Helping patients Helping patients cope with cystic...
7
CYSTIC FIBROSIS (CF) is an inherited auto- somal recessive disorder of the exocrine glands that affects the lungs and digestive system of children and adults. Approxi- mately 30,000 people in the United States have been diagnosed with CF, and it affects all races (primarily Caucasians). Girls and boys are affected equally. Additionally, it’s estimated that about 1 in every 31 Ameri- cans are carriers of the defective CF gene, without actually having the disease. This disease was once considered strictly one of childhood because many children who had it didn’t survive past their early years. Currently, the estimated survival age for people with CF extends to the mid to late 30s. In fact, more than 40% of patients living with CF are age 18 or older. The great increase in life expectancy of patients with CF over the past few decades is due to many advances in diagnosis and treatment. In this article, I’ll discuss the genetics of CF and its effects on various organ systems. I’ll also take a look at how the disease is screened for and diagnosed. Finally, I’ll review current treatments and therapies for CF, as well as how to best assist your patients in coping with this chronic disorder. It’s in the genes To understand how CF develops, you need to understand inherited autosomal recessive genetic disorders. All genes come in pairs. A recessive gene is one that’s expressed only when both copies of the gene are pre- sent. Carriers of the CF gene have one nor- mal gene and one abnormal gene in the pair, but don’t have the actual disease. In order for a child to inherit CF, he must in- herit both copies of the defective gene, one from each parent (see Inheritance of CF). If both parents are CF carriers, each preg- nancy has a 25% chance of producing a child with CF. If the child doesn’t inherit the dis- ease, there’s a 50% chance that he’ll be a CF carrier like his parents. So what exactly is CF? Patients with CF have a mutation in a gene that encodes a protein called cystic fibrosis transmembrane conductance regulator (CFTR). This protein is responsible for transporting sodium and chloride ions across cell membranes in the epithelial lining of the ducts of exocrine glands, which include sweat glands, sinuses, bronchial mucosa, the pancreas, salivary glands, the intestines, the biliary tract, and the reproductive tract. Abnormal function of 48 Nursing made Incredibly Easy! November/December 2008 Helping patients cope Helping patients cope A life-threatening genetic disease that affects the respiratory and gastrointestinal systems, cystic fibrosis has no cure, but patients with the disease are living longer than ever before. Find out what you need to know about the latest advances in diagnosis and treatment so you can help your patients get the care they need. Heather Brown-Guttovz, RN, BSN Head Nurse • Southfield Pediatric Center • Southfield, Mich.
Transcript of Helping patients Helping patients cope with cystic...

CYSTIC FIBROSIS (CF) is an inherited auto-somal recessive disorder of the exocrineglands that affects the lungs and digestivesystem of children and adults. Approxi-mately 30,000 people in the United Stateshave been diagnosed with CF, and it affectsall races (primarily Caucasians). Girls andboys are affected equally. Additionally, it’sestimated that about 1 in every 31 Ameri-cans are carriers of the defective CF gene,without actually having the disease.
This disease was once considered strictlyone of childhood because many childrenwho had it didn’t survive past their earlyyears. Currently, the estimated survival agefor people with CF extends to the mid to late30s. In fact, more than 40% of patients livingwith CF are age 18 or older. The greatincrease in life expectancy of patients withCF over the past few decades is due to manyadvances in diagnosis and treatment.
In this article, I’ll discuss the genetics ofCF and its effects on various organ systems.I’ll also take a look at how the disease isscreened for and diagnosed. Finally, I’llreview current treatments and therapiesfor CF, as well as how to best assist yourpatients in coping with this chronic disorder.
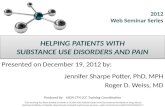
It’s in the genesTo understand how CF develops, you needto understand inherited autosomal recessivegenetic disorders. All genes come in pairs.A recessive gene is one that’s expressedonly when both copies of the gene are pre-sent. Carriers of the CF gene have one nor-mal gene and one abnormal gene in thepair, but don’t have the actual disease. Inorder for a child to inherit CF, he must in-herit both copies of the defective gene, onefrom each parent (see Inheritance of CF).
If both parents are CF carriers, each preg-nancy has a 25% chance of producing a childwith CF. If the child doesn’t inherit the dis-ease, there’s a 50% chance that he’ll be a CFcarrier like his parents.
So what exactly is CF? Patients with CFhave a mutation in a gene that encodes aprotein called cystic fibrosis transmembraneconductance regulator (CFTR). This proteinis responsible for transporting sodium andchloride ions across cell membranes in theepithelial lining of the ducts of exocrineglands, which include sweat glands, sinuses,bronchial mucosa, the pancreas, salivaryglands, the intestines, the biliary tract, andthe reproductive tract. Abnormal function of
48 Nursing made Incredibly Easy! November/December 2008
Helping patients cope with cystic fibrosisHelping patients cope with cystic fibrosis
A life-threatening genetic disease that affectsthe respiratory and gastrointestinal systems,cystic fibrosis has no cure, but patients withthe disease are living longer than ever before.Find out what you need to know about thelatest advances in diagnosis and treatmentso you can help your patients get the carethey need.Heather Brown-Guttovz, RN, BSNHead Nurse • Southfield Pediatric Center • Southfield, Mich.

November/December 2008 Nursing made Incredibly Easy! 49
e with cystic fibrosise with cystic fibrosis

CFTR in these cells leads to abnormal trans-port of water and salt across the epithelialsurfaces. This causes abnormally thick secre-tions in many different organs and disruptstheir normal functions.
Early warningSigns of CF generally appear at birth or dur-ing early infancy. The first sign of CF mayoccur right after birth, when the passage ofmeconium (the dark greenish feces thathave collected in the intestines of a full-termfetus) is delayed. Infants with the disordertypically develop recurrent respiratory infec-tions or failure to thrive, prompting an ex-ploration into a CF diagnosis. Children mayalso exhibit signs of pancreatic insufficiencyearly in life, resulting in the passing of fre-quent, fatty, bulky, foul-smelling stools(steatorrhea) and poor growth despite agood appetite.
Systems affected by CFThe effects of CF can involve multiple or-gans. Over 1,000 different mutations of theCF gene have been identified, each one
causing different signs and symptoms, aswell as variable progression of the disease.The following organ systems are typicallyaffected in people with CF.
Respiratory systemPatients with CF have thick and viscous air-way secretions that result in a continuouscycle of obstruction, infection, and inflam-mation. Thick mucus is very difficult to ex-pel by coughing, and it becomes stagnantand clogs the patient’s airways (see Whatthe lungs look like in CF). This excessivelythick mucus is the perfect breeding groundfor bacteria. The resulting chronic infectionleads to irreversible lung damage.
Additional respiratory symptoms includenasal polyps and chronic sinusitis. Air trap-ping in the lungs can lead to development ofa barrel-shaped chest. Clubbing of the fin-gers and toes may also occur.
Gastrointestinal (GI) system Abnormally thickened pancreatic fluids canblock the pancreatic ducts, preventing thesecretion of essential digestive enzymes intothe intestine. Pancreatic insufficiency affects85% to 90% of patients with CF, preventingthe body from being able to digest nutri-ents. Fats, protein, and fat-soluble vitamins(A, D, E, and K) are malabsorbed, leadingto nutritional deficiencies, delayed growth,weight gain, and steatorrhea. Plugged pan-creatic ducts lead to pancreatic damage.
Gastroesophageal reflux disease is com-mon in patients with CF due to hypersecre-tion of gastric acid and hyposecretion ofbicarbonate. Chronic coughing and posturaldrainage techniques used to mobilize respi-ratory secretions and aid expectoration canfurther aggravate this condition. AdditionalGI complications related to CF include distalintestinal obstructive syndrome, constipa-tion, and liver disease.
Reproductive system In both men and women, CF affects the re-productive system. Puberty may be delayed
50 Nursing made Incredibly Easy! November/December 2008
Child(Does nothave CF)
Father(Carrier of CF gene)
Mother(Carrier of CF gene)
Normal gene
Defective gene
Child(Carrier of CF gene)
Child(Carrier of CF gene)
Child(Has CF)
Inheritance of CF

in both boys and girls. Nearly all men withCF are sterile due to absent or malformedvas deferens. Women may have decreasedfertility caused by thick cervical secretionsblocking sperm movement. A variety of fer-tility treatments are available to help thesepatients achieve pregnancy. Genetic coun-seling is required to help couples under-stand the risk of passing on the disease.
Endocrine system An additional CF complication is cystic fi-brosis-related diabetes (CFRD), which canoccur in 20% to 30% of patients over age 20.The main cause of CFRD is insulin defi-ciency due to obstruction of the pancreaticduct. However, impaired glucose metabo-lism is also a factor. Most patients withCFRD require insulin therapy to managetheir diabetes.
Sweating out the diagnosisFor the past 40 years, the gold standard fordiagnosing CF has been the quantitative pi-locarpine iontophoresis sweat test, which isused to measure the amount of chloride inthe patient’s sweat; in someone with CF, theconcentration of chloride in sweat is veryhigh.
During this simple procedure, pilocarpineis applied to a small area of the arm or leg;an electrode is placed over the area to delivera weak electric current and stimulate sweat.Sweat is applied to a gauze pad or filterpaper and sent to the lab for analysis.Diagnosis is made as follows:• sweat chloride concentration less than40 mmol/L is normal• concentration between 40 and 60mmol/L is borderline• concentration greater than 60mmol/L is diagnostic of CF.
Genetic testing may be performed ifthe patient’s sweat test is positive orborderline to confirm the diagnosis.The presence of CF mutations in bothCFTR genes also confirms the diagnosis.
Newborn screening tests can be per-formed on blood to evaluate for CF.The screening test evaluates levels ofimmunoreactive trypsinogen, which ifelevated can indicate CF and prompt addi-tional testing. The CDC recommends that allstates consider adding CF testing to theirnewborn screening blood tests. Detecting CFearly helps improve the child’s growth andcognitive development, decrease incidencesof hospitalization, and improve survival.
November/December 2008 Nursing made Incredibly Easy! 51
Diagnosis ismade by
studying apatient’s
sweat—nokidding!
What the lungs look like in CF
Unobstructed bronchial tubes
Bronchial tubes are blocked by mucus
Healthy lungs Lungs with CF

What treatments areavailable?Patients with CF typically receive care froma team of physicians, nurses, dietitians, res-piratory therapists, and social workers at aCF care center. The goals of treatment in-clude prevention and treatment of lung anddigestive problems, ensuring proper nutri-tion, promoting physical activity, and en-suring appropriate psychosocial support.The following are specific ways in which
you can help CF patients achieve thesegoals.
• Antibiotic therapy. Progressivelung damage due to chronic infec-tion and inflammation is responsi-ble for the majority of morbidityand mortality in patients with CF.Prevention and appropriate treat-ment of lung infections is the maingoal of CF treatment. Because of
excessive thickened airway secre-tions, pulmonary infections are com-
mon and difficult to treat. Yourpatient’s sputum culture and sensi-
tivity results will determine theappropriate antibiotic therapy (see Medica-tions to treat CF).
The most common organisms that causelung infections in patients with CF areStaphylococcus aureus, Haemophilus influenzae,and Pseudomonas aeruginosa. Given orally,intravenously, and by inhalation via nebuliz-er, antibiotics are indicated when the patienthas acute pulmonary exacerbations and tosuppress bacterial flora during remissions. Apatient with CF may require higher thannormal doses of antibiotics, a combination oftwo different antibiotics, and a longer dura-tion of therapy to clear his lung infections.
Patients chronically infected withPseudomonas experience increased lunginflammation and decreased lung function.The Cystic Fibrosis Foundation publishednew guidelines for the treatment of thispathogen in November 2007. Chronic use ofinhaled tobramycin in patients with CF ages6 and up with moderate-to-severe lung dis-
ease is recommended to decrease exacerba-tions and improve lung function. This treat-ment is also recommended for patients withasymptomatic or mild lung disease todecrease exacerbations. Chronic use ofazithromycin has also been recommendedfor CF patients ages 6 and up with P. aerugi-nosa that’s continually present in airway cul-tures to improve lung function and reducethe number of exacerbations.• Airway clearance techniques. A vital com-ponent of CF pulmonary treatment is effec-tive airway clearance maneuvers to help thepatient expectorate thick airway secretions.Not clearing these secretions can lead to ob-structed airflow, impaired gas exchange,and infection.
Your patient can choose from various air-way clearance maneuvers, including postur-al drainage techniques, positive end-expira-tory pressure therapy, a high-frequencychest compression vest, and a flutter device.
Sessions of airway clearance maneuverstypically take 1 hour to allow for coughingand expectoration of mucus. Teach yourpatient to perform these sessions beforemeals because frequent coughing can triggervomiting. He’ll typically require airwayclearance once or twice a day for mainte-nance. During times of acute pulmonaryexacerbation, airway clearance maneuversare done more frequently.
Also encourage your patient to exerciseregularly, as this helps to clear the airways,maintain overall health, and minimize CFcomplications. He may participate in anytype of exercise program or sport he enjoys.• Additional pulmonary therapies. A vari-ety of medications are used to promoteairway clearance, improve lung function,reduce inflammation, and increase oxygena-tion. Dornase alfa nebulizer solution can beused as mucolytic therapy to thin secretionsso they’re easier to expectorate. Hypertonicsaline given via nebulizer helps to drawmore water into the airways, thinning mu-cus and making it easier to expectorate.Bronchodilators administered by nebulizer,
52 Nursing made Incredibly Easy! November/December 2008
Looks likethere are
many ways tokeep us clear.

such as albuterol, are given to open the air-ways and improve lung function. Adminis-tering mucolytic therapy and bronchodila-tors before airway clearance techniques mayimprove the outcome. Oral nonsteroidalanti-inflammatory drugs are also used inthe treatment of CF. The Cystic FibrosisFoundation recommends chronic use of oralibuprofen to slow the loss of lung functionin patients ages 6 and up with forced expi-ratory volume in the first second greaterthan 60% predicted.• Nutritional management. Maintainingproper nutrition is essential in the treatmentof CF. As most patients with CF have in-creased nutritional needs, encourage a high-calorie, high-protein diet to ensure propergrowth and development.
Patients with pancreatic insufficiency
need to take pancreatic enzyme supplementswith food to help aid nutrient absorption.Instruct your patient to take these supple-ments before or during all meals and snacks.Patients with pancreatic insufficiency requiredaily vitamin supplementation with a multi-vitamin and supplements of vitamins A, D,E, and K because they have difficulty absorb-ing these fat-soluble vitamins.
During acute pulmonary exacerbations,shortness of breath and increased work ofbreathing can make meeting nutritionalneeds difficult for a patient with CF. Short-term or long-term supplemental parenteralor enteral feedings may be necessary to meethis caloric needs. Because your patient withCF is at a risk for dehydration, instruct himto increase fluid and salt intake during hotweather and while exercising.
November/December 2008 Nursing made Incredibly Easy! 53
Medications to treat CFGI systemLactulose Given to prevent constipation.Multivitamins, iron; vitamins A, E, D, Given because the production and absorp-and K when deficient tion of vitamins are decreased by the thick
secretions. Give water-soluble vitamins for better absorption.
Pancreatic enzyme concentrates such Given to decrease the fat and bulk ofas pancrelipase (Viokase) stools. Give immediately before or with
meals and snacks to increase theabsorption of nutrients.
Ursodeoxycholic acid or ursodiol Used to treat and possibly preventprogressive liver disease in CF. It improvesthe viscosity of biliary secretions.
Respiratory systemBronchodilators (albuterol, terbutaline) Used to open airways. They’re used before
chest physiotherapy (CPT) and to relievesymptoms; administered via nebulizer.
Dornase alpha (Pulmozyme) Used with standard CF therapies toimprove pulmonary function and todecrease risk of respiratory tract infectionsrequiring parenteral antibiotics; adminis-tered via nebulizer.
Aerosol antibiotics (gentamicin, Administered via nebulizer after CPT.ticarcillin, tobramycin) Aerolized antibiotics decrease systemic
absorption. Oral and I.V. antibiotics Prolonged administration with high doses
given to treat infection; specific drug basedon culture sensitivity.

Is a transplant necessary?Lung transplantation is becoming morecommon in CF patients with severe lungdisease. The patient may receive healthytransplanted lungs from a cadaver or lunglobes from two different living donors. Suc-cess rates of lung transplants in patientswith CF equal or exceed those with otherlung disorders; 90% of CF patients are alive1 year after transplant, and 50% survivelonger than 5 years. Specific eligibility re-quirements for lung transplant are deter-mined by the transplant center, and thewait for donor lungs can be very long.
Complications of lung transplantation inpatients with CF can include organ rejectionand an increased risk of infection and malig-nancies due to having to take immunosup-pressant drugs. However, successful trans-plants can greatly improve the patient’squality of life.
Helping patients and families copePatients with CF and their families requireextensive psychosocial support. Parentsmust learn to cope with having a child witha chronic life-shortening illness, managedaily treatments and medications, and en-dure the financial hardships that accom-pany the high cost of managing this disease.The Cystic Fibrosis Foundation (http://www.cff.org) is an excellent source of sup-port with access to support groups, up-to-date treatment options and research materi-als, and financial assistance options. Thepatient’s CF care center with its team of ex-pert professionals is another great supportsystem for the family.
As a patient with CF ages, he must learnthe importance of his daily treatment plan toslow disease progression and begin to takean active role in his own care to foster asense of independence. As he gets older,acute illness will become more frequent asthe disease process worsens. As the patient’scondition deteriorates, sensitive discussionsregarding end-of-life care must take place.
Patients and their families can makeinformed choices regarding end-of-life carewith the assistance of the healthcare team.
Slowing the progressionAs a chronic, life-shortening disease that af-fects multiple organ systems, CF causes fre-quent illnesses and hospitalizations for thepatient who has it. He must learn how toeffectively incorporate his individualizedrange of therapies into his everyday life tohelp slow disease progression. Encourageyour patient that advances in treatment op-tions, including lung transplantation, areimproving quality of life and extending lifeexpectancy for people with this disease. n
Learn more about itAll Things Nursing. Philadelphia, Pa., Lippincott Williams &Wilkins, 2008.
Aronson BS, Marquis M. Care of the adult patient withcystic fibrosis. Medsurg Nursing. 13(3):143-155, June 2004.
Brown-Guttovz H. Help your patient cope with cystic fibro-sis. LPN2008. 4(3):50-55, May/June 2008.
Butzon F, Criddle LM. A 23-year-old woman with cysticfibrosis, acute hypotension, and cardiac arrest. Journal ofEmergency Nursing. 32(6):506-508, December 2006.
Cystic Fibrosis Foundation. http://www.cff.org . AccessedAugust 19, 2007.
Flume PA, et al. Cystic fibrosis pulmonary guidelines:Chronic medications for maintenance of lung health. Ameri-can Journal of Respiratory and Critical Care Medicine. 176(10):957-969, November 2007.
Gardner J. What you need to know about cystic fibrosis.Nursing2007. 37(7):52-55, July 2007.
Grosse SD, et al. Newborn screening for cystic fibrosis:Evaluation of benefits and risks and recommendations forstate newborn screening programs. MMWR. 53(RR13):1-36,October 2004.
Grossman S, Grossman LC. Pathophysiology of cysticfibrosis implications for critical care nurses. Critical CareNurse. 25(4): 46-51, August 2005.
Hadjiliadis D. Special considerations for patients with cysticfibrosis undergoing lung transplantation. Chest. 131(4):1224-1231, April 2007.
Kreindler JL, Orenstein DM. Comprehensive care is key tosurvival and quality of life: Monitoring adolescents withcystic fibrosis. Journal of Respiratory Diseases. 27(7):298-306,July 2006.
March of Dimes. Quick reference and fact sheets: Cysticfibrosis. http://www.marchofdimes.com/professionals/14332_1213.asp. Accessed August, 19, 2007.
Minasian C, et al. Cystic fibrosis in neonates and infants.Early Human Development. 81:997-1004, October, 2005.
The Merck Manual for Healthcare Professionals. Cysticfibrosis. http://www.merck.com/mmpe/sec19/ch278/ch278a.html. Accessed August, 19, 2007.
54 Nursing made Incredibly Easy! November/December 2008
Advances intreatment have
extended lifeexpectancy.