
Hepatic vein Doppler waveform changes in early stage (Child-Pugh A) chronic parenchymal liver...
5
Hepatic Vein Doppler Waveform Changes in Early Stage (Child-Pugh A) Chronic Parenchymal Liver Disease Kemal Arda, MD, Murat Ofelli, MD, Umit C ¸ alikoglu, MD, Tu ¨ lay Olc ¸ er, MD, and Turhan Cumhur, MD Abstract: Doppler waveform changes can be found in chronic parenchymal liver dis- ease, especially in the late stages. We investigated the contribution of Doppler ultra- sound in diagnosing early-stage chronic parenchymal liver disease. In this prospective study, 30 patients who had been diagnosed with chronic liver disease (Child-Pugh class A) and 30 healthy subjects were studied. The diagnosis was confirmed with histopathologic examinations of biopsy specimens in 17 patients. The Doppler US examination of hepatic veins was performed in all the patients and healthy subjects. The Doppler US pattern was classified into three groups according to the Doppler signal characteristics: (1) type 0, triphasic waveform, the presence of a short phase of reversed flow, (2) type I, decreased amplitude of the phasic oscillations without the short phase of reversed flow, and (3) type II, complete flat waveform. Normal hepatic vein waveforms (type 0) were found in 8 patients (26.66%) and abnormal hepatic waveforms (type I + type II) in 22 patients (73.33%). The results of Doppler ultrasonography were correlated with the diagnosis of early-stage chronic pa- renchymal liver disease (Child-Pugh class A). In all the subjects of the control group, the Doppler waveform of hepatic veins showed the triphasic pattern (type 0). In the statistical evaluation using Fisher’s exact test we observed that there was a significant difference (p < 0.05) between the control group and the patient group with respect to the presence of abnormal (type I + type II) Doppler waveform. The diagnostic accuracy in the patients who had biopsy was 76.47% and that in the patients who did not was 69.23%. © 1997 John Wiley & Sons, Inc. Indexing Words: Hepatic veins z Liver cirrhosis z Doppler ultrasound Cirrhosis is a chronic, diffuse, parenchymal liver disease defined as widespread hepatic fibrosis with nodule formation. In the late stages (Child- Pugh B and Child-Pugh C) of chronic parenchy- mal liver disease, definite ultrasonographic find- ings, such as echo coarseness or brightness, irregular outline, increased ultrasound attenua- tion, can be found. 1–3 In these stages, parenchy- mal fibrosis can alter the compliance of the wall of the hepatic veins, and this decreases and flattens phasic oscillations. 1 However, in the early stage of this disease (Child-Pugh class A), the value of ultrasonography and Doppler ultrasonography is controversial. Considering that fibrosis, a component of cir- rhosis, could alter hepatic vein waveform in early- stage chronic parenchymal liver disease (Child- Pugh class A), we evaluated the diagnostic value of image-directed Doppler ultrasonography in this stage of the disease. SUBJECTS AND METHODS We prospectively examined 30 patients (13 women and 17 men) between 18 and 64 years of age (mean age: 41 years) admitted to our hospi- tal for liver disease between June 1, 1994 and October 30, 1994. Thirty healthy volunteers (16 From the Department of Radiology, Ankara, Turkey. For re- print requests contact Kemal Arda, MD, Ilker 1. Cadde 14/2 Dikmen, 06460 Ankara, Turkey. J Clin Ultrasound 25:15–19, January 1997 © 1997 by John Wiley & Sons, Inc. CCC 0091-2751/97/010015-05 15 VOL. 25, NO. 1, JANUARY 1997
Transcript of Hepatic vein Doppler waveform changes in early stage (Child-Pugh A) chronic parenchymal liver...

Hepatic Vein Doppler Waveform Changes inEarly Stage (Child-Pugh A) Chronic
Parenchymal Liver Disease
Kemal Arda, MD, Murat Ofelli, MD, Umit Calikoglu, MD, Tulay Olcer, MD,and Turhan Cumhur, MD
Abstract: Doppler waveform changes can be found in chronic parenchymal liver dis-ease, especially in the late stages. We investigated the contribution of Doppler ultra-sound in diagnosing early-stage chronic parenchymal liver disease.
In this prospective study, 30 patients who had been diagnosed with chronic liverdisease (Child-Pugh class A) and 30 healthy subjects were studied. The diagnosis wasconfirmed with histopathologic examinations of biopsy specimens in 17 patients.
The Doppler US examination of hepatic veins was performed in all the patients andhealthy subjects. The Doppler US pattern was classified into three groups according tothe Doppler signal characteristics: (1) type 0, triphasic waveform, the presence of ashort phase of reversed flow, (2) type I, decreased amplitude of the phasic oscillationswithout the short phase of reversed flow, and (3) type II, complete flat waveform.
Normal hepatic vein waveforms (type 0) were found in 8 patients (26.66%) andabnormal hepatic waveforms (type I + type II) in 22 patients (73.33%). The results ofDoppler ultrasonography were correlated with the diagnosis of early-stage chronic pa-renchymal liver disease (Child-Pugh class A). In all the subjects of the control group,the Doppler waveform of hepatic veins showed the triphasic pattern (type 0).
In the statistical evaluation using Fisher’s exact test we observed that there was asignificant difference (p < 0.05) between the control group and the patient group withrespect to the presence of abnormal (type I + type II) Doppler waveform. The diagnosticaccuracy in the patients who had biopsy was 76.47% and that in the patients who didnot was 69.23%. © 1997 John Wiley & Sons, Inc.Indexing Words: Hepatic veins z Liver cirrhosis z Doppler ultrasound
Cirrhosis is a chronic, diffuse, parenchymal liverdisease defined as widespread hepatic fibrosiswith nodule formation. In the late stages (Child-Pugh B and Child-Pugh C) of chronic parenchy-mal liver disease, definite ultrasonographic find-ings, such as echo coarseness or brightness,irregular outline, increased ultrasound attenua-tion, can be found.1–3 In these stages, parenchy-mal fibrosis can alter the compliance of the wall ofthe hepatic veins, and this decreases and flattensphasic oscillations.1 However, in the early stageof this disease (Child-Pugh class A), the value of
ultrasonography and Doppler ultrasonography iscontroversial.Considering that fibrosis, a component of cir-
rhosis, could alter hepatic vein waveform in early-stage chronic parenchymal liver disease (Child-Pugh class A), we evaluated the diagnostic valueof image-directed Doppler ultrasonography inthis stage of the disease.
SUBJECTS AND METHODS
We prospectively examined 30 patients (13women and 17 men) between 18 and 64 years ofage (mean age: 41 years) admitted to our hospi-tal for liver disease between June 1, 1994 andOctober 30, 1994. Thirty healthy volunteers (16
From the Department of Radiology, Ankara, Turkey. For re-print requests contact Kemal Arda, MD, Ilker 1. Cadde 14/2Dikmen, 06460 Ankara, Turkey.
J Clin Ultrasound 25:15–19, January 1997© 1997 by John Wiley & Sons, Inc. CCC 0091-2751/97/010015-05
15VOL. 25, NO. 1, JANUARY 1997

women and 14 men) between 23 and 62 years ofage (mean age: 35.7 years) were also investigatedas a control group. The causes of the patients’admissions are summarized in Table 1.On physical examination, we found splenomeg-
aly in 17 patients (56.7%), hepatomegaly in 6 pa-tients (20%), palmar erythema in 1 patient(3.3%), and no significant physical findings in 8patients (26.7%).All patients were classified as class A by the
Child-Pugh classification system and no evidenceof decompensating liver disease was found. Onlyone patient (3.3%) had a bilirubin level greaterthan 2 mL/dL, an abnormal level.In all patients tested for hepatitis antibodies,
Hbs Ag was positive in 11 patients (36.7%), antiHbs Ag positive in 3 patients (10%), anti Hbc Agpositive in 7 patients (23.3%), anti HAV positivein 7 patients (23.3%), anti HCV positive in 3 pa-tients (10%), and anti Delta Ag positive in 2 pa-tients (6.7%).Chronic liver disease had been diagnosed by
clinical, biochemical, and ultrasonographic find-ings in all patients. In addition, liver biopsy underUS guidance was performed in 17 patients(56.7%). Histopathological examinations of thesespecimens indicated fibrosis in all cases. We di-agnosed chronic parenchymal liver disease usingthe following criteria: (1) the presence of ascites,hepatomegaly, splenomegaly, and internal echochanges in the liver; (2) the presence of the anglesign in the US examination; (3) disturbances ofliver function tests in biochemical examinations;(4) the presence of hepatitis markers in enzymeimmunoassay (EIA); and (5) high values of pro-thrombin time in hematological tests.Patients with signs of cardiac failure were not
included in the study because the Doppler wave-form of hepatic veins can be changed in such pa-tients. All patients had no clinical, radiologic, orsonographic evidence of cardiac failure, and theirECGs showed sinus rhythm.Ultrasonographic and image-directed Doppler
sonographic examinations were done with a con-vex 3.5–3.75 MHz probe and a 3.5–3.75 MHz
pulsed Doppler device (Toshiba Sonolayer 250SSA and 270 SSA scanners). Every patient wasexamined by US while supine after fasting over-night. The image-directed Doppler sonographicexamination of the hepatic veins was performedusing the method described by Bolondi.4
A sample volume, as large as at least 1⁄3 of thevessel’s diameter, was positioned within themiddle hepatic vein at a distance of 3 cm to 6 cmfrom the outlet into the inferior vena cava, keep-ing the angle of incidence of the Doppler ultra-sound beam between 20° and 50°. We asked thepatients to stop breathing at the end of a non-forced expiration and recorded at least 5 secondsof the trace. We used a wall filter of 100 Hz. Ul-trasonographic examinations were preformed inall patients by two radiologists.The Doppler US pattern was classified into one
of three groups according to the Doppler signalcharacteristics:1. Type 0; triphasic waveform, presence of a short
phase of reversed flow (two negative wavesand one positive or the opposite, depending onthe scan used) (Figure 1).
2. Type I; decreased amplitude of the phasic os-cillations without the short phase of reversedflow (Figure 2).
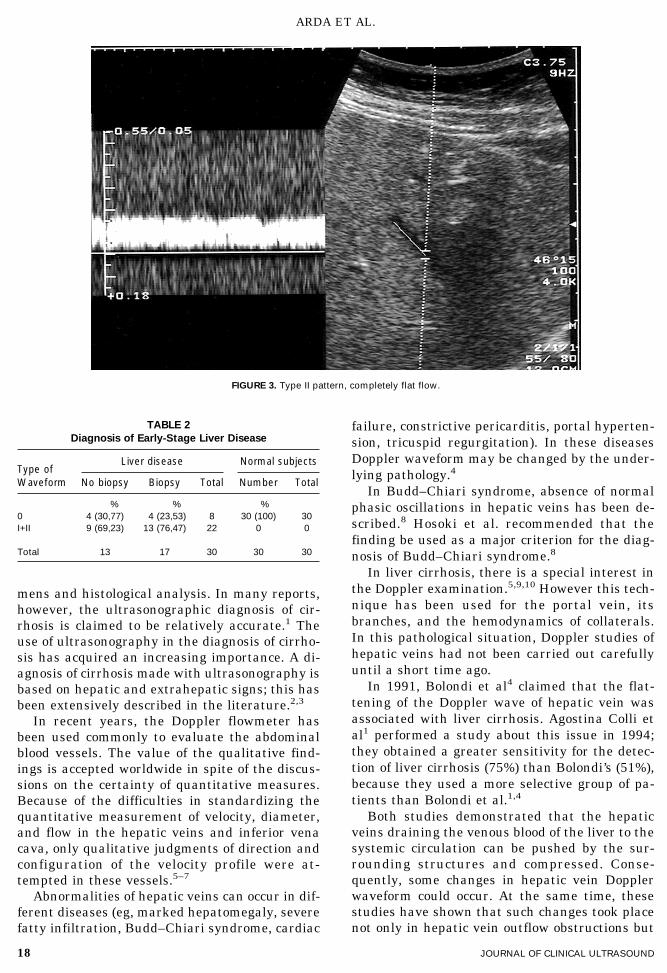
3. Type II: completely flat waveform without anyphasic oscillation (Figure 3).
The results were evaluated statistically usingFisher exact test.
RESULTS
In all the subjects of the control group (30 sub-jects, 100%) the Doppler waveform of hepaticveins showed the triphasic pattern (type 0). Nofalse positives were seen.In the research group, 8 patients of 30 (26.7%)
had normal hepatic waveforms (type 0), 22 of 30(73.3%) had an abnormal pattern; 18 patients of22 (81.8%) had type I and 4 of 22 (18.2%) had typeII waveforms.In all 17 patients who were examined with bi-
opsy, the results of histopathological examina-tions were chronic parenchymal liver disease. Inthe research group, 13 of 17 (76.5%) patients whohad been examined histopathologically had ab-normal hepatic waveforms; 12 of 13 (92.3%) pa-tients had type I and 1 of 13 (7.7%) had type IIwaveforms. The other 4 patients with histopath-ological evaluations of liver biopsy had normal he-patic waveforms.When compared statistically by using Fisher
exact test, it was observed that there was a sig-nificant difference (p < 0.05) between the control
TABLE 1
Clinical Characteristics
ComplaintNo. ofpatients Percent
%
Weakness 15 50.0
Haematemesis, melena 5 16.66
Nausea, vomiting, pyrosis 4 13.33
Abdominal distention, pain 4 13.33
Lower extremities edema 2 6.66
ARDA ET AL.
16 JOURNAL OF CLINICAL ULTRASOUND

group and the patient group (Child-Pugh class A)with respect to the presence of abnormal (type I +type II) Doppler waveforms. The diagnostic accu-racy of this waveform evaluation for the patientswith liver disease diagnosed histopathologicallywas 76.5% and for the patients who were diag-nosed by other methods was 69.2%. All statisticalresults are summarized in Table 2.
DISCUSSION
The basic pathological process characterizing cir-rhosis is an extensive collagen deposition with re-placement of hepatocytes and distortion of thenormal hepatic lobular architecture.The definition and classification of chronic
liver disease depend on adequate biopsy speci-
FIGURE 1. Doppler waveform shows normal triphasic pattern in hepatic vein (type 0).
FIGURE 2. Type I pattern, decreased amplitude of phasic oscillations without reversed flow phase.
HEPATIC VEIN DOPPLER ULTRASOUND
17VOL. 25, NO. 1, JANUARY 1997
mens and histological analysis. In many reports,however, the ultrasonographic diagnosis of cir-rhosis is claimed to be relatively accurate.1 Theuse of ultrasonography in the diagnosis of cirrho-sis has acquired an increasing importance. A di-agnosis of cirrhosis made with ultrasonography isbased on hepatic and extrahepatic signs; this hasbeen extensively described in the literature.2,3
In recent years, the Doppler flowmeter hasbeen used commonly to evaluate the abdominalblood vessels. The value of the qualitative find-ings is accepted worldwide in spite of the discus-sions on the certainty of quantitative measures.Because of the difficulties in standardizing thequantitative measurement of velocity, diameter,and flow in the hepatic veins and inferior venacava, only qualitative judgments of direction andconfiguration of the velocity profile were at-tempted in these vessels.5–7
Abnormalities of hepatic veins can occur in dif-ferent diseases (eg, marked hepatomegaly, severefatty infiltration, Budd–Chiari syndrome, cardiac
failure, constrictive pericarditis, portal hyperten-sion, tricuspid regurgitation). In these diseasesDoppler waveform may be changed by the under-lying pathology.4
In Budd–Chiari syndrome, absence of normalphasic oscillations in hepatic veins has been de-scribed.8 Hosoki et al. recommended that thefinding be used as a major criterion for the diag-nosis of Budd–Chiari syndrome.8
In liver cirrhosis, there is a special interest inthe Doppler examination.5,9,10 However this tech-nique has been used for the portal vein, itsbranches, and the hemodynamics of collaterals.In this pathological situation, Doppler studies ofhepatic veins had not been carried out carefullyuntil a short time ago.In 1991, Bolondi et al4 claimed that the flat-
tening of the Doppler wave of hepatic vein wasassociated with liver cirrhosis. Agostina Colli etal1 performed a study about this issue in 1994;they obtained a greater sensitivity for the detec-tion of liver cirrhosis (75%) than Bolondi’s (51%),because they used a more selective group of pa-tients than Bolondi et al.1,4
Both studies demonstrated that the hepaticveins draining the venous blood of the liver to thesystemic circulation can be pushed by the sur-rounding structures and compressed. Conse-quently, some changes in hepatic vein Dopplerwaveform could occur. At the same time, thesestudies have shown that such changes took placenot only in hepatic vein outflow obstructions but
FIGURE 3. Type II pattern, completely flat flow.
TABLE 2
Diagnosis of Early-Stage Liver Disease
Type ofWaveform
Liver disease Normal subjects
No biopsy Biopsy Total Number Total
% % %
0 4 (30,77) 4 (23,53) 8 30 (100) 30
I+II 9 (69,23) 13 (76,47) 22 0 0
Total 13 17 30 30 30
ARDA ET AL.
18 JOURNAL OF CLINICAL ULTRASOUND

also in liver parenchyma, in the presence of dif-fuse change.1,4
The pulsatility of the hepatic vein trace prob-ably reflects the macroscopic compliance of livertissue; pathological processes that change compli-ance will lower hepatic vein pulsatility. Bolondi etal showed that the underlying mechanism of thechange in the hepatic vein waveform could be re-lated to the amount of liver fibrosis, which pro-gressively reduces phasic oscillations in hepaticveins subsequent to a lack of compliance of thetissue, and even the hypertrophy of the hepaticcells might exert a possible compression on thehepatic vein because of the limited capacity of theliver capsule to stretch.1,4
In addition to Bolondi’s findings, we tried todemonstrate that these mechanisms could alsochange the hepatic vein Doppler waveform in theearly stage of chronic parenchymal liver disease.By adding ultrasonography and biochemical tests(the latter being insufficient for diagnosis in theearly stage [Child-Pugh class A] of diffuse paren-chymal liver disease), we tried to show that diag-nostic accuracy could be increased.Of the 17 patients diagnosed by liver biopsy, 4
(23.52%) had type 0, 12 (70.58%) had type I, and1 (5.88%) had type II Doppler waveforms. The his-tological, ultrasonographic, and biochemical find-ings of the 4 patients who had normal Dopplerwaveforms were not different from those of theother 13 patients’ waveforms.In hepatic vein Doppler US of 13 patients who
had not been examined histopathologically, 4 pa-tients (30.76%) had type 0, 6 (46.15%) had type I,and 3 (23.07%) had type II waveforms.There was no significant difference between
the hepatic vein Doppler waveform data in thepatients who had biopsy and in those who did not:22 of 30 (73.33%) chronic liver disease patientshad type I and type II, and 8 patients (26.66%)had type 0 waveforms. The diagnostic accuracywas 76.47% in the patients who had biopsy and69.23% in the patients who did not.Our findings showed that image-directed
Doppler ultrasonography, in conjunction with ul-
trasonographic and biochemical examinations,may be useful for the early-stage diagnosis ofchronic parenchymal liver disease.
ACKNOWLEDGMENT
We acknowledge the assistance of consultantstatistician S. Kenan Kose, Department of Biosta-tistics, Ankara University, Ankara, Turkey.
REFERENCES
1. Colli A, Cocciolo M, Riva C, et al: Abnormalities ofDoppler waveform of the hepatic veins in patientswith chronic liver disease. AJR 162:833–837, 1994.
2. Di Leio A, Cestari C, Lomazzi A, et al: Cirrhosis:diagnosis with sonographic study of the liver sur-face. Radiology 172:389–392, 1989.
3. Hess CF, Schmiedi U, Koebel G, et al: Diagnosis ofliver cirrhosis with US; receiver-operating charac-teristic analysis of multidimensional caudate lobeindexes. Radiology 171:349–351, 1989.
4. Bolondi L, Bassi S, Gaiani S, et al: Liver cirrhosischanges of Doppler waveform of hepatic veins. Ra-diology 178:513–516, 1991.
5. Ohnishi K, Saito M, Koen H, et al: Pulsed Dopplerflow as a criterion of portal venous velocity: com-parison with cineangiographic measurements. Ra-diology 154:495–498, 1985.
6. Dauzat M, Pamier LC: Portal vein blood flow mea-surements using pulsed Doppler and electromag-netic flowmetry in dogs: a comparative study. Gas-troenterology 96:913–919, 1989.
7. Barbara L: The value of Doppler US in the study ofhepatic hemodynamics: consensus conference Bo-logna, Italy 12 September 1989. J Hepatology 10:353–355, 1990.
8. Hosoki T, Kuroda C, Tokunda K: Hepatic venousoutflow obstruction: evaluation with pulsed Duplexsonography. Radiology 170:733–737, 1989.
9. Ohnishi K, Sato S, Pugliese D, et al: Changes ofsplanchnic circulation with progression of chronicliver disease studied by echo Doppler flowmetry.Gastroenterology 82:507–511, 1987.
10. Bolondi L, Gaiani S, Li Bassi S, et al: Diagnosis ofBudd–Chiari syndrome by pulsed Doppler ultra-sound. Gastroenterology 100:1324–1331, 1991.
HEPATIC VEIN DOPPLER ULTRASOUND
19VOL. 25, NO. 1, JANUARY 1997


















