Heart Failure : An Introduction Pathophysiology and Treatment fellowship... · In the diagram the...
83
Heart Failure : An Introduction Pathophysiology and Treatment Allen S. Anderson, MD Medical Director, Bluhm Center for Heart Failure Professor of Medicine, Feinberg School of Medicine
Transcript of Heart Failure : An Introduction Pathophysiology and Treatment fellowship... · In the diagram the...

Heart Failure : An Introduction Pathophysiology and Treatment
Allen S. Anderson, MD Medical Director, Bluhm Center for Heart Failure Professor of Medicine, Feinberg School of Medicine

Case example • 76 year old attorney. 1 week PTA developed
SOB, edema and orthopnea. No chest pain. • Elevated JVP, bilateral rales, ankle edema,
pleural effusions, and a heart rate of 140 BPM. No murmur, rub or gallop. BP 130/80.
• CXR showed CHF. Spiral CT of chest negative for PE. Cardiac enzymes mildly elevated.
• EKG read as sinus tachycardia and poor r progression −> cardiology consult.

1/29/01
76-year-old attorney with effort dyspnea for 1 week:

1/29/01
76-year-old attorney with effort dyspnea for 1 week:

1/30/01 Monitor strip
Right CSM 1/30/01

Case example (continued)
• Treatment – I.V. digoxin & furosemide, oral Lopressor,
nasal O2, ASA, nitrates −> rate slowed −> later atrial fibrillation with pauses.
• Emergency Doppler echocardiogram – Global hypokinesis with EF 15%.
• Continued medical therapy for 3 days until stable with controlled heart rate.

What would you do next?
• A dobutamine stress echo showed significant ischemia and viability.
• A cardiac cath was done next.

Dobutamine Stress Echo showing myocardial viability

Coronary angiogram
Main left: 80%
LAD: 70% diagonal 1
RCA 60% stenosis mid RCA
LV gram: systolic global hypokinesis; EF 35%
To OR CABG
Post op EF = 55% Normal LV

Key Areas of Interest • Is the patient in heart failure? • What is the underlying heart disease? • What caused the heart to fail at this time? • What is the best therapy to correct the
underlying pathophysiology? • And how do we keep the patient out of the
hospital?

Heart Failure Defined
A clinical syndrome characterized by the inability of the heart to generate sufficient cardiac output to meet the metabolic demands of the end organs (despite adequate venous return) or to do so only with increased cardiac filling pressures.

“Congestive” Heart Failure Defined
A clinical syndrome of sodium and water retention leading to breathlessness
caused by neurohormonal activation in the setting of cardiac disease


How long does the physician wait before interrupting a patient giving a medical history?
Answer: 23 seconds
Patient-Physician Communication: Why and How Traveline JM, Ruchinskas R, D’Alonzo Jr GE JAOA. 2005. 105 (No. 1): 13-18



BUN ( Creatinine )
20(1)

Neck Veins Go to YouTube and search for audio version of Dr. Heywood’s neck vein video. Also check out a search for S3 and S4 to see a
video of how to pick up certain sounds and murmurs.




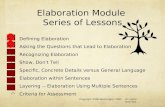
CC: Chest pressure for 2 hours HPI: 50 YO diabetic businessman had CABG 9 years ago & 2 hrs ago awoke at 2 AM with new substernal chest pressure 5/10 with SOB but no dizziness, nausea, vomiting or sweating. Pressure increased despite sitting up & 1 TNG and he called 911. He also has HTN, high chol & smokes 1 PPD. In the ED he had positive markers and EKG changes of an anterior STEMI and a new murmur typical for a VSD. CXR showed HF.

CC
HPI
Risk Factors Pertinent Positives
Pertinent Negatives
Target Organ Involvement Complications
CC: Chest pressure for 2 hours HPI: 50 YO diabetic businessman had CABG 9 years ago & 2 hrs ago awoke at 2 AM with new substernal chest pressure 5/10 with SOB but no dizziness, nausea, vomiting or sweating. Pressure increased despite sitting up & 1 TNG and he called 911. He also has HTN, high chol & smokes 1 PPD. In the ED he had positive markers and EKG changes of an anterior STEMI and a new murmur typical for a VSD. CXR showed HF.
In the diagram the parts of the HPI are in darker blue and are really elaboration of the CC. The illustrated story (yellow text box) is condensed but includes his coronary risk factors, pertinent positive and negative symptoms, target organ involvement (acute MI) and two complications (VSD and heart failure). In a full illustration there would be much more detail: “Little things are infinitely the most important.” Also note the HPI clearly begins years before the CC and is written in chronological order.

4 basic clinical principles will help lead to the correct diagnosis and treatment
• Don’t take the history from the patient; allow the person to tell his or her story.
• Observe. Selective attention is the heart of the physical examination.
• When ordering a laboratory test, know what question you want answered and be sure to check on the results.
• If an organ or an organ system fails, look for a precipitating cause.

With experience, one day you will be able to select from the myriad of details in the H&P what is relevant, pertinent or critical from what is not.

Cardiac Physiology

Circulatory System
Heart: Generates pressure and flow Blood vessels: Conduit plus
•Large arteries: distribution, elastic recoil •Arterioles: resistance •Capillaries: exchange •Veins: capacitance (storage)
Blood: an anticoagulated pick up and delivery system


Prime Determinants of LV Function (and MVO2)
• Heart rate • Contractility • Preload • Afterload
.

Load = Wall Stress
• Wall stress ~ Pressure x Volume • Preload is mostly volume • Afterload is mostly pressure

A B
C D
Load = Wall Stress = ∆P x R LaPlace
R R

Pathophysiology of heart failure

LV DYSFUNCTION
• Systolic –Trouble emptying –Inotropy
• Diastolic –Trouble filling –Lusitropy

Systolic and Diastolic Dysfunction
EF decreased EF normal or increased
Normal Systolic Dysfunction
Diastolic Dysfunction

Myocardial injury
Cardiac function
Activation of Neurohormonal systems (SNS, RAAS, etc.)
Acute
(Adaptive) Chronic
(Maladaptive)
CURRENT PARIDIGM FOR HEART FAILURE
Adapted from E. Braunwald. 1999

Myocardial injury
Cardiac function
Activation of Neurohormonal systems (SNS, RAAS, etc.)
Acute
(Adaptive) Chronic
(Maladaptive)
CURRENT PARIDIGM FOR HEART FAILURE
Blockers
Adapted from E. Braunwald. 1999

Frank-Starling Mechanism Normal and Heart Failure

ACC/AHA Recommendations Class I
• History & Physical – family history – functional capacity – Labs
• Echocardiogram—2D/doppler • Chest X-Ray • ECG • Cardiac Catheterization
– Angina, if candidate for revascularization

History
• Previous cardiac disease, including childhood • Other medical diseases • Exposure to cardiotoxins
– ETOH, illicit drugs, chemotherapy, chest XRT • Pregnancies/complications • Syncope • Embolic events

Heart Failure Symptoms & Signs
• Dyspnea • Orthopnea • PND • Wheezing • Edema • Abdominal discomfort • Anorexia/early satiety • Fatigue
• Rales or Clear Lungs • S3 Gallop • Displaced PMI/LV heave • Audible wheezing • Hepatic congestion • Cool extremities • Oliguria • Altered mental status

Facial Urination due to Congestive Heart Failure
To the Editor.—We recently saw a patient in congestive heart failure whose main complaint was wetting his face every time he urinated. This case report describes this unusual presentation.
Comment.—Severe angulation of the penis, due to congestive heart failure, is a very unusual finding. A review of standard urological texts does not mention such a complication.
Gould L, Martinucci L, Patel C. JAMA. 1986:255:2448.
“An 87-year old man was admitted to the hospital because of swelling of his legs and his urine hitting him in the face….The scrotum was edematous and the penis was folded on itself and directed at the patient’s head.”

Classification of Heart Failure The New York Heart Association (NYHA) classification system1-3 Functional Capacity Objective Assessment Class I: No limitation A. No CV disease Class II: Slight limitation B. Minimal CV disease Class III: Marked limitation C. Moderate CV disease Class IV: Symptoms at rest D. Severe CV disease
1. ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure. 2001. Available at: http://www.acc.org/clinical/guidelines/failure/hf_index.htm. Accessed September 18, 2003; 2. Gomberg-Maitland et al. Arch Intern Med. 2001;161:342-352; 3. Packer and Cohn, eds. Am J Cardiol. 1999;83(suppl 2A):1A-38A.
High risk with no symptoms
Structural heart disease with no
symptoms
Structural heart disease with symptoms
(dyspnea, fatigue, reduced exercise
tolerance)
Refractory symptoms
requiring special interventions
A B C D

Evolution of HF Therapy
Period Clinical Endpoint Pathophysiology Therapy
Pre-1970 Edema Na+ retention Diuretics
1970-1985 Symptoms Hemodynamics Inotropes Vasodilators Diuretics
1985-1995 Survival Neurohormonal Activation
ACE I’s β-blockers
1995- Cellular mechanism
Apoptosis Antioxidants Cytokine antagonists NO-regulators

Non- cardiac factors
Low ejection fraction
Arrhythmia
Death
Pump failure
Symptoms: Dyspnea Fatigue Edema
Chronic heart failure
• Neurohormonal stimulation
• Endothelial dysfunction
• Vasoconstriction • Renal sodium retention
Adapted from: Cohn JN. N Engl J Med. 1996;335:490-498.
Pathogenesis of Systolic Heart Failure HFrEF
Remodeling
Left ventricular dysfunction
• Coronary artery disease
• Hypertension • Cardiomyopathy • Valvular disease

Stages, Phenotypes and Treatment of HF

Major Therapeutic Options for HFrEF
•ACE inhibitor
•Aldosterone receptor blocker
•Angiotensin receptor blocker (if ACE-I intolerant)
•Beta-blocker
•Diuretic
•Digoxin
Adapted from: ESC Task Force; 2001 ACC/AHA Guidelines.

Trial ACE-I (%) RR (95% CI)
Mortality
CONSENSUS I
SOLVD (Treatment)
SOLVD (Prevention)
Heart Failure
Post-MI
TRACE (trandolapril)
0.56 (0.34–0.91)
0.82 (0.70–0.97)
0.92 (0.79–1.08)
0.81 (0.68–0.97)
0.73 (0.60–0.89)
SMILE (zofenopril) 0.75 (0.40–1.11)
Totals
0.78 (0.67–0.91)
39
35
15
20
17
5
35
21
Controls (%)
54
40
16
25
23
6.5
42
25
Effect of ACE Inhibitors on Mortality in Heart Failure Patients
SAVE (captopril)
AIRE (ramipril)

RAAS in Heart Failure Angiotensinogen
( Liver )
Angiotensin I
Angiotensin II
AT1 AT2
AT1 Receptor Blocker
ACE Inhibitor
Renin Inhibitor -
- -
JG cells: Renin
ACE

Hypokalemia, Hypomagnesemia,
arrhythmias
Pathologic LVH/myocardial
fibrosis
The Renin Angiotensin Aldosterone System
Elevated ALDOSTERONE
Fluid retention And edema
Morbidity Mortality
Angiotensinogen
Angiotensin I
Angiotensin II
Heart Failure
Renin
ACE ACEI reduces Angiotensin II levels
ACTH
Other
K+ ↑
Na+ ↓

ACE INHIBITORS
• Approximately 7000 patients enrolled in clinical trials
• Improvement in cardiac function, symptoms, and clinical status
• Decrease in all cause mortality by 20%-25% • Decrease in combined risk of death or
hospitalization by 25%-30%

Myth: ARBs are ACE inhibitors that do not cause a cough.
I. M. Grais, M.D.

ACE Inhibitor plus Spironolactone 25 mg/day Further Reduces Mortality
0 6 12 18 24 30 36
Months
Risk reduction 30% P <0.0001
Spironolactone
Placebo
0.45
0.50
0.55
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Prob
abili
ty o
f sur
viva
l
Pitt B, Zannad F, Remme WJ, et al. N Engl J Med. 1999;341:709-717.

↑ CNS sympathetic outflow
↑ Cardiac sympathetic activity ↑ Renal sympathetic activity
Sodium retention Myocyte hypertrophy
Myocyte injury Increased arrhythmias
Disease progression
α1 β1 β1 β2 α1
↑ Vascular sympathetic activity
Vasoconstriction
α1
Activation of RAS
Adrenergic Pathway in Heart Failure Progression

Effect of Beta-Blockers on Mortality in Heart Failure Patients
34% lower risk (0.53–0.81) P=0.0062 after adjusted interim analysis
MERIT-HF (metoprolol)
34% lower risk P< 0.0001
CIBIS-II (bisoprolol)
38% lower risk (18%-53%) P< 0.001
US Carvedilol
35% lower risk*
COPERNICUS (carvedilol)
8.5% lower risk P=NS
BEST (bucindolol)
Clinical Trial
All-cause mortality
All-cause mortality
Combined end point: risk of hospitalization or death
All-cause mortality
All-cause mortality
Trial End Point Risk Reduction, % (95% CI)
*Preliminary data from XXII Congress of the European Society of Cardiology



Effectiveness of Individual Therapies in Preventing Events
From Evidence-Based Trials
DIG trial / 3 years
-
40
Digoxin
RALES trial / 2 years
57
138
Spironolactone
MERIT-HF study / 1 year
38
65
Beta-Blockers
Treatment arm of the SOLVD trial / 3.5 years
13
99
ACE-I
Evidence-Based Trial / Average Follow-Up
Deaths (prevented)
Hospital Admissions (prevented)
Therapy
Adapted from: Remme WJ et al. Eur. Heart J. 2001;22:1527-1560.
Events prevented per 1000 patient-hours of treatment

HF Preserved Systolic Fxn HFpEF

Diastolic Dysfunction: “The Devil is in Diastole”
• Fibrosis • Hypertrophy • Ischemia • Restrictive cardiomyopathy • Myocardial infarction

Treatment of HFpEF Recommendations COR LOE
Systolic and diastolic blood pressure should be controlled according to published clinical practice guidelines I B
Diuretics should be used for relief of symptoms due to volume overload I C
Coronary revascularization for patients with CAD in whom angina or demonstrable myocardial ischemia is present despite GDMT
IIa C
Management of AF according to published clinical practice guidelines for HFpEF to improve symptomatic HF
IIa C
Use of beta-blocking agents, ACE inhibitors, and ARBs for hypertension in HFpEF IIa C
ARBs might be considered to decrease hospitalizations in HFpEF IIb B
Nutritional supplementation is not recommended in HFpEF
III: No Benefit C

Acute Heart Failure
Diagnosis and Treatment

Diagnosis of CHF: Clinical Challenge
• Symptoms and signs of heart failure like shortness of breath and edema have a broad differential diagnosis
• Physical exam is neither sensitive nor specific for CHF and, even in good hands, there are often errors
• CXR findings have limited accuracy for CHF • One-third to one-half of patients with CHF have
normal systolic function Maisel A. et al. J Am Coll Cardiol 2001;37(2):379-85
Presenter
Presentation Notes
Slide 11 The diagnosis of HF is a difficult one to make. Shortness of breath is a symptom associated with many disease states; physical examination is neither sensitive nor specific for CHF. One-third to one-half of patients with CHF have normal pumping function of the heart. Echocardiograms are useful for diagnosis of HF, and provide information to aid in estimating the ejection fraction. The procedure serves as an expensive means to rule in or rule out patients for HF. Echocardiograms are not always available, and require sophisticated technicians and interpretation.

The Physical Exam As A Diagnostic Test
PCWP>20- 22 mmHg Sensitivity Specificity Can’t tell
Orthopnea 90% 95% JVP inc. 80% 98% 15% Valsalva 90% 90% 25% HJ Reflux 92% 81% ? Perip edema 25% 95% 5% Rales 15% 95%
From Ewy, McIntyre et al, Stevenson & Perloff, Zema et al.

Invasive Hemodynamic Assessment
• Invasive • Significant Complications • Expensive • Requires ICU or Cath Lab setting • Data sometimes difficult to interpret

Goals of Acute HF Therapy
• Alleviate symptoms • Treat volume overload • Preserve/improve end organ function • Limit hospitalization • Initiate/optimize chronic therapy • Prevent readmission • Improve long-term outcomes

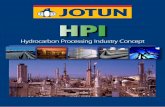
Rapid Assessment of Hemodynamic Status
Congestion at Rest
Low Perfusion
at Rest C
NO
NO YES
YES
L
A B Warm &
Dry Warm &
Wet
Cold & Wet Cold & Dry
(Complex) (Low Profile)
Signs/Symptoms of Congestion:
Orthopnea / PND JV Distension Hepatomegaly Edema Rales (rare in chronic
heart failure) Elevated est. PA
systolic Valsalva square wave
Possible Evidence of Low Perfusion: Narrow pulse pressure Cool extremities Sleepy / obtunded Hypotension with ACE inhibitor Low serum sodium Renal Dysfunction (one cause)
Presenter
Presentation Notes
Slide 20 The hemodynamic profiles of patients with advanced HF. The majority (90%) of patients presenting with acute decompensated HF are volume overloaded (“wet”). These patients may have cardiac index that is unchanged or decreased. Most patients with decreased cardiac index have elevated systemic vascular resistance, though a minority will have unchanged or low SVR. The signs and symptoms of congestion include orthopnea, jugular venous distention, and peripheral edema. Signs and symptoms of low perfusion include narrow pulse pressure, cool extremities, and decreased mental status.

Current Treatment of Acute Heart Failure
Diuretics Aquaretics
Ultrafiltration
Reduce fluid
Volume Na+
& H20
Vasodilators
Decrease Preload
And Afterload
Inotropes
Augment Contract-
ility
Presenter
Presentation Notes
Slide 27 Patients with HF frequently present to the hospital with worsened symptoms in a hypervolemic state. Therapy may initially target this excess fluid incorporating diuretics along with vasodilators to help reduce the overloaded state. Current therapies offer symptomatic benefits to patients with HF. Diuretics reduce fluid volume resulting in decreased pulmonary congestion and swelling of extremities. Vasodilators decrease blood vessel constriction, reducing preload and afterload, improving ventricular function and cardiac output. Inotropic agents stimulate the heart muscle, increasing contractility and cardiac output.


Diuretic Resistance • Poor oral absorption due to gut edema • Decreased perfusion of kidney results in decreased delivery
of loop diuretics • Decreased GFR results in decreased filtered load of sodium • Volume depletion activates plasma renin activity and
stimulates SNS • Increased proximal tubule reabsorbtion of sodium,
particularly in setting of elevated AII and elevated catecholamine levels
• Increased distal reabsorbtion of sodium, stimulated by aldosterone
• Associated with tubular hypertrophy: resetting basal rates of sodium reabsorbtion.

Diuretic Principles
• The right dose is what it takes to effect diuresis – as high as it takes – as low as you can
• High dose loop vs loop+metolazone • Continuous IV infusion of loop diuretic • Flexible dosing • Daily weights

Most Common IV Medications All Enrolled Discharges (n=105,388) October 2001-January 2004
0 10 20 30 40 50 60 70 80 90
100
Patie
nts
(%)
IV Diuretic Dobutamine Dopamine Milrinone Nesiritide Nitroglycerin Nitroprusside
IV Vasoactive Meds
88%
6% 6% 10% 3% 1%
10%
Presenter
Presentation Notes
Most Common IV Medications�All Enrolled Discharges (N = 105,388) October 2001–January 2004 The use of IV vasoactive medications is shown on this slide. IV diuretics are used in 88% of patients admitted with ADHF. Data on file, Scios Inc.

Colors of Salt
• White • Black • Red • Yellow • Green • Brown • Clear
• Table salt • Soy sauce • Catsup • Mustard • Pickles • Soups & gravies • Saline

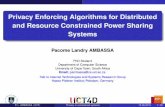
Profiles and Therapies of Advanced Heart Failure
Yes
R. Bourge, UAB Cardiology (adapted from L. Stevenson) Stevenson LW. Eur J Heart Failure 1999;1:251-257
No Warm and Dry PCW and CI
normal
Warm and Wet PCW elevated
CI normal
Cold and Wet PCW elevated CI decreased
Cold and Dry PCW low/normal
CI decreased
Vasodilators Nitroprusside Nitroglycerine
Nesiritide Relaxin
Inotropic Drugs Dobutamine
Milrinone Calcium Sensitizers
Nl SVR High SVR
Congestion at Rest
Low Perfusion
at Rest
No
Yes
Presenter
Presentation Notes
Slide 21 The hemodynamic profiles of patients with advanced HF. The majority of patients with heart failure are volume overloaded (“wet”). These patients may have cardiac index that is unchanged or decreased. Most patients with decreased cardiac index have elevated systemic vascular resistance, though a minority will have unchanged or low SVR. Vasodilators would be expected to have therapeutic benefits in the “wet and warm” and the majority of “wet and cold patients.” While intravenous intropic therapy is often employed to reduce filling pressures and improve cardiac output, intravenous vasodilator therapy in the setting of vasoconstriction can often achieve similar results without the risks of aggravating ischemia and arrhythmias, and with easier transition to oral vasodilator regimens. Patients with signs of systemic hypoperfusion that are “dry” would be expected to have therapeutic benefits with volume loading and/or inotropic agents.

Preload: diuretics-thiazides, loop, aldosterone antagonists, RAAS inhibition Afterload: vasodilators, nitrates, hydralazine, RAAS inhibition (ACEI, ARBs), recombinant B-type natriuretic peptide, now new LCZ696 which raises natriuretic peptides in combination with enalapril Contractility: digitalis, Beta-blockers, phosphodiesterase inhibitor Heart Rate: digitalis, Beta-blockers

A man with known ischemic cardiomyopathy and an ejection fraction of 0.15% on good therapy entered the ED with newly increased heart failure. His B-type natriuretic peptide (BNP) level was 2,000 pg/mL.
What is the key question the cardiologist asks the resident?

The attending asked the ED resident, “Why is he in heart failure?” When the medical resident said that he didn’t know, the attending asked, “Has anything changed in recent weeks?”

80 YO man with dementia & Parkinson’s was admitted with pneumonia and a fever of 103F. Rx: I.V. fluids and antibiotics. He developed severe dyspnea due to pulmonary edema. EKG showed sinus rhythm at 60 BPM but no acute changes.
What key question did the consulting cardiologist ask?

Why, he wondered, would an elderly man with pneumonia, a high fever, and pulmonary edema not have sinus tachycardia?
Two common causes for such a paradoxical finding would be sick sinus syndrome and hypothyroidism. TFTs confirmed the suspected severe hypothyroidism.

Gregory: “Is there any point to which you would wish to draw my attention?” Holmes: “To the curious incident of the dog in the nighttime.” Gregory: “The dog did nothing in the nighttime.” Holmes: “That was the curious incident.”
The Dog in the Nighttime Syndrome

“It is much more important to know what sort of a patient has a disease than what sort of a disease a patient has.”
Sir William Osler

“The art of the practice of medicine is to be learned only by experience; ‘tis not an inheritance; it cannot be revealed. Learn to see, learn to hear, learn to feel, learn to smell, and know that by practice alone can you become expert.”
Osler, The Teacher, p. 198

Fini

Therapy CO PCWP BP HR Arrhy thmia
Shorter Onset
Longer Offset
Dopamine (ng/kg/min) Low (<3) Mod (3–7) High (7–15)
↔ ↑
↑↑
↔ ↔ ↔
↔ ↑
↑↑
↔ ↑
↑↑
↔ ↑↑
↑↑↑
+++ +++ +++
0 0 0
Dobutamine ↑↑↑ ↓ ↔ ↑ ↑↑ +++ 0
Milrinone ↑↑ ↓ ↓ ↑ ↑↑ + ++
Nitroglycerin ↑ ↓↓ ↓↓ ↔ ↔ +++ 0
Nesiritide ↑ ↓↓ ↓ ↔ ↔ ++ ++
Nitroprusside ↑ ↓↓ ↓↓↓ ↔ ↔ ++++ 0 ↑ increase; ↓ decrease; + effect (number of and qualitatively associated with degree of effect); 0 no effect
Intravenous Agents for Heart Failure
Reference: Adapted from Young JB. Rev Cardiovasc Med .2001;2(suppl 2):S19.
Presenter
Presentation Notes
IV Agents for HF The relative benefits and possible limitations of IV HF therapies are summarized. Unlike other agents, including positive inotropes, nesiritide administration leads to a beneficial increase in cardiac output as well as decreases in PCWP and blood pressure, without affecting heart rate or rhythm. Young JB. Rev Cardiovasc Med. 2001;2(suppl 2):S19