Serologie testing for HSV is often avail-able, btit the time necessary to obtain the final resultlimits its relevance in clinical practice. Indirect im-munofluorescence is utilized to compare HSV anti-body levels within the first 3 days of infection to thosepresent 1 month later. A four-fold increase of HSVspecific IgG is consistent with a recent infection.^
Viral culture. Herpes simplex virus isolation in tissueculture demonstrates a high degree of both sensitivityand specificity, but the time required to obtain resultslimits its usefulness. A fresh vesicle fluid specimen is
456 Voiume 34, Number 6, 2003

• Huber
carefully obtained and placed in viral transportmedium, transported to tbe lab, and inoculated intoViral growtb medium. After 24 to 48 hours, the culturescan he examined for viral-specific cytopathic eflect.«"^^
Polymerase chain reaction <PCR). Pclymerasechain reaction represents the current state of the artfor establishing the presence of HSV in lesion speci-mens, but it is labor intensive, expensive, and not uni-versally available." Due to its high specificity and sen-sitivity, PCR can be utilized to detect low-level HSVshedding prior to tbe onset of a clinically apparent le-sion.^ Results are avaiiabie witbin 24 bours, and spe-cial transport medium is not required to transport tbespecimens to the lab.'"-'
Consuitations
Extraoral involvement of herpes simplex, especially inthe immuocompromised patient warrants a multidisci-phnary approacb to management. Evidence of any ex-traoral involvement or dissemination warrants appro-priate medical consultation or referral.
Ophthaimoiogy. Herpes simplex virus infection isthe most frequent cause of corneal blindness in theUS. An ophthalmologic examination should be ob-tained if there is any evidenee or suspicion of herpeskeratitis, as noted by ocular pain, visual impairment,chemosis, or conjunctivitis.^-
Dermatology. A dermatology consultation is indi-cated with the presence of cutaneous lesions, such ashepetic whitlow or eczema herpeticum."'''^'^'^'"'^^''For a small but significant group of patients, recurrentherpes simplex is associated with erythema mulitforme(EM). Herpes simplex-associated erythema multiforme(HAEM) typically develops within three weeks of her-petic infection and may recur after a herpetic recur-rence. It has been estimated that over öO /o of all casesof erythema multiforme are associated with herpessimplex recurrence.'"^^-^'
Neuroiogy. Herpes simplex virus remains the singlemost common cause of sporadic encephalitis world-wide. HSV-2 is most frequently associated witb neonatalencephalitis, while HSV-1 is most often associated withencephalitis affecting children and adults. ^ Initial symp-toms may be nonspeeific and include headache, malaise,fever, and vomiting. The observance of signs and symp-toms of central nervous system involvement such as al-tered alertness, dysphasia, hemiparesis, visual fielddeficits, or seizure mandate immediate consultationwith neurology. In spite of proper therapy, only 40% ofsurvivors will have minimal or no sequelae. "••' • • •"Recent research has implicated HSV with Bell's palsy.^
Gastroenteroiogy. The occurrence of acute feverwith the sudden onset of pain and odynophagiashould raise the suspicion of herpes esophagitis and
warrants further evaluation. Most reported casesoccur in patients with immune compromise."«'^*
Infectious disease. Of particular concern for thedentist is reactivation of latent HSV in ¡mmunocom-promised individuals. In such patients, HSV lesionsmay be more extensive, persistent, and may lead to vis-ceral dissemination.2'i''i5"5wi,4-i,46,55,s6,5s Reactivationof latent HSV is a widely recognized cause of oral ul-cérations observed during cancer chemotherapy, bonemarrow transplantation, and antirejection drug tber-apy after organ transplantation,*''ä.25,2s,3W74ii.ei of partic-ular importance for the clinician, tbe clinical presenta-tion of recurrence in the immunocompromised patientmay be widespread, mimicking a primary HSV infec-tion or other ulcerative oral conditions, --"'' '"* Herpessimplex virus infection must be considered in the dif-ferential diagnosis for all oral ulcerative conditions af-fecting an immunocompromised patient.
PATiENT MANAGEMENT AND TREATMENT
Goais of treatment
There is currently no cure for HSV infection and itsestablishment of latency. For both primary and recur-rent cases, management is directed at (1) promotinglesion healing; (2) providing palliation; (3) ensuringadequate food and fluid intake; and (4) preventing fur-ther viral spread. The best tberapy for HSV is depen-dent on the clinician's sound evaluation of both theclinical presentation and patient's overall health. Forexample, the management of RHL affecting a healthyskier will differ greatly from the management of a per-sistent RHL affecting an AIDS patient. In the former,the clinician is essentially dealing with an annoyance,whereas in the latter, the clinician may be dealing witha potentially life-tbreatening condition.
Evidence to support drug ttierapy
Evidence to support drug tberapy for HSV bas im-proved in the last two decades, in large part becauseof the need to identify effective therapies for genitalherpes and HSV infections in the growing immuno-compromised patient population. For such patients,specific antiviral protocols, particularly with acyclovir,have been sbown to demonstrate a clear therapeuticbenefit and have been incorporated into standardpractice.' •'' • "•"••'" •"• ' Studies addressing the use ofantiviral therapy to treat orofacial HSV in the im-munocompetent patient have yielded mixed and, altimes, contradictory results.' •" '•'''• -™ For this reason,specific protocols for the use of antivirals in dentistryrepresents an area of dynamic review.
Quintessenoe Inlernationai 457

Huber
TABLE 2 FDA status of some drugs to treat RHL»"
Acyclovir ointment 5%
Penciclovir cream 1%
Approved only for immunocom-promised patientsApproved
Acyclovir capsules and tablets Not approvedFamciolovir tabletsVal acyclovir cap lets
Approved for HIV-infected onlyApproved
initiation of therapy
Supportive and palliative therapy is indicated for allpatients suffering primary berpetic gingivostomatitis.Antivirai therapy should be considered for any case ofHSV affecfing an immunocompromised patient due totbe increased risk of complications sucb as persis-tence, encephalitis, and systemic spread.
Choice of drugs for primary fierpes
Primary line of treatment. Tbe treatment of mildcases of primary herpetic gingivostomatitis is directedat relieving oral discomfort and improving tbe pa-tient's ability to eat and drinii. The patient is in-structed in the importance of maintaining proper by-dration, nutrition, and hygiene.^^•^^•'' A topicalanestbetic agent mixed witb kaopectate used as anoral rinse for 2 minutes before eaeb meal is prescribed,as is an antipyretic/analgesic to relieve fever and oralpain. When topical anestbetic agents sucb as dycio-nine or lidocaine are used, patients are cautionedabout the potential for a reduced gag reilex and tbeneed for caution wbile eating and drinking to avoidairway compromise.'' In addition, the use of topical li-docaine in pédiatrie patients has been associated withan increased risk of seizure."- For patients unable toeat and drink comfortably, nutritional supplements areadded to the above regimen. Over the counter prod-ucts such as Ensure Plus and Carnation InstantBreakfast should be taken 3 to 5 times per day.''Hospitalization is rarely necessary. Tbe benefit or ne-cessity of antiviral therapy in treating primary oralherpes in tbe immunocompetent patient bas not beenclearly establisbed.""-'^''''
Secondary line of treatment. For tbe immunocom-promised patient {ie, AIDS, organ transplant recipient,cbemotherapy patient, etc), antiviral therapy should beadded to the treatment regimen. Systemic acyclovirtherapy, botb parenteral and oral, accelerates tbe reso-lution of viral shedding, reduces pain, and reducestime to healing."** Acyclovir is generally well tolerated,but intravenous infusion is associated with an in-creased risk of reversible renai toxicity due to crys-talline nepbropathy. Tbis complication is most likely
to occur in situations of bigb-dose bolus infusion, de-bydration, or preexisting renal disease. Otber adverseeffects include nausea, vomiting, ligbt beadcdness, di-apboresis, and rash.''^'^ For intravenous administra-tion, tbe regimen is 5 mg/kg (infused over 1 bour}every 8 bours for 5 to 10 days. A generally acceptedoral regimen is 400 mg taken 3 to 5 times per day for
Tertiary line of treatment. For immunocompro-mised patients wbo are either intolerant to acycloviror fail to improve with acyclovir therapy, foscarnettherapy should be initiated. ^ Acyclovir treatment fail-ure is usually associated witb HSV infections causedby thymidine kinase-deficient strains of HSV."*"'' -'Foscarnet does not require activation via pbospboryla-tion by viral tbymidine kinase. It is active againstHSV-l, HSV-2, VZV, cytomegalovirus (CMV), in-fluenza A and B, bepatitis B virus (HBV), and HIV«Foscarnet causes potentially fatal renal impairment inmore than 25% of patients.-*"' Adequate hydration iscritical, as is proper monitoring and dose adjustmentto minimize toxicity. Other adverse reactions includepronounced electrolyte imbalances, seizures, anemia,neutropenia, fever, nausea, vomiting, diarrhea, andheadache. Induction therapy typically consists of 40mg/kg every 8 to 12 hours for 14 to 21 days.''^"
Choice of drugs for recurrent herpes
Primary line of treatment. For patients whose RHL isclearly related to ultraviolet (UV) light exposure, lipbalms and lotions viitb a sun protective factor (SPF)of at least 15 are useful for preventing sun-inducedberpes labialis.""'*" Recurrent herpes labialis, thoughpainful and sometimes unsightly, is self-limiting andoften docs not require treatment. Proper hygiene to re-duce transmission and autoinnoculation should be en-forced and palliation with cocoa butter ointment,lanolin-based lip preparations, or petrolatum mayprove beneficial." For patients desiring specific antivi-ral therapy, the Food and Drug Administration (FDA)has approved the use of two prescription antiherpeticagents {Tahle 2).
Topical penciciovir 1% cream (see DrugiMonograph) has been sbown to speed lesion healingand reduce pain.' *"'-*'' The cream should be applied tothe affected area during the initial prodrome and thenevery 2 hours while awake for 4 days.'' '* ' ''*' A pro-drug of acyclovir, oral valacyelovir (see Drug Mono-graph) has been sbown to reduce pain and speed le-sion bealing by about 1 day, wben patients take 2 g ofvalacyelovir at tbe onset of prodrome and 2 g 12hours later.*^
In wbat may seem to be a paradox, tbe FDA bas yetto approve tbe use of acyclovir and famciciovir for the
458 Volume 34, Number 6. 2003

Huber
treatment of RHL in the immunocompetent pafient.Several controlled studies have faiied to demonstrate aconsistent cost-effective benefit for acyclovir use in themanagement of recurrent HSV in the immunocompe-tent patient "•3766,68.71, 5 Furthermore, there is concernthe indiscriminate use of acyclovir, or any antiviraldrug for that matter, promotes the emergence of resis-tant HSV strains.'!"iwse purtunatcly, clinical diseasecaused by resistant strains of HSV appears to occurmainly in the immunocompromised,'*"'-^ However,newly released information may lead the FDA to re-consider its posifion on the use of acyclovir and famci-clovir in the management of RHL, In a recently pub-lished review evaluafing two parallel and independenttrials using acyclovir cream 5''.o to treat RHL, a signifi-cant one-half day reduction in lesion duration wasdemonstrated.^5 In another published report, pafientsgiven 500 mg of famciclovir, a prodrug of penciclovir,3 fimes a day for 5 days experienced a 2-day reductionin healing time compared to controls,'"
Finally, the novel agent docosanol was shown to re-duce RHL lesion duration in a recently publishedstudy,"' It has the distinction of being the first nonpre-scripfion over-the-counter antiviral drug approved forthe treatment of RHL. However, the validity of its trueanfiviral efficacy has been questioned, and furtherstudy is recommended,**
In addition to the above, a wide variety of otheragents have been reported to be efficacious In themanagement of RHL (Table 3). Further studies to vali-date the efficacy of these putative agents are necessarybefore a firm recommendafion regarding their use canbe made.
Secondary line of treatment. For the immunocom-promised, antiviral therapy has been shown to im-prove many healing parameters of recurrent HSV in-fection (loss of virus in lesion, reduced pain, andaccelerated lesion healing),^'"^ Topical acyclovir 5%ointment (see Drug Monograph) applied at prodrometo the affected area every 2 hours until resolution maybe sufficient to control RHL.'" For patients unrespon-sive to topical therapy, fhe use of oral famciclovir isindicated (see Drug Monograph). The recommendeddosage is 500 mg twice daily for 7 days, initiated atprodrome. In addition, the off-label use of oral acy-clovir (see Drug Monograph) has been shown to be ef-fective, "' ' ^ Since a variety of dosing regimens withoral acyclovir have been shown to be effective, theclinician should attempt to identify a regimen thatmaximizes clinical response and patient compliancewhile minimizing cost. For episodic therapy, theprompt (at the first prodromal symptom) administra-tion of oral acyclovir, 400-mg capsules 3 fimes per dayfor 10 days, may be sufficient. For patients who siifferfrequent recurrences, typically defined as more than
TABLE 3 Putative agents effective againstrecurrent herpes labialis
Ascorbic acid solution (ASCOXAL)""Ascorbic acid + citrus bioflavanoid labiets (Peridin-C)»Lysine™Herbai compounds^'Lithium carbonate"Foscarnet cream 3%''Topical undecylenic acid cream15%"Betadine oral painl^Balm mint extract (1% Lo-701)*'Aspirin^'Topical tetracaine^s
six episodes per year, chronic suppressive therapy withoral acyclovir, 400 mg 2 fimes per day, may preventrecurrence. Patients who suffer from HAEM may alsobenefit from acyclovir prophylaxis,'"•-'•s'
Tertiary iine of treatment. For immonuocompro-mised patients who are either intolerant to acycloviror are infected with an acyclovir resistant strain ofHSV, the treatment of choice is foscarnet
SUMMARY
tn spite of recent advances addressing the overall un-derstanding of the pathogenesis of HSV and availabletreatment modalifies for HSV, a cure remains elusive.For all cases, attenfion to proper nutrifion, hydrafion,and hygiene is a must. When indicated, preventivemeasures should be encouraged. The use of antiviralagents should be based on proven therapeutic indica-tions. For the immunocompromised pafient, antiviraltherapy significantly reduces the increased morbidityand mortality associated with HSV infection. For theimmunocompetent pafient, the benefit and necessityof antiviral drug therapy for the management of HSV,especiaiiy RHL, remains an area of contentious re-view. To date, topical penciclovir and oral valacyclovirare the only prescripfion antiviral agents approved bythe FDA for the treatment of RHL.
REFERENCES
1, Oakley C, Epslein JB, Sherlock CH. Reactivation of herpessimplex virTis. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1997;84;272-278.
2, Stewart JA, Reef SE, Peliett PE, Corey L, Whitley RJ. Herpesvirus infections in persons infected with human immunodefi-ciency virus. Clin Infec Dis I995;21(suppl l);S114-S120.
3, Greenberg MS, Herpes virus infections. Dent Clin NorthAm 1996;40:359-368,
Quintessenceinternationai 459

Huber
4. Corey L, Spear PG. Infections with herpes simplex vimses(First of two parts]. NEnglJ Med 1986;314:686-691.
5. Eversole LR. Intlammatory diseases of the mucous mem-branes. Part 1, Viral and fungal infections. J Calif DentAssoc 1994;22;52-57,
6. Miller CS, Danaher R], )acob RJ. Molecular aspects of her-pes simplex virus 1 latency, reactivation, and recurrence.Crit Rev Oral Biol Med 1998;9:541-562,
7. Rilcy LE. Herpes s imples virus. Semin Per inatol1998:22:284-292,
8. Corey L. First-episode, recurrent, and asymptomatic herpessimplex infections. J Am Acad Dermatol 1998; 18:169-172.
9. Epstein JB, Sherlock C, Page ]L, Spinelli J, Phillips GClinical study of herpes simplex virus infection in leukemia.Oral Surg Oral Med Oral Pathol 1990;70:38-43,
10. Vestey JP, Nroval M, Mucocutaneous infections with herpessimplex virus and their management. Clin Exp Dermatol1992; 17:221-237.
11. Spruance SL, Freeman D], Stewart fCB, et al. The naturalhistory of ultraviolet radiation-induced herpes simplex labi-alis and response to therapy with peroral and topical formu-lations of acyclovir, J Infect Dis 1991;163:728-734,
12. Merchant VA, Molinari JA, Sabes WR, Herpetic whitlow:Report of a case with multiple recurrences. Oral Surg OralMed Oral Pathol 1983;55:568-571.
13. Mcrtz GJ, Critchlow CW, Benedetti J, et al. Double-blindplacebo-eontrolled trial of oral acyclovir in first-episodegenital herpes simplex infection. J Am Med Assoc1984;252:1147-1151.
14. Mindel A, Weiler IVD, Faherty A, Sutherland S, Fiddian AP,Adler MW, Acyclovir in first attacks of genital herpes andprevention of recurrences, Genitouriu Mtd 1986;62:28-32.
15. Meyers JD, Treatment of herpes virus infections in the im-munocompromised host, Scand J Infect Dis SuppI 1985:47:128-136.
16. Wutzler P. Antiviral therapy of herpes simplex and varicella-zoster virus infections, lntervirology 1997;40:343-356.
17 Scott DA, Coulter WA, Biagioni PA, O'Neill HO, Lamey PJ.Detection of herpes simplex virus type 1 shedding in theoral cavity by polymerase chain reaction and enzyme-linlîedimmunosorbent assay at the prodromal stage of recrudes-cent herpes labialis. J Oral Pathol Med 1997;26:305-309.
18. Scott DA, Coulter WA, Lamey PJ, Oral shedding of herpessimplex virus type 1: A review. ) Oral Pathol Med 1997:26:441-447,
19. Rooney JF, Bryson Y, Mannix ML, et al. Prevention of ultra-violet-light-induced herpes lahiaüs by sunscreen. Lancet1991;338:14i9-1422.
20. Padgett DA, Sheridan JF, Dome J, Berntson GG, CandeloraJ, Glaser R. Social stress and the reactivation of latent her-pes simplex virus type 1, Proc Nati Acad Sei USA 1998;95:7231-7235,
21. Dalkvist ), Robins TB, Wahlin R, Bartsch E, Forsheck M.Herpes simplex and mood: A prospective study. PsychosomMed 1995;57:127-137
22. Bales JF. Viral encephalitis. Med Clin North Am 1993;77:25-42,
23. Christie SN, McCaughey C, Marley JJ, Coyle PV, Scott DA,Lamey PJ, Recrudescent herpes simplex infection mimick-ing primary herpetic gingivostomatitis, J Oral Pathol Med1998i27:8-10.
24. Siegel MA. Strategies for management of commonly en-cotintered oral mucosal disorders, ¡ Calif Dent AssocI999;27:21O-212,215,2!8-219,
25. Gold D, Corey L, Acyclovir prophylaxis for herpes simplexvirus infection. Antimicrob Agents Chemother 1987;31:361-367.
26. Lycke E. Virological aspects of herpes virus infections,Scand lnlect Dis 1985;(suppl 47¡:9-15,
27 Eversole LR, Viral infections of the head and neck amongHJV-seropositive patients. Oral Surg Oral Med Oral Patho!1992:73:155-163,
28. Eisen D, Essell J, Broun ER, Oral cavity complications ofbone marrow transplantation, Semin Cutan Med Surg1997; 16:265-272,
29. Saral R, Burns WH, Laskin OL, Santos GW, Lietman PSAeyclovir prophylaxis of herpes-simplex-virus infections. NEnglJMed 1981;305:63-67
30. Terezhalmy GT, Bottomley WK, Pelleu GB. The use ofwater-soluble bioflavanoid-ascorbic acid complex in thetreatment of recurrent herpes iabialis. Oral Surg Oral MedOral Pathol 1978:45:56-62.
31. Hicks ML, Terezhaimy GT Herpes virus hominis type 1: Asummary of structure, composition, growth cycle, and cy-topathogenic effects. Oral Surg Oral Med Oral Pathol 1979:48:311-318,
32. Corey L, Spear PG, Infections with herpes simplex viruses(Second of two parts). N Engl ¡ Med 1986;314:749-757,
33. Emmert DH. Treatment of common cutaneous herpes sim-plex virus infections. Am Fam Physician 2000 ;61 :1697-1704,1705-1706,1708.
34. Hijikata Y, Tsukamoto Y. Effect of herbal therapy on herpeslabialis and herpes genitalis. Biotherapy 1998:11:235-240.
35. Simmons A. An open-Iahel study conducted to evaluate theefficacy of Betadine cold sore paint . Dermatology1997:195(suppl2]:85-88,
36. Woo SB, Fu-Keung Lee S, Oral recrudescent herpes simplexvirus infection. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1997:83:239-243.
37. Kesson A. Use of aciclovir in herpes simplex virus infections,J Paediatr Child Health 1998:34:9-13.
38. Olick M, Goldman H. Viral infections in the dental setting:Potential eflects on pregnant HCWs. J Am Dent Assoc1993;124:79-85.
39. Amir J, Harel L, Smetana Z, Varsano 1, Treatment of herpessimplex gingivostomatitis with aciclovir in children: A ran-domised double blind placebo control led study, BMJ1997:314:1800-1803,
40. Laskaris G. Oral manifestations of infectious diseases. DentClin North Am I996;40:395-423,
41. Meyers JD, Wade JC, Mitchell CD, et al, Multieenter collab-orative trial of intravenous aeyclovir for treatment of muco-cutaneous herpes simplex virus infection in the immuno-compromised host. Am J Med 1982:73:229-235,
42. Stanberry LR, Floyd-Rcising SA, Connelly BL, Alter S],Gilchrist MJR, Rubino C, Myers MG, Herpes simplexviremia: Report of eight pédiatrie cases and review of theliterature. Clin Infect Dis 1994:18:401-407
43. Wade JC, McLaren C, Meyers JD, Frequency and significanceof acyclovir-resistant herpes siinplex virus isolated from mar-row transplant patients receiving multiple courses of treat-ment with acyelovir. J Infect Dis 1983:148:1077-1082.
460 Voiume 34, Number 6, 2003

• Huber
44. Reichart PA. Oral ulcérations in HIV infection. Oral Dis1997;3(stLppl 11S180-S1K2,
45. Heitndahl A. Prevention and managetiient of oral infectionsin cancer patients, Support Care Caticer 1999:7:224-228.
46. Itin PH, Latitenschiagcr S. Viral iesions of tiie mouth inHlV-infected patients. Dermatoiogy 1997;194:l-7
47. Lundgren G, Wiiczek H. Lonnqvist B, Lindhoim A, WahrenB, Ringden O. Acyclovir prophyia:^is in bonc marrow trans-plant patients. Scatid ) Inftct Dis Suppi 1985;47:137-144.
48. Nahata MC. Clinical use of antiviral drugs. Dnjg Inteli ClinPharm ¡987:21:599-405.
49. Keating MR. Antivirai agents for non-human immunodefi-ciency virus infections. Mayo Clin Proc 1999:74:1266-1283.
50. Redding SW, Montgotnery MT. Acyclovir prophyiaxis fororal herpes simplex virus infection in patients with honemarrow t ransplants . Oral Surg Oral Med Orai Pathol1989;67:680-683.
51. Sculiy C, Laskaris G, Pindborg J, Porter SR, Reichart P Oralmanifestations of HIV infection and liieir management. I.More common lesions. Oral Surg Orai Med Oral Pathol1991:71:158-166,
52. Cohen S, Wiliiamson GM. Stress atid infectious disease ir;humatis, Psyciiol Bui 1991,109:5-24.
53. Logan HL. Lutgendorf S, Hartwig A, Liliy J, Berberich SL.Immune, stress and mood mariters related to recurrent oralherpes outbreaks. Oral Surg Orai Med Orai Patiioi OraiRadiol Endod 1998;86:48-34.
54. Nahass GT, Goidstein BA, Zhu WY, Serfiitig U, Pcnneys NS,Leonardi CL, Comparison of Tzanck smear, viral culture,and DNA diagnostic methods in detection of herpes sim-plex and varicel la-zoster infection, J Am Med Assoc1992:268:2541-2544.
55. Patton LL, van der Horst C. Oral infections and other mani-festations of HIV disease. Infect Dis Clin North Am 1999:13:879-900.
56. Ramos-Gomez F|, Flaitz C. Catapano P, Murray P, ivlilnesAR, Dorenbaum A. Ciassification, diagnostic criteria, andtreatment recommendations for orofacial manifestations inHlV-fnfected pédiatrie patients. ] Clin Pediatr Dent 1999;23:85-96,
57. Terezhalmy GT, Tyler MT, Ross GR. Eczema herpeticum:Atopic dermatitis complicated by primary herpetic gingivo-stomatitis- Oral Surg Oral Med Oral Pathol 1979;48:513-516.
58. Robayna MG. Harranz P, Rubio FA, Pena )M, Gonzaies J,Casado M. Destructive herpetic vviiitiow in AIDS: Report ofthree cases. Br J Dermatol 1997; 137:812-815.
59. Brice SL, Krzemien D, Weston WL, Huff JC. Detection ofiierpes simpiex virus DNA in cutaneous iesions of erythemamultiforme. J Invest Dermatol 1989:93:183-187
60. Lemak MA, Duvic M, Bean SE Oral acyclovir for the pre-vention of iierpes-associated erytliema multiforme. | AmAcad Dcrmatoi 1986:15:50-54.
61. Katz J, Livneh A, Shemer J, Danon YL, Peretz B, Herpessimplex-associated erythema multifortne (HAEM): A clini-cal therapeutic diiemma. Pediatr Dent 1999 ;21:359-362.
62 Noone ), Longe S. Bell's palsy in the primary care setting: Acase study. Clin Exceil Nurse Pract 1998;2:2O6-2I1.
63, Ashenburg C, Rothstein FC, Dahms BB. Herpes esophagitisin the immunocompetent child. J Pediatr 1986;108:584-587.
64 Matsumoto J, Sumiyoshi A. Herpes simplex esophagitis-Astudy in autopsy series. Am ] Clin Pathol 1985;84:96-99.
65. "Wade )C, Newton B, McLaren C, Flournoy N, Keeney RE,Meyers JD. Intravenous acyeiovir to treat mucocutaneousherpes simplex virus infectioti after marrow transpiantation.Ann Intern Med 1982:96:265-269.
66. Raborn GW, Martel AY, Grace MGA, McGaw WT. Oralacyclovir in prevention of herpes labiaiis. Oral Surg OralMed Oral Pathoi Orai Radiol Endod 1998:85:55-59.
67 Mindel A. Is it meaningful to treat patients with recurrentherpetic infections? Scand J Infect Dis SuppI 1991:80:27-32.
68. Raborn GW, McGaw WT, Grace M. Percy |. Treatment ofherpes iabialis with acyclovir. Review of three clinical trials.AmJ Med 1988;85:39-42.
69. Spruance SL, Nett R, Marbury T, Wolff R. Johnson J,Spaulding T. Acyclovir cream for treatment of herpes sim-plex labiaiis: Resuits of two randomized, doubie-biind, vehi-cle-eon trol i ed, multicenter ciinical triais Antimicrob AgentsChemother 2002 ;46.2238-2243.
70. Spruance SL, Rowe NH, Rayborn GW, Thibodeau EA,D'Ambrosio JA Bernstein DI. Peroral fameiclovir in thetreatment of experimental ultraviolet radiation-induced her-pes simplex iabialis: A double-blind, dose-ranging, placebo-controiled, multicenter trial. J Infect Dis 1999:179:303-310.
71. Siegei MA, Silverman S Ir, Soilecito TP (eds). Clinician'sGuide to Treatment of Common Oral Lesions, ed 5,Baltimore: American Academy of Oral Medicine, 2001.
72. Hess GP. Watson PD. Seizures secondary to orai viscous ii-docaine. Ann Emerg Mcd 1988;17:725-727
73. Wagstaff A], Fauids D, Goa KL. Aciciovir-A reappraisai ofits antivirai activity, pharmacokinetic properties and thera-peutic efficacy. Drugs 1994:47:153-205,
74. Hamuy R, Berman B. Treatment of herpes simples virus in-fections with topical antiviral agents. Eur ] Dermatol1998:8:310-319.
75. Lacy CF, Armstrong LL, Goldman MP, Lance LL. DrugInformation Handbook, ed 10. Hudson, OH: Lexi-Comp,2002.
76. Westheim AI, Tenser RB, Mariis JG, Acyclovir resistance ina patient with chronic mucocutaneous herpes simpiex infec-tion. J Am Acad Dermatol 1987; 17:875-880
77. Erlich KS, Mills j ; Chatis P, Merti GJ, Busch DF, FoilansbeeSE, Grant RM, Criimpaciœr CS. Acyclovir-resistant herpessimpiex virus infections in patients with the acquired im-munodeficiency syndrome. N EngI J Med 1989:320:293-296.
78. Chatis PA, Milicr CH, Schräger LE, Crumpacker CS.Successful treatment with foseamet of an acyclovir-resistantmucocutaneous infection with herpes simplex virus in a pa-tient with acquired immunodeficiency syndrome, N EngI JMed 1989;320:297-300.
79. lino T, Gondo H, Ohno Y, et ai. Suceessfui foscarnet ther-apy for mucocutaneous infection with herpes simplex virusin a recipient after unrelated bone marrow transpiant ation.Bone Marrow Transplant 1996:18:1185-1188.
80. Alrabiah FA, Sacks SL. New antiherpes vims agents, theirtargets and therapeutic potential Drugs 1996;52:17-32.
81. Sacks SL, Wiison B. Fameiclovir/penciclovir Adv Exp MedBioi 1999:458:135-147
82. Lazarus HM, Beianger R, Candoni A, ct ai. Intravenous pen-ciciovir for treatment of herpes simplex infections in im-mun ocom promised patients: Results of a multicenter, acy-clovir-controlled triai. Atitimicrob Agents Chemother1999:43:1192-1197
Quintessence International 461

Huber —
87.
Spruanee SL. Rowe NH. Raborn GW. Thibodeau EA.D'Ambrosio JA, Bernstein DI. Püroral famcielovir in thetreatment of experimental uitravioiet radiation-induced her-pes simplex labialis: A double-blind, dose-ranging, piacebocontrolied, muiticenter triai. J Infect Dis 1999;179:303-310.Boon R, Goodman JJ, Martinez J, Marks GL, Gamble M,Welch C. Penciciovir cream for the treatment of sunlight-in-duced herpes simplex lahialis; A randomized, double-blind,placebo-controiied triai. Pencielovir cream herpes labialisstudy group. Clin Ther 2000:22:76-90.Abramowicz M. Valvcyciovir (valtrex) for herpes labialis.Med Lett Drugs Ther 2002;44:95-98.Sande MA, Armstrong D, Corey L, et al. Perspectives onswitching oral acyclovir from prescription to over-the-counter status: Report ot a consensus panel. Clin Infect Dis1998:26:659-665.
Sacks SL, Thisted RA, Jones TM, et al. Clinical efficacy oftopieal docosanol 10% cream for herpes simplex labialis: Amuiticenter. randomized, placebo-controlled trial. J AmAcad Dermatol 2001;45:222-230.Spruance SL. N-docosanol (Abreva) for herpes lahialis:Prohlems and questions. J Am Acad Dermatul 2002;47:457-458.Hovi T. Hirvimies A. Stenvik M, Vuola E. Pippuri R. Topicaltreatment of recurrent mucocutaneous herpes with ascorbicacid-containing solution. Antiviral Res 1995;27:263-27Ü.
90. Wright EF. Clinical effectiveness ot lysine in treating recur-rent aphthous ulcers and herpes labialis. Gen Dent1994:42:40-42.
91. Bschor T. Compiete suppression of recurrent herpes labialiswith iithium carbonate. Pharmacopsychiatry 1999:32:158.
92. Bernstein Dl, Schleupner CJ, Evans TG, et al. Effect of fos-carnet cream on experimental UV radiation-induced herpeslabialis. Antimicrob Agents Chemother 1997:41:1961-1964.
93. Shafran SD. Sacks SL, Aoki FY, et al. Topical undecylenicacid for herpes simplex labialis: A muiticenter, placebo-con-trolied trial. J Infect Dis 1997:176:78-83.
94. Koytchcv R, Aiken RG, Dundarov S. Balm mint extract (Lo-701] for topical treatment of recurring herpes labiaiis.Phytomedicine 1999:6:225-230.
95. Karadi I, Karpati S, Romics L. Aspirin in the management ofrecurrent herpes simplex virus infection. Ann Intern Med1998;128:696-697
96. Kaminester LH, Pariser RJ, Pariser DM, et al. A double-blind, placebo-controlled study of topicai tetracaine in thetreatment of herpes labiahs. J Am Acad Dermatol 1999:41:996-1001.
97 Whitley RJ, Levin M, Burton N, et al. Infections caused hyherpes simpiex virus in the immunocompromised host:Natural history and topieai acyciovir therapy. J Infect Dis1984:150:323-329.
462 Volume 34, Number 6, 2003

• Huber
RECURRENT HERPES LABIALIS: R, PENCICLOVIR
Penciclovir ¡s a topical antivira! agent. It is a guanine nucleoside analogue structurally related to acy-clovir. In HSV-1 or HSV-2 infected cells, viral thymidine kinase phosphorylates penciclovir to amonophospi^ate form. Cellular kinases then convert the monophosphatB form to penciciovir triphos-phate. Penciclovir triphosphate competes with deoxyguanosine triphosphate to be incorporated intonew viral DNA by HSV poiymerase. leading to replication inhibition. Penoiclovir is iess potent thanacyclovir, but Its triphosphate form attains higher concentrations in HSV-infected cells, and it persistsmuch longer in the cell than acyclovir triphosphate. Pregnancy risk factor B.
1. Indications
2. Contraindications
3. Drug interactions
4. Ad tn i ti i strati on(route and dosage)
5. Monitored efficacyand toxicity
6. Length oftreatment
7. Cessation oftreatment
8. Instructions tothe patient
•Topical treatment of recurrent herpes simplex labiaiis.
• Previous adverse reactions to tamciclovir or penciclovir.* Hypersensitivity to the drug or any of its components.
• No significant drug interactions known.
• Topical: Apply cream to atlected area at tirst sign or symptoms of herpes labialis (ie, tingling,buming. itching, etc) and then every 2 fiours while awake for 4 days.
• Dosage form: 1% cream.
• Reduced viral shedding and pain, lesion resolution, and negative virai culture lor HSV.
• 4 days.
• No tapering necessary.
• Begin use at first prodromai symptom of recurrent herpes labiaiis.• Avoid contact with eyes.•VJash bands before and after appiication.• Report any sign of adverse reaction.• Penciciovir does not cure HSV.
For additional information, please review the manufacturer's recommendations.
Quintessence International 463

• Huber
RECURRENT HERPES LABIALIS: R. VALACYCLOVIR
Valacyclom Is the L-valyl ester of acyclovir. It is rapidiy absorbed after oraf ingestion and convertedby intestinai and hepatic enzymes Into aoyciovir. Its mechanism of action is identical to tíiat of acy-clovir. Pregnancy risk factor B.
1. Indications
2. Contraindications
3. Drug interactions
4. Administration(route and dosage)
5. Monitored efficacyand toxicjty
6, Length oftreatment
7, Cessation oftreatment
8, Instructions to thepatient
•Treatment of recurrent herpes iabiaiis in patients at least 12 years old,
' Hypersensitivity to vaiacyciovir, acyciovir, or any component ol its tormulation,
• Decreased renal clearance noted with cimetidine or probenecid. No dosage adjustmentneeded in patients with normai tenai function.
' Oral: Take 2 g by mouth at first prodromai symptom of recurrent herpes labialis and thentake 2 g by mouth 12 hours iater.
> Dosage forms: 500 mg capiet, 1000 mg capiet,
• Efficacy: Reduced viral shedding and pain, lesion resolution, and negative viral culture forHSV.
•Toxicity: Seizures, somnoience, confusion, eievated serum creatinine, renal failure,
• 1 day.
• No tapering necessary.
• Begin use at first prodromai symptom of reourrent herpes labialis,• Report any signs of adverse reaction,• Valacyclovir does not cure HSV,
For additional information, please review fhe manufacturer's recommendations.
464 Voiume 34. Number ß, 2003

• Huber
RECURRENT HERPES LABIALIS: R« FAMCICLOVIR
Famcidovir is a prodrug ot antivirai penciclovir. its mechanism of action is identicai to that of penci-dovir. After absorption, it is rapidiy biotranshrmed to the active drug penoiotovir Pregnancy risi< fac-tor B.
1. Indications
2. Contraindications
3. Drug interactions
4. Administration(route and dosage)
5. Monitored efficacyand toxicity
6. Length oftreatment
7. Cessation oftreatment
8. Instructions to tnepatient
• Treatment ot recurrent mucocutaneous herpes simpiex [ntections in HiV-infected patients.
> Previous adverse reactions to famciclovir or penciclovir or any component of its formation,
' Concurrent use of cimetidine, prcbenecid, or theophyiine may resulf in increased plasmalevels of penciciovir,
• Oral: Initiate therapy at first prodromal symptom. Take 500 mg by mouth twice daily for 7days.
• Di3sage forms' 125 mg tablet, 250 mg tablet, 500 mg tablet.
• Efficacy: Reduced viral shedding and pain, lesion resolution, and negative viral culture forHSV,
• 7 days.
• No tapering necessary.
• Begin use at first prodromal symptom of recurrent herpes labialis.• Report any signs of adverse reaction,• Famciclovir does not cure HSV.
For additional information, please review the manufacturer's recommendations.
Quintessencelnternationai465

ORAL HERPES SIMPLEX INFECTION: R. ACYCLOVIR
Acyeiovir is a guanine nudeoside analogue effective against i^SV-1, HSV-2. variceiia-zoster i/irus(VZV), and cytomegaiovirus (CMV). In tiie infected ceiis, virai tiiymidine i<inase piiospiiorylates acy-eiovir to acyclovir monophosphate, which then is converted to acyclovir triphosphate by other ceiiu-iar enzymes. Acyeiovir triphosphate inhibits DNA synthesis and virai replication by competing withdeoxyguanosine triphosphate tor incorporation by virai poiymerase into virai DNA. Pregnancy risi<factor B.
1. Indications
2. Contraindications
3. Drug interactions
4. Adrninistration(route and dosage)
5. Monitored efficacyand toxicity
6. Length oftreatment
7. Cessation oftreat tnent
8. Instructions to thepatient
'Treatment ot primary and recurrent mucocutaneous herpes in immunocomprotnised pa-tients.
• Hypersensitivity to acyclovir or any compon9nt of its formulation.
• Increased cenlral nervous system side effects with zidovudine or probenicid.
• Oral:
• Episodic therapy—Initiate therapy promptly al earliest symptom of prodrome ¡400 mg 3times per day for 10 days],
•Chronic suppressive therapy—400 mg 2 times daily.• Topical: Apply ointment liberally to recurrent lesion every 3 hours 6 times per day for 7
days.• Intravenous: 5 mg/kg every 8 hours for 7 days. Bolus administration must be avoided.
Administration must take placo over 1 hour and be accompanied by adequate hydration toreduce the risk of renal toxicity.
• Dosage forms: 5% ointment: 200 mg capsules; powder for injection (500 mg [10 mL], 1000mg |20 mL]); oral suspension (200 mg/5 mL}.
• Efficacy: Reduced viral shedding and pain, lesion resolution, and negative viral culture forHSV
•Toxicity: Seizures, somnolence, confusion, elevated serum creatinine, renal lailure.
• 7 to 10 days for episodic treatment, indefinite for chronic suppressive treatment.
• No tapering necessary.
• Begin use at first prodromal symptom ol recurrent herpes labialts.• Avoid contact with eyes.• Wash hands before and atter application,• Report any signs of adverse reaction,• Acyclovir does not cure HSV.
For additionai information, please review the manufacturer's recommendations.
466 Volume 34. Number 6, 2003

• Huber
ORAL HERPES SIMPLEX INFECTION: R, FOSCARNET
Foscarnet is an inorganic anaiogue which acts as a noncompetetive inhibitor against many PNA andDNA poiymerases, as well as i-liV reverse transcriptase. it is not dependent on virai thymidine iii-nase for activation. Its use is associated with a high incidence of renai impairment and serum andeiectroiyte imbalances. These potentiaiiy fatai reacfions render foscarnet a second-iine drug of iastresort. Pregnancy risi< factor category C.
1. Itidications
2. Contraindications
3. Drug interactions
4. Administration(route and dosage)
5. Monitored efficacyand toxicity
6. Length oftreatment
7. Cessation oftreatment
8. instructions to thepatient
• Treatment of primary and recurrent muoooutaneous harpes in immunocompromisedpatients who are either intolerant to acyclovir or in whom treatment has failed.
• Hypersensitivity to toscarnet: creatine clearance (CI J under 0.4 mL/minute/kg duringtherapy.
• Increased risk of renal failure associated with concutrenf use of other nephrotoxic drugs,such as cyclosporin. aminoglycosides. pentamidine. and amphotericin B. Concurrent usewith ciprofloxadn increases seizure risk.
• Dosage form: injection 24 mg/mL (250 mL. 500 mL)•Intravenous drug therapy—40 mg/kg every 8 to 12hoursfor 14 to21 days.
• Meticulous monitoring of renal function and electroiytes and appropriate dosage adjust-ment is criticai to minimize toxicity.
• Efficacy: Reduced viral shedding and pain, lesion resolution, and negative viral culture torHSV.
• Toxicity: Seizures, somnoience. confusion, elevated serum creatinine, renai failure, elec-trolyte imbalances.
• 14 to 24 days for episodic treatment: indefinite for chronic suppressive treatment.
• No tapering necessary.
• Report any signs of adverse reaction.• Report any numbness in extremeties, paresthesias. or perioral tingling.• Foscarnet does not cure HSV.
For additional information, please review the manufacturer s recommendations.
Ouintessenoe International467