Heart. Congestive heart failure or heart failure : condition : heart is unable to adequately pump...
110
Heart
-
Upload
erick-reynolds -
Category
Documents
-
view
222 -
download
2
Transcript of Heart. Congestive heart failure or heart failure : condition : heart is unable to adequately pump...

Heart


Congestive heart failure
• or heart failure : condition : heart is unable to
adequately pump blood throughout the body
• Characterized :
– shortness of breath (dyspnea) – abnormal fluid retention, which
usually results in swelling (edema) in the feet and legs.

Heart failure
• Left-sided heart failure
• Right-sided heart failure

Left-sided heart failure. When LV cannot adequately
pump blood out of the left atrium, or when one or more of the heart valves becomes leaky or narrowed (stenotic), blood can "back up" into the lungs

left-sided heart failure: • lungs become congested with fluid
(called pulmonary edema), – causing difficulty breathing and– interfering with the movement of
oxygen from the lungs into the bloodstream, causing fatigue.

Right-sided heart failure • abnormality or condition affects
the flow of blood through the right ventricle, pressure in the blood vessels increases and fluid is forced from the blood vessels into body tissues.
• causes swelling (edema), usually in the feet and legs, and sometimes, in the abdomen.

The NYHA functional class
(the New York Heart Association)
• determine how much CHF limits their lifestyle
• Useful in following the course of disease and assessing the effects of therapy
• Aid in the dental management

Class I: No symptoms at any level of exertion,
no limitation of physical activity
Class II: Slight limitation of physical activity.
Fatigue, palpitations and dyspnea with
ordinary physical activity but
comfortable at rest
Class III: marked limitation of activity. Less than
ordinary physical activity results in symptoms,
but patients are comfortable at rest
Class IV: Symptoms are present at rest, and any
physical exertion exacerbates the symptoms

Congestive heart failureCongestive heart failure
Potential problem related to dental care
1. sudden death from cardiac arrest or
arrhythmia
2. Myocardial infarction
3. CVA
4. Infective endocarditis if CHF is caused
by rheumatic heart dis., congenital
heart dis.

CHFCHF
Potential problem related to dental care 5. Shortness of breath 6. Drug side effects : orthostatic hypotension (diuretics,vasodilators) arrhythmia (digoxin overdose) nausea, vomiting (digoxin, vasodilators) palpitations (vasodilators) 7. Infection

Prevention of complication 1. Detection and referral to physician 2. No routine dental care until under good
medical management (class I or II and possibly III)
3. Good medical management – cause of heart failure
- hypertension - valvular dis. (rheumatic heart dis.) - congenital heart dis., MI - Renal failure - Thyrotoxicosis - chronic obstructive lung disease
4. Class I or II, use max. 0.036 mg epinephrine
avoid vasoconstrictors in class III or IV
5. Semisupine or upright position
(decrease collection of fluid in lung)
6. Terminate appointment if patient becomes fatigue
7. Drug considerations
digitalis – N/V
anticoagulants - PT = 2times or less,
- INR = 3.0 or less
antidysrhythmic agents, antihypertensive
avoidance of outpatient general anesthesia

CHFCHF
Emergency care
1. Conservative in acute congestive failure:
drug for pain control and
antibiotics for infection
2. Under good medical management:
deal with underlying cause and presence of
any complications in dental management

Endocarditis
• Inflammation of endocardium
• most common structures involved are the heart valves.
• Endocarditis can be classified by etiology as either infective or non-infective

Infective endocarditis
• valves of the heart do not actually receive any blood supply of their own, defense mechanisms (such as white blood cells) cannot enter.
• If an organism (such as bacteria) hold on the valves, the body cannot get rid of them.

• If valve damaged (for instance in rheumatic fever) bacteria have a chance to hold.
• clinically divided into
–acute and subacute endocarditis.
This classifies both the tempo of progression and severity of disease.

• Subacute bacterial endocarditis (SBE) : often due to streptococci of low virulence and mild to moderate illness which progresses slowly over weeks and months
• Acute bacterial endocarditis (ABE) : fulminant illness over days to weeks,
more likely due to Staphylococcus aureus (greater virulence, or disease-producing capacity)

Aetiology and pathogenesis• altered blood flow around the valves is a
risk factor in obtaining endocarditis.
• The valves may be damaged congenitally, from surgery, by auto-immune mechanisms, or simply as a consequence of old age.
• The damaged part of a heart valve becomes covered with a blood clot, a condition known as non-bacterial thrombotic endocarditis (NBTE).

• In healthy individual, a bacteraemia would normally be cleared quickly with no adverse consequences.
• If a heart valve is damaged and covered with a piece of a blood clot, the valve provides a place for the bacteria to attach themselves and an infection can be established.
• The bacteraemia is often caused by minor dental procedures, such as a tooth removal.
• Another causes result from a high number of bacteria getting into the bloodstream. (Colorectal cancer, serious urinary tract infections and IV drug use)
• With a large number of bacteria, even a normal heart valve may be infected.
• A more virulent organism (Staphylococcus aureus) is usually responsible for infecting a normal valve.

• Intravenous drug users : right heart valves infected (veins that are injected enter the right side of the heart)
• The injured valve is most commonly affected when there is a pre-existing disease. (rheumatic heart disease this is the aortic and the mitral valves) : left heart valves

Clinical and pathological features
• Fever (often spiking)
• Continuous presence of micro-organisms in the bloodstream determined by serial collection of blood cultures
• Vegetations on valves on echocardiography
• Septic emboli, causing circulatory problems (stroke, gangrene of fingers)
• Chronic renal failure
Clinical and pathological features• Osler's nodes (painful subcutaneous lesions
in the distal fingers) • Janeway lesions (painless hemorrhagic
cutaneous lesions on the palms and soles) • Roth spots on the retina • Conjunctival petechiae • A new or changing heart murmur,
particularly murmurs suggestive of valvular incompetence
• Splinter haemorrhages

Micro-organisms responsible• Many types of organism • isolated by blood culture• Alpha-haemolytic streptococci,
that are present in the mouth will often be the organism isolated if a dental procedure caused the bacteraemia.

• If bacteraemia was introduced through the skin, such as contamination in surgery, during catheterisation, or in an IV drug user
Staphylococcus aureus
• A third important cause of endocarditis is Enterococci (abnormalities in the gastrointestinal or urinary tracts)
• Enterococci : causes of nosocomial or hospital-acquired endocarditis.
• alpha-haemolytic streptococci and Staphylococcus aureus : causes of community-acquired endocarditis.

Treatment• High dose antibiotics ( by intravenous
route) • Antibiotics are continued for a long time,
typically two to six weeks.• Surgical removal of the valve is necessary
in patients who fail to clear micro-organisms from their blood in response to antibiotic therapy, or in patients who develop cardiac failure resulting from destruction of a valve

• A removed valve is usually replaced with an artificial valve which may either be mechanical (metallic) or obtained from an animal such as a pig (bioprosthetic valves)
• Infective endocarditis is associated with a 25% mortality.

ENDOCARDITIS RISK STRATIFICATIONENDOCARDITIS RISK STRATIFICATION
Endocarditis prophylaxis recommended
High risk• Prosthetic heart valves• Prior bacterial endocarditis• Complex cyanotic congenital heart disease• Surgically constructed systemic
pulmonary shunts or conduct

ENDOCARDITIS RISK STRATIFICATIONENDOCARDITIS RISK STRATIFICATION
Endocarditis prophylaxis recommended
Moderate risk
• Most other congenital cardiac malformations
• Acquired valvular dysfunction
• Hypertrophic cardiomyopathy
• Mitral valve prolapse with regurgitations and/or thickened leaflets

ENDOCARDITIS RISK STRATIFICATIONENDOCARDITIS RISK STRATIFICATION
Endocarditis prophylaxis not recommendedNegligible risk• Isolated secundum atrial septal defect• Surgical repair of ASD, VSD, or PDA (without
residua beyond 6 mo.)• Prior coronary artery bypass graft• Mitral valve prolapse without regurgitation• Physiologic, functional, or innocent heart
murmurs

ENDOCARDITIS RISK STRATIFICATIONENDOCARDITIS RISK STRATIFICATION
Endocarditis prophylaxis not recommended
Negligible risk• Previous Kawasaki dis. without valvular
dysfunction• Previous rheumatic fever without valvular
dysfunction• Cardiac pacemakers and implanted
defibrillators

DENTAL AND ORAL SURGERY PROCEDURES DENTAL AND ORAL SURGERY PROCEDURES AND ENDOCARDITIS PROPHYLAXISAND ENDOCARDITIS PROPHYLAXIS
Endocarditis prophylaxis recommended in high- and moderate-risk cardiac conditions • Exodontia• Periodontal procedures• Incision and drainage of abscesses• Dental implant placement and uncovering• Reimplantation of avulsed teeth• Endodontic therapy or apical surgery • Placement of intermaxillary fixation

DENTAL AND ORAL SURGERY PROCEDURES DENTAL AND ORAL SURGERY PROCEDURES AND ENDOCARDITIS PROPHYLAXISAND ENDOCARDITIS PROPHYLAXIS
Endocarditis prophylaxis recommended in
high- and moderate-risk cardiac conditions • Reduction of contaminated maxillofacial
fractures• Osteotomies• Subgingival placement of antibiotic fibers or
strips• Intraligamentary LA injections • Prophylactic dental or implant cleaning• Intraoral biopsies
DENTAL AND ORAL SURGERY PROCEDURES DENTAL AND ORAL SURGERY PROCEDURES AND ENDOCARDITIS PROPHYLAXISAND ENDOCARDITIS PROPHYLAXIS
Endocarditis prophylaxis not recommended • Restorative dentistry• Nonintraligamentary LA injections• Postoperative suture removal• Placement of removable orthodontic or
prosthodontic appliances• Taking oral impressions• Shedding (naturally) of primary teeth

ANTIBIOTIC PROPHYLACTIC REGIMENS FOR ANTIBIOTIC PROPHYLACTIC REGIMENS FOR DENTAL DENTAL
AND ORAL SURGICAL PROCEDURESAND ORAL SURGICAL PROCEDURES
circumstance drug regimen
Standard prophylaxis
amoxicillin Adults : 2 g po
Children : 50 mg/kg po
1 hr before procedure
Unable to take oral medications
ampicillin Adults : 2g IM or IV
Children : 50 mg/kg IM or IV
Within 30 min of procedure
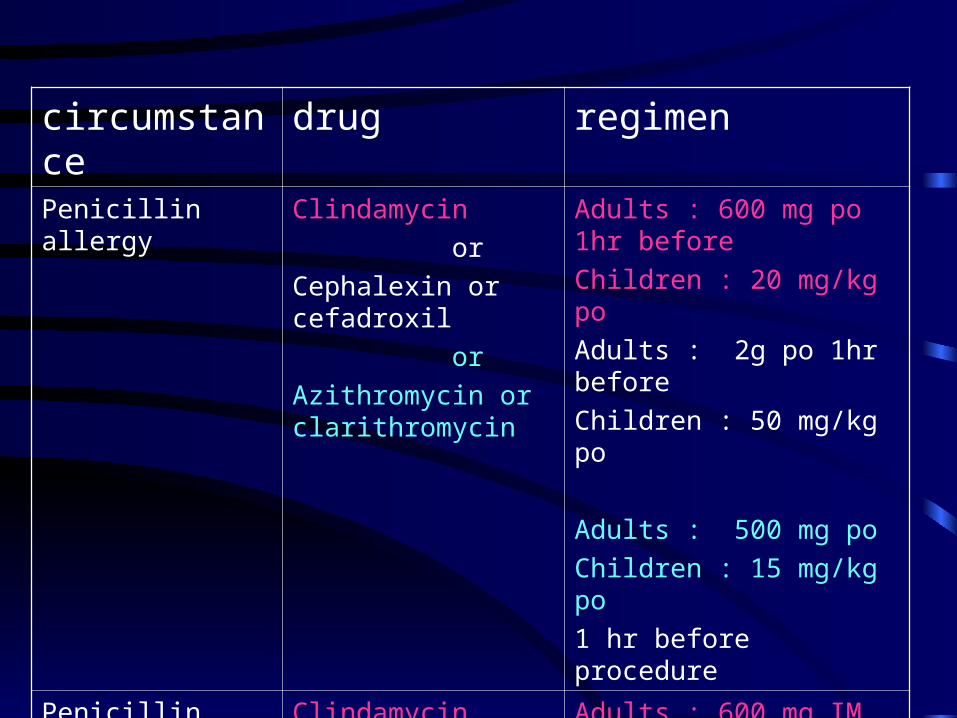
circumstance drug regimenPenicillin allergy Clindamycin
or
Cephalexin or cefadroxil
or
Azithromycin or clarithromycin
Adults : 600 mg po 1hr before
Children : 20 mg/kg po
Adults : 2g po 1hr before
Children : 50 mg/kg po
Adults : 500 mg po
Children : 15 mg/kg po
1 hr before procedure
Penicillin allergy and unable to take oral medications
Clindamycin
or
cefazolin
Adults : 600 mg IM or IV
Children : 20 mg/kg IM or IV
within 30 min of procedure
Adults : 1 g IM or IV
Children : 25 mg/kg IM or IV
within 30 min of procedure

Congenital heart disease
• defect of heart that exists primarily at birth
• environmental, such as chemicals, drugs, or infection (i.e. rubella)
• genetic
• mother's excessive intake of alcohol and drugs while pregnant

Classifications
• Acyanotic
• Cyanotic

• Cyanotic : Disorders that cause profusion or an
insufficient amount of oxygen in the blood pumped throughout the body (bluish-grey discoloration of the skin)
• truncus arteriosus, total anomalous pulmonary venous return, tetralogy of Fallot, transpositon of the great arteries, and tricuspid atresia.

Types of congenital heart disease
• Patent ductus arteriosus
• Obstruction defects :
pulmonary valve stenosis
aortic valve stenosis
coarctation of the aorta
• Septal defects

Signs and Symptoms
related to the type and severity of defects.
• no signs
• exhibit shortness of breath,
• cyanosis, chest pain, syncope, sweating, heart murmur, respiratory infections, underdeveloping of limbs and muscles, poor feeding, or poor growth

Patent ductus arteriosus
• In developing fetus, ductus arteriosus (DA) is a shunt connecting the pulmonary artery to the aortic arch
• allows blood from the right ventricle to bypass the fetus' fluid-filled lungs.
• During fetal development, shunt protects the lungs from being overworked and allows the right ventricle to strengthen.

• first breath, the lungs open and pulmonary pressure decreases below that of the left heart.
• At the same time, the lungs release bradykinin to constrict the smooth muscle wall of the DA and reduce blood flow.
• reduced pulmonary resistance, more blood flows from the pulmonary arteries to the lungs and lungs deliver more oxygenated blood to the left heart. This further increases aortic pressure so that blood no longer flows from the pulmonary artery to the aorta via the DA.

PDA
• normal newborns, DA is closed within 15 hours after birth, and is completely sealed after three weeks.
• A nonfunctional vestige of the DA, called ligamentum arteriosum, remains in the adult heart.
• not close in the newborn, the blood that is suppose to flow through the aorta goes to the lungs : PDA
• common in premature infants


Signs and symptoms
• oxygenated blood flow from aorta to pulmonary arteries
• some of infant's oxygenated blood does not reach the body, and the infant becomes short of breath and cyanotic.
• Tachycardia : increasing the speed with which blood is oxygenated and delivered to the body
• Untreated : suffer from congestive heart failure

Atrial septal defects (ASD)
• communication between atria of the heart and may involve the interatrial septum.
• possible for blood from left side of heart to right side,
• or resulting in mixing of arterial and venous blood

• foramen ovale remains open during fetal development (allow blood from the venous system to bypass the lungs and go to the systemic circulation)
• prior to birth, the oxygenation of the blood is via the placenta and not the lungs.
• A layer of tissue begins to cover the foramen ovale during fetal development, and will close completely soon after birth
• After birth, pressure in the pulmonary circulation drops, and foramen ovale closes

• approximately 30% of adults the foramen ovale does not seal over.
• In this case, elevation of pressure in the pulmonary circulation (ie: pulmonary hypertension) can cause opening of the foramen ovale. This is known as a patent foramen ovale (PFO).

• right ventricle have to push out more blood than the left ventricle due to the left-to-right shunt.
• Eventually the pulmonary vasculature will develop pulmonary hypertension to try to divert the extra blood volume away from the lungs.

• lead to right ventricular failure (dilatation and decreased systolic function of the right ventricle) or elevations of the right sided pressures to levels greater than the left sided pressures.
• uncorrected, pressure in right side > left side
• cause pressure in right atrium > left atrium This will reverse the pressure gradient across the ASD, and the shunt will reverse; a right-to-left shunt will exist.
• Once right-to-left shunting occurs, a portion of oxygen-poor blood will get shunted to the left side of the heart and ejected to the peripheral vascular system. This will cause signs of cyanosis
types of atrial septal defects.
• They are differentiated – involve other structures of the heart and– how they are formed during the developmental
process during early fetal development

1. Ostium secundum atrial septal defect
• most common type of ASD• 6-10% of all congenital heart diseases• usually from :
– enlarged foramen ovale, – inadequate growth of the septum secundum, – or excessive absorption of the septum primum.
• 10 to 20 percent of individuals with ostium secundum ASDs also have mitral valve prolapse
Complications of an uncorrected secundum
ASD
• pulmonary hypertension,
• right-sided heart failure,
• atrial fibrillation or flutter,
• stroke
• Eisenmenger's syndrome.

2. Ostium primum atrial septal defect
• endocardial cushion defect
• defect in the atrial septum at the level of the tricuspid and mitral valves
• often involves the endocardial cushion
most common congenital heart defect that is
associated with Down's syndrome

3. Sinus venosus atrial septal defect
• defect in the septum involves the venous inflow (superior vena cava or the inferior vena cava)
4. Common or single atrium
• failure of development of the embyologic components that contribute to the atrial septal complex

Treatment
• Closure of an ASD in individuals under age 25 has been shown to have a low risk of complications
• have a normal lifespan

Ventricular septal defect • defect in the ventricular septum• Congenital VSDs : the most common congenital
heart defect • associated with other congenital conditions, such
as Down syndrome• ventricular septum
– muscular (inferior) – membranous portion (superior) - is close to the
AV node is most commonly affected

Pathophysiology
• Large VSDs result in a significant left-to-right shunt and increase load on the right ventricle. If untreated, they result in hypertrophy of the right ventricle, which ultimately leads to right heart failure and death.


Treatment
• Treatment
– surgical
– conservative
• Smaller congenital VSDs often close on their own (as the heart grows) and are treated conservatively
Tetralogy of Fallot
• significant and complex congenital heart defect.

involves four different heart malformations:1.ventricular septal defect (VSD) 2.Pulmonic stenosis: Right ventricular
outflow tract obstruction, a narrowing at or just below the pulmonary valve.
3.Overriding aorta: The aorta is positioned over the VSD instead of in the left ventricle.
4.Right ventricular hypertrophy (RVH): The right ventricle is more muscular than normal.


• Sometimes pulmonary valve is completely obstructed (pulmonary atresia).
• Infants and young children with unrepaired TOF are often cyanotic (some oxygen-poor blood is pumped to the body)

• The development of right ventricular hypertrophy is a result of a longstanding, untreated disease.
• right-to-left shunt

• Squatting
simple procedures such as knee-chest position which reduces systemic venous return (to reduce the right-to-left shunting), increases systemic vascular resistance
Surgical TreatmentA temporary operation may be done at first if the baby is small
Complete repair later

Pulmonary valve stenosis
• reduction of flow of blood to the lungs• The most common cause is congenital• cyanosis• secondary to other conditions such as
endocarditis • valve may become narrowed (stenotic) or
leaky (insufficient). The stenosis, insufficiency or both can be mild to severe.
Surgical Treatment
If stenosis is severe, the pulmonary valve must be opened to increase blood flow to the lungs. A balloon-tipped catheter is used
• If the insufficiency is severe, an operation is required to repair or replace the pulmonary valve.

Coarctation of the aorta
การตี�บคอดของ aorta

Symptoms : decreased exercise performance, cold feet or legs, and shortness of breath.
Other symptoms include:
• dizziness or fainting
• headache
• nosebleed
• leg cramps with exercise
• hypertension with exercise
• Note: There may be no symptoms.
Signs and tests:
• examination : high BP in the arms and
low BP in the legs,
significant BP difference between the arms and legs.
The femoral pulse is weaker than the carotid pulse, or the femoral pulse may be totally absent.


Congenital heart disease
• Potential problem
1. Infective endocarditis, infective endarteritis
2. Prolonged bleeding – Thrombocytopenia– Lack of coagulation factor (thrombosis in small
vessels)– Anticoagulation medication

3. Infection : leukopenia
4. Congestive heart failure– Infection– Cardiac arrest– Cardiac dysrhythmia– Breathing difficulties (pulmonary edema)

Prevention of complications
1. Detection
2. Referral for medical Dx. and treatment
3. Consult before dental Treatment
4. Prophylactic antibiotic before dental
procedure

5. Avoidance of dehydration in oral infection
6. Bleeding time and prothrombin time before surgery, consult if prolonged
7. White blood cell count
Low : antibiotic
8. Effective local anesthetic – maximum epinephrine 0.036 mg, aspirate, injection slowly

Valvular heart disease

Mitral stenosis
• the valve does not open completely,
• so the left atrium has to have a higher pressure than normal to have the blood overcome the increased gradient caused by the mitral valve stenosis

Symptoms and signs
• Pulmonary hypertension• Exertional dyspnea• Orthopnea
• congestive heart failureTreatment requires replacement of thediseased valve with a porcine valve, or an prosthetic valve.

Aortic insufficiency
• aortic regurgitation (AR), • leaking of the aortic valve that causes blood
to flow in the reverse direction during ventricular diastole, from the aorta into the left ventricle.
• some of the blood that was already ejected from the heart is regurgitating back into the heart

Etiology
• Most cases : secondary to rheumatic fever and the consequent rheumatic heart disease
• Less common causes : calcification of the mitral valve leaflets, and as a form of congenital heart disease

Aortic valve stenosis• The more constricted the valve, the higher
the gradient between the LV and the aorta.• LV has to generate an increased pressure in
order to overcome the increased afterload caused by the stenotic aortic valve and eject blood out of the LV
• Due to the increased pressures generated by the left ventricle, the myocardium of the LV undergoes hypertrophy

• thickening of the walls of the LV. The type of hypertrophy most commonly seen in AS is concentric hypertrophy, meaning that all the walls of the LV are (approximately) equally thickened
Etiology
• include acute rheumatic fever, bicuspid aortic valve and congenital anomalies.
• As individuals age, calcification of the aortic valves may occur and result in stenosis.

Symptoms and signs of aortic stenosis
• Symptomatic
– syncope, angina and congestive heart failure
• Treatment requires replacement of the diseased valve with a porcine aortic valve or a cadaveric aortic valve, or an prosthetic aortic valve.
Aortic insufficiency
• aortic regurgitation (AR), • leaking of the aortic valve that causes blood
to flow in the reverse direction during ventricular diastole, from the aorta into the left ventricle.
• some of the blood that was already ejected from the heart is regurgitating back into the heart

Etiology• half of the cases of aortic insufficiency are
due to the aortic root dilatation : idiopathic in over 80% of cases
• aging and hypertension, Marfan syndrome, aortic dissection, and syphilis
• 15% the cause is bicuspidal aortic valve• 15% due to retraction of the cusps
(postinflammatory processes of endocarditis in rheumatic fever and collagen vascular diseases)
• regurgitant flow causes :
– decrease in the diastolic blood pressure,
– increase in the pulse pressure and hypertension
• pressure overload causes left ventricular hypertrophy (LVH).

Acute aortic insufficiency
• acute perforation of aortic valve due to endocarditis
• sudden increase in the volume of blood in the left ventricle
• pressure of the left ventricle will increase
• causes pressure in the left atrium to rise, and the individual will develop congestive heart failure

Severe acute aortic insufficiency
is considered a medical emergency
• immediate surgery for aortic valve replacement

Chronic aortic insufficiency
• left ventricle adapts by hypertrophy and dilatation of the left ventricle, and the volume overload is compensated
• Eventually the left ventricle will become decompensated, and filling pressures will increase : symptoms of congestive heart failure
Valvular heart disease
Potential problem
1. Infective endocarditis
2. Prolonged bleeding
- Anticoagulation medication
3. Congestive heart failure

Prevention of complications 1. Detection 2. Referral for medical Dx. and treatment or consult before dental Tx. 3. Prophylactic antibiotic before dental procedure 4. Bleeding time and prothrombin time before surgery, consult if prolonged 5. Effective local anesthetic – maximum epinephrine 0.036 mg, aspirate, injection slowly

Ischemic heart disease
Definition • weakened heart pumps (due to previous
heart attacks or due to current blockages of the coronary arteries)
• Cardiomyopathy - ischemic

Causes, incidence, and risk factors
• coronary arteries are blocked. • Ischemic cardiomyopathy is a
common cause of congestive heart failure.
• heart attack, angina or unstable angina.
• A few patients may not have noticed any previous symptoms.

Risks include :• personal or family history of heart
attack, angina, unstable angina, atherosclerosis,or other coronary artery diseases.
• High blood pressure, smoking, diabetes, high fat diet, high blood cholesterol, obesity
• (rarely) stress can precipitate

Symptoms • chest pain
o under the sternum may radiate to the neck, jaw, back, shoulder, arm
o may feel tight, pressure, crushing, squeezing o may or may not be relieved by rest or
nitroglycerin
• sensation of feeling the heart beat (palpitations)
• irregular or rapid pulse• shortness of breath, especially with activity
• shortness of breath that occurs after lying down
• cough• fatigue, weakness, faintness • decreased alertness or concentration • decreased urine output • excessive urination at night • overall swelling• breathing difficulty when lying down

Physical examination • may be normal• may reveal signs of fluid buildup (leg swelling, enlarged liver,
"crackles" in the lungs, extra heart sounds, or an elevated pressure in the neck vein)
• may be other signs of heart failure.
MIMI
Potential problem related to dental care1. Cardiac arrest2. MI3. Angina pectoris4. Congestive heart failure5. Bleeding tendency secondary to
anticoagulant6. Electrical interference with pacemaker

Prevention of complication
1. No routine dental care until at least 6 mo after MI
(increase risk of new infarction and arrhythmia)
2. Consultation before starting routine dental care
3. Morning appointments
4. Short appointments
5. Terminate appointment if fatigue , short of
breath, change in pulse rate or rhythm
Inform physician
Chest pain – manage as unstable angina

6. LA with max. epinephrine 0.036 mg,
aspiration, inject slowly
avoid use of vasopressor to control loss of blood, in gingival packing material
do not use epinephrine In LA in severe arrhythmia
7. Premedication with diazepam 5-10 mg before
appointment and/or the night before
8. Anticoagulant medication
surgery or scaling for patient taking coumadin:
consult physician, PT = 2 times normal or less,
INR< 3.0, ASA or other antiplatelet aggregation may have increased bleeding

9. Digitalis – prone to N/V, avoid stimulating gag reflex
10. Antisialagogues – atropine and scopolamine may cause tachycardia; check physician before use
11. Antiarrhythmic agents (quinidine, procainamide) –nausea,vomit, hypotension
oral ulceration may indicate agranulocytosis
12. Avoid use of electrocautery in patients with pacemaker

Treatment plan modifications
1. 6 mo. or more after infarction with no complications, any routine dental care can be performed
2. complications such as CHF are present, dental Tx. should be limited to immediate needs only

Emergency care
1. During first 6 mo. After infarction, emergency
dental care only after consultation
- Conservative as possible
- Drug for pain control
- Antibiotics for infection
- Pulpotomy rather than extraction
2. More than 6 mo. after infarction
a. no complications – can receive any treatment indicated
b. complications – medical consultation