Hemodialysis related induction of interleukin-6 production by peripheral blood mononuclear cells
7
Kidney International, Vol. 42 (1992), pp. 320—326 Hemodialysis related induction of interleukin-6 production by peripheral blood mononuclear cells BRUNO MEMOLI, CARMELO LIBETTA, TERESA RAMPINO, ANTONIO DAL CANTON, GIUSEPPE CONTE, GIUSEPPE SCALA, MARIA R. RuocCo, and VITT0RI0 E. ANDREUCCI Departments of Nephrology, 11 Faculty of Medicine, University of Naples and University of Catanzaro; Department of Nephrology, I Faculty of Medicine and Department of Biochemistry and Medical Biotechnology, II Faculty of Medicine, University of Naples, Italy Hemodialysis related induction of interleukin-6 production by periph- eral blood mononuclear cells. Interleukin-6 (IL-6) has a complex spec- trum of biological activities, for example, growth and differentiation of B cells and synthesis of acute-phase proteins by the liver. To evaluate the role of this cytokine in the inflammatory response induced by blood interaction with hemodialysis membranes, we have investigated the IL-6 synthesis and release in supernatant of 24-hour cultured peripheral blood mononuclear cells (PBMC) isolated from: (a) 10 hemodialyzed patients, (b) seven patients with advanced chronic renal failure (GFR slO mI/mm), and (c) eight healthy control subjects. In the same groups of subjects we evaluated the relationship between IL-6 synthesis and release and beta-2-microglobulin (f32m) production. Before and after dialytic treatment hemodialysis patient blood samples were drawn using the following criteria: (1) after two months of dialysis with cuprophan membranes, (2) after one and two months of dialysis with polymethyl- methacrylate (PMMA) membranes, and finally, (3) after one further month of dialysis with cuprophan membranes. IL-6 was determined after 72 hours of incubation of PBMC supernatant serial dilutions with IL-6-dependent hybridoma cell line, 7TD1. Compared to IL-6 synthesis in control subjects (6.0 5.6 U/3 x 106 PBMC/24 hr), hemodialyzed patients, when treated with cuprophan membranes, showed signifi- cantly higher value of IL-6 production both before (23 13 U13 X 106 PBMC/24 hr) and after (26.2 11.3 U/3 x 10 PBMC/24 hr) the dialytic session. When patients were hemodialyzed with PMMA membranes, at the start of dialysis IL-6 levels were not significantly different from values observed in healthy controls (10.6 4 U/3 x 10 PBMC/24 hr, after 1 month of dialysis and 7.8 U/3 x 106 PBMC/24 hr, after 2 months, respectively). When the patients were switched back to cuprophan membranes, IL-6 production was greatly increased after one month of dialysis (CU2, 44.6 9,4 U/3 x 106 PBMC/24 hr, at the start of dialysis) reaching values significantly higher than those obtained in the first period with cuprophan membranes. No difference was observed be- tween the values of IL-6 production obtained pre- and post-dialysis with cuprophan or PMMA membranes. IL-6 production values in uremic non-dialyzed patients were similar to values found in control subjects (8.6 6.4 U/3 x 106 PBMC/24 hr). f32m release showed a behavior quite similar to IL-6 throughout the study, In fact, a statistically significant linear relationship was obtained between j32m and IL-6 values of production (r = 0.8296, P < 0.001), In conclusion, our results show higher levels of IL-6 production in hemodialyzed patients treated with cuprophan membranes, thereby suggesting a chronic stimulation. j3m production is highly related to IL-6 production; this relationship sug- gests a possible implication for this cytokine in the pathogenesis of dialysis amyloidosis. Received for publication November 12, 1991 and in revised form March 25, 1992 Accepted for publication March 26, 1992 © 1992 by the International Society of Nephrology Blood interaction with hemodialysis membranes may result in the activation of circulating leucocytes and production of inflammatory cytokines [1—10]. These may account for both acute symptoms, such as fever and hypotension, and chronic disorders, such as muscle wasting, osteopenia, beta-2-micro- globulin (f32m) release and amyloidosis, in hemodialyzed pa- tients [11—18]. Several culprits have been suggested for cytokines induction during extracorporeal circulation, including complement acti- vation [19—22], bacterial contamination of dialysate [2, 6, 7, 23, 24], leucocyte adherence [25, 26], and acetate [27]. The type of dialysis membrane, however, seems to play a critical role because different membranes activate complement to a different extent, thus conditioning both cytokine and beta-2-microglob- ulin release [28—321. In the past few years, interleukin-6 (IL-6) has emerged as a monocyte/macrophage product regulating a complex spectrum of functions, including bone marrow stem cell proliferation, B lymphocyte differentiation and immunoglobulin secretion, T lymphocyte activation, acute phase protein induction, and release of other cytokines such as IL-i and TNF [33—39]. Recently, high plasma levels of IL-6 have been shown in uremic patients both on RDT and not yet treated with hemodialysis [40]. The specific effects of hemodialysis per se, and of different dialysis membranes on IL-6 release by peripheral leucocytes, however, have not yet been defined and were the object of the present study. In addition, we investigated the relation between IL-6 production and beta-2-microglobulin leucocyte synthesis and release. Methods Patients and control subjects We studied seven patients (4 male, 3 female; age 54.5 years; age range 38 to 61) with advanced chronic renal failure (GFR, evaluated with creatinine clearance 9.18 ml/min; range 7 to 10 mi/mm) and 10 hemodialyzed (HD) patients (6 male and 4 female; age 59.4 years; range 40 to 63). For at least one year prior to the study HD patients were dialyzed with cuprophan membrane dialyzers three times a week. Five patients used a bicarbonate bath for more than one year. 320
-
Upload
vittorio-e -
Category
Documents
-
view
212 -
download
0
Transcript of Hemodialysis related induction of interleukin-6 production by peripheral blood mononuclear cells

Kidney International, Vol. 42 (1992), pp. 320—326
Hemodialysis related induction of interleukin-6 production byperipheral blood mononuclear cells
BRUNO MEMOLI, CARMELO LIBETTA, TERESA RAMPINO, ANTONIO DAL CANTON,GIUSEPPE CONTE, GIUSEPPE SCALA, MARIA R. RuocCo,
and VITT0RI0 E. ANDREUCCI
Departments of Nephrology, 11 Faculty of Medicine, University of Naples and University of Catanzaro; Department of Nephrology, I Facultyof Medicine and Department of Biochemistry and Medical Biotechnology, II Faculty of Medicine, University of Naples, Italy
Hemodialysis related induction of interleukin-6 production by periph-eral blood mononuclear cells. Interleukin-6 (IL-6) has a complex spec-trum of biological activities, for example, growth and differentiation ofB cells and synthesis of acute-phase proteins by the liver. To evaluatethe role of this cytokine in the inflammatory response induced by bloodinteraction with hemodialysis membranes, we have investigated theIL-6 synthesis and release in supernatant of 24-hour cultured peripheralblood mononuclear cells (PBMC) isolated from: (a) 10 hemodialyzedpatients, (b) seven patients with advanced chronic renal failure (GFRslO mI/mm), and (c) eight healthy control subjects. In the same groupsof subjects we evaluated the relationship between IL-6 synthesis andrelease and beta-2-microglobulin (f32m) production. Before and afterdialytic treatment hemodialysis patient blood samples were drawn usingthe following criteria: (1) after two months of dialysis with cuprophanmembranes, (2) after one and two months of dialysis with polymethyl-methacrylate (PMMA) membranes, and finally, (3) after one furthermonth of dialysis with cuprophan membranes. IL-6 was determinedafter 72 hours of incubation of PBMC supernatant serial dilutions withIL-6-dependent hybridoma cell line, 7TD1. Compared to IL-6 synthesisin control subjects (6.0 5.6 U/3 x 106 PBMC/24 hr), hemodialyzedpatients, when treated with cuprophan membranes, showed signifi-cantly higher value of IL-6 production both before (23 13 U13 X 106PBMC/24 hr) and after (26.2 11.3 U/3 x 10 PBMC/24 hr) the dialyticsession. When patients were hemodialyzed with PMMA membranes, atthe start of dialysis IL-6 levels were not significantly different fromvalues observed in healthy controls (10.6 4 U/3 x 10 PBMC/24 hr,after 1 month of dialysis and 7.8 U/3 x 106 PBMC/24 hr, after 2 months,respectively). When the patients were switched back to cuprophanmembranes, IL-6 production was greatly increased after one month ofdialysis (CU2, 44.6 9,4 U/3 x 106 PBMC/24 hr, at the start of dialysis)reaching values significantly higher than those obtained in the firstperiod with cuprophan membranes. No difference was observed be-tween the values of IL-6 production obtained pre- and post-dialysis withcuprophan or PMMA membranes. IL-6 production values in uremicnon-dialyzed patients were similar to values found in control subjects(8.6 6.4 U/3 x 106 PBMC/24 hr). f32m release showed a behavior quitesimilar to IL-6 throughout the study, In fact, a statistically significantlinear relationship was obtained between j32m and IL-6 values ofproduction (r = 0.8296, P < 0.001), In conclusion, our results showhigher levels of IL-6 production in hemodialyzed patients treated withcuprophan membranes, thereby suggesting a chronic stimulation. j3mproduction is highly related to IL-6 production; this relationship sug-gests a possible implication for this cytokine in the pathogenesis ofdialysis amyloidosis.
Received for publication November 12, 1991and in revised form March 25, 1992Accepted for publication March 26, 1992
© 1992 by the International Society of Nephrology
Blood interaction with hemodialysis membranes may resultin the activation of circulating leucocytes and production ofinflammatory cytokines [1—10]. These may account for bothacute symptoms, such as fever and hypotension, and chronicdisorders, such as muscle wasting, osteopenia, beta-2-micro-globulin (f32m) release and amyloidosis, in hemodialyzed pa-tients [11—18].
Several culprits have been suggested for cytokines inductionduring extracorporeal circulation, including complement acti-vation [19—22], bacterial contamination of dialysate [2, 6, 7, 23,24], leucocyte adherence [25, 26], and acetate [27]. The type ofdialysis membrane, however, seems to play a critical rolebecause different membranes activate complement to a differentextent, thus conditioning both cytokine and beta-2-microglob-ulin release [28—321.
In the past few years, interleukin-6 (IL-6) has emerged as amonocyte/macrophage product regulating a complex spectrumof functions, including bone marrow stem cell proliferation, Blymphocyte differentiation and immunoglobulin secretion, Tlymphocyte activation, acute phase protein induction, andrelease of other cytokines such as IL-i and TNF [33—39].Recently, high plasma levels of IL-6 have been shown in uremicpatients both on RDT and not yet treated with hemodialysis[40]. The specific effects of hemodialysis per se, and of differentdialysis membranes on IL-6 release by peripheral leucocytes,however, have not yet been defined and were the object of thepresent study. In addition, we investigated the relation betweenIL-6 production and beta-2-microglobulin leucocyte synthesisand release.
Methods
Patients and control subjects
We studied seven patients (4 male, 3 female; age 54.5 years;age range 38 to 61) with advanced chronic renal failure (GFR,evaluated with creatinine clearance 9.18 ml/min; range 7 to 10mi/mm) and 10 hemodialyzed (HD) patients (6 male and 4female; age 59.4 years; range 40 to 63). For at least one yearprior to the study HD patients were dialyzed with cuprophanmembrane dialyzers three times a week. Five patients used abicarbonate bath for more than one year.
320

Memo/i el a!: IL-6 production in hemodialyzed patients 321
No patient had clinical evidence for infectious or inflamma-tory diseases or malignancy; none was diabetic nor on steroidor immunosuppressive therapy.
Eight sex- and age-matched healthy volunteers were includedin the study as controls.
Design of the study
A cross over design was used in the study. In the first phaseof the study all patients were evaluated during dialysis with newcuprophan membrane (Bellco Italy; membrane surface 1.0 m2;membrane thickness 11 t; sterilization, ethylene oxide) for twomonths. The patients were then switched to dialysis withpolymethylmethacrylate (PMMA, Toray, Tokyo, Japan; mem-brane surface 1.0 m2; membrane thickness 30 sterilization,gamma ray) for two months; finally, they were then switched toa second period of dialysis with new cuprophan membrane(same filter of the first period) for one additional month. Therewere no changes throughout all phases of the study in thefollowing dialysis parameters: axial blood flow, ultrafiltrationflow rate, dialysis time and dialysate flow rate and composition(5 patients used bicarbonate bath and 5 patients used acetatebath thorough all the study). In all dialysis sessions (during the3 phases of the study) we used the same type of blood lines(PiVipOIR, BelIco Italy).
During the different phases of the study patients were mea-sured two times a month, at midweek, for predialysis BUN andserum creatinine concentrations.
Blood samples
Blood samples (15 ml) were collected in heparinized tubes incontrols and uremic (dialyzed and non-dialyzed) patients. Indialyzed patients blood samples were obtained before and afterdialytic session: at the end of the first cuprophan period (CU 1),at the end of each month of treatment with PMMA (PMMA1and PMMA2, respectively) and at the end of the secondcuprophan period (CU2).
IL-6 and 2m production was measured in supernatant ofperipheral blood mononuclear cells (PBMC) isolated and cul-tured for 24 hours.
Preparation of PBMC
Fifteen milliliters of whole blood were carefully layered overlymphocytes-separation medium (Flow Laboratories, Irvine,Scotland, UK) allowing gradient density centrifugation. Cellpellets were washed twice with RPMI 1640 (Flow Laborato-ries), counted using a coulter counter and then resuspended at3 x 106/ml, in Iscove's (Flow Laboratories) containing 1%de-complemented fetal calf serum (Gibco), 100 lU/mi penicillin(Gibco) and 100 Wml streptomycin (Gibco). On average,PBMC contained 80% of lymphocytes and 20% of monocytes.The average percents of monocytes were not different (range 18to 21%) in the various groups (controls, uremics, CU1, PMMAand CU2).
PBMC were placed in 15 ml polypropylene round-bottomtubes (Falcon), at 37°C in a 5% CO2 saturated humidity incu-bator. After 24 hours of incubation the supernatant was re-moved.
7TDI bioassay of IL-6
In agreement with other authors [401, it is well establishedthat average sensitivity of IL-6 bioassay is about 50 to 100 timesgreater than that of IL-6 immunoassay (ELISA). Therefore, wedecided to measure IL-6 supernatant levels by IL-6 activityassay. In particular, IL-6 levels were determined by the capac-ity to induce the proliferation of IL-6-dependent murine hybrid-oma cell line, (provided by Dr. J. Van Snick, Ludwig Institutefor Cancer Research, Brussels, Belgium) [41, 42]. 7TD1 cellsare cultured in Iscove's medium (Flow Laboratories) supple-mented with 10% heat-inactivated fetal calf serum (Flow Lab-oratories), 1.5 mrvi L-glutamine, 0.24 mrvi L-asparagine, 0.55mM L-arginine, 50 /LM 2-mercaptoethanol, 0.1 mt hypoxan-thine, 16 LM thymidine, 50 pg/mi gentamicin, and at least 20U/mi (0.02 to 0.2 ng/ml) of human recombinant IL-6 (rIL-6, 1 xi07 U/ml, provided by Dr. T. Kishimoto, Division of Immunol-ogy, Institute for Molecular and Cellular Biology, Osaka Uni-versity, Osaka, Japan).
Before the assay, spent medium is removed and cells arewashed twice with fresh medium (without IL-6) to eliminatetraces of remaining IL-6. Cells are then resuspended in culturemedium (without cold thymidine and IL-6) at 20,000 cells/miand 100 d of this suspension is added to duplicate serialdilutions of samples in the same volume. Incubation is carriedout in 96-well, flat-bottom, gamma irradiated plates (MicrotestIII, Becton Dickinson, New Jersey, USA) for 72 hours. Differ-ent dilutions of recombinant human IL-6 are also included in thesame volume of the samples (100 d) to verify the validity of thebio-assay.
7TD1 growth factor activity was determined by measuringtritiated timidine incorporation in the cells. To measure timidineincorporation, 7TD1 cultures were pulsed with 0.5 nCi of[3H]-thimidine (Amersham International, London UK, specificactivity 48 Ci/mmol) for the last four hours and collected by anautomated cell harvester (Packard Micromate 196, PackardInstruments Company, Meriden, Connecticut, USA). Thimi-dine incorporation in cells was determined in the samples, ascpm, by a scintillation counter (Packard 1500 Tri-Carb).
IL-6 activity in experimental samples was measured in U/mi.One IL-6 unit was defined as the dilution that produces thehalf-maximal growth of the cells [41].
Under these conditions, the lowest detectable concentrationof IL-6 in supernatant from the zero level was 4 U/mI. Super-natant samples below this detection limit were assumed to havea value of 2 U/ml. This detection limit corresponds on averageto 8 pg/mI, and is lower than the limits reported by others forcommercially available immunoassays [401.
In our laboratory, we tested and recently reported [43] thespecificity of the 7TD1 response to IL-6 with an anti-IL-6 goatpolyclonal neutralizing antibody.
Beta-2-microglobulin assay
The quantity of /32m released by PBMC after 24 hours ofincubation was determined in the supernatant by using solid-phase radioimmunoassay (Abbott, Germany). The titrationcurve was linear from 50 to 4000 nglml, with an interassayvariation of less than 3%.

322 Me,noli et al: IL-6 production in hemodialyzed patients
52 -i
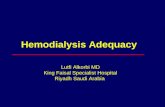
CU1 PMMA1 PMMA2 CU2Fig. 2. IL-6 production after incubating PBMC for 24 hours. Resultsfrom 10 dialyzed patients before (0) andafter () dialysis session. TheIL-6 values were obtained at the end of the first period of dialysis withcuprophan membranes (CU!), after one (PMMA1) and two (PMMA2)months of dialysis with polymethylmethacrylate membranes and afterone further month of dialysis with cuprophan membranes (CU2). IL-6production in CU! (both pre and post dialysis) were significantly greaterthan in PMMAI and PMMA2 (P < 0.01). IL-6 production in CU2 weresignificantly greater than in CU! (P < 0.05), PMMA1 and PMMA2 (P <0.01).
Effects of different membranes. IL-6 production was differentwith different membranes. Thus, the values obtained with
_____________________________ PMMA membranes after one month (PMMAI = 10.6 4.0 U/3x 106 PBMC/24 hr, at the start of dialysis) and after two months(PMMA2 = 7.8 4.4 U/3 x 106 PBMC/24 hr, at the start ofdialysis) of dialysis were not different from controls and muchlower than those obtained after cuprophan (Fig. 2).
When the patients were switched back to the new cuprophanmembrane, the IL-6 production by their PBMC in culture wasgreatly increased after one month of dialysis (CU2, 44.6 9.4U/3 x 106 PBMC/24 hr, at the start of dialysis) reaching valuessignificantly higher than those obtained with the first periodwith cuprophan membrane (Fig. 2).
Effect of dialytic treatment. No difference was observedbetween the values of IL-6 production obtained pre- andpost-dialysis with cuprophan or PMMA membranes (Fig. 2). Nodifference was obtained between the patients using acetate andthose using bicarbonate bath.
IL-6 production Production of 132m in supernatant
50
40
30
20
10
0
48-
32 -
28-I.-
24-
8-
4-
..
S
S.• S...
•S5•
C UR CU1
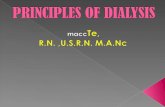
Fig. 1. IL-6 production after incubating PBMC for 24 hours. Resultsfrom 8 healthy subjects (C), 7 uremic non-dialyzed patients (UR) and 10dialyzed patients (at the start of dialysis session, at the end of firstperiod of dialysis with cuprophan membranes, CU 1). IL-6 production inCUI is significantly greater than in C (P < 0.005) and UR (P < 0.05).
Statistical analysisStttistical analysis was carried out using the analysis of
variance for repeated measures (Newman-Keuls), paired t-testand regression analysis (BMDP software). The differences wereconsidered to be significant for P < 0.05.
Results
Comparison among controls, uremic non-dialyzed and hemo-dialyzed patients. Figure 1 shows IL-6 production obtained ineight control subjects (C), in seven uremic non-dialyzed pa-tients (UR) and in ten patients on RDT (at the start of dialysissession) with cuprophan membranes (CU1).
Compared to IL-6 synthesis in control healthy subjects (6.05.6 U13 x 106 PBMC/24 hr) and UR patients (8.6 6.4 U/3 )<106 PBMC/24 hr), the patients usually dialyzed with newcuprophan membranes (CU 1) showed a statistically-significanthigher value of IL-6 production (23 13 U/3 x 106 PBMCI24hr, at the start of dialysis). No difference was observed betweenUR patients and control subjects.
In Figure 3 the values of f32m production by PBMC are shownfor controls, non-dialyzed uremic patients and dialyzed pa-tients.
The values of f32m release were significantly greater inpatients dialyzed with cuprophan membrane (CU1 and CU2)than in controls (C), uremic non-dialyzed patients (UR) andpatients dialyzed with PMMA membranes (PMMA1 andPMMA2), with no difference between the values obtainedbefore and after dialytic treatment.
/32m release obtained at the end of the second cuprophanperiod was significantly higher than the value obtained at theend of the first cuprophan period (Fig. 3).

50
Memoli et a!: JL-6 production in hemodialyzed patients 323
Fig. 3. Beta-2-microglobulin production afterincubating PBMC for 24 hours. Results in 8control subjects (C), 7 uremic non-dialyzedpatients (UR) and 10 dialyzed patients before(3) and after () dialysis session at the endof the first period of dialysis with cuprophanmembranes (CU1), after one (PMMAI) andtwo (PMMA2) months of dialysis withpolymethylmethacrylate membranes and afterone further month of dialysis with cuprophanmembranes (CU2). Beta-2-microglobulinvalues in CU! (both pre- and post-dialysis)were significantly greater than in C, UR,PMMA1 and PMMA2 (P < 0.01). Beta-2-microglobulin values in CU2 (both pre- and
_______ __________ post-dialysis) were significantly greater than inCUI (P < 0.05) and C, UR, PMMAI andPMMA2 (P < 0.01).
Fig. 4. Comparison between IL-6 (--0--) andbeta-2-microglobulin (t) productions inuremic non-dialyzed patients (UR) anddialyzed patients (before dialysis session) atthe end of first period of dialysis withcuprophan membranes (CUJ), after one(PMMAJ) and two (PMMA2) months ofdialysis with polymethylmethacrylatemembranes, and after one further month ofdialysis with cuprophan membranes (CU2).
Relationship between IL-6 and f32m productionThe behavior of IL-6 and that of /32m were quite similar
throughout the study, as shown in Figure 4.A linear relation was obtained when values of /32m production
were plotted against values of IL-6 production (r =0.8296, P <0.001; Fig. 5).
Since the inclusion of several samples from the same sub-jects, that is, hemodialyzed patients, might influence the regres-sion analysis, intercorrelations of IL-6 or /32m productionvalues for different dialysis membranes were also calculated.No significant correlation among these values was found,confirming the independence of the observations from the samesubjects.
Finally, no differences were observed in BUN (respectively70.05 12.13, 72.17 14.38 and 69.20 9.17 mg/dl) and serumcreatinine (respectively 9.28 2.57, 9.76 2.93 and 9.04 2.40mgfdl) concentrations registered two times a month in hemodi-
alyzed patients during the three different periods of the study(CU1, PMMA and CU2).
Discussion
In this study, we have shown that PBMC of uremic patientsregularly hemodialyzed with a cuprophan dialyzer producehigher amounts of IL-6 in culture than PBMC from normalsubjects or non-dialyzed uremic patients. These findings clearlyindicate that the interaction of PBMC with cuprophan activatesPBMC and suggest that the high levels of plasma IL-6 found byothers in dialyzed patients [40] is secondary to increased in vivoproduction by circulating cells.
IL-6 production was high in PBMC sampled from hemodia-lyzed patients both before and after a single dialytic session,indicating that regular dialysis treatment with a cuprophanmembrane causes prolonged activation of monocytes.
I700
600
500
400
300
200
100
0I
I94I
x
CD-J
C UR
nil40
30
20
10
0
CU1 PMMA1 PMMA2 CU2
600
500
400 x
300C
LVV .0100 if
E
0CUI-.a)
UR CU1 PMMA1 PMMA2 CU2

324 Memoli et a!: IL-6 production in hemodialyzed patients
After dialyzing the same patients for one month with PMMA,a reduction of IL-6 production by PBMC was observed, whichwas similar to those of uremic non-dialyzed patients andhealthy control subjects. This reduction was confirmed aftertwo months. This effect of PMMA proves further that PMMA ismore biocompatible than cuprophan, and may be accounted forby the low capacity of PMMA membranes to activate comple-ment [29].
Recently, Vanholder et al [44] suggested that accumulation ofuremic solutes could play a role in chronic stimulation ofmonocytes. In our study, no differences were observed in smallmolecules (BUN and creatinine) concentrations during thedifferent phases of the study (when either cuprophan or PMMAwere used); these results seem to exclude any role of a differentaccumulation of these solutes on monocytes chronic activation.
When the patients were switched back to dialysis withcuprophan membranes a great increase of IL-6 production wasobserved, with values significantly greater than those obtainedwith cuprophan before PMMA (Fig. 2). This behavior suggestsa more intense responsiveness of PBMC after a period ofPMMA dialysis; such observation is consistent with that ofZaoui, Stone and Hakim [32], who have recently demonstratedthat dialysis with PMMA membranes increases HLA and f3,mexpression on circulating cells. It is likely that synthesis of IL-6during the first period of dialysis with cuprophan was reducedbecause of the repetitive stimulation of monocytes prior totesting, whereas during the second exposure to cuprophan, themonocytes had not been activated for a prolonged period oftime and were therefore able to up-regulate their synthesisquickly.
The high production of IL-6 by PBMC may have importantclinical implications since it is well known that elevated IL-6plasma levels can play a role in the systemic inflammatoryreaction to an infection or injury. Studies using highly sensitiveIL-6-dependent hybridoma growth assays show that IL-6 levelsare elevated in patients who develop an acute phase responsewith changes in circulating protein levels [45, 46].
Interleukin-6 is the major regulator of the hepatic acute phase
protein response during inflammation [47—52]. In humans,changes referred to acute phase proteins are characterized bydecreased synthesis of albumin, modest increase in synthesis ofa number of positive acute phase proteins and, most strikingly,by dramatic increase in synthesis (up to 1000-fold or more) ofthe two major acute phase proteins, C-reactive protein andserum amyloid A [49). These effects are observed also in vitroupon stimulation of hepatocytes with human rIL-6 [48, 49].
There are no studies in the literature on the effect of IL-6plasma levels in uremic patients on the release of acute phaseproteins. We can only hypothesize that repeated inductions ofacute phase proteins may cause complications mainly related toamyloidosis disease, including carpal tunnel syndrome, Os-teopenia, joint fibrosis and muscle wasting [53]. Further inves-tigations with measurement of acute phase protein release inuremic patients are, however, needed to clarify this importantissue.
Our results demonstrate that the production of /32m by PBMCis different with different types of membranes used for dialysistreatment (Fig. 3) and that the 132m production is related to IL-6production (Figs. 4 and 5). This relationship further suggests apossible implication of this cytokine in the pathogenesis ofdialysis amyloidosis.
Interestingly, uremic non-dialyzed patients show a low 132mrelease, as well as a low IL-6 production (Figs. 2, 3 and 4).
In conclusion, the production of IL-6 by PBMC of uremicpatients treated with cuprophan dialyzers is increased. InPBMC, the increased production of IL-6 is associated withincreased 2m release. Both the abnormal IL-6 production andthe increased release of J3,m are normalized after an one-monthtreatment with a more biocompatible membrane.
00
1000
900
800
700
600
500
400
300
200
100
0
I-.
0
0
0
0
0
0 5 10 15 20 25 30 35 40 45 50 55IL-6, U/3 x 106 PBMC/24 hr
Fig. 5. Relationship between IL-6 and beta-2-micro globulin productions in control subjects,ure,nic non-dialyzed patients and dialyzedpatients, at the start of dialysis, in all phasesof the study. P < 0.001; r = 0.8270; y =—1.4689 + 15.068x.
Acknowledgments
This study was partially supported by a MURST 60% grant. Part ofthis study was presented at the 23rd Annual Meeting of the AmericanSociety of Nephrology, Washington, D.C., December 2—5, 1990.

Memo/i et a/: IL-6 production in hemodia/yzed patients 325
Reprint requests to Bruno Memo/i, M.D., Department of Nephrol-ogy, ii Faculty of Medicine, University of Nap/es, Via S. Pansini 5(EdUlcio 5), 80131, Napoli, italy.
References
1. DINARELLO CA, MIER JW: Current concepts: Lymphokines. NEngi J Med 317:940—945, 1987
2. LUGER A, KOVARIK J, STUMMVOLL HK, URBANSKA A, LUGERTA: Blood-membrane interaction in hemodialysis leads to in-creased cytokine production. Kidney tnt 32:84—88, 1987
3. LONNEMANN G, BINGEL M, KOCH KM, SHALDON S, DINARELLOCA: Plasma interleukin-1 activity in humans undergoing hemodial-ysis with regenerated cellulosic membranes. Lymphokine Res 6:63—70, 1987
4. LONNEMANN G, VAN DER MEER JWM, CANNON JG, DINARELLOC, KOCH KM, GRANOLLERAS C, DESCHODT G, SHALDON S:Induction of tumor necrosis factor during extracorporeal bloodpurification. N EngI J Med 317:963—964, 1987
5. LONNEMAN G, BINGEL M, FLOEGE J, KOCH KM, SHALDON S,DINARELLO CA: Detection of endotoxin-like interleukin-l inducingactivity during in vitro hemodialysis. Kidney mt 33:29—35, 1988
6. BINGEL M, LONNEMANN U, KOCH KM. DINARELLO CA, SHAL-DON S: Plasma interleukin-1 activity during hemodialysis: Theinfluence of dialysis membranes. Nephron 50:273—276, 1988
7. BLUMENSTEIN M, SCHMIDT B, WARD RA, ZIEGLER-HEITBROCKHWL, GURLAND HJ: Altered interleukin-1 production in patientsundergoing hemodialysis. Nephron 50:277—281, 1988
8. HAEFFNER-CAVAILLON N, CAVAILLON JM, CIANCIONI C, BACLEF, DELONS S, KAZATCHKINE MD:In vivo induction of interleu-kin-I during hemodialysis. Kidney mt 35:1212—1218, 1989
9. HERBELIN A, NGUYEN AT, ZINGRAFF J, URENA P, DESCAMPS-LATSCHA B: Influence of uremia and hemodialysis on circulatinginterleukin-1 and tumor necrosis factor. Kidney tnt 37:116—125,1990
10. KIMMEL PL, PHILLIPS TM, PHILLIPS B, BOSCH JP: Effect of renalreplacement therapy on cellular cytokine production in patientswith renal disease. Kidney tnt 38:129—135, 1990
11. HENDERSON LW, KOCH KM, DINARELLO CA, SHALDON S: He-modialysis hypotension: The interleukin hypothesis. Blood Purif1:3—8, 1983
12, DINARELLO CA, KOCH KM, SHALDON S: Interleukin-1 and itsrelevance in patients treated with hemodialysis. Kidney tnt 33:S21—S26, 1988
13. COLTON CK: The interleukin hypothesis: A quantitative assess-ment. Kidney mt 33:S27—S29, 1988
14. BERNIER GM, FANFER MW: Synthesis of beta-2-microglobulin bystimulated lymphocytes. J immunol 109:407—409, 1972
15. KIN K, KASAHARA T, IToH Y: Beta-2-microglobulin production byhighly purified human T and B-lymphocytes in cell culture stimu-lated with various mitogens. immunology 36:47—51, 1979
16. NACHBAUR K, TROPPMAIR J, BIELING P: Cytokines in control ofbeta-2-microglobulin release. immunobiology 177:55—65, 1988
17. KNUDSEN PJ, NG AK, LIU Z: Beta-2-microglobulin synthesis isincreased during activation of human monocytes. Blood Purf6:178—187, 1988
18. KNUDSEN PJ, LEON J, NG AK, SHALDON S, FLOEGE J, KOCH KM:Hemodialysis-related induction of beta-2-microglobulin and inter-leukin-1 synthesis and release by mononuclear phagocytes. Neph-ron 53:188—193, 1989
19. OKUSAWA 5, DINARELLO CA, YANCEY KB, ENDRES 5, LAWLEYTJ, FRANK MM, BURKE JF, GELFAND JA: C5a induction of humaninterleukin 1. Synergistic effect with endotoxin or interferon. JImmunol 139:2635—2640, 1987
20. HAEFFNER-CAVAILLON N, CAVAILLON JM, LAUDE M, KAZATCH-KINE MD: C3a (C3adesArg) induces production and release ofinterleukin 1 by cultured human monocytes. J immunol 139:794—
799, 198721. OKUSAWA S, YANCEY KB, VAN DER MEER JWM, ENDRES S,
LONNEMANN G, HEFTER K, FRANK MM, BURKE JF, DINARELLOCA, GELFAND JA: C5a stimulates secretion of tumor necrosisfactor from human mononuclear cells in vitro. Comparison with
secretion of interleukin 113 and interleukin lc. J Exp Med 168:443—448, 1988
22. HAEFFNER-CAVAILLON N, FISCHER E, BACLE F, CARRENO MP,MAILLET F, CAVAILLON JM, KAZATCHKINE MD: Complementactivation and induction of interleukin-l production during hemo-dialysis. Contr Nephrol 62:86—98, 1988
23. SCHLINDER R, LONNEMANN G, SHALDON S, KOCH KM,DINARELLO CA: Transcription, not synthesis, of interleukin I andtumor necrosis factor by complement. Kidney tnt 37:85—93, 1990
24. LAUDE-SHARP M, CAROFF M, SIMARD L, PuSINERI C, KAZATCH-KINE MD, HAEFFNER-CAVAILLON N: Induction of IL-l duringhemodialysis: Transmembrane passage of intact endotoxins (LPS).Kidney mt 38:1089—1094, 1990
25. BETZ M, HAENSCH GM, RAUTERBERG EW, BOMMER J, RITZ E:
Cuprammonium membranes stimulate interleukin- 1 release andarachidonic acid metabolism in monocytes in the absence ofcomplement. Kidney tnt 34:67—73, 1988
26. L0NNEMANN G, KOCH KM, SHALDON S, DINARELLO CA: Studieson the ability of hemodialysis membranes to induce, bind, and clearhuman interleukin 1. J Lab C/in Med 112:76—86, 1988
27. BINGEL M, KOCH KM, LONNEMANN U, DINARELLO CA, SHAL-DON S: Enhancement of in vitro human interleukin-1 production bysodium acetate. Lancet i:l4—16, 1987
28. CHENOWETH D, CHEUNG AK, HENDERSON LW: Anaphylatoxinformation during hemodialysis: Effects of different dialyzer mem-branes. Kidney mt 24:764—769, 1983
29. HAKIM RM, FEARON DT, LAZARUS JM: Biocompatibility of dialy-sis membranes: Effects of chronic complement activation. Kidneymt 26:194—200, 1984
30. KUNITOMO T: Development of new artificial kidney systems. Am JSurg 146:594—598, 1984
31. CHEUNG AK, PARKER CJ, WILCOX L, JANATOVA J: Activation ofthe alternative pathway of complement by cellulosic hemodialysismembranes. Kidney mt 36:257—265, 1989
32. ZA0uI M, STONE WJ, HAKIM RM: Effects of dialysis membraneson Beta-2-microglobulin production and cellular expression. Kid-ney mt 38:962—968, 1990
33. WONG GG, CLARK SC: Multiple actions of interleukin-6 within acytokine network. immunol Today 9(5): 137—139, 1988
34. CHIU CP, MOULDS C, COFFMAN RL, RENNICK D, LEE F: Multiplebiological activities are expressed by a mouse interleukin-6 cDNAclone isolated from bone marrow stromal cells. Proc Nati Acad SciUSA 85:7099—7103, 1988
35. TOVEY MG, CONTENT J, GREESR I, GUGENHEIM J, BLANCHARD B,GUYMARHO J, POUPART P, GIGOU M, SHAW A, FIERS W: Genes forIFN-$-2 (IL-6), tumor necrosis factor and IL-i are expressed athigh levels in the organs of normal individuals. J immunol 141:3106—3110, 1988
36. MAKOTO A, LOUSSARARIAN AH, ADELMAN DC, SAITO M, KOEF-FLER HP: Role of lymphotoxin in expression of interleukin 6 inhuman fibroblasts. J C/in invest 85:121—129, 1990
37. LE J, VILCEK J: Interleukin 6: A multifunctional citokine regulatingimmune reactions and the acute phase protein response. Lab invest61:588—602, 1989
38. WAAGE A, HALSTENSEN A, SHALABY R, BRANDTZAEGP, KIERULFP, ESPEVIK T: Local production of tumor necrosis factor, IL-i andinterleukin-6 in meningococcal meningitis. J Exp Med 170:1859—1867, 1989
39. BHARDWAJ N, SANTHANAM U, LAU LL, TATTER SB, GHRAYEB J,RIvELIs M, STEINMAN RM, SEHOALPB, MAY LT: IL-6/IFN-f32 insinovial effusions of patients with rheumatoid arthritis and otherarthritides. JImmunol 143:2153—2159, 1989
40. HERBELIN A, URENA P, NGUYEN AT, ZINGRAFF J, DESCAMPS-LATSCHA B: Elevated circulating levels of interleukin-6 in patientswith chronic renal failure. Kidney tnt 39:954—960, 1991
41. VAN SNICK J, CAYPI-IAS 5, VINK A, UYTTENHOVE C, COULIE PG,RUBIRA MR, SIMPSON RJ: Purification and NH2-terminai aminoacid sequence of a T-cell-derived lymphokine with growth factoractivity for B-cell hybridomas. Proc Nat/ Acad Sci USA 83:9679—9687, 1986
42. VAN DAMME J, OPDENAKKER G, SIMPSON RJ, RUBIRA MR.CAYPHAS S, VINK A, BILLIAU A, VAN SNICK J: Identification ofthe human 26-kD protein, interferon 132. as a B cell hybridomal

326 Memoli et a!: IL-6 production in hemodialyzed patients
plasmocitoma growth factor induced by interleukin 1 and tumornecrosis factor. J Exp Med 165:914—919, 1987
43. SCALA G, QuINT0 I, Ruocco MR, ARCUCCI A, MALLARDO M,CARETTO P, F0RNI G, VENUTA S: Expression of an exogenousInterleukin 6 gene in human Epstein Barr virus B cells confersgrowth advantage and in vivo tumorigenicity. JExp Med 172:61—68,1990
44. VANHOLDER R, RING0IR 5, DHONDT A, HAKIM R: Phagocytosis inuremic patients: A prospective and cross sectional study. Kidneymt 39:320—327, 1991
45. NLJSTEN MWN, DE GR00T ER, TEN Duis HJ, KLASEN Hi, HACKCE, AARDEN LA: Serum levels of interleukin-6 and acute phaseresponses. Lance: 2:921, 1987
46. SHENKIN A, FRASER WD, SERIES i, WINSTANLEY FP, MCCART-NEY AC, BURNS HJG, VAN DAMME J: The serum interleukin 6response to elective surgery. Lymphokine Res 8:123—127, 1989
47. GAULDIE J, NORTHEMANN W, FEY GH: IL-6 functions as anexocrine hormone in inflammation. J Immunol 144:3804—3808, 1990
48, GEIGER T, ANDUS T, KLAPPROTH J, HIRANO T, KISHIMOTO T,
HEINRICH PC: Induction of rat acute-phase proteins by interleukin6 in vivo. Eur J Immunol 18:717—721, 1988
49, HEINRICH PC, CASTELL JV, ANDUS T: Interleukin-6 and the acutephase response. Biochem J 265:621—636, 1990
50. GANAPATHI MK, MAY LT, SCHULTZ D, BRABENEC A, WEINSTEINJ, SEHGAL PB, KIJSHNER I: Role of interleukin-6 in regulatingsynthesis of C-reactive protein and serum amyloid A in humanhepatoma cell lines. Biochem Biophys Res Comm 157:271—277,1988
51. RAMADORI G, VAN DAMME J, RIEDER H, MEYER ZUM BUSCHEN-FELDE KH: Interleukin 6, the third mediator of acute-phase reac-tion, modulates hepatic protein synthesis in human and mouse.Comparison with interleukin 1/3 and tumor necrosis factor-a. Eur JImmuno! 18:1259—1264, 1988
52. MARINK0vIc 5, JAHREIS GP, WONG GG, BAUMANN H: IL-6modulates the synthesis of a specific set of acute phase plasmaproteins in vivo. J Immunol 142:808—812, 1989
53. SHALDON S, DINARELLO CA: The relationship between biocom-patibility and interleukin 1. Life Support Syst 5:341—345, 1987