Healthy & Fit
20
Healthy & Fit: A Community Action Plan for Franklin County Children & Families E X E C U T I V E S U M M A R Y
Transcript of Healthy & Fit
Healthy & Fit:A Community Action Plan forFranklin County Children & Families
E X E C U T I V E S U M M A R Y

Commissioned by:
Osteopathic Heritage FoundationRichard Vincent, President & CEOTerri Donlin, Director of Programs1500 Lake Shore Drive, Suite 230Columbus, OH 43204www.osteopathicheritage.org
Community Planning Conducted by:
Children’s Hunger AllianceWilliam J. Dolan, Chief Executive OfficerDianne Radigan, Chief Operating OfficerJ.D. Beiting, Special Projects Manager370 South Fifth StreetColumbus, OH 43215www.childrenshungeralliance.org
The Ohio State UniversityCollege of Human EcologyDr. Gail Kaye, PhD, RD1787 Neil AvenueColumbus OH 43210
Vision Franklin County children, especially those most at risk, will be fit and have healthy weights as a result of long term, dynamic communitywide efforts to create effective, child focused and family centered programming and environments.
Mission To create an environment that supports life-long,healthy food and fitness behaviors in Franklin Countychildren through the efficient and effective coordination of community resources.
Healthy & Fit:A Community Action Plan forFranklin County Children & Families
Acknowledgements i
Guiding Concepts 1
Prevalence Data 2
The Process 4
The Findings 5
Strategies for Providing 7
a Healthy Food and Fitness
Environment for Children
Continuing the Effort 9
Conclusion 10
Logic Model 11
T A B L E O F C O N T E N T S

Leadership Council
• Lisa Courtice PhD, The Columbus Foundation• William J. Dolan, Children’s Hunger Alliance• Terri Donlin, Osteopathic Heritage Foundation• Jewell K. Garrison, Columbus Medical
Association Foundation• Janet Jackson, United Way of Central Ohio• John Jackson, Cardinal Health• Gail Kaye PhD, The Ohio State University• Teresa Long MD, Columbus Health Department• Robert Murray MD, Children’s Hospital
and Abbott Laboratories• Dianne Radigan, Children’s Hunger Alliance• Arlene Shoemaker, Franklin County Commissioner• Charleta Tavares, Columbus City Council• Susan Tilgner, Franklin County Health Department• Richard Vincent, Osteopathic Heritage Foundation
Key Stakeholder Survey Design and Adult Focus Groups
• Gail Kaye PhD, The Ohio State University• Ana Claudia Zubieta PhD,
Consultant to The Ohio State University• Claudia Byrne, The Ohio State University
Extension Office
Child Focus Groups
• Leesa Martin, Abbott Laboratories• Nancy Fritz, The Fritz Group
Survey Design Expert Committee
• Michelle Vander Stouw, United Way of Central Ohio• Lynnette Cook PhD, United Way of Central Ohio• Roberta Garber, Community Research Partners• Kathy Cowen, Columbus Health Department
Nutrition Expert CommitteeFacilitated by: Gail Kaye PhD, The Ohio State University
• Robert Murray MD, Children’s Hospital and Abbot Laboratories
• Angie Norton, Ohio Department of Health• Gina French MD, Children’s Hospital• Shelly Roth, Children’s Hunger Alliance• Misty Davis, Columbus Public Schools
Physical Activity Expert Committee Facilitated by: Diane Barnes, Columbus Public Schools
• Jackie Goodway PhD, The Ohio State University• Michelle Park, Ohio Parks and Recreation• Dannell Haines, The Ohio State University• Monica Turner, YMCA of Central Ohio
Cultural Diversity Expert CommitteeFacilitated by: Manisha Maskay PhD, Columbus Health Department
• Olivia Thomas MD, Children’s Hospital• Eric Troy, Eternal Sports• Sylvia Wooden, New Fellowship of
Christians Church• Hannah Dillard, The Mayor’s Office –
City of Columbus• Hugo Melgar Quinonez, The Ohio State University
Marketing and Media Expert CommitteeFacilitated by: Ray Caruso, The Center for Participative Leadership
• Pete McGinty, Experience Columbus• Kim Kelly-Bartley, White Castle System, Inc.• Julie Carrier, Ohio Food Industry Foundation• June Wedd, American Dairy Association
& Dairy Council
Acknowledgements
The Osteopathic Heritage Foundation and Children’s Hunger Alliance thank those who helped contribute to the community planning process:
i Healthy & Fit: A Community Action Plan for Franklin County Children

Strategy Team Members• Mary Beth Arensberg, Abbott Labs-
Ross Products Division• Cresha Auck, American Heart Association• Lynne Ayres, Foundation for Healthy Communities• Gail Baker, Central Ohio Restaurant Association• Diane Barnes, Columbus Public Schools• Diane Bennett, Action for Children• Andrea Cambern, WBNS-10 TV, Inc.• Tom Carlisi, The Winners League• Marie Carmen Lambea, Ohio Hispanic Coalition• Julie Carrier, Ohio Food Industry Foundation• Vonda Castro, Communities in Schools• Suzanne Christman, Dietetics Association• Diane Conley, Westerville City Schools• Linda Day Mackessy, YMCA of Central Ohio• Hannah Dillard, City of Columbus• Rosalyn dePalo, Osteopathic Heritage Foundation• Pam Early, South Western City Schools• Mike Eiland, ClearChannel Radio• Lynn Esselstein, Ohio Dietetic Association• Mary Ey, Columbus Public Schools• Josephus Foster, Fountain of Hope• Chuck Gillespie, WSYX ABC 6• Humberto Gonzalez, Legg Mason • Cheryl Graffagrino, OhioHealth• Jeanne Grothaus, Central Ohio Diabetes Association• Peg Hanley, Metro Parks• Sidney Hargro, The Columbus Foundation• Sloan Harl, G & J Pepsi Co.• Judy Hatcher, Columbus Metropolitan Area
Community Action Organization• Dudley Hawkey, Columbus Public Schools• Cheryl Hay, Greater Columbus Chamber of Commerce• Laura Hill PhD, The Center for
Eating Disorders & Psychotherapy• Alan Huff, Neighborhood House• Mattie James, Child Development Council Head Start• Saunie Jones, White Castle System, Inc.• Kim Kelly-Bartley, White Castle System, Inc.
• Mary Kershaw, The Ohio State University Extension, Franklin County
• Betsy Loeb, Action for Children• Manisha Maskay PhD, Columbus Health Department• Pete McGinty, Experience Columbus• Pat McKnight, Mount Carmel College of Nursing• Hugo Melgar-Quinonez, The Ohio State University• Karen Morrison, OhioHealth• Sara Neikirk, Communities in Schools• John O’Meara, Columbus Metro Parks• Joy Parker, Mount Carmel Outreach• Kellee Patterson, Children's Hospital• Dave Proctor, Columbus Metropolitan Area
Community Action Organization• Nancy Rini, Columbus Public Schools• Laura Rooney, American Cancer Society,
Ohio Division• Shelly Roth, Children's Hunger Alliance• Gary Serelson, Columbus Recreation & Parks• Vicky Steck, Sanese Services• Maggie Summers, United Way of Central Ohio• Mari Sunami, Southside Settlement House• Jason Tinch, Directions for Youth• Carol Trowbridge, YWCA• Eric Troy, Eternal Sports• Michelle Vander Stouw, United Way of Central Ohio• Steve Votaw, Directions for Youth• Noreen Warnock, Greater Columbus Foodshed Project• June Wedd, American Dairy Association
& Dairy Council • Vanessa Williams, Greater Columbus
Chamber of Commerce• Jerome Willis, Trinity Baptist• Julie Winland, Columbus Public School Nurses• Greg Winslow, American Heart Association• Heather Witt, Columbus Medical
Association Foundation• Sylvia Wooden, New Fellowship of Christians Church• Sally Yurchuck, United Way of Central Ohio
iiHealthy & Fit: A Community Action Plan for Franklin County Children

1. Research and evidence-based, effective programming will be at the core of the efforts.
2. The plan will be guided by strong leadership and provide for input from a variety of community sources.
3. It is critical to remain sensitive to the needs and beliefs of the varied cultures in Franklin County.
4. The plan will build upon existing services, expanding and enhancing organizational capacities where appropriate.
5. Collaboration is essential in this multi-faceted, multi-sector approach to influence policy, expand programs and make a significant impact.
6. Community members, especially those in under-resourced neighborhoods, mustbe involved in the developmental andinterventional processes.
7. The role of parents must be recognized and respected.
8. Communication efforts will be simple, consistent and evidence-based.
9. The plan will be dynamic, evolving as new evidence, models and programs emerge.
10. An effective leadership structure is necessary to sustain a unified, consistent and successful community wide effort.
11. Quality outcomes measurement is necessary to demonstrate impact.
Executive Summary
G U I D I N G C O N C E P T S
The Osteopathic Heritage Foundation,aware of and concerned about the growingprevalence of overweight children inFranklin County, earmarked foundationfunding to address the issue. Thus began aprocess to create a comprehensive communityplan based on primary research and literaturereview, as well as local leadership and community input from a variety of sources. A socio-ecological model was utilized toidentify and develop strategies to fullyengage those who are in the position ofinfluencing nutrition and fitness choices of our youth and families.
A Leadership Council was convened to provide insight, establish guiding conceptsand develop a vision and mission for theeffort. The Leadership Council includedrepresentatives from the OsteopathicHeritage Foundation, Columbus MedicalAssociation Foundation, ColumbusFoundation, United Way of Central Ohio,Columbus and Franklin County healthdepartments, Cardinal Health, The OhioState University, Columbus City Council,Franklin County Commissioners and a pediatrician. Children’s Hunger Alliance facilitated the process.
1 Healthy & Fit: A Community Action Plan for Franklin County Children & Families

Franklin County zip codes with highest prevalence of overweight adults.
Obesity has risen to epidemic levels in the U.S. It leadsto devastating and costly health problems and reduces lifeexpectancy. Obesity is a significant risk factor for seriousconditions such as type 2 diabetes,heart disease, certain cancers and is associated with depression andseveral other medical conditions.1
The economic impact of obesity has grown dramatically. In 2000,the total cost related to obesity –including both health care andexpenses and the loss of productivity– was estimated to be $117 billion($61 billion direct and $56 billionindirect).2 This estimate of cost is 9.1% of total US health care expenditures.
According to the 2000 Franklin County/Columbus Health Assessment, the highestprevalence of overweight adults is found in the following urban zip codes:
Downtown Columbus 43215 5. 43211 = 69.3%
3. 43219 = 70.0%
1. 43203 = 71.7%
43205 = 64.2%
43206 = 62.3%
6. 43232 = 66.4%
4. 43207 = 69.6%
2Healthy & Fit: A Community Action Plan for Franklin County Children & Families
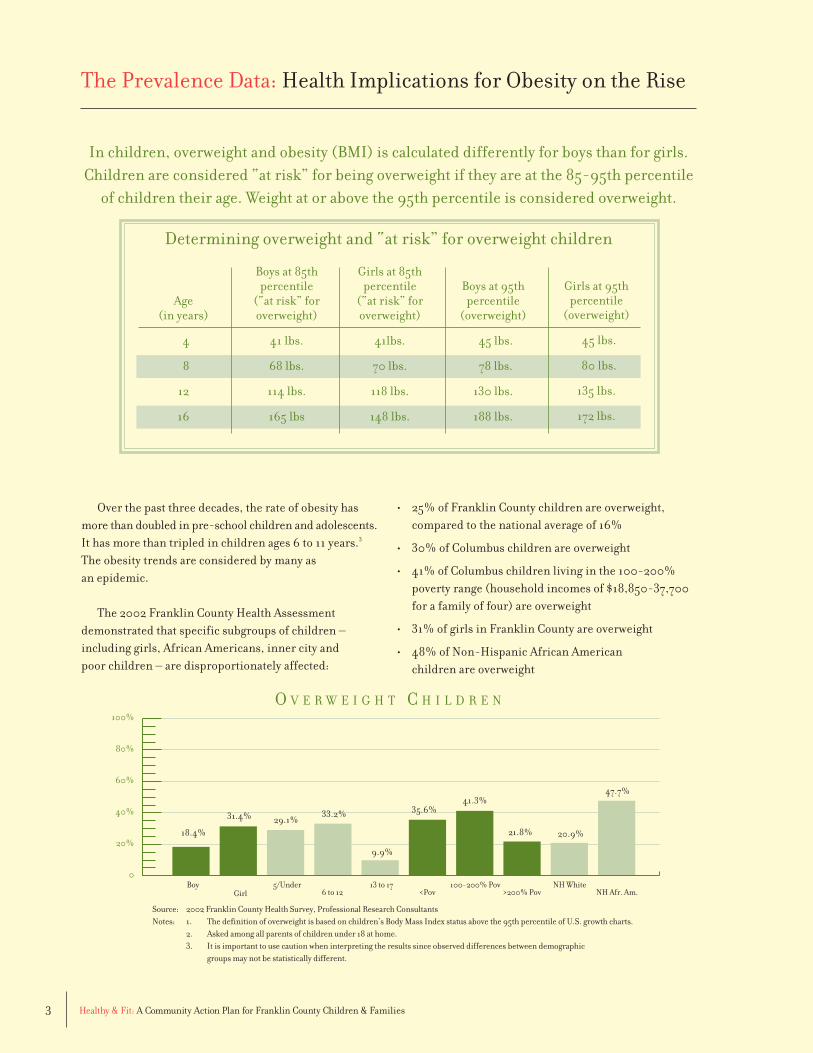
The Prevalence Data: Health Implications for Obesity on the Rise
2. 43223 = 70.3%
Obesity in adults is stated in terms of body massindex, (BMI), a measure defined as weight relative toheight (kg/(m2)). In adults, being overweight is defined
as a BMI ≥ 25, and obesity as a BMI ≥ 30.
A 5’10” man’s, healthy weight would be 130-179 pounds (BMI of 19-24).He would be considered overweight at180-209 pounds (BMI of 26-29). At 210pounds or more, he would be consideredobese (BMI 30 or higher). For FranklinCounty adults in 2002, self reportedheights and weights indicated that 61.7%of adults were overweight and 26% obese.
“I like to
jump rope,
jog, run,
play with
the dog.”
– 9 yr old female
The Prevalence Data: Health Implications for Obesity on the Rise
3 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
Over the past three decades, the rate of obesity has more than doubled in pre-school children and adolescents.It has more than tripled in children ages 6 to 11 years.3
The obesity trends are considered by many as an epidemic.
The 2002 Franklin County Health Assessment demonstrated that specific subgroups of children –including girls, African Americans, inner city and poor children – are disproportionately affected:
Determining overweight and “at risk” for overweight children
Age (in years)
4
8
12
16
Boys at 85thpercentile
(“at risk” foroverweight)
41 lbs.
68 lbs.
114 lbs.
165 lbs
Girls at 85thpercentile
(“at risk” foroverweight)
41lbs.
70 lbs.
118 lbs.
148 lbs.
Boys at 95thpercentile
(overweight)
45 lbs.
78 lbs.
130 lbs.
188 lbs.
Girls at 95thpercentile
(overweight)
45 lbs.
80 lbs.
135 lbs.
172 lbs.
In children, overweight and obesity (BMI) is calculated differently for boys than for girls. Children are considered “at risk” for being overweight if they are at the 85-95th percentile
of children their age. Weight at or above the 95th percentile is considered overweight.
• 25% of Franklin County children are overweight, compared to the national average of 16%
• 30% of Columbus children are overweight
• 41% of Columbus children living in the 100-200%poverty range (household incomes of $18,850-37,700for a family of four) are overweight
• 31% of girls in Franklin County are overweight
• 48% of Non-Hispanic African American children are overweight
0
20%
40%
60%
80%
100%
18.4%
31.4% 29.1%33.2%
9.9%
35.6%41.3%
21.8% 20.9%
47.7%
BoyGirl
5/Under6 to 12
13 to 17<Pov
100-200% Pov>200% Pov
NH WhiteNH Afr. Am.
O V E R W E I G H T C H I L D R E N
Source: 2002 Franklin County Health Survey, Professional Research ConsultantsNotes: 1. The definition of overweight is based on children’s Body Mass Index status above the 95th percentile of U.S. growth charts.
2. Asked among all parents of children under 18 at home.3. It is important to use caution when interpreting the results since observed differences between demographic
groups may not be statistically different.

4Healthy & Fit: A Community Action Plan for Franklin County Children & Families
The Process: Developing a Community Action Plan
The collaborative effort brought together various serviceproviders and stakeholders involved in the nutrition andfitness of youth in Franklin County. A Leadership Councilwas formed, consisting of local foundation, corporate,government and health leaders, to bring knowledge, skills, and resources to the initiative. A Strategy Team, with broad-basedmembership across ninecommunity sectors, providedadditional advice andknowledge to ensure anassessment was conductedin the most effective manner. Expert AdvisoryCommittees provided content in the areas ofsurvey design, nutrition,
physical activity, culturalconsiderations, and socialmarketing. The Ohio State University College of Human Ecology provided faculty as well as undergraduateand graduate student support for survey design, conductingfocus groups and interviews. The effort involved an evaluation of community assets, best practices, modelprograms and gaps in services. This led to the developmentof a long-term strategic plan designed to overcome issuesand barriers contributing to the prevalence of overweightchildren as well as to identify funding streams to supportstrategic recommendations.
Assessment methodology included gathering data and input from a variety of sources, including families,schools, businesses, government, early childhoodproviders, the food and fitness industries, the media, the medical community and the faith-based community.This was important as the intent was to identify major
contributing factors from the perspective of professionals, parents, and kids. Results from a Key Stakeholder Surveyrevealed the actions variouscommunity sectors can taketo address childhood over-weight and the behaviorscontributing to the trends. Parent Focus Groups disclosed the food and fitness behaviors
and barriers that contribute to the issue in various neighborhoods. Sixteen Child Focus Groups providedinsight into youth food and fitness behaviors and perceptions. National experts were interviewed, someduring visits to Chicago, San Diego, and Cleveland, tolearn more about successful strategies and programs used in other cities. Also, a Literature Review assessing clinicalpublications, quality evidence-based programming andposition papers provided substantial knowledge of thecontributing factors and potential opportunities foraddressing the childhood obesity epidemic.
“Raven said that it
is good for you to exercise.”
– 8 yr old female
5 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
The Findings: Behaviors Contributing to Overweight Prevalence
Addressing this health issue is complex due to the genetic, cultural, socioeconomic, psychological, and environmental factorsinvolved. Over several decades, these factorshave produced a gradual trend toward ‘energyintake’ greater than ‘energy expenditure’, resulting in more people being overweight. The following findings are an indication of this imbalance:
Nutrition• The average infant consumes 10-23% more calories
than the Estimated Energy Requirement 4
• Carbonated soft drinks account for more than 50% of American children’s total beverage consumption 5
• In middle and high schools, 75% of the drinks and85% of the snacks are of poor nutritional value 6
• The increase in portion size parallels the prevalence of overweight and obesity 7
• When used as a reward, food usually tends to be of low nutritional value 8
Physical Activity• Children attending daily physical education
dropped from 42% in 1991 to 32% in 2001 9
• 48% of girls and 26% of boys do not exercise vigorously on a regular basis 10
• Children spend an average of five-and-a-half hours a day watching TV and using media such as computers and video games 11
• Exposure to media advertising and obesity are positively correlated 12
• Televised advertising messages lead to unhealthy eating habits, particularly for children under eight years of age who are unable to understand the difference between information and advertised messages. 13
Environmental Findings• Many parents do not feel their children are safe
when they play outside 14
• Low-income families have limited access to physical activity venues 8
• Low-income communities often have limited access to nutrient-rich and low calorie foods 8
• Uninformed parents misjudge their children’s weight status and misunderstand the health implications of excess weight 14
• Children are more likely to have an active lifestyle if their parents exercise with them 14
• Research confirms the need to deliver consistent food and fitness messages that are positive, realistic,make life easier and relate to alleviation of disease. 15

6Healthy & Fit: A Community Action Plan for Franklin County Children & Families
The Findings: Behaviors Contributing to Overweight Prevalence
From Vision to Resulting Key Behaviors:Once the factors and trends leading to
childhood overweight and obesity were understood, a Socio-Ecological Model was applied to identify the main sectors of the community that influence children’slives and behaviors. The model, used successfully byother communities to achieve behavior change, identifiesgroups that are key to achieving a change in youth and family eating and physical activity habits.
Although the solution to the childhood overweight epidemic may seem as simple as balancing the equation of “energy in = energy out”, the issues are complex andinvolve societal and individual behavior changes to influence overfeeding and physical inactivity. Impactingbehavior changes throughout a community requires acommitment from families, schools, faith organizations,community organizations, the food and fitness industries,the medical community, the media, and government.Each sector must be involved in the sustained prevention
effort, providing programming and support as well as communicating a consistent message about healthyfood and fitness behaviors.
A successful collaborative effort will result in a widespread practice of six key behaviors for maintaining a healthy and fit weight in children:
1. Children are active for at least 60 minutes every day
2. Infants and children gain motor skills for lifetime activity
3. Children limit TV and video game/computer use time to less than 2 hours a day
4. Parents and guardians provide infants and childrenwith nutritious, age-appropriate foods. Infants arebreastfed, when possible
5. Caregivers and schools provide children with nutritious portions of food that meet energy needs
6. Children choose nutrient-rich foods and healthfulbeverages that meet energy needs
Media Government
Food IndustryNeighborhood Environment
SchoolsMedical Community
Early Childhood Providers
AfterschoolTime/Faith-based
Societal Level
Community Level
Inter-personal Level
CHILD
Family
The Workplace
Policy
S O C I O - E C O L O G I C A L M O D E L

Following is a summary of how sectors identified in the Socio-Ecological Model will fulfill their respective roles in ensuring Franklin County’s children are healthy and fit. Detailed strategies are included later in this report.
7 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
LeadershipAn effective leadership infrastructure will sustain a
unified, consistent and community wide effort to providenutrition and physical activity resources for children.
This work will be done by a facilitating entity, with guidance from the Leadership Council and supportfrom the Strategy Team, Expert Advisory Workgroups and contracting strategic partnerships. This entity will be instrumental in increasing awareness, engaging stakeholders, generatingresources, implementing/assisting others in implementing programs,and assessing and reportingprogress on food and fitnessbehaviors. Work will includecreating a community widesocial marketing campaigntargeted at parents and youthwith positive messages frommany sectors; assessing thecultural appropriateness of programs; creating anevaluation system to measure effectiveness of community programs; and continuing to support consumer and best practices research for effective programming.
The CommunityLocal government, food and fitness industries, and
community-based organizations will expand existingefforts to provide healthy nutrition and physical activityprograms and venues.
Local government agencies have critical roles to play and can make the health of children a priority by a)helping to increase resources; and b) by supporting thedevelopment of policies that promote access to healthyfood, and environments that foster physical activity.
Government agencies will partner to develop andimplement an integrated plan for Columbus and FranklinCounty. The plan should be based on an assessment of current status related to community access to
healthy food and opportunitiesfor physical activity.
The food industry will increase access to and provideinformation about healthy foodchoices; develop educational tools for grocers; provideimproved nutrition informationon restaurant menus; and offer more nutritious foods in restaurants, vending machinesand other food purchase venues.The fitness industry will provideconvenient recreation and fitnessopportunities – especially to
underserved populations – by supplying resources and in-kind support to communities.
By coordinating existing efforts and resources,Community-based organizations, neighborhood leaders and residents will improve access to food sources, educate and deliver culturally appropriate services to low-income families, and locally promote a lifestyle of healthy nutrition and fitness.
Strategies for Providing a Healthy Food and Fitness Environment for Children

8Healthy & Fit: A Community Action Plan for Franklin County Children & Families
The Education SystemEarly childhood programs, schools, and after-
school programs will provide a positive environment to help children gain skills, knowledge, and habits for lifetime fitness.
Early childcare providers have a direct impact at a critical age for developing life-long food and fitnessbehaviors. Building on existing initiatives, childcareproviders will offer nutritious food, utilizing USDA funded food and resources where possible, and willschedule time for daily physical activity.
Schools will teach healthy eating and fitness behaviors and will provide nutritious food and dailyphysical activity, establish wellness councils, expand federally funded school breakfast and lunch programsand provide high nutritional valued foods in vendingmachines. Schools will be encouraged to incorporate BMI and related nutrition and fitness information inroutine health screenings, appropriately communicatingfindings to parents and guardians. Schools will explorethe possibility of creating a “model school feeder system”that bundles multiple interventions into one school system. If successful, this feeder system can serve as a model for future initiatives.
After-school programs, through existing initiatives, will provide an environment and curriculum to supportnutrition education, healthy eating, utilizing USDA funded food and resources where possible, and daily physical activity.
FamiliesThe medical community, faith-based providers, and
employers will deliver effective programming, consistentmessages, and support to help families adopt healthfulfood and fitness practices.
Physicians and other health providers have significant influence and will offer families a broad spectrum of advice, education and services. This willinclude providing advice focusing on prevention andeducation activities, intervention and referrals for theco-morbid conditions of obesity including endocrine,gastrointestinal, cardiovascular, nutritional, and sleepconditions. Research will help identify best practices in education, prevention, and intervention and these best practices will be provided to physicians and they will be encouraged to utilize family visits to promote food and fitness behaviors.
Faith-based organizations will support the health and fitness of their members by providing internal healthprograms, group support services and positive messagesabout the benefits of healthful food and fitness behavior.
Employers will provide information, incentives and programs for workers to adopt healthful food and fitness practices for their families. Employers will be encouraged to adopt proven fitness programs,supporting obesity prevention efforts with employeeincentives, and participating in the countywide social marketing campaign.
Strategies for Providing a Healthy Food and Fitness Environment for Children
“Without family you
wouldn’t have any support.”
– 13 year old male
9 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
The future of this initiative has beeninformed by the partners of the community planning process over this past year. Theirrecommendations describe an ongoing leadership infrastructure to support the work of all and facilitate funding, implementationand evaluation of the effort. The key leadershipcomponents of this community initiativeinclude the following:
Facilitating Entity• Each sector will be involved in the sustained
prevention effort, providing programming and support as well as communicating a consistent message about healthy food and fitness behaviors. The facilitating entity will ensure that the effort’sstrategies stay focused, relationships are built and maintained, additional funding is secured and the evaluation and social marketing efforts are informative as well as comprehensive.
Leadership Council• The role of the Leadership Council is to assure
the mission and vision are realized and to support the initiative with time, influence and resources. The Leadership Council will review progress, assureresources and funding are utilized effectively and a social marketing campaign, policy initiatives, and evaluation are carried out.
Strategic Working Groups• Strategic working groups will develop more
specific plans for each sector, advise on plan content,progress, additional needs, message/media, policy,funding and evaluation components. Each committeewill be based on one of the following sectors:• Government Agencies• Education Systems• Community and Faith Based Organizations• Medical and Health• Food and Fitness Industry and Corporations• Marketing/messaging
Using the strategies from this report, the leadership infrastructure will produce specific and detailed actions aimed to promote positive fitness behaviors. Collectively, the work of this infrastructure will result in the engagement of the broader community via a planned approach. It is a system that encourages all sectors of the community to work in concert toencourage good nutrition and physical activity and to make resources available that support healthy choices and quality lifestyles. Some of these actions can occur immediately, while others will take longer to implement. Overall, this leadership infrastructure is adaptable to the ever changing needs of the community effort to address obesity in children and families.
Continuing the Effort
“… my kids are seeing it first hand now with my mom being ill … then I had diabetes … I lost 30 lbs …
we are all more aware of what we eat.”

10Healthy & Fit: A Community Action Plan for Franklin County Children & Families
It is important to note the challenges faced by the community in impacting positive behavioral changes and reversing the reported trends toward overweight and obesity. Significant and measurable progress will take years and will only occur with thesteadfast commitment of the partners that have provided input into the definition of the problem and requisite long-term strategies to impact the health status of the community. Just as changes in tobacco use have taken generations, we believe to truly impact the issue of obesity in children and families will also take decades. This work, while well planned and thoughtful, is a beginning step in a long-term effort.
New partnerships, visions, and ideas are forming as a result of the meetings of leadership and strategyteams. A collective understanding of the severity of the
1 US Dept of Health and Human Services. Strategic plan for NIH obesity research. NIH publication no. 04-5493. August 2004.2 DHHS (U.S. Dept of Health and Human Services). 2001a. The Surgeon General’s Call to Action to Prevent and Decrease
Overweight and Obesity. Rockville, MD: Public Health Service, Office of the Surgeon General3 Ogden CL, Flegal KM, Carroll MD, Johnson CL. 2002a. Prevalence and trends in overweight among US children and adolescents,
1999-2000. J Am Med Assoc 288(14): 1728-17324 Feeding Infants and Toddlers Study: What foods are infants and toddlers eating? J. Am Dietic Assoc. (2004) 104:S22-S305 Kennedy E, Powell R. Changing eating patterns of American children: a view from 1996. J Am Coll Nutr 1997;16:524-9 6 Carangelo C. Why are Americans so fat? Food Management. 1995; 30:63-687 Young LR, Nestle M. The Contribution of Expanding Portion Sizes to the US Obesity Epidemic.
American Journal of Public Health. 2002; 92:246-2498 Chamberlin LA, Sherman SN, Jain A, Powers SW, Whitaker RC. The Challenge of Preventing and Treating Obesity
in Low-Income, Preschool Children. Arch Pediatr Adolesc Med. 2002;156:662-6689 CDC, Youth Risk Behavior Survey, 199910 CDC, Youth Risk Behavior Survey, 199911 Roberts D, Foehr U., Kids & Media in America, (Cambridge, MA: University Press, 2004)12 Kaiser Foundation. The Role of Media in Childhood Obesity. (Issue Brief, February, 2004: pg. 5)13 Wilcox BL, Kunkel D, Cantor J, Dowrick P, Linn S, Palmer E. 2004. Report of the APA Task Force on Advertising and Children.
Washington, DC: American Psychological Association14 The Robert Wood Johnson Foundation. Active Living, Diversity Project Report. 2003 15 The Robert Wood Johnson Foundation. Active Living, Diversity Project Report. 2003
problem, its impact on health, and mobilization of the community to address it is realized now more thanever. The common theme in key stakeholder gatheringsthroughout this assessment process has been to shift thesocial paradigm to a new direction, or create a “tippingpoint” for healthier children and families. It is up to theFranklin County community to advance the initiative to the point where we can state with confidence that our children and families are healthy and fit.
Contact Information:If you are interested in getting more information
about the content of this report and/or are interested in participating in this community initiative, please contact:
J.D. BeitingChildren’s Hunger Alliance
(614) 341 7700 x [email protected]
Conclusion

11 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
L O G I C
Nutrition• The average infant consumes
10 to 23% more calories than theEstimated Energy Requirement16
• Carbonated soft drinks account for over 50% of American children’stotal beverage consumption17
• A survey of vending machines in middle and high schools reports 75% of the drinks and 85% of the snacks are of poor nutritional value18
• The trend toward larger portion sizes has occurred in parallel with increases inthe prevalence of overweight and obesity18
• Food is used as a reward, and usuallytends to be food of low nutritional value19
Physical Activity • The percentage of children attending
daily physical education dropped from 42% in 1991 to 32% in 200120
• A Centers for Disease Control andPrevention (CDC) survey reports 48% of girls and 26% of boys do notexercise vigorously on a regular basis.21
• Children today spend an average of five-and-a-half hours a day watching TV and using media.22
• At least 6 studies positively correlatemedia advertising and obesity 23
• The American Psychological Association recently concluded that televised advertising messages can lead to unhealthy eating habits, particularly for children under eightyears of age who are unable to criticallycomprehend advertised messages.24
Environmental Factors • Parents do not feel that their children
are safe when they play outside25
• Low income families have limited access to physical activity venues 26
• Low income communities often havelimited access to nutrient rich and low calorie food.25
• Uninformed parents misjudge their children’s weight status and misunderstand the health implications of excess weight 27
• Parents want their family to be healthy and do the right thing 27
• Children are more likely to have an active lifestyle if their parents exercise with them 28
• Research confirms the need to deliverconsistent food and fitness messages thatare realistic, make life easier, are positive,and related to alleviation of disease. 29
References for Contributing Factors are listed on following page
Leadership InfrastructureCreate an infrastructure representing all sectors to: • Sustain a unified, consistent communitywide effort• Increase awareness through a communitywide social
marketing campaign aimed at parents and youth• Engage stakeholders on an ongoing basis• Identify and generate resources to support the initiative• Evaluate the effort, and report progress on the food and fitness
behaviors of children• Continue and support research on best practices and
effective programming
The Community• Franklin Co., Columbus, and local municipal leaders:
• Increase resources and support policy to improve the food and fitness of children in schools and community
• Revise zoning and capital improvement plans for future developments to include spaces for recreation and physical activity
• Increase access to nutritious food venues, gardens, and markets• Increase access and program capabilities of parks, green space,
and recreation venues• Improve the safety of streets, sidewalks, and routes to school • Continue community health assessments• Provide resources for culturally appropriate services,
including social marketing • The food industry expands access to and delivers knowledge of healthy
food choices through industry and government educational programs• The fitness industry and government entities provides convenient
opportunities for regular recreation and physical activity for families • Community based organizations and neighborhood leaders expand
community gardens, educate and deliver services to help families develop a lifestyle of healthy food and fitness
The Education System• Childcare providers are trained using evidence-based nutrition and
physical activity programming, with assistance from content specialists.• Childcare providers offer nutritious USDA funded food and physical
activities on a daily basis• Schools, school agencies, parents and other stakeholders
form school wellness councils to guide food and fitness curriculum and environment in schools
• Schools teach healthy food and fitness behaviors and provide nutritiousUSDA funded School Breakfast, Lunch and physical activity daily.
• School Health Services incorporate BMI measurement, appropriate referrals and parent education into routine health assessments.
• Schools use evaluation tools to assess the quality of food they make available to students, and they offer nutritious choices.
• After school programs provide nutritious meals, nutrition education and physical activity programs that build skills, with assistance from content specialists.
• Explore possibility of creating a model school feeder system, that bundles multiple interventions into one neighborhood
The Family• Physicians and health professionals offer families a broad spectrum of
services including a primary focus on prevention and education programs• Expand medical treatment, intervention, referral and research
programs for childhood obesity • Faith-based organizations provide programs, support services and
positive messages about the benefits of healthful food and fitness behavior • The Workplace provides information, incentives and programs
for parents to adopt healthful food and fitness practices for their family
Contributing Factors Strategies

12Healthy & Fit: A Community Action Plan for Franklin County Children & Families
M O D E L
• All key sectors participate in influencing healthful food and fitness behaviors of children
• Multi-media messages result in healthy food and fitness behaviors of youth and families
• Continued assessment and evaluation leads to successful program interventions, and improved program outcomes
• Funding is secured to continue efforts that impact food and fitness of youth
1. Children are active for at least 60 minutes every day
2. Infants and children gain motor skills for lifetime activity
3. Children limit TV and video game/computer use time to less than 2 hours a day
4. Parents and guardians provide infants and children with nutritious, age-appropriate foods.Infants are breastfed, when possible
5. Caregivers and schools provide children with nutritious portions of food that meet energy needs
6. Children choose nutrient-rich foods and healthful beverages that meet energy needs
• The physical environment of Franklin County has safe neighborhoods for walking and exercising, accessible greenspace for recreation, free or low cost activity programs and venues, and access to nutritious food for all families
• Community coalitions and public health agencies use evaluation tools to measure the impact and availability of food and fitness activities and programs
• Grocery stores and restaurants sell healthy options, portion sizes equal to energy needs, and provide resources for nutrition and physical activity education for children
• Families receive neighborhood support and resources fromcommunity based organizations to live healthy and fit lifestyles.
• All Franklin Co. childcare centers and caregivers provide nutritious food and physical activity
• Wellness councils guide healthy school environments• Healthy breakfast and lunch programs are available
in all Franklin Co. schools • Competitive food venues offer nutritious options• Franklin County schools provide 30 minutes
of continual movement daily• Model school feeder system demonstrates multiple
interventions successfully improve the food and fitness behaviors of children
• All Franklin Co. after school programs provide nutritious food and healthy physical activity environment for children
• The medical community provides effective guidance to families to help children be fit
• Faith-based organization’s provide opportunities for healthy lifestyle activities
• The workplace becomes a supportive environment for parents to receive messages and programs about healthful food and fitness for their families
Future BehaviorsOutcomes

13 Healthy & Fit: A Community Action Plan for Franklin County Children & Families
16. Fox MK, Pac S, Devaney B, Jankowski L. Feeding infants and toddlers study: What foods are infants and toddlers eating?. JADA. January 2004, (S) 104:1
17. Kennedy E, Powell R. Changing eating patterns of American children: a view from 1996. J Am Coll Nutr 1997;16:524-9
18. Young LR, Nestle M. The Contribution of Expanding Portion Sizes to the US Obesity Epidemic. American Journal of Public Health. 2002; 92:246-249
19. American Institute of Cancer Research. New Survey shows Americans ignore importance of portion size in managing weight. Available at: http://www.aicr.org. Accessed October 27, 2000.
20. U.S. Department of Health and Human Services. Physical activity and health: a report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 1996.
21. CDC, Youth Risk Behavior Survey, 1999
22. Andersen RE, Crespo CJ, Bartlett SJ, Cheskin LJ, Pratt M. Relationship of physical activity and television watching with body weight and level of fatness among children: Results from the Third National Health and Nutrition Examination Survey. JAMA 1998;279:938-42.
23. Dietz, W and Gortmaker, S., “Do We Fatten Our Children at the TV Set? Obesity and Television Viewing in Children and Adolescents”, Pediatrics 75 (1985): 807-812
24. Kaiser Foundation. The Role of Media in Childhood Obesity. (Issue Brief, February, 2004: pg. 5)
25. The Robert Wood Johnson Foundation. Active Living, Diversity Project Report. 2003
26. Burdette HL, Whitaker RC. Neighborhood playgrounds, fast food restaurants, and crime: relationships to overweight in low-income preschool children. Preventive Medicine 38 (2004) 57-63
27. Crawford PB, Gosliner W, Anderson C, Strode P, Becerra-Jones Y. Counseling Latina Mothers of Preschool Children about Weight Issues: Suggestions for a New Framework. JADA (2004) 104:387-394
28. Chamberlin LA, Sherman SN, Jain A, Powers SW, Whitaker RC. The Challenge of Preventing and Treating Obesity in Low-Income, Preschool Children. Arch Pediatr Adolesc Med. 2002;156:662-668
29. Agrams WS, Hammer LD, McNicholas F. 2004. Risk factors for childhood overweight: A prospective study from birth to 9.5 years. The Journal of Pediatrics 145(1):20-25
R E F E R E N C E S T O L O G I C M O D E L C O N T R I B U T I N G F A C T O R S
“Our communities are going to have to back each other up to make a difference in the health of our kids.”
- Mother of 4 school age children




















