Health Reform and Primary Care Mona Sarfaty, MD MPH Department of Family and Community Medicine...
37
Health Reform and Primary Care Mona Sarfaty, MD MPH Department of Family and Community Medicine Jefferson School of Population Health November 2010
-
Upload
christopher-shaw -
Category
Documents
-
view
218 -
download
0
Transcript of Health Reform and Primary Care Mona Sarfaty, MD MPH Department of Family and Community Medicine...
Health Reform and Primary Care
Mona Sarfaty, MD MPH
Department of Family and Community Medicine
Jefferson School of Population Health
November 2010
Presenter Disclosures
The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Mona Sarfaty, MD MPH
No relationships to disclose

Outline of Concepts
• Primary Care
–History
–Definition and characterisics
–Benefits of primary care
• Primary Care in Crisis
• Reform on Primary Care
• Patient Centered Medical Home (Demonstrations)

History: Primary Care and U.S. Health Care
• No primary care until the 1960’s
• Post war growth of specialties
• “Primary care” as area of concentration (1960’s)
–Family Medicine (AAFP, STFM)
–General Internal Medicine (SGIM)
–Primary Care Pediatrics

Simple Definitions Simple Definitions of Primary Care (web)of Primary Care (web)
• Primary care is a term used for the activity of a health care provider who acts as a first point of consultation for all patients. Continuity of care is a key characteristic of primary care.
• The level of care that encompasses routine care of individuals with common health problems and chronic illnesses that can be managed on an outpatient basis.
• Family health services provided by doctors, dentists, pharmacists, optometrists and ophthalmic medical practitioners, practice nurses, health visitors and allied health professionals

Characteristics (Traditional)
First Contact AccessibilityUse by people for each new problem
Longitudinality/Continuity
Relationship between a provider and its populationUse by people over time regardless of the type of problem; person-focused character of provider/patient relationship
Comprehensiveness Broad range of services Recognition of situations where services are needed
Coordination Mechanism for achieving continuity Recognition of problems that require follow-up
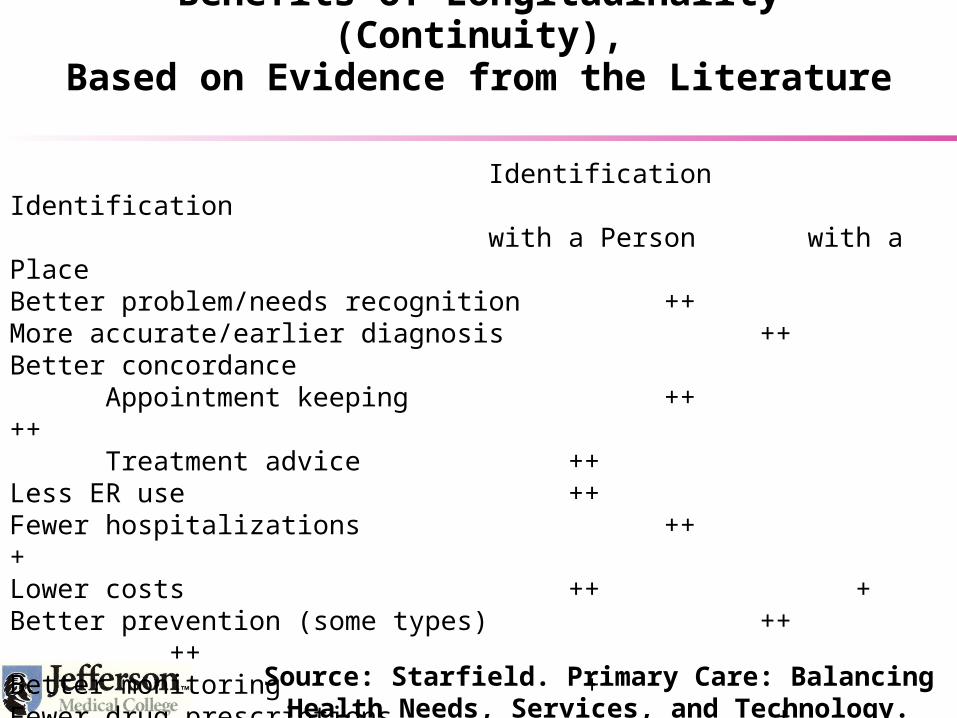
Identification Identificationwith a Person with a Place
Better problem/needs recognition ++More accurate/earlier diagnosis ++Better concordance
Appointment keeping ++ ++Treatment advice ++
Less ER use ++Fewer hospitalizations ++ +Lower costs ++ +Better prevention (some types) ++ ++Better monitoring +Fewer drug prescriptions +Less unmet needs ++ +Increased satisfaction ++
++ Source: Starfield. Primary Care: Balancing Health Needs, Services, and Technology. Oxford U. Press, 1998.
Benefits of Longitudinality (Continuity),Based on Evidence from the Literature

Primary Care: Quality and Cost*
• Within the United States, adults with a primary care physician rather than a specialist had 33 percent lower costs of care and were 19 percent less likely to die.
• In the United States, an increase of just one primary care physician is associated with 1.44 fewer deaths per 10,000 persons.
• In the United States, each additional primary care physician per 10,000 persons is associated with a decrease in mortality rate of 3 to 10 percent.
*Barbara Starfield, APHA.
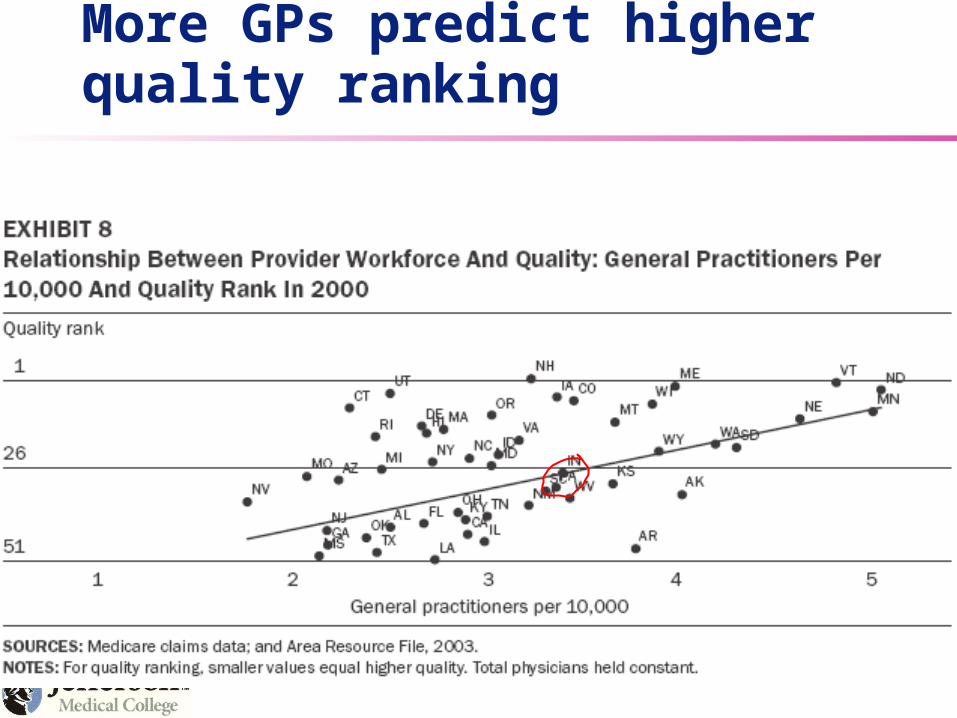
More GPs predict higher quality ranking

GPs are associated with less spending
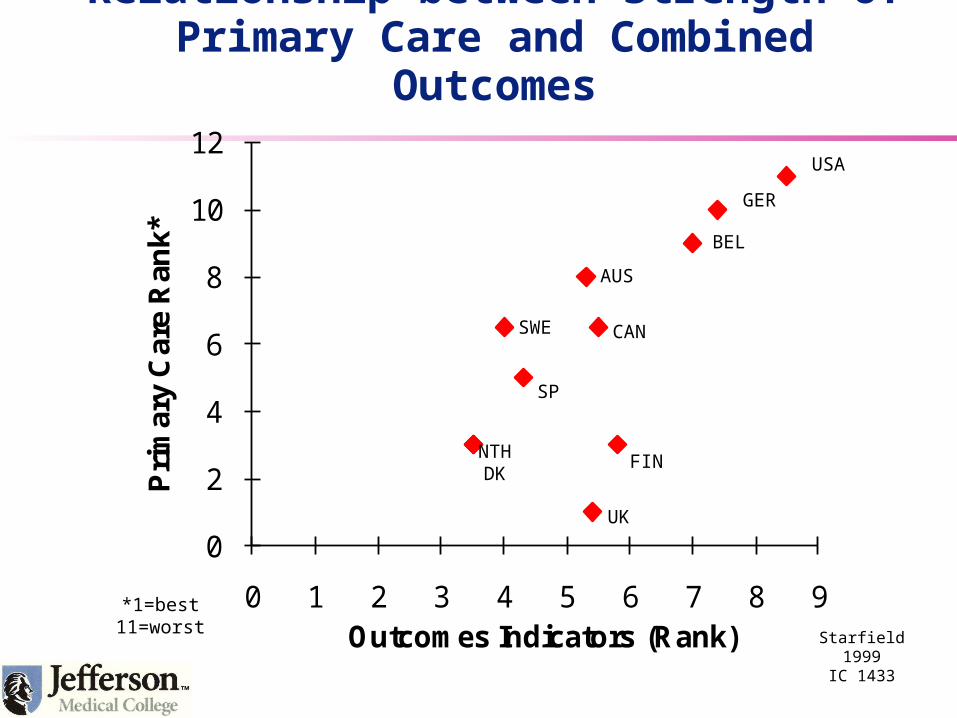
Relationship between Strength of Primary Care and Combined Outcomes
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7 8 9
Pri
mar
y C
are
Ran
k*
Outcomes Indicators (Rank)
USA
GER
BEL
AUS
SWE
SP
CAN
FIN
UK
NTHDK
*1=best11=worst
Starfield 1999IC 1433

0123456789
101112
0 1 2 3 4 5 6 7 8 9 10 11 12 13
System Characteristics (Rank*)
Pra
ctic
e C
ha
ract
eri
stic
s (R
an
k*)
UK
NTH
SP
FIN CANAUS
SWE JAP
GER FRBEL
US
DK
*Best level of health indicator is ranked 1; worst is ranked 13; thus, lower average ranks indicate better performance.
Based on data in Starfield & Shi, Health Policy 2002; 60:201-18.
U.S. Rank: Characteristics Facilitating Primary Care, 1990s

Specific Outcome Example: Coordination Problems with Medical Tests
17 16 1520
710
14
21
3235
27 28
21
33 32
45
0
20
40
60
AUS CAN FR GER NETH NZ UK US
1 or 2 doctors 4 or more doctors
Base: Adults with any chronic condition
Percent reported any medical test/record coordination problems* in past 2 years
Data collection: Harris Interactive, Inc.Source: 2008 Commonwealth Fund International Health Policy Survey of Sicker Adults.
* Test results/medical records not available at time of appointment and/or doctors ordered medical test that had already been done.

What We Already Know
• Improving health outcomes (improving effectiveness)
• Keeping costs manageable (improving efficiency)
A primary care oriented system is important for
Starfield 09/05PC 3316

From the New England Journal of Medicine*
•
U.S. primary care is in crisis. The ranks of primary care physicians are thinning, with many burning out and trainees shunning primary care fields.
• In a roundtable discussion moderated by Dr. Thomas Lee, four experts — Drs. Thomas Bodenheimer, Allan Goroll, Barbara Starfield, and Katharine Treadway — explore the crisis, as well as possible solutions for training, practice, compensation, and systemic change.
• View the video of this roundtable discussion and contribute your thoughts
* 11/13/08 on the web

Primary Care System in Crisis
• Fragmented uncoordinated patient care
• Inconsistent delivery of evidence based care, especially chronic & preventive care
• Misaligned reimbursement system
• Increased expectations of reimbursers
• Shrinking primary care workforce

Workforce
• The number of US medical students choosing primary care careers has declined precipitously
• Factors discouraging recruitment/retention
–Low compensation
–Rising malpractice premiums
–Professional isolation (in many settings)
–Limited time off (in many settings)
• The Affordable Care Act
• Provisions to Address Primary Care

ACA Provisions Would Help Increase the Primary Care Workforce
• Scholarships and loan repayment
• Increased federal matching to state Medicaid programs
• Increased payment to rural clinicians
• Requires state Medicaid plans to pay primary care clinicians no less than 100% of Medicare rate for 2013 and 2014
Practitioner Specific Provisions
• Creates an incentive payment program for primary care providers with incentive payments equal to 10% of a "primary care practitioner's" allowed charges under Medicare Part B for primary care services on or after Jan. 1, 2011, before Jan. 1, 2016.
• To qualify, primary care services must account for at least 60 percent of an individual professional's allowed charges under Medicare Part B. CMS is required to make payments to qualifying physicians on a quarterly basis.
Primary Care Providers in the ACA
• In addition, the law specifies that eligibility for the primary care incentive payment is not related to any other payment Congress has authorized. For example, family physicians practicing in federally designated Health Professional Shortage Areas are eligible for a separate 10 percent bonus payment, as well as the primary care incentive payment.
Some 2013 Provisions Increase Access to Primary Care
• Doubles the size of the community health center program nationwide
• Expansions of Insurance Coverage
• Through consumer protections
–Eliminates exclusions based on pre-existing conditions
–Eliminates annual limits

2015: One More Provision Addressing Quality and Cost
• Physician payment tied to quality:
higher quality higher payment
lower quality lower payment
Adapted from http://www.healthcare.gov/law/about/order/byyear.html

Q: How can primary care physicians improve quality?
A: 1.. Trying harder to the same think is foolish. Redesign is needed.
2. The Patient-Centered Medical Home (PCMH) has emerged as the leading strategy around which primary care will be redesigned.
A Remedy
Patient Centered
Medical Home

Patient Centered Medical Home
• •
• Original concepts developed in 1980s by American Academy Pediatrics (AAP) as “medical home”• Children with special needs• State level demos of BMCH (involved family/community)
• Future of family medicine project, AAFP adapted and focused on the “personal medical home”
• ACP put Chronic Care elements into “advanced” medical home.” • Crossing the Quality Chasm by IOM: “the system of care should
revolve around the patient, respect patient preferences and put the patient in control.”
*ACP, AAFP, AAP and AOA. Joint Principals of the Patient-Centered Medical Home, March 2007.

The Patient-Centered Medical Home:Principles of Four 1º Care Societies
• Personal Physician
• Whole person orientation
• Coordinated and integrated care
• Safe and high-quality care (e.g., evidenced-based medicine, appropriate use of HIT, continuous QI)
• Enhanced access to care
• Payment that recognizes the added value provided to patients who have a patient-centered medical home
ACP, AAFP, AAP and AOA. Joint Principals of the Patient-Centered Medical Home, March 2007. ( Patient Centered Primary Care Collaborative: pcpccc.net)

PCPCC Payment ModelMay 2007
Key physician and practice accountabilities/ value added
services and tools
Proactively work to keep patients healthy and manage existing illness or conditions
Coordinate patient care among an organized team of health
care professionals
Utilize systems at the practice level to achieve higher quality of
care and better outcomes
Focus on whole person care for their patients (including
behavioral health)
Pe
rform
ance S
tand
ards
Incentiv
es
Incentives
Incentives
16
28


EVIDENCE OF COST SAVINGS & QUALITY IMPROVEMENT
Commonwealth Fund has reported:
• A medical home can reduce or even eliminate racial and ethnic disparities in access and quality for insured persons.
Denmark has organized its entire health care system around patient-centered medical homes, achieving the highest patient satisfaction ratings in the world. Denmark has among the lowest per capita health expenditures and highest primary care rankings.
Center for Evaluative Clinical Sciences at Dartmouth, states in the US relying more on primary care have:
•lower Medicare spending, lower resource inputs, lower utilization, and better quality of care.
30
“Amidst the debate about health care reform, there appears to be near unanimity around the fact that a reformed U.S. health care system requires at it’s foundation a robust system of primary care.”
Landon BE, Gill JM, Antonelli RC, Rich EL, J. Gen Int Med 25(6) 581-3
Patient Centered Medical Home in Government
• Increasingly realized that a strong primary care system is foundational to achieving a high quality accessible efficient and affordable health care for all Americans.
–David Meyer, AHRQ

The Patient-Centered Primary Care Collaborative
ACP
Providers 333,000
primary carePurchasers –
Most of the Fortune 500
Payers Patients
AAP AAFP AOA
ABIM ACC
ACOI AHI
IBM Ohio
General Electric
FedEx
Microsoft
Dow
Merck & Co.
Business Coalitions
BCBSA United
Aetna
CIGNA
Humana
WellPoint
Kaiser Permanente
AARP AFL-CIO
National Consumers League
SEIU Foundation for Informed
Decision Making
Examples of Broad Stakeholder Support & Participation
The Patient-Centered
Medical Home 80 Million lives
33
Geisinger
Iowa

State Initiatives to Advance Medical State Initiatives to Advance Medical HomesHomes
in Medicaid/SCHIPin Medicaid/SCHIP
= Identified to have a medical home initiative
Source: National Academy for State Health Policy State Scan, November
200834
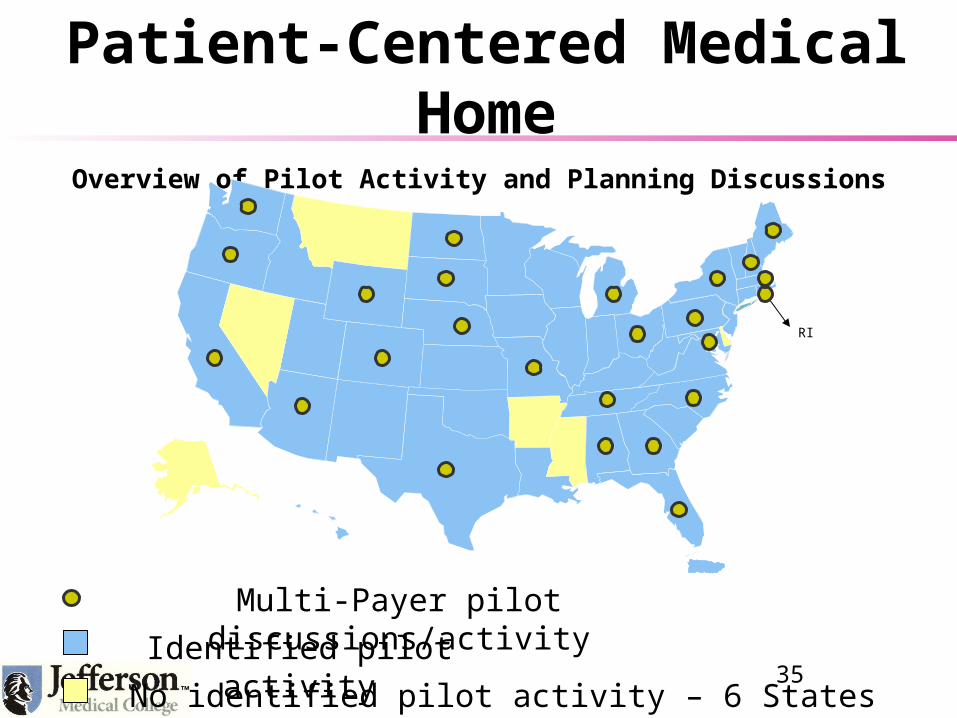
Patient-Centered Medical HomeOverview of Pilot Activity and Planning Discussions
RI
Multi-Payer pilot discussions/activity
Identified pilot activity
No identified pilot activity – 6 States35

Health Reform and the Medical Home
• Federal government also believes the the PCMH model is a basis for achieving the health services that are needed
• Most activity is at AHRQ but there is an interagency working group that is focused on how to advance the PCMH concept.
Conclusion: Parallel Trends
• The progress achieved by Health Care Reform will require a reinvented primary care system.
• The patient centered medical home is an effort to reinvent that system.
• Several other elements will be crucial to the success of the PCMH
–Payment Reform – better incentives (FFS –NOT)
– Information Technology (EMR) (in ARRA)
–Workforce Development (in ACA)