Healthiest Wisconsin 2010 Status Report to the Public Health Council State Health Plan Committee...
50
Healthiest Wisconsin 2010 Status Report to the Public Health Council State Health Plan Committee (October 18, 2007) Mental Health and Mental Disorders Bureau of Mental Health and Substance Abuse Services Division of Mental Health & Substance Abuse Services Wisconsin Department of Health & Family Services
-
date post
20-Dec-2015 -
Category
Documents
-
view
214 -
download
1
Transcript of Healthiest Wisconsin 2010 Status Report to the Public Health Council State Health Plan Committee...
Healthiest Wisconsin 2010Status Report to the Public Health Council
State Health Plan Committee
(October 18, 2007)
Mental Health and Mental Disorders
Bureau of Mental Health and Substance Abuse ServicesDivision of Mental Health & Substance Abuse Services
Wisconsin Department of Health & Family Services
HW2010 MH presentation 10-18-2007 2
Presentation Outline Introduction to policy recommendations
and MH HW2010 objectives Overview of mental health in Wisconsin
Prevalence Unmet need for treatment Social and economic factors Disparities Outcomes Expenditures
Mental health HW2010 objectives past efforts, current status, and future efforts
Discussion of recommendations

HW2010 MH presentation 10-18-2007 3
Overview - Mental Health Policy/ Programmatic Recommendations
1) Enact insurance parity to combat financial barriers to access to MH care.
2) Implement screening for depression, substance abuse, and trauma in primary care.
3) Reduce health disparities for MH consumers in both primary and MH care.
4) Promote effective MH treatment.5) Combat stigma through education with
targeted audiences.
HW2010 MH presentation 10-18-2007 4
Overview of MH HW2010 Objectives
1) Increase mental health screening and referral
2) Increase cultural competence of services provided to MH consumers
3) Decrease stigma4) Increase access to care through the
use of evidence-based practices

HW2010 MH presentation 10-18-2007 5
Data Sources and Limitations National Surveys on Drug Use and Health (NSDUH)
Brief module used to define MH needs Behavioral Risk Factor Surveillance Survey (BRFSS)
Phone survey that excludes cell phone userso National Comorbidity Study (NCS) Youth Risk Behavior Survey (YRBS)
Only children in grades 9-12 included Human Services Reporting System (HSRS)
Variable quality and completeness MH/AODA Functional Screen
Adults with a serious mental illness (SMI) and for limited programs
Mental Health Statistical Improvement Project’s (MHSIP) Satisfaction Survey
Wisconsin United for Mental Health (WUMH) stigma surveys
State administrative data (expenditures, etc.)

HW2010 MH presentation 10-18-2007 6
Prevalence of Mental Health Needs for Adults
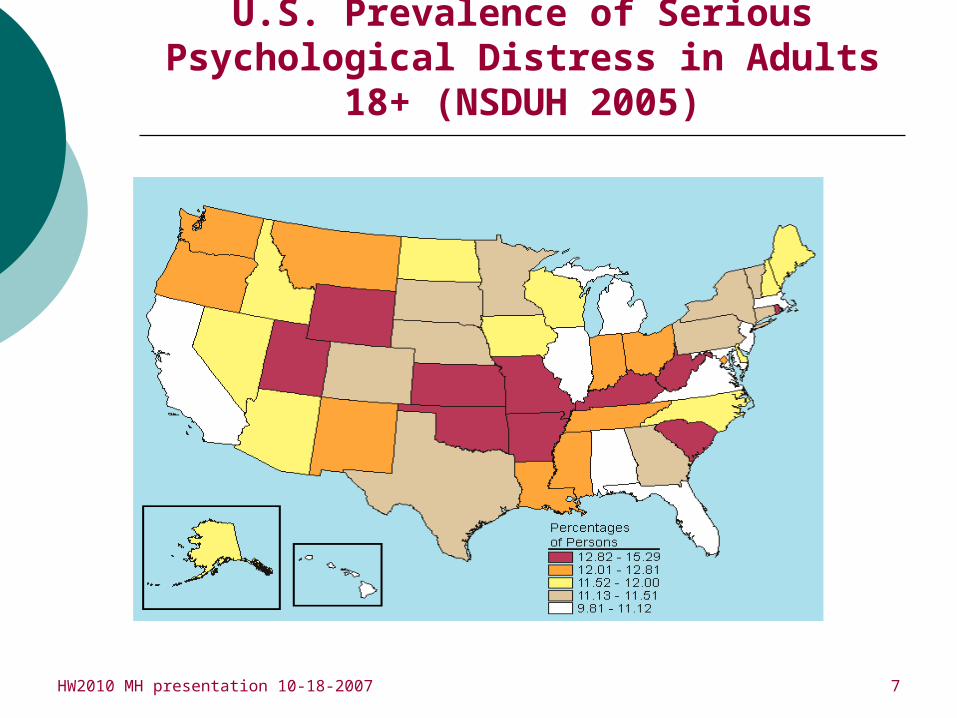
o 11.8% (486,079) of Wisconsin adults aged 18+ experienced serious pyschological distress (SPD) in the past year compared to the 11.6% national average (NSDUH, 2004-05).
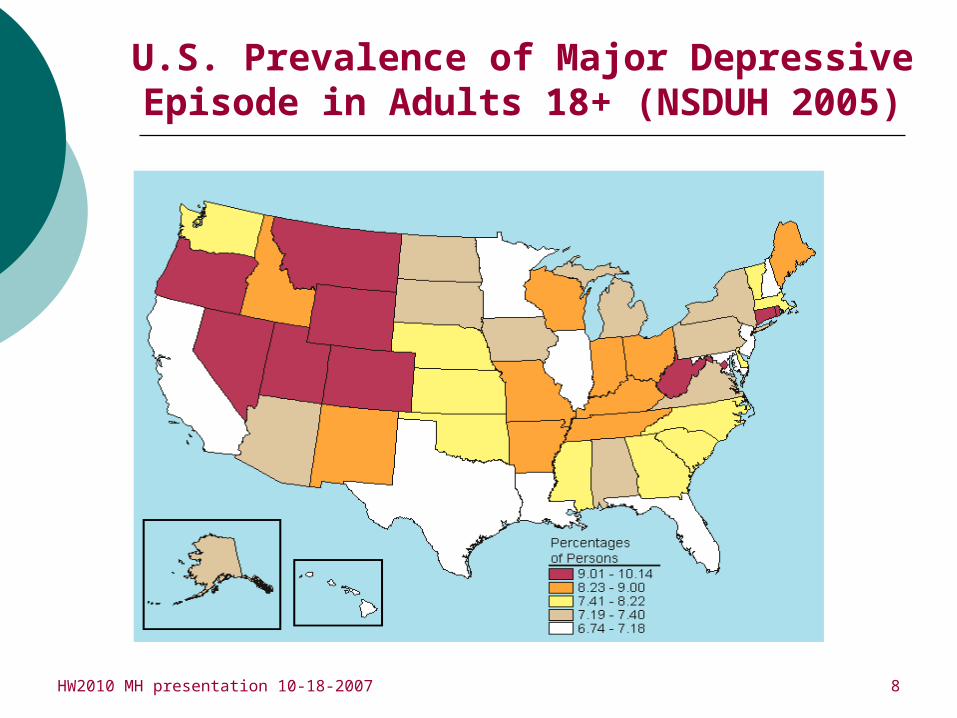
Wisconsin’s SPD national rank is 25th. 8.4% (346,022) of Wisconsin adults aged 18+
experienced a major depressive episode (MDE) in the past year compared to the 7.6% national average (NSDUH, 2004-05).
Wisconsin’s MDE national rank is 35th.
HW2010 MH presentation 10-18-2007 7
U.S. Prevalence of Serious Psychological Distress in Adults 18+ (NSDUH 2005)
HW2010 MH presentation 10-18-2007 8
U.S. Prevalence of Major Depressive Episode in Adults 18+ (NSDUH 2005)
HW2010 MH presentation 10-18-2007 9
Prevalence of Depression in Youth
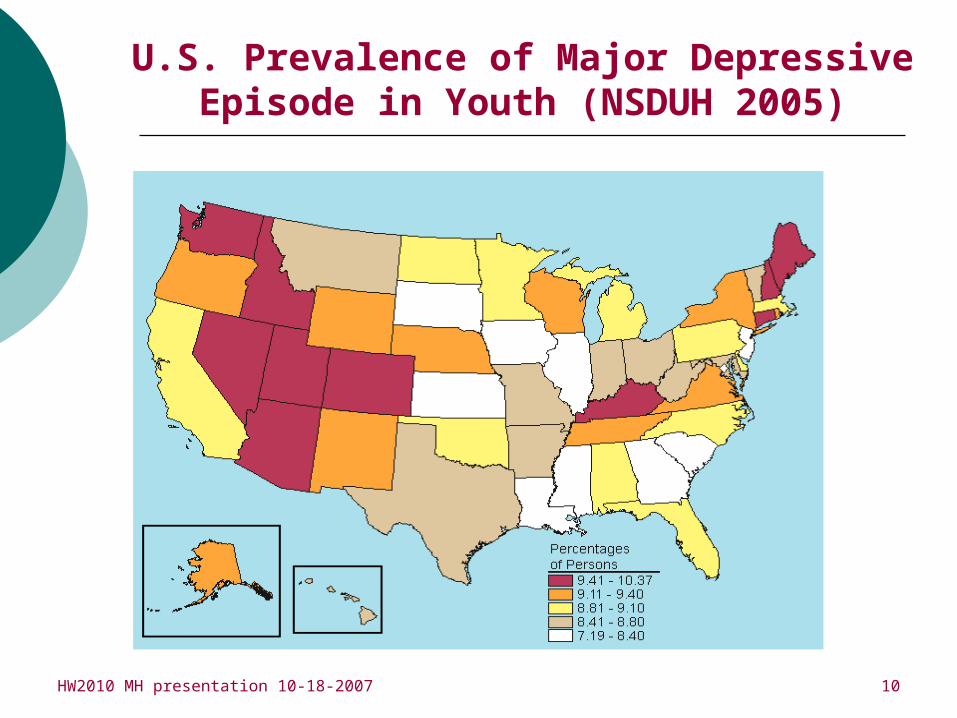
9.4% of Wisconsin youth aged 12-17 experienced a major depressive episode (MDE) in the past year compared to the 8.8% national average (NSDUH, 2004-05).
Wisconsin’s MDE national rank is 11th. 28.5% of students nationwide experienced
periods of depression that limited their functioning in 2005 compared to 27.6% in Wisconsin (YRBSS) The 2005 youth depression rate (YRBSS) in
Wisconsin increased from 25.3% in 2003. The female youth depression rate was 33.3% in
2005 compared to 22.2% for males.
HW2010 MH presentation 10-18-2007 10
U.S. Prevalence of Major Depressive Episode in Youth (NSDUH 2005)

HW2010 MH presentation 10-18-2007 11
Prevalence of Suicide Among Youth
Wisconsin ranks 8th in youth suicides in the U.S. Average WI suicide rate from 1999-2003 for 15-19 yr.
olds was 10.9/100,000. (IA-10.6, MN-9.4, IN-8.3, MI-7.8, IL-6.1).
HW2010 MH presentation 10-18-2007 12
Prevalence of Co-occurring Disorders – U.S. (NSDUH 2005)
In 2005, adults who used illicit drugs in the past year were significantly more likely to have SPD compared with adults who did not use an illicit drug (22.0 vs. 9.6 percent).
Past year illicit drug use was higher among adults with SPD (26.9 percent) than among adults without SPD (12.1 percent).
Similarly, the rate of past month cigarette use was higher among adults with SPD (42.8 percent) than among adults without SPD (24.5 percent).
Among adults with SPD in 2005, 21.3 percent (5.2 million) were dependent on or abused illicit drugs or alcohol. The rate among adults without SPD was 7.7 percent (14.9 million).
HW2010 MH presentation 10-18-2007 13
Prevalence of Co-occurring Disorders (Wisconsin, 2004-05)
The MH/AODA Functional Screen is a Wisconsin-based screen that measures level of need within Wisconsin’s major programs for mental health consumers with a serious mental illness (SMI).
Community Support Programs (CSP) Comprehensive Community Services (CCS)
Of 3,357 consumers screened in 2004-05, 70.4% had a co-occurring physical health diagnosis and 25.8% had a co-occurring substance abuse diagnosis. 17.9% had co-occurring MH/SA/physical health diagnoses.
21.6% had a MH diagnosis only. Consumers with co-occurring MH/SA diagnoses had higher
than average rates of inpatient stays, CJ system involvement, suicide attempts, and homelessness in their history.
HW2010 MH presentation 10-18-2007 14
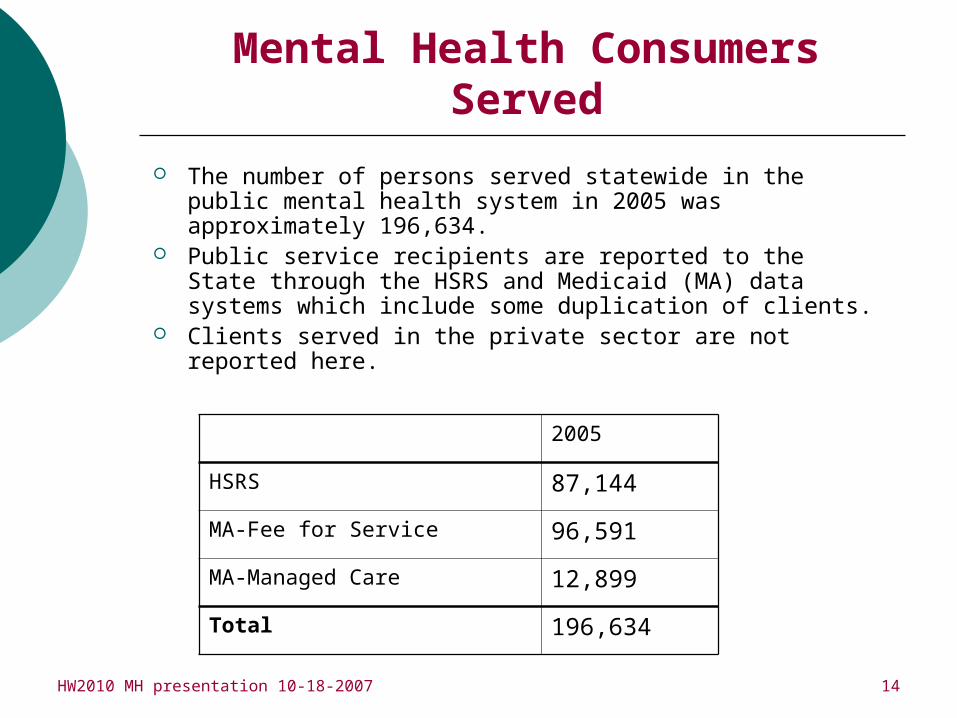
Mental Health Consumers Served
The number of persons served statewide in the public mental health system in 2005 was approximately 196,634.
Public service recipients are reported to the State through the HSRS and Medicaid (MA) data systems which include some duplication of clients.
Clients served in the private sector are not reported here.
2005
HSRS 87,144
MA-Fee for Service 96,591
MA-Managed Care 12,899
Total 196,634
HW2010 MH presentation 10-18-2007 15
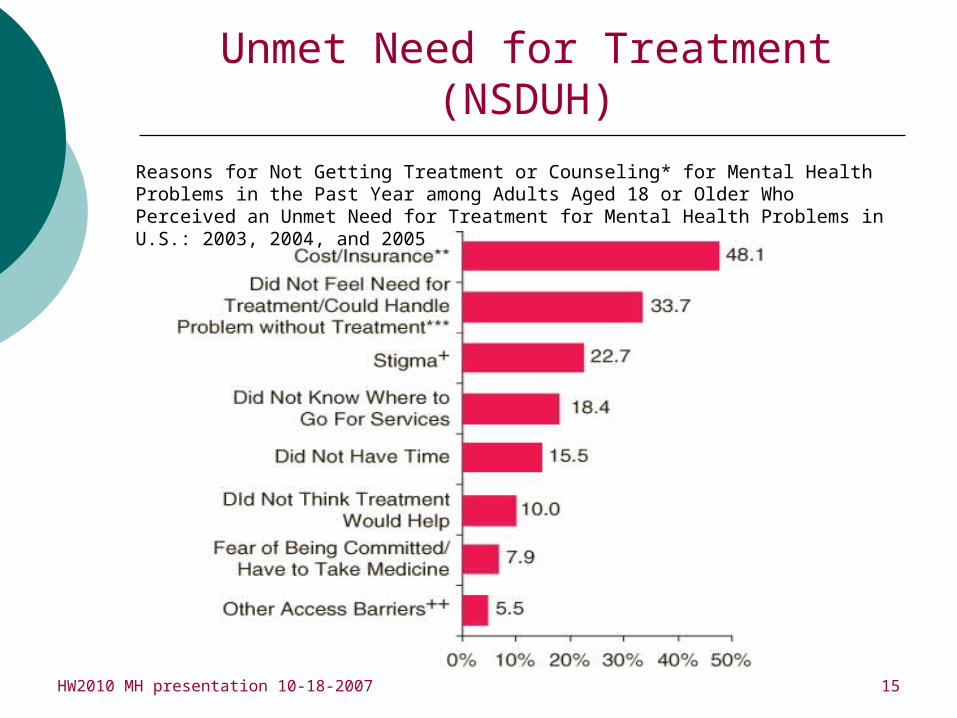
Unmet Need for Treatment (NSDUH)
Reasons for Not Getting Treatment or Counseling* for Mental Health Problems in the Past Year among Adults Aged 18 or Older Who Perceived an Unmet Need for Treatment for Mental Health Problems in U.S.: 2003, 2004, and 2005
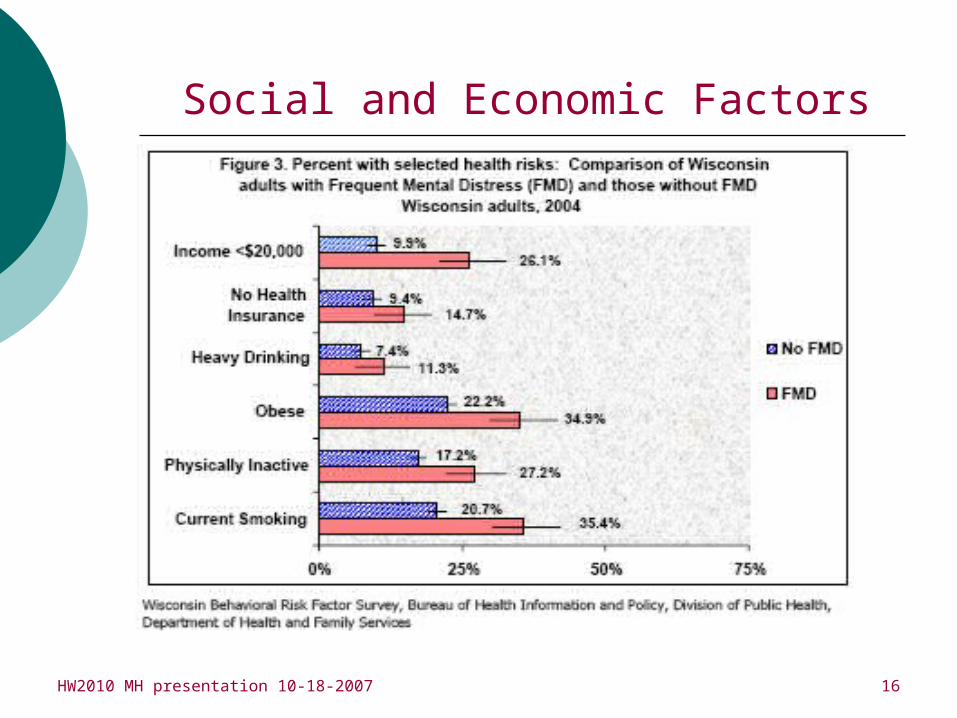
HW2010 MH presentation 10-18-2007 16
Social and Economic Factors
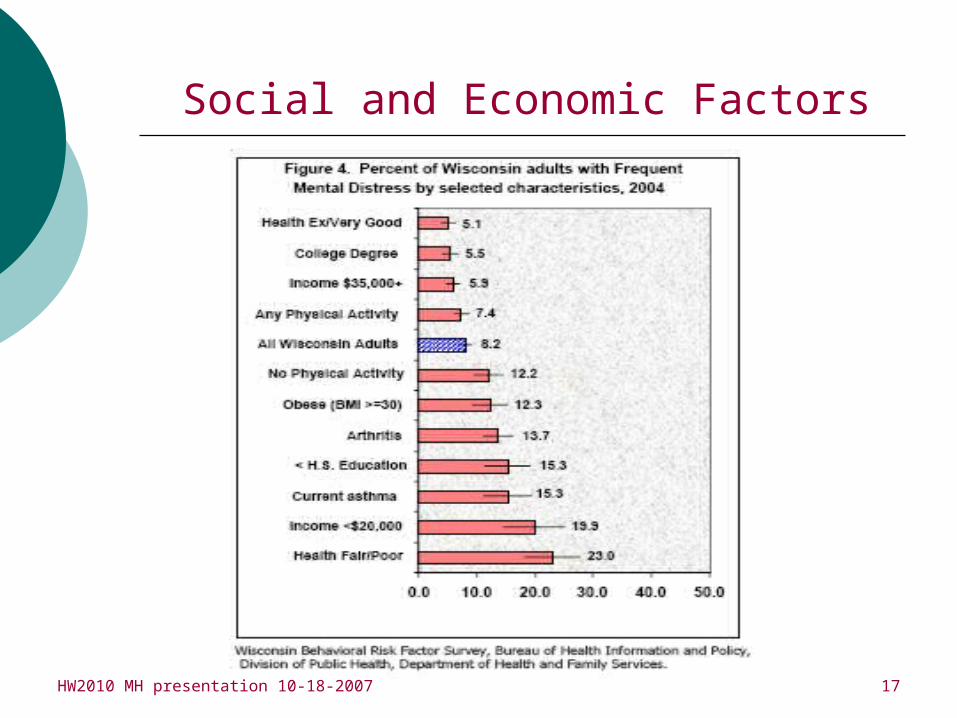
HW2010 MH presentation 10-18-2007 17
Social and Economic Factors
HW2010 MH presentation 10-18-2007 18
Social and Economic Factors - Trauma
o Approximately 8% of individuals in the U.S. – 20 million people – will be diagnosed with PTSD in their lifetime. (NTAC lit. review, 2004)
o "The more adverse childhood experiences reported, the more likely the person is to have heart disease, cancer, stroke, diabetes, skeletal fractures, liver disease, and poor self-rated health as an adult.“ (CDC, 1998)
o Up to 81% psychiatric hospital clients diagnosed with a major mental illness have experienced physical or sexual abuse. (NTAC lit. review, 2004)
o Women molested as children are at 4 times greater risk for major depression than those with no such history. (NTAC lit. review, 2004)
o More than 66% of homeless mothers have experienced severe physical violence and 43% were sexually molested during childhood. (NTAC lit. review, 2004)
o Up to two-thirds of individuals entering substance abuse treatment suffer from PTSD, or posttraumatic stress symptoms. (NTAC lit. review, 2004)
HW2010 MH presentation 10-18-2007 19
Outcomes for MH Consumers
o 28% of adult MH service recipients with a SMI were employed, 40% were unemployed, and 32% were not in the labor force (HSRS, 2005).
o 7% of adult MH service recipients with a SMI were arrested in the past year (MHSIP, 2006).
o 20% of youth MH service recipients with a SED were arrested in the past year (MHSIP, 2006).
o Studies have shown that people with mental illnesses have a 20% loss in life expectancy (Anxiety, Addiction, and Depression Treatments, Jan. 2007).

HW2010 MH presentation 10-18-2007 20
State Mental Health Expenditures*
0
100
200
300
400
500
600
700
1997 2001 2003 2005
MH
Exp
end
itu
res
(Mil
lio
ns)
Community Services Residential, Inpatient Services Total
*Federal portion of Medicaid not included. Data reported through the HSRS.
(Equitable, Adequate, and Stable Financing)
HW2010 MH presentation 10-18-2007 21
HW2010 Mental Health Objective: Increase Access to Care with EBP’s
“By 2010, Wisconsin's public mental health clients who have access to evidence-based mental health treatments will increase by 10 percent.”
Status: Improving.Notes: Need to monitor evidence-
based practice (EBP) use and implementation fidelity.

HW2010 MH presentation 10-18-2007 22
Efforts to Increase the Use of EBP’s
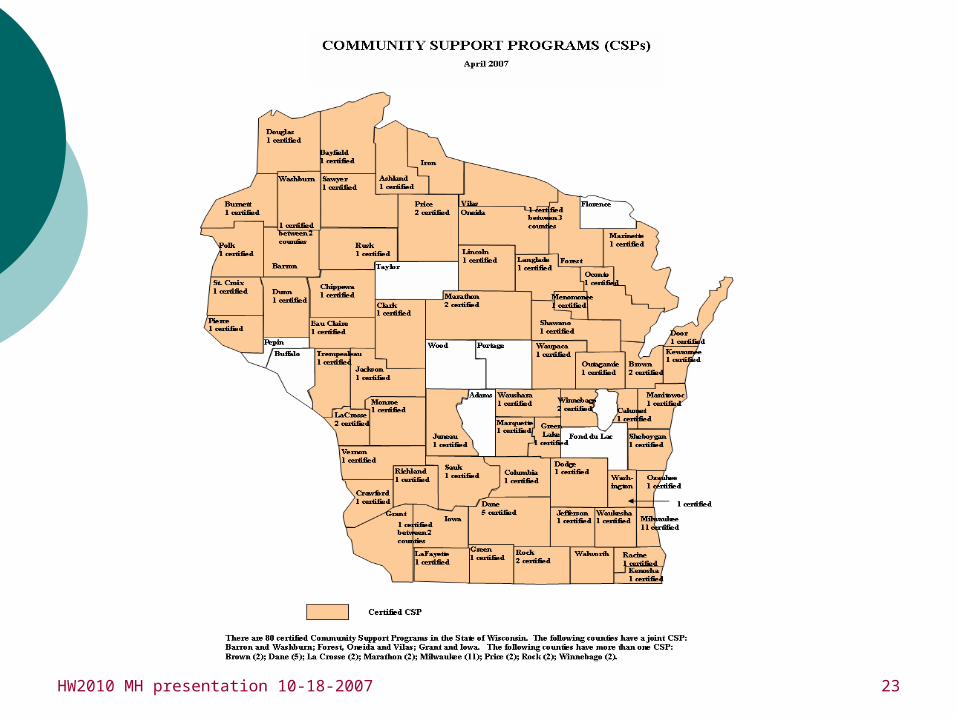
Assertive Community Treatment (ACT) recognized federally and nationally as an EBP – called Community Support Programs (CSPs) in Wisconsin
CSP is a Medicaid-reimbursable service matched with county funds
64 counties in Wisconsin currently operate 80 certified CSPs; State funds offered annually to help new counties become CSP-certified
Although based on ACT model, fidelity with which CSP is implemented is known to be variable; BMHSAS resources to monitor fidelity and provide TA are minimal.
HW2010 MH presentation 10-18-2007 23
HW2010 MH presentation 10-18-2007 24
Efforts to Increase the Use of EBPs for Consumers with a SMI
Grants to counties to implement EBPs and quality improvement systems (3 in 2006, 5 in 2007). Integrated Dual Diagnosis Treatment (IDDT) and
Motivational Interviewing – 3 counties in 2007. Illness Management and Recovery (IMR) – 2 counties in
2007. National Alliance for Mental Illness (NAMI) – WI
beginning Family Psychoeducation in 2008. DVR implemented three Supported Employment
programs from 2005-07. 2006 Bureau Conference provided training on
implementation of IDDT and other EBPs. Bureau work group currently establishing EBP
training resources for providers.
HW2010 MH presentation 10-18-2007 25
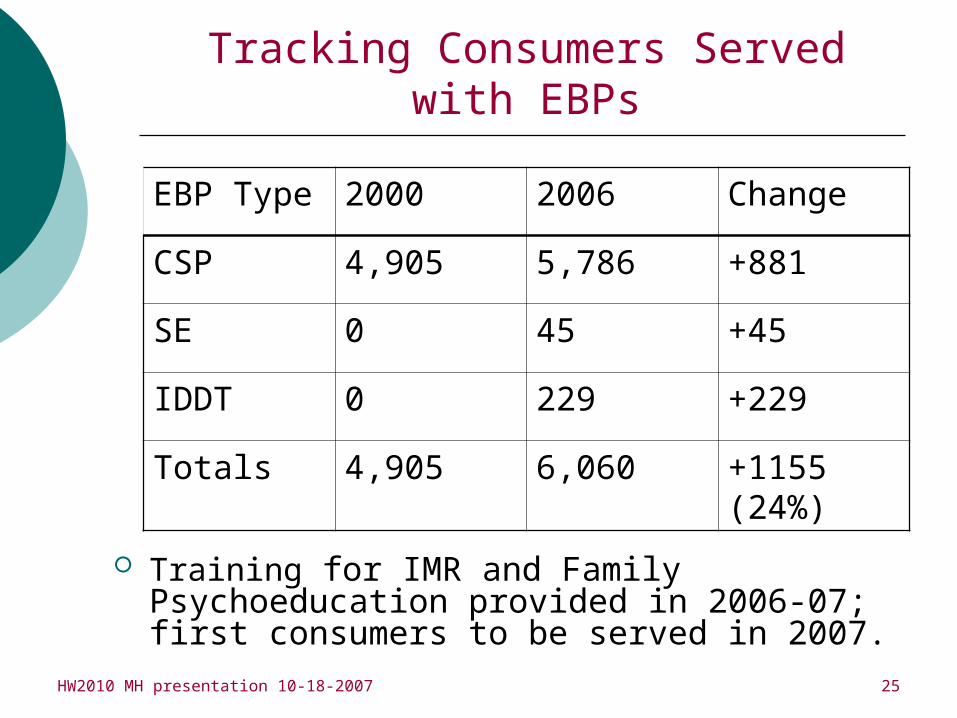
Tracking Consumers Served with EBPs
EBP Type 2000 2006 Change
CSP 4,905 5,786 +881
SE 0 45 +45
IDDT 0 229 +229
Totals 4,905 6,060 +1155 (24%)
Training for IMR and Family Psychoeducation provided in 2006-07; first consumers to be served in 2007.
HW2010 MH presentation 10-18-2007 26
HW2010 Mental Health Objective: Increase Access to Care with EBP’s
“By 2010, Wisconsin's public mental health clients who have access to best practice mental health treatments will increase by 10 percent.”
Status: ImprovingNotes: Need further work to define best
practices vs. EBPs and monitor their use and implementation fidelity
HW2010 MH presentation 10-18-2007 27
Efforts to Increase the Use of Best Practices
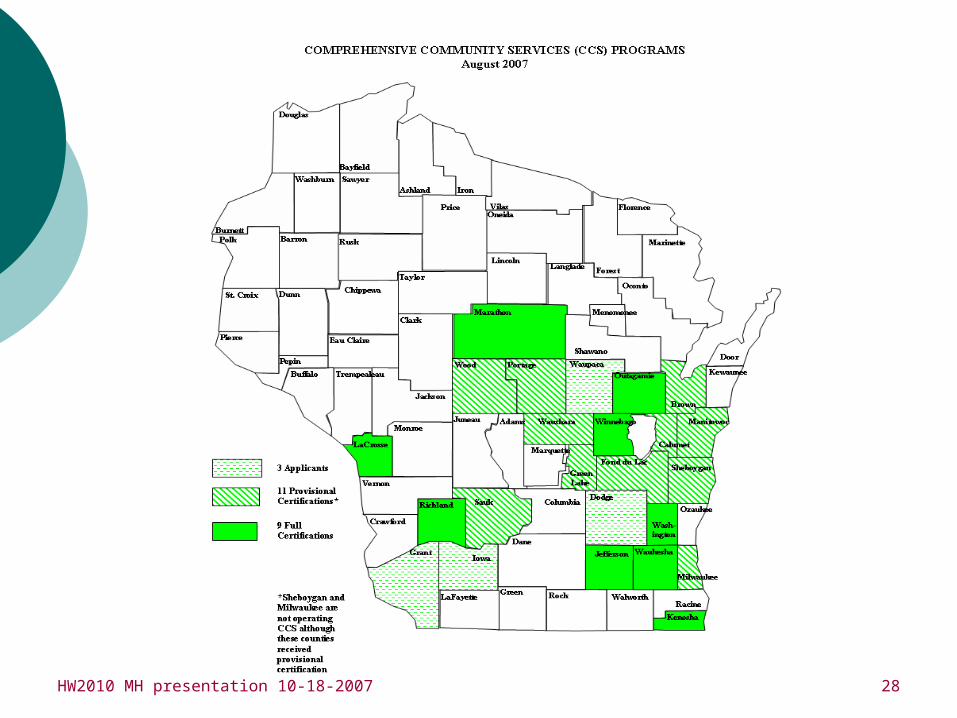
Psychosocial Rehabilitation is a federally-recognized Medicaid benefit – called Comprehensive Community Services (CCS) in Wisconsin
Children’s system of care wraparound programs – Integrated Service Projects (ISPs) and Coordinated Service Teams (CSTs)
36 counties with ISP/CSTs in 2007 Milwaukee Wraparound and Dane CCF
managed care programs
HW2010 MH presentation 10-18-2007 28
HW2010 MH presentation 10-18-2007 29
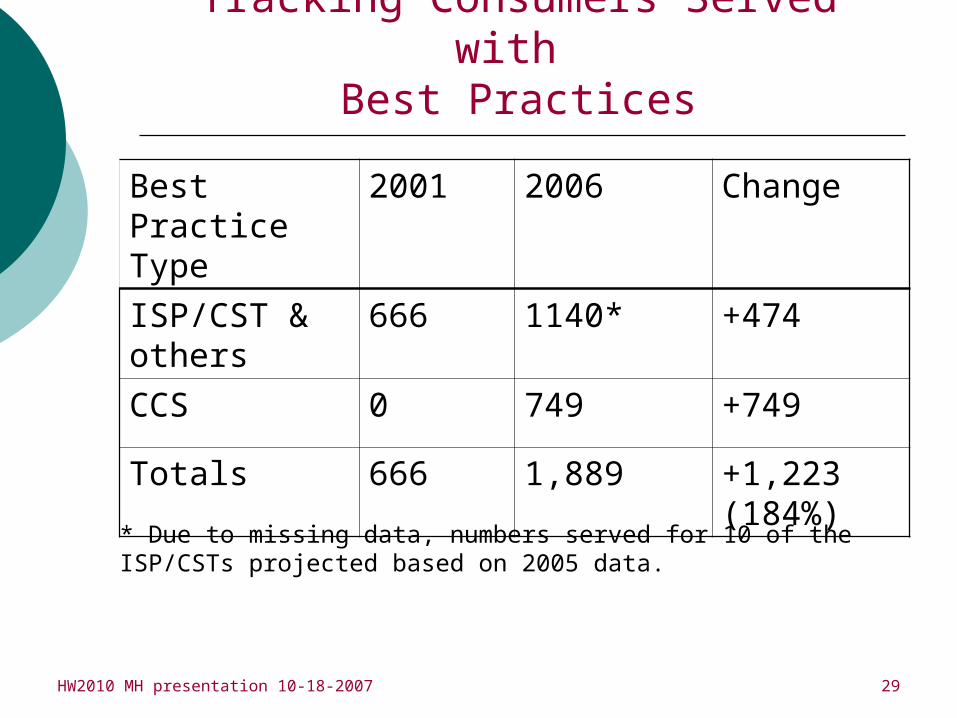
Tracking Consumers Served with Best Practices
Best Practice Type
2001 2006 Change
ISP/CST & others
666 1140* +474
CCS 0 749 +749
Totals 666 1,889 +1,223 (184%)
* Due to missing data, numbers served for 10 of the ISP/CSTs projected based on 2005 data.
HW2010 MH presentation 10-18-2007 30
HW2010 Mental Health Objective 2: Increase Cultural Competence
“By 2010, 87 percent of publicly-funded mental health consumers will feel their service provider was sensitive to their culture during the treatment planning and delivery process.“
Status: Improving with concernsNotes: Need more representative data and
need more targeted programmatic efforts and initiatives
HW2010 MH presentation 10-18-2007 31
Efforts to Eliminate Health Disparities
o Development of CSTs for Native American tribes.
Targeted grant funding for tribal system development to improve services for consumers with co-occurring disorders.
2006 focus groups on identifying Milwaukee children’s MH needs.
DHH MH interpreter training. DHH crisis and emergency preparedness work. Report on Women and Depression. Telehealth is available through the Marshfield
Clinic and a few other rural locations. DHFS has provided funding and certification.
HW2010 MH presentation 10-18-2007 32
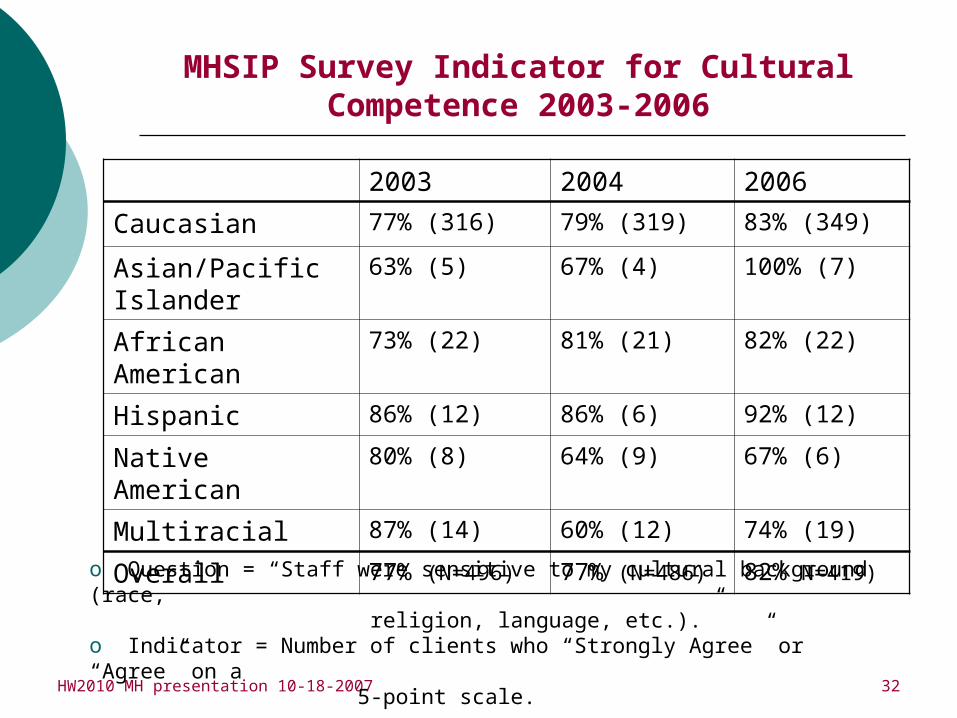
MHSIP Survey Indicator for Cultural Competence 2003-2006
2003 2004 2006
Caucasian 77% (316) 79% (319) 83% (349)
Asian/Pacific Islander
63% (5) 67% (4) 100% (7)
African American 73% (22) 81% (21) 82% (22)
Hispanic 86% (12) 86% (6) 92% (12)
Native American 80% (8) 64% (9) 67% (6)
Multiracial 87% (14) 60% (12) 74% (19)
Overall 77% (N=496) 77% (N=486) 82% N=419)
o Question = “Staff were sensitive to my cultural background (race, religion, language, etc.).”o Indicator = Number of clients who “Strongly Agree” or “Agree” on a 5-point scale.

HW2010 MH presentation 10-18-2007 33
Elimination of Health Disparities: Mental Health Prevalence by Racial and Ethnic Background
HW2010 MH presentation 10-18-2007 34
o “By 2010, an additional 15 percent of the general public will demonstrate an understanding that individuals with mental health disorders can recover through treatment to lead productive, healthy, and happy lives.”
o “By 2010, an additional 15 percent of the general public will demonstrate the belief that individuals with mental health disorders are capable of sustaining long-term productive employment.”
Status: Improving, but slowlyNotes: Challenging task to impact statewide
attitudes, but current initiatives are making an impact
HW2010 Mental Health Objective:Decrease Mental Health Stigma

HW2010 MH presentation 10-18-2007 35
Efforts to Decrease Mental Health Stigma
Within the general public, misunderstandings exist about the scientific knowledge regarding mental illness, treatment outcomes, dangerousness of persons with mental illness, and recovery.
A new MH module of the 2007 BRFSS will provide data on MH stigma to help monitor progress.
Lt. Gov. Barbara Lawton is Honorary Chair of WUMH Board and leads the Implementation Committee for the Report on Women and Depression (May, 2006).
NAMI Consumer Council tailoring website on Recovery including stigma information.
Support Grassroots Empowerment Project (GEP) - a statewide consumer-driven advocacy organization.
Mental Health Coalition of Greater La Crosse Area, Milwaukee Mental Health Task Force on Mental Health, Green Bay Mental Health Task Force for Children, Chippewa’s Children’s Mental Health all formed since 2004.

HW2010 MH presentation 10-18-2007 36
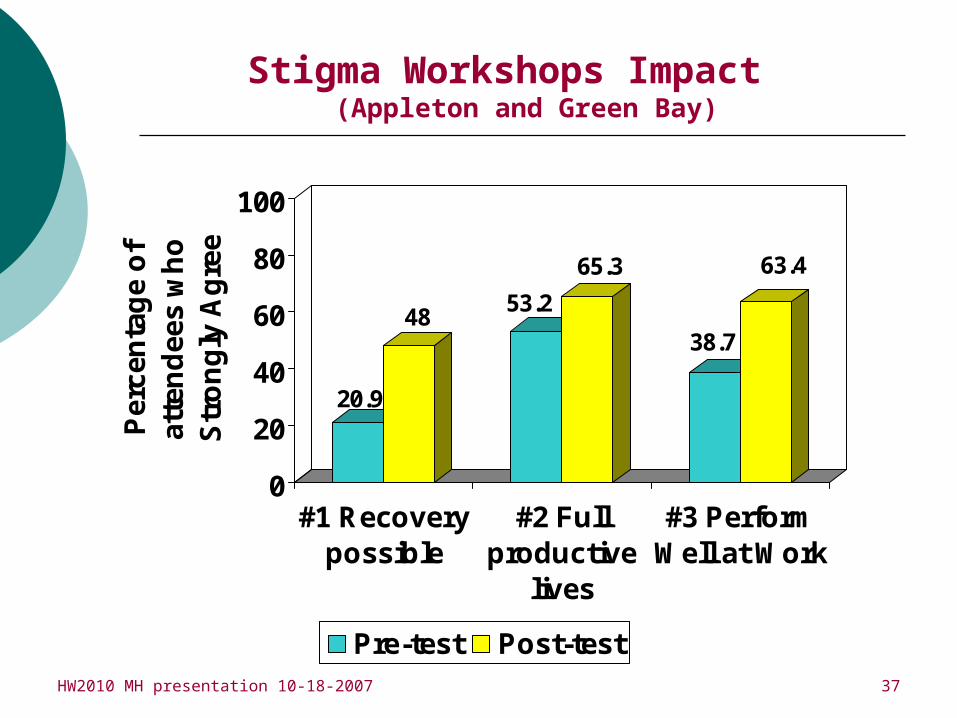
Decreasing Stigma:Wisconsin United for Mental Health
WI United for Mental Health with a mission to advocate for the elimination of stigma associated with mental illness and public education about the barriers to recovery and treatment.
Business leaders, human service workers, educators, media, and others were invited to mental health stigma awareness workshops.
Surveys conducted before stigma awareness session, post-session, and 3-month follow-up survey.
HW2010 MH presentation 10-18-2007 37
Stigma Workshops Impact (Appleton and Green Bay)
20.9
4853.2
65.3
38.7
63.4
0
20
40
60
80
100
Per
cen
tag
e o
f at
ten
dee
s w
ho
S
tro
ng
ly A
gre
e
#1 Recoverypossible
#2 Fullproductive
lives
#3 PerformWell at Work
Pre-test Post-test
HW2010 MH presentation 10-18-2007 38
o By 2010, 80 percent of State-administered employee group health plans, Medicaid-funded programs, BadgerCare, and SSI managed care will, by contract, incorporate questions for mental health problems into their screening and referral processes.
Status: Variable and slow.Notes: Focus to date has been on managed care
programs.
HW2010 Mental Health Objective:Increase Screening and Referral
HW2010 MH presentation 10-18-2007 39
o Promoting Mental Health Awareness Month activities and Depression screening days.
o Mental Health America-Wisconsin effortso Held summits in 2005 & 2006 on screening in conjunction with
Primary Care Physicians. Another planned for Nov. 2007.o Wisconsin Medical Journal publication on MH
Expanded use of Problem Oriented Screening Instrument for Teenagers (POSIT) to identify children in the Juvenile Justice system with MH/SA needs to 29 counties.
Identifying best practice tools and promoting the screening and treatment of MH/SA issues for consumers receiving Medicaid fee-for-service and Badger Care HMO services.
Badger Care Plus will be screening pregnant women for MH, SA, PTSD, and tobacco use problems.
Pilots in 10 counties to screen for MH/SA needs for children in the child welfare system.
Efforts to Increase MH Screening and Referral
(Coordination of State and Local Partnerships)
HW2010 MH presentation 10-18-2007 40
Coordination of State and Local Partnerships
Joint statement between Mental Health, Substance Abuse, and Public Health:
“We aspire to become a society that optimizes the mental, physical, social, emotional, and spiritual health of all persons. Prevention, screening, intervention, and treatment will be person and family-centered, accessible, and appropriate to the culture and language of the individuals. These principles build resiliency, facilitate recovery, and eliminate stigma.”
HW2010 MH presentation 10-18-2007 41
Key Partners County Human Services Public Health Health Care Providers and Systems DHFS, Pathways to Independence UW-Universities and Technical College System Wisconsin United for Mental Health Lt. Governor Barbara Lawton DPI and Local School Systems Department of Workforce Development: Disability Program
Navigators and Bureau of Migrant, Refugee, and Labor Services Psychologists Substance Use Providers Physicians and Provider Associations Wisconsin Council on Mental Health Consumer, Family & Advocacy Organizations Faith-Based Communities Suicide Prevention Intervention (SPI), Crisis Response Network Tribal Organizations incl. Great Lakes Inter-Tribal Council, Inc. SAMHSA, ADS Center, and partner organizations
HW2010 MH presentation 10-18-2007 42
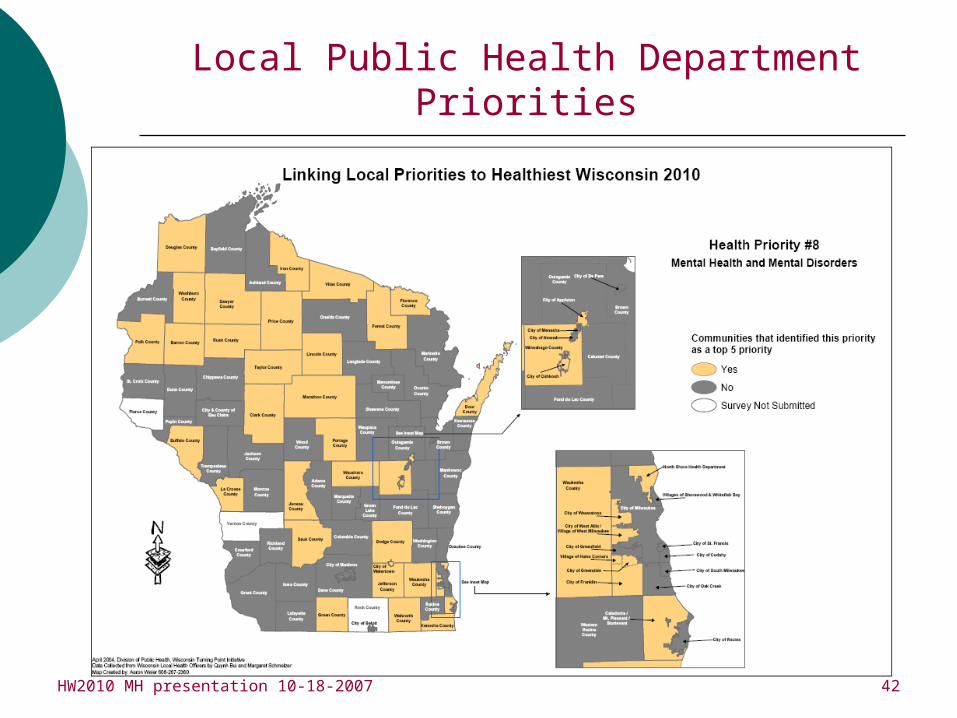
Local Public Health Department Priorities

HW2010 MH presentation 10-18-2007 43
Local Public Health Department Priorities
HW2010 MH presentation 10-18-2007 44
Primary Issues in the Mental Health System
Access to services Financial, geographical, cultural
Need for integrated services Work force training/education
Use of best available practices Lack of identification of MH needs
across all health fields

HW2010 MH presentation 10-18-2007 45
Mental Health Policy/ Programmatic Recommendations
Enact insurance parity to combat financial barriers to access to MH care Lack of parity not only prevents initial access to
MH care, but also prevents access to adequate amounts of MH care.
Wisconsin is one of 9 states without some form of mental health and substance abuse (MH/SA) health insurance parity legislation.
41 other states have some form of legislation providing MH/SA coverage that is more comparable to coverage for other medical conditions.
Continued growth of Medicaid managed care programs.
(Equitable, Adequate, and Stable Financing)

HW2010 MH presentation 10-18-2007 46
Mental Health Policy/ Programmatic Recommendations
Implement screening for depression, substance abuse, and trauma in primary care MH/SA, suicide risk screening and early
identification integrated into primary health care systems (Include protocols and tracking of screening, outcomes, and client data).
Provide models of successful MH referral and access systems within primary care to mentor and provide consultation to others.
Offer MH protocols and models for referral, so that physicians/staff have services (place) to send patients with MH/SA needs.
HW2010 MH presentation 10-18-2007 47
Mental Health Policy/ Programmatic Recommendations
Reduce health disparities for MH consumers in both primary and MH care. Promote integrated and co-located MH
services within primary care clinics. Provide training/education for MH/primary
care providers on delivery of culturally competent MH services.
Increase access to MH services for pregnant and postpartum women
Incorporate/monitor data from the Pregnancy Risk Assessment Monitoring System (PRAMS) a CDC grant, incorporating depression into a self-report survey (150 women/per month for 3 and a half years).
Increase depression screening postpartum into health care systems (i.e., Racine-All Saints Hospital, Unity Health Care, and Marshfield Clinic).
(Elimination of Health Disparities)

HW2010 MH presentation 10-18-2007 48
Mental Health Policy/ Programmatic Recommendations
Promote effective MH treatment Only 33% of people with a psychiatric disorder were
treated adequately and only 13% of those who saw general medical practitioners were treated adequately (NCS, 2001-03).
Need to facilitate the dissemination of evidence-based practices on a statewide basis by making implementation materials accessible
Need to increase the availability of training for clinicians and supervisors on the use of specific EBP’s
Need to track statewide EBP efforts and facilitate a “learning collaborative” approach in which counties will learn from each others EBP implementation experiences
Special certification and MA rates would provide incentives for providers to use EBP’s
HW2010 MH presentation 10-18-2007 49
Mental Health Policy/ Programmatic Recommendations
Combat stigma through health care and other professional education Efforts to decrease stigma will impact people
seeking treatment earlier, thus improving MH outcomes for recovery, lessens severity and duration of the disorder; may prevent need for crisis intervention, and/or ER presentation
Education and awareness to MH/MI screening across medical disciplines for early identification of risk factors and referral to treatment services and supports
Professional education about stigma and their own personal biases toward MI and persons who have MI, recovery, and person/family-centered non-stigmatizing treatment and work environments
HW2010 MH presentation 10-18-2007 50
Joyce AllenBureau Director
Bureau of Mental Health and Substance Abuse Services(266-1351; [email protected])
Rebecca CohenPlanner/Analyst
Bureau of Mental Health and Substance Abuse Services(266-2712; [email protected])
Tim ConnorResearcher
University of Wisconsin Population Health Institute(261-6744; [email protected])
Healthiest Wisconsin 2010Status Report to the Public Health Council State Health Plan
Committee