Heather Small, Aaron Ranasinghe, Jorge Mascaro, Robert ... Page/2013 CT Forum... · Heather Small,...
12
Heather Small, Aaron Ranasinghe, Jorge Mascaro, Robert Bonser, University Hospital Birmingham NHS Foundation Trust Queen Elizabeth Hospital Birmingham
Transcript of Heather Small, Aaron Ranasinghe, Jorge Mascaro, Robert ... Page/2013 CT Forum... · Heather Small,...
Heather Small, Aaron Ranasinghe, Jorge Mascaro, Robert Bonser,University Hospital Birmingham NHS Foundation Trust
Queen Elizabeth Hospital Birmingham
Introduction� 700,000 patients per annum attend Emergency Department (ED) in
the UK with chest pain
� Commonest 999 call - 30% admissions
� Vulnerable group – sudden onset, pain, anxiety, alone
� Research in ED – ethical dilemmas
Consent to research in the (ED) � Informed Consent (IC)
>24hrs, GCP-ICHGMC ‘no decision about me without me’
� Without IC Autonomy is questionedUnethical practicesHalt novel therapies
� Provisional Consent (PC) <24hrsRelationship - patient Next of Kin
Objective
� To explore the views of patients attitudes to participate in research when being admitted to hospital in the acute phase of chest pain
Methods
� 100 patients previously admitted to the ED with acute Chest Pain
� Cardiology CCU & Cardiac Surgery
� Standardised questionnaire
� Ethics Approval
Questionnaire� Provisional Consent
� Blood Sampling
� Next of Kin
� Lack of Capacity
� Death
� Data
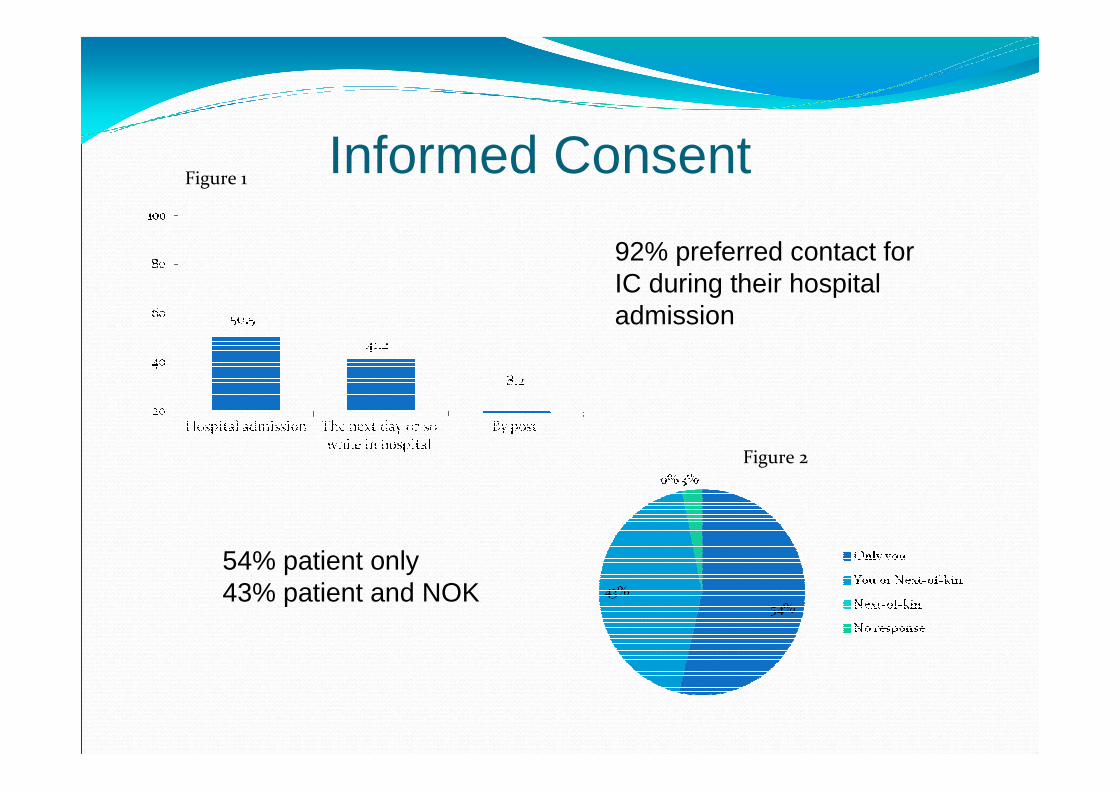
Informed Consent
92% preferred contact for IC during their hospital admission
54% patient only43% patient and NOK
Figure 1
Figure 2
Venesection
� Ninety-three percent of patients supported provisional consent prior blood sample analysis
� 98% accepted storage of samples until IC
� After IC analysis for blood samples for novel biomarkers was acceptable by 97%

• Lack of capacity – 80.4% agreed the researcher could contact their NOK for IC
• Death - Prior to or after IC 78.4% of patients would allow their NOK - IC for analysis of blood samples and review medical notes
Lack of Capacity & Death
Data� 99% content for us access their medical notes – confidential
� 97% supported an ‘expert team’ review scans/x-rays
� 97% agreed to long term outcomes to be tracked via their GP or Office of National Statistics
Summary
� Patients supported research in acute phase of admission with provisional consent and later formal informed consent by themselves or NOK
� Data useful for research in this population of patients
� Patient and Public Involvement
References
� Goodacre S, Cross E, Arnold J, Angelini K, Capewell, The health care burden of acute chest pain.Heat 2005February;91:229-230 doi:10:1136/hrt.2003.027599
� International Conference of Harmonisation – Good Clinical Practice
� Design and implementation of a stand alone chest pain evaluation centre within an academic emergency department .Winchester DE, Stomp D, Shifrin RY, Jois P CritPathw Cardiolo 2012 Sept 11(3): 123-7 doi10:10.1097/HPCOB013e31825d28b9.0
� Rugiomez A, Rodriguez LA, Wallander MA et al,Chest Pain in general practice: Incidence co-morbidity and mortalityFram.PactApr;23(2):167-74.Epub 2006 Feb3
� Clinical research without consent in adults in the emergency setting: A review of patient and public views.Lecoutrier J, Rodgers H, Ford GA, Rapley T, Stobbart Louw SJ,Murtagh MJ,BMC Med Ethics 2008 Apr 29.9.doi10:1186/1472-6939-9