HEREDITARY OPTIC NEUROPATHIES GEORGE PAPANIKOLAOU SINGLETON HOSPITAL SWANSEA.
28
HEREDITARY OPTIC NEUROPATHIES GEORGE PAPANIKOLAOU SINGLETON HOSPITAL SWANSEA
-
Upload
eunice-hood -
Category
Documents
-
view
216 -
download
1
Transcript of HEREDITARY OPTIC NEUROPATHIES GEORGE PAPANIKOLAOU SINGLETON HOSPITAL SWANSEA.
HEREDITARY OPTIC NEUROPATHIES
GEORGE PAPANIKOLAOU
SINGLETON HOSPITAL
SWANSEA
CLASSIFICATION
• MONOSYMPTOMATIC
• FAMILIAL NEUROLOGIC SYNDROMES
• MULTISYSTEM DISEASE
1:10,000-1:50,000
PATTERN OF INHERITENCE
• AD
• AR
• X-linked
• Mitochondrial
Difficulties:
• Different genotype same phenotype
• Same genotype different phenotype
• Single cases
Molecular diagnosis
DIFFERENTIAL DIAGNOSIS
• Primary retinal degenerations (CONE dystrophy)
• Toxins
• Infiltration/ compression
• MS
• Atrophic papilloedema
• Paraeoplastic
COMMON FEATURES
Primary loss of ganglion cells OA
• Bilat./ Symmetrical/ irreversible/ painless VA
• No RAPD
• Optic nerve pallor
• Colour vision defect
• VF
• ERG, VEP, PERG
• Onset: insidious (except LHON)/ congenital-late
• Intra-, inter- familial variability (EXAMINE family!!)
MONOSYMPTOMATIC OPTIC NEUROPATHIES
LEBER’S HEREDITARY OPTIC NEUROPATHY
Prevalence: 3.22/100.000
Age of onset: 15-35y BUT ANY AGE
Gender: male 80-90%
Visual loss: acute-subacute/ severe/ sequential 75% (2/12)
Pupillary light reaction relatively spared
MRI (STIR): signal mid/post, intraorbital ON, noCSF visible, CNS NAD
Blood test available

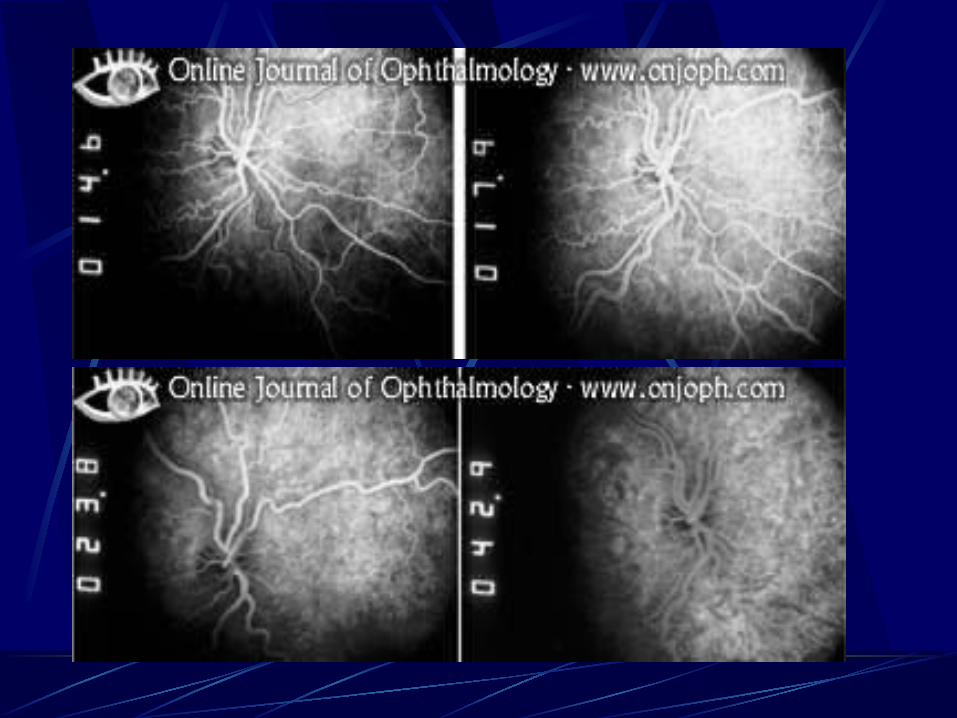
FUNDUS EXAMINATION (maternal relatives)
Circumpapillary telangiectasia
30-60%
Normal OA, all after 6/12
Pseudoedema
Absence of leakage in FFA
Consider diagnosis in any case of unexplained bilat. Opt. Neuropathy regardless of AGE, GENDER, FAMILY HISTORY, FUNDOSCOPIC APPEARENCE



ASSOCIATIONS
• Minor neurologic (MS-like)
• Leber’s plus
• Heart block (WPW, LGL) ECG
HEREDITY
• Primary mutations (90-95%)
11778: 40-90%
14484: 10-15%
3460: 8-15%
• Secondary mutations
Mitochondrial (maternal)
Complex I respiratory chain
Retina/ ON/ EOM: highly ATP dependent

PROGNOSIS
• Mutation
11778: 5% improve (3460)
14484: 60% improve
• Age (<20y)
AVOID:
Tobacco/ Alcohol
CN
Environmental toxins
DOMINANT OPTIC ATROPHY (DOA)
Prevalence:1:10000- 1:50000 (COMMONEST)
Age: within first 2 decades (4-6y)- UNAWARE
Inheritence: AD (3q- OPA1, 18q)
Penetrence:98%
Intra, interfamilial variability
No associated syndromes
Progress: insidious slow, stable
OPA1: NTG /Dynamin related GTP-ase/ inner mit. membrane

Clinical Features
VA: 6/6-PL (6/36)
Colour vision: tritan/ generalised dyschromatopsia
VF: +pseudobitemporal, + peripheral inversion of red-blue isopters
OA: subtle, temporal, entire disc
triangular excavation of temporal optic disc
MRI: signal+ visible CSF


AUTOSOMAL RECESSIVE OPTIC NEUROPATHY
• ISOLATED (very rare, ?DOA with incomplete penetrence)
• WOLFRAM’S SYNDROME (DIDMOAD
WFS-1 gene Chr. 4
Birth- 4y
• BEHR’S DISEASE
Infancy
• METHYLGLUTACONIC ACIDURIA (MGA)
OPA-3
X -LINKED HEREDITARY OPTIC NEUROPATHY
Very rare
Dutch pedigree
Slowly progressive
• other neurologic findings
• Deafness
• Retinopathy
OPA-2

FAMILIAL NEUROLOGIC SYNDROMES+ OA
SPINOCEREBELLAR ATAXIA
•ADCA+OA
Type I: brainstem signs
Type II: retinopathy (secondary OA)
Type III: cerebellum
SCA1, SCA2, SCA3, SCA6, SCA7
Later onset (2nd deacade), mild visual loss, ophthalmoplegia, ataxia, basal ganglia sympt.
• FRIEDRIECH ATAXIAS
AR/ 9q
Onset: 8-15y
Spinal degeneration+ peripheral neuropathy
OA (50%, not severe loss)
Ataxia
Loss of vibratory sensation
Extensor plantars

POLYNEUROPATHIES
• CHARCOT- MARIE-TOOTH
Onset: first two decades/ motor>sensory
AD: visual loss early childhood
AR: peripheral neuropathy in childhood
X-linked: hearing loss in infancy
Pes cavus
Foot deformities
Scoliosis
Wasting of distal extremities
Hearing loss/ OA (mild, subclinical)
• FAMILIAL DYSAUTONOMIA (RILEY-DAY)
AR/ Ashkenazi Jews
2nd decade
Polyneuropathy+autonomic dysfunction
Indiference to pain
Reduced lacrimation
Corneal scarring
OA (very common)

MULTISYSTEM DISEASE
>100
Usually AR but can be X-linked
Storage diseases and cerebral degenerations of childhood
• Mucopolysaccharidoses
• Lipidoses
• Krabbe’s
• Metachromatic leucodystrophy (MLD)(22, 50% OA)
• Adrenoleucodystrophy (X)
• Pelizaeus- Merzbacher(X)

• Cockayne (AR)
• Smith- Lemli- Opitz (AR)
• Zellweger (AR)
• Menkes (X)
• Canavan’s (AR)
• Hallerroden-Spatz (AR)
Quantitative chromosomal abnormalities
Cerebral palsy (10% OA)

Mitochondrial diseases of childhood
• Subacute necrotising encephalomyelopathy of Leigh
• MERRL
• MELAS
• CPEO
OA+other neurologic abnormalities in infant:
1. Very long chain fatty acids (ALD)
2. Aryl- sulfatase A levels (MLD)
3. Urine amino acids