
Healthy Families Annual Report 2017 - hss.gov.yk.ca · and the pathways they form make up the...
32
Healthy Families Annual Report 2017
Transcript of Healthy Families Annual Report 2017 - hss.gov.yk.ca · and the pathways they form make up the...
Healthy Families Annual Report
2017

1
Table of Contents SECTION 1: INTRODUCTION ........................................................................................................... 2
Mission Statement ............................................................................................................................. 2 Goals ....................................................................................................................................................... 2
SECTION 2: PROGRAM RATIONALE ............................................................................................ 3 Early Intervention .............................................................................................................................. 3 Brain Research .................................................................................................................................... 4 Home Visiting ..................................................................................................................................... 6
SECTION 3: THE EARLY IDENTIFICATION PROCESS ............................................................ 8 Table 1: Screening and Acceptance 2012-2017 .................................................................. 9
SECTION 4: THE GROWTH OF THE PROGRAM .................................................................... 10 Table 2: Healthy Families Yukon Program 2012 to 2017 ................................................ 10 Table 3: Ages of Children Enrolled in Healthy Families from 2012 to 2017 .............. 11 Table 4: Summary of the Program 2012-2017 ................................................................... 12
SECTION 5: PARTICIPANTS IN THE HEALTHY FAMILIES PROGRAM .......................... 13 Participant Retention Update from 2012 to 2017 .............................................................. 13
Table 5: Number of Families Enrolled In or Leaving the Program 2012-2017 .......... 13 Table 6: Reasons Families Cite for Leaving the Program 2012-2017 ......................... 14
Definition of Successful Program Completion ...................................................................... 15 SECTION 6: STAFFING ..................................................................................................................... 17
Staff Selection .................................................................................................................................. 17 Staff Training .................................................................................................................................... 18
SECTION 7: AUDITOR GENERAL OF CANADA REPORT AND RECOMMENDATIONS ....................................................................................................................... 20 SECTION 8: HEALTHY FAMILIES IN WATSON LAKE, CARMACKS, AND PELLY CROSSING ............................................................................................................................................. 25
Community of Watson Lake ........................................................................................................ 25 Communities of Carmacks and Pelly Crossing ..................................................................... 26
SECTION 9: SUMMARY AND CONCLUSIONS ......................................................................... 28 APPENDIX A: REFERENCES ........................................................................................................... 29 APPENDIX B: HEALTHY FAMILIES AMERICA STUDY CITATIONS ................................. 30

2
SECTION 1: INTRODUCTION
Healthy Families Yukon is a program designed to nurture, support and empower families within Yukon to create safe and healthy environments in which children are prepared to live healthy and responsible lives.
Prior to October 2017, Healthy Families Yukon maintained accreditation through Healthy Families America. In 2017, Healthy Families Yukon was unable to meet accreditation standards due to new Health Information and Privacy Management (HIPMA) legislation. For this and other significant reasons, the decision to no longer pursue accreditation was made in October 2017.
Mission Statement The Healthy Families Yukon program will deliver a culturally-appropriate intensive
home-based support service to children and families, prenatally and/or at birth through to school age, and in collaboration with other government and community agencies, in order to promote children’s healthy growth and development.
Goals 1. To systematically assess the strengths and needs of new parents, as well as assess
the strengths and needs of those parents who are welcoming new infants into families where older children are also present.
2. To assist parents in accessing the community services they need. 3. To enhance family functioning by building trusting nurturing relationships, teaching
problem solving, and improving family support systems. 4. To promote positive parent-child relationships. 5. To promote healthy childhood growth and development.

3
SECTION 2: PROGRAM RATIONALE
Early Intervention The priority of Healthy Families Yukon is to provide early and intensive intervention to children and families who are assessed as being overburdened. Research supports the implementation of early intervention as a means to prevent unhealthy family relationships, child abuse, developmental problems, and conversely, as a means to promote healthy parent-child interactions.
Early intervention has proven to be effective for many reasons, including that it
supports new parents in laying the foundation for a positive start with their children. The goal of early intervention is to establish positive parenting patterns from the onset. Early intervention shortly after childbirth can be a critical time, as many parents are
often eager to learn about how to be the best possible parent for their newborn. Research also supports the use of early intervention in addressing the high rate of physical abuse and neglect that occurs in overburdened families with children under
the age of two (Healthy Families America, 2015). Early intervention can provide information about abuse and can enhance the coping skills of new parents. Home visits allow Healthy Families Workers (HFW) to support parents in developing positive,
strength-based behaviours in the caring of their children as a means to decrease the potential risk of child abuse or neglect. Early intervention teaches new parents how to support their baby’s brain development, which is paramount for overall and ongoing
healthy development.
The choice to offer home visitation as the primary method of early intervention through Healthy Families Yukon stems from over twenty years of foundational research. Studies have shown that families who received early intervention services by way of home visitation showed lower levels of abuse and neglect and higher rates of education (Healthy Families America, 2015). Studies have further indicated that families who received home visitation demonstrated greater financial independence and better school performance than families who did not (Healthy Families America, 2015).

4
Families who have received home visitation have also proven to use less expensive government resources and services. It could be argued, however, that one of the greatest advantages to home visitation is the benefit of parents developing positive attitudes towards parenting, resulting in improved parent-child interactions.
Brain Research Recent advances in brain research have afforded great insight into how the infant brain develops post-birth. The infant brain continues to grow and develop well beyond infancy into adolescence and early adulthood (Board on Children, Youth, and Families, National Research Council & Institute of Medicine, 2000). This growth was once thought to be determined primarily by genetics; however, research now shows that brain growth and development is highly dependent upon a child’s environment and
experiences. (Healthy Families America, 2015). Research shows that children’s interactions with people and the environment around them are just as vital as having sufficient nutrients for the growing body. Brain ‘plasticity’ allows for the young brain to
develop and change in response to the demands of the environment that surrounds them (Board on Children, Youth, and Families, National Research Council & Institute of Medicine, 2000). The young brain learns to adapt and develop the skills required to
function throughout the lifespan. It has been further noted that, while individual genetic influences do play a role in brain development, a child’s experiences have significant influence on the manner in which genes are expressed in the developing brain (Healthy Families America, 2015). While positive early experiences help the young brain to develop well, negative experiences (e.g. neglect, abuse, etc.) can cause children with no initial demonstration of genetic abnormality to become cognitively delayed or to develop serious emotional difficulties (Healthy Families America, 2015).
The brain is comprised of many regions that perform specific functions, such as identifying what we see, processing spoken language, or assessing whether we are in danger (Board on Children, Youth, and Families, National Research Council & Institute of Medicine, 2000). The brain contains billions of neurons that send electrical or chemical messages to each other through synapses. The trillions of nerves, synapses

5
and the pathways they form make up the ‘wiring’ of the brain, allowing for the various regions to communicate and function together in a coordinated way. The number and organization of synaptic connections in the brain influence everything from the ability to recognize letters of the alphabet to capacity for managing complex social relationships.
In most regions of the brain, no new neurons are formed after birth. Instead, brain development consists of an ongoing process of wiring and re-wiring the connections among neurons. New synapses between cells are constantly being formed, while others are broken or pruned away (Board on Children, Youth, and Families, National Research Council & Institute of Medicine, 2000). This occurs throughout the lifespan. In early childhood, however, the brain is genetically programmed to produce more synapses than it will ultimately ever be capable of using. By 8 months of age, a baby may have an astounding 1,000 trillion synaptic connections. This blooming of synapses
happens at different times in different areas of the brain. Synaptic connections are maintained when they are used (e.g., a baby learning to cry to communicate a need); conversely, synaptic connections are pruned away when they are not used (e.g., a baby
no longer cries to communicate a need because of neglect over time). The pruning of synapses occurs throughout childhood as different areas of the brain develop. Pruning allows the brain to keep the connections that, through experiences, are determined to
have a purpose. Pruning increases the efficiency of the brain, informing what it can do and what it needs to do. Pruning occurs when neuronal connections are not developed or reinforced. Because the brain operates on the "use it or lose it" rule, an "over-
pruning" of these connections can occur when a child is deprived of reassuring and meaningful experiences in the early years.
Some areas of the brain can become less "plastic" or changeable once pruning has occurred. This has led to significant concern about providing what the brain needs to prune and organize itself correctly before the "windows of opportunity" close. For example, surgeons now remove congenital cataracts as early in infancy as possible, because they know that if they wait until the child is older, the neural connections
between the eyes and the brain will fail to develop properly, resulting in the inability to

6
see. Research has also reported on the critical ‘window’ for language development within the first seven months of life, increasing the importance of language-based parent interactions with infants.
Negative early experiences can also profoundly affect the development of the brain. Maltreatment increases a child’s risk of developing depression, self-destructive behaviour, eating disorders, attention deficit disorders, drug and alcohol problems, sexual promiscuity, and delinquency. Many researchers believe that these effects can be partly explained by understanding how chaotic, stressful, and traumatic experiences affect brain development (Healthy Families America, 2015).
Home Visiting Children who are abused or severely neglected are at extremely high risk of developing emotional, behavioural, social, and intellectual disabilities. By the time a child is
identified as having been neglected or abused, their circumstances have already begun to impact their developing brains. High-quality home visiting programs that start working with families as soon as the child is born have proven to be effective in
preventing abuse and neglect. The key to success with these programs is that they help parents to manage the stresses of raising children before unhealthy patterns develop. Healthy Families Yukon provides a family-centered, intensive, early intervention home
visiting program with a focus on parent-child relationships, child development, and overall family functioning.
The Healthy Families Yukon home visitation program is grounded in the evidence-based Growing Great Kids (GGK) and Growing Great Families (GGF) curriculums. This
comprehensive and culturally responsive set of curriculums begin prenatally and support the development of nurturing and empathetic parent-child relationships. The curriculums provide the structure of home visits with a focus on child development, health, provision of care, parenting concerns, positive parent-child relationships, and overall family functioning. Each age group of the GGK includes five modules: Basic Care, Play and Stimulation, Social and Emotional Development, Physical and Brain

7
Development, and Cues and Communication. The focus is on fun and interaction. The modules incorporate games and activities to encourage family participation. The GGF provides the structure for the promotion of healthy family functioning and strengthening family relationships and family values through discussions around culture, discipline, and development of positive communication skills.

8
SECTION 3: THE EARLY IDENTIFICATION PROCESS The early identification process for Healthy Families Yukon begins prenatally, or following the birth of a baby. Families are screened into this program based on identified need and willingness to participate. The program supports families in the Whitehorse area, Watson Lake, Pelly Crossing, and Carmacks.
Historically, families were screened into this program through a process that involved both Public Health Nurses (PHN) and Healthy Families Supervisors. The first step in the screening process involved the administering of a standardized screening tool – the
Healthy Families Screen, completed with parents by the PHN. This part of the process allowed the PHN to quickly reach those families who were most likely to benefit from the program. The PHN identified families that fell into any one or more of the following
demographics: single parent, common-law relationship, late or no prenatal care, or other stressors that may impact the quality of parenting (e.g., isolation or mental health concerns). The PHN also looked for two or more indicators of potential need for support
which may include: having an unstable home address, history of psychiatric care, young/teenaged parents, or a screen that contains multiple “unknown” answers for either parent. The second part of the screening process, the Parent Survey, was done
by a Healthy Families Supervisor or trained Healthy Families Worker. Families who had a “positive screen” as identified by the PHN and scored 25 or higher on the Parent Survey were offered acceptance into the Healthy Families Yukon program.
The aforementioned screening process was modified in the fall of 2017 to make the
program more responsive and accessible. Feedback from community collaterals, clients, and members of the rural communities reported that the Parent Survey served as a barrier to accessing the program. Feedback indicated that the Parent Survey was
perceived as too intrusive, and in some instances re-traumatizing for some clients. In October 2017, when Healthy Families Yukon opted to no longer pursue accreditation, the administering of the Parent Survey as a standardized practice for acceptance to the

9
program was discontinued. Further modifications to the screening process are also under revision for 2018.
Table 1: Screening and Acceptance 2012-2017
In 2017, the total number of families in Whitehorse, Watson Lake, Carmacks, and Pelly Crossing that received a positive screen was 98. Of those 98 families, 67 accepted the program. The acceptance rate is based on the number of families who received a positive screen and accepted the program when it was offered. In 2017, the acceptance rate into the program was 68%.
0
100
200
300
400
500
2017 2015 2013
total births
positive screens
declined after screen

10
SECTION 4: THE GROWTH OF THE PROGRAM
Since 2012, there has been a steady increase in the number of families enrolled overall. In 2017, 135 families were enrolled in the Healthy Families Yukon program. Table 2 shows the growth of the Healthy Families program over the past six years.
Table 2: Healthy Families Yukon Program 2012 to 2017
105
110
115
120
125
130
135
140
2012
2013
2014
2015
2016
2017
11
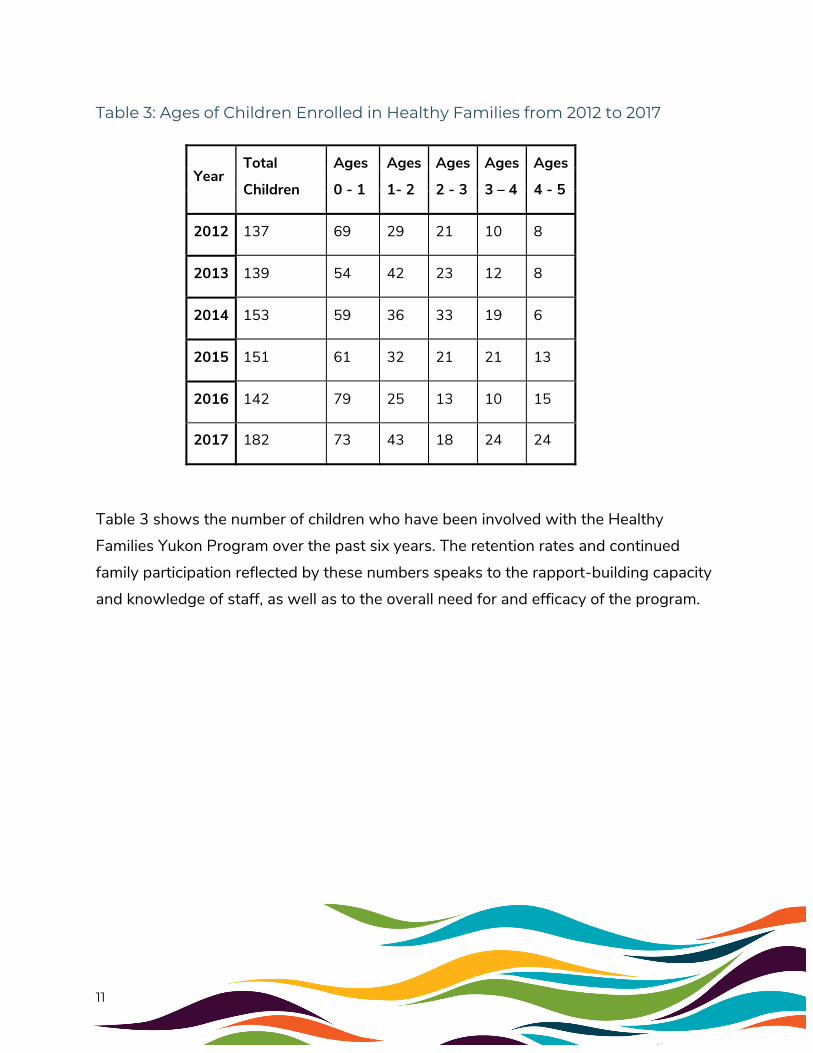
Table 3: Ages of Children Enrolled in Healthy Families from 2012 to 2017
Year Total
Children
Ages
0 - 1
Ages
1- 2
Ages
2 - 3
Ages
3 – 4
Ages
4 - 5
2012 137 69 29 21 10 8
2013 139 54 42 23 12 8
2014 153 59 36 33 19 6
2015 151 61 32 21 21 13
2016 142 79 25 13 10 15
2017 182 73 43 18 24 24
Table 3 shows the number of children who have been involved with the Healthy Families Yukon Program over the past six years. The retention rates and continued
family participation reflected by these numbers speaks to the rapport-building capacity and knowledge of staff, as well as to the overall need for and efficacy of the program.

12
Table 4: Summary of the Program 2012-2017
Year Referrals
# of Families Accepting to Participate in
Program
% Rate of Acceptance
Total # of Families Enrolled for the Year
# of Families Leaving Program for the Year
% of Families Leaving
2012 51 31 61% 118 35 30%
2013 50 40 80% 123 29 24%
2014 52 39 75% 134 49 37%
2015 61 43 70% 131 44 34%
2016 76 50 65% 127 28 22%
2017 98 67 68% 135 52 39%
Table 4 provides further detail on the Healthy Families Yukon program over the past
five years. The number of referrals has nearly doubled since 2012. Over the past six years, the number of parents enrolled in the program has increased steadily while the percentage of families leaving the program has remained relatively consistent. The
reasons that families give for leaving the program are varied, and participant retention is discussed in detail in Section 5: Participant Retention.
13
SECTION 5: PARTICIPANTS IN THE HEALTHY FAMILIES PROGRAM
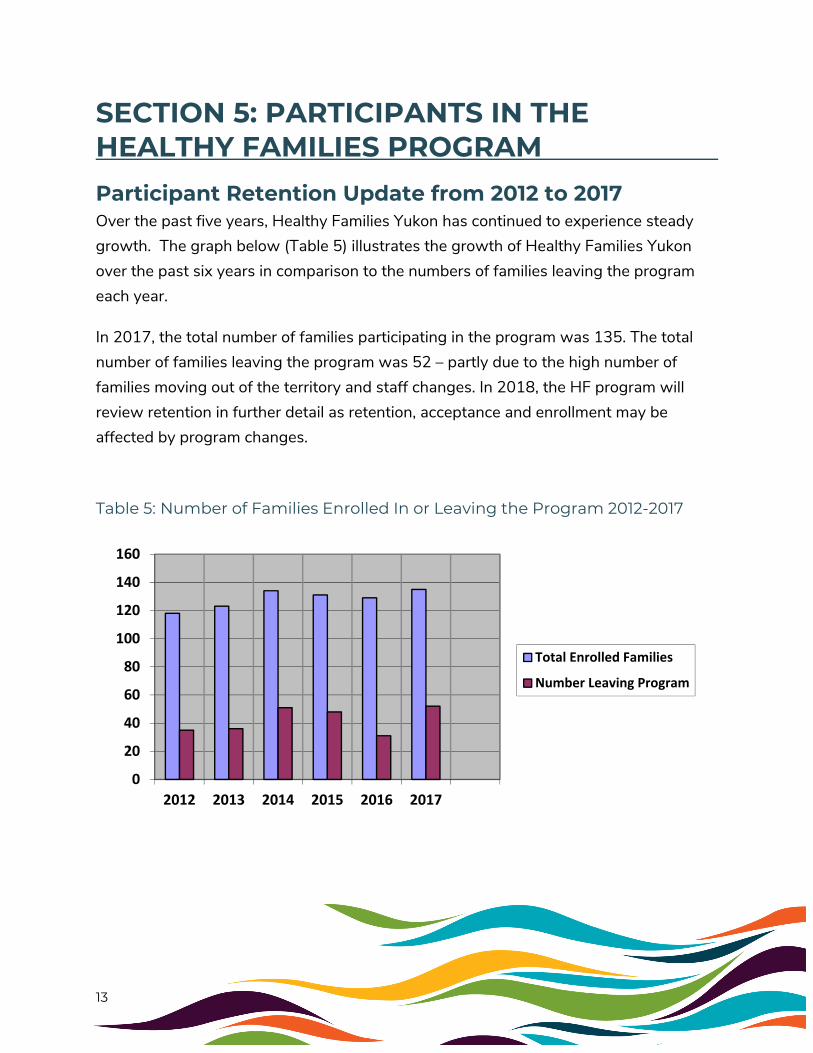
Participant Retention Update from 2012 to 2017 Over the past five years, Healthy Families Yukon has continued to experience steady growth. The graph below (Table 5) illustrates the growth of Healthy Families Yukon over the past six years in comparison to the numbers of families leaving the program each year.
In 2017, the total number of families participating in the program was 135. The total number of families leaving the program was 52 – partly due to the high number of families moving out of the territory and staff changes. In 2018, the HF program will review retention in further detail as retention, acceptance and enrollment may be affected by program changes.
Table 5: Number of Families Enrolled In or Leaving the Program 2012-2017
0
20
40
60
80
100
120
140
160
2012 2013 2014 2015 2016 2017
Total Enrolled Families
Number Leaving Program

14
Table 6: Reasons Families Cite for Leaving the Program 2012-2017
YEAR
Total
Enrolled
Families
Number
Leaving
Program
% of
Families
Leaving
Moved
Unable
to
Engage
Unable
to
Locate
Met
Program
Goals
Refused
Change
in FSW
Client
Withdrawal
Child
no
longer
in home
Death
of
Target
Child
Transfer
to other
H.F.
Program
Refused
Service
2012 118 35 30% 6 0 8 4 0 4 4 0 0 8
2013 123 36 29% 6 0 6 7 1 11 1 0 0 4
2014 134 51 38% 8 0 6 6 3 18 1 0 0 9
2015 131 48 37% 12 1 12 5 0 10 1 0 1 6
2016 129 31 24% 4 0 1 5 1 14 4 0 0 2
2017 135 52 39% 11 1 9 4 0 15 2 1 0 9
Tables 5 and 6 indicate that the retention rates in the Healthy Families Yukon Program ranged between 61 and 76 percent over the past six years. The client retention rate for 2017 was 61% and was affected by the rate of families (11) who moved to a location
where the Healthy Families Yukon program is not offered. It was further impacted by a significant staff turnover that began in 2016 and carried over into 2017. When a staff member leaves the position, the families on their caseload are transferred to another Healthy Families Worker, and given the value placed on relationship in home visiting, it is not uncommon for the family to withdraw during the time of transition. The new “buddy system” for providing coverage and promoting relationships with other staff has been developed to address client retention during staff turnover. This will be further explained in Section 6: Staffing.
15
Definition of Successful Program Completion Families enrolled in the Healthy Families Yukon program participate based on a system of levels that determines the frequency of visits. The definition for successful completion of the program to be implemented in 2018 is as follows: Level 1P (Prenatal): 2-4 visits per month
Level 1: 4 visits per month
Level 2: 2 visits per month
Level 3: 1 visit per month
Level 4: 1 visit per quarter
Level SS (Special Services): 4-6 visits per month
A family on any of the previously mentioned assigned levels can successfully complete
the program by meeting two or more of the following criteria:
1. The family determines that they are able to manage their stressors without the support of the Healthy Families program.
2. The family is able to demonstrate skill in the following areas: a. Supportive network: Maintaining a supportive network that they are able to
access when needed. b. Problem solving skills: The family uses effective problem solving skills in most
situations. c. Parent-child interactions: The family has developed positive parenting skills
that promote healthy child development. d. Health: The family is connected to and uses the appropriate primary and
mental health care resources (to include up-to-date immunizations).
A new definition of successful program completion will be implemented in 2018. Prior to the approval of this new definition, the only families that were considered as having successfully completed the program (graduating) were families remaining in the program until their child was five years old or entering kindergarten. The limitation of

16
using this criterion for successful program completion is that it omitted the acknowledgment and celebration of a family’s growth during their involvement in the program. Furthermore, it left no room to report on whether or not parents felt that their needs were met through their involvement, regardless of the age of their child when they left the program.
Prior to the revision of the criteria for successful completion, when a family left the program earlier than their child’s fifth birthday or when their child entered kindergarten, the reason recorded was that the family had withdrawn from the program, declined service, or was unavailable. There have been no closures based on graduation from the program since the implementation of the new definition of successful program completion.
2018 will mark the first year of reporting on the successful completion of the program based on the new definition.

17
SECTION 6: STAFFING
Staff Selection The services offered through the Healthy Families Yukon program require a unique type of staff member. Healthy Families Yukon Workers (HFW) and Supervisors are carefully screened, selected, and trained to ensure the best possible service provision to clients. HFWs are selected in part because of their personal characteristics, including being non-judgemental, compassionate, and having the ability to establish trusting and appropriate therapeutic relationships with clients. HFWs also have a willingness to work or have experience working in culturally diverse communities. They further demonstrate the capacity to be culturally respectful and appropriate, as well as have a capacity to engage in reflective practice. HFWs hold a firm belief that all children need
and have a right to be nurtured in a responsive and meaningful manner. HFWs further display a willingness to advocate for positive, nurturing, and non-violent methods of disciplining children.
In 2017, the Healthy Families Yukon program welcomed three new HFWs and two
new Supervisors to the team. These new hires replaced staff that had either resigned or took leave from their positions in 2016. In 2017, the Healthy Families Yukon team weathered the challenges of being under-staffed as well as navigating the transitions
of new hires into the program as they occurred. Once the team was again fully-staffed, the transition process further required the appropriate training and program acclimatization for new HFWs before being able to service clients directly. As a result,
this impacted the rate of client retention for the program. It is anticipated that the retention rates for 2018 will rise with the newly stabilized Healthy Families Yukon team.

18
Staff Training HFWs selected for the position undergo extensive training to enable them to recognize and address necessary interventions with families. Their training also supports the awareness of resources available in the community for families. HFWs participate in a detailed orientation upon starting in their position, and within the first six months of their date of hire they receive training in the following areas:
o Infant Care; o Child Development and Well Being; o Parental Health and Well Being; o Language Development (Birth to 2 years); o Role of Culture in Parenting; o Family Violence; o Substance Use; o Parental Issues; o HIV and AIDS; o Staff-related Issues.
Staff members also receive continuing intensive training specific to their role to better understand the essential components of family needs assessments and home visitation.
Included in the training is the assessing of overburdened families, completing a standardized risk assessment, the child development screening tool (Ages & Stages Questionnaire), how to engage in creative outreach, building upon family strengths,
promoting parent-child interactions, and managing crisis situations.
In 2017, staff members at Healthy Families Yukon participated in a variety of courses to help them to interact more effectively with the families on their caseload. The courses taken by HFW include:
o Healthy Families Core Training; o Car Seat Installation Training; o Blanket Exercise; o Risking Connection – Trauma Informed Care; o Compassion Fatigue;

19
o Mental Health First Aid; o ASIST – Applied Suicide Intervention Skills Training; o First Aid; o Restorative Approach; o Non-Violent Crisis Intervention.
In addition to their training, staff members receive ongoing support through individual weekly supervision. Individual supervision provides a time for workers to debrief and develop realistic and effective plans to assist families in meeting their goals. It further supports them in engaging in reflective practice, and facilitates their own personal development as caregiving professionals. Weekly supervision further serves as a time
of exploration, evaluation of client issues and gives HFWs the opportunity to discuss their concerns, frustrations and successes. It is an opportunity for staff to further develop their skills and demonstrate their areas of competency, which encourages
personal and professional growth.
The Healthy Families Yukon program has developed guidelines on conducting effective supervision. The guidelines for supervision outline that the focus should be placed on the HFW’s observations, interventions, the family dynamics, the worker’s commitment
to the family, challenges, and other home visiting issues. Supervisors are given training specific to the use of GGK and GGF curriculums to enhance the skill development of HFWs in the effective and emergent use of the curriculums. Supervision also allows for
the identification of where HFWs may need further training.
The Healthy Families Yukon Program understands that HFWs’ performance and level of competence is key to providing quality service to families. This is reflected in the selection process, and is why training and supervision are vital to effective
programming.
In 2018, another session of intensive GGK and GGF training has been planned for all new staff.

20
SECTION 7: AUDITOR GENERAL OF CANADA REPORT AND RECOMMENDATIONS
The Auditor General of Canada’s 2014 report to the Department of Health and Social Services’ (the Department) Family and Children’s Services made a number of recommendations pertaining to the Healthy Families Yukon Program.
The Auditor General of Canada recommended that Family and Children’s Services review retention in the Healthy Families Yukon Program, including defining what successful completion of the program is and linking it to the program’s objectives.
Based on these recommendations, the Department developed a definition of successful program completion. It is a departure from the previous definition that considered ageing-out of the Healthy Families program as being successful completion.
The report recommended that the Department review existing evaluation outcomes for
the Healthy Families Yukon Program. In response, the Department developed performance indicators and outcomes to ensure that Healthy Family Yukon's work is having the desired impact, and that program goals are being met.
Three performance measures were selected to reflect outcomes that underline the
overall goals of the Healthy Families Yukon Program. Results of these performance measures can be found below. The program began monitoring these outcomes in 2013, and will continue to monitor these outcomes going forward.
Outcome: Children’s health is optimized, and preventable illness is reduced.
Indicator: Increase in percentage of children (of client families) whose immunizations are up to date.

21
Numerator: Number of children of Healthy Families client families (with open files in selected calendar year) whose immunizations are up to date based on the immunization schedule in use at the Whitehorse Health Center.
Denominator: Number of children in Healthy Families client families (with open files in the selected calendar year)
Source: Administrative Data (Community Health and Healthy Families).
Rationale: Routine immunization has been shown to significantly reduce child mortality associated with infectious diseases. Young children are particularly vulnerable to a number of communicable diseases, and recent outbreaks of measles and pertussis in Canada have demonstrated the potential issues for unvaccinated populations.
Results: There was a 5% increase in children of clients whose immunizations were up to date from 2013 to 2014, an 11% decrease in 2015, and a 7% increase from 2015 to 2016. In 2017 there was a 4% increase in children whose immunizations were up to date.
65%
80%
69%
76%80%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Immunizations Up to Date
2013 2014 2015 2016 2017

22
Outcome: Children’s intellectual and social development is optimized.
Indicator: Increase in percentage of children with identified developmental concerns following through with initial appointment to referred service.
Numerator: Number of Healthy Families client children (with open files in selected calendar year) with identified developmental concerns who follow through with initial appointment to referred service.
Denominator: Number of Healthy Families client children (with open files in selected calendar year) with identified developmental concerns that are referred to a service.
Source: Administrative records at Healthy families with confirmation of attending referred service.
Rationale: While a number of services are provided directly by Healthy Families staff, additional community resources are also enlisted in ensuring optimal child development. The Child Development Center (CDC) is a primary example of a service clients are referred to when a child would benefit from additional support in achieving school readiness, appropriate social development, language skills, and other areas of development. This wrap-around model of connecting families and children to community supports provides direct benefits to the families and children. Follow-up with referral services and families helps to ensure support for client families and potentially increases feelings of community connectedness.
Results: There was an initial decrease of 13% in the number of children (clients) with identified developmental concerns who followed through with initial appointment from 2013 to 2014, with an increase of 23% from 2014 to 2015. From 2015 to 2016 there was an additional increase of 28%, and a slight decrease of 4.5% in 2017. This decrease is due in part to families declining service from the CDC upon referral by the Healthy Families Yukon program. Waitlists for service at the CDC can range between 4 to 6 months (or more) depending on the specific service requested. Longer wait times for services can be a barrier to parents’ willingness or to the possibility of receiving service prior to their child entering school.

23
Outcome: Families demonstrate parent-child interaction that permits healthy child development.
Indicator: Increase in percentage of families with child-centered goals.
Numerator: Number of client families (with open files in selected calendar year) who have identified child- centered goals.
Denominator: Number of client families (with open files in selected calendar year).
Source: Client files, individual family support plans.
Rationale: Healthy Families Workers work with families to increase or enhance understanding of social, intellectual, and physical developmental needs and milestones in early childhood. Families are encouraged to regularly set and reflect on child- centered goals appropriate to their child’s needs. Examples include “teaching a child their colours and shapes”, “establishing a bedtime routine”, “ensuring dental care is being provided”, and “taking the child to their 12-month check-up”. Parents setting appropriate child-centered goals demonstrate an understanding of and commitment to
61%
48%
72%
100%96%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Child Development Delay Tracking
2013 2014 2015 2016 2017

24
healthy childhood development and effective parenting. Client-directed goal setting may also enhance parental feelings of ownership and empowerment in their parenting.
Results: There was a 6% increase in the number of families with child-centered goals from 2013 to 2014, an increase of 28% from 2014 to 2015, and an increase of 21% from 2015 to 2016. There was a decrease of 14% in 2017 of families with child-centered goals. This decrease is due in part to the rate of staff turnover throughout the year. This impacted the consistency and frequency of visits made with families, thus affecting how long it took to introduce and complete Family Goal Plans with clients. In addition, new staff may not be as familiar with the goal planning process. In 2018, emphasis will be placed on the appropriate staff training needed to address the issue of how to engage families in creating meaningful Family Goal Plans.
27%33%
61%
82%
67%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Families with Child-Centered Goals
2013 2014 2015 2016 2017

25
SECTION 8: HEALTHY FAMILIES IN WATSON LAKE, CARMACKS, AND PELLY CROSSING
A unique component of Healthy Families in the rural communities is Universal Programming. Universal programming consists of either home visiting to assist families in times of crisis, or the offering of monthly support groups that focus on various parent and family challenges. The groups also provide an opportunity for parents to expand their social network. The children involved have the opportunity to socialize with other children and learn skills to support the development of self-regulation. One key concept of Universal Programming is partnership with other community service providers to offer parents information sessions to expand awareness and knowledge of various
topics.
Community of Watson Lake The Watson Lake Healthy Families program began in November of 2014 and began
offering Universal Programming in 2017. The new Watson Lake HFW took over from the previous worker in May 2017. The previous Watson Lake HFW relocated to Carmacks, and currently offers programming in Carmacks and Pelly Crossing. The new
Watson Lake HFW held a caseload of seven families in 2017. The following groups/community events were facilitated in Watson Lake by the current and previous HFWs:
1. January: Handle with Care group: Six mothers and five children attended. 2. January: “I Am Me” program: In partnership with Public Health, the “I Am Me”
program, the Watson Lake Public Library, the CDC, the Learning Together Program, and Emergency Medical Services organize and deliver a Teddy Bear Picnic for children ages 0-5. Approximately 50 children and families attended.
3. January: Parent-Child Mother Goose: Six mothers and eight children participated consistently in this group. Approximately 4-6 additional participants attended, with varying frequency.

26
4. February: Parent-Child Mother Goose: Six mothers and eight children participated consistently in this group. Approximately 4-6 additional participants attended, with varying frequency.
5. March: Parent-Child Mother Goose: Six mothers and eight children participated consistently in this group. Approximately 4-6 additional participants attended, with varying frequency.
6. May: Handle with Care Facilitator Training: Offered in partnership with the CDC. Four participants attended.
7. June: Handle with Care: This session was held in partnership with the Watson Lake Family Centre and Child and Adolescent Therapeutic Services (now the Child Youth and Family Treatment Team, or CYFTT). Four participants attended.
8. September: Healthy Families Open House: 30 people in attendance (9 parents, 12 children, and 9 community workers).
9. December: Healthy Families groups and drop-ins: There were six events in total, serving approximately 110 participants. The participants included parents, grandparents, and other relatives; 18 children under age five; and 18 community agency representatives.
10. In addition to these events, the Watson Lake HFW partnered with a counsellor from Mental Wellness and Substance Use as well as the Help and Hope Society for Families to deliver “Courageous Women” – an addictions program based on the principles of Seeking Safety. The group ran for eight weeks from October to November, with eight participants.
Communities of Carmacks and Pelly Crossing The Carmacks/Pelly Crossing Healthy Families program began offering Universal
Programming in July 2017. The Carmacks/Pelly Crossing HFW held a caseload of nine clients in 2017, and facilitated the following groups and community events:
1. July (Carmacks): Shaping Your Child’s Future: This group was facilitated in partnership with the Little Salmon Carmacks First Nation. Three participants were in attendance.
2. July (Pelly Crossing): Shaping Your Child’s Future: This group was facilitated in partnership with Selkirk First Nation. Three participants were in attendance.

27
3. August (Carmacks): Positive Self-Talk: The Brain Science. This group was facilitated in partnership with the Little Salmon Carmacks First Nation. Six participants were in attendance.
4. October (Carmacks): Healthy Families Yukon Open House: 28 people were in attendance (six parents, three children, and 19 community members and service providers).
5. October (Pelly Crossing): Healthy Families Yukon Open House: 43 people were in attendance (eight parents, 11 children, and 24 community members and service providers).

28
SECTION 9: SUMMARY AND CONCLUSIONS
The year 2017 was productive for the Healthy Families Yukon Program. The program implemented changes to make its delivery more accessible and responsive to its clients. Barriers to the enrollment process were removed in response to feedback from clients and community partners. The pursuit of accreditation was also discontinued in 2017, as the standards were no longer in compliance with the new HIPMA legislation. This allowed for increased flexibility in how the program is delivered. In addition, the hiring of new staff impacted the program in a positive way. New staff brought new perspectives, and returned the team to a full complement both in Whitehorse and the rural communities.
The Healthy Families Yukon Program continues in its commitment to achieving the
performance measures implemented in response to the Auditor General of Canada 2014 Report, including immunization rates, tracking of developmental delays, and child-centered goals. As well, a staff training plan for 2018 has been created to further
enhance home visitation practices for HFWs. These trainings will, in part, address identified training needs outlined in this report: client retention, supporting families to follow through on referrals to address developmental delays, and engaging families in
developing meaningful Family Goal Plans. Further review is also being planned in 2018 to address the criteria underlined in the initial screening to the program.
The team at Healthy Families Yukon is committed to ensuring quality services, and their dedication in providing a high level of service rooted in best practice for children and families is commendable. The program looks forward to serving families with the same level of commitment, enthusiasm, and quality of service in 2018 and beyond.

29
APPENDIX A: REFERENCES
Shonkoff, J. & Phillips D. (2000). From Neurons to Neighborhoods, The Science of Early Childhood Development-Board on Children, Youth, and Families-National Research Council and Institute of Medicine. Washington, D.C.: National Academy Press.

30
APPENDIX B: HEALTHY FAMILIES AMERICA STUDY CITATIONS Anisfeld, E., Sandy, J., & Guterman, N. B. (2004). Best Beginnings: A randomized
controlled trial of a paraprofessional home visiting program: Technical report. Report to the Smith Richardson Foundation and New York State Office of Children and Family Services. New York: Columbia University School of Social Work. Additional Sources: Executive summary, Narrative summary.
LeCroy & Krysik (2011). Randomized trial of the Healthy Families Arizona home
visiting program. Children and Youth Services Review, 33, 1761-1766. Mitchell-Herzfeld et al (2005). Evaluation of Healthy Families New York: First year
program impacts. Office of Children and Family Services. Available at: ocfs.state.ny.us/main/prevention/assets/HFNY_FirstYearProgramImpacts.pdf
Caldera, et al. (2007). Impact of a statewide home visiting program on parenting and on
child health and development. Child Abuse & Neglect, 31(8), 829-852. Landsverk, et al. (2002). Healthy Families San Diego Clinical Trial: Technical Report.
Child and Adolescent Services Research Center, San Diego Children’s Hospital and Health Center.
Lee, E., Mitchell-Herzfeld, S., Lowenfels, A. A., Greene, R., Dorabawila, V., &
DuMont, K. A. (2009). Reducing low birth weight through home visitation: A randomized controlled trial. American Journal of Preventive Medicine, 36(2), 154–160. doi:10.1016/j.amepre.2008.09.029
DuMont, K., Mitchell-Herzfeld, S., Greene, R., Lee, E., Lowenfels, A., Rodriguez, M.,
et al. (2008). Healthy Families New York (HFNY) randomized trial: Effects on early child abuse and neglect. Child Abuse & Neglect, 32(3), 295–315.
Duggan, Caldera, et al. (2007). Impact of a statewide home visiting program to prevent
child abuse. Child Abuse & Neglect, 31(8), 801-828.

31
Duggan, A., McFarlane, E., Fuddy, L., Burrell, L., Higman, S. M., Windham, A., et al.
(2004). Randomized trial of a statewide home visiting program: Impact in preventing child abuse and neglect. Child Abuse & Neglect, 28(6), 597-622.
DuMont, K., Kirkland, K., Mitchell-Herzfeld, S., Ehrhard-Dietzel, S., Rodriguez, M.
L., Lee, E., Layne, C., & Greene, R. (2010). A randomized trial of Healthy Families New York (HFNY): Does home visiting prevent child maltreatment? Washington, DC: National Institute of Justice.
Kirkland, K., & Mitchell-Herzfeld, S. (2012). Evaluating the effectiveness of home
visiting services in promoting children’s adjustment in school: Final report to the Pew Center on the States. Rensselaer, NY: New York State Office of Children and Family Services, Bureau of Evaluation and Research.
Bair-Merritt, M. H., Jennings, J. M., Chen, R., Burrell, L., McFarlane, E., Fuddy, L.,
et al. (2010). Reducing maternal intimate partner violence after the birth of a child: A randomized controlled trial of the Hawaii Healthy Start home visitation program. Archives of Pediatrics and Adolescent Medicine, 164(1), 16-23.
















![SYMPLECTIC ORIGAMI arXiv:0909.4065v2 [math.SG] 21 … · plex structures, one can give in the spirit of [GGK] a proof that the equivariant spin-Cquantization of Mis, ... An origami](https://static.fdocuments.us/doc/165x107/5af8bf7d7f8b9a2d5d8c05b8/symplectic-origami-arxiv09094065v2-mathsg-21-structures-one-can-give-in.jpg)
