Health Sector Sudan - World Health Organization · Data source: State Ministries of Health, WHO and...
62
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 1 Health Sector Sudan [HeRAMS] Health Resources Availability Mapping System Darfur Region Report Report: Quarter 1 - 2017
Transcript of Health Sector Sudan - World Health Organization · Data source: State Ministries of Health, WHO and...
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 1
Health Sector Sudan
[HeRAMS] Health Resources Availability Mapping System
Darfur Region Report
Report: Quarter 1 - 2017

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 2
HeRAMS (Health Resources Availability Mapping System) is a standardized approach supported by a
software-based platform that aims at strengthening the collection, collation and analysis of information
on the availability of health resources and services in humanitarian context. It aims to address the
needs/gaps expressed by the health sector on coordination and management by providing timely,
relevant, and reliable information.
HeRAMS started in Sudan early 2008 and has been jointly developed by Health Information Service Unit
of WHO Sudan Office and Health Action in WHO-HQ and approved by Ministry of health. Darfur crisis
context was taken as model by using its data to test the system. Since then, HeRAMS has evolved to be
one of the key information management tool that the global health cluster is using to assist the
implementation of the Health Cluster/Sector approach at country level. HeRAMS has been further
implemented in many crises situations such as; Haiti 2009, Pakistan Floods 2010, Syria conflict, etc.
HeRAMS provides a tool for assessing, monitoring, and processing a comprehensive set of available data
collected at health facility level. It covers; exact geographical location of the HF, demographic data on
catchment area, type, functionality, building type, inpatient capacity, managing and supporting partners,
health personnel, access and security, and health services provided at different levels of healthcare.
This report provides a summary of the analysis of the available health resources and services in Darfur
region, which consists of five states and 63 localities; it is considering the key parameters covered by the
system. The report is produced with the data provided mainly by State Ministries of Health and also by
national and international non-governmental organizations working in, and members of the Health
Sector in Darfur region. The list of NGOs is shown in the annex 1.
Further information could be provided upon request.
Dr. Salah Eldin Mubark Elkhalifa
Director, Health Emergency & Epidemic Control
Federal Ministry of Health
Telephone: +249 123 399 997
Email: [email protected]
Dr. Naeema Al Gasseer Dr. Camilo Valderrama
WHO Representative Health Cluster Coordinator
World Health Organization World Health Organization
Khartoum Khartoum
Email: [email protected] Email : [email protected]
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 3
Table of Contents 1. Darfur Region - (All States) ........................................................................................................................ 6
1.1 Primary Health Care System Composition .......................................................................................... 6
1.2 Health Partners in Darfur .................................................................................................................... 7
1.3 Health Personnel Gap Analysis ........................................................................................................... 8
1.3.1 Rural Hospitals ...................................................................................................................... 8
1.3.2 Primary Health Care Centre .................................................................................................. 9
1.3.3 Basic Health Unit ................................................................................................................. 10
1.4 Health Services in Darfur .................................................................................................................. 11
1.4.1 Provision of Minimum Basic Health Package (MBHP) ........................................................ 11
1.4.2 Provision of Basic Essential Obstetric Care (BEOC): ............................................................ 12
1.4.3 Provision of Maternal & Newborn service at PHCC Level ................................................... 13
1.4.4 Provision of health services at community level ................................................................ 13
1.4.5 Provision of services at primary health care level .............................................................. 14
2. North Darfur ............................................................................................................................................ 16
2.1 Distribution of Primary Health Care facilities: .................................................................................. 16
2.2 Management of health facilities ....................................................................................................... 17
2.3 Health Partners in North Darfur........................................................................................................ 19
2.3.1 NGO health partners .................................................................................................................. 20
2.4 Health Personnel in North Darfur ..................................................................................................... 21
2.3.1 Health Personnel Gap Analysis .................................................................................................. 23
2.5 EWARS reporting HFs in North Darfur .............................................................................................. 25
2.6 Provision of Minimum Basic Health Package in North Darfur .......................................................... 26
3. South Darfur ............................................................................................................................................ 27
3.1 Distribution of Primary Health Care facilities ................................................................................... 27
3.2 Management of health facilities ....................................................................................................... 28
3.3 Health Partners in South Darfur........................................................................................................ 29
3.3.1 NGO health partners .................................................................................................................. 30
3.4 Health Personnel in South Darfur ..................................................................................................... 31
3.4.1 Health Personnel Gap Analysis in South Darfur ......................................................................... 33
3.5 EWARS reporting HFs in South Darfur .............................................................................................. 35
3.6 Provision of Minimum Basic Health Package in South Darfur .......................................................... 36

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 4
4. East Darfur .............................................................................................................................................. 37
4.1 Distribution of Primary Health Care facilities: .................................................................................. 37
4.2 Management of health facilities ....................................................................................................... 38
4.3 Health Partners in East Darfur .......................................................................................................... 39
4.3.1 NGO health partners .................................................................................................................. 39
4.4 Health Personnel in East Darfur ........................................................................................................ 40
4.4.1 Health Personnel Gap Analysis in East Darfur ........................................................................... 41
4.5 EWARS reporting HFs in East Darfur ................................................................................................. 43
4.6 Provision of Minimum Basic Health package in East Darfur ............................................................. 44
5. West Darfur ............................................................................................................................................. 45
5.1 Distribution of Primary Health Care facilities ................................................................................... 45
5.2 Management of health facilities ....................................................................................................... 46
5.3 Health Partners in West Darfur:........................................................................................................ 47
5.3.1 NGO health partners .................................................................................................................. 48
5.4 Health Personnel in West Darfur ...................................................................................................... 48
5.4.1 Health Personnel Gap Analysis in West Darfur .......................................................................... 49
5.5 EWARS reporting HFs in West Darfur ............................................................................................... 51
5.6 Provision of Minimum Basic Health package in West Darfur ........................................................... 52
6. Central Darfur ......................................................................................................................................... 53
6.1 Distribution of Health facilities ......................................................................................................... 53
6.2 Management of health facilities ....................................................................................................... 54
6.3 Health Partners in Central Darfur ..................................................................................................... 55
6.3.1 NGO health partners .................................................................................................................. 55
6.4 Health Personnel in Central Darfur ................................................................................................... 56
6.4.1 Health Personnel Gap Analysis in Central Darfur .................................................... 58
6.4 EWARS reporting HFs in Central Darfur ............................................................................................ 59
6.5 Provision of Minimum Basic Health package in Central Darfur ........................................................ 60
Annex-: List of Health Partners working in Darfur per State

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 5
Acronyms
BHU Basic Health Unit
CD Central Darfur
CHW Community Health Worker
ED East Darfur
EWARS Early Warning Alert and Response System
Func Functional
HeRAMS Health Resources Availability Mapping System
HF Health Facility
HP Health Partner
MA Medical Assistant
MBHP Minimum basic health package
MO Medical Officer
Mob Clinic Mobile Clinic
MW Midwife
ND North Darfur
Non-func Non functional
Nut. Staff Nutritionist / Nutrition staff
PHCC Primary Health Care Center
PHO Public Health Officer
RH Rural Hospital
SD South Darfur
SMOH State Ministry of Health
VTMW Village Trained Midwife
WD West Darfur
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 6
1. Darfur Region - (All States)
1.1 Primary Health Care System Composition
Primary Health Care System in Darfur states is composed of Rural Hospitals, Primary Health Care
Centers, Basic Health Units and Mobile Clinics. In some states however, there are also State Hospitals
with teaching faculties, these are excluded from this report.
Following decreasing trends in 2015, 2016 witnessed increases in both the total number of HFs (Health
Facilities) and those functional type. In 2016, the number of HFs slightly increased to 1,181. In Q/Q4
2016, the total functional was 813 which increased to 826 in Q1 2017.
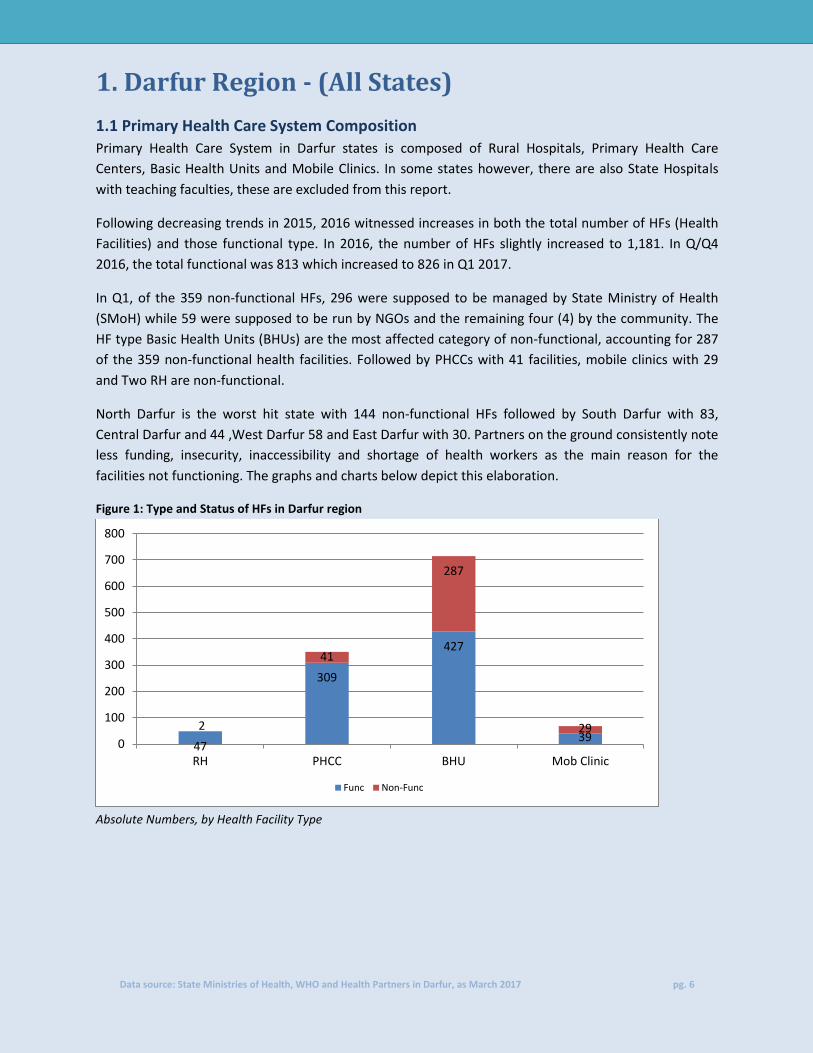
In Q1, of the 359 non-functional HFs, 296 were supposed to be managed by State Ministry of Health
(SMoH) while 59 were supposed to be run by NGOs and the remaining four (4) by the community. The
HF type Basic Health Units (BHUs) are the most affected category of non-functional, accounting for 287
of the 359 non-functional health facilities. Followed by PHCCs with 41 facilities, mobile clinics with 29
and Two RH are non-functional.
North Darfur is the worst hit state with 144 non-functional HFs followed by South Darfur with 83,
Central Darfur and 44 ,West Darfur 58 and East Darfur with 30. Partners on the ground consistently note
less funding, insecurity, inaccessibility and shortage of health workers as the main reason for the
facilities not functioning. The graphs and charts below depict this elaboration.
Figure 1: Type and Status of HFs in Darfur region
Absolute Numbers, by Health Facility Type
47
309
427
39 2
41
287
29 0
100
200
300
400
500
600
700
800
RH PHCC BHU Mob Clinic
Func Non-Func
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 7
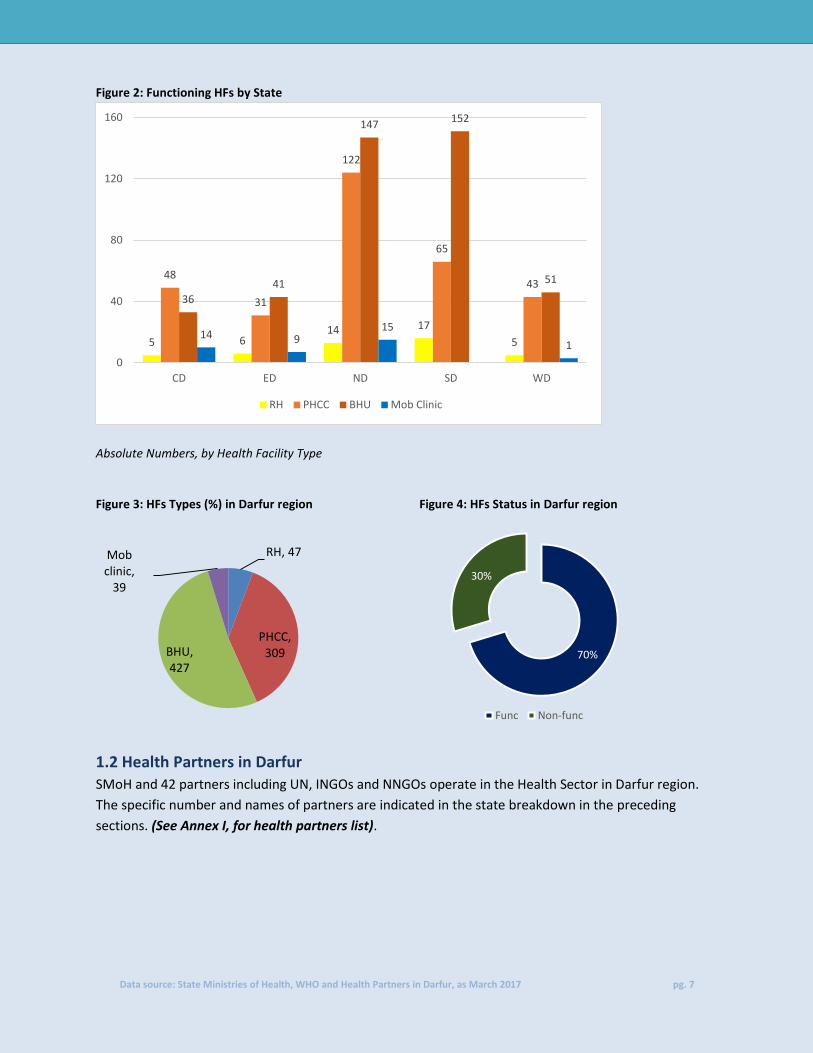
Figure 2: Functioning HFs by State
Absolute Numbers, by Health Facility Type
Figure 3: HFs Types (%) in Darfur region Figure 4: HFs Status in Darfur region
1.2 Health Partners in Darfur SMoH and 42 partners including UN, INGOs and NNGOs operate in the Health Sector in Darfur region.
The specific number and names of partners are indicated in the state breakdown in the preceding
sections. (See Annex I, for health partners list).
RH, 47
PHCC, 309 BHU,
427
Mob clinic,
39
70%
30%
Func Non-func
5 6 14 17
5
48
31
122
65
43
36
41
147 152
51
14 9 15
1
0
40
80
120
160
CD ED ND SD WD
RH PHCC BHU Mob Clinic

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 8
Figure 5: Summary of the health actors and the number of managed functioning HFs by type
1.3 Health Personnel Gap Analysis
Below is a brief analysis of the gaps in health staff availability against the national health standards for different types of health facilities. Detailed analysis follows in each state sections in the document. Based on the HeRAMS data, gaps in health staffing has been analyzed against the local Health System standards set by the Sudan’s Federal Ministry of Health (FMoH).
1.3.1 Rural Hospitals
In Rural hospitals, the minimum standard set is at least one Medical Officer (MO), one Medical Assistant (MA), three Nurses, one Midwife (MW), one Vaccinator, one Nutrition staff (Nut. Staff), one Public Health Office (PHO) and one Laboratory personnel (lab personnel). This is the bare minimum, more is recommended. Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
Information gathered from the field as in the graph below shows that, on average there are more
personnel, apart from PHO than the required standard to run the 47 RHs in Darfur States. The biggest
challenge however is the disparity between RHs located in urban centers and those in the rural areas.
For example, there are more than required MOs in Ed Daein and Zalingi but none in Niteaga, Kerinik , El
Ferdous and Mohjrea RHs. This disparity applies to other core medical staff as well. Details of the
specific facilities are in the states analysis below.
1
144
59
27
231
46
159
346
12
563
6 22 28
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RH PHCC BHU Mob clinic Total
NGO Govt(SMoH and NHI) Community

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 9
Figure 5: Comparison of available personnel and standards in RHs in Darfur region
Data collected indicated that there are only 42 PHOs to run the 47 RHs, which is less than the required
minimum standard of 47. In addition to the disparity based on location, the situation gets dire.
1.3.2 Primary Health Care Centre
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses,
one Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare
minimum, more is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff and Lab. Personnel
The challenge gets more pronounced as the type of facility changes from RH to PHCC. As was with RHs,
disparity of the location of the facility was the biggest challenge. In addition to this, PHCCs have less staff
in key areas. There are fewer Nurses, PHOs and Lab. personnel to run the 309 PHCCs. The standard set
for nurses is 618 but there are only 552 available nurses. Likewise, for PHOs, the standard is 309 but only
86 are available, same with lab personnel, the standard is 309 but only 142 are available.
47 47 141
47 47 47 47 47
78 127
508
42
175
109 129
68
0
100
200
300
400
500
600
700
MO MA Nurse PHO MW Vacc Nut Staff Lab Person
Standard Available

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 10
Figure 6: Comparison of available personnel and standards in PHCCs in Darfur region
1.3.3 Basic Health Unit
The minimum standard set for a BHU is at least one Medical Assistant, one Nurse, one Midwife, one
VTMW, one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
Standard is: MA, Nurse, MW, VTMW, Nutrition staff and Vaccinator.
Further down the pecking order, the challenge gets more pressing as the type of facility changes from RH to PHCC and to BHUs despite the lower requirements. BHUs have difficulty in attracting and maintaining qualified staff because they are under-resource financially and technically.
Data collected from the field shows that 125 of the 427 functioning BHUs are run by community based personnel, most of whom are only trained in basic health care. They often work part time at their homes or business locations.
309
618
309 309 309 309 309
442
552
86
758
369 362
142
0
200
400
600
800
1000
1200
1400
MA Nurse PHO MW Vacc Nut Staff Lab Person
Standard Available
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 11
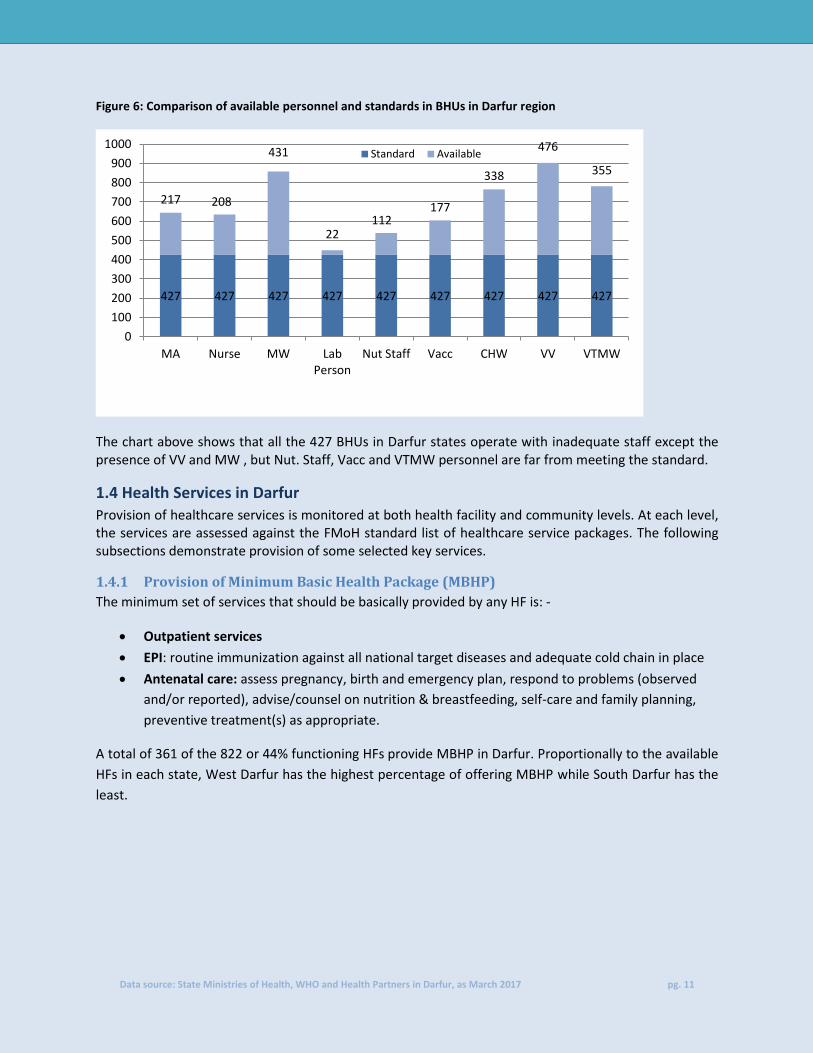
Figure 6: Comparison of available personnel and standards in BHUs in Darfur region
The chart above shows that all the 427 BHUs in Darfur states operate with inadequate staff except the presence of VV and MW , but Nut. Staff, Vacc and VTMW personnel are far from meeting the standard.
1.4 Health Services in Darfur
Provision of healthcare services is monitored at both health facility and community levels. At each level, the services are assessed against the FMoH standard list of healthcare service packages. The following subsections demonstrate provision of some selected key services.
1.4.1 Provision of Minimum Basic Health Package (MBHP)
The minimum set of services that should be basically provided by any HF is: -
Outpatient services
EPI: routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatment(s) as appropriate.
A total of 361 of the 822 or 44% functioning HFs provide MBHP in Darfur. Proportionally to the available
HFs in each state, West Darfur has the highest percentage of offering MBHP while South Darfur has the
least.
427 427 427 427 427 427 427 427 427
217 208
431
22 112
177
338
476
355
0
100
200
300
400
500
600
700
800
900
1000
MA Nurse MW LabPerson
Nut Staff Vacc CHW VV VTMW
Standard Available

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 12
Figure 7: Darfur states showing number and percentage of HFs offering MBHP
* Percentage of HFs providing the MBHP out of the total functioning HFs
1.4.2 Provision of Basic Essential Obstetric Care (BEOC):
Parenteral antibiotics + oxytocic/anticonvulsant drugs + manual removal of placenta + removal of
retained products with Manual Vacuum Aspiration (MVA) + assisted vaginal delivery 24hours a day and
7 days a week.
Figure 7: Darfur states showing number and percentage of HFs offering BEOC
* Percentage of HFs providing the BEOC out of the total functioning HFs
Ministry of Health regulation states that any health facility should provide the full elements of BEOC
services otherwise to be reported zero if only partially provided.
Overall in Darfur states the provision of BEOC coverage is at 26.5%. West Darfur, has the least coverage
and East Darfur, with the most coverage
126
65
27 70
73
172
38
60 164
27
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ND CD ED SD WD
With Without
75 25 34
71
13
223 78 53
163
87
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ND CD ED SD WD
With Without

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 13
1.4.3 Provision of Maternal & Newborn service at PHCC Level
This service includes antenatal care, skilled care during childbirth, basic emergency obstetric care and
post-partum care, a detailed composition is in the table below.
Figure 8: Darfur states showing percentage of PHCCs providing maternal and newborn services
* Percentage of HFs providing the maternal and newborn services out of the total functioning PHCCs
PHC
Level
P62 Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatments) as appropriate P63 Skilled care during childbirth for clean and safe normal delivery
P65 Basic emergency obstetric care (BEmOC): parenteral antibiotics + oxytocic/ anticonvulsant drugs
+ manual removal of placenta + removal of retained products with manual vacuum aspiration
(MVA) + assisted vaginal delivery 24 hours a day and 7 days a week. P66 Post-partum care: examination of mother and newborn (up to 6 weeks), respond to observed
signs, support breast feeding, promote family planning
Basic emergency obstetrics care is the maternal and newborn service less provided across all PHCCs in
Darfur states but specifically in Central Darfur, West Darfur and North Darfur. Conversely, antenatal
care is the service provided in most PHCCs and evenly distributed across the states.
1.4.4 Provision of health services at community level
Provision of health service at community level includes services under the broader category of collection
of vital statistics, child health, nutrition, communicable diseases and maternal and new born as shown in
the table below.
In general, the lowest coverage for the services provided at community care level is reported from North
Darfur state, where the interventions are provided in less than 50% of the HFs. Conversely, West Darfur
has the best coverage; all the community level services are provided in more than 64% of the HFs in the
state.
92%
71%
84% 85%
95%
64% 61% 58%
81%
88%
35%
61%
25%
60%
12%
69%
42%
70%
85%
74%
0%
25%
50%
75%
100%
CD ED ND SD WD
P62 P63 P65 P66
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 14
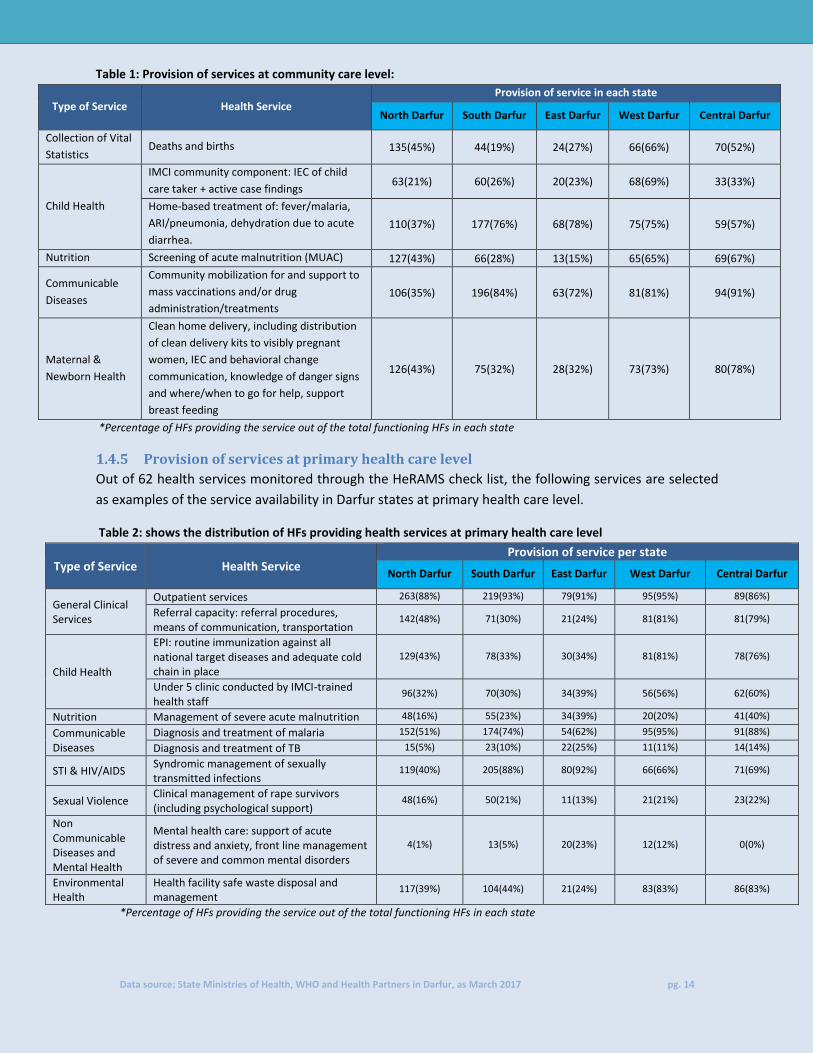
Table 1: Provision of services at community care level:
Type of Service Health Service Provision of service in each state
North Darfur South Darfur East Darfur West Darfur Central Darfur
Collection of Vital
Statistics Deaths and births 135(45%) 44(19%) 24(27%) 66(66%) 70(52%)
Child Health
IMCI community component: IEC of child
care taker + active case findings 63(21%) 60(26%) 20(23%) 68(69%) 33(33%)
Home-based treatment of: fever/malaria,
ARI/pneumonia, dehydration due to acute
diarrhea.
110(37%) 177(76%) 68(78%) 75(75%) 59(57%)
Nutrition Screening of acute malnutrition (MUAC) 127(43%) 66(28%) 13(15%) 65(65%) 69(67%)
Communicable
Diseases
Community mobilization for and support to
mass vaccinations and/or drug
administration/treatments
106(35%) 196(84%) 63(72%) 81(81%) 94(91%)
Maternal &
Newborn Health
Clean home delivery, including distribution
of clean delivery kits to visibly pregnant
women, IEC and behavioral change
communication, knowledge of danger signs
and where/when to go for help, support
breast feeding
126(43%) 75(32%) 28(32%) 73(73%) 80(78%)
*Percentage of HFs providing the service out of the total functioning HFs in each state
1.4.5 Provision of services at primary health care level
Out of 62 health services monitored through the HeRAMS check list, the following services are selected
as examples of the service availability in Darfur states at primary health care level.
Table 2: shows the distribution of HFs providing health services at primary health care level
Type of Service Health Service Provision of service per state
North Darfur South Darfur East Darfur West Darfur Central Darfur
General Clinical Services
Outpatient services 263(88%) 219(93%) 79(91%) 95(95%) 89(86%)
Referral capacity: referral procedures, means of communication, transportation
142(48%) 71(30%) 21(24%) 81(81%) 81(79%)
Child Health
EPI: routine immunization against all national target diseases and adequate cold chain in place
129(43%) 78(33%) 30(34%) 81(81%) 78(76%)
Under 5 clinic conducted by IMCI-trained health staff
96(32%) 70(30%) 34(39%) 56(56%) 62(60%)
Nutrition Management of severe acute malnutrition 48(16%) 55(23%) 34(39%) 20(20%) 41(40%)
Communicable Diseases
Diagnosis and treatment of malaria 152(51%) 174(74%) 54(62%) 95(95%) 91(88%)
Diagnosis and treatment of TB 15(5%) 23(10%) 22(25%) 11(11%) 14(14%)
STI & HIV/AIDS Syndromic management of sexually transmitted infections
119(40%) 205(88%) 80(92%) 66(66%) 71(69%)
Sexual Violence Clinical management of rape survivors (including psychological support)
48(16%) 50(21%) 11(13%) 21(21%) 23(22%)
Non Communicable Diseases and Mental Health
Mental health care: support of acute distress and anxiety, front line management of severe and common mental disorders
4(1%) 13(5%) 20(23%) 12(12%) 0(0%)
Environmental Health
Health facility safe waste disposal and management
117(39%) 104(44%) 21(24%) 83(83%) 86(83%)
*Percentage of HFs providing the service out of the total functioning HFs in each state

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 15
The table above depicts the distribution of HFs providing health service at primary health care level.
General Clinical services which includes outpatient services and referral services are provided in most of
the HFs in Darfur. Up to 93% of HFs in South Darfur state provides this service, making it the best
performing state. The least performing state in providing this service is Central Darfur with 86%.
Conversely, mental health care service is provided in fewest HFs in the region. All the HFs in Central
Darfur doesn’t provide this service. Only four HFs (1%) in North Darfur does, while 13(5%) in South
Darfur and 20 (23%) in East Darfur.

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 16
2. North Darfur
2.1 Distribution of Primary Health Care facilities
Health Facilities are classified into different standard categories based on the provision of services, staffing and population coverage; they are
Rural Hospitals (RH), Primary Health Care Centers (PHCC), Basic Health Units (BHU), and Mobile Clinics. The following table provides the
distribution of the existing health facilities (static and mobile); showing the number and percentage of the functional facilities out of total. See
acronyms for the initials used.
Table 3: Distribution of HFs in North Darfur by locality and facility type
State Locality
RH PHCC BHU Mob Clinic Total
Func Total % Func Func Total % Func Func Total % Func Func Total % Func Func Total % Func
No
rth
Dar
fur
Ailliet 1 1 100% 7 7 100% 21 21 100% 0 0 0% 29 29 100%
Alwaha 1 1 100% 4 5 80% 7 8 88% 2 2 100% 14 16 88%
Dar el Salam 1 1 100% 5 7 71% 4 8 50% 0 0 0% 10 16 63%
El Fasher 0 0 0% 42 48 87% 23 33 70% 5 7 71% 70 88 80%
El Kuma 0 0 0% 4 4 100% 3 7 43% 0 0 0% 7 11 64%
El Malha 1 1 100% 9 9 100% 6 11 54% 0 0 0% 16 21 76%
El Taweisha 2 2 100% 7 8 88% 7 11 64% 0 0 0% 16 21 76%
El Tina 1 1 100% 0 0 0% 1 2 50% 0 0 0% 2 3 67%
ElSeraif 1 1 100% 1 1 100% 2 12 17% 0 0 0% 4 14 28%
Kalemando 0 1 0% 2 3 67% 14 14 100% 0 0 0% 16 18 89%
Kebkabiya 1 1 100% 7 9 78% 8 28 28% 1 1 100% 17 39 43%
Kornoi 1 1 100% 0 1 0% 2 13 15% 0 0 0% 3 15 20%
Kutum 1 1 100% 14 14 100% 8 24 33% 0 0 0% 23 39 59%
Mellit 1 1 100% 9 9 100% 14 14 100% 6 6 100% 30 30 100%
Saraf Omra 1 1 100% 1 1 100% 10 0% 0 0 0% 2 12 17%
Tawilla 0 0 0% 3 6 50% 7 24 29% 0 7 0% 10 37 27%
Um Buru 0 0 0% 1 2 50% 5 6 83% 1 1 100% 7 9 78%
Umm Keddada 1 1 100% 6 6 100% 15 18 83% 0 0 0% 22 25 88%
Total 14 15 93% 122 140 89% 147 264 56% 15 24 63% 298 443 67%

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 17
Following an increase from 440 to 443 between Q4 2016 and Q1/Q2 2017, the number functioning HFs slightly decreased from 299 (68% of total
Q4 – 2016 facilities) to 298 (67% of total Q1 – 2017 facilities) . These changes are noted as below: -
The increases were noted in Kornoi locality, after Kornoi RH began operation.
Furthermore, in El Malha locality, One BHU and One PHC began operation thereby increasing the number of facilities in the locality to 16.
A further increase due to one BHU which began operation in Kabkabiya locality , and decreased of One PHCC and One BHU in El Fasher locality ,
also One BHU in El Seraif Locality , One PHCC in Kalemando and Um Baro localities were decreased during Q1 2017 .
The rest of the localities didn’t experience any change in health facilities status.
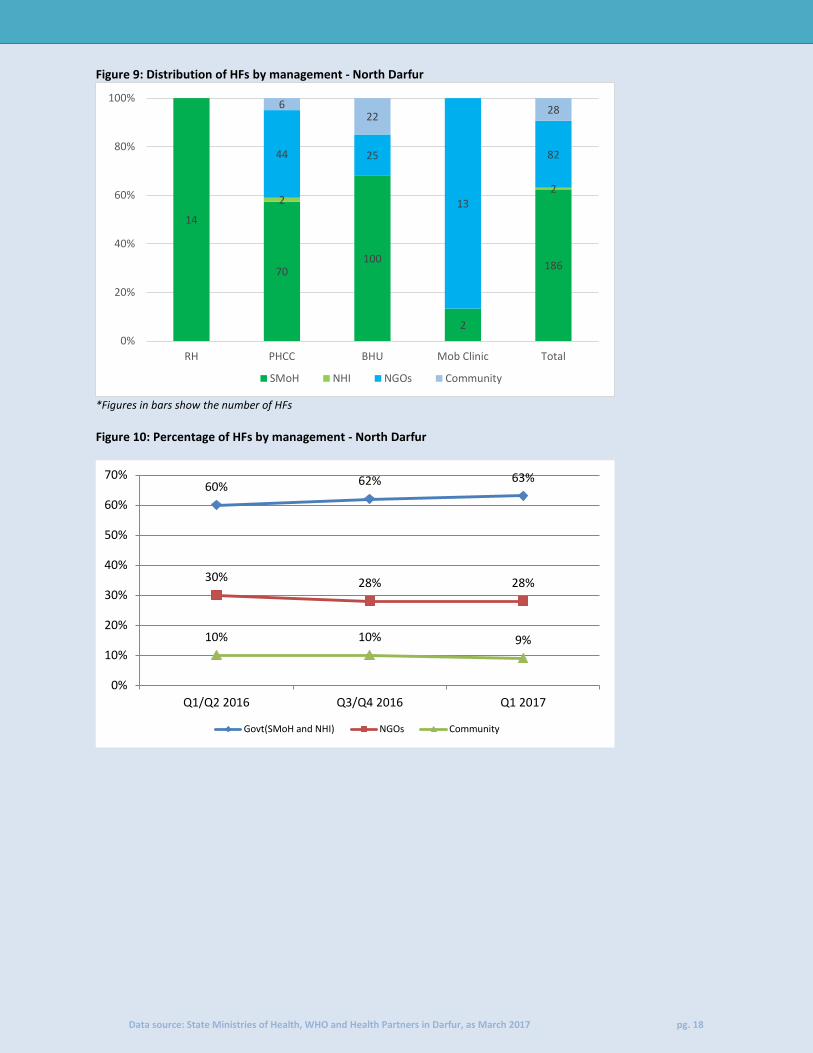
2.2 Management of health facilities
Management of health facilities means the primary focal entity who takes charge of admission and providing services to the patients. The below
graph shows the respective entities that manage the health facilities.
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 18
Figure 9: Distribution of HFs by management - North Darfur
*Figures in bars show the number of HFs Figure 10: Percentage of HFs by management - North Darfur
14
70 100
2
186
2 2
44 25
13
82
6 22
28
0%
20%
40%
60%
80%
100%
RH PHCC BHU Mob Clinic Total
SMoH NHI NGOs Community
60% 62% 63%
30% 28% 28%
10% 10% 9%
0%
10%
20%
30%
40%
50%
60%
70%
Q1/Q2 2016 Q3/Q4 2016 Q1 2017
Govt(SMoH and NHI) NGOs Community
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 19
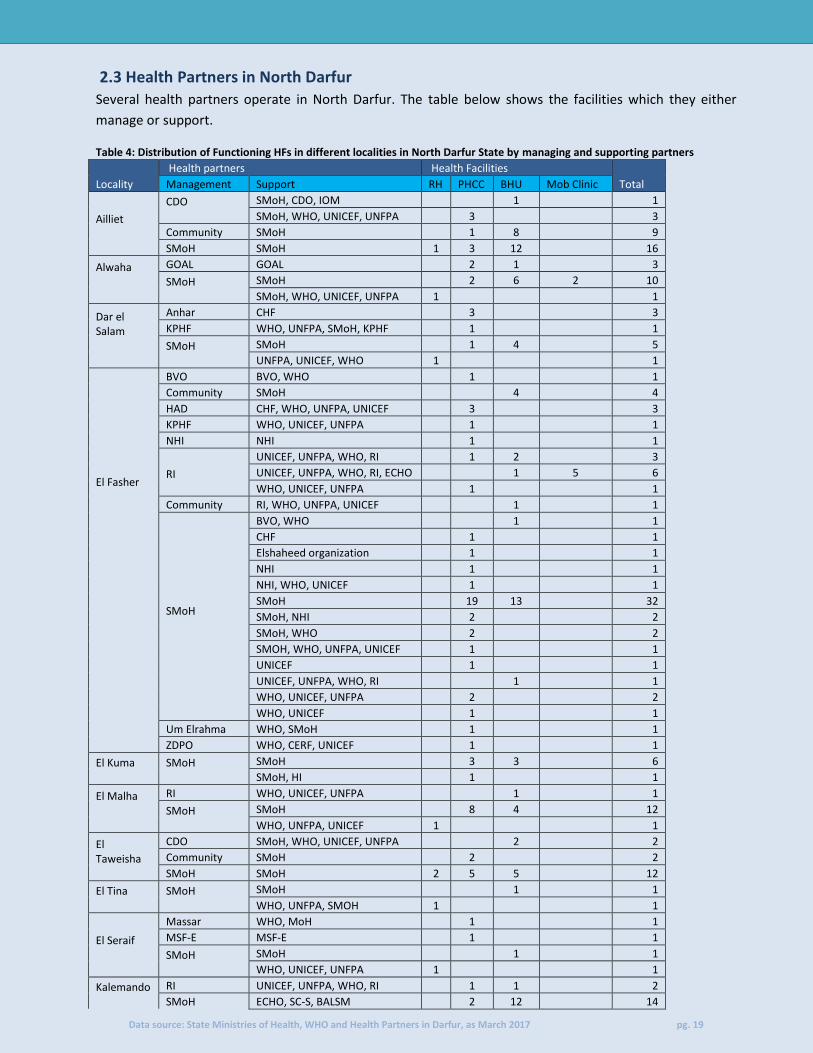
2.3 Health Partners in North Darfur
Several health partners operate in North Darfur. The table below shows the facilities which they either
manage or support.
Table 4: Distribution of Functioning HFs in different localities in North Darfur State by managing and supporting partners
Locality
Health partners Health Facilities Total Management Support RH PHCC BHU Mob Clinic
Ailliet
CDO
SMoH, CDO, IOM
1
1
SMoH, WHO, UNICEF, UNFPA
3
3
Community SMoH
1 8
9
SMoH SMoH 1 3 12
16
Alwaha
GOAL GOAL
2 1
3
SMoH
SMoH
2 6 2 10
SMoH, WHO, UNICEF, UNFPA 1
1
Dar el Salam
Anhar CHF
3
3
KPHF WHO, UNFPA, SMoH, KPHF
1
1
SMoH
SMoH
1 4
5
UNFPA, UNICEF, WHO 1
1
El Fasher
BVO BVO, WHO
1
1
Community SMoH
4
4
HAD CHF, WHO, UNFPA, UNICEF
3
3
KPHF WHO, UNICEF, UNFPA
1
1
NHI NHI
1
1
RI
UNICEF, UNFPA, WHO, RI
1 2
3
UNICEF, UNFPA, WHO, RI, ECHO
1 5 6
WHO, UNICEF, UNFPA
1
1
Community RI, WHO, UNFPA, UNICEF
1
1
SMoH
BVO, WHO
1
1
CHF
1
1
Elshaheed organization
1
1
NHI
1
1
NHI, WHO, UNICEF
1
1
SMoH
19 13
32
SMoH, NHI
2
2
SMoH, WHO
2
2
SMOH, WHO, UNFPA, UNICEF
1
1
UNICEF
1
1
UNICEF, UNFPA, WHO, RI
1
1
WHO, UNICEF, UNFPA
2
2
WHO, UNICEF
1
1
Um Elrahma WHO, SMoH
1
1
ZDPO WHO, CERF, UNICEF
1
1
El Kuma
SMoH
SMoH
3 3
6
SMoH, HI
1
1
El Malha
RI WHO, UNICEF, UNFPA
1
1
SMoH
SMoH
8 4
12
WHO, UNFPA, UNICEF 1
1
El Taweisha
CDO SMoH, WHO, UNICEF, UNFPA
2
2
Community SMoH
2
2
SMoH SMoH 2 5 5
12
El Tina
SMoH
SMoH
1
1
WHO, UNFPA, SMOH 1
1
El Seraif
Massar WHO, MoH
1
1
MSF-E MSF-E
1
1
SMoH
SMoH
1
1
WHO, UNICEF, UNFPA 1
1
Kalemando
RI UNICEF, UNFPA, WHO, RI
1 1
2
SMoH ECHO, SC-S, BALSM
2 12
14
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 20
SMoH
1
1
Kebkabiya
Anhar
UNICEF
1
1
WHO
1
1 2
Massar WHO, MoH
2
2
MSF-E MSF-E
1
1
NHI NHI
1
1
SMoH
SMoH
4
4
UNICEF, UNFPA, WHO
2
2
WHO, UNICEF, UNFPA 1
1
ZDPO UNICEF, UNFPA, WHO
2
2
Kornoi SMoH SMoH 1
2
3
Kutum
Ayadi Elrahma WHO
1
1
GOAL GOAL
10 3
13
SMoH
SMoH
1 4
5
SMoH, WHO, UNICEF
1
1
UNICEF, UNFPA
1
1
UNICEF, UNFPA, WHO
1
1
WHO, UNICEF, UNFPA 1
1
Mellit
Community SMoH
1 6
7
RI
UNICEF, UNFPA, WHO, RI
1
1
UNICEF, UNFPA, WHO, RI, OFDA
3 3
SMoH
SMoH
3 3
6
UNICEF, WHO
1
1
WHO, UNICEF, UNFPA 1
1
SRCS ECHO, UNICEF, WFP
3 5 3 11
Saraf Omra
SMoH
SMoH
1
1
WHO, UNICEF, UNFPA 1
1
Tawilla
Community SMoH
1
1
MSF-E MSF-E
1
1
SAEKAR WHO, UNICEF, SAKAR
1
1
SMoH
SMoH
5
5
WHO, SMoH
1
1
WHO, UNICEF
1
1
Um Buru
Anhar WHO
1 1
SMoH
SMoH
1 3
4
WHO
2
2
Umm Keddada
Community SMoH
2 3
5
RI UNICEF, UNFPA, WHO, RI
1
1
SMoH SMoH 1 3 12
16
Total 14 122 147 15 298
In addition to SMoH and the community, 29 health partners operate in North Darfur. Twelve of whom are
based in El Fasher locality, followed by El Seraif locality with eight. Other localities have between 1 and 8 as
shown in the table above.
Ayadi Elrahma, Um Elrahma, Anhar, SAEKER, CDO, BVO and Elshaheed organization, Al Massar, HAD, KPHP
and Zulfa (ZDPO) are NNGOs in North Darfur
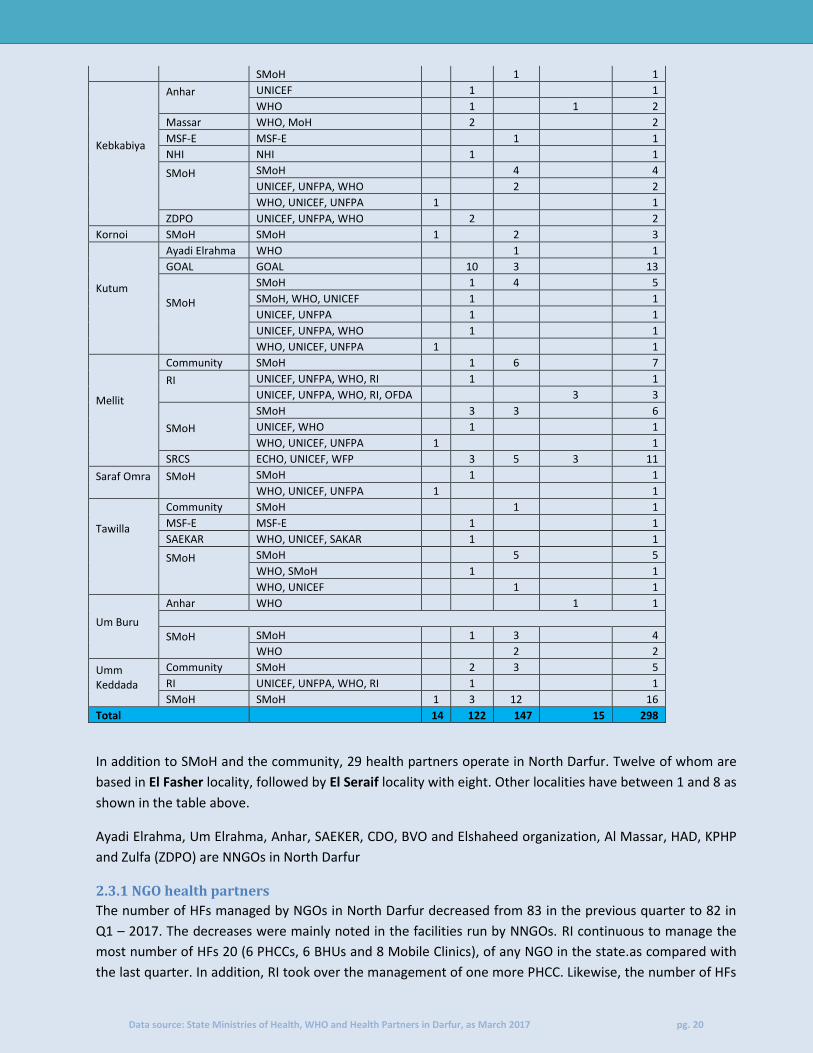
2.3.1 NGO health partners
The number of HFs managed by NGOs in North Darfur decreased from 83 in the previous quarter to 82 in
Q1 – 2017. The decreases were mainly noted in the facilities run by NNGOs. RI continuous to manage the
most number of HFs 20 (6 PHCCs, 6 BHUs and 8 Mobile Clinics), of any NGO in the state.as compared with
the last quarter. In addition, RI took over the management of one more PHCC. Likewise, the number of HFs

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 21
managed by GOAL 16 same as in previous quarter (12 PHCCs and 4 BHUs) currently, the second highest of
any NGO in the state.
The number of HFs managed by NNGOs still same as previous quarter in the state, Anhar managed seven
HFs currently , BVO managed one. In addition, the number of HFs managed by HAD dropped from Four in
the previous quarter to three currently. Likewise the number of HFs managed by Al Massar same as
previous Quarter , no change .
Figure 11: Health partners managing HFs North Darfur and facility types
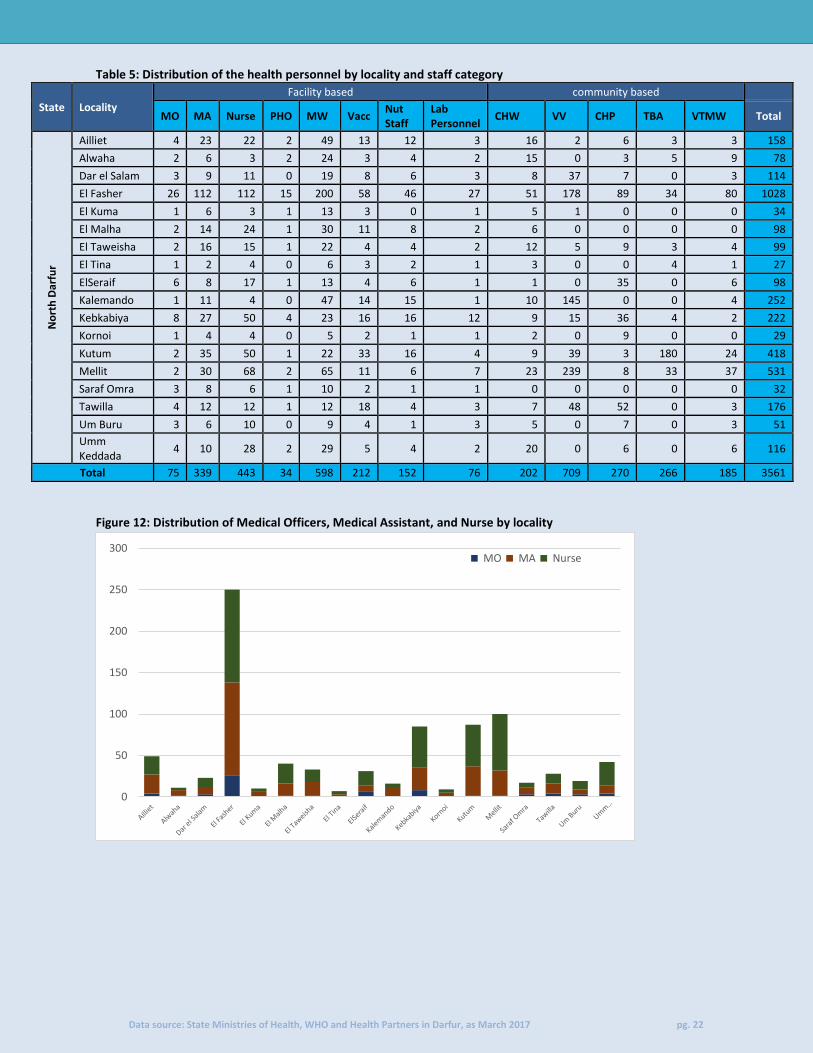
2.4 Health Personnel in North Darfur
Health personnel are categorized as HF based staff (health staff working at the HF) and community based
staff (the community staff working in the community in the catchment area of the HF (i.e. village/camp)).
As with the decreased of HFs in North Darfur, the total number of medical personnel also further decreased
from 3,717 in Q4 - 2016 to 3,561 currently. Of these, 1,929 (54%) are facility based while 1,632 (46%) are
community based.
This decrease however is more on the number of community based staff compared to the number of
facility based staff members. For example, the number of VVs in El Fashier decreased from 178 personnel in
the previous quarter to 163 currently.
Despite a decrease from 1,077 in the previous quarter to 1,028 currently, Elfasher locality still has the most
number of medical personnel in the state. Meanwhile, with 27 medical personnel, El Tina locality has the
least number of medical personnel.
1 3
22
4 1
3 5
2 5
2
8
3 5
1
3
6
12
3 1
3 2
1
6
1 1
3
1 1 0
5
10
15
20
25BHU Mob_clinic PHCC
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 22
Table 5: Distribution of the health personnel by locality and staff category
State Locality
Facility based community based
MO MA Nurse PHO MW Vacc Nut Staff
Lab Personnel
CHW VV CHP TBA VTMW Total
No
rth
Dar
fur
Ailliet 4 23 22 2 49 13 12 3 16 2 6 3 3 158
Alwaha 2 6 3 2 24 3 4 2 15 0 3 5 9 78
Dar el Salam 3 9 11 0 19 8 6 3 8 37 7 0 3 114
El Fasher 26 112 112 15 200 58 46 27 51 178 89 34 80 1028
El Kuma 1 6 3 1 13 3 0 1 5 1 0 0 0 34
El Malha 2 14 24 1 30 11 8 2 6 0 0 0 0 98
El Taweisha 2 16 15 1 22 4 4 2 12 5 9 3 4 99
El Tina 1 2 4 0 6 3 2 1 3 0 0 4 1 27
ElSeraif 6 8 17 1 13 4 6 1 1 0 35 0 6 98
Kalemando 1 11 4 0 47 14 15 1 10 145 0 0 4 252
Kebkabiya 8 27 50 4 23 16 16 12 9 15 36 4 2 222
Kornoi 1 4 4 0 5 2 1 1 2 0 9 0 0 29
Kutum 2 35 50 1 22 33 16 4 9 39 3 180 24 418
Mellit 2 30 68 2 65 11 6 7 23 239 8 33 37 531
Saraf Omra 3 8 6 1 10 2 1 1 0 0 0 0 0 32
Tawilla 4 12 12 1 12 18 4 3 7 48 52 0 3 176
Um Buru 3 6 10 0 9 4 1 3 5 0 7 0 3 51
Umm Keddada
4 10 28 2 29 5 4 2 20 0 6 0 6 116
Total 75 339 443 34 598 212 152 76 202 709 270 266 185 3561
Figure 12: Distribution of Medical Officers, Medical Assistant, and Nurse by locality
0
50
100
150
200
250
300 MO MA Nurse

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 23
Figure 13: Distribution of Midwife, Village Trained Midwife, and Traditional Birth Attendant by locality
2.3.1 Health Personnel Gap Analysis
Below is the analysis of the gaps in health staff availability against the national staff standards for RHs, PHCC and BHUs. There are no standards for mobile clinics; this will not be analyzed in this section. Based on the HeRAMS data, gaps in health staff has been analyzed against the local Health System standards at RH, PHCC and BHU levels. 2.4.1.1 Rural Hospitals
In Rural hospitals, the minimum standard set is at least one Medical Officer, one Medical Assistant, three Nurses, one Midwife, one Vaccinator, one Nutrition staff, one Public Health Office and one Laboratory personnel. This is the bare minimum, more is recommended. Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
According to the latest information collected from the field, Kabkabeya, Kutum Hospital, Saraf Umra and
Umm Keddada RHs are the only facilities which fully meet the required standard set by MoH. As previously
noted in the last quarter report, Um Sayalla meet all requirement but have only one nurse as opposed to
the three according to the standard.
The most notable specialist across all is the absence of PHOs and Vaccinators. The below bullets show the
facilities with missing key personnel according to the set standards.
Gabir RH lacks a nurse and Um Sayalla lack two nurses
PHOs are absent in Dar Salam, El Lait, Gabir, Malha , Krnoi and Tina RHs.
Vaccinators Gap in El Lait, Elserif, Eltwisha and Mallit RHs.
Lab. Personnel in absent in Elserif RH.
0
50
100
150
200
250
300
350
MW TBA VTMW
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 24
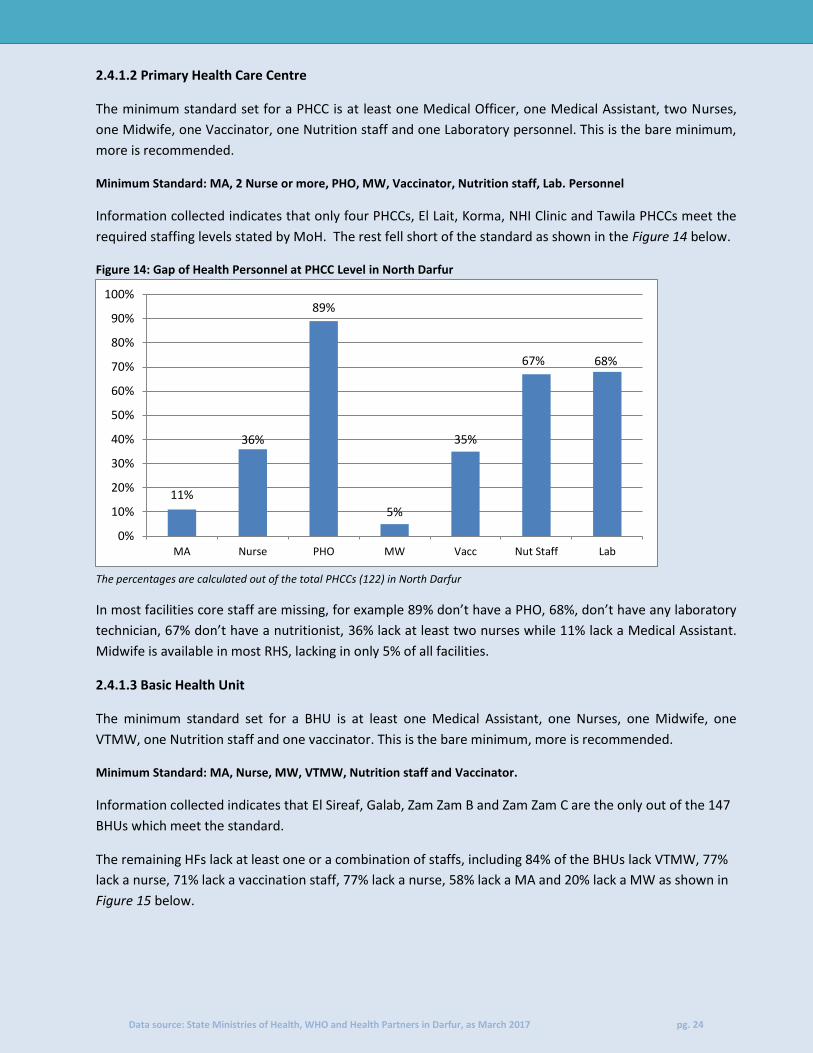
2.4.1.2 Primary Health Care Centre
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses,
one Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare minimum,
more is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff, Lab. Personnel
Information collected indicates that only four PHCCs, El Lait, Korma, NHI Clinic and Tawila PHCCs meet the
required staffing levels stated by MoH. The rest fell short of the standard as shown in the Figure 14 below.
Figure 14: Gap of Health Personnel at PHCC Level in North Darfur
The percentages are calculated out of the total PHCCs (122) in North Darfur
In most facilities core staff are missing, for example 89% don’t have a PHO, 68%, don’t have any laboratory
technician, 67% don’t have a nutritionist, 36% lack at least two nurses while 11% lack a Medical Assistant.
Midwife is available in most RHS, lacking in only 5% of all facilities.
2.4.1.3 Basic Health Unit
The minimum standard set for a BHU is at least one Medical Assistant, one Nurses, one Midwife, one
VTMW, one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
Minimum Standard: MA, Nurse, MW, VTMW, Nutrition staff and Vaccinator.
Information collected indicates that El Sireaf, Galab, Zam Zam B and Zam Zam C are the only out of the 147
BHUs which meet the standard.
The remaining HFs lack at least one or a combination of staffs, including 84% of the BHUs lack VTMW, 77%
lack a nurse, 71% lack a vaccination staff, 77% lack a nurse, 58% lack a MA and 20% lack a MW as shown in
Figure 15 below.
11%
36%
89%
5%
35%
67% 68%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MA Nurse PHO MW Vacc Nut Staff Lab

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 25
Figure 15: Gap of Health Personnel at BHU Level in North Darfur
The percentages are calculated out of the total BHUs (147) in North Darfur
2.5 EWARS reporting HFs in North Darfur EWARS is an essential service for detection of unusual diseases and outbreaks of communicable diseases. In Darfur however, only a few facilities are designated sites due to the existence of the equipment and necessary training for the EWARS staff. The table below shows summary of the number of functioning HFs designated under EWARS
Table 6: Showing localities with designated EWARS HFs
State Locality EWARS Designated Site Total HFs in the locality % EWARS in Locality
No
rth
Dar
fur
Ailliet 3 29 10%
Alwaha 3 14 21%
Dar el Salam 5 10 50%
El Fasher 12 70 17%
El Kuma 0 7 0%
El Malha 0 16 0%
El Taweisha 2 16 13%
El Tina 0 2 0%
ElSeraif 2 4 50%
Kalemando 1 16 6%
Kebkabiya 6 17 35%
Kornoi 0 3 0%
Kutum 11 23 48%
Mellit 6 30 20%
Saraf Omra 1 2 50%
Tawilla 4 10 40%
Um Buru 4 7 57%
Umm Keddada 0 22 0%
Total 60 298 20%
Of the 298 health facilities in North Darfur, 60 (20%) of them are designated EWARS HFs (mostly PHCCs &
BHUs). Um Buru locality has the highest number of designated HFs at 57%, conversely, Kalemando has the
lowest number of designated HFs at 6%.
El Kuma, El Malha, El Tina, Kornoi and Umm Keddada localities don’t have any designated EWARS facility.
58%
77%
20%
71%
81% 84%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
MA Nurse MW Vacc Nut Staff VTMW
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 26
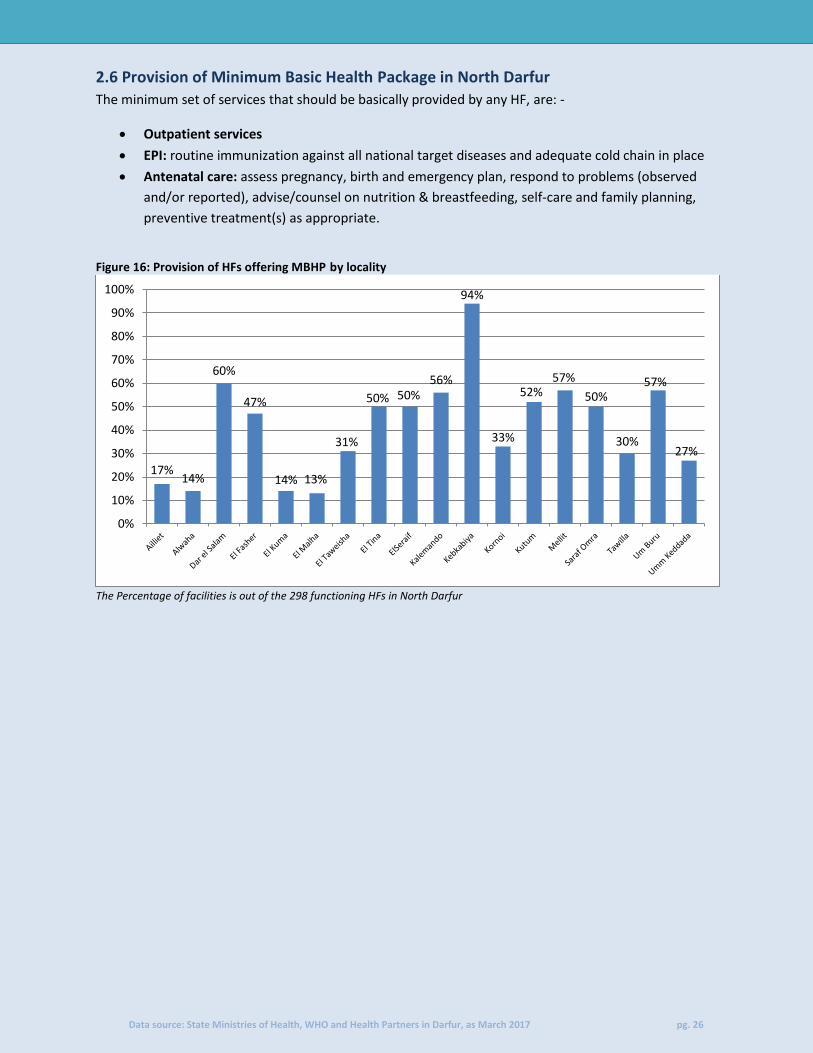
2.6 Provision of Minimum Basic Health Package in North Darfur
The minimum set of services that should be basically provided by any HF, are: -
Outpatient services
EPI: routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatment(s) as appropriate.
Figure 16: Provision of HFs offering MBHP by locality
The Percentage of facilities is out of the 298 functioning HFs in North Darfur
17% 14%
60%
47%
14% 13%
31%
50% 50% 56%
94%
33%
52% 57%
50%
30%
57%
27%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 27
3. South Darfur
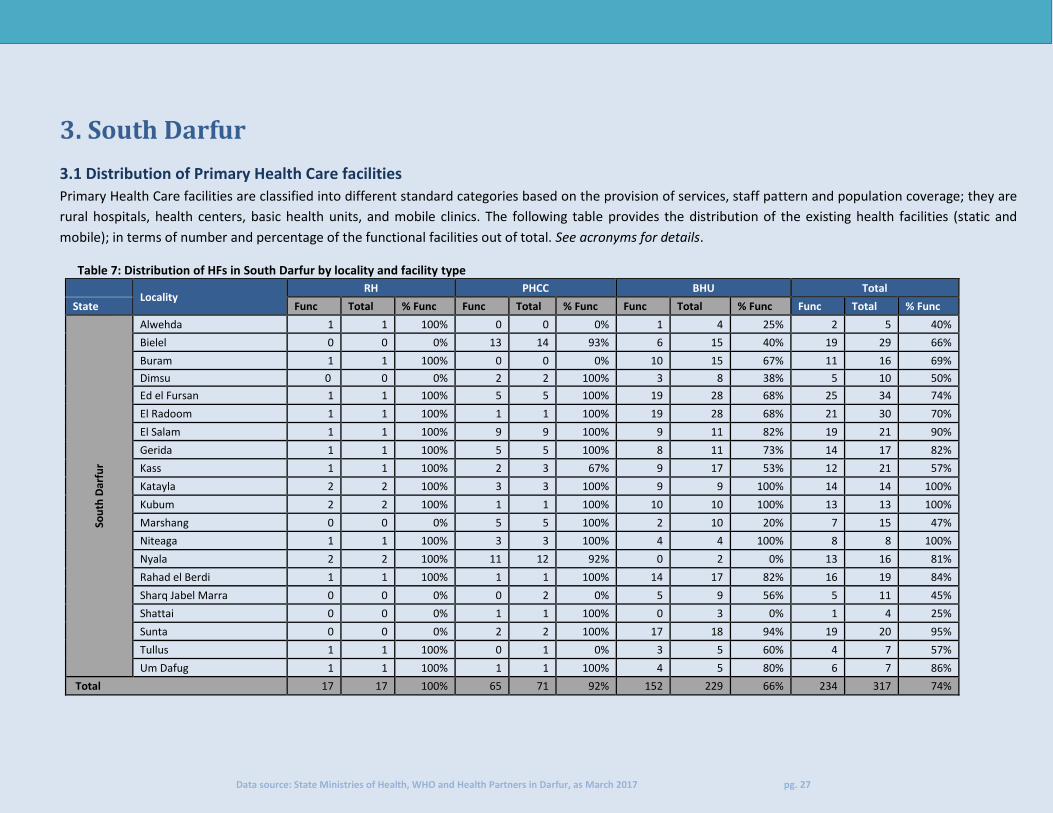
3.1 Distribution of Primary Health Care facilities
Primary Health Care facilities are classified into different standard categories based on the provision of services, staff pattern and population coverage; they are
rural hospitals, health centers, basic health units, and mobile clinics. The following table provides the distribution of the existing health facilities (static and
mobile); in terms of number and percentage of the functional facilities out of total. See acronyms for details.
Table 7: Distribution of HFs in South Darfur by locality and facility type
Locality
RH PHCC BHU Total
State Func Total % Func Func Total % Func Func Total % Func Func Total % Func
Sou
th D
arfu
r
Alwehda 1 1 100% 0 0 0% 1 4 25% 2 5 40%
Bielel 0 0 0% 13 14 93% 6 15 40% 19 29 66%
Buram 1 1 100% 0 0 0% 10 15 67% 11 16 69%
Dimsu 0 0 0% 2 2 100% 3 8 38% 5 10 50%
Ed el Fursan 1 1 100% 5 5 100% 19 28 68% 25 34 74%
El Radoom 1 1 100% 1 1 100% 19 28 68% 21 30 70%
El Salam 1 1 100% 9 9 100% 9 11 82% 19 21 90%
Gerida 1 1 100% 5 5 100% 8 11 73% 14 17 82%
Kass 1 1 100% 2 3 67% 9 17 53% 12 21 57%
Katayla 2 2 100% 3 3 100% 9 9 100% 14 14 100%
Kubum 2 2 100% 1 1 100% 10 10 100% 13 13 100%
Marshang 0 0 0% 5 5 100% 2 10 20% 7 15 47%
Niteaga 1 1 100% 3 3 100% 4 4 100% 8 8 100%
Nyala 2 2 100% 11 12 92% 0 2 0% 13 16 81%
Rahad el Berdi 1 1 100% 1 1 100% 14 17 82% 16 19 84%
Sharq Jabel Marra 0 0 0% 0 2 0% 5 9 56% 5 11 45%
Shattai 0 0 0% 1 1 100% 0 3 0% 1 4 25%
Sunta 0 0 0% 2 2 100% 17 18 94% 19 20 95%
Tullus 1 1 100% 0 1 0% 3 5 60% 4 7 57%
Um Dafug 1 1 100% 1 1 100% 4 5 80% 6 7 86%
Total 17 17 100% 65 71 92% 152 229 66% 234 317 74%
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 28
The number of HFs in South Darfur in Q1 2017 is 317 following a little increase from 316 in Q4 2016. Two
changes were noted in the Management of HFs after KPHF Takeover one clinic in Otash Camp and NIDO
NNGOs handed over Sheikh Musa clinic to SMoH. In total, 234 of the 317 HFs in South Darfur are
functional, broken down as 17 RHs (all function), 71 PHCCs (91.5% or 65 function), 229 BHUs (66.3% or 152
function).
Katayla (14 HFs), Kubum (13 HFs) and Niteaga (8 HFs) localities have all the HFs in those localities
functioning while only one Health Facility out of three in Shattai function.
Note: The 3 State Hospitals in Nyala locality are all functioning, they are, Teaching Hospital, Military
Hospital and Police Hospital. However, they are not analyzed amongst the health service delivery due to
the restriction in public usage.
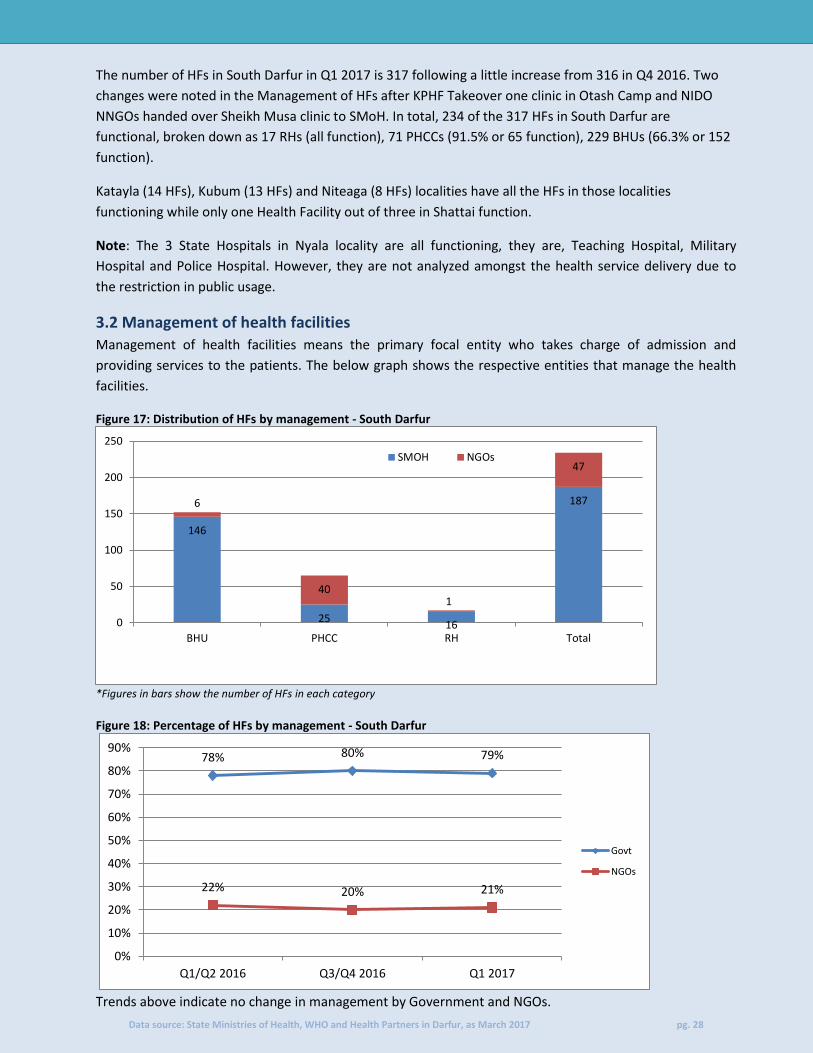
3.2 Management of health facilities
Management of health facilities means the primary focal entity who takes charge of admission and
providing services to the patients. The below graph shows the respective entities that manage the health
facilities.
Figure 17: Distribution of HFs by management - South Darfur
*Figures in bars show the number of HFs in each category Figure 18: Percentage of HFs by management - South Darfur
Trends above indicate no change in management by Government and NGOs.
146
25 16
187 6
40 1
47
0
50
100
150
200
250
BHU PHCC RH Total
SMOH NGOs
78% 80% 79%
22% 20% 21%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Q1/Q2 2016 Q3/Q4 2016 Q1 2017
Govt
NGOs
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 29
There has been a slight change in the management of facilities by both NGOs and the government. The only
change was the handover of three PHCCs from World Vision to the SMoH.
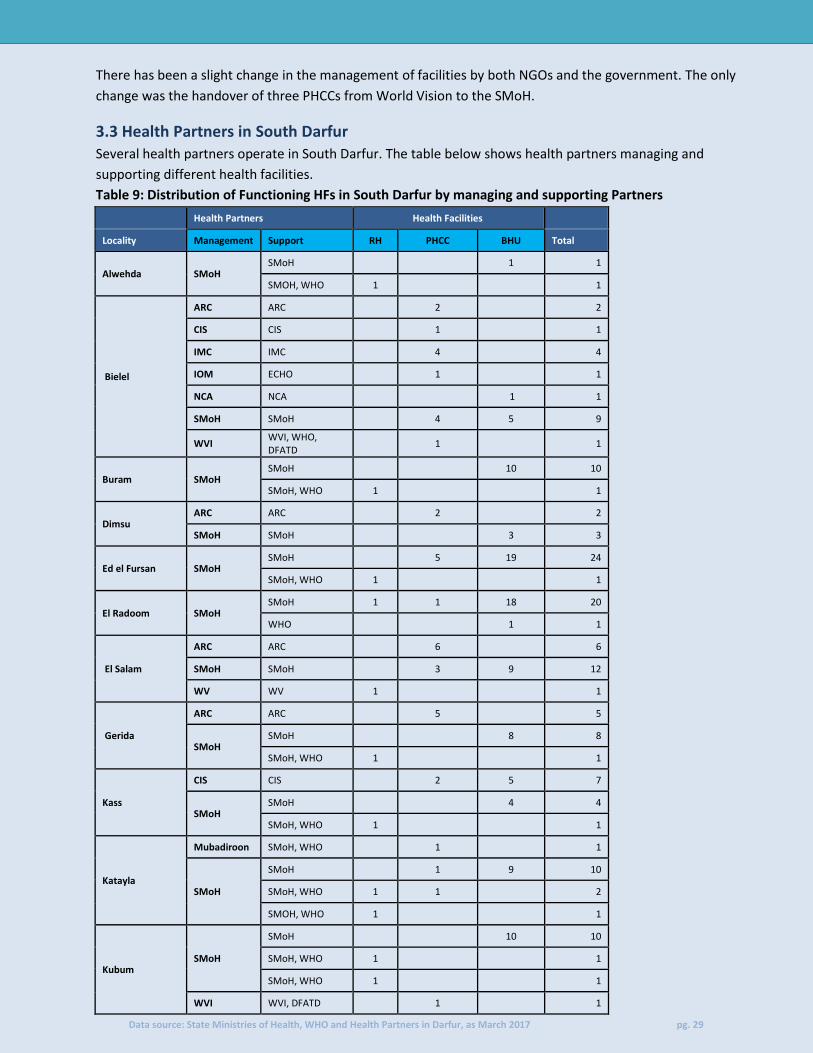
3.3 Health Partners in South Darfur
Several health partners operate in South Darfur. The table below shows health partners managing and
supporting different health facilities.
Table 9: Distribution of Functioning HFs in South Darfur by managing and supporting Partners
Health Partners Health Facilities
Locality Management Support RH PHCC BHU Total
Alwehda SMoH SMoH 1 1
SMOH, WHO 1 1
Bielel
ARC ARC 2 2
CIS CIS 1 1
IMC IMC 4 4
IOM ECHO 1 1
NCA NCA 1 1
SMoH SMoH 4 5 9
WVI WVI, WHO, DFATD
1 1
Buram SMoH SMoH 10 10
SMoH, WHO 1 1
Dimsu ARC ARC 2 2
SMoH SMoH 3 3
Ed el Fursan SMoH SMoH 5 19 24
SMoH, WHO 1 1
El Radoom SMoH SMoH 1 1 18 20
WHO 1 1
El Salam
ARC ARC 6 6
SMoH SMoH 3 9 12
WV WV 1 1
Gerida
ARC ARC 5 5
SMoH SMoH 8 8
SMoH, WHO 1 1
Kass
CIS CIS 2 5 7
SMoH SMoH 4 4
SMoH, WHO 1 1
Katayla
Mubadiroon SMoH, WHO 1 1
SMoH
SMoH 1 9 10
SMoH, WHO 1 1 2
SMOH, WHO 1 1
Kubum SMoH
SMoH 10 10
SMoH, WHO 1 1
SMoH, WHO 1 1
WVI WVI, DFATD 1 1

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 30
Marshang
SMoH SMoH 2 2
WVI
WVI 1 1
WVI, WHO, DFATD
1 1
WVI, WHO, OFDA 3 3
Niteaga
SMoH SMoH 1 2 4 7
WVI WVI, WHO, DFATD
1 1
Nyala
KPHF KPHF 1 2 3
Muslim aid.UK
Muslim aid.UK 1 1
RHF RHF 1 1
SMoH SMoH 1 5 5
WVI
WVI, WHO, OFDA 1 1
WVI, WHO, DFATD
1 1
Rahad el Berdi SMoH SMoH 1 14 15
SMoH, WHO 1 1
Sharq Jabel Marra
SMoH SMoH 5 5
Shattai SMoH SMoH 1 1
Sunta SMoH SMoH 17 17
WHO 2 2
Tullus SMoH SMoH 3 3
SMoH, WHO 1 1
Um Dafug SMoH SMoH 1 4 5
RHF RHF 1 1
Total 17 65 152 234
In addition to SMoH, 14 other partners manage or support HFs in South Darfur. As shown in the table
above, Nyala locality has the highest presence of partners with 8 working in the locality. Alwehda, Buaram,
Shattai and Sharq Jabel Marra localities have only SMoH working there although still receiving support from
WHO.
UNICEF and UNFPA provide regular support (drugs and medical supplies), either directly to the NGOs
managing the HFs or through the SMoH while WHO provides drugs, kits and equipment for PHCC and RHs
to fill any identified gaps and also respond to emergencies.
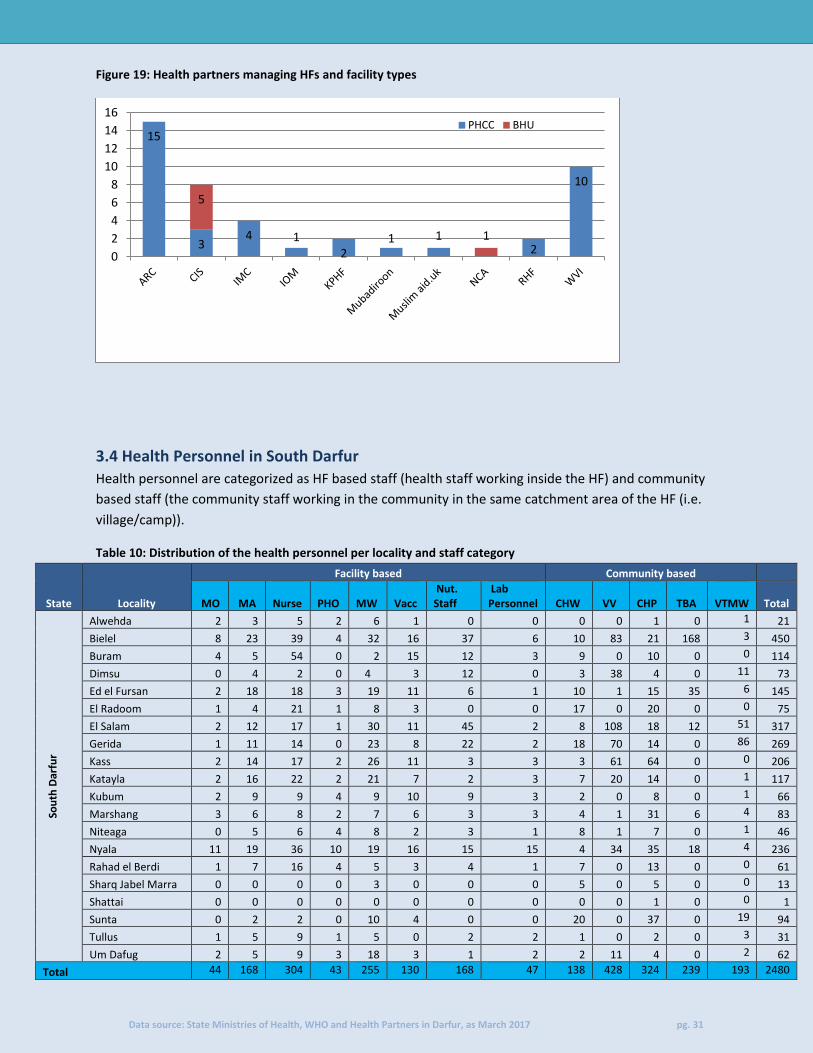
3.3.1 NGO health partners
Of the 234 functioning HFs in South Darfur, 47 HFs in South Darfur are managed by NGOs. ARC manages 15
(all PHCCs), the most of any NGO in the state. Followed by WVI with 10 (all PHCCs) then CIS with 8 (3 PHCCs
and 5 BHUs). The rest as shown in the graph below manage less than 5 HFs each.
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 31
Figure 19: Health partners managing HFs and facility types
3.4 Health Personnel in South Darfur
Health personnel are categorized as HF based staff (health staff working inside the HF) and community
based staff (the community staff working in the community in the same catchment area of the HF (i.e.
village/camp)).
Table 10: Distribution of the health personnel per locality and staff category
State
Locality
Facility based Community based
MO MA Nurse
PHO
MW
Vacc
Nut. Staff
Lab Personnel CHW VV
CHP TBA
VTMW Total
Sou
th D
arfu
r
Alwehda 2 3 5 2 6 1 0 0 0 0 1 0 1 21
Bielel 8 23 39 4 32 16 37 6 10 83 21 168 3 450
Buram 4 5 54 0 2 15 12 3 9 0 10 0 0 114
Dimsu 0 4 2 0 4 3 12 0 3 38 4 0 11 73
Ed el Fursan 2 18 18 3 19 11 6 1 10 1 15 35 6 145
El Radoom 1 4 21 1 8 3 0 0 17 0 20 0 0 75
El Salam 2 12 17 1 30 11 45 2 8 108 18 12 51 317
Gerida 1 11 14 0 23 8 22 2 18 70 14 0 86 269
Kass 2 14 17 2 26 11 3 3 3 61 64 0 0 206
Katayla 2 16 22 2 21 7 2 3 7 20 14 0 1 117
Kubum 2 9 9 4 9 10 9 3 2 0 8 0 1 66
Marshang 3 6 8 2 7 6 3 3 4 1 31 6 4 83
Niteaga 0 5 6 4 8 2 3 1 8 1 7 0 1 46
Nyala 11 19 36 10 19 16 15 15 4 34 35 18 4 236
Rahad el Berdi 1 7 16 4 5 3 4 1 7 0 13 0 0 61
Sharq Jabel Marra 0 0 0 0 3 0 0 0 5 0 5 0 0 13
Shattai 0 0 0 0 0 0 0 0 0 0 1 0 0 1
Sunta 0 2 2 0 10 4 0 0 20 0 37 0 19 94
Tullus 1 5 9 1 5 0 2 2 1 0 2 0 3 31
Um Dafug 2 5 9 3 18 3 1 2 2 11 4 0 2 62
Total 44 168 304 43 255 130 168 47 138 428 324 239 193 2480
15
3 4 1
2 1 1
2
10
5
1
0
2
4
6
8
10
12
14
16PHCC BHU

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 32
The number of medical personnel in this quarter indicates increase by 8% from 2,279 in Q4/– 2016 to 2,480
in Q1- 2017. Of these 1,159 (47%) are facility based while 1,321(53%) are community based staff.
As it was reported in the previous quarter, Shattai locality has only one HFs which operates with only One
CHP. On the other hand, Bielel Locality has 450 personnel.
Figure 21: Distribution of Medical Officers, Medical Assistant and Nurse by locality
0
10
20
30
40
50
60
70
80 MO MA Nurse
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 33
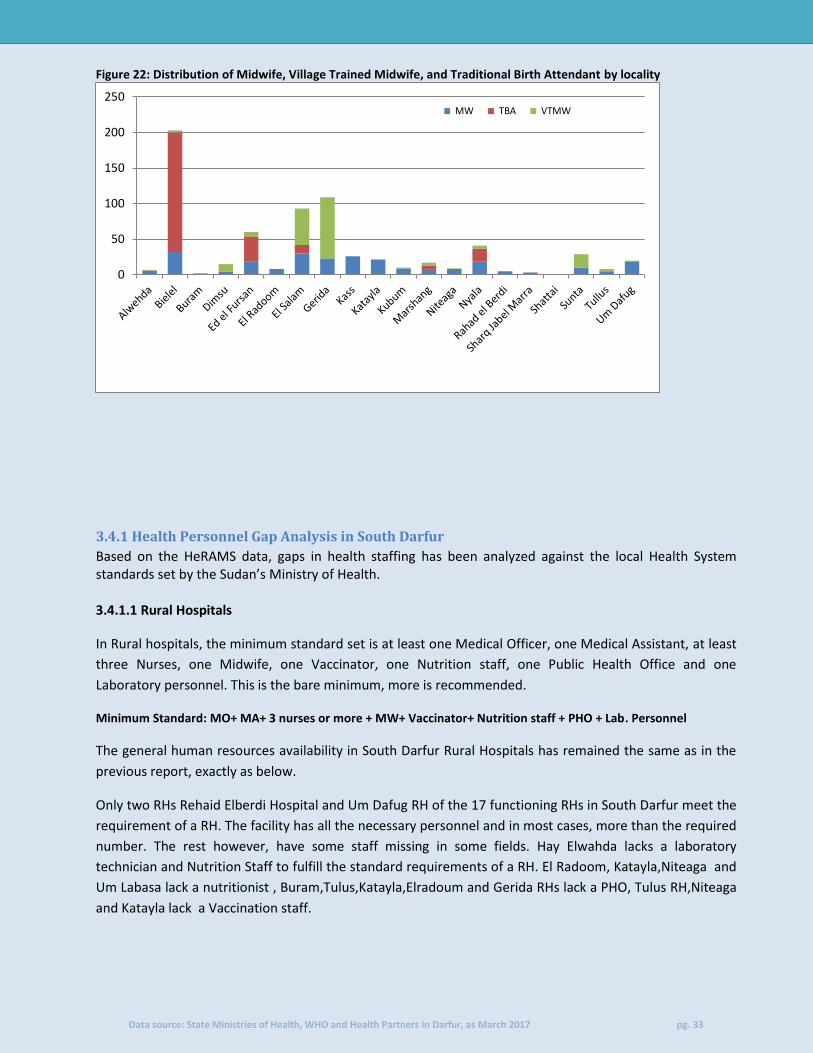
Figure 22: Distribution of Midwife, Village Trained Midwife, and Traditional Birth Attendant by locality
3.4.1 Health Personnel Gap Analysis in South Darfur
Based on the HeRAMS data, gaps in health staffing has been analyzed against the local Health System standards set by the Sudan’s Ministry of Health. 3.4.1.1 Rural Hospitals
In Rural hospitals, the minimum standard set is at least one Medical Officer, one Medical Assistant, at least
three Nurses, one Midwife, one Vaccinator, one Nutrition staff, one Public Health Office and one
Laboratory personnel. This is the bare minimum, more is recommended.
Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
The general human resources availability in South Darfur Rural Hospitals has remained the same as in the
previous report, exactly as below.
Only two RHs Rehaid Elberdi Hospital and Um Dafug RH of the 17 functioning RHs in South Darfur meet the
requirement of a RH. The facility has all the necessary personnel and in most cases, more than the required
number. The rest however, have some staff missing in some fields. Hay Elwahda lacks a laboratory
technician and Nutrition Staff to fulfill the standard requirements of a RH. El Radoom, Katayla,Niteaga and
Um Labasa lack a nutritionist , Buram,Tulus,Katayla,Elradoum and Gerida RHs lack a PHO, Tulus RH,Niteaga
and Katayla lack a Vaccination staff.
0
50
100
150
200
250 MW TBA VTMW
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 34
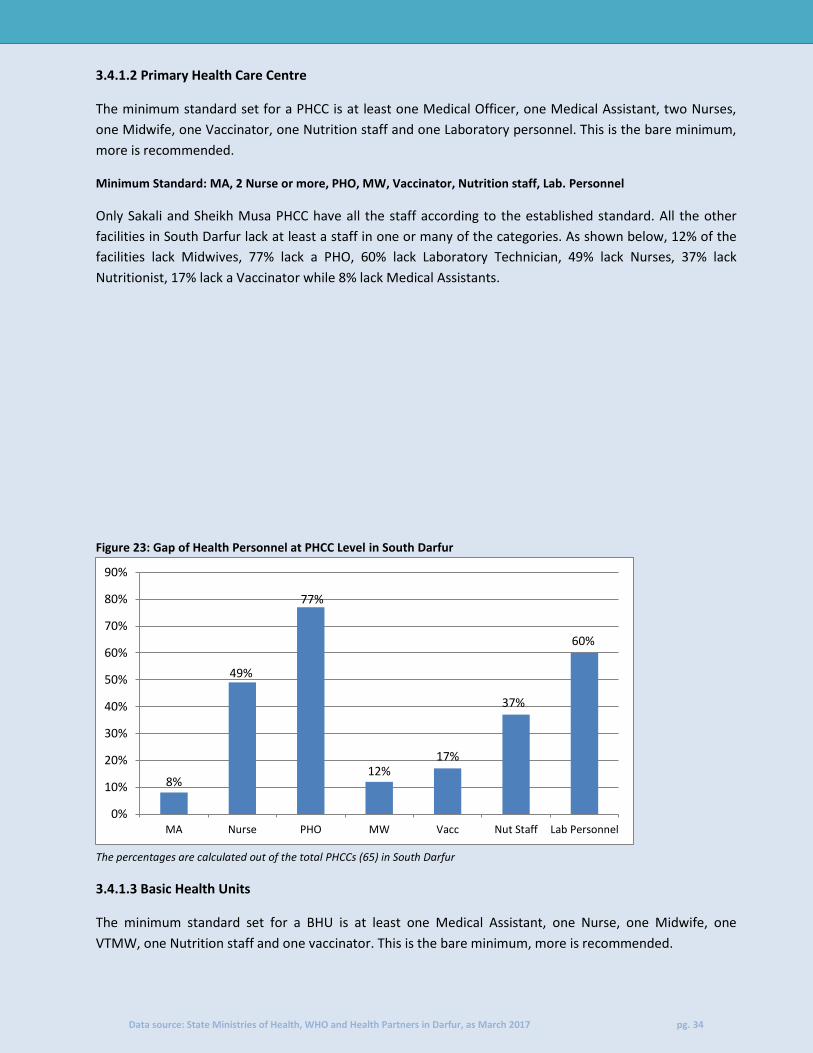
3.4.1.2 Primary Health Care Centre
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses,
one Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare minimum,
more is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff, Lab. Personnel
Only Sakali and Sheikh Musa PHCC have all the staff according to the established standard. All the other
facilities in South Darfur lack at least a staff in one or many of the categories. As shown below, 12% of the
facilities lack Midwives, 77% lack a PHO, 60% lack Laboratory Technician, 49% lack Nurses, 37% lack
Nutritionist, 17% lack a Vaccinator while 8% lack Medical Assistants.
Figure 23: Gap of Health Personnel at PHCC Level in South Darfur
The percentages are calculated out of the total PHCCs (65) in South Darfur
3.4.1.3 Basic Health Units
The minimum standard set for a BHU is at least one Medical Assistant, one Nurse, one Midwife, one
VTMW, one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
8%
49%
77%
12% 17%
37%
60%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
MA Nurse PHO MW Vacc Nut Staff Lab Personnel

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 35
Minimum Standard: MA, Nurse, MW, VTMW, Nutrition staff and Vaccinator
Like in the PHCCs, no changes were recorded in the number of medical personnel working in BHUs in South
Darfur.
Only Gereida BHU has the required staff composition of a BHU. The rest lack one or most of the staff. Most
facilities, 97% lack a VTMW, 96% lack nutritionist, while 89% lack vaccinators, 81% lack Midwifes, 78% lack
nurses while 68% lack medical assistants.
Figure 24: Gap of Health Personnel at BHU Level in North Darfur
The percentages are calculated out of the total BHUs (152) in South Darfur
3.5 EWARS reporting HFs in South Darfur EWARS is an essential service for detection of unusual diseases and outbreaks of communicable diseases. In Darfur however, only a few facilities are designated sites due to the existence of the equipment and necessary training for the EWARS staff. The table below shows summary of the number of functioning HFs designated under EWARS
Table 11: Distribution of functioning HFs reporting under EWARS
Locality EWARS designated sites Total HFs in the Locatiy % EWARS designated sites
Alwehda 1 2 50%
Bielel 12 19 63%
Dimsu 2 5 40%
Ed el Fursan 6 25 24%
El Salam 9 19 47%
Gerida 7 14 50%
Kass 8 12 67%
Katayla 5 14 36%
Kubum 1 13 8%
Marshang 5 7 71%
Niteaga 1 8 13%
Nyala 11 13 85%
Sunta 1 19 5%
Um Dafug 2 6 33%
Total 71 176 40%
68%
78% 81% 89%
96% 97%
0%
20%
40%
60%
80%
100%
120%
MA Nurse MW Vacc Nut Staff VTMW

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 36
Of the 234 health facilities in South Darfur, 71 (30%) of them are designated EWARS HFs (mostly PHCCs &
BHUs). In addition, only 40% of HFs of the localities that have EWARS designated sites, as shown above.
Nyala locality has the highest number of designated HFs at 85%. Conversely, Sunta has the lowest number
of designated HFs at 5%.
Buram, El Radoom, Rahad el Berdi, Sharq Jebel Marra, Shattai and Tullus localities don’t have any
designated EWARS reporting units.
3.6 Provision of Minimum Basic Health Package in South Darfur The minimum set of services that should be basically provided by any HF, are:
Outpatient services
EPI: routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatment(s) as appropriate.
Figure 25: Provision of HFs offering MBHP by locality
The Percentage of facilities is out of the 234 functioning HFs in South Darfur
26%
60% 56%
42% 50%
33%
50%
69%
14% 12% 8%
89%
67%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 37
4. East Darfur
4.1 Distribution of Primary Health Care facilities:
Health Facilities are classified into different standard categories based on the provision of services, staffing and population coverage; they are
Rural Hospitals (RH), Primary Health Care Centers (PHCC), Basic Health Units (BHU), and Mobile Clinics. The following table provides the
distribution of the existing health facilities (static and mobile); showing the number and percentage of the functional facilities out of total. See
acronyms for the initials used.
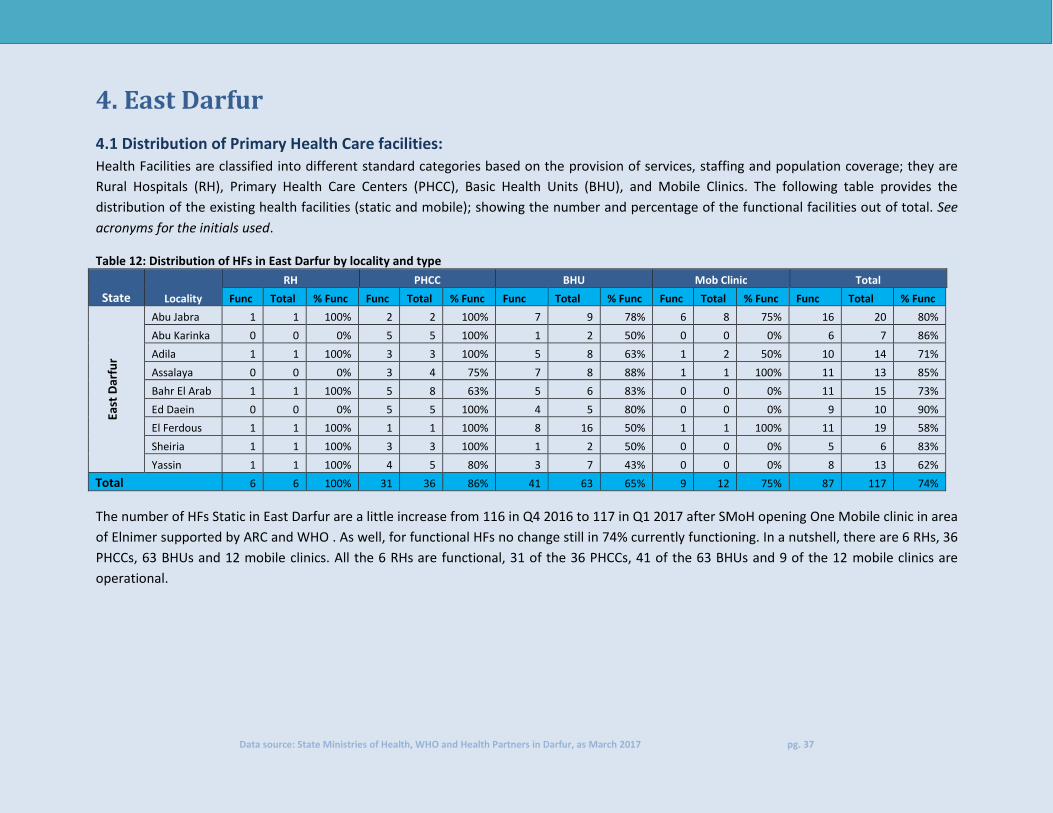
Table 12: Distribution of HFs in East Darfur by locality and type
State Locality
RH PHCC BHU Mob Clinic Total
Func Total % Func Func Total % Func Func Total % Func Func Total % Func Func Total % Func
East
Dar
fur
Abu Jabra 1 1 100% 2 2 100% 7 9 78% 6 8 75% 16 20 80%
Abu Karinka 0 0 0% 5 5 100% 1 2 50% 0 0 0% 6 7 86%
Adila 1 1 100% 3 3 100% 5 8 63% 1 2 50% 10 14 71%
Assalaya 0 0 0% 3 4 75% 7 8 88% 1 1 100% 11 13 85%
Bahr El Arab 1 1 100% 5 8 63% 5 6 83% 0 0 0% 11 15 73%
Ed Daein 0 0 0% 5 5 100% 4 5 80% 0 0 0% 9 10 90%
El Ferdous 1 1 100% 1 1 100% 8 16 50% 1 1 100% 11 19 58%
Sheiria 1 1 100% 3 3 100% 1 2 50% 0 0 0% 5 6 83%
Yassin 1 1 100% 4 5 80% 3 7 43% 0 0 0% 8 13 62%
Total 6 6 100% 31 36 86% 41 63 65% 9 12 75% 87 117 74%
The number of HFs Static in East Darfur are a little increase from 116 in Q4 2016 to 117 in Q1 2017 after SMoH opening One Mobile clinic in area
of Elnimer supported by ARC and WHO . As well, for functional HFs no change still in 74% currently functioning. In a nutshell, there are 6 RHs, 36
PHCCs, 63 BHUs and 12 mobile clinics. All the 6 RHs are functional, 31 of the 36 PHCCs, 41 of the 63 BHUs and 9 of the 12 mobile clinics are
operational.
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 38
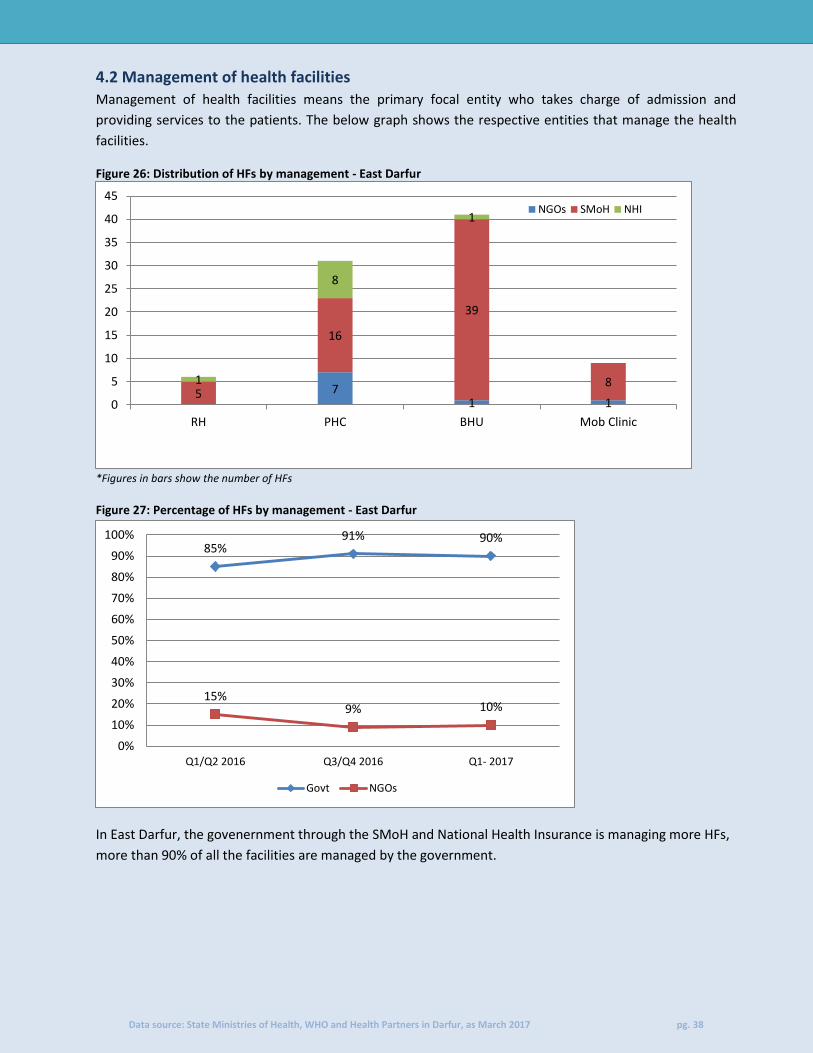
4.2 Management of health facilities
Management of health facilities means the primary focal entity who takes charge of admission and
providing services to the patients. The below graph shows the respective entities that manage the health
facilities.
Figure 26: Distribution of HFs by management - East Darfur
*Figures in bars show the number of HFs Figure 27: Percentage of HFs by management - East Darfur
In East Darfur, the govenernment through the SMoH and National Health Insurance is managing more HFs,
more than 90% of all the facilities are managed by the government.
7 1 1
5
16
39
8 1
8
1
0
5
10
15
20
25
30
35
40
45
RH PHC BHU Mob Clinic
NGOs SMoH NHI
85% 91% 90%
15% 9% 10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Q1/Q2 2016 Q3/Q4 2016 Q1- 2017
Govt NGOs
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 39
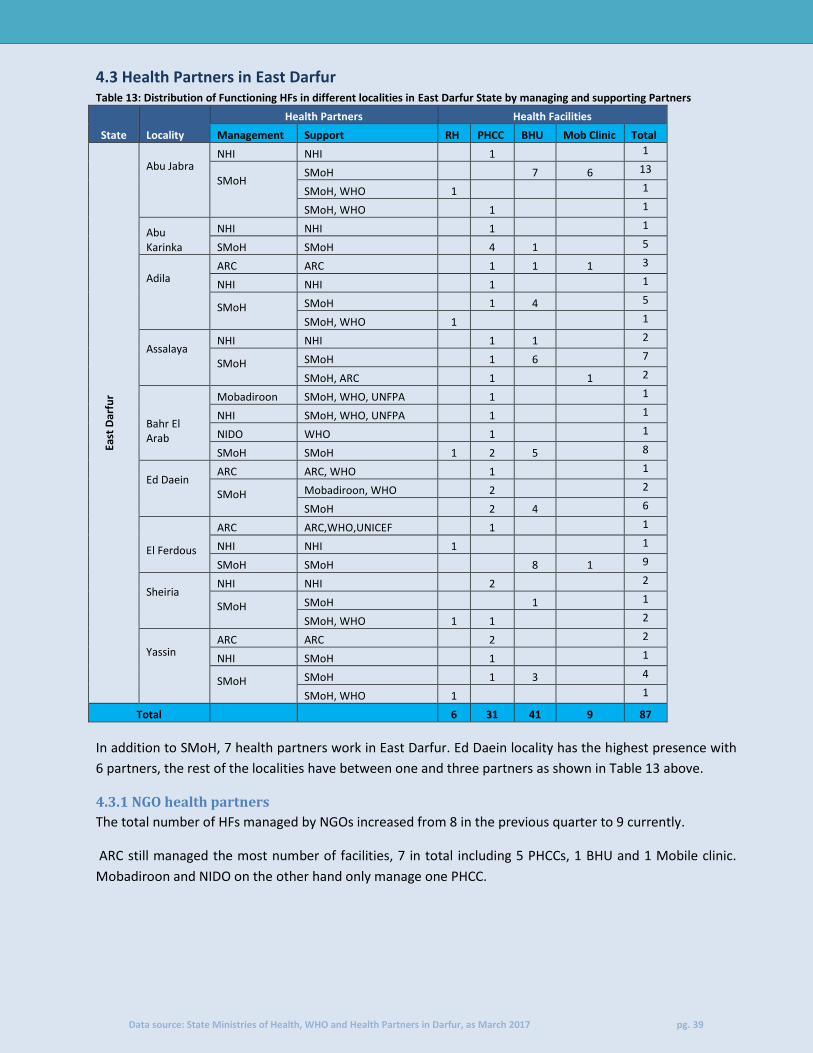
4.3 Health Partners in East Darfur Table 13: Distribution of Functioning HFs in different localities in East Darfur State by managing and supporting Partners
State Locality
Health Partners Health Facilities
Management Support RH PHCC BHU Mob Clinic Total
East
Dar
fur
Abu Jabra
NHI NHI
1
1
SMoH
SMoH
7 6 13
SMoH, WHO 1
1
SMoH, WHO
1
1
Abu Karinka
NHI NHI
1
1
SMoH SMoH
4 1
5
Adila
ARC ARC
1 1 1 3
NHI NHI
1
1
SMoH
SMoH
1 4
5
SMoH, WHO 1
1
Assalaya
NHI NHI
1 1
2
SMoH
SMoH
1 6
7
SMoH, ARC
1
1 2
Bahr El Arab
Mobadiroon SMoH, WHO, UNFPA
1
1
NHI SMoH, WHO, UNFPA
1
1
NIDO WHO 1 1
SMoH SMoH 1 2 5
8
Ed Daein
ARC ARC, WHO
1
1
SMoH
Mobadiroon, WHO
2
2
SMoH
2 4
6
El Ferdous
ARC ARC,WHO,UNICEF
1
1
NHI NHI 1
1
SMoH SMoH
8 1 9
Sheiria
NHI NHI
2
2
SMoH
SMoH
1
1
SMoH, WHO 1 1
2
Yassin
ARC ARC
2
2
NHI SMoH
1
1
SMoH
SMoH
1 3
4
SMoH, WHO 1
1
Total 6 31 41 9 87
In addition to SMoH, 7 health partners work in East Darfur. Ed Daein locality has the highest presence with
6 partners, the rest of the localities have between one and three partners as shown in Table 13 above.
4.3.1 NGO health partners
The total number of HFs managed by NGOs increased from 8 in the previous quarter to 9 currently.
ARC still managed the most number of facilities, 7 in total including 5 PHCCs, 1 BHU and 1 Mobile clinic.
Mobadiroon and NIDO on the other hand only manage one PHCC.

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 40
Figure 28: Health partners managing HFs and facility types
4.4 Health Personnel in East Darfur Health personnel are categorized as HF based staff (health staff working inside the HF) and community based staff
(the community staff working in the community in the same catchment area of the HF (i.e. village/camp)).
Table 14: Distribution of the health personnel per locality and staff category
State
Locality
Facility based Community based
MO MA Nurse PHO MW Vacc Nut Staff
Lab Person CHW VV CHP TBA VTMW Total
East
Dar
fur
Abu Jabra 4 4 8 3 8 6 1 5 36 13 17 3 10 118
Abu Karinka 1 4 3 5 9 4 1 1 1 5 3 0 4 41
Adila 2 8 9 11 18 7 14 4 14 13 5 43 2 150
Assalaya 1 7 2 10 15 8 0 0 5 24 10 12 11 105
Bahr El Arab 3 9 6 2 14 16 10 11 9 30 9 4 6 129
Ed Daein 13 13 41 6 25 11 19 8 1 12 11 112 8 280
El Ferdous 0 11 12 3 11 7 6 3 11 30 8 10 19 131
Sheiria 2 2 8 0 16 3 4 2 7 0 4 3 9 60
Yassin 1 9 6 1 18 8 14 2 29 1 4 1 8 102
Total 27 67 95 41 134 70 69 36 113 128 71 188 77 1,116
Following an increase from 1,015 in Q4 2016 to 1,116 in Q1 2017, of these, 539 (48%) are facility based,
while the remaining 577 (52%) are community based.
As it was in the last quarter, Ed Daein has the highest number of medical personnel at 280 followed by
Adila with 150. Conversely, Abu Karinka has the lowest number of health workers at 41 personnel. As
shown in the Table 14 above.
5
1 1
1
1
0
1
2
3
4
5
6
7
8
PHC BHU Mob clinic
ARC NIDO Mobadiroon

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 41
Figure 27: Distribution of Medical Officers, Medical Assistants and Nurses by locality
Figure 28: Distribution of Midwives, Village Trained Midwives, and Traditional Birth Attendants by locality
4.4.1 Health Personnel Gap Analysis in East Darfur
Based on the HeRAMS data, gaps in health staffing has been analyzed against the local Health System standards set by the Sudan’s Ministry of Health. 4.4.1.1 Rural Hospitals
In Rural hospitals, the minimum standard set is at least one Medical Officer, one Medical Assistant, at least three nurses, one Midwife, one Vaccinator, one Nutrition staff, one Public Health Officer and one Laboratory personnel. This is the bare minimum, more is recommended.
4 1 2 1 3 13
0 2 1
4 4
8 7 9
13
11 2
9
8
3
9
2
7
41
12
8
6
0
10
20
30
40
50
60
70
80
Abu Jabra AbuKarinka
Adila Assalaya Bahr ElArab
Ed Daein El Ferdous Sheiria Yassin
MO MA Nurse
8 9 18 15 14
25 11 16 18 3 0
43
12 4
112
10 3 1 10 4
2
10
6
8
19 9 8
0
20
40
60
80
100
120
140
160
Abu Jabra Abu Karinka Adila Assalaya Bahr ElArab
Ed Daein El Ferdous Sheiria Yassin
MW TBA VTMW
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 42
Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
All the six RHs in East Darfur start improving for the minimum standards set by the MoH. Abu Jabra meet all
except they lack a nutritionist, Assalaya and Sheiria meet all but lack a PHO for Sheiria and lack of
nutritionist and Lab Personnel for Assalaya . still Ferdous RH they don’t have MO same as previous report.
Mohajrea and Abu Matarig face the worst challenge in medical personnel. Mohajrea lack a MO, the
required three nurses and a PHO. Meanwhile Abumatarig lack a MA, the required three Nurses and a PHO.
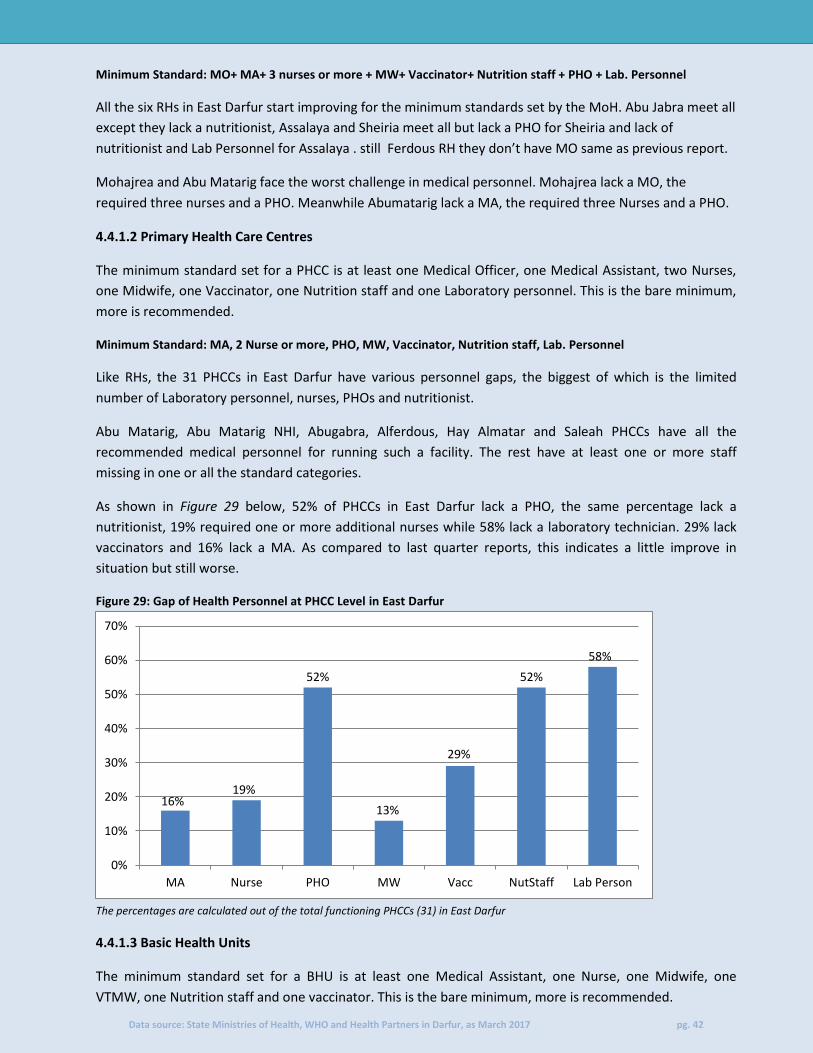
4.4.1.2 Primary Health Care Centres
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses,
one Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare minimum,
more is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff, Lab. Personnel
Like RHs, the 31 PHCCs in East Darfur have various personnel gaps, the biggest of which is the limited
number of Laboratory personnel, nurses, PHOs and nutritionist.
Abu Matarig, Abu Matarig NHI, Abugabra, Alferdous, Hay Almatar and Saleah PHCCs have all the
recommended medical personnel for running such a facility. The rest have at least one or more staff
missing in one or all the standard categories.
As shown in Figure 29 below, 52% of PHCCs in East Darfur lack a PHO, the same percentage lack a
nutritionist, 19% required one or more additional nurses while 58% lack a laboratory technician. 29% lack
vaccinators and 16% lack a MA. As compared to last quarter reports, this indicates a little improve in
situation but still worse.
Figure 29: Gap of Health Personnel at PHCC Level in East Darfur
The percentages are calculated out of the total functioning PHCCs (31) in East Darfur
4.4.1.3 Basic Health Units
The minimum standard set for a BHU is at least one Medical Assistant, one Nurse, one Midwife, one
VTMW, one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
16% 19%
52%
13%
29%
52%
58%
0%
10%
20%
30%
40%
50%
60%
70%
MA Nurse PHO MW Vacc NutStaff Lab Person
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 43
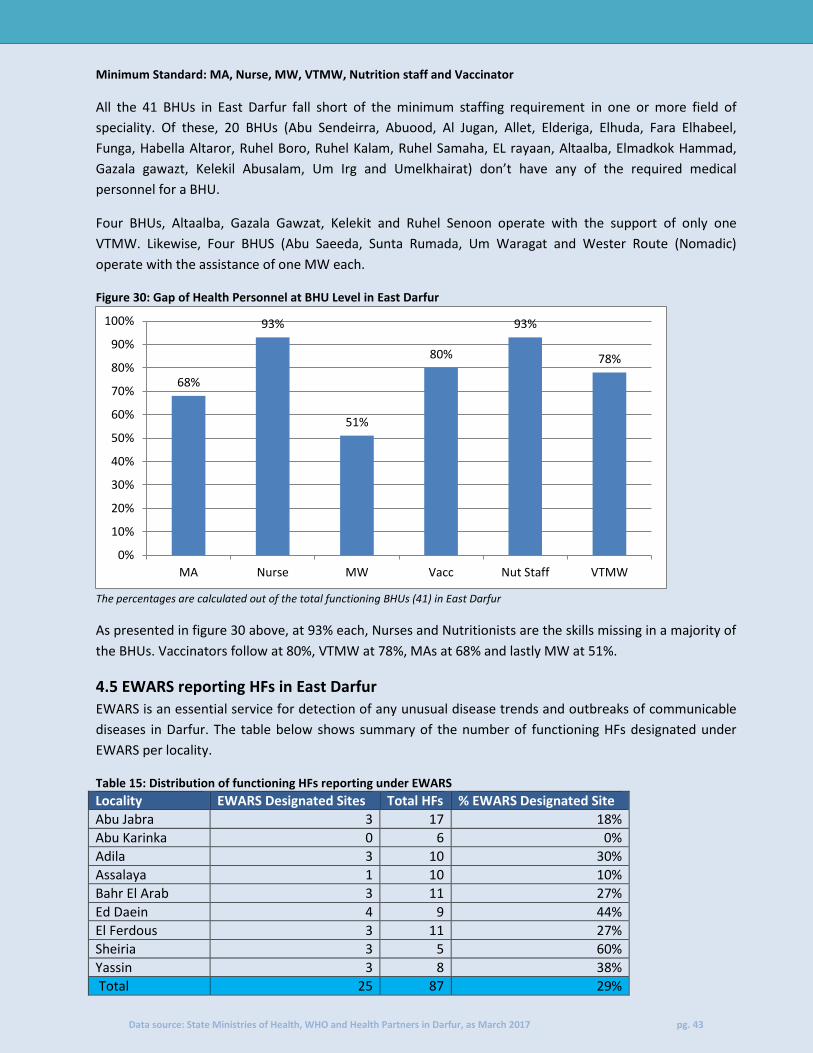
Minimum Standard: MA, Nurse, MW, VTMW, Nutrition staff and Vaccinator
All the 41 BHUs in East Darfur fall short of the minimum staffing requirement in one or more field of
speciality. Of these, 20 BHUs (Abu Sendeirra, Abuood, Al Jugan, Allet, Elderiga, Elhuda, Fara Elhabeel,
Funga, Habella Altaror, Ruhel Boro, Ruhel Kalam, Ruhel Samaha, EL rayaan, Altaalba, Elmadkok Hammad,
Gazala gawazt, Kelekil Abusalam, Um Irg and Umelkhairat) don’t have any of the required medical
personnel for a BHU.
Four BHUs, Altaalba, Gazala Gawzat, Kelekit and Ruhel Senoon operate with the support of only one
VTMW. Likewise, Four BHUS (Abu Saeeda, Sunta Rumada, Um Waragat and Wester Route (Nomadic)
operate with the assistance of one MW each.
Figure 30: Gap of Health Personnel at BHU Level in East Darfur
The percentages are calculated out of the total functioning BHUs (41) in East Darfur
As presented in figure 30 above, at 93% each, Nurses and Nutritionists are the skills missing in a majority of
the BHUs. Vaccinators follow at 80%, VTMW at 78%, MAs at 68% and lastly MW at 51%.
4.5 EWARS reporting HFs in East Darfur
EWARS is an essential service for detection of any unusual disease trends and outbreaks of communicable
diseases in Darfur. The table below shows summary of the number of functioning HFs designated under
EWARS per locality.
Table 15: Distribution of functioning HFs reporting under EWARS
Locality EWARS Designated Sites Total HFs % EWARS Designated Site
Abu Jabra 3 17 18%
Abu Karinka 0 6 0%
Adila 3 10 30%
Assalaya 1 10 10%
Bahr El Arab 3 11 27%
Ed Daein 4 9 44%
El Ferdous 3 11 27%
Sheiria 3 5 60%
Yassin 3 8 38%
Total 25 87 29%
68%
93%
51%
80%
93%
78%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MA Nurse MW Vacc Nut Staff VTMW

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 44
All the localities in East Darfur have at least one EWARS facility except Abu Karinka locality. However, only 25 (29%) of the 87 HFs are designated EWARS sites. Ed Daein locality has the highest number of HFs at 44%.
4.6 Provision of Minimum Basic Health package in East Darfur
The minimum set of services that should be basically provided by any HF, are:
Outpatient services
EPI: routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatment(s) as appropriate.
Figure 31: Provision of HFs offering MBHP by locality
Percentage represents the percentage of HFs providing the MBHP out of the total functioning HFs
19% 17%
40%
27% 27%
55%
27%
20%
62%
0%
10%
20%
30%
40%
50%
60%
70%
Abu Jabra Abu Karinka Adila Assalaya Bahr El Arab Ed Daein El Ferdous Sheiria Yassin
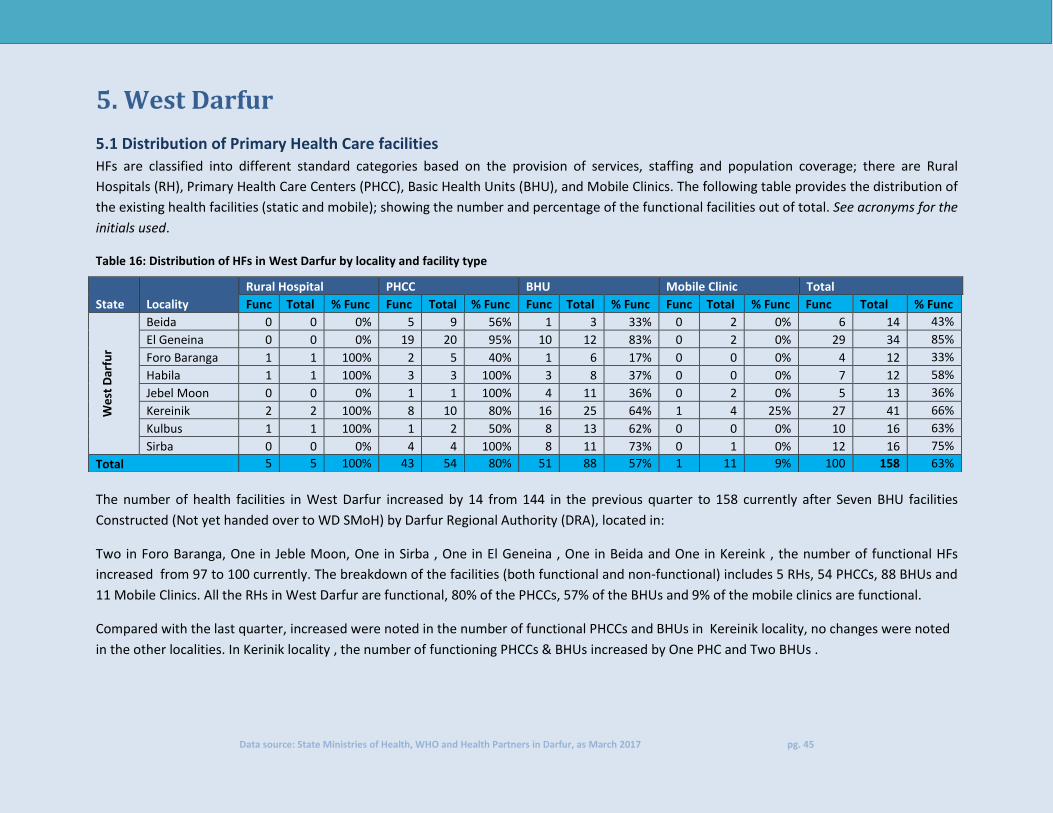
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 45
5. West Darfur
5.1 Distribution of Primary Health Care facilities
HFs are classified into different standard categories based on the provision of services, staffing and population coverage; there are Rural
Hospitals (RH), Primary Health Care Centers (PHCC), Basic Health Units (BHU), and Mobile Clinics. The following table provides the distribution of
the existing health facilities (static and mobile); showing the number and percentage of the functional facilities out of total. See acronyms for the
initials used.
Table 16: Distribution of HFs in West Darfur by locality and facility type
The number of health facilities in West Darfur increased by 14 from 144 in the previous quarter to 158 currently after Seven BHU facilities
Constructed (Not yet handed over to WD SMoH) by Darfur Regional Authority (DRA), located in:
Two in Foro Baranga, One in Jeble Moon, One in Sirba , One in El Geneina , One in Beida and One in Kereink , the number of functional HFs
increased from 97 to 100 currently. The breakdown of the facilities (both functional and non-functional) includes 5 RHs, 54 PHCCs, 88 BHUs and
11 Mobile Clinics. All the RHs in West Darfur are functional, 80% of the PHCCs, 57% of the BHUs and 9% of the mobile clinics are functional.
Compared with the last quarter, increased were noted in the number of functional PHCCs and BHUs in Kereinik locality, no changes were noted
in the other localities. In Kerinik locality , the number of functioning PHCCs & BHUs increased by One PHC and Two BHUs .
State Locality
Rural Hospital PHCC BHU Mobile Clinic Total
Func Total % Func Func Total % Func Func Total % Func Func Total % Func Func Total % Func
We
st D
arfu
r
Beida 0 0 0% 5 9 56% 1 3 33% 0 2 0% 6 14 43%
El Geneina 0 0 0% 19 20 95% 10 12 83% 0 2 0% 29 34 85%
Foro Baranga 1 1 100% 2 5 40% 1 6 17% 0 0 0% 4 12 33%
Habila 1 1 100% 3 3 100% 3 8 37% 0 0 0% 7 12 58%
Jebel Moon 0 0 0% 1 1 100% 4 11 36% 0 2 0% 5 13 36%
Kereinik 2 2 100% 8 10 80% 16 25 64% 1 4 25% 27 41 66%
Kulbus 1 1 100% 1 2 50% 8 13 62% 0 0 0% 10 16 63%
Sirba 0 0 0% 4 4 100% 8 11 73% 0 1 0% 12 16 75%
Total 5 5 100% 43 54 80% 51 88 57% 1 11 9% 100 158 63%
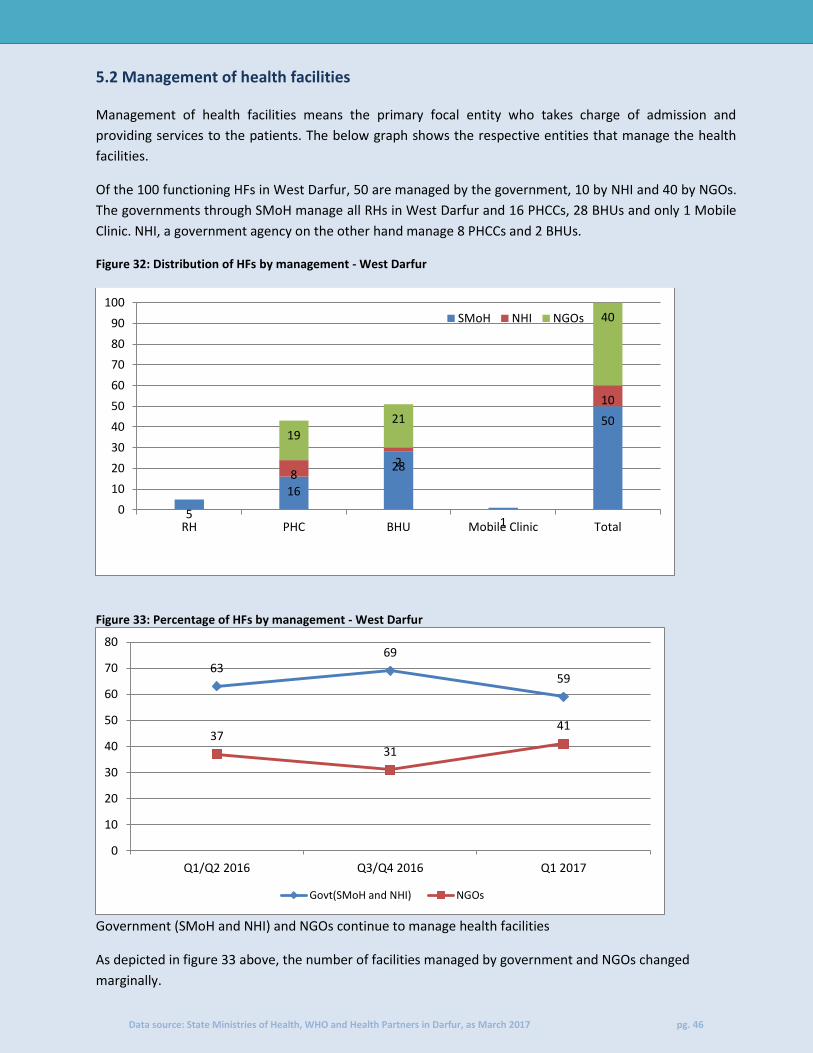
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 46
5.2 Management of health facilities
Management of health facilities means the primary focal entity who takes charge of admission and
providing services to the patients. The below graph shows the respective entities that manage the health
facilities.
Of the 100 functioning HFs in West Darfur, 50 are managed by the government, 10 by NHI and 40 by NGOs.
The governments through SMoH manage all RHs in West Darfur and 16 PHCCs, 28 BHUs and only 1 Mobile
Clinic. NHI, a government agency on the other hand manage 8 PHCCs and 2 BHUs.
Figure 32: Distribution of HFs by management - West Darfur
Figure 33: Percentage of HFs by management - West Darfur
Government (SMoH and NHI) and NGOs continue to manage health facilities
As depicted in figure 33 above, the number of facilities managed by government and NGOs changed
marginally.
5
16
28
1
50
8 2
10
19
21
40
0
10
20
30
40
50
60
70
80
90
100
RH PHC BHU Mobile Clinic Total
SMoH NHI NGOs
63 69
59
37 31
41
0
10
20
30
40
50
60
70
80
Q1/Q2 2016 Q3/Q4 2016 Q1 2017
Govt(SMoH and NHI) NGOs
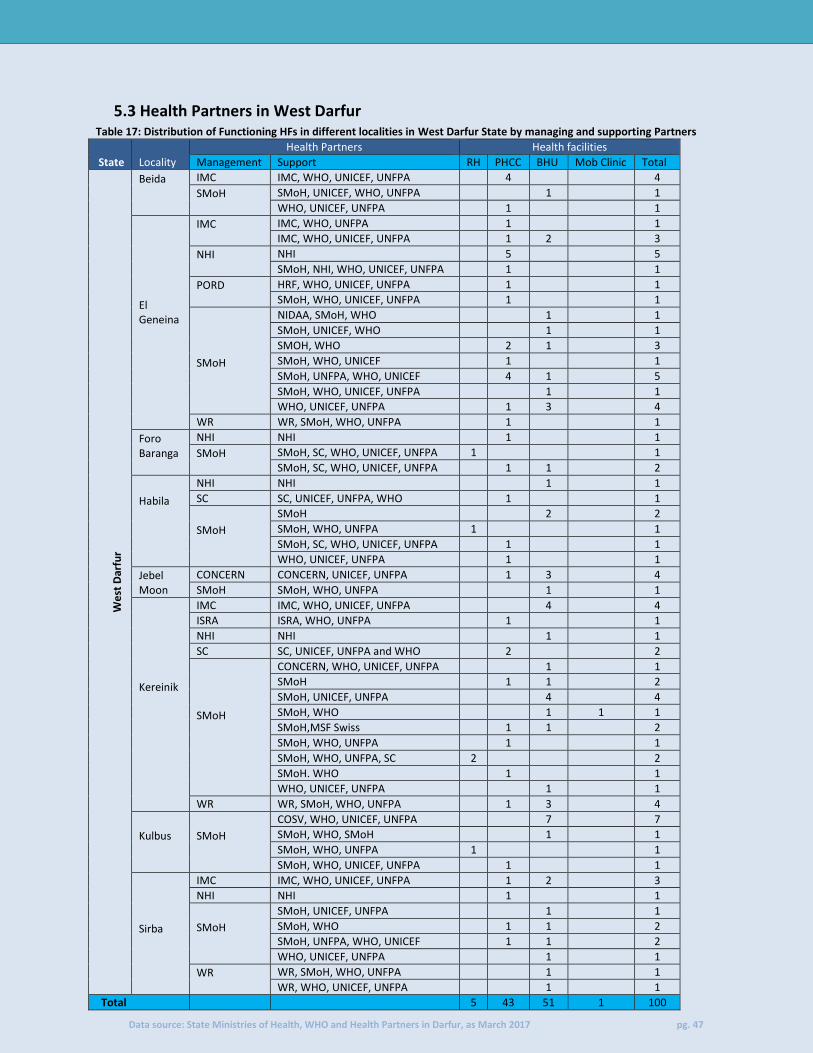
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 47
5.3 Health Partners in West Darfur Table 17: Distribution of Functioning HFs in different localities in West Darfur State by managing and supporting Partners
State Locality
Health Partners Health facilities
Management Support RH PHCC BHU Mob Clinic Total
We
st D
arfu
r
Beida
IMC IMC, WHO, UNICEF, UNFPA
4
4
SMoH
SMoH, UNICEF, WHO, UNFPA
1
1
WHO, UNICEF, UNFPA
1
1
El Geneina
IMC
IMC, WHO, UNFPA
1
1
IMC, WHO, UNICEF, UNFPA
1 2
3
NHI
NHI
5
5
SMoH, NHI, WHO, UNICEF, UNFPA
1
1
PORD
HRF, WHO, UNICEF, UNFPA
1
1
SMoH, WHO, UNICEF, UNFPA
1
1
SMoH
NIDAA, SMoH, WHO
1
1
SMoH, UNICEF, WHO
1
1
SMOH, WHO
2 1
3
SMoH, WHO, UNICEF
1
1
SMoH, UNFPA, WHO, UNICEF
4 1
5
SMoH, WHO, UNICEF, UNFPA
1
1
WHO, UNICEF, UNFPA
1 3
4
WR WR, SMoH, WHO, UNFPA
1
1
Foro Baranga
NHI NHI
1
1
SMoH
SMoH, SC, WHO, UNICEF, UNFPA 1
1
SMoH, SC, WHO, UNICEF, UNFPA
1 1
2
Habila
NHI NHI
1
1
SC SC, UNICEF, UNFPA, WHO
1
1
SMoH
SMoH
2
2
SMoH, WHO, UNFPA 1
1
SMoH, SC, WHO, UNICEF, UNFPA
1
1
WHO, UNICEF, UNFPA
1
1
Jebel Moon
CONCERN CONCERN, UNICEF, UNFPA
1 3
4
SMoH SMoH, WHO, UNFPA
1
1
Kereinik
IMC IMC, WHO, UNICEF, UNFPA
4
4
ISRA ISRA, WHO, UNFPA
1
1
NHI NHI
1
1
SC SC, UNICEF, UNFPA and WHO
2
2
SMoH
CONCERN, WHO, UNICEF, UNFPA
1
1
SMoH
1 1
2
SMoH, UNICEF, UNFPA
4
4
SMoH, WHO
1 1 1
SMoH,MSF Swiss
1 1
2
SMoH, WHO, UNFPA
1
1
SMoH, WHO, UNFPA, SC 2
2
SMoH. WHO
1
1
WHO, UNICEF, UNFPA
1
1
WR WR, SMoH, WHO, UNFPA
1 3
4
Kulbus
SMoH
COSV, WHO, UNICEF, UNFPA
7
7
SMoH, WHO, SMoH
1
1
SMoH, WHO, UNFPA 1
1
SMoH, WHO, UNICEF, UNFPA
1
1
Sirba
IMC IMC, WHO, UNICEF, UNFPA
1 2
3
NHI NHI
1
1
SMoH
SMoH, UNICEF, UNFPA
1
1
SMoH, WHO
1 1
2
SMoH, UNFPA, WHO, UNICEF
1 1
2
WHO, UNICEF, UNFPA
1
1
WR
WR, SMoH, WHO, UNFPA
1
1
WR, WHO, UNICEF, UNFPA
1
1
Total 5 43 51 1 100

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 48
In addition to SMoH, 14 health partners work in West Darfur. Both El Geneina and Kereinik localities have
the highest presence with 9 partners each as shown in Table 17 above.
5.3.1 NGO health partners
A total of 40 out of the 100 HFs in West Darfur are managed by NGOs. At 15 HFs, IMC (7 PHCCs and 8 BHUs)
manages the majority of HFs in the state. NNGOs ISRA and PORD manage one and two PHCCs respectively.
The other facilities manage between one and thirteen. The Figure 34 below shows the disaggregation of
the HFs managed by the NGOs.
Figure 34: Health partners managing HFs and facility types
5.4 Health Personnel in West Darfur
Health personnel are categorized as HF based staff (health staff working inside the HF) and community
based staff (the community staff working in the community in the same catchment area of the HF (i.e.
village/camp)).
Table 18: Distribution of the health personnel per locality and staff category
Facility based Community based
State Locality MO MA
Nurse
PHO
MW
Vacc
Nut Staff
Lab Person
CHW VV
CHP TBA
VTMW Total
We
st D
arfu
r
Beida 1 9 17 2 30 8 18 2 6 24 6 89 132 344
El Geneina 17 42 58 9 59 36 26 16 28 36 29 120 84 560
Foro Baranga 5 7 18 2 8 7 10 3 4 2 4 3 9 82
Habila 5 7 25 4 17 7 9 3 7 1 7 0 8 100
Jebel Moon 0 4 5 4 14 5 4 1 5 4 5 1 1 53
Kereinik 7 23 52 5 81 37 24 6 27 27 23 78 108 498
Kulbus 1 12 11 9 5 12 10 2 10 19 10 5 14 120
Sirba 2 14 12 0 15 13 6 1 11 14 11 85 41 225
Total 38 118 198 35 229 125 107 34 98 127 95 381 397 1,982
The number of medical personnel working in West Darfur was increased from 1,495 in Q4/ 2016 to 1,982
currently Of these, 8,84 (45%) are facility based, while the remaining 1,098 (55%) are community based.
3
8 5
1
7
1 2 3
2
0
2
4
6
8
10
12
14
16
Concern IMC ISRA PORD SC WR
BHU Mob clinic PHCC

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 49
Kereinik has the highest number of health personnel at 498 followed by El Geneina with 560. While Jebel
Moon locality has the lowest number of staff 53.
As it was in the last quarter, the net 487 increase in medical personnel due to proper data collection done
during Q1-2017, The number of MOs increased by 4, MAs by One, nurses by 5, MWs by 63, Vaccinators by
1, Nutritionist by 19 and lab personnel by one, CHW by 10, VVs by 6, CHPs decreased by 214, TBAs by 344
and VTMW by 251, resulting to a net increase of 487.
Figure 35: Distribution of Medical Officers, Medical Assistants and Nurses by locality
Figure 36: Distribution of Midwives, Village Trained Midwives, and Traditional Birth Attendants by locality
5.4.1 Health Personnel Gap Analysis in West Darfur
Based on the HeRAMS data, gaps in health staffing has been analyzed against the local Health System Standards set by the Sudan’s Ministry of Health.
0
20
40
60
80
100
120
140
Beida El Geneina Foro Baranga Habila Jebel Moon Kereinik Kulbus Sirba
MO MA Nurse
0
50
100
150
200
250
300
Beida El Geneina ForoBaranga
Habila Jebel Moon Kereinik Kulbus Sirba
MW TBA VTMW

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 50
5.4.1.1 Rural Hospitals
In a RHs, the minimum standard set is at least one Medical Officer, one Medical Assistant, at least three nurses, one Midwife, one Vaccinator, one Nutrition staff, one Public Health Office and one Laboratory personnel. This is the bare minimum, more is recommended. Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
The situation in all RHs in West Darfur remains the same as reported in the previous quarter. Of the five
HFs in West Darfur, two RHs (Kereinik and Morni) fall short of the minimum requirement. The gaps are in a
MO for Kerreinik RH and a MW for Morni RH. On the other hand, Forabaranga Town RH is best staffed,
surpassing the set minimum standards.
5.4.1.2 Primary Health Care Centres
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses,
one Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare minimum,
more is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff, Lab. Personnel
PHCCs in West Darfur have various personnel gaps, the biggest of which is the absence of PHO and
laboratory staff. Of the 43 functioning HFs, 72% and 58% don’t have a PHO and laboratory personnel
respectively. In addition, the number of nurses is below the standard (79% of HFs below the standard) but
all the facilities have at least one nurse.
The same facilities five PHCCs (Al Maglis, Ardamta HI, Kereinik, Mornei, Beida and Um Dowain HI) reported
in the last quarter meet the set standard for PHCCs. The rest are functioning with skeleton staff, the worst
of which is Kongi PHCC with only 2 nurse, one vaccinator , Ganderni PHCC with 2 Nurse , one vaccinator and
one Nutrition staff and Um Dalbaa with only two nurses and one vaccinator.
Figure 37: Gap of Health Personnel at PHCC Level-West Darfur
The percentages are calculated out of the total functioning PHCCs (43) in West Darfur
5.4.1.3 Basic Health Units
9%
79%
72%
12%
5%
23%
58%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
MA Nurse PHO MW Vacc Nut Staff LabPersonnel

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 51
The minimum standard set for a BHU is at least one Medical Assistant, one Nurse, one Midwife, one
VTMW, one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
Minimum Standard: MA, Nurse, MW, VTMW, Nutrition staff, Vaccinator
Of the 51 functioning BHUs in West Darfur, 12 meet the minimum to operate as a BHU, they are:- Azerni,
Condebi, Durti, Gokar, Hajar Assal, Rijil Kubri, Zeinah, Door Shari, Kongay, Adawie, and Muli BHUs. The rest
have gaps in one or more of the personnel category.
The biggest gap in BHUs is the absence of nutritional personnel. Twenty-eight (29) or 57% of the 51 BHUs
don’t have a nutritionist. Other gaps were identified in VTMWs, MWs, Nurses and Mas as illustrated in
Figure 38 below.
Furthermore, there gaps are in Abu Zer BHU and Sawani BHU which has only one vaccinator and one
VTMW for both of them . While Buri, and Masmagei BHU are managed by one nurse and one PHO .
Figure 38: Gap of Health Personnel at BHU level - West Darfur
The percentages are calculated out of the total functioning BHUs (51) in West Darfur
5.5 EWARS reporting HFs in West Darfur
EWARS is an essential service for detection of any unusual disease trends and outbreaks of communicable
diseases in Darfur. The table below shows summary of the number of functioning HFs designated under
EWARS per locality.
Table 21: Distribution of functioning HFs reporting under EWARS
State Locality EWARS Designated sites Total HFs in the locality % EWARS
We
st D
arfu
r
Beida 3 6 50%
El Geneina 7 29 24%
Foro Baranga 3 4 75%
Habila 2 7 29%
Jebel Moon 0 5 0%
Kereinik 10 24 42%
Kulbus 1 10 10%
Sirba 4 12 33%
Total 30 97 31%
16% 18%
21%
12%
57%
31%
0%
10%
20%
30%
40%
50%
60%
MA Nurse MW Vacc Nut Staff VTMW

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 52
All localities in West Darfur except Jabel Moon have EWARS designated sites, however, only 31% of the
facilities are EWARS designated sites. Foro Baranga locality has the greatest number of facilities, 75% with
EWARS designated sites.
5.6 Provision of Minimum Basic Health package in West Darfur
The minimum set of services that should be basically provided by any HF, are:
Outpatient services
EPI : routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed
and/or reported), advise/counsel on nutrition & breastfeeding, self-care and family planning,
preventive treatment(s) as appropriate.
Figure 39: Provision of Minimum Basic Health package per locality
The graph above shows the percentage of facilities offering minimum basic health care services in each locality.
83% 83%
75% 71%
20%
70%
60%
83%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Beida El Geneina ForoBaranga
Habila Jebel Moon Kereinik Kulbus Sirba
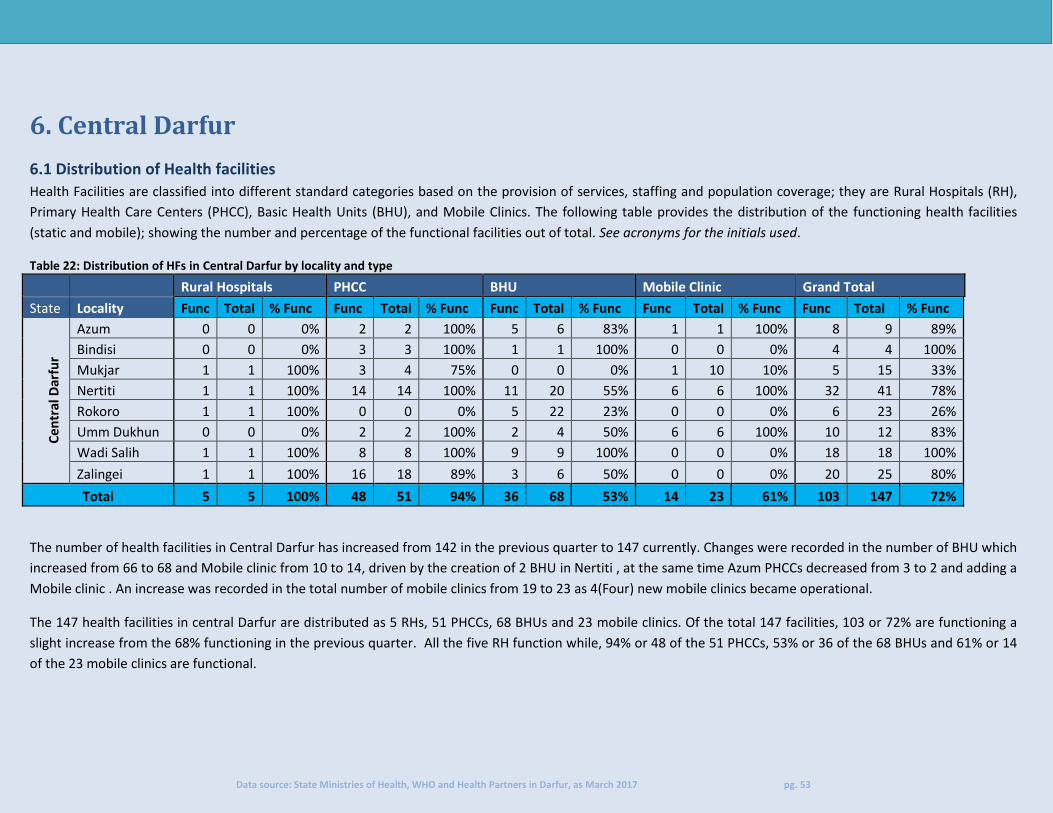
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 53
6. Central Darfur
6.1 Distribution of Health facilities
Health Facilities are classified into different standard categories based on the provision of services, staffing and population coverage; they are Rural Hospitals (RH),
Primary Health Care Centers (PHCC), Basic Health Units (BHU), and Mobile Clinics. The following table provides the distribution of the functioning health facilities
(static and mobile); showing the number and percentage of the functional facilities out of total. See acronyms for the initials used.
Table 22: Distribution of HFs in Central Darfur by locality and type
Rural Hospitals PHCC BHU Mobile Clinic Grand Total
State Locality Func Total % Func Func Total % Func Func Total % Func Func Total % Func Func Total % Func
Ce
ntr
al D
arfu
r
Azum 0 0 0% 2 2 100% 5 6 83% 1 1 100% 8 9 89%
Bindisi 0 0 0% 3 3 100% 1 1 100% 0 0 0% 4 4 100%
Mukjar 1 1 100% 3 4 75% 0 0 0% 1 10 10% 5 15 33%
Nertiti 1 1 100% 14 14 100% 11 20 55% 6 6 100% 32 41 78%
Rokoro 1 1 100% 0 0 0% 5 22 23% 0 0 0% 6 23 26%
Umm Dukhun 0 0 0% 2 2 100% 2 4 50% 6 6 100% 10 12 83%
Wadi Salih 1 1 100% 8 8 100% 9 9 100% 0 0 0% 18 18 100%
Zalingei 1 1 100% 16 18 89% 3 6 50% 0 0 0% 20 25 80%
Total 5 5 100% 48 51 94% 36 68 53% 14 23 61% 103 147 72%
The number of health facilities in Central Darfur has increased from 142 in the previous quarter to 147 currently. Changes were recorded in the number of BHU which
increased from 66 to 68 and Mobile clinic from 10 to 14, driven by the creation of 2 BHU in Nertiti , at the same time Azum PHCCs decreased from 3 to 2 and adding a
Mobile clinic . An increase was recorded in the total number of mobile clinics from 19 to 23 as 4(Four) new mobile clinics became operational.
The 147 health facilities in central Darfur are distributed as 5 RHs, 51 PHCCs, 68 BHUs and 23 mobile clinics. Of the total 147 facilities, 103 or 72% are functioning a
slight increase from the 68% functioning in the previous quarter. All the five RH function while, 94% or 48 of the 51 PHCCs, 53% or 36 of the 68 BHUs and 61% or 14
of the 23 mobile clinics are functional.

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 54
6.2 Management of health facilities
Management of health facilities means the primary focal entity who takes charge of admission and providing
services to the patients. The below graph shows the respective entities that manage the health facilities.
Figure 40: Distribution of HFs by type and management - Central Darfur
Of the functional 103 HFs in Central Darfur, 43 are management by SMoH, 49 by NGOs and 11 by the NHI
shown figure 40 above. As compared to the previous quarter, changes in management only occurred in HFs
managed by NGOs. the PHCCs managed by NGOs are 29 same as the previous Quarter . In BHUs, the number
of HFs managed by NGOs increased from 3 (three) to 7 (seven) as compared to the last quarter. In Mobile
clinics, the number increased from 9 to 13, mainly in Nertiti locality where WR started operating 3 (Three)
mobile clinics.
Figure 41: Percentage of HFs by management - Central Darfur
5
12
25
1
43
7
4
11
29
7
13
49
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RH PHC BHU Mob clinic Total
SMoH NHI NGOs
23%
42%
49%
77%
58% 51%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Q1/Q2 2016 Q3/Q4 2016 Q1 2017
NGOs Govt(SMoH and NHI)
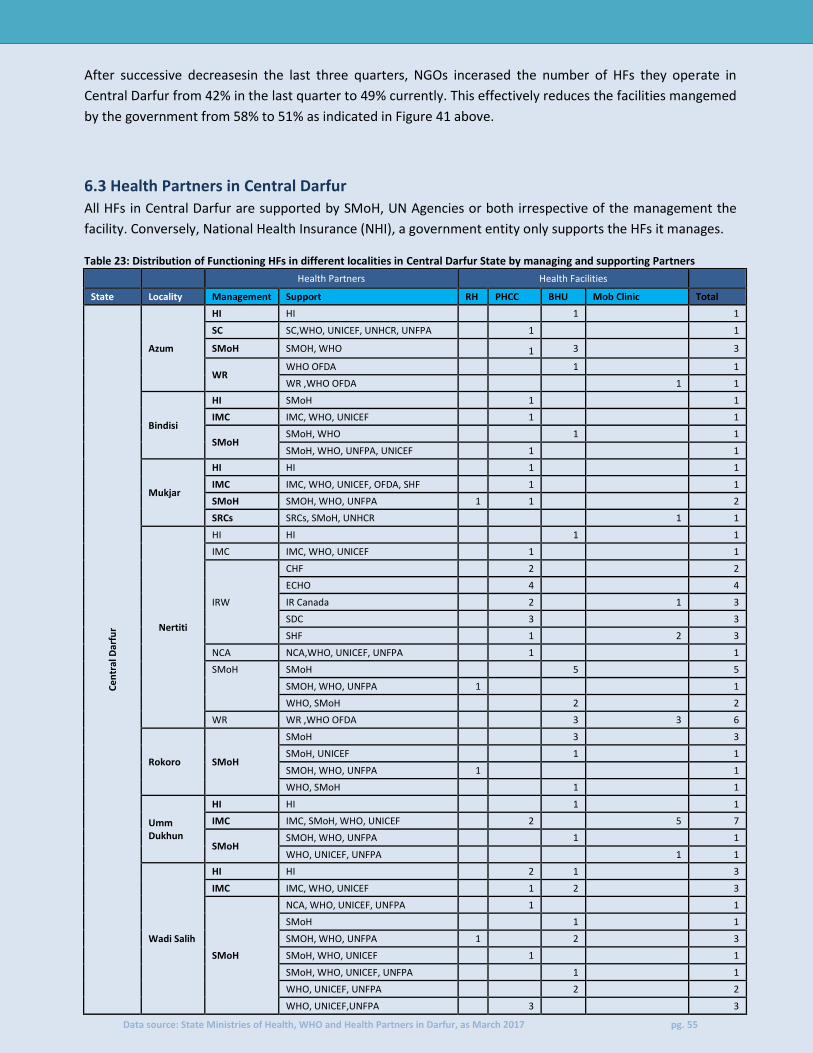
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 55
After successive decreasesin the last three quarters, NGOs incerased the number of HFs they operate in
Central Darfur from 42% in the last quarter to 49% currently. This effectively reduces the facilities mangemed
by the government from 58% to 51% as indicated in Figure 41 above.
6.3 Health Partners in Central Darfur All HFs in Central Darfur are supported by SMoH, UN Agencies or both irrespective of the management the
facility. Conversely, National Health Insurance (NHI), a government entity only supports the HFs it manages.
Table 23: Distribution of Functioning HFs in different localities in Central Darfur State by managing and supporting Partners
Health Partners Health Facilities
State Locality Management Support RH PHCC BHU Mob Clinic Total
Ce
ntr
al D
arfu
r
Azum
HI HI 1 1
SC SC,WHO, UNICEF, UNHCR, UNFPA 1 1
SMoH SMOH, WHO 1 3 3
WR WHO OFDA 1 1
WR ,WHO OFDA 1 1
Bindisi
HI SMoH 1 1
IMC IMC, WHO, UNICEF 1 1
SMoH SMoH, WHO 1 1
SMoH, WHO, UNFPA, UNICEF 1 1
Mukjar
HI HI 1 1
IMC IMC, WHO, UNICEF, OFDA, SHF 1 1
SMoH SMOH, WHO, UNFPA 1 1 2
SRCs SRCs, SMoH, UNHCR 1 1
Nertiti
HI HI 1 1
IMC IMC, WHO, UNICEF 1 1
IRW
CHF 2 2
ECHO 4 4
IR Canada 2 1 3
SDC 3 3
SHF 1 2 3
NCA NCA,WHO, UNICEF, UNFPA 1 1
SMoH SMoH 5 5
SMOH, WHO, UNFPA 1 1
WHO, SMoH 2 2
WR WR ,WHO OFDA 3 3 6
Rokoro SMoH
SMoH 3 3
SMoH, UNICEF 1 1
SMOH, WHO, UNFPA 1 1
WHO, SMoH 1 1
Umm Dukhun
HI HI 1 1
IMC IMC, SMoH, WHO, UNICEF 2 5 7
SMoH SMOH, WHO, UNFPA 1 1
WHO, UNICEF, UNFPA 1 1
Wadi Salih
HI HI 2 1 3
IMC IMC, WHO, UNICEF 1 2 3
SMoH
NCA, WHO, UNICEF, UNFPA 1 1
SMoH 1 1
SMOH, WHO, UNFPA 1 2 3
SMoH, WHO, UNICEF 1 1
SMoH, WHO, UNICEF, UNFPA 1 1
WHO, UNICEF, UNFPA 2 2
WHO, UNICEF,UNFPA 3 3
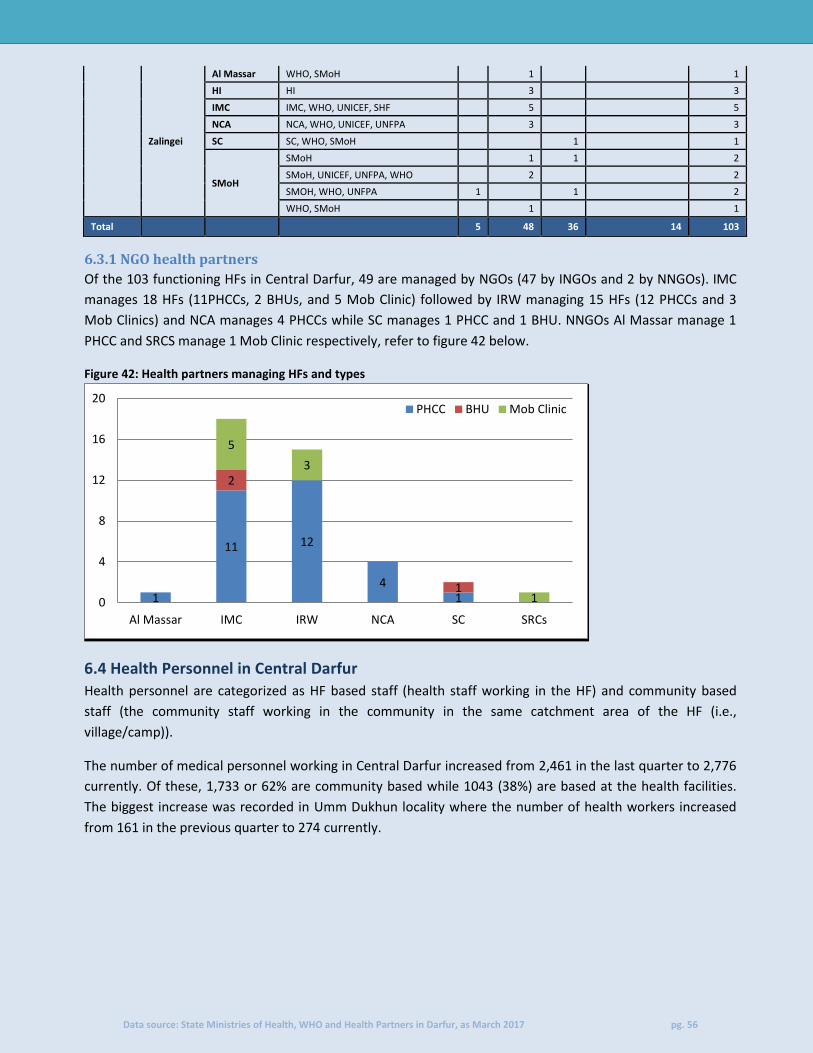
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 56
Zalingei
Al Massar WHO, SMoH 1 1
HI HI 3 3
IMC IMC, WHO, UNICEF, SHF 5 5
NCA NCA, WHO, UNICEF, UNFPA 3 3
SC SC, WHO, SMoH 1 1
SMoH
SMoH 1 1 2
SMoH, UNICEF, UNFPA, WHO 2 2
SMOH, WHO, UNFPA 1 1 2
WHO, SMoH 1 1
Total 5 48 36 14 103
6.3.1 NGO health partners
Of the 103 functioning HFs in Central Darfur, 49 are managed by NGOs (47 by INGOs and 2 by NNGOs). IMC
manages 18 HFs (11PHCCs, 2 BHUs, and 5 Mob Clinic) followed by IRW managing 15 HFs (12 PHCCs and 3
Mob Clinics) and NCA manages 4 PHCCs while SC manages 1 PHCC and 1 BHU. NNGOs Al Massar manage 1
PHCC and SRCS manage 1 Mob Clinic respectively, refer to figure 42 below.
Figure 42: Health partners managing HFs and types
6.4 Health Personnel in Central Darfur
Health personnel are categorized as HF based staff (health staff working in the HF) and community based
staff (the community staff working in the community in the same catchment area of the HF (i.e.,
village/camp)).
The number of medical personnel working in Central Darfur increased from 2,461 in the last quarter to 2,776
currently. Of these, 1,733 or 62% are community based while 1043 (38%) are based at the health facilities.
The biggest increase was recorded in Umm Dukhun locality where the number of health workers increased
from 161 in the previous quarter to 274 currently.
1
11 12
4 1
2
1
5
3
1 0
4
8
12
16
20
Al Massar IMC IRW NCA SC SRCs
PHCC BHU Mob Clinic

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 57
Table 23: Distribution of the health personnel per locality and staff category
Facility based Community based
State Locality MO MA Nurse PHO MW
Vacc
Nut Staff
Lab Person
CHW VV
CHP
TBA
VTMW Total
Ce
ntr
al D
arfu
r
Azum 1 9 14 2 15 10 5 2 6 14 32 21 13 144
Bindisi 0 5 14 1 6 17 4 4 12 36 3 33 3 138
Mukjar 2 8 12 3 7 15 18 3 1 65 28 42 10 214
Nertiti 4 33 48 3 43 31 33 18 21 26 228 187 110 785
Rokoro 1 7 11 0 10 7 0 1 9 12 0 0 5 63
Umm Dukhun 1 9 22 1 29 14 61 1 4 2 8 120 4 276
Wadi Salih 3 17 70 4 48 24 28 7 20 34 132 63 22 472
Zalingei 12 35 105 3 45 26 38 13 78 42 71 177 39 684
Total 24 123 296 17 203 144 187 49 151 231 502 643 206 2,776
Nertiti locality has the highest while Rokoro locality has the lowest number of staff members in all categories
as depicted in Table 23 above.
Figure 43: Distribution of Medical Officers, Medical Assistants and Nurses by locality
Figure 44: Distribution of Midwives, Village Trained Midwives, and Traditional Birth Attendants by locality
0
20
40
60
80
100
120
140
160
Azum Bindisi Mukjar Nertiti Rokoro UmmDukhun
Wadi Salih Zalingei
MO MA Nurse
0
50
100
150
200
250
300
350
400
Azum Bindisi Mukjar Nertiti Rokoro UmmDukhun
Wadi Salih Zalingei
MW TBA VTMW

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 58
6.4.1 Health Personnel Gap Analysis in Central Darfur
Based on the HeRAMS data, gaps in health staffing has been analyzed against the local Health System standards set by the Sudan’s Ministry of Health. 6.4.1.1 Rural Hospitals
In a Rural hospital, the minimum standard set is at least one Medical Officer, one Medical Assistant, at least three nurses, one Midwife, one Vaccinator, one Nutrition staff, one Public Health Office and one Laboratory personnel. This is the bare minimum, more is recommended. Minimum Standard: MO+ MA+ 3 nurses or more + MW+ Vaccinator+ Nutrition staff + PHO + Lab. Personnel
Based on HeRAMS data, four (4) of the 5 RHs in Central Darfur meet this minimum standards. Zalingei RH
performs better that all RHs in the state because it has at least five folds (12 MOs, 35 MAs, 105 Nurses, 45
MWs, 26 Vaccinators, 3 PHOs, 38 Nutrition Staff and 13 laboratory personnel) more than the minimum
standard.
Golo RH is the only facility which doesn’t meet the bare standard; the facility lacks a PHO and a nutrition
staff.
6.4.1.2 Primary Health Care Centres
The minimum standard set for a PHCC is at least one Medical Officer, one Medical Assistant, two Nurses, one
Midwife, one Vaccinator, one Nutrition staff and one Laboratory personnel. This is the bare minimum, more
is recommended.
Minimum Standard: MA, 2 Nurse or more, PHO, MW, Vaccinator, Nutrition staff, Lab. Personnel
PHCCs in Central Darfur have various personnel gaps, the biggest of which is the absence of a PHO and
laboratory personnel. Only sex of the facilities has a PHO and 24 have Laboratory personnel.
Of the 48 functioning PHCCs, Only Deleig, PHCC have the required number of staff meeting the minimum
standard above.
Medical Assistants are available in all the PHCCs except Kabar and Moradaf PHCCs. Mukjar has four MAs.
Figure 45: Gap of Health Personnel at PHCC Level – Central Darfur
The percentages are calculated out of the total functioning PHCCs (48) in Central Darfur
4%
44%
87%
2% 4% 10%
48%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MA Nurse PHO MW Vacc Nut Staff LabPersonnel

Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 59
6.4.1.3 Basic Health Units
The minimum standard set for a BHU is at least one Medical Assistant, one Nurses, one Midwife, one VTMW,
one Nutrition staff and one vaccinator. This is the bare minimum, more is recommended.
Minimum Standard: MA, Nurse, MW, VTMW, Nutrition staff, Vaccinator
As it was in the previous quarter, the biggest gap in BHUs still remains the absence of nutritional personnel.
Only 9 of the 33 functioning BHUs have a nutritionist. Furthermore, the absence of VTMW has come up this
quarter, only 10 BHUs have one VTMW.
Of the 36 functioning BHUs, Al Salam, Abdowi, Noor El salaam, Mali, Nertiti Center8, Jabal Ahmer and Ordi
meet the minimum requirement for a BHU.
The table below shows the gap in each speciality in BHUs.
Figure 46: Gap of Health Personnel at BHU level - Central Darfur
The percentages are calculated out of the total functioning BHUs (36) in Central Darfur
6.5 EWARS reporting HFs in Central Darfur
EWARS is an essential service for detection of any outbreaks of communicable diseases. The table below
shows summary of the number of functioning HFs designated under EWARS in Central Darfur per locality.
Table 26: Distribution of functioning HFs reporting under EWARS
State Locality EWARS % EWARS Total HFs
Cen
tral
Dar
fur
Azum 2 25% 8
Bindisi 2 50% 4
Mukjar 1 20% 5
Nertiti 2 6% 32
Rokoro 0 0% 6
Umm Dukhun 0 0% 10
Wadi Salih 6 33% 18
Zalingei 11 55% 20
Total 24 23% 103
8% 6%
14%
8%
64%
28%
0%
10%
20%
30%
40%
50%
60%
70%
MA Nurse MW Vacc Nut Staff VTMW
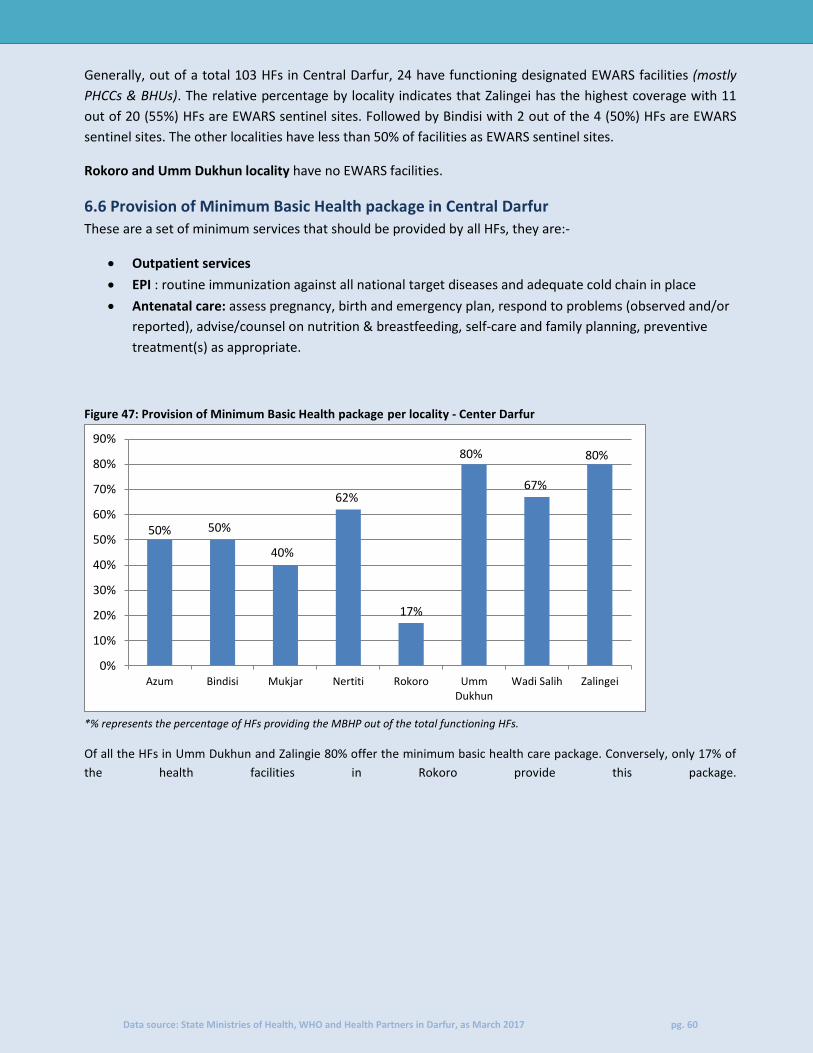
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 60
Generally, out of a total 103 HFs in Central Darfur, 24 have functioning designated EWARS facilities (mostly
PHCCs & BHUs). The relative percentage by locality indicates that Zalingei has the highest coverage with 11
out of 20 (55%) HFs are EWARS sentinel sites. Followed by Bindisi with 2 out of the 4 (50%) HFs are EWARS
sentinel sites. The other localities have less than 50% of facilities as EWARS sentinel sites.
Rokoro and Umm Dukhun locality have no EWARS facilities.
6.6 Provision of Minimum Basic Health package in Central Darfur
These are a set of minimum services that should be provided by all HFs, they are:-
Outpatient services
EPI : routine immunization against all national target diseases and adequate cold chain in place
Antenatal care: assess pregnancy, birth and emergency plan, respond to problems (observed and/or
reported), advise/counsel on nutrition & breastfeeding, self-care and family planning, preventive
treatment(s) as appropriate.
Figure 47: Provision of Minimum Basic Health package per locality - Center Darfur
*% represents the percentage of HFs providing the MBHP out of the total functioning HFs.
Of all the HFs in Umm Dukhun and Zalingie 80% offer the minimum basic health care package. Conversely, only 17% of
the health facilities in Rokoro provide this package.
50% 50%
40%
62%
17%
80%
67%
80%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Azum Bindisi Mukjar Nertiti Rokoro UmmDukhun
Wadi Salih Zalingei
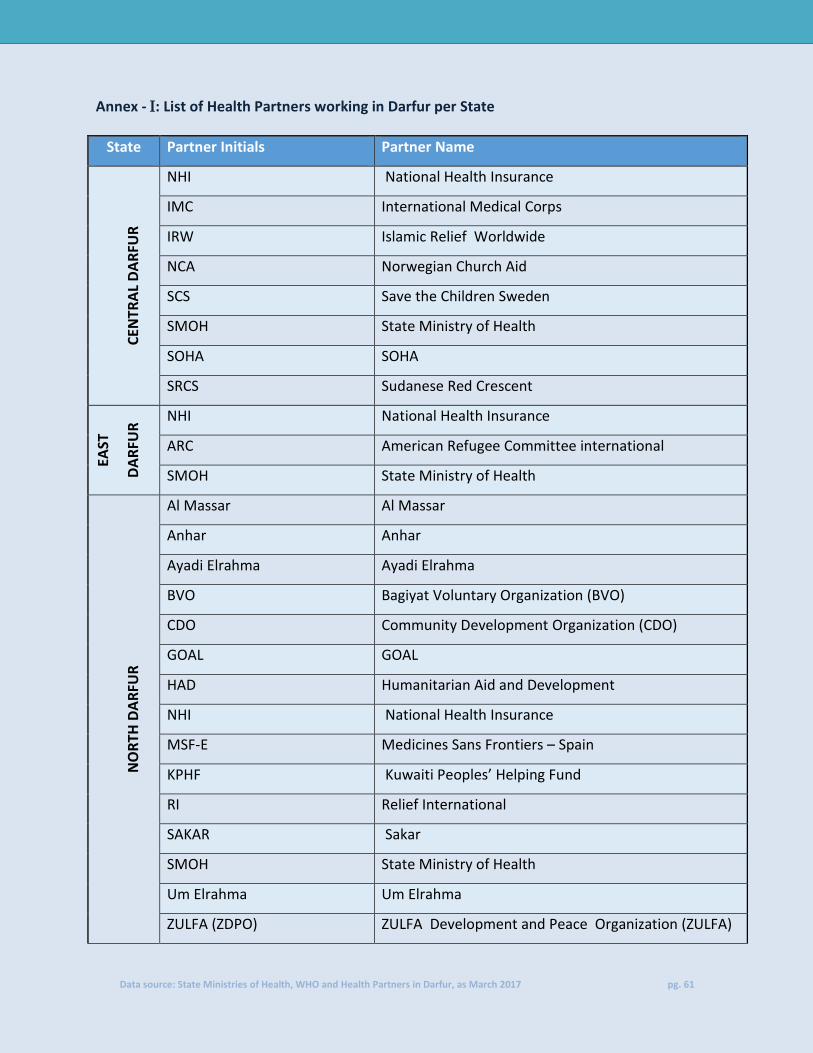
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 61
Annex - : List of Health Partners working in Darfur per State
State Partner Initials Partner Name C
ENTR
AL
DA
RFU
R
NHI National Health Insurance
IMC International Medical Corps
IRW Islamic Relief Worldwide
NCA Norwegian Church Aid
SCS Save the Children Sweden
SMOH State Ministry of Health
SOHA SOHA
SRCS Sudanese Red Crescent
EAST
DA
RFU
R NHI National Health Insurance
ARC American Refugee Committee international
SMOH State Ministry of Health
NO
RTH
DA
RFU
R
Al Massar Al Massar
Anhar Anhar
Ayadi Elrahma Ayadi Elrahma
BVO Bagiyat Voluntary Organization (BVO)
CDO Community Development Organization (CDO)
GOAL GOAL
HAD Humanitarian Aid and Development
NHI National Health Insurance
MSF-E Medicines Sans Frontiers – Spain
KPHF Kuwaiti Peoples’ Helping Fund
RI Relief International
SAKAR Sakar
SMOH State Ministry of Health
Um Elrahma Um Elrahma
ZULFA (ZDPO) ZULFA Development and Peace Organization (ZULFA)
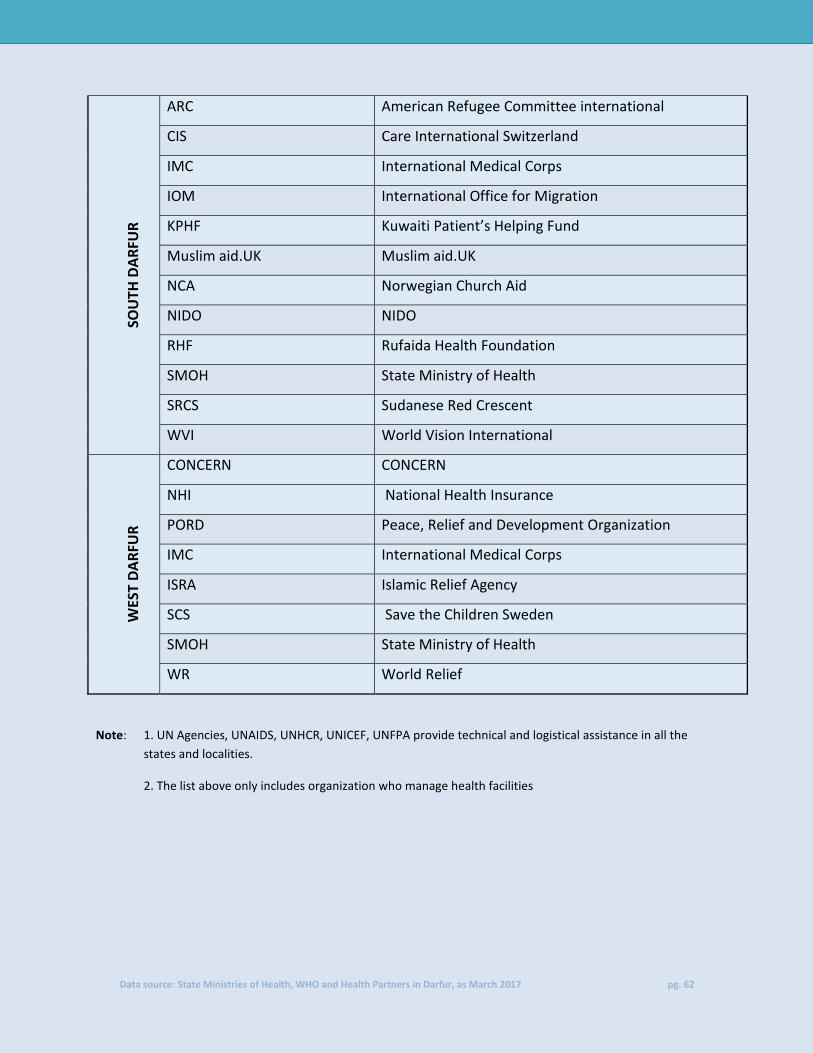
Data source: State Ministries of Health, WHO and Health Partners in Darfur, as March 2017 pg. 62
SOU
TH D
AR
FUR
ARC American Refugee Committee international
CIS Care International Switzerland
IMC International Medical Corps
IOM International Office for Migration
KPHF Kuwaiti Patient’s Helping Fund
Muslim aid.UK Muslim aid.UK
NCA Norwegian Church Aid
NIDO NIDO
RHF Rufaida Health Foundation
SMOH State Ministry of Health
SRCS Sudanese Red Crescent
WVI World Vision International
WES
T D
AR
FUR
CONCERN CONCERN
NHI National Health Insurance
PORD Peace, Relief and Development Organization
IMC International Medical Corps
ISRA Islamic Relief Agency
SCS Save the Children Sweden
SMOH State Ministry of Health
WR World Relief
Note: 1. UN Agencies, UNAIDS, UNHCR, UNICEF, UNFPA provide technical and logistical assistance in all the
states and localities.
2. The list above only includes organization who manage health facilities







![[HeRAMS ] - HumanitarianResponse...HeRAMS (Health Resources Availability Mapping System) is a standardized approach supported by a software-based platform that aims at strengthening](https://static.fdocuments.us/doc/165x107/5f16569e89c56e2c29038bcf/herams-humanitarianresponse-herams-health-resources-availability-mapping.jpg)