Hepatitis c Rev

of 5
-
Upload
ahmed-abouelwafa -
Category
Documents
-
view
215 -
download
0
Transcript of Hepatitis c Rev
-
8/14/2019 Hepatitis c Rev
1/5
OCTOBER 2007 20(10) www.jaapa.com JAAPA 21
EARN CATEGORY I CME CREDIT by reading this article and the article beginning on page 42 and successfullycompleting the posttest on page 49. Successful completion is defined as a cumulative score of at least 70%correct. This material has been reviewed and is approved for 1 hour of clinical Category I (Preapproved) CME creditby the AAPA. The term of approval is for 1 year from the publication date of October 2007.
LEARNING OBJECTIVES Outline the epidemiology of hepatitis C, how it is transmitted, and what can be done to prevent it Describe the natural history, clinical presentation, and diagnosis of hepatitis C Discuss the standard of care for hepatitis C, how the disease is monitored, and what other
therapeutic options might become available
CME
Hepatitis C virus infection:A current reviewThe standard therapy for hepatitis C cures 40% to 50% of infections, but new treatmentsnow being studied in clinical trials may improve these numbers.
Douglas L. Senecal, PA-C; Joseph Morelli, MD
Hepatitis Cthe disease caused by infectionwith the hepatitis C virus (HCV)is the num-
ber one indication for liver transplantationand one of the most common causes ofchronic liver disease worldwide.1,2 HCV is a
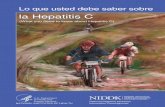
positive, single-stranded RNA virus in the Flaviviridae familythat is transmitted through parenteral exposure. The virusdirectly infects the hepatocyte yet is proposed to be noncyto-pathic; hepatic parenchymal damage occurs as a conse-quence of the hosts immune response and subsequent devel-opment of an inflammatory infiltrate, as seen in Figure 1.HCV was first isolated in 1989; before this occurred, sero-logic evaluation for the virus was impossible, leaving peopleexposed to blood products at risk for infection. Fortunately,testing techniques have now evolved to the point that evenvery small levels of virus can be detected. Eleven HCVgenotypes have been identified, with prevalence dependingon geographic location. In the United States, genotypes 1, 2,3, and 4 are most common, with genotype 1 comprising 75%of US infections.2,3
Todays standard therapy, pegylated interferon combinedwith ribavirin, offers an overall cure rate of approximately40% to 50%.4,5 However, specifically targeted antiviral thera-pies, such as the protease and polymerase inhibitors now inclinical trials, may improve on the current standard of care.Because hepatitis C is being diagnosed more frequently andthe treatment regimens are complex, PAs play an integralrole in providing care.
EPIDEMIOLOGY AND PREVENTION
The CDC has estimated that 3.9 million Americans havebeen exposed to HCV and that 2.7 million Americans have
active chronic HCV infection.2,3 An estimated 26,000 infec-tions are acquired each year, and the 10,000 to 12,000 yearlydeaths occur in those whose infections progress to cirrhosisor hepatocellular carcinoma (HCC).2,3 Risk factors for HCVtransmission that should prompt screening at the primarycare level are listed in Table 1 (page 22).
As with all infectious diseases, prevention of viral transmis-sion is key. Some experts have suggested that sharing tooth-
brushes and razors poses greater risk than does monoga-
FIGURE 1. This liver biopsy specimen from a patient with
chronic hepatitis C shows an inflammatory infiltrate around the
portal tract.
-
8/14/2019 Hepatitis c Rev
2/5
mous heterosexual intercourse. Sexual transmission hasundergone much scrutiny, however, as studies have quotedanywhere from 2% to 22% infection rates, depending onsexual practices.6,7 The American Association for the Studyof Liver Diseases (AASLD) states that sexual practices neednot be altered in monogamous heterosexual couples, as therisk of infection is minimal.6 However, advising couples touse barrier protection is reasonable.
NATURAL HISTORY
The natural history of HCV infection guides patient educa-tion and influences the decision of whether a patient shouldundergo therapy. In patients infected with HCV, 10% to 20%will have spontaneous clearance and chronic infection willdevelop in the other 80% to 90%.8 The chronic infection willprogress to cirrhosis (over a period of 20 to 30 years), inapproximately 20% to 30% of patients.8 The progression offibrosis is more rapid in patients who are older at the time ofinfection, nonwhite, infected with HIV, have hepatic steato-sis, or consume alcohol.9 Studies have shown that viral loaddoes not predict disease progression and can fluctuate as
22 JAAPA OCTOBER 2007 20(10) www.jaapa.com
CME Hepatitis Cmuch as one log in a days time, making this marker anunreliable gauge of disease progression.9 Serial testing ofquantitative HCV RNA is not recommended outside of thetreatment setting.
The natural history of patients with HCV-induced cirrho-sis is quite alarming. Once this condition has been diag-nosed, the risk is as high as 3.9% per year that decompensa-tion of underlying cirrhosis will occur and be accompanied
by HCC, ascites, bleeding from varices, jaundice, hepaticencephalopathy, or renal/pulmonary dysfunction.10 Fortu-nately, only 20% to 25% of all patients with cirrhosis willever decompensate and require transplantation.10 When de-compensation does occur, the overall 5-year survival is ap-proximately 50%, and recent studies show the major causeof death in this population to be HCC.10 Because the riskfor HCC is relatively high, screening patients with cirrhosisevery 6 to 12 months with abdominal imaging and alpha-fetoprotein levels is recommended.11,12
CLINICAL PRESENTATION AND DIAGNOSIS
Hepatitis C has historically been a silent disease, and mostpatients with acute infection do not present with the symp-toms or extrahepatic effects listed in Table 2. Patientswho have established cirrhosis are more commonly symp-tomatic because of the manifestations of advanced liverdisease.13
Acute hepatitis C The incubation period of HCV is 2 to26 weeks, and only about 20% of patients with acute HCVinfection develop clinical signs and symptoms.14 Serum HCVRNA has been found to be the most sensitive marker ofacute infection, and the level will be positive 7 days to 8weeks after infection (often well before antibody production
begins, which occurs approximately 50 days after infec-tion).14 Nevertheless, an HCV antibody test should beordered along with testing for HCV RNA to ensure that thepatient did not have pre-existing chronic hepatitis with anoth-er acute hepatitis superimposed. Acute HCV infection isdefined by a positive result on HCV polymerase chain reac-tion (PCR) testing two times in a row.15 Spontaneous clear-ance is represented by a negative result on PCR testing per-formed monthly for 3 months, along with formation ofHCV antibodies.15
Medical knowledge
Interpersonal & communication skills
Patient care
Professionalism
Practice-based learning and improvement
Systems-based practice
KEY POINTS Hepatitis C is the number one indication for liver transplantation and one of the most com-
mon causes of chronic liver disease worldwide.
Understanding the natural history of HCV infection is paramount because this understanding
guides patient education and influences therapy.
Most acute HCV infections go unnoticed; the viral incubation period is between 2 and 26 weeks,
and only about 20% of patients with acute infection develop clinical signs and symptoms.
The standard definition of chronic HCV infection is the persistence of HCV RNA in the serum
for longer than 6 months.
Therapy with pegylated interferon combined with ribavirin offers an overall cure rate of
approximately 40% to 50%; rates are higher for some genotypes of HCV. Specifically target-
ed antiviral therapies, now in clinical trials, may improve on the current standard of care.
COMPETENCIES
TABLE 1. Risk factors for hepatitis C
Birth to a mother with positive antibodies for HCV
Blood transfusion before 1992
Hemodialysis
History of cocaine use
History of tattoos
IV drug use
Multiple sexual partners
Needlestick or mucosal exposure (in a health care worker)
Organ transplant before 1992
Sex with an HCV-infected patient
Treatment with clotting factor for hemophilia before 1987
Unexplained elevations of liver enzymes
-
8/14/2019 Hepatitis c Rev
3/5
Continued on page 24
Chronic hepatitis C The standard definition ofchronicHCV infectionis the persistence of HCV RNA in the serumfor longer than 6 months. Initial HCV antibody testing isusually prompted by a history of risk factors or elevated liver
enzymes. Unfortunately, false-negative results are often seenin patients undergoing hemodialysis or in immunocompro-mised patients; furthermore, those who spontaneously clearthe virus will still produce antibodies to HCV.14 In eithercase, confirmatory testing with quantitative HCV RNAwould be preferred over a qualitative test because responseto therapy can be predicted based on viral load along withother factors such as HCV genotype.16
MANAGEMENT
In patients with acute infection, the benefits of treatmentalmost always outweigh the risk, but patients with confirmedHCV infection should be assessed for the relative barriers totreatment noted in Table 3. Next, the HCV genotype and
potential duration of infection should be determined; thisinformation will indicate whether obtaining a liver biopsy willyield information that will affect the decision to treat. Severalsubgroups of patients, such as those infected with genotypes 2or 3 and patients with clinical findings of cirrhosis, may notrequire liver biopsy as it will rarely influence management.Most would agree that patients infected with HCV genotypes2 and 3 should undergo therapy unless there are major barri-ers to treatment. On the other hand, patients infected withHCV genotype 1 with relative barriers to therapy may benefitfrom liver biopsy, which allows the provider to tailor the deci-sion to treat based on the histologic findings. For instance, apatient with advanced fibrosis on biopsy should have aggres-sive therapy to halt disease progression, whereas a patientwith minimal disease has the option of awaiting more effica-cious therapies with fewer side effects.
Some investigators are looking into the efficacy of measur-ing fibrosis using noninvasive methods. Serologic assays have
been found to be helpful only when fibrosis is either minimalor advanced; their predictive value for patients with middle-stage fibrosis is poor.17 Ultrasound elastography is currently
being investigated as another assessment tool, but factorssuch as body mass index and ascites appear to limit its sensi-tivity and specificity.18
Once the appropriate data have been considered and thedecision to treat has been made, patients should be coun-seled on treatment side effects and be reassured that all sideeffects will regress once medications are withdrawn. The sideeffects associated with pegylated interferon are fatigue, low-grade fever, myalgia, arthralgia, headache, hair loss, diarrhea,and weight loss. The side effects associated with ribavirin areheadache, pruritus, rash, and cough. These side effects canoften be minimized if the patient is premedicated with aceta-minophen and/or diphenhydramine and remains well hydrat-ed throughout therapy. The potential adverse events notedin Table 4 should be emphasized so the patient is aware ofassociated risks before committing to therapy.
OCTOBER 2007 20(10) www.jaapa.com JAAPA 23
TABLE 2. Signs and symptoms of hepatitis C
Anorexia
Arthralgia
Autoimmune thyroiditis
Essential mixed cryoglobulinemia
Fatigue
Leukocytoclastic vasculitis
Membranoglomerulonephritis
Myalgia
Nausea
Polyarteritis nodosa
Porphyria cutanea tarda
Right upper quadrant pain
TABLE 3. Relative barriers to treatment
Active substance abuse
Adherence issues
Baseline hematologic abnormalities
Established cirrhosis
Financial issues
Pre-existing autoimmune disease
Social support concerns
Uncontrolled psychiatric disease
Uncontrolled thyroid disease
TABLE 4. Adverse events associated with therapy
Anemia
Cardiac decompensation
Decompensation of underlying cirrhosis
Exacerbation of autoimmune disease
Exacerbation of thyroid disease
Neutropenia
Pancreatitis
Pulmonary toxicity
Retinal disease
Thrombocytopenia
Worsening psychiatric disease
-
8/14/2019 Hepatitis c Rev
4/5
Therapy Pegylated interferon is available in two forms,peginterferon alfa-2a, which is initiated at a fixed dosage of180 mcg/wk SC, and peginterferon alfa-2b, which is dosed at1.5 mcg/kg/wk SC. Contraindications to these agents include
decompensated cirrhosis, an absolute neutrophil count lessthan 1,000 cells/L, a platelet count less than 50,000 cells/L,severe depression, active substance abuse, retinopathy, anduntreated autoimmune or thyroid disease. For patients infect-ed with HCV genotypes 1, 4, 5, or 6, ribavirin is dosed at1,000 mg/d for those weighing less than 75 kg and at 1,200mg/d for those weighing more than 75 kg. For patients infect-ed with HCV genotypes 2 or 3, ribavirin is dosed at 800mg/d regardless of weight. Contraindications to ribavirin area hemoglogin less than 10 g/dL, coronary artery disease,renal insufficiency, and active or potential pregnancy. If preg-nancy might occur during or 6 months following therapy,two modes of contraception should be used.
The current AASLD guidelines for acute HCV infection
suggest treatment with full-dose pegylated interferon mono-therapy for 6 months after the patient has been given 2 to 4months to spontaneously clear the virus and has not doneso.19,20 With this therapy, rates of curecalled a sustained viro-logic response (SVR)have been cited at 81% to 91%.19,20
The current therapeutic regimen for chronic HCV infec-tion is derived based on genotype. For infection with HCV
24 JAAPA OCTOBER 2007 20(10) www.jaapa.com
CME Hepatitis Cgenotypes 1, 4, 5, or 6, the current regimen consists of pegy-lated interferon and weight-based ribavirin for 12 weeks, atwhich time HCV RNA should be measured to assess forearly virologic response (EVR) (EVR is defined as a two-log
drop from baseline). Should the patient achieve an EVR,then therapy should be continued for a total of 48 weeks.4,5
Those who have not achieved an EVR at 12 weeks have aless than 3% chance of achieving SVR and should be takenoff therapy.4,5 Once therapy is complete, HCV RNA testingis done to assess whether an end-of-treatment (EOT) re-sponse has been achieved; this is defined by a negative HCVRNA at the end of therapy. Lastly, HCV RNA should bemeasured 24 weeks later to assess for SVR. After 48 weeksof therapy, the estimated SVR for genotype 1 patients isapproximately 50%4,5 (see the algorithm).
For infections with HCV genotypes 2 or 3, the currentstandard of care is 24 weeks of pegylated interferon and non-weight-based ribavirin. HCV RNA is measured at EOT and
24 weeks after EOT to assess for SVR, which is achieved inapproximately 76% to 81% of patients.4,5
For treatment of patients with both hepatitis C and HIVinfection, the same regimens are used, bearing in mind thatthese patients have a lower SVR.21-23 Before treatment isstarted, HIV disease must be well-controlled, as evidenced
by suppressed viremia and a CD4+ cell count of greater
ALGORITHM. Treatment of hepatitis C
Check HCV RNA at EOT and 24 weeksafter therapy to assess for SVR
Key: EOT, end of treatment; HCV, hepatitis C virus; SVR, sustained virologic response.
HCV infection confirmed with HCV RNA
Determine HCV genotype and viral load
Genotypes 1, 4, 5, 6 Genotypes 2, 3
Treat for 12 wk with pegylated interferonand weight-based ribavirin
Treat for 24 wk with pegylated interferonand ribavirin, 800 mg/d
2 log drop
Continue therapy to48 wk
-
8/14/2019 Hepatitis c Rev
5/5
than 250 cells/L. In patients receiving highly active anti-retroviral therapy, screening for drug interactions beforetreatment and monitoring during treatment are essential.
Monitoring Baseline studies prior to therapy should include
a CBC with differential, AST, ALT, alkaline phosphatase,total bilirubin, albumin, thyroid-stimulating hormone, freethyroxine, prothrombin time/international normalized ratio,
beta-human chorionic gonadotropin in women, and quantita-tive HCV RNA with HCV genotyping. Once baseline valuesare established and therapy is initiated, patients should have
blood drawn for a CBC twice a week for the first 8 weeks; ifno cytopenia is noted, a monthly CBC should suffice. Every3 months, liver and thyroid function should be assessed.
Patients who experience aggressive cytopenia should beconsidered for dose reduction or treatment with epoetin alfaor filgrastim. A dose reduction of pegylated interferon is rec-ommended when the WBC count drops to less than 1,500cells/L or the absolute neutrophil count drops to less than
750 cells/L. Bone marrow stimulation with filgrastim is initi-ated when the WBC count drops to less than 1,000 cells/Lor the absolute neutrophil count drops to less than 500cells/L. The dosage of filgrastim is 300 mcg 1 to 3 timesweekly, depending on hematologic response, with a goal of anabsolute neutrophil count greater than 1,000 cells/L. Dosereduction of ribavirin is recommended when the hemoglobindrops more than 2 g/dL in a 4-week period. Bone marrowstimulation with epoetin alfa is initiated at 40,000 units andtitrated up to 60,000 units every 7 to 10 days, depending onresponse. Therapy is initiated if the hemoglobin drops to lessthan 11 g/dL or falls more than 3 g/dL from baseline. Thetarget hemoglobin is in the range of 10 to 12 g/dL.
POTENTIAL NEW THERAPIES
The most promising new therapies for hepatitis C are theprotease/polymerase inhibitors, which are currently undergo-ing clinical trials. Additional compounds being studied in-clude a ribavirin analog, taribavirin, to address the hemolyticanemia associated with standard ribavirin and longer-actinginterferon; and albumin-interferon alpha, which will offer
biweekly as opposed to weekly dosing of interferon.24,25
Although supporting data are limited, the clinician maysometimes find it appropriate to tailor therapy based on rapidvirologic response(RVR), defined as a negative HCV RNAafter 4 weeks of therapy.26 Some clinicians are using longercourses of therapy in patients with genotype 3 HCV infec-tion and a high viral load, or in patients with genotypes 1 or3 HCV infection who do not obtain an RVR. Studies to sup-port this have been done for genotype 1, but there are nodata for genotype 3.26 Additionally, shortening therapy ingenotype 2 and 3 patients who have an RVR has been ex-amined, but the data have yet to be evaluated and confirmedin large, controlled trials.27 JAAPA
Douglas Senecal and Joseph Morelli practice in the Department of
Hepatology, University of Florida College of Medicine, Gainesville. They have
indicated no relationships to disclose relating the content of this article.
OCTOBER 2007 20(10) www.jaapa.com JAAPA 25
DRUGS MENTIONEDAcetaminophen Peginterferon alfa-2a (Pegasys)Albumin-interferon alpha (Albuferon)* Peginterferon alfa-2b (PEG-Intron)Diphenhydramine Ribavirin (Copegus, Rebetol)Epoetin alfa (Epogen, Procrit) Taribavirin (Viramidine)*
Filgrastim (Neupogen) *Investigational agent
REFERENCES
1. Fattovich G, Giustina G, Degos F, et al. Morbidity and mortality in compensated cirrhosis type C:a retrospective follow-up study of 384 patients. Gastroenterology. 1 997;112(2):463-472.
2. Alter MJ, Kruszon-Moran D, Nainan OV, et al. The prevalence of hepatitis C virus infection in theUnited States, 1988 through 1994. N Engl J Med. 1999;341(8):556-562.
3. Armstrong GL, Alter MJ, McQuillan GM, Margolis HS. The past incidence of hepatitis C virusinfection: implications for the future burden of chronic liver disease in the United States.Hepatology. 2000;31(3):777-782.
4. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitisC virus infection. N Engl J Med. 2002;347(13):975-982.
5. Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared withinterferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial.Lancet. 2001;358(2986):958-965.
6. Stroffolini T, Lorenzoni U, Menniti-Ippolito F, et al. Hepatitis C virus infection in spouses: sexualtransmission or common exposure to the same risk factors? Am J Gastroenterol. 2001;96(11):3138-3141.
7. Vandelli C, Renzo F, Roman L, et al. Lack of evidence of sexual transmission of hepatitis Camong monogamous couples: results of a 10-year prospective follow-up study. Am JGastroenterol. 2004;99(5):855-859.
8. Alter MJ, Margolis HS, Krawczynski K, et al. The natural history of community-acquired hepatitisC in the United States. The Sentinel Counties Chronic non-A, non-B Hepatitis Study Team. N EnglJ Med. 1992;327(27):1899-1905.
9. Poynard T, Bedossa P, Opolon P. Natural history of liver fibrosis progression in patients withchronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet. 1997;349(9055):825-832.
10. Sangiovanni A, Prati GM, Fasani P, et al. The natural history of compensated cirrhosis due tohepatitis C virus: a 17-year cohort study of 214 patients. Hepatology. 2006;43(6):1303-1310.
11. Tanaka H, Nouso K, Kobashi H, et al. Surveillance of hepatocellular carcinoma in patients withhepatitis C virus infection may improve survival. Liver Int. 2006;26(5):543-551.
12. Fattovich G, Llovet JM. Risk factors for hepatocellular carcinoma in HCV-cirrhosis: what weknow and what is missing. J Hepatol. 2006;44(6):1013-1016.
13. Tong MJ, el-Farra NS, Reikes AR, Co RL. Clinical outcomes after transfusion-associated hepatitisC. N Engl J Med. 1 995;332(22):1463-1466.
14. Alter MJ. The detection, transmission, and outcome of hepatitis C virus infection. Infect AgentsDis. 1993;2(3):155-166.
15. Gerlach JT, Diepolder HM, Zachoval R, et al. Acute hepatitis C: high rate of both spontaneousand treatment-induced viral clearance. Gastroenterology. 2003;125(1):80-88.
16. EASL International Consensus Conference on Hepatitis C. Paris, 26-28 February 1999. Consensusstatement. European Association for the Study of the Liver. J Hepatol. 1999;30(5):956-961.
17. Imbert-Bismut F, Ratziu V, Pieroni L, et al; MULTIVIRC Group. Biochemical markers of liver fibro-sis in patients with chronic hepatitis C virus infection: a prospective study. Lancet. 2001;357(9262):1069-1075.
18. Ziol M, Handra-Luca A, Kettaneh A, et al. Noninvasive assessment of liver fibrosis by measure-ment of stiffness in patients with chronic hepatitis C. Hepatology. 2005;41(1):48-54.
19. Kamal SM, Fouly AE, Kamel RR, et al. Peginterferon alfa-2b therapy in acute hepatitis C: impactof onset of therapy on sustained virologic response. Gastroenterology. 2006;130(3):632-638.
20. Hwang SJ, Lee SD, Chan CY, et al. A randomized controlled trial of recombinant interferonalpha-2b in the treatment of Chinese patients with acute post-transfusion hepatitis C. JHepatol. 1994;21(5):831-836.
21. Thomas DL. Hepatitis C and human immunodeficiency virus infection. Hepatology. 2002;36(5)(suppl 1):S201-S209.
22. Graham CS, Baden LR, Yu E, et al. Influence of human immunodeficiency virus infection on thecourse of hepatitis C virus infection: a meta-analysis. Clin Infect Dis. 2001;33(4):562-569.
23. Chung RT, Anderson J, Volberding P, et al. Peginterferon alfa-2a plus ribavirin versus interferonalfa-2a plus ribavirin for chronic hepatitis C in HIV-coinfected persons. N Engl J Med. 2004;351(5):451-459.
24. Bain VG, Kaita KD, Yoshida EM, et al. A phase 2 study to evaluate the antiviral activity, safety,and pharmacokinetics of recombinant human albumin-interferon alfa fusion protein in geno-type 1 chronic hepatitis C patients. J Hepatol. 2006;44(4):671-678.
25. Balan V, Nelson DR, Sulkowski MS, et al. A Phase I/II study evaluating escalating doses ofrecombinant human albumin-interferon-alpha fusion protein in chronic hepatitis C patientswho have failed previous interferon-alpha-based therapy. Antivir Ther. 2006;11(1):35-45.
26. Snchez-Tapias JM, Diago M, Escartn P, et al; TeraViC-4 Study Group. Peginterferon-alfa2a plusribavirin for 48 versus 72 weeks in patients with detectable hepatitis C virus RNA at week 4 oftreatment. Gastroenterology. 2006;131(2):451-460.
27. Andriulli A, Dalgard O, Bjoro K, Mangia A. Short-term treatment duration for HCV-2 and HCV-3infected patients. Dig Liver Dis. 2006;38(10):741-748.