Health policy responses to the financial crisis in Europe · financial crisis in the European...
132
POLICY SUMMARY 5 Health policy responses to the financial crisis in Europe Philipa Mladovsky, Divya Srivastava, Jonathan Cylus, Marina Karanikolos, Tamás Evetovits, Sarah Thomson, Martin McKee
Transcript of Health policy responses to the financial crisis in Europe · financial crisis in the European...

POLICY SUMMARY 5
Health policyresponses to thef inancial crisis in Europe
Philipa Mladovsky, Divya Srivastava,Jonathan Cylus, Marina Karanikolos,Tamás Evetovits, Sarah Thomson,Martin McKee

© World Health Organization 2012 and World HealthOrganization, on behalf of the European Observatoryon Health Systems and Policies 2012
Address requests about publications of the WHORegional Office for Europe to:
PublicationsWHO Regional Office for EuropeScherfigsvej 8DK-2100 Copenhagen Ø, Denmark
Alternatively, complete an online request form fordocumentation, health information, or for permissionto quote or translate, on the Regional Office web site(http://www.euro.who.int/pubrequest).
All rights reserved. The Regional Office for Europe ofthe World Health Organization welcomes requests forpermission to reproduce or translate its publications,in part or in full.
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part ofthe World Health Organization concerning the legalstatus of any country, territory, city or area or of itsauthorities, or concerning the delimitation of itsfrontiers or boundaries. Dotted lines on mapsrepresent approximate border lines for which theremay not yet be full agreement.
The mention of specific companies or of certainmanufacturers’ products does not imply that they are endorsed or recommended by the World HealthOrganization in preference to others of a similarnature that are not mentioned. Errors and omissionsexcepted, the names of proprietary products aredistinguished by initial capital letters.
All reasonable precautions have been taken by theWorld Health Organization to verify the informationcontained in this publication. However, the publishedmaterial is being distributed without warranty of anykind, either express or implied. The responsibility forthe interpretation and use of the material lies with the reader. In no event shall the World HealthOrganization be liable for damages arising from itsuse. The views expressed by authors, editors, or expertgroups do not necessarily represent the decisions orthe stated policy of the World Health Organization.
This policy summary is one of a new series to meet the needs of policy-makers andhealth system managers.
The aim is to develop key messages to supportevidence-informedpolicy-making, and theeditors will continue to strengthen the series by working withauthors to improve theconsideration given to policy options andimplementation.
Keywords:
FINANCING, HEALTH
DELIVERY OF HEALTH CARE –economics
HEALTH POLICY
PUBLIC HEALTHADMINISTRATION
HEALTH SYSTEM PLANS –organization andadministration

Health policy responses to the financial crisis in Europe
Philipa Mladovsky, Divya Srivastava, Jonathan Cylus,Marina Karanikolos, Tamás Evetovits, Sarah Thomson,Martin McKee


Health policy responses to thefinancial crisis in Europe
Contents Page
Acknowledgements iv
Executive summary v
Key messages ix
1 Introduction 1
2 Understanding health policy responses to the financial crisis 3
3 Methods 9
4 Results 10
5 Conclusions 27
References 29
Annexes 38
Authors
Philipa Mladovsky, Research Fellow, EuropeanObservatory on Health Systems and Policies andLSE Health.Divya Srivastava, Research Officer, LSE Health,London School of Economics and Political Science.Jonathan Cylus, Technical Officer/ResearchFellow, European Observatory on Health Systemsand Policies and LSE Health.Marina Karanikolos, Technical Officer/ResearchFellow, European Observatory on Health Systemsand Policies and the London School of Hygieneand Tropical Medicine.Tamás Evetovits, Health Economist, WHO BarcelonaOffice for Health Systems Strengthening.Sarah Thomson, Senior Research Fellow, EuropeanObservatory on Health Systems and Policies,Deputy Director of the Observatory’s LSE hub andResearch Fellow and Deputy Director of LSE Health.Martin McKee, Professor of European PublicHealth at LSHTM, London School of Hygiene &Tropical Medicine.
Editors
WHO Regional Office forEurope and EuropeanObservatory on HealthSystems and Policies
EditorGovin Permanand
Editorial BoardJosep FiguerasClaudia SteinJohn LavisDavid McDaidElias Mossialos
Managing EditorsKate Willows FrantzenJonathan NorthCaroline White
The authors and editors aregrateful to the reviewerswho commented on thispublication and contributedtheir expertise.
No: 5
ISSN 2077-1584

Acknowledgements
This policy summary is the result of a collaboration between the EuropeanObservatory on Health Systems and Policies, the WHO Regional Office forEurope, and the European Commission (Directorate-General (DG) forEmployment, Social Affairs and Inclusion). The study benefited from researchundertaken for a project funded by the European Commission (DG forEmployment, Social Affairs and Inclusion) on Health Status, Health Care and Long-term care in the European Union (EU), Contract No. VC/2008/932(Srivastava & Mladovsky, 2011).
We are grateful to Josep Figueras, Matthew Jowett, Nora Markova, EricaRichardson, Tiziana Leone, David Stuckler, experts at DG for Health andConsumers (DG SANCO) and DG for Employment, Social Affairs and Inclusion,participants of the European Health Policy Group meeting in Copenhagen inApril 2012 and an anonymous referee for their comments on previous drafts of this policy summary; and to Katharina Hecht for her assistance in managingpart of the data collection. We are particularly grateful to the following countryexperts who contributed by completing the questionnaires and without whomthis study would not have been possible: Albania: Genc Burazeri; Armenia:Lyudmila Niazyan; Austria: Maria M. Hofmarcher and Leslie Tarver; Azerbaijan:Fuad Ibrahimov; Belarus: Aleksander Grakovich; Belgium: Sophie Gerkens andMaria Isabel Farfan-Portet; Bosnia and Herzegovina: Drazenka Malicbegovic;Bulgaria: Evgenia Delcheva; Croatia: Martina Bogut; Cyprus: Mamas Theodorou;Czech Republic: Tomas Roubal; Denmark: Karsten Vrangbæk; England: VanessaSaliba; Estonia: Triin Habicht; Finland: Jan Klavus; France: Sandra Mounier-Jack;Georgia: George Gotsadze; Germany: Marcial Velasco-Garrido; Greece: DaphneKaitelidou; Hungary: Barbara Koncz; Iceland: Sigrun Gunnarsdottir; Ireland:Steven Thomas; Israel: Amir Shmueli; Italy: Margherita Giannoni; Kyrgyzstan:Baktygul Akkazieva; Latvia: Anita Villerusa; Lithuania: Skirmante Starkuviene;Malta: Natasha Azzopardi Muscat; Netherlands: Ronald Batenburg; Norway:Anne-Karin Lindahl; Poland: Adam Kozierkiewicz; Portugal: Leonor BacelarNicolau; Republic of Moldova: Valeriu Sava; Romania: Victor Olsavszky; RussianFederation: Kirill Danishevskiy; Serbia: Vukasin Radulovic; Slovakia: LuciaKossarova; Slovenia: Rade Pribakovic; Spain: Alexandrina Stoyanova; Sweden:Anna Melke; Switzerland: Raphaël Bize; the former Yugoslav Republic ofMacedonia: Fimka Tozija; Turkey: Salih Mollahaliloğlu; Ukraine: Valery Lekhan;Uzbekistan: Mohir Ahmedov. The responsibility for any mistakes is ours.
Policy summary
iv

Executive summary
Introduction
The global financial crisis that began in 2007 can be classified as a healthsystem shock – that is, an unexpected occurrence originating outside the health system that has a large negative effect on the availability of healthsystem resources or a large positive effect on the demand for health services.Economic shocks present policy-makers with three main challenges:
• Health systems require predictable sources of revenue with which to planinvestment, determine budgets and purchase goods and services. Suddeninterruptions to public revenue streams can make it difficult to maintainnecessary levels of health care.
• Cuts to public spending on health made in response to an economic shock typically come at a time when health systems may require more, not fewer, resources – for example, to address the adverse health effectsof unemployment.
• Arbitrary cuts to essential services may further destabilize the healthsystem if they erode financial protection, equitable access to care and thequality of care provided, increasing health and other costs in the longerterm. In addition to introducing new inefficiencies, cuts across the boardare unlikely to address existing inefficiencies, potentially exacerbating thefiscal constraint.
In 2009, WHO’s Regional Committee for Europe adopted a resolution(EUR/RC59/R3) urging Member States to ensure that their health systems wouldcontinue to protect and promote universal access to effective health servicesduring a time of economic crisis. To date, there has been no systematic cross-country analysis of health policy responses to the financial crisis in Europe,although some overviews of health system responses to the crisis have beenpublished. This policy summary aims to address a gap in the literature bypresenting a framework for analysing health policy responses to economicshocks; summarizing the results of a survey of health policy responses to thefinancial crisis in the European Region’s 53 Member States; and discussing the potential effects of these responses on health system performance.
Understanding health policy responses to the financial crisis
When confronted by an economic shock affecting the health sector, policy-makers may decide to maintain, decrease or increase current levels of publicexpenditure on health. With each option they could also reallocate funds withinthe health system to enhance efficiency. A range of tools can be used to alter
Health policy responses to the financial crisis in Europe
v

expenditure levels, categorized under the following policy domains: the level of contributions for publicly financed care; the volume and quality of publiclyfinanced care; the cost of publicly financed care.
In making decisions about which tools to use, policy-makers need to considerthe impact of proposed reforms on the attainment of health system goals.Achieving fiscal balance is likely to be important in the context of a financialcrisis but generally it is not regarded as a primary goal of the health system – on a par with or overriding health policy goals such as health gain or financialprotection – since, if it were, it could be achieved by cutting public spending onhealth without regard for the consequences. This stands in contrast to the goalof efficiency. The purpose of trying to increase efficiency in the health sector is tomaximize outcomes for a given level of public resources devoted to health care.
Governments’ responses exist in a context of broader constraints andopportunities within and external to the health system. Public policy responsesto economic shocks should vary according to the nature of the shock. The crisishas had devastating consequences for some countries in Europe, particularlythose with high levels of pre-existing debt and deficit, which have found itdifficult to borrow to sustain public spending. Inability to obtain affordablecredit or to generate revenue through taxation severely constrains a highlyindebted country’s fiscal space, leaving it with little option but to cut publicspending. Political preferences may also influence public policy responses.
Survey results
The results of the survey suggest that the response to the crisis across theEuropean Region varied considerably across health systems and, in part,depended on the extent to which countries experienced a significant downturnin their economies. Some countries introduced no new policies, while othersintroduced many. Some health systems were better prepared than others due tofiscal measures they had taken before the crisis, such as accumulating financialreserves. There were many instances in which policies planned before 2008were implemented with greater intensity or speed as they became more urgentor politically feasible in face of the crisis, particularly the restructuring ofsecondary care. There were also cases where planned reforms were sloweddown or abandoned in response to the crisis.
Policies intended to change the level of contributions for publiclyfinanced health care
Several countries reported cuts in the national health budget in response to thefinancial crisis. In some countries, cuts were partly caused by rising unemploymentwhich reduced revenue from social insurance contributions. In a few cases,
Policy summary
vi

social insurance revenues and expenditures continued to increase, in part dueto the counter-cyclical contribution rate paid by the state for economicallyinactive people. Several countries increased or instituted user charges inresponse to the crisis. In contrast, others reported expanding benefits.
Policies intended to affect the volume and quality of publicly financedhealth care
In general the statutory benefits package and the breadth of populationcoverage were not radically changed following the financial crisis but somereductions were made, usually at the margin. In terms of policies to reducedemand for health services, several countries increased taxes on alcohol andcigarettes, but very few pursued health promotion policies such as healthyeating, exercise and screening in response to the crisis. Only one countryincreased waiting times as an explicit response to the crisis, although waitingtimes may also be increasing elsewhere as an indirect result of other healthpolicy reforms.
Policies intended to affect the costs of publicly financed health care
Many countries introduced or strengthened policies to reduce the price ofmedical goods or improve the rational use of medicines. In most cases thesepolicies were part of ongoing reforms. The crisis increased efforts to negotiatepharmaceutical prices in some national markets.
Some countries reduced the salaries of health professionals, froze them,reduced their rate of increase or used other approaches to lower salaries.Several countries reduced the health service prices paid to providers or linkedpayment to improved performance to realize efficiency gains and contain costs.Several governments are restructuring their Ministry of Health, statutory healthinsurance funds or other purchasing agencies in an attempt to increaseefficiency and reduce overhead costs.
In many countries, the economic crisis created an impetus to speed up theexisting process of restructuring the hospital sector through closures, mergersand centralization, a shift towards outpatient care and improved coordinationwith or investment in primary care.
Conclusions
The survey results indicate that European Region countries have employed a mix of policy tools in response to the financial crisis. Some countries seem to have used the crisis to increase efficiency, although little has been done to enhance value through policies to improve public health, which is a missed opportunity.
Health policy responses to the financial crisis in Europe
vii

Policies to secure financial sustainability in the face of the financial crisis, and to improve the health sector’s fiscal preparedness for financial crises, should be consistent with the fundamental goals of the health system.
To risk over-simplifying, policy tools likely to promote health system goalsinclude: increased risk pooling; strategic purchasing, where contracts arecombined with accountability mechanisms including quality indicators, patient-reported outcome measures and other forms of feedback; health technologyassessment to assist in setting priorities, combined with accountability,monitoring and transparency measures; controlled investment in the healthsector, particularly for health infrastructure and expensive equipment; publichealth measures to reduce the burden of disease; price reductions forpharmaceuticals combined with cost–effectiveness evidence and othermeasures to promote rational prescribing and dispensing; shifting frominpatient to day-case or ambulatory care, where appropriate; integration andcoordination of primary care and secondary care, and of health and social care;reducing administrative costs while maintaining capacity to manage the healthsystem; fiscal policies to expand the public revenue base; counter-cyclicalmeasures, including subsidies, to protect access and financial protection,especially among poorer people and regular users of health care; and, outsidethe health sector, active labour market programmes and social support servicesto mitigate some of the adverse effects of economic downturns.
Policy tools that risk undermining health system goals include: reducing thescope of essential services covered; reducing population coverage; increases in waiting times for essential services; user charges for essential services; andattrition of health workers caused by reductions in salaries.
The discussion highlights the trade-offs involved in any policy decision. Thesetrade-offs should be understood and made explicit so that decision-makers can openly weigh evidence against ideology in line with societal values. Policydecisions should be guided by a focus on enhancing value in the health systemrather than on identifying areas in which cuts might most easily be made.Viewing fiscal balance as a constraint to be respected, rather than as anobjective in its own right allows decision-makers to shift the terms of debateaway from balancing the budget at any cost towards an emphasis onmaximizing the health system’s performance.
Policy summary
viii

Key messages
• Economic shocks present policy-makers with three main challenges:
– Health systems require predictable sources of revenue. Suddeninterruptions to public revenue streams can make it difficult tomaintain necessary levels of health care.
– Cuts to public spending on health made in response to an economicshock typically come at a time when health systems may requiremore, not fewer, resources – for example, to address the adversehealth effects of unemployment.
– Arbitrary cuts to essential services may further destabilize the healthsystem if they erode financial protection, equitable access to care andthe quality of care provided, increasing costs in the longer term. Inaddition to introducing new inefficiencies, cuts across the board areunlikely to address existing inefficiencies, potentially exacerbating the fiscal constraint.
• The response to the crisis across the European Region varied across health systems. Some countries introduced no new policies, while others introduced many. Some health systems were better prepared thanothers due to fiscal measures they had taken before the crisis, such asaccumulating financial reserves. There were many instances in whichpolicies planned before 2008 were implemented with greater intensity or speed as they became more urgent or politically feasible in face of thecrisis. There were also cases where planned reforms were slowed down or abandoned in response to the crisis.
• European Region countries employed a mix of policy tools in response tothe financial crisis. Some of the policy responses were positive, suggestingthat some countries have used the crisis to increase efficiency. The breadthand scope of statutory coverage was largely unaffected and in some casesbenefits were expanded for low-income groups. However, some countriesreduced the depth of coverage by increasing user charges for essentialservices, which is a cause for concern. Little was done to increaseefficiency through policies to improve public health.
• Policies to secure financial sustainability in the face of the financial crisis,and to improve the health sector’s fiscal preparedness for financial crises,should be consistent with the fundamental goals of the health system.
• To risk over-simplifying, policy tools likely to promote health system goalsinclude: risk pooling; strategic purchasing; health technology assessment;controlled investment; public health measures; price reductions for
Health policy responses to the financial crisis in Europe
ix

pharmaceuticals combined with rational prescribing and dispensing;shifting from inpatient to day-case or ambulatory care; integration andcoordination of primary care and secondary care, and of health and socialcare; reducing administrative costs while maintaining capacity to managethe health system; fiscal policies to expand the public revenue base; andcounter-cyclical measures, including subsidies, to protect access andfinancial protection, especially among poorer people and regular users of health care.
• Policy tools that risk undermining health system goals include: reducingthe scope of essential services covered; reducing population coverage;increases in waiting times for essential services; user charges for essentialservices; and attrition of health workers caused by reductions in salaries.
• Where the short-term situation compels governments to cut publicspending on health, the policy emphasis should be on cutting wisely tominimize adverse effects on health system performance, enhancing valueand facilitating efficiency-enhancing reforms in the longer run.
Policy summary
x

1 Introduction
The global financial crisis that began in 2007 can be classified as a healthsystem shock – that is, an unexpected occurrence originating outside the healthsystem that has a large negative effect on the availability of health systemresources or a large positive effect on the demand for health services. Economicshocks present three risks which health policy-makers need to contend with.First, health systems require predictable sources of revenue with which to planinvestment, determine budgets and purchase goods and services. Suddeninterruptions to public revenue streams can make it difficult to maintain necessarylevels of health care. Second, cuts to public spending on health made in responseto an economic shock typically come at a time when health systems may requiremore, not fewer, resources – for example, to address the adverse health effectsof unemployment (see Box 1). Third, the nature of the health policy response to an economic shock may further destabilize the health system, particularly ifarbitrary cuts to essential services erode financial protection, equitable access to care and the quality of care provided, increasing health and other costs andexacerbating the fiscal constraint.
In 2009, WHO’s Regional Committee for Europe adopted a resolution(EUR/RC59/R3) urging Member States to ensure that their health systems would continue to protect and promote universal access to effective healthservices during a time of economic crisis (WHO Regional Office for Europe,2009). The resolution built on momentum created by the 2008 Tallinn Charter,which noted that health systems promoted both health and wealth; thatinvestment in health was an investment in future human development; andthat well-functioning health systems were essential for any society to improvehealth and attain health equity (WHO Regional Office for Europe, 2008). Morerecently, WHO has addressed the challenge of sustaining equity, solidarity andhealth gain in the context of the financial crisis, highlighting the diversity ofhealth policies pursued by Member States in response to budgetary pressures(WHO Regional Office for Europe, 2011b).
To date, there has been no systematic cross-country analysis of health policyresponses to the financial crisis in Europe, although some overviews of healthsystem responses to the crisis have been published (Schneider, 2009; EuropeanCommission & Economic Policy Committee (AWG), 2010; Doetter and Gotze,2011; European Hospital and Healthcare Federation, 2011; WHO RegionalOffice for Europe, 2011b; European Federation of Nurses Associations, 2012).1
This policy summary aims to address a gap in the literature by presenting aframework for analysing health policy responses to economic shocks;
1 In addition, an article based on an earlier draft of this policy summary has beenpublished (Mladovsky et al., 2012).
Health policy responses to the financial crisis in Europe
1

Policy summary
2
summarizing the results of a survey of health policy responses to the financialcrisis in the European Region’s 53 Member States; and discussing the potential effects of these responses on health system performance.
Box 1. Effects of economic downturns on health
Research on health during the Great Depression in the United States in 1929–1937 showed that while suicides rose, overall mortality fell due to a decrease in infectious diseases and road-traffic accidents (Fishback, Haines & Kantor, 2007). A recent study using city- and state-level mortalities by cause shows that, apartfrom rises in suicides and falls in road-traffic deaths, overall mortality changeswere unrelated to the depression itself (Stuckler et al., 2011a).
The recession following the collapse of the Soviet Union in the early 1990s haddevastating consequences for population health across the region, with mortalityincreases of up to 20% in some countries. The pace of transition, including massprivatization and the absence of a social safety net in some of the countries,extensively affected life expectancy rates (Stuckler, King & McKee, 2009). Manyex-communist countries regained their pre-transition life expectancy levels onlytwo decades later. The adverse consequences of rapid economic reforms werefound to be lower in countries in which many people were members of socialorganizations such as trade unions, religious groups or sports clubs (Stuckler, King & McKee, 2009).
Countries affected by the South East Asian economic crisis of the 1990s adopteddifferent recovery strategies. Thailand and Indonesia, which reduced spending onsocial protection, experienced short-term increases in mortality, while Malaysiamanaged to sustain social protection programmes and showed no obvious changein death rates (Waters, Saadah & Pradhan, 2003; Hopkins, 2006; Chang et al., 2009).
These examples show how health outcomes following recession may differ, inpart depending on the context and causes of the crisis, but also depending on a country’s response.
A series of studies using aggregate-level data have suggested that health mightnot be affected by economic downturns in high-income countries, as mortalitytends to fall when the economy slows down and rise when the economy speedsup (Ruhm, 2000, 2003, 2008; Gerdtham & Ruhm, 2006). This effect has beenobserved at least in the short run, with the extent of the effect varyingsubstantially for different age groups (Joyce & Mocan, 1993), sexes (Chang et al., 2009) and diseases (Waters, Saadah & Pradhan, 2003), and the results are somewhat sensitive to the indicators used to measure economic change(Gerdtham & Johannesson, 2005; Svensson, 2007; Economou, Nikolau &Theodossiou, 2008; Stuckler, Meissner & King, 2008). Noting the counterintuitivenature of these findings (Catalano & Bellows, 2005), researchers have suggestedthat recessions may have a positive impact on health because increased leisuretime allows people to engage in health-enhancing activities such as exercise, or to cut down on over-consumption of food and alcohol.

2 Understanding health policy responses to the financial crisis
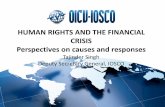
Fig. 1 depicts a framework for describing possible health policy responses to health system shocks. The framework has three main dimensions: healthexpenditure options, policy domains and outcomes. First, when confronted byan economic shock affecting the health sector, policy-makers may decide tomaintain, decrease or increase current levels of public expenditure on health.With each option they could also reallocate funds within the health system toenhance efficiency.
Health policy responses to the financial crisis in Europe
However, other research shows that economic downturns pose clear risks tohealth due to suicides and alcohol-related mortality (Stuckler et al., 2009; Stuckler,Basu & McKee, 2010; Suhrcke et al., 2011). These studies also find that adverseeffects can be partly mitigated by providing job reintegration programmes andsupport to families during periods of economic instability, as well as maintainingregulation of the alcohol industry to avoid hazardous drinking as a copingmechanism. Where such measures have been in place, the health benefits ofeconomic crises, such as declining road-traffic accidents as people drive less, tendto outweigh the risks, improving population health, at least in the short-term.
In summary, while additional research is needed to understand the longer-termand indirect effects of economic crises on health and health systems, someevidence from previous economic downturns suggests that recession, especiallyaccompanied by increases in unemployment, is damaging to public health(Kaplan, 2012; McKee, Basu & Stuckler, 2012). Maintaining spending on socialprotection, particularly on active labour market programmes, is likely to reducenegative effects on health.
Given the long delays in publishing mortality data in many countries, onlypreliminary conclusions can be drawn about the effects of the current crisis inEurope. However, research to date confirms a sharp rise in suicides in the countriesworst affected and a fall in deaths from road-traffic accidents, most notable incountries where initial accident levels were highest (Stuckler et al., 2011b).
More detailed evidence emerging from Greece, the European country that hasbeen hardest hit by the financial crisis, points to a worsening of mental healthstatus in the past two years (Economou et al., 2011; Madianos et al., 2011); self-reported general health has also deteriorated since the start of the crisis and there has been a significant increase in the number of people who felt theyneeded health care, but did not access it (Kentikelenis et al., 2011); the numberof new HIV cases among injecting drug users (IDU) has risen dramatically, thoughtto be caused by reduced service provision (EMCDDA & ECDC, 2011).
3

Fig. 1. Health policy responses to the financial crisis and other economic shocks
Second, a range of policy tools within three main policy domains can be usedto alter expenditure levels. These can be categorized as:
• the level of contributions for publicly financed care (the size of the nationalhealth budget, social insurance contributions and transfers from the healthbudget, aspects of fiscal policy such as earmarking taxes for health, shiftingto private expenditure on health in the form of user charges or privatehealth insurance);
• the volume and quality of publicly financed care (the statutory benefitspackage, population coverage, non-price rationing in the form of waiting times);
• the cost of publicly financed care (the price of medical goods, health workersalaries, payments to providers, overhead costs, service reconfiguration).
In many cases, policies will affect more than one of these factors. For example,altering the price of medical goods will not only change the unit cost of care; it may also change the volume of medical goods provided and the level ofcontributions, if user charges are involved.
Third, when making decisions policy-makers need to consider the impact of anyproposed reforms on the attainment of health system goals. Health system
Policy summary
4
Healthexpenditure Policy domains Outcomes
Cut
Increase
Maintain
Reallocate
Financing/contributions
Volume and qualityof services
Costs
Effect on healthsystem goals
Financial crisis and other constraints/opportunities

goals can be articulated in many ways; different policy documents put forwarda range of goals (see WHO, 2000, 2010; Figueras, Lessof & Srivastava, 2006;Kutzin, 2008):
• health status: improving health outcomes and health service outcomes
• financial protection: ensuring people do not suffer financial hardship when using needed health care
• efficiency: maximizing health gain from given resources and avoidingwaste, enhancing value by ensuring benefits outweigh costs
• equity: ensuring health services are distributed in relation to need andcontributions are set according to capacity to pay
• quality: combines clinical effectiveness with patient experience andtherefore captures safety, effectiveness, accessibility, acceptability
• responsiveness: meeting people's legitimate non-health expectationsabout how the health system treats them
• transparency: providing reliable information about features of the healthsystem such as benefits, costs and quality
• accountability: monitoring and evaluation of performance which isassociated with tangible consequences (penalties or rewards).
Fig. 2 makes explicit the links between health care expenditure, policy tools andgoals or outcomes. Changes to expenditure should be considered in the light oftheir potential impact on the attainment of health system goals. Achieving fiscalbalance is likely to be important in the context of a financial crisis but generallyit is not regarded as a primary goal of the health system – on a par with oroverriding health policy goals such as health gain or financial protection – since,if it were, it could be achieved by cutting public spending on health withoutregard for the consequences (Thomson et al., 2009). This stands in contrast tothe goal of efficiency. The purpose of trying to increase efficiency2 in the healthsector is to maximize outcomes for a given level of public resources devoted tohealth care (Weinstein & Stason, 1977). Efficiency gains imply achieving similaroutcomes at lower cost, better outcomes at similar cost or better outcomes at
2 Technical efficiency refers to the physical relation between resources (capital and labour)and health outcomes: obtaining the maximum level of output for a given level of inputor a minimum level of input for a given level of output. Productive efficiency refers tominimizing total cost for given output, or the maximization of health outcome for agiven level of cost. Allocative efficiency refers to maximizing the value of the output orthe appropriate combination of health programmes to maximize the health of society(Palmer & Torgerson, 1999).
Health policy responses to the financial crisis in Europe
5

greater cost, where the benefits exceed the extra cost involved (Chernew et al.,1998; Palmer & Torgerson, 1999; Docteur & Oxley, 2003; Goetghebeur, Forrest& Hay, 2003; Dormont, Grignon & Huber, 2005; OECD, 2006; Pammolli et al.,2008). As we have noted, arbitrary cuts to public spending on health inresponse to an economic shock may undermine health system performance byreducing financial protection, equitable access to care and the quality of careprovided. This in turn might reduce efficiency by lowering health outcomes andincreasing health and other costs in the longer term. In addition to introducingnew inefficiencies, cuts across the board are unlikely to address existinginefficiencies, potentially exacerbating the fiscal constraint (Kutzin, 2008;Thomson, Foubister & Mossialos, 2009).
All three sets of responses exist in a context of broader constraints andopportunities within and external to the health system. Public policy responsesto economic shocks should vary according to the nature of the shock. Thecurrent economic crisis, considered by many to be the worst since the GreatDepression, was triggered by a combination of easy access to credit,irresponsible lending and high-risk investment involving complex financialinstruments. When investment-related loans could not be repaid, the financialinstruments lost considerable value (Wade, 2009) and financial institutions andothers holding or exposed to these securities suffered massive losses. Lenderreluctance to take on further liabilities led to liquidity shortages and concernsabout the solvency of financial institutions, deepening the crisis and causing itto extend well beyond the financial sector. Although the crisis to some extentoriginated in the United States (US), it quickly spread to other countries,resulting in bank failures, stock market crashes, drops in asset prices, negativegross domestic product (GDP) growth, rising unemployment and, ultimately,bailouts of entire countries.
The crisis has had devastating consequences for some countries in Europe,particularly those with high levels of pre-existing debt and deficit, which havefound it difficult to borrow to sustain public spending. Inability to obtainaffordable credit or to generate revenue through taxation severely constrains a highly indebted country’s fiscal space, leaving it with little option but to cutpublic spending. Within the Eurozone, national inability to form independentmonetary policy also limits policy options for combating the crisis. For Greece,Ireland and Portugal, bailout packages from the European Commission, theInternational Monetary Fund (IMF) and the European Central Bank (the “troika”)have actually mandated public sector reforms (including reforms to the healthsector) as conditionality for the receipt of funds, removing national autonomyin some areas of public policy (Fahy, 2012).
Policy summary
6

Fiscal space may be further constrained by a rapid increase in unemployment. In the European Region, unemployment rates rose from 7.4% in 2008 to 8.6%in 2009 (WHO Regional Office for Europe, 2012). Rising unemployment notonly reduces household consumption and tax revenues; it also adds to pressureon the government’s welfare budget, as the need for unemployment and othersocial security benefits, including health benefits, increases. Countries that relyon the labour market to finance health care may find that paying social insurancecontributions for a growing number of unemployed people is another source offiscal pressure. Finally, political preferences may influence public policy responsesas much as the magnitude of the fiscal constraint created or exacerbated by theeconomic shock.
In the context of pressure for cuts in public spending, the health sector is likelyto be affected. Research suggests that public spending on health in Europe hastended to fall after previous economic crises, often at a faster rate than othertypes of government expenditure (Cylus, Mladovsky & McKee, in press). Recenthealth expenditure data suggest that a similar pattern is emerging in manycountries (see section 4). The health sector may be vulnerable to budget cutsfor a range of reasons. Public spending on health accounts for a substantialproportion of total government expenditure: nearly 13% on average in theEuropean Region (see Table 1). Health system inefficiencies may make itpolitically difficult to argue for maintaining current levels of public expenditureon health during a period of fiscal austerity. It may also be easier to cut publicspending on health than to make cuts in other areas of social protection, such as pensions, either because there is more scope for efficiency gains in the health system or because health benefits are less clearly defined than other benefits (Fahy, 2012). Conversely, counter-cyclical health policies such as holding financial reserves earmarked for health or linking governmentcontributions for economically inactive groups of people to average earnings in previous years may ease pressure to cut public spending on health (WHORegional Office for Europe, 2011b).
Other factors that may influence the nature, scale and intensity of the healthpolicy response to the crisis include the capacity of key stakeholders forimplementation (e.g. availability of human resources and expertise); theavailability and use of evidence to inform reforms (e.g. effective healthtechnology assessment (HTA) systems in place); political feasibility (e.g. policiesmay be resisted or overturned by politicians, professionals or the public, or,conversely, planned “unpopular” policies may become more politically feasiblein the context of the crisis); and the presence of other public sector reforms(e.g. cuts or stimulus packages affecting pensions, jobs, welfare benefits andthe unemployment rate).
Health policy responses to the financial crisis in Europe
7

Table 1. Public expenditure on health as a percentage of total governmentexpenditure, WHO European Region
Policy summary
8
Country 2008 2009 Difference2008–2009
Kazakhstan 8.3 11.3 3.0Monaco 15.8 18.5 2.7Tajikistan 5.0 6.4 1.4Azerbaijan 2.5 3.7 1.2Bosnia and Herzegovina 14.0 15.1 1.1Republic of Moldova 13.0 14.1 1.1Uzbekistan 8.6 9.6 1.0Belarus 8.2 8.8 0.6Italy 13.6 14.2 0.6Malta 12.4 13.0 0.6Albania 8.2 8.4 0.2Georgia 7.3 7.5 0.2Kyrgyzstan 11.5 11.7 0.2Switzerland 19.9 20.0 0.1Andorra 21.3 21.3 0.0Austria 15.8 15.8 0.0Belgium 14.8 14.8 0.0Bulgaria 9.1 9.1 0.0Croatia 17.6 17.6 0.0Cyprus 5.8 5.8 0.0Czech Republic 13.3 13.3 0.0Denmark 15.3 15.3 0.0Finland 12.6 12.6 0.0France 16.0 16.0 0.0Germany 18.0 18.0 0.0Greece 13.0 13.0 0.0Hungary 10.2 10.2 0.0Iceland 13.1 13.1 0.0Ireland 16.0 16.0 0.0Israel 10.0 10.0 0.0Latvia 10.2 10.2 0.0

Source: WHO, 2012.
3 Methods
To map health policy responses to the financial crisis, we analysed healthexpenditure data from the Health for All and WHOSIS databases and sent aquestionnaire to a network of health policy experts in the European Region’s53 Member States. Most of the experts were based in universities, WHOcountry offices and other non-governmental organizations. Completedquestionnaires were received in March and April 2011.
Health policy responses to the financial crisis in Europe
Country 2008 2009 Difference2008–2009
Lithuania 12.8 12.8 0.0Luxembourg 13.7 13.7 0.0Montenegro 13.6 13.6 0.0Netherlands 16.2 16.2 0.0Norway 16.7 16.7 0.0Poland 10.9 10.9 0.0Portugal 15.4 15.4 0.0Romania 11.8 11.8 0.0San Marino 13.6 13.6 0.0Slovenia 12.9 12.9 0.0Spain 15.2 15.2 0.0Sweden 13.8 13.8 0.0Turkey 12.8 12.8 0.0Turkmenistan 7.0 7.0 0.0Ukraine 8.6 8.6 0.0United Kingdom 15.1 15.1 0.0Serbia 14.1 13.9 -0.2Estonia 11.9 11.7 -0.2Armenia 7.2 6.6 -0.6Russian Federation 9.2 8.5 -0.7Slovakia 15.4 14.0 -1.4The former Yugoslav Republic of Macedonia 13.6 12.1 -1.5
9

Because it was not always clear to what extent a policy was, in fact, a responseto the crisis, as opposed to being part of an ongoing reform process, we askedrespondents to divide policies into two groups based on whether they were(a) defined by the relevant authorities in the country as a response to the crisisor (b) either partially a response to the crisis (i.e. planned before the crisis butimplemented with greater or less speed or intensity than planned) or possibly a response to the crisis (i.e. planned and implemented since the start of thecrisis, but not defined by the relevant authorities as a response to the crisis).Both types of policies are reported here. We also asked respondents to provideevidence of the impact of policy responses on health system performance, butin almost every case they reported that evidence was not yet available.
Survey responses were categorized using the framework (Fig. 1). All of the data were analysed separately by two researchers (i.e. two people extracted the same data to ensure accuracy) and summarized in tables. The tables wereverified by the respondents and by experts from WHO. The completed policysummary was reviewed by experts from WHO, the World Bank and theOrganisation for Economic Co-operation and Development (OECD). Annex 1contains the full results of the survey.
The study has several limitations. First, as we anticipated, it is difficult to definewhether or not policies are in fact a response to the financial crisis. Second, we asked respondents to provide information distinguishing between types ofhealth care (curative, preventative, long-term care, medical goods, etc.) wherepossible, but comparing types of health care across countries is challenging,particularly due to the lack of a common definition of the term “public health”(McKee & Jacobson, 2000; Kaiser & Mackenbach, 2008). Where necessary, we clarified terminology with respondents. Third, the information provided byexperts may be of varying completeness and quality. Fourth, we have not beenable to systematically include information on each health system’s degree offiscal preparedness. Some countries may have introduced measures to improveefficiency or cut costs just before the crisis began, so that there was not muchroom for further reform. It is possible to capture this in case studies, butdetailed analysis covering 53 countries was beyond the scope of this exercise.Finally, evaluating policy responses to the financial crisis in a general way maybe misleading because different policies need to be considered in context toestablish actual impact on health system performance and health expenditure.
4 Results
Forty-five countries responded to the questionnaire. Their responses are summarized below (for more detailed results, see Annex 1), with a brief commentary on the potential impact of each policy tool on health system performance.
Policy summary
10

4.1 Overview
WHO data indicate that, between 1998 and 2008, government spending onhealth as a share of GDP increased in most European countries (35 out of 53).From 2007 to 2008 real GDP per person contracted in just one country (Ireland)but grew in all others, ranging from 2.8% in France to 21.1% in the RussianFederation (Fig. 2). From 2008 to 2009 public expenditure on health per capitagrew in all but nine countries (Fig. 2).3 This suggests there was no immediatebudgetary response in the health sector to the financial crisis. However, GDPgrowth from 2008 to 2009 indicates a bleaker outlook: the size of the realeconomy contracted in 38 countries to varying degrees (from -0.1% in Portugalto -13.9% in Ukraine). Overall, real GDP per capita contracted by -3.4% in the European Region. The decline in GDP could take time to affect politicaldecisions that influence public spending on health, so data for 2010 and 2011should give a better picture of the trends when they become available.
Between 1998 and 2008, total government spending as a share of GDPdecreased in the European Region (from 42.4% to 40.9% in aggregate); thatis, the public sector’s share of the economy (the size of government) becamesmaller. During this period, public spending on health grew to consume agreater share of total government spending (rising from 11.6% in 1998 to12.8% in 2008), because governments maintained or increased the healthshare of the government budget (WHO Regional Office for Europe, 2011b).However, from 2008 to 2009 only 14 countries had an increase in publicspending on health as a share of total government expenditure, ranging from0.1% to 3% (Table 1). Most of these were Member States that have beenlargely unaffected by the financial crisis and where public expenditure on healthis increasing from a very low base. This suggests that in affected countries, thefinancial crisis may already be having a negative effect on the prioritygovernments accord to health budgets.
The effect of the financial crisis on health policy varied across health systems inEurope and in part depended on the extent to which countries experienced asignificant downturn in their economies. Within the European Region, Albania,Azerbaijan, Israel and Norway were mostly insulated from the crisis andtherefore reported no direct health policy responses at all. Of the countries thatwere affected by the crisis, some introduced several new policies in response(Czech Republic, Greece, Ireland, Portugal, Republic of Moldova); in Greece,Ireland and Portugal the reforms were part of a broader debt restructuringprocess which required intervention from the EU, the European Central Bank
3 Cyprus (-0.1%), the former Yugoslav Republic of Macedonia (-1.0%), Serbia (-2.4%),Hungary (-3.4%), Romania (-8.0%), Ukraine (-12.9%), Iceland (-13.1%), Lithuania (-16.8%)and Latvia (-16.9%) all experienced a drop in real public health expenditure per capita.
Health policy responses to the financial crisis in Europe
11

Fig. 2. GDP growth and change in public spending on health per capita, WHO European Region
Source: GDP data from WHO Regional Office for Europe, 2011a; health spending data fromWHO, 2011.Note: Data purchasing power parity (PPP) adjusted.
Policy summary
12
-20% -10% 0% 10% 20% 30% 40% 50% 60% 70% 80%
Azerbaijan
Tajikistan
Kyrgyzstan
Kazakhstan
Turkey
Montenegro
Republic of Moldova
Spain
Ireland
Portugal
Italy
Poland
Luxembourg
Denmark
United Kingdom
Germany
Georgia
Netherlands
Albania
Switzerland
Belgium
Uzbekistan
Russian Federation
Greece
Czech Republic
Armenia
Slovenia
Bosnia and Herzegovina
Turkmenistan
Finland
Belarus
Norway
Bulgaria
Austria
France
Slovakia
Sweden
Malta
Estonia
Israel
Croatia
Cyprus
The former Yugoslav Republic of Macedonia
Serbia
Hungary
Romania
Ukraine
Iceland
Lithuania
Latvia
-0.1
5.7
-2.4
6.3
6.35.8
14.3
4.9-13.1
8.6
15.6
6.7
15.6
15.4 15.4
1.9
6.7
6.4
6.9
4.6
-3.4
9.9
-12.9
6.7
6.7 8.2
16.3 16.3
6.7 6.7
-16.9 -16.9
-16.8 -16.8
-8.0-8.0
0.0
3.60.2
5.4 0.5
3.0
5.35.4
5.0
2.6 2.9
11.5
13.5
2.8
4.6
5.7
6.9
3.1
3.3
3.4
3.6
3.7
4.2
3.6
11.4
11.4
10.5
14.0
5.9
5.9
3.4
3.1
6.1
21.1
4.6
4.6
9.6
-4.9
34.6
4.3
11.9
8.6
-1.0
6.7
3.6
9.9
73.7
6.4
5.4
9.09.0
7.87.8
10.910.3
13.013.1
14.8
5.5
4.7
7.97.9
8.08.0
4.7
7.58.28.2
8.28.2
8.88.8
5.3
9.1
17.5
9.1
4.3
6.76.74.4
6.86.83.7
7.5
7.6
8.5
17.5
26.626.6
28.328.3
Per capita government expenditure on health (PPP int. $) 2008–2009Real GDP US PPP per capita growth 2007–2008
ugoslav Republic of MacedoniaThe former Y
-13.1
-2.4
Latvia
Lithuania
Iceland
Ukraine
Romania
yHungar
Serbia
ugoslav Republic of Macedonia
Cyprus
Croatia
-12.9
-3.4
--1166.9
--116.6..8
----88.0
-1.0
4.9
-2.4
5.7
-0.1 88.6
115.5..6
4115.5.4
6.6..7
9.9
-3.4
88..2
116.6..3
76.6..7
-1.0
0.0
Israel
Estonia
Malta
Sweden
Slovakia
France
Austria
Bulgaria
wayNor
Belarus
Finland
urkmenistanT
1.9
4.6
5.4
14.0
10.5
11.4
11.4
3.6
4.2
3.7
3.6
3.4
3.3
3.1
4.6
2.8
13.5
11.5
2.9 2.6
3.0
0.55.4
0.23.6
0.0
zegovinaBosnia and Her
Slovenia
Armenia
Czech Republic
Greece
Russian Federation
Uzbekistan
Belgium
Switzerland
Albania
Netherlands
Georgia
Germany
14.3
5.86.3
6.3
67 6..7
6.66.4
66.9
6 11
3.6 5.9
7
9.6
4.66
4.6
21.1
6.1
56 5.9
10.5
5.7
5.0
5.45.3
99.0
57..8
4.7 6.
4
5.57.
46 7
4.46Germany
United Kingdom
Denmark
Luxembourg
Poland
Italy
Portugal
Ireland
Spain
Republic of Moldova
Montenegro
urkeyT
Kazakhstan
-4.9
4.3
7.6
4.3
9.9
4.3
3.1
3.4
14.813.113.0
10.310.9
7.7.9
8.8..0
4.7
3
7.5.558.8.2
7.55
8.8.2
8.8..8
5.3
9.9..1
117.7.5
4.3
66..7
6.6.8
7
3.7
7.67.6
226.6.6
-10%-20%
Kyrgyzstan
ajikistanT
Azerbaijan
40%30%20%10%0%
9.99.9
11.9 34.6
8.5228.8.3
Real GDP US PPP per capita growth 2007–2008Per capita government expenditure on health (PPP int. $) 2008–2009
80%70%60%50%40%73.7
Real GDP US PPP per capita growth 2007–2008Per capita government expenditure on health (PPP int. $) 2008–2009

and the IMF. In other affected countries, however, very few or no policychanges were made (Denmark, Iceland, Finland, Germany, Kyrgyzstan, Malta,Poland, Russian Federation, Slovakia, Switzerland, the former Yugoslav Republicof Macedonia, Uzbekistan). In either case, there were many instances in whichpolicies planned before 2008 were implemented with greater intensity or speedas they became more urgent or (more often) politically feasible in face of thecrisis, particularly the restructuring of secondary care. In general, a wide rangeof measures was used, covering all three policy domains presented in Fig. 1.
There were also cases where planned reforms were slowed down or abandonedin response to the crisis. For example, Romania abandoned a plan to build eightnew hospitals and Ireland did not build one in four of proposed new healthfacilities. In Bulgaria the government decided to postpone full prohibition ofsmoking in public places. Also in Bulgaria, a policy to introduce a system ofcompulsory private health insurance, which was anyway unpopular with thepublic and doctors’ unions, was rejected by a new government that wished toretain control of public resources and institutions through the National HealthInsurance Fund. Bosnia and Herzegovina had difficulty implementing its recentlypassed health insurance laws due to a lack of reliable sources of funding, andtherefore decided to wait until after the crisis. In Georgia the transfer of hospitalinfrastructure ownership from the state to the private sector stalled due to the withdrawal of investors as a result both of the financial crisis and war with Russian Federation in 2008; the process was resumed in 2010. Ukraineattempted to introduce programmes seeking to increase efficiency, but mostwere not implemented due to a lack of political will. On the other hand, somegovernments were able to employ the financial crisis as a lever to strengthentheir position in ongoing negotiations with other health system stakeholders, in particular with the pharmaceutical sector (e.g. Austria, Latvia, Poland,Portugal, Russian Federation, Serbia, Slovenia and Turkey).
A few of the policy measures planned or implemented in response to the crisis were quickly reversed due to their unpopularity with key stakeholders,particularly efforts to reform provider payment. In Bulgaria the Ministry ofFinance attempted to take control of setting health service prices but thereform was strongly resisted by the medical union and eventually reversed. For a short period Hungary introduced tighter volume controls in the paymentof inpatient care providers but this was also reversed due to pressure fromhospitals. In the former Yugoslav Republic of Macedonia the value of acapitation point for primary care physicians was briefly decreased by 10%before doctors’ protests led to its reversal. In Romania a new system of payinggeneral practitioners (GPs), including a cap on the number of hours worked perweek, was proposed as part of a revised framework contract but rejected byGPs. In Ukraine the government attempted to stabilize rising pharmaceutical
Health policy responses to the financial crisis in Europe
13

prices by placing a cap on retail prices, which resulted in the closure ofpharmacies. The approach was fiercely resisted by the pharmaceutical industry and the government responded by implementing softer price controlmechanisms, which accounted for fluctuations in national currency rates.
A handful of countries were in the process of undergoing significant healthsector reforms funded by loans from international organizations such as theIMF, the World Bank and the EU when the crisis struck, so cost-cutting orefficiency-increasing measures were a continuation (Romania and Serbia). Many of the Commonwealth of Independent States (CIS) countries have verylow levels of health expenditure and a high proportion of spending throughout-of-pocket payments, leaving very little room for cutting public spending on health (Table 1). Some of them also have ongoing obligations to externalfunders to increase their public health spending annually (e.g. Kyrgyzstan) and programmes aimed at increasing health system efficiency planned beforethe crisis are currently being implemented. One or two countries had beenworking to slow health expenditure growth in recent years, making it difficultto determine whether or not new policies were explicit responses to the crisis(e.g. Croatia, Switzerland).
Some countries were better prepared than others due to fiscal measures they had taken before the crisis (the Czech Republic, Estonia, Italy, Lithuania,Republic of Moldova and Slovakia). These countries were able to draw onreserves or employ other counter-cyclical mechanisms that can compensate for the reduction of payroll tax revenues. For example, at the start of the crisis,the Estonian government cut back on public expenditure, including on health (a political decision made to comply with Maastricht criteria so that Estoniacould join the Eurozone; Estonia had low external debt and a low currentaccount deficit, meaning that deficit financing was a viable alternative). TheEstonian health system was better prepared for fiscal constraint than those of many of its neighbours. Better preparedness originated mainly from twosources. First, a pre-commitment to prioritize health spending in a downturn by allowing the health sector to accumulate reserves in the health insurancefund put the health insurance fund in a relatively strong position when it cameto budget negotiations with the Ministry of Finance. As a result, a transparentpolitical debate took place over the question of where to cut and how much to cut. Second, the Estonian health system invested appropriately in the healthsector before the crisis; when the crisis struck, the system could cope withdelays in investment without sacrificing health system goals such as quality of care in the short run. This stands in contrast to other countries, such asHungary, where the health system had already exhausted its (non-structural)efficiency reserves by the time the financial crisis began, meaning that healthsystem goals were likely to be eroded much faster.
Policy summary
14

Some countries prioritized paying off health sector debts at the expense ofhealth expenditure growth. In others, health budgets were ring-fenced whileother sectors experienced cuts (Belgium, Denmark and England). The Finnishgovernment implemented an economic stimulus package to mitigate some ofthe negative effects of the economic downturn.
4.2 Policies intended to change the level of contributions for publiclyfinanced health care
4.2.1 National health budget
Several countries reported cuts in the national health budget in response to thefinancial crisis (Bulgaria, Croatia, Estonia, Hungary, Iceland, Ireland, Italy, Greece,Latvia, Romania, Portugal, Spain). In some of these the health budget was reducedby over 20% (for example in Bulgaria and Latvia). Cuts were partly caused byrising unemployment which reduced revenue from social insurance contributions(Bulgaria, Estonia, Hungary, Romania). In other countries, social insurancerevenues and expenditures continued to increase (Austria, the Czech Republic,Poland, Slovakia; in the latter due to the high and counter-cyclical contributionrate paid by the state for economically inactive people), and the national health budget also rose in France, Denmark, the former Yugoslav Republic ofMacedonia and Turkey. In Denmark the education budget was used to cross-subsidize the health budget. It was maintained at previous levels in Albania,Belgium, England and Norway. Latvia received a World Bank loan in response to the crisis, to cover access to health services by poorer population groups.
As noted, decisions about whether to increase or decrease public spending on health in response to a health system shock may be driven by a mixture of political preferences and technical considerations. In the current crisis, large fiscal imbalances have left some countries with little or no choice in theirresponse; Greece and Portugal have been were particularly affected and wererequired to implement public sector cuts as part of bailout conditionalities.Where the short-term situation is such that governments are compelled to cutpublic spending on health, the policy emphasis should be on cutting wisely tominimize adverse effects on health system performance, enhancing value asmuch as possible and facilitating efficiency-enhancing reforms in the longerrun. The rest of this document is concerned with how this might be achieved.
4.2.2 Fiscal policy
Notwithstanding increases in taxes on alcohol and cigarettes (see below), fewcountries have reformed fiscal policy to increase revenue for health systemfinancing. In Italy, regions with large health care deficits have raised local taxesto recover deficits. In France, a new tax of 2% on certain sources of income
Health policy responses to the financial crisis in Europe
15

was set up in 2009 to finance social security (including health) expenditure and was subsequently increased to 4% in 2010 and 6% in 2011. Hungaryintroduced a public health tax on food and drinks with a high sugar content.
Although increases in taxation may reduce the need to increase governmentborrowing, very few countries have used fiscal policy to raise revenue for healthservices in response to the current crisis. Reluctance to introduce higher taxes forhealth care may be underpinned by valid technical and political considerations(such as a negative effect on the labour market, productivity and competitiveness),but the perception that tax-based financing of health care is as a general ruleunsustainable is unfounded (Thomson, Foubister & Mossialos, 2009).
4.2.3 Statutory health insurance revenue
Some countries increased employer/employee contribution rates either acrossthe board or for specific population subgroups (Bulgaria, Greece, Portugal,Romania, Slovenia). Slovakia reduced the state’s contribution for economicallyinactive people. Hungary lowered the contribution rate and the governmentincreased its budget transfers on behalf of non-contributing but eligiblepopulation groups to compensate the statutory health insurance fund for the loss of revenue (this was its most explicit and progressive response to thefinancial crisis; see WHO Regional Office for Europe, 2011b). In the Republic of Moldova, the rate of discount for statutory health insurance increased from50% to 75% for low-income populations. Turkey transferred responsibility forhealth care payments for government employees and their dependants fromthe Ministry of Finance to the Social Security Institute. Switzerland debatedincreasing premium subsidies for low-income families, but no measures werepassed. Slovakia and Lithuania already had in place counter-cyclical measuresfor government subsidies for those insured by the state in order to sustainstatutory health insurance revenue during a downturn. In Austria and Romaniathe government introduced subsidies to bail out social health insurance funds in order to help them pay off debts or prevent further indebtedness.
In countries that rely predominantly on employment-based social insurancecontributions, revenue can be maintained by lifting income or earnings ceilings, broadening the contribution base to encompass non-wage income or increasing transfers from the government budget (Thomson, Foubister &Mossialos, 2009). All of these are likely to be relevant options for governmentswanting to stimulate employment while maintaining or increasing publicspending on health (Thomson, Foubister & Mossialos, 2009). Another strategythat may be useful for smoothing some revenue over economic cycles is tomake government contributions for economically inactive groups of peoplecounter-cyclical by linking them to average earnings in previous years, as is thecase in Lithuania and Slovakia.
Policy summary
16

4.2.4 User charges (coverage depth)
Several countries increased or introduced user charges for health services inresponse to the crisis (Armenia, Czech Republic, Denmark, Estonia, France,Greece, Ireland, Italy, Latvia, Netherlands, Portugal, Romania, RussianFederation, Slovenia, Switzerland, Turkey). In some countries, user charges wereintroduced or increased in the hospital sector (Armenia, Czech Republic, Estonia(for inpatient nursing care), France, Ireland, Romania, Russia). Pharmaceuticals were subject to increased user charges in several countries (Czech Republic,France, Ireland, Latvia, Portugal, Slovenia). In England, a programme to expandthe range of long-term conditions that benefit from free prescriptions wasannounced by the previous government but not implemented; this will now no longer be taken forward. User charges were increased for ambulatory carein Greece, Italy, Romania and Turkey. User charges for emergency departmentsincreased in Ireland and for services not considered urgent in Italy. InSwitzerland the co-insurance rate will increase from 10% to 15% for peoplewho opt for traditional insurance plans (to encourage people to subscribe to a managed-care model of insurance).
Some countries introduced or increased charges for specific services such as in vitro fertilization (IVF) (Denmark and the Netherlands), ambulance transport(France and Slovenia), physiotherapy (the Netherlands), some mental healthservices (the Netherlands), some vaccines such as yellow fever, Japaneseencephalitis, typhoid, meningitis and rabies tetravalent (Portugal), GP homevisits (Romania), non-acute spa treatment, dental prostheses and someophthalmologic appliances (Slovenia), and doctor declarations attesting to the incapacity of a patient (Portugal) (see section 4.3.1 below on reductions in the benefit package).
In contrast, other countries reported expanding benefits, targeting low-incomegroups in the area of pharmaceuticals (Austria, France, Ireland, Italy, Republic of Moldova), reducing user charges (Croatia for primary care and outpatientprescription drugs) or abolishing user charges for some services (Italy, Hungary –although in Hungary’s case it was not a response to the crisis but it helped topromote financial protection).
Evidence from this study and a study on previous crises (Cylus, Mladovsky &McKee, in press) suggests that policy-makers may rely on user charges andother policies that shift costs to patients in an effort to slow aggregateexpenditure growth. However, user charges increase the financial burden onhouseholds (Wagstaff et al., 1992) and have been shown to be equally likely to reduce the use of high-value (cost-effective) and low-value care and areparticularly likely to reduce use among lower-income individuals and olderpeople, even when the level of user charges is low (Lohr et al., 1986; Manning
Health policy responses to the financial crisis in Europe
17

et al., 1987; Newhouse & Rand Corporation Insurance Experiment Group,1993; Gemmill, Thomson & Mossialos, 2008). Applying or increasing usercharges in primary or ambulatory specialist care may worsen health outcomesand lead to increased spending in other areas (e.g. emergency care). As a result,the potential for cost savings or enhanced efficiency is limited. Targeted usercharges selectively applied to low-value services or with exemptions or caps forpoorer households or regular users of care are more likely to enhance efficiency.However, it may not always be possible to identify low-value care and thetransaction costs involved may be significant (Braithwaite & Rosen, 2007; Bach, 2008; Thomson, Foubister & Mossialos, 2009).
4.3 Policies intended to affect the volume and quality of publiclyfinanced health care
4.3.1. Health benefits (coverage scope)
In general the statutory benefits package was not radically changed followingthe financial crisis, but some reductions were made, usually at the margin. Mostcountries did not report how coverage decisions were made. Only the CzechRepublic and Estonia reported plans to make greater use of HTA in evaluatingthe benefits package (although in the case of Estonia this was part of an ongoingprocess which was viewed more favourably by policy-makers in light of thecrisis). Reported mandatory coverage reductions included lower reimbursementof: dental care for certain population groups (Estonia, Ireland); IVF, physiotherapy,mental health services and coverage of care outside the EU (the Netherlands);cosmetic surgery (Portugal); non-acute spa treatment, certain medicines, non-urgent ambulance services, dental prostheses and some ophthalmologicappliances (Slovenia); eyeglasses (Switzerland); and temporary sickness benefitspaid by the statutory health insurance fund (Estonia, Hungary and Lithuania).The Russian Federation postponed adding outpatient prescription drugs to thebenefits package to 2013. On the other hand, Armenia included primary care in the basic primary care package, although this was part of ongoing reforms.Other countries expanded the scope of benefits in a targeted way, and theseare discussed under coverage breadth and contributions (section 4.3.2).
A fundamental objective of health policy at any time, but particularly during an economic crisis, is to maintain access to essential services for the population,especially for poorer people and regular users of health care (World Bank,2009). Changing the range of services included in the statutory benefitspackage (coverage scope) can be a valuable tool for setting priorities in thehealth system, particularly if changes are based on evidence and aim topromote the use of high-value care and discourage the use of low-value care. It can also be used to explicitly ration the quantity of care available. Evidence on clinical practice variation and inappropriate use of services may provide
Policy summary
18

justification for limiting volume of care and enforcing clinical practiceguidelines, but targeted implementation of these policies remains a challenge.Hungary introduced volume limits to inpatient services, but left it to thehospitals and doctors themselves to ration care implicitly or explicitly. In times of resource constraint countries may apply budget cuts across the whole sector,reducing funding for the majority of services available. However, cuts across theboard run the risk of undermining access to needed services, adversely affectingfinancial protection, health and efficiency. In contrast, selective, evidence-basedand transparent reductions in the scope of coverage represent an opportunityfor enhancing efficiency without undermining health system performance(Thomson, Foubister & Mossialos, 2009).
To this end, many countries have adopted HTA in the last two decades to assistin setting priorities (Velasco-Garrido & Busse, 2005), mainly in the area ofpharmaceuticals, and to devise clinical guidelines (Draborg et al., 2005; Lavis et al., 2007; Sorenson, Drummond & Kanavos, 2008). However, its use indetermining the contents of the benefits package has been limited due totechnical and political challenges and resource constraints (Ettelt S et al., 2007;Sorenson, Drummond & Kanavos, 2008). HTA is therefore more likely to beuseful as part of a longer-term strategy for enhancing efficiency than as a tool for quick decision-making. Nevertheless, countries with established HTAprogrammes will be better placed to make informed decisions in times ofeconomic crisis.
4.3.2. Population coverage (coverage breadth)
Ireland was the only country to remove eligibility for some aspects of statutorycoverage from some residents; in 2008 the Irish government excluded wealthyindividuals over the age of 70 from statutory coverage of primary care, althoughsince the general election in February 2011 the government has announcedplans to extend coverage to the whole population (universal coverage). TheCzech Republic reported reducing entitlement at the margin by reducingstatutory coverage for foreigners. Cyprus attributed its further postponement of implementation of universal coverage to the financial crisis, while Hungaryintroduced incentives for improved checks for eligibility for statutory coverageto identify and penalize those who avoid paying contributions. Several countriesreported expanding statutory coverage for previously uninsured groups ofpeople (Belarus, Bosnia and Herzegovina, Georgia, Republic of Moldova) orintroducing universal coverage (the former Yugoslav Republic of Macedonia).Thus, particularly in the former Union of Soviet Socialist Republics (USSR), somecountries without universal coverage are expanding eligibility for benefits totargeted population groups, but as part of ongoing reforms rather than inresponse to the economic crisis.
Health policy responses to the financial crisis in Europe
19

The share of the population entitled to statutory benefits is a crucialdeterminant of financial protection in the health system. Restricting eligibilityfor statutory coverage (e.g. on the basis of household income) may lead to an absolute reduction in public spending on health. However, evidence fromGermany and the Netherlands demonstrates that it adds to rather thanalleviates fiscal pressure in the health system (Thomson & Mossialos, 2006;Albrecht, Schiffhorst & Kitzler, 2007). This is partly due to the loss of contributionsfrom wealthier households. It is also due to segmentation of the national riskpool, which leaves the statutory risk pool with a concentration of older, poorerand sicker people and people with non-contributing dependants (Thomson &Mossialos, 2006). The Netherlands abandoned this policy in 2006 and Germanyhas taken numerous measures to mitigate its adverse effects.
Lowering the breadth, scope and depth of coverage creates a role for voluntaryhealth insurance (VHI). However, the market failures that characterize VHI, inparticular information problems relating to adverse selection and risk selection,mean that those reliant on voluntary cover may be placed at risk (Barr, 2004),particularly older people and people in poor health (Mossialos & Thomson, 2004;Thomson & Mossialos, 2006, 2009). In addition, the European experience of VHI indicates that in most countries it fails to address gaps in statutorycoverage: VHI market development is frequently very limited, particularlyoutside EU15 countries; VHI policies often do not develop to cover the mostimportant gaps; and where they are available, they may not be accessible tothose who need them most, even where the market is extensively regulated(Thomson & Mossialos, 2009).
4.3.3. Non-price rationing (waiting times, service dilution and delay)
The Estonian Health Insurance Fund supervisory board attempted to ration thevolume of care provided by deciding to increase maximum waiting times foroutpatient specialists’ visits from four to six weeks in March 2009. No othercountries reported increasing waiting as an explicit policy response to thefinancial crisis. Rather, in some countries health sector reforms may haveinadvertently led to increases in waiting times, such as in Ireland, wherechanges in health policy have led to a 9% increase in the number of patientson a waiting list between 2009 and 2010.
Changing waiting times may alter demand for publicly financed care withoutundermining health outcomes if patients on longer waiting lists choose privatealternatives (Hoel & Sæther, 2003) or choose to withdraw from treatment. Areview of the literature on waiting times (Garber, 2000) suggests that resourcesshould be allocated to different treatments according to their cost–effectiveness.However, reducing timely access to care may have an adverse impact on clinicalquality, which would undermine the goal of improving health. Its use as a policy
Policy summary
20

tool may also be limited by legitimate user expectations regarding acceptablestandards of health care.
There is an unexplored area of non-price based rationing mechanisms that areless tangible to both patients and policy-makers, and also difficult to research.These may take different forms of delaying, denying and diluting clinicalservices (“quality skimping”), with significant implications for health gain andefficiency of the use of limited resources. There is anecdotal evidence of such a response by providers to budget cuts. Delaying care in a non-transparentmanner and deviating from clinical practice guidelines on the grounds of costconsiderations are just two of the many implicit rationing mechanisms on thesupply side. Where monitoring of provider compliance with clinical standards isweak and professional organizations are less rigorous in enforcing good clinicalpractice, implicit rationing mechanisms may hide some of the adverse effects of the financial crisis. While waiting lists may not be a desired alternative formof rationing, they certainly make the process explicit and more transparent.Targeted research programmes are needed to explore the magnitude of implicitrationing and provide evidence to inform policy-makers (WHO, 2011).
4.3.4 Changing individuals’ behaviour (health prevention and promotion)
As previously mentioned, comparing international data on public healthfinancing and policy is challenging due to the lack of a pan-European definitionof the term “public health”. The following evidence on the effect of thefinancial crisis on public health in Europe is therefore illustrative and cannotserve as a comprehensive overview.
Several countries increased taxes on alcohol and cigarettes (Bulgaria, Estoniaand Ukraine, while the Czech Republic plans to do so in 2012) or pursuedhealth promotion policies, such as encouragement for healthy eating, exerciseand screening (Belgium, Bosnia and Herzegovina, Greece, Hungary, Republic ofMoldova). These policies seek to reduce the need for health care and aregenerally intended to lower the volume of publicly financed care provided. Fourcountries reported cuts to public health budgets. In Estonia, the Ministry’shealth expenditure fell by 24% in 2009 compared to 2008. This was partiallyachieved through cutting administrative costs and cutting the public healthbudget from 2009. Cuts focused on non-communicable diseases (NCDs) andprogrammes on communicable diseases were protected. EU social funds wereused to compensate for the reduction in NCD budget, but these funds will nolonger be available from 2012. In Italy, there were plans to cut the fund fordisease prevention and health promotion from EUR 29.6 to EUR 5.9 million in2011. In Latvia the public health budget was cut by 88.6% from 2008 to 2010.In Ukraine, expenditure on preventative services reduced by 9%. Threecountries reported the closure or merger of public health bodies. In Iceland,
Health policy responses to the financial crisis in Europe
21

there were plans to merge the Directorate of Health and the Public HealthInstitute in 2011. In Latvia, the Public Health Agency was closed in 2009. Manypublic health functions were distributed to other institutions and some werelost. In Lithuania, there was a reorganization of public health, resulting in themerger of seven public health institutions in 2009–2010.
Evidence on the economic benefits of prevention has grown in recent years,supporting broad public health promotion and preventative measures (e.g. systematic screening for hypertension, cholesterol, some cancers, healthadvice on diet, alcohol and smoking), although gaps remain (Schwappach,Boluarte & Suhrcke, 2007). Most published work is from the United States and Australia, however (Atun, 2004; Atun, Bennett & Duran, 2008). There isevidence to suggest that taxation can be a useful policy tool to address publichealth concerns and generate government revenue (Chaloupka & Warner,2000). Along with fiscal measures, an OECD study indicates that healtheducation and promotion, regulation and counselling on diet, smoking andalcohol by family doctors are cost–effective measures (Sassi, 2010). Thesepolicies could increase the efficiency of health service delivery in the medium to long term, but they may not address short-term fiscal constraints.
4.4 Policies intended to affect the costs of publicly financed health care
4.4.1 Prices of medical goods
Many countries introduced or strengthened policies to reduce the price ofmedical goods (pharmaceuticals, medical devices and equipment) or improve therational use of drugs (Austria, Belgium, Belarus, Bosnia and Herzegovina, Croatia,the Czech Republic, France, Estonia, Greece, Iceland, Ireland, Hungary, Latvia,Lithuania, Malta, Republic of Moldova, Poland, Portugal, Romania, RussianFederation, Serbia, Slovakia, Slovenia, Spain, the former Yugoslav Republic ofMacedonia, Turkey). A wide variety of measures were used, including genericsubstitution, INN prescribing, claw-back mechanisms, price negotiations andlengthening prescription validity. In most cases these policies were part ofongoing reforms, but the crisis often prompted, speeded up or intensifiedimplementation. Bulgaria and the Czech Republic are also in the process ofincreasing government regulation of the purchasing of medical devices. At thesame time, in many countries VAT increases affecting pharmaceuticals and otherproducts have to some degree attenuated the benefits to patients gained frommeasures designed to reduce prices.
The crisis increased efforts to negotiate pharmaceutical prices in some nationalmarkets, highlighting the importance of the public authority as a monopsonybuyer. Improved government procurement practices and positive lists contributeto lower medicine prices when balanced with regulated wholesale and retail
Policy summary
22

mark-ups (WHO, 2004). The range of approaches used by countries to controlprices can include free pricing, ex ante pricing relative to a substitute, internationalreference pricing, price volume agreements, price cuts, profit controls and ex post pricing relative to a substitute (Office of Fair Trading, 2007).
However, the positive effects of price controls may be offset by increases in thequantity of drugs prescribed or a change in the product mix to include moreexpensive medicines. For example, the downward effect on prices attributed to reference pricing is often short-lived (Lopez-Casasnovas & Puig-Junoy, 2000;Donatini et al., 2001; Nink, Schroder & Selke, 2001). As a result, pricing policiesshould be combined with policies targeting health professionals to encouragerational prescribing and dispensing in primary and secondary care. Again,however, savings might be offset by increases in volume and therefore short-lived (Harris & Scrivener, 1996; Buzzelli et al., 2006; Andersson et al., 2007;Mossialos & Srivastava, 2008). Nevertheless, even if such policy measures donot lower pharmaceutical expenditure, they may enhance efficiency withoutany negative effect on health outcomes. Policies to promote greater use ofgeneric medicines are likely to lower pharmaceutical expenditure and enhanceefficiency (Mrazek & Frank, 2004). In contrast, policies that aim to cut publicspending on prescription drugs by shifting costs to households are generallyfound to be of limited effectiveness and are discussed in the section on usercharges above.
4.4.2 Salaries and motivation of health sector workers
Some countries reduced the salaries of health professionals (Cyprus, France,Greece, Ireland, Lithuania, Romania), froze them (England, Portugal, Slovenia) orreduced their rate of increase (Denmark). Other approaches to lowering salariesincluded increasing public sector pension contributions substantially and reducingthe benefits, leading to a de facto pay cut (England), cutting overtime and night shifts, and lengthening shifts that require fewer staff and costs (Iceland),and making workers accept lower wages in order to maintain their contracts(privately contracted housekeeping and IT support staff in Serbia). In the CzechRepublic physicians managed to resist cuts to their salaries through negotiationor protests. Albania, which was largely insulated from the crisis, and Belarusand Ukraine continued to increase health worker salaries. In 2011 the formerYugoslav Republic of Macedonia approved the employment of additional healthworkers to improve quality and access to public health institutions, as well as to prevent qualified medical staff from leaving the public sector.
Employee wages, salaries and allowances account for 42.3% of public spendingon health in the 18 countries of the European Region for which data areavailable (WHO, 2006). This helps to explain the policy focus on cutting salariesin many countries. However, these policies may exacerbate wage imbalances
Health policy responses to the financial crisis in Europe
23

across countries (depending on the relative change in wages in net immigrationcountries compared to net emigration countries), possibly increasing healthworker migration in Europe and other regions, and adding to problems ofhuman resource shortages, which risks undermining quality and efficiency in the health system (Wismar et al., 2011). Wage imbalances could also becreated within countries if health sector wages fall at a different rate to wagesin other sectors. Policy-makers can apply a range of non-financial tools to retainworkers and improve performance, including clear job descriptions, professionalnorms and codes of conduct, the proper matching of skills to the tasks in hand, supervision, information and communication, infrastructure includingequipment and supplies, life-long learning, team management and teamworking, and responsibility with accountability (WHO, 2006). Improvements inthese areas may provide some limited help in retaining health workers facingsalary reductions and freezes.
A longer-term view of increasing efficiency in the supply of human resources for health would consider a broader range of strategies, in particular changingthe skill mix and substitution of health workers’ roles (typically nurses and GPstaking on some of the work of specialists or nurses taking on some of the workof GPs) to reduce the unit cost of labour or improve productivity. Reviews havefound that nurse substitution typically has either no or some improved effect on the quality of care, suggesting that this policy has the potential to increaseefficiency (McKee, Dubois & Sibbald, 2006). However, cost savings depend onthe magnitude of the salary differential between doctors and nurses, and maybe offset by the lower productivity of nurses compared to doctors (Laurant et al., 2005).
4.4.3 Payments to providers
In response to the crisis several countries have reduced the tariffs (i.e. prices)paid to providers (Estonia, Ireland, Romania, Slovenia) or linked payment toimproved performance to realize efficiency gains and contain costs (newcontractual measures to manage provider costs in Bosnia and Herzegovina;reported plans to introduce diagnosis-related group (DRG) payments forinpatient care in Bulgaria and the Czech Republic; pay for performance (P4P) inItaly; per capita payment in primary care in Portugal; performance assessmentand result-based financing in the Republic of Moldova). The crisis speeded upreforms in this area in some countries (Austria), but in others reforms wereresisted (Bulgaria, Hungary, the former Yugoslav Republic of Macedonia). InUkraine, a system of health services quality control has been developed, but hadno practical effect due to the lack of measures to deal with non-compliance.Planned changes to the legal status of health service providers in the RussianFederation affecting their payment mechanisms have been postponed until 2013.
Policy summary
24

Measures that target the supply side offer considerable scope for improvinghealth system functioning in comparison to those focused on curtailingutilization by patients. Changes in how health care is purchased and providersare reimbursed offer significant potential to enhance efficiency, quality andequity. Many EU countries have moved away from passive reimbursement ofproviders towards strategic purchasing, explicitly linking resource allocation to information on population health needs, cost–effectiveness and providerperformance (Figueras, Robinson & Jakubowski, 2005). Measures include theuse of health needs assessment, HTA, contracting, quality monitoring andperformance-based payment. In addition, most countries set case-based tariffscentrally, which may promote provider competition based on quality, wherequality information is available (Busse et al., 2011).
Volume and outcome contracts combined with prospective activity-basedpayments employing some case-mix measures, such as DRGs, have been linked to increased hospital efficiency. However, these types of contracts require sophisticated design in order to prevent gaming by providers, while the necessary information systems are in place in only a very few countries in Europe (Figueras, Robinson & Jakubowski, 2005). In physician payment,typically at the primary care level, fee-for-service and capitation have beenfound to be flawed methods for motivating physicians to achieve specific goals.Payment innovations that blend elements of fee-for-service, capitation and caserates can promote health system goals. These innovations include capitationwith fee-for-service carve-outs, department budgets with individual fee-for-service or “contact” capitation, and case rates for defined episodes of illness(Robinson, 2001). P4P is also growing in popularity, although evidence from the United States and the United Kingdom suggests policy-makers should pay careful attention to how any P4P scheme is designed and implemented(Maynard, 2008). In any provider payment reform, various other factors arelikely to influence successful implementation, including the way provision isorganized and regulation.
4.4.4 Overhead costs: restructuring the Ministry of Health andpurchasing agencies
Several governments are restructuring the Ministry of Health, statutory healthinsurance funds or other purchasing agencies in an attempt to reduce overheadcosts and increase efficiency (Bulgaria, Croatia, the Czech Republic, England,Iceland, Latvia, Lithuania, Portugal, Romania).
Reducing the number of civil servants or removing their employment conditions(tenure, pay, pensions) is one way of cutting public spending on health but risksloss of skilled staff and strike action by public sector workers, as demonstratedby recent trends across Europe (Parry, 2011). Depending on the context, it also
Health policy responses to the financial crisis in Europe
25

risks losing experienced personnel at a time of rapid reform, which requiresincreased, not decreased, capacity for planning and oversight.
Reforming health insurance market structure (e.g. by consolidating risk pools)can also reduce overhead costs (Kutzin, 2008; Thomson, Foubister & Mossialos,2009). In addition, addressing fragmented pooling may contribute significantlyto financial sustainability because a lower number of pools means less need for complex and resource-intensive risk adjustment and, by strengthening the power of purchasers in relation to providers, may lead to better (morestrategic) purchasing.
4.4.5 Provider infrastructure and capital investment
In many countries, the economic crisis created an impetus to: speed up theexisting process of restructuring the hospital sector through closures, mergersand centralization (Denmark, Greece, Latvia, Portugal, Slovenia); shift towardsoutpatient care (Belarus, Ireland, Greece, Lithuania); improve coordination with or investment in primary care (Armenia, Lithuania, Republic of Moldova,Netherlands); merge health centres (Iceland); and reorganize emergencymedical services (the former Yugoslav Republic of Macedonia). Some countriesabandoned (Romania) or stalled (Georgia) investment plans to build newhospitals, slowed modernization programmes involving upgrading of hospitaland ambulance services (Armenia) and purchasing of expensive equipment(Belarus), or reduced the share of capital expenditure (Ukraine). In contrast,some countries increased funding for modernization of public health providersusing resources from the mandatory health insurance fund (Republic ofMoldova) or developed e-health systems, with the implementation of anintegrated health management information system and electronic health card(Latvia, the former Yugoslav Republic of Macedonia) and a new electronicprescription system (Croatia).
The hospital sector absorbs a large part (35–70%) of national healthexpenditure in the European Region (Rechel et al., 2009). Most countries are in the process of reducing hospital capacity in order to increase efficiency byclosing unnecessary facilities and replacing expensive inpatient care with morecost–effective alternatives such as day surgery (McKee & Healy, 2002). Thesechanges have generally been shown to have no negative impact on quality ofcare. However, while they may enhance efficiency they do not necessarily lowerpublic spending, since savings are used elsewhere in the health system. Also,unidentified costs may be borne by patients and their carers and need to beadequately monitored (Clarke, 1996). To preserve quality of care, it is clear that reducing acute care capacity must be accompanied by investment inalternative services, such as community-based care (sometimes termed
Policy summary
26

“hospital reconfiguration”). In western Europe planning strategies have beenmore successful in this respect than market forces (Healy & McKee, 2002).
Some governments have sought to finance capital investment through greateruse of market competition, while others are opting for a publicly led approachto capital investment. The former approach, characterized by public–privatepartnerships (PPPs), has been highly problematic. It may act as a barrier tocollaboration between facilities offering complementary services to a definedpopulation, leading to fragmentation and duplication. Furthermore, PPPs donot generate new financial resources for the health sector but are simply a way of raising debt finance, often transferring risk to future generations. Thismay benefit governments that need to meet short-term fiscal targets but doesnot necessarily reduce costs or increase efficiency in the longer term (Rechel et al., 2009).
Reductions in hospital capacity reflect a growing emphasis on coordinatingprimary, secondary and tertiary care with a view to delivering care in lower-costsettings where possible and appropriate; expanding the scope of what can beprovided in lower-cost settings; and strengthening intra-system coordination toimprove quality and address the inefficiency effects of fragmentation in delivery(Saltman, Rico & Boerma, 2006; Figueras et al., 2008). GP gatekeeping is anestablished way of coordinating care, although caution is required to ensure itdoes not lead to unnecessary delays in obtaining specialist care when needed.Recent developments include primary care-based networks, nurse-led strategies(France, the Netherlands, Sweden, the United Kingdom), disease managementprogrammes, the use of multidisciplinary teams to support audit and qualitymonitoring, financing reforms to better integrate care involving risk-basedfunding or reallocation (Netherlands and Germany), bonuses for recruitingpatients (France) and paying providers for performance (France, the UnitedKingdom) (Nolte, Knai & McKee, 2008). Evidence of the effectiveness of suchreforms is inconclusive. In the key area of integration of care for people withchronic conditions, there is a lack of data on quality of care and patientoutcomes across different approaches and on transferability across differentsystems. The evidence does suggest that reforms cannot be relied on to yieldcost savings (Nolte & McKee, 2008).
5 Conclusions
The survey results indicate that European Region countries have employed amix of policy tools in response to the financial crisis. Some countries seem tohave used the crisis to try to increase efficiency, particularly in the hospital andpharmaceutical sectors, although little has been done to enhance value throughpolicies to improve public health, which is a missed opportunity.
Health policy responses to the financial crisis in Europe
27

To date, the breadth and scope of statutory coverage have largely beenunaffected. Some countries have actually expanded benefits for low-incomegroups, to strengthen access to health care. However, several countries havelowered coverage depth by increasing user charges for essential services, whichis a cause for concern. The international evidence suggests that user chargesdisproportionately affect low-income groups and regular users of care, and areunlikely to reduce public or total spending on health in the longer term due toreduced use of necessary care and, in some cases, increased use of free butmore resource-intensive services such as emergency care.
While research provides insight into the potential impact of many of the policiesadopted, each policy needs to be carefully evaluated in the context in which itis introduced, since both a given health system’s starting point and a specificpolicy’s design will play an important role in determining outcomes. To risksimplifying, policy options can be divided into two categories: those that arelikely to enhance efficiency and will not have an adverse impact on, or mayeven promote, other health system goals; and those that are likely to have more harmful effects.
Policy tools likely to promote health system goals:
• Increased risk pooling
• Strategic purchasing, where contracts are combined with accountabilitymechanisms including quality indicators, patient-reported outcomemeasures and other forms of feedback
• HTA to assist in setting priorities, combined with accountability, monitoring and transparency measures
• Controlled investment in the health sector, particularly for healthinfrastructure and expensive equipment
• Public health measures to reduce the burden of disease
• Price reductions for pharmaceuticals combined with cost–effectivenessevidence and other measures to promote rational prescribing anddispensing
• Shifting from inpatient to day-case or ambulatory care, where appropriate
• Integration and coordination of primary care and secondary care, and of health and social care
• Reducing administrative costs while maintaining capacity to manage the health system
• Fiscal policies to expand the public revenue base
Policy summary
28

• Counter-cyclical measures introduced before the onset of a health system shock
• Targeting financial protection measures towards poorer people and regularusers of health care.
Policy tools that risk undermining health system goals:
• Reducing the scope of essential services covered
• Reducing population coverage
• Increases in waiting times for needed services
• User charges for essential services
• Attrition of health workers caused by imbalances in salaries relative to therest of the economy and, where relevant, foreign labour markets.
This policy summary has highlighted the wide range of health policy responsesto the financial crisis across Europe and noted some of the trade-offs involved.The crisis has left a few countries with little or no choice but to introduce cuts.Where the short-term situation compels governments to cut public spending on health, the policy emphasis should be on cutting wisely to minimize adverse effects on health system performance, enhancing value and facilitatingefficiency-enhancing reforms in the longer run.
References
Albrecht M, Schiffhorst G, Kitzler C (2007). Finanzielle Auswirkungen undtypische Formen des Wechsels von Versicherten zwischen GKV und PKV. In: Klusen N, Meusch A, eds. Beiträge zum Gesundheitsmanagement. Baden-Baden, Nomos.
Andersson K et al. (2007). Impact of a generic substitution reform on patients’and society’s expenditure for pharmaceuticals. Health Policy, 81(2–3):376–384.
Atun RA (2004). What are the advantages and disadvantages of restructuring ahealth care system to be more focused on primary care services? Copenhagen,WHO Regional Office for Europe (Health Evidence Network report).
Atun RA, Bennett S, Duran A (2008). When do vertical (stand-alone)programmes have a place in health systems? Policy brief. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Bach P (2008). Cost sharing for health care – Whose skin? Which game? New England Journal of Medicine, 358:411–413.
Health policy responses to the financial crisis in Europe
29

Barr N (2004). The economics of the welfare state (4th edition). Oxford, Oxford University Press.
Braithwaite R, Rosen AB (2007). Linking cost sharing to value: an unrivalled yet unrealized public health opportunity. Annals of Internal Medicine,146(8):602–605.
Busse R et al., eds. (2011). Diagnosis-related groups in Europe: moving towards transparency, efficiency and quality in hospitals. Maidenhead, Open University Press.
Buzzelli C et al. (2006). Impact of generic substitution on pharmaceutical prices and expenditures in OECD countries. Journal of Pharmaceutical Finance,Economics and Policy, 15(1):41–63.
Catalano R, Bellows B (2005). Commentary: if economic expansion threatenspublic health, should epidemiologists recommend recession? InternationalJournal of Epidemiology, 34(6):1212–1213.
Chaloupka F, Warner W (2000). The economics of smoking. In: Cuyler AJ,Newhouse JP, eds. Handbook of Health Economics. Amsterdam, Elsevier.
Chang S et al. (2009). Was the economic crisis 1997–1998 responsible forrising suicide rates in East/Southeast Asia? A time-trend analysis for Japan,Hong Kong, South Korea, Taiwan, Singapore and Thailand. Social Science & Medicine, 68(7):1322–1331.
Chernew ME et al. (1998). Managed care, medical technology, and health carecost growth: a review of the evidence. Medical Care Research and Review,55(3):259–288.
Clarke A (1996). Why are we trying to reduce length of stay? Evaluation of thecosts and benefits of reducing time in hospital must start from the objectivesthat govern change. Quality in Health Care, 5(3):172–179.
Cylus J, Mladovsky P, McKee M (in press). Is there a statistical relationshipbetween economic crises and changes in government health expendituregrowth? An analysis of 24 European countries. Health Services Research[epub ahead of print].
Docteur E, Oxley H (2003). Health care systems – lessons from the reformexperience. Paris, OECD (OECD Health Working Papers No. 9).
Doetter LF, Gotze R (2011). Health care policy for better or for worse?Examining NHS reforms during times of economic crisis versus relative stability.Social Policy & Administration, 45(4):488–505.
Donatini A et al. (2001). Health care systems in transition: Italy. Copenhagen,European Observatory on Health Care Systems.
Policy summary
30

Dormont H, Grignon M, Huber H (2005). Health expenditures and thedemographic rhetoric: reassessing the threat of ageing. Lausanne, IEMS,Université de Lausanne (Working Paper No. 05-01).
Draborg E et al. (2005). International comparison of the definition and thepractical application of health technology assessment. International Journal of Technology Assessment in Health Care, 21:89–95.
Economou A, Nikolau A, Theodossiou I (2008). Are recessions harmful to healthafter all? Evidence from the European Union. Journal of Economic Studies,35:368–384.
Economou M et al. (2011). Increased suicidality amid economic crisis in Greece.Lancet, 378(9801):1459.
EMCDDA, ECDC (2011). HIV in injecting drug users in the EU/EEA, following a reported increase of cases in Greece and Romania. Lisbon, EuropeanMonitoring Centre for Drugs and Drug Addiction, European Centre for DiseasePrevention and Control (http://www.emcdda.europa.eu/publications/joint-publications/hiv-in-injecting-drug-users-2011, accessed 13 June 2012).
Ettelt S et al. (2007). The systematic use of cost–effectiveness criteria to informreviews of publicly funded benefits packages. Report commissioned by theDepartment of Health. London, London School of Hygiene & Tropical Medicine.
European Commission, Economic Policy Committee (AWG) (2010). Europeaneconomy. Joint report on health systems. Brussels, European Commission,Directorate-General for Economic and Financial Affairs (Occasional Papers 74)(http://ec.europa.eu/economy_finance/publications/occasional_paper/2010/pdf/ocp74_en.pdf, accessed 28 March 2012).
European Federation of Nurses Associations (2012). Caring in crisis. The impact of the financial crisis on nurses and nursing. A comparative overview of34 European countries. Brussels, European Federation of Nurses Associations.(http://www.efnweb.org/version1/en/documents/EFNReportontheImpactoftheFinancialCrisisonNursesandNursing-January2012.pdf, accessed 28 March 2012).
European Hospital and Healthcare Federation (2011). The crisis, hospitals andhealthcare. Brussels, HOPE Publications (http://www.hope.be/05eventsandpublications/docpublications/86_crisis/86_HOPE-The_Crisis_Hospitals_Healthcare_April_2011.pdf, accessed 13 June 2012).
Fahy N (2012). Who is shaping the future of European health systems? BritishMedical Journal, 344:e1712.
Figueras J, Lessof S, Srivastava D (2006). Managing paradox. In: Marinker M, ed.Constructive conversations about health: policy and values. Abingdon, Radcliffe.
Health policy responses to the financial crisis in Europe
31

Figueras J, Robinson R, Jakubowski E (2005). Purchasing to improve healthsystems performance: drawing the lessons. In: Figueras J, Robinson R,Jakubowski E, eds. Purchasing to improve health systems performance.Maidenhead, Open University Press:44–80.
Figueras J et al., eds. (2008). Health systems, health and wealth: assessing thecase for investing in health systems. Copenhagen, WHO Regional Office forEurope on behalf of the European Observatory on Health Systems and Policies.
Fishback P, Haines M, Kantor S (2007). Births, deaths, and New Deal reliefduring the Great Depression. Review of Economics and Statistics, 89(1):1–14.
Garber A (2000). Advances in cost–effectiveness analysis. In: Culyer AJ,Newhouse JP, eds. Handbook of Health Economics. Amsterdam, Elsevier.
Gemmill MC, Thomson S, Mossialos E (2008). What impact do prescriptiondrug charges have on efficiency and equity? Evidence from high-incomecountries. International Journal for Equity in Health, 7:12.
Gerdtham UG, Johannesson M (2005). Business cycles and mortality: results from Swedish microdata. Social Science & Medicine, 60(1):205–218.
Gerdtham UG, Ruhm CJ (2006). Deaths rise in good economic times: evidence from the OECD. Economic and Human Biology, 4(3):298–316.
Goetghebeur MM, Forrest S, Hay JW (2003). Understanding the underlyingdrivers of inpatient cost growth: a literature review. American Journal ofManaged Care, 9(1):3–12.
Harris CM, Scrivener G (1996). Fundholders’ prescribing costs: the first fiveyears. British Medical Journal, 313:1531–1534.
Healy J, McKee M (2002). The evolution of hospital systems. In: McKee M,Healy J, eds. Hospitals in a changing Europe. Buckingham, Open UniversityPress:14–35.
Hoel M, Sæther EM (2003). Public health care with waiting time: the role ofsupplementary private health care. Journal of Health Economics, 22:599–616.
Hopkins S (2006). Economic stability and health status: evidence from East Asiabefore and after the 1990s economic crisis. Health Policy, 75(3):347–357.
Joyce T, Mocan N (1993). Unemployment and infant health: time-series evidencefrom the state of Tennessee. Journal of Human Resources, 281:185–203.
Kaiser S, Mackenbach JP (2008). Public health in eight European countries: an international comparison of terminology. Public Health, 122(2):211–216.
Policy summary
32

Kaplan GA (2012). Economic crises: some thoughts on why, when and wherethey (might) matter for health – a tale of three countries. Social Science &Medicine, 74(5):643–646.
Kentikelenis A et al. (2011). Health effects of financial crisis: omens of a Greektragedy. Lancet, 378(9801):1457–1458.
Kutzin J (2008). Health financing policy: a guide for decision-makers.Copenhagen, WHO Regional Office for Europe (Health Financing Policy Paper2008/1).
Laurant M et al. (2005). Substitution of doctors by nurses in primary care.Cochrane Database System Review, (2):CD001271.
Lavis JN et al. (2007). Towards optimally packaged and relevance assessedhealth technology assessments. Report submitted to the Canadian Agency forDrugs and Therapeutics in Healthcare, Hamilton, McMaster University, Programin Policy Decision-Making.
Lohr K et al. (1986). Effect of cost sharing on use of medically effective and lesseffective care. Medical Care, 29:3–38, suppl. 39.
Lopez-Casasnovas G, Puig-Junoy J (2000). Review of the literature on referencepricing. Health Policy, 54(2):87–123.
McKee M, Healy J (2002). Hospitals in a changing Europe. Buckingham, OpenUniversity Press.
McKee M, Jacobson B (2000). Public health in Europe. Lancet, 356(9230):665–670.
McKee M, Basu S, Stuckler D (2012). Health systems, health and wealth: the argument for investment applies now more than ever. Social Science & Medicine, 74(5):684–687.
McKee M, Dubois CAD, Sibbald BS (2006). Changing professional boundaries.In: Dubois CAD, McKee M, Nolte E, eds. Human resources for health in Europe.Maidenhead, Open University Press:63–78.
Madianos M et al. (2011). Depression and economic hardship across Greece in2008 and 2009: two cross-sectional surveys nationwide. Social Psychiatry andPsychiatric Epidemiology, 46(10):943–952.
Manning WG et al. (1987). Health insurance and the demand for medical care: evidence from a randomized experiment. American Economic Review,77(3):251–277.
Maynard A (2008). Payment for performance (P4P): international experience anda cautionary proposal fo Estonia. Copenhagen, WHO Regional Office for Europe.
Health policy responses to the financial crisis in Europe
33

Mladovsky P et al. (2012). Health policy in the financial crisis. Eurohealth, 18:1.
Mossialos E, Srivastava D (2008). Pharmaceutical policies in Finland: challengesand opportunities. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Mossialos E, Thomson S (2004). Voluntary health insurance in the EuropeanUnion. Copenhagen, WHO Regional Office for Europe on behalf of theEuropean Observatory on Health Systems and Policies.
Mrazek M, Frank RG (2004). The off-patent pharmaceutical market. In:Mossialos E, Mrazek M, Walley T, eds. Regulating pharmaceuticals in Europe:striving for efficiency, equity and quality. Maidenhead, Open UniversityPress:260–278.
Newhouse JP, Rand Corporation Insurance Experiment Group (1993). Free forall? Lessons from the Rand health insurance experiment. Cambridge, MA,Harvard University Press.
Nink K, Schroder H, Selke GW (2001). Der Arzneimittelmarkt in der BDR. In:Schwabe U, Paffrath D, eds. Arzneiverordnungs-Report 2001. Berlin, Springer.
Nolte E, McKee M (2008). Integration and chronic care: a review. In: Nolte E,McKee M, eds. Caring for people with chronic conditions: a health systemperspective. Maidenhead, Open University Press:64–91.
Nolte E, Knai C, McKee M (2008). Managing chronic conditions – experience in eight countries. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
OECD (2006). Projecting OECD health and long-term care expenditures: whatare the main drivers? Paris, OECD (Economics Department Working Papers No. 477).
Office of Fair Trading (2007). The pharmaceutical price regulation scheme.London, Office of Fair Trading (Report No. 885).
Palmer S, Torgerson DJ (1999). Definitions of efficiency. British Medical Journal,318(7191):1136.
Pammolli F et al. (2008). Medical devices, competitiveness and impact on publichealth expenditure. Study prepared for DG Enterprise European Commission,University of Florence.
Parry R (2011). The public sector workforce in recession 2010–11 – the course of policy development in the Euro area and the UK. Paper for the annual conference of the Social Policy Association, Lincoln, 4–6 July 2011(http://www.social-policy.org.uk/lincoln2011/Parry%20P4.pdf, accessed 13 June 2012).
Policy summary
34

Rechel B et al. (2009). Conclusions and critical success factors. In: Rechel B et al.eds. Investing in hospitals of the future. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems andPolicies:249–264.
Robinson JC (2001). Theory and practice in the design of physician paymentincentives. Milbank Quarterly, 79(2):149–177, III.
Ruhm CJ (2000). Are recessions good for your health? Quarterly Journal ofEconomics, 115:617–650.
Ruhm CJ (2003). Good times make you sick. Journal of Health Economics,22(4):637–658.
Ruhm CJ (2008). A healthy economy can break your heart. Demography,44:829–848.
Saltman RB, Rico A, Boerma W (2006). Primary care in the driver’s seat?Organizational reform in European primary care. Maidenhead, Open UniversityPress.
Sassi F (2010). Obesity and the economics of prevention: fit not fat. Paris, OECD.
Schneider P (2009). Mitigating the impact of the economic crisis on publicsector health spending. Washington, DC, World Bank.
Schwappach DL, Boluarte TA, Suhrcke M (2007). The economics of primaryprevention of cardiovascular disease – a systematic review of economicevaluations. Cost Effective Resource Allocation, 5:5.
Sorenson C, Drummond M, Kanavos P (2008). Ensuring value for money inhealth care: the role of health technology assessment in the European Union.Copenhagen, WHO Regional Office for Europe on behalf of the EuropeanObservatory on Health Systems and Policies.
Srivastava D, Mladovsky P (2011). Health policy at a time of economic crisis.Research note produced for the EC as part of the Health and Living ConditionsNetwork of the European Observatory on the Social Situation and Demography.
Stuckler D, Basu S, McKee M (2010). Budget crises, health, and social welfareprogrammes. British Medical Journal, 340:c3311.
Stuckler D, King L, McKee M (2009). Mass privatisation and the post-communistmortality crisis: a cross-national analysis. Lancet, 373(9661):399–407.
Stuckler D, Meissner CM, King LP (2008). Can a bank crisis break your heart?Global Health, 4:1.
Health policy responses to the financial crisis in Europe
35

Stuckler D et al. (2009). The public health effect of economic crises andalternative policy responses in Europe: an empirical analysis. Lancet,374(9686):315–323.
Stuckler D et al. (2011a). Banking crises and mortality during the GreatDepression: evidence from US urban populations, 1929–1937. Journal of Epidemiology and Community Health, 66(5):410–419.
Stuckler D et al. (2011b). Effects of the 2008 recession on health: a first look at European data. Lancet, 378(9786):124–125.
Suhrcke M et al. (2011). The impact of economic crises on communicabledisease transmission and control: a systematic review of the evidence. PLoS One, 6(6):e20724.
Svensson M (2007). Do not go breaking your heart: do economic upturns reallyincrease heart attack mortality? Social Science & Medicine, 65(4):833–841.
Thomson S, Mossialos E (2006). Choice of public or private health insurance:learning from the experience of Germany and the Netherlands. Journal ofEuropean Social Policy, 16(4):315–327.
Thomson S, Mossialos E (2009). Private health insurance in the EuropeanUnion. Brussels, European Commission (DG Employment, Social Affairs andEqual Opportunities).
Thomson S, Foubister T, Mossialos E (2009). Financing health care in theEuropean Union. Challenges and policy responses. Copenhagen, WHO RegionalOffice for Europe on behalf of the European Observatory on Health Systemsand Policies.
Thomson S et al. (2009). Addressing financial sustainability in health systems.Copenhagen, WHO Regional Office for Europe on behalf of the EuropeanObservatory on Health Systems and Policies (Joint HEN-OBS policy summary 1).
Velasco-Garrido M, Busse R (2005). Health technology assessment: an introduction to objectives, role of evidence and structure in Europe.Copenhagen, WHO Regional Office for Europe on behalf of the EuropeanObservatory on Health Systems and Policies (Observatory policy briefs No. 8).
Wade R (2009). From global imbalances to global reorganisations. CambridgeJournal of Economics, 33:539–562.
Wagstaff A et al. (1992). Equity in the finance of health care: someinternational comparisons. Journal of Health Economics, 11(4):361–387.
Waters H, Saadah F, Pradhan M (2003). The impact of the 1997–98 East Asianeconomic crisis on health and health care in Indonesia. Health Policy Plan,18(2):172–181.
Policy summary
36

Weinstein M, Stason W (1977). Foundations of cost–effectiveness analysis forhealth and medical practices. New England Journal of Medicine, 296:716–721.
WHO (2000). World health report. Geneva, World Health Organization.
WHO (2004). The world medicines situation. Geneva, World Health Organization.
WHO (2006). World health report: working together for health. Geneva, WorldHealth Organization.
WHO (2010). World health report. Health systems financing: the path touniversal coverage. Geneva, World Health Organization.
WHO (2011) [WHO Statistical Information System (WHOSIS)]. Geneva, WorldHealth Organization (http://www.who.int/whosis/en, accessed 12 April 2012).
WHO (2012) [WHO Statistical Information System (WHOSIS)]. Geneva, WorldHealth Organization (http://www.who.int/whosis/en, accessed 12 April 2012).
WHO Regional Office for Europe (2008). The Tallinn Charter: health systems for health and wealth. Copenhagen, WHO Regional Office for Europe(www.euro.who.int/__data/assets/pdf_file/0008/88613/E91438.pdf, accessed26 March 2012).
WHO Regional Office for Europe (2009). Health in times of global economiccrisis: implications for the WHO European Region – overview of the situation in the WHO European Region. Copenhagen, WHO Regional Office for Europe.
WHO Regional Office for Europe (2011a). Health for All database [online/offline database]. Copenhagen, WHO Regional Office for Europe(http://data.euro.who.int/hfadb/, accessed 8 August 2011).
WHO Regional Office for Europe (2011b). Section IV. Sustaining equity, solidarity and health gain in the context of the financial crisis. In: Interim report on implementation of the Tallinn Charter. Copenhagen, WHO RegionalOffice for Europe.
WHO Regional Office for Europe (2012). Health for All database [online/offline database]. Copenhagen, WHO Regional Office for Europe(http://data.euro.who.int/hfadb/, accessed 11 April 2012).
Wismar M et al. (2011). Health professional mobility and health systems:evidence from 17 European countries. Euro Observer, 13(2).
World Bank (2009). Protecting pro-poor health services during financial crises.Lessons from experience. Washington, DC, World Bank.
Health policy responses to the financial crisis in Europe
37

Policy summary
38
An
nex
1
Tab
le A
.1. P
olic
ies
targ
etin
g f
inan
cial
co
ntr
ibu
tio
ns
to t
he
hea
lth
sys
tem
in t
he
con
text
of
the
eco
no
mic
cri
sis,
W
HO
Eu
rop
ean
Reg
ion
No
tes:
No
info
rmat
ion
was
ava
ilabl
e fo
r A
ndor
ra, K
azak
hsta
n, L
uxem
bour
g, M
onac
o, M
onte
negr
o, S
an M
arin
o, T
ajik
ista
n an
d Tu
rkm
enis
tan.
Text
not
in it
alic
s in
dica
tes
a po
licy
whi
ch w
as d
efin
ed b
y th
e re
leva
nt a
utho
ritie
s in
the
cou
ntry
as
a re
spon
se t
o th
e cr
isis
. Tex
t in
ital
ics
indi
cate
s a
polic
y w
hich
was
eith
er p
artia
lly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed b
efor
e th
e cr
isis
but
impl
emen
ted
afte
r w
ithgr
eate
r/le
ss s
peed
/inte
nsity
tha
n pl
anne
d; o
r po
ssib
ly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed a
nd im
plem
ente
d si
nce
the
star
t of
th
e cr
isis
, but
not
def
ined
by
the
rele
vant
aut
horit
ies
as a
res
pons
e to
the
cris
is. A
bla
nk c
ell i
ndic
ates
no
polic
y re
spon
se t
o th
e cr
isis
(n
ot n
o re
spon
se t
o th
e su
rvey
).
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Alb
ania
Ther
e h
ave
bee
n s
om
e sm
all
red
uct
ion
s in
th
e ex
tern
alfi
nan
cial
ass
ista
nce
pro
vid
edto
Alb
ania
sin
ce t
he
star
t o
f th
e cr
isis
. Ho
wev
er,
acco
rdin
g t
o t
he
Min
istr
y o
fH
ealt
h t
her
e h
ave
bee
n n
om
ajo
r co
nse
qu
ence
s in
th
eh
ealt
h s
ecto
r as
a r
esu
lt
and
pu
blic
hea
lth
car
eex
pen
dit
ure
as
a p
erce
nta
ge
of
the
ove
rall
bu
dg
et (
i.e.
7.6%
in 2
008,
8.1
% in
200
9)an
d a
s a
per
cen
tag
e o
fg
ross
do
mes
tic
pro
du
ct(G
DP)
(i.e
. 2.5
% in
200
8 an
d 2
.7%
in 2
009)
hav
eb
een
rea
son
ably
sta
ble
si
nce
at
leas
t 20
06.

Health policy responses to the financial crisis in Europe – Annexes
Arm
enia
Dat
a fr
om
th
e N
atio
nal
Hea
lth
Acc
ou
nts
(N
HA
)sh
ow
th
at a
lth
ou
gh
GD
Pan
d t
ota
l go
vern
men
tsp
end
ing
bo
th in
crea
sed
in
ab
solu
te t
erm
s in
200
8co
mp
ared
to
200
7, p
ub
licex
pen
dit
ure
s o
n h
ealt
h f
ell
sig
nif
ican
tly
fro
m A
MD
66
bill
ion
to
AM
D 5
3 b
illio
n.
This
red
uct
ion
was
du
e to
the
eco
no
mic
cri
sis
and
was
con
trar
y to
th
e g
oal
s o
f th
eg
ove
rnm
ent’
s h
ealt
h p
olic
yto
incr
ease
pu
blic
fu
nd
sal
loca
ted
to
th
e h
ealt
hse
cto
r an
d t
he
Pove
rty
Red
uct
ion
Str
ateg
y ad
op
ted
by
the
go
vern
men
t fo
r th
ep
erio
d 2
004–
2015
.
In 2
011,
th
eg
ove
rnm
ent
intr
od
uce
d p
atie
nt
co-p
aym
ents
fo
r a
ran
ge
of
serv
ices
no
min
ally
co
vere
du
nd
er t
he
stat
uto
ryb
enef
its
pac
kag
e. A
maj
or
mo
tiva
tio
n is
to
incr
ease
go
vern
men
tre
ven
ues
, as
ho
spit
als
wer
e se
en b
y th
eM
inis
try
of
Fin
ance
as
a m
ajo
r ar
ea o
f th
e “b
lack
eco
no
my”
.H
ence
fo
rmal
izin
gu
no
ffic
ial p
aym
ents
is
th
e g
oal
.
Au
stri
aTh
e A
ust
rian
Min
istr
y o
fH
ealt
h in
tro
du
ced
th
eA
ust
rian
Hea
lth
Fu
nd
La
w in
Sep
tem
ber
200
9 to
safe
gu
ard
th
e re
ven
ues
of
sick
nes
s fu
nd
s an
d p
reve
nt
them
fro
m p
lun
gin
g
furt
her
into
deb
t d
ue
to
the
eco
no
mic
do
wn
turn
.Th
e H
ealt
h F
un
d m
easu
res
incl
ud
e an
an
nu
alg
ove
rnm
ent
cash
su
bsi
dy
for
the
sick
nes
s fu
nd
s to
hel
p b
alan
ce t
he
bu
dg
etan
d a
lso
req
uir
e si
ckn
ess
fun
ds
to c
ut
cost
s. T
he
go
vern
men
t co
ntr
ibu
tio
n t
oth
e H
ealt
h F
un
d w
as s
et a
t
In a
mea
sure
aim
ing
to o
ffer
fin
anci
alre
lief
to s
oci
ally
vuln
erab
le p
olic
yh
old
ers,
as
of
1Ja
nu
ary
2008
ace
ilin
g w
as s
et o
np
resc
rip
tio
n f
ees,
targ
eted
esp
ecia
lly
at p
eop
le w
ith
hig
hd
rug
nee
ds
and
low
inco
mes
. Un
der
th
en
ew la
w, a
cap
is s
etat
2%
of
an in
sure
dp
erso
n’s
an
nu
al n
etin
com
e sp
ent
on
pre
scri
pti
on
dru
gco
sts,
aft
er w
hic
h t
he
39

Policy summary
40
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Au
stri
a (c
on
t.)
EUR
100
mill
ion
in 2
009
bu
tin
201
1 it
was
cu
t to
EU
R 4
0m
illio
n d
ue
to b
ud
get
con
solid
atio
n a
s a
resu
lt o
fth
e cr
isis
. Th
e g
ove
rnm
ent
has
ple
dg
ed t
o c
on
trib
ute
EUR
40
mill
ion
an
nu
ally
thro
ug
h t
o f
isca
l yea
r 20
14b
ut
it r
emai
ns
to b
e se
enw
het
her
th
e p
olic
y w
illco
nti
nu
e af
ter
that
.
A D
ebt
Forg
iven
ess
Law
w
as a
lso
intr
od
uce
d t
o
wri
te o
ff d
ebts
acc
um
ula
ted
by
the
fun
ds
wit
h y
earl
yin
stal
men
ts o
f EU
R 1
50m
illio
n b
etw
een
201
0 an
d 2
012.
As
par
t o
f th
e H
ealt
h F
un
dla
w, t
he
Fed
erat
ion
of
Soci
alH
ealt
h In
sura
nce
Fu
nd
s w
asre
qu
ired
to
su
bm
it a
ro
adm
ap f
or
cost
-co
nta
inm
ent
effo
rts
in n
ego
tiat
ion
wit
hp
rovi
der
s, e
spec
ially
th
ed
oct
ors
ass
oci
atio
n.
insu
red
per
son
isex
emp
t fr
om
all
pre
scri
pti
on
dru
gch
arg
es f
or
the
rem
ain
der
of
the
cale
nd
ar y
ear.
Init
ial c
alcu
lati
on
s b
y th
e Fe
der
atio
n
of
Soci
al H
ealt
hIn
sura
nce
Fu
nd
sp
red
icte
d t
hat
th
en
ew e
xem
pti
on
wo
uld
ben
efit
app
roxi
mat
ely
300
000
peo
ple
. Giv
enth
e re
ven
ue
loss
es
for
stat
uto
ry h
ealt
hin
sura
nce
th
ere
isu
nce
rtai
nty
ove
r th
esu
stai
nab
ility
of
the
po
licy
in li
gh
t o
f th
eec
on
om
ic d
ow
ntu
rn.
It a
lso
rem
ain
s to
be
seen
wh
eth
er t
he
go
vern
men
t w
illco
mp
ensa
te s
oci
alin
sura
nce
fo
r th
ere
ven
ue
loss
es a
nd
wh
o w
ill u
ltim
atel
yp
ay f
or
the
cap
.

Health policy responses to the financial crisis in Europe – Annexes
Aze
rbai
jan
Del
ay in
imp
lem
enta
tio
n
of
maj
or
hea
lth
fin
anci
ng
refo
rm, i
ncl
ud
ing
intr
od
uct
ion
of
man
dat
ory
hea
lth
insu
ran
ce. I
n J
anu
ary
2008
, bef
ore
th
e cr
isis
beg
an, t
he
Pres
iden
t o
fA
zerb
aija
n s
ign
ed t
he
dec
ree
app
rovi
ng
“T
he
Co
nce
pt
for
Hea
lth
Fin
anci
ng
Ref
orm
an
dIn
tro
du
ctio
n o
f M
and
ato
ryH
ealt
h In
sura
nce
fo
r 20
08–2
012”
. Th
e C
on
cep
td
escr
ibed
ove
rall
app
roac
hes
to
hea
lth
fin
anci
ng
ref
orm
inA
zerb
aija
n, i
ncl
ud
ing
th
e es
tab
lish
men
t o
f an
ind
epen
den
t si
ng
le-p
ayer
agen
cy u
nd
er t
he
Cab
inet
o
f M
inis
ters
, in
tro
du
cin
gn
ew p
rovi
der
pay
men
tm
ech
anis
ms
and
per
cap
ita
allo
cati
on
of
hea
lth
car
efu
nd
s. In
Au
gu
st 2
008,
th
e C
abin
et o
f M
inis
ters
app
rove
d t
he
Act
ion
Pla
nfo
r im
ple
men
tati
on
of
the
Co
nce
pt.
Ho
wev
er,
to d
ate
it h
as n
ot
bee
nim
ple
men
ted
. Th
e cr
isis
mig
ht
hav
e af
fect
ed t
oso
me
exte
nt
the
will
ing
nes
so
f th
e g
ove
rnm
ent
tola
un
ch t
he
refo
rms,
bu
t th
is is
no
t th
e m
ain
sta
ted
reas
on
fo
r th
e st
alem
ate.
41

Policy summary
42
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Bel
aru
sA
list
of
med
ical
serv
ices
exe
mp
t fr
om
val
ue
add
ed
tax
(VA
T) h
as b
een
app
rove
d.
In 2
009
the
tax
syst
em in
Bel
arus
chan
ged
fro
m o
ne
wit
h m
arg
inal
rat
esto
on
e w
ith
a f
lat
rate
of
12.0
% o
fsa
lary
.
Fro
m 2
009,
th
eg
ove
rnm
ent
has
b
een
inve
stig
atin
gu
ser
char
ges
po
licie
sas
a w
ay o
f ra
isin
gre
ven
ue.
Incr
ease
in e
xpo
rt
of
hig
h-t
ech
med
ical
serv
ices
to
rai
seg
ove
rnm
ent
reve
nu
es (
in 2
010
reac
hin
g U
SD 1
8.6
mill
ion
, exc
eed
ing
the
exp
ecte
d a
mo
un
tb
y U
SD 3
.1 m
illio
n).
Bel
giu
mG
iven
th
e cu
rren
t ec
on
om
icsi
tuat
ion
, th
ere
was
ad
ebat
e o
n w
het
her
to
resp
ect
the
ann
ual
gro
wth
no
rm o
f 4.
5% t
hat
was
esta
blis
hed
in 2
004,
th
efi
nal
dec
isio
n t
aken
was
in
fav
ou
r o
f “p
rote
ctin
g”
the
hea
lth
car
e b
ud
get
.
Enla
rgem
ent
of
the
gro
up
en
titl
ed
to in
crea
sed
reim
bu
rsem
ent
of
hea
lth
car
e ex
pen
ses:
fro
m 2
007,
low
-in
com
e fa
mili
es
(or
ind
ivid
ual
s) a
reel
igib
le. I
n 2
011
the
inco
me
ceili
ng
was
fixe
d a
t EU
R 1
5 16
3.96
and
incr
ease
d b
y EU
R 2
807.
26 f
or
each
add
itio
nal
fam
ilym
emb
er. N
ewre
imb
urs
emen
ts f
or
pat
ien
ts w
ith
cer
tain
chro
nic
co
nd
itio
ns
wer
e al
so in
tro
du
ced
.
Bo
snia
an
dH
erze
go
vin
a

Health policy responses to the financial crisis in Europe – Annexes
43
Bu
lgar
iaTh
e M
inis
try
of
Hea
lth
bu
dg
et r
edu
ced
fro
mB
GN
713
mill
ion
in 2
008
toB
GN
537
mill
ion
in 2
009
and
BG
N 5
70 m
illio
n in
201
0.
Plan
ned
NH
IF (
Nat
ion
alH
ealt
h In
sura
nce
Fu
nd
)re
ven
ues
in 2
009
wer
e B
GN
2.4
7 m
illio
n b
ut
on
ly B
GN
2.2
1 m
illio
n
was
co
llect
ed. P
lan
ned
exp
end
itu
res
wer
e B
GN
2.0
7 m
illio
n b
ut
real
exp
end
itu
res
wer
e B
GN
1.7
5 m
illio
n.
The
go
vern
men
t in
crea
sed
the
soci
al h
ealt
h in
sura
nce
(SH
I) c
on
trib
uti
on
rat
e fr
om
6% t
o 8
% o
f in
com
e in
2009
. Th
e ad
dit
ion
al in
com
ew
as t
ran
sfer
red
into
are
serv
e fu
nd
to
pay
fo
rh
ealt
h in
sura
nce
ref
orm
–th
e g
ove
rnm
ent
pro
po
sed
com
pu
lso
ry in
sura
nce
pro
vid
ed b
y p
riva
te f
un
ds.
Ho
wev
er t
his
po
licy
was
un
po
pu
lar
wit
h t
he
pu
blic
and
do
cto
rs u
nio
ns
and
was
reje
cted
by
the
new
go
vern
men
t, w
hic
h w
ish
edto
ret
ain
co
ntr
ol o
f p
ub
licre
sou
rces
an
d in
stit
uti
on
sth
rou
gh
th
e N
HIF
. In
201
1th
e g
ove
rnm
ent
agre
ed
to u
se t
he
extr
a fu
nd
ing
dir
ectl
y o
n h
ealt
h s
ervi
ces
and
acc
epte
d a
bal
ance
db
ud
get
fo
r th
e N
HIF
(i.e
. to
spen
d a
ll th
e fu
nd
s ra
ised
).

Policy summary
44
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Cro
atia
Go
vern
men
t d
ebt
for
hea
lth
exp
end
itu
res
amo
un
ted
to
HR
K 4
.8 b
illio
n in
200
8; t
he
go
al t
hu
s b
ecam
e to
red
uce
the
def
icit
an
d e
nsu
re t
hat
spen
din
g is
fin
ance
d o
nly
fro
m r
even
ues
, wit
h n
ewb
orr
ow
ing
on
ly t
o c
ove
rp
revi
ou
s lia
bili
ties
. By
the
end
of
2010
, th
e g
ove
rnm
ent
had
red
uce
d t
he
bu
dg
et f
or
hea
lth
by
HR
K 1
.5 b
illio
n(w
ith
un
pai
d d
ebt
red
uce
db
y al
mo
st 2
0%).
In 2
011,
to
red
uce
th
ed
efic
it, t
he
go
vern
men
tp
asse
d n
ew le
gis
lati
on
o
n f
isca
l res
po
nsi
bili
ty(i
ncl
ud
ing
in t
he
hea
lth
sect
or)
in o
rder
to
en
sure
that
sp
end
ing
is f
inan
ced
on
ly b
y re
ven
ues
an
d n
ewb
orr
ow
ing
is o
nly
to
co
ver
pre
vio
us
liab
iliti
es o
r fo
rd
evel
op
men
t. O
ffic
e-h
old
ers
fro
m s
tate
leve
l to
loca
lle
vel i
n C
roat
ia w
ill h
ave
to o
ffer
th
eir
resi
gn
atio
n
if it
is e
stab
lish
ed t
hat
th
ey
hav
e b
reac
hed
th
e fi
scal
acco
un
tab
ility
leg
isla
tio
n.
Acc
ord
ing
to
th
e le
gis
lati
on
,th
e to
tal e
xpen
dit
ure
of
the
gen
eral
bu
dg
et (
the
go
vern
men
t’s
bu
dg
et
plu
s b
ud
get
s o
f lo
cal s
elf-
Intr
od
uce
d in
201
1:
– h
ealt
h c
are
con
trib
uti
on
so
n p
ensi
on
s (w
ith
dif
fere
nti
atio
n r
elat
ive
to t
he
pen
sio
n a
mo
un
t)
– sp
ecia
l co
ntr
ibu
tio
ns
rela
ted
to
hig
h-r
isk
beh
avio
urs
(“h
ealt
h t
ax
on
to
bac
co”)
– re
imb
urs
emen
t o
f co
sts
of
med
ical
tre
atm
ent
for
traf
fic
acci
den
ts f
rom
insu
ran
ce c
om
pan
ies
– co
-pay
men
t in
pri
mar
yh
ealt
h c
are;
co
-pay
men
tp
er p
resc
rip
tio
n
– in
com
e fr
om
sup
ple
men
tary
hea
lth
insu
ran
ce.
Co
-pay
men
ts h
ave
bee
n r
edu
ced
fro
mH
RK
15
in 2
009
toH
RK
10
for
pri
mar
yca
re v
isit
s an
dp
resc
rip
tio
ns.
Sup
ple
men
tary
hea
lth
insu
ran
cep
rem
ium
s in
crea
sed
in 2
010,
dep
end
ing
on
inco
me:
an
insu
red
per
son
(em
plo
yee)
wit
h a
mo
nth
ly s
alar
y o
rin
com
e o
f m
ore
th
an H
RK
510
8 p
ays
HR
K13
0 p
er m
on
thin
stea
d o
f H
RK
80;
an
insu
red
per
son
(pen
sio
ner
) w
ith
a
mo
nth
ly p
ensi
on
o
r in
com
e o
f m
ore
than
HR
K 5
108
pay
sH
RK
80
per
mo
nth
inst
ead
of
HR
K 5
0.C
erta
in c
ateg
ori
es o
fin
sura
nce
are
exe
mp
tfr
om
pay
men
t(d
epen
ds
on
: hea
lth
stat
us,
eco
no
mic
stat
us,
ag
e, e
tc.)
.

Health policy responses to the financial crisis in Europe – Annexes
go
vern
men
t u
nit
s an
dfi
nan
cial
pla
ns
for
extr
a-b
ud
get
ary
use
rs)
is t
o b
ere
du
ced
an
nu
ally
by
on
ep
erce
nta
ge
po
int
of
the
pro
ject
ed G
DP.
Cyp
rus
Cze
ch R
epu
blic
Dec
reas
e in
Min
istr
y o
f H
ealt
h b
ud
get
by
CZK
200
0 m
illio
n (
abo
ut
30%
dec
reas
e) in
201
0co
mp
ared
to
200
8.
Ther
e w
as a
slig
ht
incr
ease
in S
HI r
even
ues
fro
m 2
008
to 2
011
du
e to
use
of
fin
anci
al r
eser
ves.
Incr
ease
of
pre
miu
ms
for
self
-em
plo
yed
(eq
ual
izat
ion
of
curr
ent
dis
par
itie
s w
ith
emp
loye
es)
and
cei
ling
fo
r p
rem
ium
pay
men
tssl
igh
tly
rais
ed t
o in
crea
seco
ntr
ibu
tio
n o
f h
igh
ear
ner
sp
lan
ned
fo
r 20
12/2
013.
Incr
ease
of
use
rch
arg
es f
or
inp
atie
nt
stay
fro
m C
ZK 6
0 to
CZK
100
per
day
inh
osp
ital
pla
nn
ed f
or
2012
. A la
w is
pla
nn
edfo
r 20
12 w
hic
h w
illin
tro
du
ce t
he
po
ssib
ility
of
char
gin
gco
-pay
men
ts f
or
mo
re“l
uxu
rio
us”
car
e,w
hic
h w
ill b
e o
f th
esa
me
qu
alit
y as
th
est
and
ard
car
e p
rovi
ded
un
der
SH
I bu
t w
ith
bet
ter
(ho
tel-
typ
e)am
enit
ies.
The
Min
istr
y o
f H
ealt
hcu
t re
imb
urs
emen
tra
te o
f d
rug
s b
yin
sura
nce
fu
nd
s b
y7%
bet
wee
n 2
009
and
201
1. T
his
can
resu
lt in
an
incr
ease
of
co-p
aym
ents
by
pat
ien
ts if
th
eim
po
rter
/pro
du
cer
do
es n
ot
red
uce
th
ew
ho
lesa
le p
rice
.
45

Policy summary
46
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Den
mar
kC
on
tin
ued
gro
wth
in h
ealt
hca
re b
ud
get
s b
y D
KK
5b
illio
n t
hro
ug
h 2
011–
2013
fin
ance
d in
par
t th
rou
gh
cro
ss-s
ub
sid
izat
ion
of
the
hea
lth
bu
dg
et f
rom
th
eed
uca
tio
n b
ud
get
.
Fro
m 2
011,
intr
od
uct
ion
of
use
rch
arg
es f
or
in v
itro
fert
iliza
tio
n.
Esto
nia
The
hea
lth
insu
ran
ce b
ud
get
on
hea
lth
car
e (t
emp
ora
rysi
ck le
ave
ben
efit
s ex
clu
ded
)d
ecre
ased
by
1% in
200
9co
mp
ared
to
200
8, w
hic
hw
as a
chie
ved
by
usi
ng
colle
cted
res
erve
s to
fill
th
eg
ap b
etw
een
rev
enu
es a
nd
exp
end
itu
res.
Th
e M
inis
try’
sh
ealt
h e
xpen
dit
ure
red
uce
db
y 24
% in
200
9 co
mp
ared
to 2
008.
Th
is w
as p
arti
ally
ach
ieve
d t
hro
ug
h c
utt
ing
adm
inis
trat
ive
cost
s an
dcu
ttin
g t
he
pu
blic
hea
lth
bu
dg
et f
rom
200
9.
Cu
ts f
ocu
sed
on
no
nco
mm
un
icab
le d
isea
ses
(NC
Ds)
an
d p
rog
ram
mes
o
n c
om
mu
nic
able
dis
ease
sw
ere
pro
tect
ed. E
uro
pea
nU
nio
n (
EU)
soci
al f
un
ds
wer
e u
sed
to
co
mp
ensa
tefo
r th
e re
du
ctio
n in
NC
Db
ud
get
bu
t th
ese
fun
ds
will
no
lon
ger
be
avai
lab
lefr
om
201
2.
In 2
009
the
dec
reas
e in
SH
Ire
ven
ues
was
11%
an
d in
2010
5%
, du
e to
incr
ease
du
nem
plo
ymen
t an
dd
ecre
ased
sal
arie
s.
Esto
nia
n H
ealt
h In
sura
nce
Fun
d (
EHIF
) ac
cum
ula
ted
sub
stan
tial
res
erve
s b
efo
reth
e cr
isis
. Th
e g
ove
rnm
ent
did
no
t al
low
th
ese
rese
rves
to b
e d
eple
ted
du
rin
g t
he
init
ial p
erio
d o
f th
e cr
isis
,b
ut
late
r th
ese
rese
rves
wer
e g
rad
ual
ly u
sed
to
com
pen
sate
fo
r th
ed
ecre
asin
g r
even
ues
o
f th
e EH
IF.
15%
co
-in
sura
nce
rat
efo
r n
urs
ing
inp
atie
nt
care
was
intr
od
uce
dfr
om
201
0.

Health policy responses to the financial crisis in Europe – Annexes
47
Fin
lan
dU
ser
char
ges
fo
rp
ub
lic h
ealt
h s
ervi
ces
rais
ed b
y 10
% in
201
0(u
ser
char
ges
are
revi
sed
eve
ry s
eco
nd
year
bas
ed o
n t
he
pu
blic
pen
sio
ns
ind
ex).
An
incr
easi
ng
nu
mb
ero
f m
un
icip
alit
ies
are
intr
od
uci
ng
ser
vice
vou
cher
s. T
he
incr
ease
d u
se o
fse
rvic
e vo
uch
ers
isex
pec
ted
to
mit
igat
ep
ub
lic s
ecto
r co
stp
ress
ure
s an
din
crea
se t
he
free
do
mo
f ch
oic
e o
f th
e u
sers
of
serv
ices
. Acc
ord
ing
to a
su
rvey
co
nd
uct
edb
y Si
tra
and
th
eA
sso
ciat
ion
of
Fin
nis
hLo
cal a
nd
Reg
ion
alA
uth
ori
ties
, ser
vice
vou
cher
s ar
ep
arti
cula
rly
use
d f
or
soci
al s
ervi
ces.
Th
eir
intr
od
uct
ion
fo
r u
sein
hea
lth
car
e se
rvic
esw
as p
lan
ned
fo
r 20
11.
Fran
ceSi
nce
th
e ec
on
om
ic c
risi
s,th
e h
ealt
h b
ud
get
has
incr
ease
d s
har
ply
an
d
the
def
icit
has
ris
en f
rom
EUR
4.4
bill
ion
in 2
008
toEU
R 1
0.6
bill
ion
in 2
009.
Th
eh
ealt
h b
ud
get
am
ou
nte
d t
oEU
R 1
1.9
bill
ion
in 2
010
and
was
pla
nn
ed t
o b
e re
du
ced
to E
UR
11.
3 b
illio
n in
201
1.In
201
0 th
e to
tal i
ncr
ease
inh
ealt
h s
pen
din
g w
as 3
.2%
com
par
ed t
o 2
009.
Th
ein
crea
se in
th
e d
efic
it is
Follo
win
g t
he
chan
ge
in t
he
law
in20
07, t
he
allo
cati
on
of
reve
nu
es f
rom
tob
acco
tax
in 2
009
was
incr
ease
d a
nd
is
no
w p
aid
to
th
eh
ealt
h in
sura
nce
bu
dg
et a
t a
rate
o
f 98
.75%
.
Incr
ease
in a
new
con
trib
uti
on
th
at
is a
pp
lied
on
so
me
reve
nu
es (
“fo
rfai
t
Sin
ce 2
008
new
co
-pay
men
ts f
or
pre
scri
pti
on
dru
gs,
do
cto
r vi
sits
an
dam
bu
lan
ce t
ran
spo
rtar
e n
ot
reim
bu
rsab
leb
y p
riva
te v
olu
nta
ryh
ealt
h in
sura
nce
.
The
soci
al s
ecu
rity
bu
dg
et o
f N
ove
mb
er20
10 in
clu
ded
th
efo
llow
ing
mea
sure
s to
incr
ease
rev
enu
es:
a d
ecre
ase
fro
m 3
5%

Policy summary
48
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Fran
ce (
con
t.)
linke
d b
oth
wit
h h
igh
erex
pen
ses
and
low
erre
ven
ues
fro
m t
ax (
e.g
.G
ener
al S
oci
al C
on
trib
uti
on
,th
e in
com
e ta
x ea
rmar
ked
for
soci
al s
ecu
rity
sp
end
ing
).In
201
1 th
e p
lan
nin
gb
ud
get
ary
assu
mp
tio
n
was
th
at e
xpen
ses
for
hea
lth
wo
uld
incr
ease
ove
rall
by
2.9%
inco
mp
aris
on
wit
h 2
010.
The
soci
al s
ecu
rity
bu
dg
et
of
No
vem
ber
201
0 in
clu
ded
a n
um
ber
of
mea
sure
s to
red
uce
co
sts
and
incr
ease
reve
nu
es. I
t w
as a
nti
cip
ated
that
sav
ing
s in
201
1 in
hea
lth
exp
ense
s w
ou
ldre
ach
EU
R 2
bill
ion
.
soci
al s
ur
l’ép
arg
ne
sala
rial
e”),
wh
ich
was
set
up
in 2
009
and
wh
ose
rat
e h
asin
crea
sed
fro
m 2
% in
2009
to
4%
in 2
010
and
6%
in 2
011.
Tax
and
so
cial
con
trib
uti
on
re
liefs
hav
e b
een
intr
od
uce
d s
ince
2007
to
pro
mo
teem
plo
ymen
t.
to 3
0% o
f th
e ra
te
of
reim
bu
rsem
ent
of
ph
arm
aceu
tica
ls; a
dec
reas
e fr
om
65%
to
60%
fo
r th
e ra
te
of
reim
bu
rsem
ent
of
med
ical
pro
ced
ure
s.Th
is c
om
es in
ad
dit
ion
to t
he
incr
ease
fro
mEU
R 1
6 to
EU
R 1
8 p
erd
ay f
or
the
pat
ien
t’s
con
trib
uti
on
to
a s
tay
in h
osp
ital
th
at w
asin
tro
du
ced
in 2
010.
In a
dd
itio
n, F
ren
chst
atu
tory
hea
lth
insu
ran
ce h
as a
pp
lied
a n
ew r
ule
sin
ce 2
009
that
pen
aliz
es p
atie
nts
wh
o d
o n
ot
follo
wth
e ag
reed
med
ical
pat
hw
ay b
y in
crea
sin
gth
eir
co-p
aym
ent
con
trib
uti
on
by
40%
.
Geo
rgia
Wh
ile t
he
stat
e b
ud
get
fo
r th
e h
ealt
h s
ecto
r g
rew
ever
y ye
ar s
ince
200
6,
the
bu
dg
et f
or
2011
was
red
uce
d b
y 7.
9% c
om
par
edto
201
0.
Exp
ansi
on
of
hea
lth
insu
ran
ce f
or
the
po
or
(co
ntr
ibu
tio
ns
by
the
go
vern
men
t); f
or
som
ep
ub
lic s
ecto
r em
plo
yees
(fu
nd
ed b
y g
ove
rnm
ent)
and
vo
lun
tary
hea
lth
insu
ran
ce (
stat
e-su
bsi
diz
edfo
r lo
w-i
nco
me
fam
ilies
).Pr
emiu
ms
for
the
Med
ical
Insu
ran
ce P
rog
ram
me
(MIP
)
Exp
ansi
on
of
size
of
self
-in
sure
d e
nro
lled
in p
rep
aid
ris
k p
oo
lsth
rou
gh
intr
od
uct
ion
of
Vo
lun
tary
Hea
lth
Insu
ran
ce (
VH
I) –
in20
09 t
he
shar
e o
fp
op
ula
tio
n e
nro
lled
in t
hes
e sc
hem
esre
ach
ed 9
.7%
.

Health policy responses to the financial crisis in Europe – Annexes
49
are
fully
pai
d b
y th
eg
ove
rnm
ent
and
pu
rch
ased
fro
m p
riva
te in
sura
nce
com
pan
ies.
In 2
011
the
go
vern
men
t re
du
ced
bu
dg
et a
lloca
tio
ns
for
MIP
as a
res
ult
of
insu
ran
cep
rem
ium
op
tim
izat
ion
.
In 2
010,
a n
atio
nal
su
rvey
esti
mat
ed h
ealt
h in
sura
nce
cove
rag
e to
be
30%
of
the
po
pu
lati
on
(20
% u
nd
er t
he
sub
sid
ized
, po
vert
y-fo
cuse
dM
IP a
nd
10%
th
rou
gh
volu
nta
ry e
nro
lmen
t).
Ger
man
y
Gre
ece
In M
ay 2
010,
Gre
ece
was
pu
t u
nd
er t
he
sup
ervi
sio
n
of
Euro
pea
n C
om
mis
sio
n,
the
Euro
pea
n C
entr
al B
ank
(EC
B)
and
th
e In
tern
atio
nal
Mo
net
ary
Fun
d (
IMF)
du
e to
the
pu
blic
def
icit
an
d d
ebts
as w
ell a
s th
e cr
edit
cri
sis.
The
Mem
ora
nd
um
th
atG
reec
e si
gn
ed d
icta
tes
a se
ries
of
mea
sure
sre
ferr
ing
to
th
e h
ealt
hse
cto
r, fo
cusi
ng
esp
ecia
llyo
n r
edu
ctio
n o
f p
ub
licex
pen
dit
ure
. In
th
e co
nte
xto
f th
e M
emo
ran
du
m, p
ub
lich
ealt
h e
xpen
dit
ure
had
to
be
red
uce
d b
y 0.
5% o
f G
DP
du
rin
g 2
011.
Fro
m 2
011,
th
e ci
vil
serv
ants
’ SH
I fu
nd
em
plo
yer
(i.e
. sta
te)
con
trib
uti
on
ra
te is
set
at
5.1%
of
civi
lse
rvan
ts’ s
alar
ies,
wh
ile t
he
con
trib
uti
on
of
the
fun
d’s
pen
sio
ner
s is
gra
du
ally
bei
ng
incr
ease
d f
rom
2.5
5%to
4%
in 2
013.
Pre
vio
usl
y,th
e p
ub
lic s
ecto
r d
id n
ot
con
trib
ute
a s
pec
ific
per
cen
tag
e; d
epen
din
g
on
th
e n
eed
s o
f th
e so
cial
sec
uri
ty f
un
d, t
he
con
trib
uti
on
of
the
pu
blic
sect
or
(go
vern
men
t) w
asth
rou
gh
th
e st
ate
bu
dg
et.
Wit
h t
he
init
iati
on
of
the
new
so
cial
sec
uri
ty f
un
d f
or
Fro
m 2
011,
an
incr
ease
in u
ser
char
ges
fro
m E
UR
3
to E
UR
5 in
ou
tpat
ien
td
epar
tmen
ts o
f p
ub
licfa
cilit
ies;
use
r ch
arg
esin
hea
lth
cen
tres
rem
ove
d f
or
cert
ain
vuln
erab
le g
rou
ps.

Policy summary
50
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Gre
ece
(co
nt.
)Th
e h
ealt
h b
ud
get
fo
r 20
11d
ecre
ased
by
EUR
1.4
bill
ion
,w
ith
EU
R 5
68 m
illio
n s
aved
thro
ug
h m
easu
res
dic
tate
db
y th
e M
emo
ran
du
m r
elat
edto
sal
arie
s an
d b
enef
its
cuts
and
EU
R 8
40 m
illio
n s
aved
thro
ug
h c
uts
in o
per
atin
gco
sts
of
ho
spit
als.
the
Gre
ek p
op
ula
tio
n(E
OPY
Y –
Nat
ion
al H
ealt
hSe
rvic
e O
rgan
izat
ion
) th
e5.
1% w
as s
pec
ifie
d in
th
eM
emo
ran
du
m.
Hu
ng
ary
The
cen
tral
ly s
et b
ud
get
fo
rth
e h
ealt
h in
sura
nce
fu
nd
(HIF
) d
id n
ot
chan
ge
mu
chn
om
inal
ly b
etw
een
200
8an
d 2
011,
wh
ich
imp
lies
that
rea
l exp
end
itu
re o
nh
ealt
h d
ecre
ased
wh
enad
just
ing
fo
r in
flat
ion
.O
vera
ll, a
slig
ht
red
uct
ion
ing
ove
rnm
ent
exp
end
itu
re o
nh
ealt
h a
s a
shar
e o
f G
DP.
The
tota
l exp
end
itu
re f
rom
the
HIF
, in
clu
din
g a
lso
th
eca
sh b
enef
its,
was
HU
F 14
45m
illio
n in
200
8 an
d w
asex
pec
ted
to
be
HU
F 14
59m
illio
n in
201
1.
Sin
ce 2
009
the
hea
lth
con
trib
uti
on
pai
d b
y th
eem
plo
yer
dec
lined
fro
m 5
%to
2%
fo
r ea
rnin
gs
bel
ow
twic
e th
e m
inim
um
wag
e,w
hile
it r
emai
ned
5%
fo
rth
ose
ab
ove
th
is t
hre
sho
ld.
To c
om
pen
sate
th
e H
IF f
or
the
loss
in r
even
ues
, th
ece
ntr
al b
ud
get
co
ntr
ibu
tio
no
n b
ehal
f o
f el
igib
le b
ut
no
n-c
on
trib
uti
ng
per
son
s(p
ensi
on
ers,
yo
un
gst
ers,
ho
mel
ess,
etc
.) w
as r
aise
dfr
om
HU
F 45
00/p
erso
n t
oH
UF
9300
/per
son
.
This
en
taile
d a
maj
or
shif
t in
the
reve
nu
e m
ix f
or
hea
lth
:g
ener
al t
ax r
even
ue
tran
sfer
sto
HIF
alm
ost
do
ub
led
ino
rder
to
co
mp
ensa
te f
or
the
red
uct
ion
of
the
SHI
reve
nu
es d
ue
to r
edu
ctio
no
f th
e SH
I co
ntr
ibu
tio
nra
tes,
wh
ich
was
mea
nt
to s
tim
ula
te la
bo
ur
mar
ket.
Ch
ang
es in
use
rch
arg
es N
OT
as a
resp
on
se t
o t
he
cris
is,
bu
t re
leva
nt
in t
he
con
text
of
the
cris
isre
spo
nse
mea
sure
s.
In 2
008
the
follo
win
gfe
es w
ere
abo
lish
ed:
HU
F 30
0 p
er v
isit
fo
rse
rvic
es o
f G
Ps,
den
tist
s, o
utp
atie
nt
care
an
d o
utp
atie
nt
reh
abili
tati
on
; HU
F60
0 p
er v
isit
in c
ase
of
mis
sin
g p
aper
s in
ou
tpat
ien
t ca
re,
wh
ere
adm
itta
nce
pap
ers
are
nee
ded
;H
UF
1000
per
vis
it
in c
ase
of
cau
sele
ssu
se o
f n
igh
t d
uty
.In
pat
ien
t d
aily
fee
:H
UF
300
per
day
.
Fro
m 2
008
ph
arm
aceu
tica
l an
dm
edic
al a
pp
lian
ceco
mp
anie
s w
ere
ob
liged
to
pay
a f
eeto
th
e g
ove
rnm
ent
exch
equ
er f
or
the
pro
mo
tio
nal
act
ivit
yo
f th
eir
med
ical
sal
esre
pre
sen
tati
ves.
Th
isam
ou
nts
to
aro
un
dH
UF
5 m
illio
n p
erye
ar (
app
rox.
EUR
2000
0) f
or
asa
les
rep
rese
nta
tive
of
ph
arm
aceu
tica
lsan
d H
UF
1 m
illio
n
for
on
e in
th
e ar
ea
of
med
ical
pro
du
cts.

Health policy responses to the financial crisis in Europe – Annexes
51
In 2
010,
th
e it
emiz
ed h
ealt
hco
ntr
ibu
tio
n (
a ta
x o
fH
UF
1950
per
mo
nth
per
emp
loye
e p
aid
by
emp
loye
rs)
was
ab
olis
hed
.
Sin
ce 2
008,
GPs
(g
ener
alp
ract
itio
ner
) an
d o
ut-
an
din
pat
ien
t p
rovi
der
s g
et H
UF
50 c
om
pen
sati
on
fo
r ea
cho
nlin
e el
igib
ility
ch
eck
(ch
ecki
ng
th
e va
lidat
ion
of
insu
ran
ce b
y so
cial
sec
uri
tyn
um
ber
). T
his
do
es n
ot
mea
n t
hat
pat
ien
ts w
ith
ou
tva
lid in
sura
nce
sta
tus
will
no
t b
e tr
eate
d, b
ut
the
HIF
will
rep
ort
to
th
e ta
x ag
ency
wh
ich
, in
tu
rn, c
olle
cts
un
pai
d c
on
trib
uti
on
sre
tro
spec
tive
ly. T
his
mea
sure
targ
eted
imp
rove
d c
olle
ctio
n.
Icel
and
The
nat
ion
al b
ud
get
has
bee
n c
ut
con
sid
erab
ly
po
st-c
risi
s, in
clu
din
gap
pro
xim
atel
y 5%
an
nu
alcu
ts t
o t
he
hea
lth
car
e an
d s
oci
al s
ecu
rity
sec
tors
.A
cco
rdin
g t
o n
atio
nal
stat
isti
cs, p
er c
apit
a to
tal
hea
lth
exp
end
itu
re g
row
thw
as -
3.1%
in 2
009
and
-4.
0% in
201
0. A
s o
f M
arch
2009
, th
e M
inis
try
of
Hea
lth
has
red
uce
d e
xpen
dit
ure
s,in
clu
din
g f
or
equ
ipm
ent,
dru
gs,
op
erat
ing
exp
ense
san
d p
atie
nt
tran
spo
rt.

Policy summary
52
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Icel
and
(co
nt.
)Th
e b
ud
get
of
the
Nat
ion
alU
niv
ersi
ty H
osp
ital
has
bee
nre
du
ced
by
app
roxi
mat
ely
18%
fro
m 2
007
to 2
010.
Irel
and
The
2009
hea
lth
bu
dg
etin
crea
sed
by
1%.
Savi
ng
s in
th
e h
ealt
hb
ud
get
of
ove
r EU
R 1
bill
ion
ann
ou
nce
d in
201
0 b
ud
get
.
In 2
011,
th
e o
vera
ll b
ud
get
for
hea
lth
was
do
wn
by
a fu
rth
er E
UR
746
mill
ion
(a
yea
r-o
n-y
ear
6.6%
cu
t fo
rth
e H
ealt
h S
ervi
ce E
xecu
tive
(HSE
)).
Incr
ease
d f
un
ds
to c
ove
rin
crea
sin
g n
um
ber
s o
fp
eop
le o
n lo
w in
com
esel
igib
le f
or
med
ical
car
ds
(by
Sep
tem
ber
200
9,1.
4m
illio
n p
eop
le w
ere
cove
red
by
med
ical
car
ds,
up
by
4% y
ear
on
yea
r):
incr
ease
in t
he
2009
med
ical
card
bu
dg
et e
qu
ival
ent
to a
1% r
eal i
ncr
ease
in f
un
din
gp
er c
apit
a; s
up
ple
men
tary
bu
dg
et a
nn
ou
nce
d in
No
vem
ber
200
9 an
d e
xtra
fun
ds
(EU
R 2
30 m
illio
n)
wer
e m
ade
avai
lab
le f
or
2010
in t
he
Dec
emb
erb
ud
get
.
In 2
009,
th
e h
ealt
hle
vy, a
su
rro
gat
ein
com
e ta
x, w
asd
ou
ble
d t
o 4
% o
n
all e
arn
ing
s u
p t
oEU
R 7
5 03
6 an
dra
ised
to
5%
on
earn
ing
s o
ver
EUR
75
036.
Th
e th
resh
old
o
f p
aym
ent
was
als
ore
du
ced
.
Tax
relie
f fo
r p
riva
ten
urs
ing
ho
mes
an
dh
osp
ital
s w
as t
o s
top
as p
art
of
a b
road
erp
olic
y o
f en
din
gp
rop
erty
-rel
ated
tax
relie
f, h
ow
ever
no
exac
t en
d d
ate
was
nam
ed. P
allia
tive
care
co
nti
nu
es t
o b
eel
igib
le f
or
tax
relie
f.
Fro
m 2
009,
fo
r th
etw
o-t
hir
ds
of
the
po
pu
lati
on
wit
ho
ut
med
ical
car
ds
(med
ical
card
s co
nfe
r fr
eeac
cess
to
GPs
an
dw
aive
ho
spit
alin
pat
ien
t fe
es f
or
tho
se u
nd
er c
erta
inin
com
e th
resh
old
san
d s
om
e p
eop
le
ove
r 70
yea
rs o
f ag
e)u
ser
char
ges
incr
ease
dfo
r p
ub
lic (
17%
) an
dp
riva
te (
20%
) b
eds
inp
ub
lic h
osp
ital
s, u
seo
f th
e em
erg
ency
dep
artm
ent
in p
ub
lich
osp
ital
s, e
mer
gen
cyd
epar
tmen
t ch
arg
es,
and
ded
uct
ible
s fo
rth
e d
rug
s p
aym
ent
sch
eme
(wh
ich
reim
bu
rses
no
n-
med
ical
car
d h
old
ers
for
cost
of
dru
gs
ove
ra
cert
ain
am
ou
nt)
.
In t
he
2010
bu
dg
et:
intr
od
uct
ion
of
a50
cen
t ch
arg
e fo
r

Health policy responses to the financial crisis in Europe – Annexes
53
The
2011
bu
dg
et: m
ino
rfu
nd
ing
incr
ease
s to
can
cer
care
(EU
R 1
0 m
illio
n),
ho
mec
are
pac
kag
es
(EU
R 8
mill
ion
) ch
ildp
rote
ctio
n (
EUR
9 m
illio
n)
and
th
e Fa
ir D
eal
(EU
R 6
mill
ion
), w
hic
hp
rovi
des
fin
anci
al s
up
po
rtfo
r p
eop
le a
sses
sed
as
nee
din
g lo
ng
-ter
m
nu
rsin
g h
om
e ca
re.
a p
resc
rip
tio
n f
or
all
med
ical
car
d h
old
ers
up
to
a m
axim
um
of
EUR
10
per
fam
ily p
erm
on
th; i
ncr
easi
ng
th
ed
rug
s re
imb
urs
emen
tth
resh
old
to
EU
R 1
20(f
rom
EU
R 1
00 in
2009
) a
mo
nth
fo
r th
e 70
% o
f th
ep
op
ula
tio
n w
ho
pay
for
thei
r o
wn
dru
gs.
Isra
el
Ital
yFo
r th
e h
ealt
h c
are
sect
or,
inre
aliz
atio
n o
f th
e ag
reem
ent
bet
wee
n t
he
stat
e an
d t
he
reg
ion
s in
Dec
emb
er 2
010,
add
itio
nal
res
ou
rces
wer
efo
rese
en a
mo
un
tin
g t
oEU
R1.
1 m
illio
n in
201
0,
as w
ell a
s EU
R 4
00 m
illio
n
and
EU
R30
0 m
illio
n,
resp
ecti
vely
, in
th
e tw
ofo
llow
ing
yea
rs, i
n o
rder
to
incr
ease
Nat
ion
al H
ealt
hSe
rvic
e fu
nd
ing
an
d t
oin
crea
se t
he
fun
d f
or
lon
g-
term
car
e an
d t
he
fun
d f
or
soci
al p
olic
y, a
s w
ell a
s to
fin
ance
inve
stm
ents
in p
ub
licsa
nit
ary
infr
astr
uct
ure
s.
Ho
wev
er, i
n 2
011
a n
ewse
ries
of
cuts
in h
ealt
h c
are
exp
end
itu
res
was
fo
rese
enb
y th
e g
ove
rnm
ent.
Th
eN
atio
nal
Co
mm
issi
on
on
Fro
m 2
010,
reg
ion
sw
ith
larg
e h
ealt
hca
re d
efic
its
hav
eh
ad t
o r
aise
loca
lta
xes
to r
eco
ver
def
icit
s.
For
2010
–201
1,re
mo
ved
fee
of
EUR
10
for
spec
ialis
tan
d d
iag
no
stic
serv
ices
.
The
2011
Fin
anci
alLa
w in
tro
du
ces
incr
ease
s in
co
-pay
men
t fe
es f
or
visi
ts t
o d
oct
ors
an
dan
alys
is (
EUR
10+
) an
d f
or
inte
rven
tio
ns
in e
mer
gen
cy w
ard
sn
ot
just
ifie
d b
yu
rgen
t si
tuat
ion
s (E
UR
25+
).

Policy summary
54
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Ital
y (c
on
t.)
Soci
al A
ffai
rs in
Par
liam
ent
(Co
mm
issi
on
e A
ffar
iso
cial
id
ella
Cam
era)
has
dis
cuss
eda
seri
es o
f cu
ts in
wel
fare
as
par
t o
f th
e 20
11 F
inan
cial
Law
. Th
e cu
ts w
ere
very
exte
nsi
ve. I
n 2
011,
inve
stm
ent
in h
ealt
h c
are
infr
astr
uct
ure
s w
as t
o b
e cu
t fr
om
ove
r EU
R 1
bill
ion
to E
UR
236
mill
ion
. Res
earc
hfu
nd
ing
fo
r th
e p
ub
lich
ealt
h c
are
sect
or
was
to
be
cut
fro
m E
UR
91.
9 m
illio
n t
oEU
R 1
8.4
mill
ion
. Th
e fu
nd
for
dis
ease
pre
ven
tio
n a
nd
hea
lth
pro
mo
tio
n w
as t
o b
ecu
t fr
om
EU
R 2
9.6
mill
ion
to
EUR
5.9
mill
ion
. Pal
liati
veca
re w
as t
o b
e cu
t to
on
lyEU
R 1
mill
ion
. Res
ou
rces
fo
rse
mi-
auto
mat
ic d
efib
rilla
tors
and
rel
ated
eq
uip
men
t in
pu
blic
pla
ces
was
to
be
red
uce
d f
rom
EU
R 4
mill
ion
to E
UR
2 m
illio
n.
Fro
m 2
010
a ti
gh
ter
bu
dg
etca
p w
as f
ixed
fo
r re
gio
ns’
ph
arm
aceu
tica
l exp
end
itu
re.
The
bu
dg
et f
or
dru
gs
has
bee
n r
edu
ced
in a
bso
lute
valu
e b
y EU
R 8
00 m
illio
nst
arti
ng
fro
m 2
010,
bei
ng
fixe
d a
t 13
.3%
of
tota
l pu
blic
hea
lth
car
e ex
pen
dit
ure
.C
on
seq
uen
tly
the
leve
l of

Health policy responses to the financial crisis in Europe – Annexes
55
fin
anci
ng
by
the
stat
e w
asre
du
ced
by
EUR
800
mill
ion
fro
m t
he
year
201
0.
Kyr
gyz
stan
Latv
iaTh
e h
ealt
h c
are
exp
end
itu
reb
ud
get
incr
ease
d b
etw
een
2005
an
d 2
008
reac
hin
g
LVL
576.
56 m
illio
n. F
rom
2009
it d
ecre
ased
fal
ling
to
LV
L 50
3.73
mill
ion
, an
dLV
L 43
2.78
mill
ion
in 2
010.
The
follo
win
g s
pec
ific
fin
anci
al c
uts
in e
xpen
dit
ure
wer
e m
ade
by
the
Min
istr
yo
f H
ealt
h in
201
0 co
mp
ared
to
200
8: t
reat
men
t -4
0.4%
;p
ub
lic h
ealt
h -
88.6
%;
cen
tral
ad
min
istr
atio
n -
58.6
%; m
edic
al a
nd
hea
lth
edu
cati
on
at
un
iver
sity
-41
.7%
; ad
min
istr
atio
n
of
hea
lth
car
e fi
nan
cin
g -
67.7
%. F
un
din
g in
th
eb
ud
get
fo
r w
ork
of
hea
rth
ealt
h c
abin
ets
and
co
ntr
ol
and
ep
idem
iolo
gic
alsu
rvei
llan
ce d
ecre
ased
by
86.9
% a
nd
fu
nd
ing
fo
rh
ealt
h s
tati
stic
s re
du
ced
b
y 74
% in
201
0 co
mp
ared
to 2
008.
In 2
009
the
ph
arm
aceu
tica
lre
imb
urs
emen
t b
ud
get
w
as d
ecre
ased
by
7.1%
com
par
ed t
o 2
008.
Pri
mar
y
The
Cab
inet
of
Min
iste
rs a
men
ded
Reg
ula
tio
ns
on
th
eR
eim
bu
rsem
ent
of
Phar
mac
euti
cals
.Th
ese
cam
e in
to f
orc
ein
200
9; t
hei
r ef
fect
sw
ere
the
red
uct
ion
o
f th
e p
erce
nta
ge
of
reim
bu
rsem
ent
for
cert
ain
dia
gn
ose
sfr
om
75%
to
50%
an
d f
rom
90%
to
75%
for
oth
er d
iag
no
ses.
Thu
s th
e fi
nan
cial
bu
rden
was
par
tial
lysh
ifte
d t
o p
atie
nts
.C
on
seq
uen
tly,
th
ere
was
an
incr
ease
inp
atie
nt
co-p
aym
ent
by
59%
in 2
009
com
par
ed t
o 2
008.
This
res
ult
ed in
an
aver
age
leve
l of
pat
ien
t co
-pay
men
tsin
th
e re
imb
urs
emen
tsy
stem
of
app
roxi
-m
atel
y 30
% in
200
9.A
t th
e sa
me
tim
e,10
0% r
eim
bu
rsem
ent
was
mai
nta
ined
fo
r

Policy summary
56
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Latv
ia (
con
t.)
care
was
set
as
a p
rio
rity
, so
cuts
in t
he
reim
bu
rsem
ent
of
ph
arm
aceu
tica
ls w
ere
pro
po
rtio
nal
ly s
mal
ler
than
cu
ts in
th
e se
cto
r o
f in
pat
ien
t h
ealt
h c
are.
the
mo
st s
ever
ed
iag
no
ses,
su
ch
as o
nco
log
y an
den
do
crin
olo
gy.
Mo
sto
f th
e co
-pay
men
tin
crea
ses
wer
e fo
rca
rdio
vasc
ula
r sy
stem
dis
ease
s. T
he
red
uct
ion
of t
he r
ate
of r
eim
-bu
rsem
ent
was
a
shor
t-te
rm m
easu
re
to r
edu
ce c
ost
s; it
was
un
der
sto
od
th
at it
cou
ld s
erio
usl
y af
fect
pu
blic
hea
lth
ind
icat
ors
in t
he
lon
ger
ter
m. T
he
rate
of
reim
bu
rsem
ent
for
card
iova
scu
lar
dis
ease
s h
as b
een
incr
ease
d t
o t
he
pre
vio
us
leve
l of
75%
from
1N
ovem
ber
2010
.
The
Soci
al S
afet
y N
etw
as in
tro
du
ced
inLa
tvia
at
the
end
of
2009
an
d is
fin
ance
db
y a
loan
fro
m t
he
Wo
rld
Ban
k. M
ost
of
the
Soci
al S
afet
y N
etsp
end
ing
on
hea
lth
care
is in
ten
ded
to
cove
r th
e co
-pay
men
to
f p
atie
nts
fo
r h
ealt
hca
re s
ervi
ces
and
to
pro
vid
e 10
0%

Health policy responses to the financial crisis in Europe – Annexes
57
reim
bu
rsem
ent
of
med
icin
al p
rod
uct
sfo
r th
e le
ss w
ell-
off
–th
ose
wh
o r
ecei
ve
less
th
an L
VL
120
per
mo
nth
, eq
uiv
alen
t to
EU
R 1
70. I
t w
asp
lan
ned
th
at t
his
mea
sure
will
en
d o
n31
Dec
emb
er 2
011.
Lith
uan
iaIn
200
8 g
ove
rnm
ent
exp
end
itu
re o
n h
ealt
h w
asLT
L 10
00.7
mill
ion
bu
t it
dec
lined
to
LTL
854
.4 m
illio
nin
200
9. In
200
9 th
e b
ud
get
of
the
Co
mp
uls
ory
Hea
lth
Insu
ran
ce F
un
d (
CH
IF)
rem
ain
ed a
t th
e sa
me
leve
las
in 2
008.
Ho
wev
er, i
n
the
year
201
0 it
s b
ud
get
dec
reas
ed b
y 8%
co
mp
ared
to y
ears
200
9 an
d 2
008
(LTL
4.0
1 b
illio
n c
om
par
edto
LTL
4.3
9 b
illio
n).
Du
e to
incr
easi
ng
un
emp
loy -
men
t, t
he
amo
un
t o
f m
on
eyco
llect
ed b
y th
e C
HIF
sig
nif
ican
tly
dec
lined
du
rin
gre
cen
t ye
ars,
wh
erea
s st
ate
sub
sid
ies
for
peo
ple
insu
red
by
the
stat
e m
ore
th
ando
uble
d (f
rom
LTL
674
mill
ion
in 2
007
to L
TL 7
81 m
illio
n in
2008
, LTL
1.1
bill
ion
in 2
009
and
LTL
1.5
bill
ion
in 2
010)
.Th
e su
bsi
die
s fo
r th
ose
insu
red
by
the
stat
ein
crea
sed
fro
m L
TL 3
53 in
2007
to
LTL
428
in 2
008,
LT
L 60
5 in
200
9, a
nd
LTL
744
in 2
010
per
insu
red
per
son
per
yea
r. Fo
r th
e ye
ar 2
011
it w
as p
lan
ned
th
at t
he
stat
ew
ou
ld p
ay L
TL 7
33 p
erin
sure
d p
erso
n. A
cco
rdin
gto
hea
lth
insu
ran
cele
gis
lati
on
, in
an
y g
iven
year
, th
is a
mo
un
t is
calc
ula
ted
as
app
roxi
mat
ely
on
e-th
ird
of
the
aver
age
gro
ss s
alar
y in
th
e co
un
try
two
yea
rs p
revi
ou
sly.

Policy summary
58
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Mal
ta
Net
her
lan
ds
Co
-pay
men
ts w
ere
tob
e in
crea
sed
fo
rce
rtai
n s
ervi
ces
fro
m20
10, a
s a
resu
lt o
fre
stri
ctio
ns
in t
he
ben
efit
pac
kag
e.
No
rway
The
stat
e b
ud
get
has
bee
nm
ain
tain
ed t
hro
ug
ho
ut
the
cris
is d
ue
to s
ub
stan
tial
oil
reve
nu
es.
Pola
nd
It w
as e
xpec
ted
th
at in
201
1th
ere
wo
uld
be
a 2.
6%in
crea
se in
th
e N
atio
nal
Hea
lth
Fu
nd
’s (N
HF)
rev
enu
esan
d e
xpen
dit
ure
s co
mp
ared
to 2
010,
du
e to
mo
der
ate
incr
ease
s o
f u
nem
plo
ymen
t.B
y co
mp
aris
on
, th
e N
HF'
sre
ven
ues
an
d e
xpen
dit
ure
sin
crea
sed
by
11.5
% in
200
9co
mp
ared
to
200
8 an
d a
bo
ut
8% in
201
0 co
mp
ared
to
2009
. In
200
9, t
he
go
vern
-m
ent
cut
its
inve
stm
ent
exp
end
itu
res
in h
ealt
h c
are
infr
astr
uct
ure
by
hal
f. T
he
low
er e
xpen
dit
ure
s w
ere
con
tin
ued
in s
ub
seq
uen
tst
ate
bu
dg
ets.

Health policy responses to the financial crisis in Europe – Annexes
59
Port
ug
alTh
e g
ove
rnm
ent
has
init
iate
d a
co
mp
reh
ensi
vere
form
pac
kag
e to
imp
rove
effi
cien
cy a
nd
to
red
uce
sig
nif
ican
tly
the
cost
s o
f th
e h
ealt
h c
are
sect
or.
Au
tho
riti
es e
xpec
ted
th
ep
acka
ge
to y
ield
sav
ing
sw
ort
h E
UR
700
mill
ion
in20
11, o
f w
hic
h E
UR
100
mill
ion
is p
art
of
anad
dit
ion
al c
on
solid
atio
np
acka
ge.
Th
e g
ove
rnm
ent
is c
om
mit
ted
to
ach
ieve
furt
her
co
st s
avin
gs
of
EUR
200
mill
ion
in 2
012
by
cutt
ing
op
erat
ion
al
cost
s b
y 10
%.
Thro
ug
h t
he
Fun
daç
ão p
ara
a C
iên
cia
e a
Tecn
olo
gia
(FC
T), t
he
stat
e su
bsi
diz
esre
sear
ch a
nd
dev
elo
pm
ent
(R&
D),
gra
nts
hig
her
edu
cati
on
res
earc
hsc
ho
lars
hip
s an
d a
war
ds
fun
din
g t
o r
esea
rch
un
its.
In20
11, s
om
e R
&D
un
its
wer
ein
form
ed t
hat
a la
rge
par
to
f th
e p
red
icte
d f
un
din
gw
ou
ld n
ot
be
avai
lab
le a
nd
man
y re
sear
ch s
cho
lars
hip
sar
e al
so b
ein
g e
limin
ated
. It
is n
ot
clea
r h
ow
far
th
e cu
tsw
ill g
o.
AD
SE (
hea
lth
sys
tem
fo
rp
ub
lic s
ecto
r w
ork
ers)
refo
rm in
201
1: t
he
con
trib
uti
on
of
1.5%
o
f th
e sa
lary
of
pu
blic
wo
rker
s w
as n
ot
pla
nn
ed
to b
e in
crea
sed
, bu
t th
eco
ntr
ibu
tio
n o
f 1.
3% o
fp
ensi
on
ers
was
pla
nn
ed
to in
crea
se b
y 0.
1% p
er
year
un
til i
t m
atch
es t
he
con
trib
uti
on
of
acti
vew
ork
ers.
Use
r ch
arg
es o
f th
eN
HS
(Nat
ion
al H
ealt
hSe
rvic
e) w
ere
up
dat
edan
d in
cen
tive
s w
ere
crea
ted
to
pro
mo
teth
e p
aym
ent
of
thes
ech
arg
es (
sin
ce s
om
ep
eop
le ig
no
red
eman
ds
for
pay
men
t,si
nce
th
is is
ask
ed f
or
afte
r th
e se
rvic
e h
asb
een
giv
en).
Fro
m 2
011:
(1)
Incr
ease
in c
har
ges
app
lied
to
so
me
vacc
ines
, su
ch a
sye
llow
feve
r, Ja
pan
ese
ence
ph
alit
is, t
yph
oid
,m
enin
git
is a
nd
rab
ies
tetr
aval
ent.
Th
ese
char
ges
of
less
th
anEU
R 1
per
vac
cin
ein
crea
sed
to
EU
R 5
0–10
0 p
er v
acci
ne.
(2
) In
crea
se in
ch
arg
esas
ked
fo
r d
oct
or
dec
lara
tio
ns
by
ah
ealt
h a
uth
ori
ty o
r a
pu
blic
hea
lth
pro
fess
ion
al f
rom
less
than
EU
R 1
to
EU
R 2
0;d
oct
or
dec
lara
tio
ns
atte
stin
g t
o t
he
inca
pac
ity
of
a p
atie
nt
for
hea
lth
rea
son
s b
ya
med
ical
bo
ard
to
EUR
50;
do
cto
rd
ecla
rati
on
s o
f ap
pea
l

Policy summary
60
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Port
ug
al(c
on
t.)
by
a m
edic
al b
oar
d t
oEU
R 1
00. T
his
mea
ns
that
a d
isab
led
per
son
wh
o w
ants
to
acc
ess
fisc
al b
enef
its
(pay
ing
less
inco
me
tax,
fo
rin
stan
ce, o
r p
ayin
g le
ssta
xes
wh
en b
uyi
ng
a
car
adap
ted
fo
rd
isab
led
peo
ple
), a
nd
for
wh
om
ask
ing
fo
r a
do
cto
r’s
dec
lara
tio
no
f ap
pea
l by
a m
edic
alb
oar
d is
man
dat
ory
to
acce
ss t
hes
e b
enef
its,
no
w h
as t
o p
ay m
uch
mo
re t
han
bef
ore
.
Stat
e su
bsi
dy
for
som
ep
har
mac
euti
cal d
rug
sw
as c
ance
lled
, to
tally
or
par
tial
ly: I
n 2
010,
a
law
wh
ich
gra
nte
d10
0% s
tate
su
bsi
dy
for
som
e an
ti-
dep
ress
ants
, an
ti-
psy
cho
tic
and
oth
erd
rug
s as
soci
ated
wit
hth
e tr
eatm
ent
of
afe
w s
erio
us
men
tal
illn
esse
s (s
uch
as
sch
izo
ph
ren
ia,
dem
enti
a, a
uti
sm,
bip
ola
r d
iso
rder
) w
as r
evo
ked
. Th
ose
pat
ien
ts n
ow
hav
e to
pay
5–1
0% o
f th
e co
st

Health policy responses to the financial crisis in Europe – Annexes
61
of
trea
tmen
t. T
he
Ord
er o
f M
edic
alD
octo
rs o
ffic
ially
sta
ted
thei
r o
pp
osi
tio
n t
oth
e m
easu
re. F
rom
Jan
uar
y 20
11, 1
6 ty
pes
of
ph
arm
aceu
tica
ld
rug
s (f
or
wh
ich
med
ical
pre
scri
pti
on
was
no
t m
and
ato
ry)
wer
e n
o lo
ng
ersu
bsi
diz
ed, i
ncl
ud
ing
par
acet
amo
l, an
tiac
ids
and
an
tivi
rals
.
Rep
ub
lic o
fM
old
ova
Ther
e w
as a
red
uct
ion
of
6% in
GD
P in
200
9. T
he
hea
lth
bu
dg
et a
lso
fel
l in
this
yea
r. H
ow
ever
, th
e 20
10an
d 2
011
bu
dg
ets
wer
e n
ot
affe
cted
by
the
cris
is a
s th
eco
un
try’
s ec
on
om
yst
abili
zed
.
Ther
e w
as a
7%
incr
ease
in
tra
nsf
ers
fro
m t
he
stat
eb
ud
get
to
man
dat
ory
hea
lth
insu
ran
ce f
un
ds
in20
09 t
o c
om
pen
sate
fo
rfa
llin
g r
even
ues
fro
mp
ayro
ll ta
x.
The
rate
of
dis
cou
nt
incr
ease
d f
rom
50%
to
75
% r
edu
ctio
n o
f in
sura
nce
pre
miu
ms
for
fin
anci
ally
and
eco
no
mic
ally
vu
lner
able
ind
ivid
ual
s an
d s
oci
ally
dis
adva
nta
ged
cat
ego
ries
o
f se
lf-e
mp
loye
d, m
ost
lyfr
om
th
e co
un
trys
ide
and
the
agri
cult
ura
l sec
tor.
The
tari
ffs
for
med
ical
serv
ices
pro
vid
ed o
nth
e b
asis
of
ou
t-o
f-p
ock
et p
aym
ent
are
con
tro
lled
by
the
stat
ean
d a
re p
erio
dic
ally
revi
sed
dep
end
ing
on
cert
ain
mac
ro-e
cono
mic
crit
eria
. Ad
dit
ion
ally
,as
a m
easu
re t
oim
pro
ve f
inan
cial
ris
kp
rote
ctio
n, i
n 2
010,
the
Min
istr
y o
f H
ealt
hin
tro
du
ced
pri
celim
itat
ion
fo
r m
ost
imp
ort
ant
and
esse
nti
al d
rug
s an
dp
har
mac
euti
cals
imp
ort
ed a
nd
dis
trib
ute
d w
ith
inp
har
mac
ies
net
wo
rk.

Policy summary
62
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Ro
man
iaM
inis
try
of
Hea
lth
bu
dg
etre
du
ced
fro
m R
ON
4,9
69m
illio
n in
200
8 to
RO
N 4
,417
mill
ion
in 2
011.
Th
e h
ealt
hse
cto
r w
as p
rote
cted
inco
mp
aris
on
to
oth
er p
ub
licse
cto
rs in
ter
ms
of
bu
dg
etar
y cu
ts.
The
shri
nki
ng
eco
no
my
has
resu
lted
in lo
wer
leve
ls o
fco
ntr
ibu
tio
ns
of
emp
loye
rsan
d e
mp
loye
es t
o t
he
HIF
.Th
e g
ove
rnm
ent
inte
rven
edw
ith
su
bsi
die
s fr
om
th
e st
ate
bu
dg
et t
o t
he
HIF
in 2
009
and
201
0 to
co
ver
the
insu
rer’
s d
ebts
to
ph
arm
acie
san
d w
ho
lesa
lers
. In
201
0 th
esu
bsi
dy
amo
un
ted
to
ab
ou
t24
% o
f th
e to
tal h
ealt
hb
ud
get
. Nev
erth
eles
s, t
he
HIF
bu
dg
et d
ecre
ased
fro
mRO
N 1
6,77
5 m
illio
n in
200
8 to
RO
N 1
6,49
7 m
illio
n in
201
1.
Plan
s to
rai
se a
dd
itio
nal
fin
anci
al r
eso
urc
es (
bet
ter
colle
ctio
n o
f p
rem
ium
s,en
larg
emen
t o
f th
ep
rem
ium
co
llect
ion
bas
is b
yre
du
cin
g t
he
nu
mb
er o
f ta
xan
d c
on
trib
uti
on
exc
epti
on
s,b
ette
r m
anag
emen
t o
f th
esy
stem
) w
ere
ann
ou
nce
d in
2010
. Fro
m 1
Jan
uar
y 20
11,
pen
sio
ner
s w
ith
an
inco
me
of
ove
r R
ON
740
per
mo
nth
will
co
ntr
ibu
te 5
.5%
of
thei
rp
ensi
on
to
th
e H
IF.
New
use
r ch
arg
es
to b
e im
ple
men
ted
du
rin
g 2
011
incl
ud
edth
e fo
llow
ing
co
-p
aym
ents
: RO
N 5
fo
ra
visi
t to
a G
P, R
ON
15
for
a h
om
e vi
sit
by
aG
P, R
ON
10
for
on
ed
ay in
ho
spit
al, R
ON
50 f
or
con
tin
uo
us
ho
spit
aliz
atio
n f
or
seve
ral d
ays.
Th
em
axim
um
leve
l of
co-p
aym
ent
will
n
ot
exce
ed R
ON
600
per
ind
ivid
ual
per
ye
ar. T
he
law
on
co
-pay
men
ts a
lso
stip
ula
tes
exce
pti
on
s,su
ch a
s ve
tera
ns,
reti
red
per
son
s w
ith
less
th
an R
ON
700
inco
me
per
mo
nth
,ch
ildre
n, e
tc. I
n 2
010
a lim
it o
n t
he
nu
mb
ero
f re
imb
urs
ed v
isit
s to
a G
P an
d s
pec
ialis
tp
hys
icia
n f
or
the
sam
e co
nd
itio
n w
asin
tro
du
ced
fo
r th
efi
rst
tim
e: a
max
imu
mo
f fi
ve v
isit
s. In
201
1th
e m
axim
um
nu
mb
ero
f vi
sits
dec
reas
ed t
oth
ree.
If a
pat
ien
tw
ants
to
use
mor
e th
an

Health policy responses to the financial crisis in Europe – Annexes
63
the
stat
ed n
um
ber
of
visi
ts s
/he
has
to
pay
ou
t o
f p
ock
et.
Ru
ssia
nFe
der
atio
nTh
ere
wer
e ex
pec
tati
on
s o
fsl
igh
t in
crea
se in
th
e h
ealt
hb
ud
get
in 2
011
and
inu
pco
min
g y
ears
du
e to
an
incr
ease
in c
om
pu
lso
ryh
ealt
h in
sura
nce
con
trib
uti
on
s. H
ow
ever
, it
is n
ot
clea
r h
ow
mu
chre
gio
nal
go
vern
men
ts
will
dec
reas
e h
ealt
h c
are
fun
din
g o
nce
gre
ater
fu
nd
s ar
e av
aila
ble
inin
sura
nce
sys
tem
.
New
law
on
hea
lth
insu
ran
ce p
rop
ose
d in
Jan
uar
y 20
11 a
nd
isex
pec
ted
to
be
pas
sed
inau
tum
n 2
012.
Th
e p
ayro
llC
om
pu
lso
ry M
edic
alIn
sura
nce
(C
MI)
tax
will
incr
ease
fro
m 3
.1%
to
5.
1%. T
he
reve
nu
e fr
om
th
ead
dit
ion
al t
wo
per
cen
tag
ep
oin
ts w
ill b
e ac
cum
ula
ted
in a
sp
ecia
l fu
nd
an
d
use
d f
or
the
Pres
iden
tial
pro
gra
mm
e o
f h
ealt
h c
are
mo
der
niz
atio
n c
on
sist
ing
o
f re
no
vati
on
of
faci
litie
s,st
and
ard
izat
ion
of
care
an
d in
form
atiz
atio
n.
A n
ew la
w t
o b
eco
me
op
erat
ion
al 2
012
will
leg
aliz
e o
ut-
of-
po
cket
fees
in s
tate
-ow
ned
faci
litie
s.
Serb
iaTh
e fi
nan
cial
cri
sis
has
red
uce
d t
he
volu
me
of
hea
lth
sec
tor
inve
stm
ents
sin
ce20
09, a
lth
ou
gh
th
ere
are
larg
e va
riat
ion
sin
th
e ch
ang
e in
inve
stm
ent
by
reg
ion
.Th
e Eu
rop
ean
Inve
stm
ent
Ban
k an
dW
orl
d B
ank
hav
eco
nti
nu
ed t
o p
rovi
de
fun
din
g, f
avo
ura
ble
loan
s, a
nd
sp
on
sore
do
ther
pro
ject
s.

Policy summary
64
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Slo
vaki
aD
ue
to a
dec
reas
e in
con
trib
uti
on
s fr
om
emp
loye
es a
nd
th
e se
lf-
emp
loye
d, t
he
rate
of
incr
ease
in h
ealt
h in
sura
nce
com
pan
ies’
(H
ICs)
rev
enu
esd
eclin
ed in
200
9 (i
t w
as o
nly
+2.
6%, c
om
par
ed t
o +
12.5
%in
200
8). H
IC r
even
ues
wer
ep
rote
cted
to
so
me
exte
nt
by
the
hig
h c
on
trib
uti
on
rate
by
the
stat
e fo
r th
eec
on
om
ical
ly in
acti
vep
op
ula
tio
n w
hic
h in
200
9w
as 4
.9%
of
the
aver
age
nat
ion
al in
com
e o
f th
ep
revi
ou
s tw
o y
ears
. Th
isre
sult
ed in
an
an
ti-c
yclic
alch
arac
ter
of
stat
e p
aym
ents
.
Wh
ile t
he
stat
e’s
con
trib
uti
on
rat
e fo
r th
e ec
on
om
ical
ly in
acti
vep
op
ula
tio
n h
as b
een
gra
du
ally
incr
easi
ng
sin
ce19
93 (
wh
en it
was
4%
) an
d r
each
ed 4
.9%
in 2
009,
in 2
010
the
go
vern
men
td
ecid
ed t
o r
edu
ce it
to
4.78
%.
Slo
ven
iaM
easu
res
ado
pte
d b
y th
eN
HIF
res
ult
ed in
to
tal
savi
ng
s o
f EU
R 1
35.9
mill
ion
in 2
009
and
EU
R 2
39 m
illio
nin
201
0.
In 2
009
the
NH
IF in
tro
du
ced
the
follo
win
g m
easu
res
to im
pro
ve c
olle
ctio
n o
fre
ven
ues
: mo
re in
ten
sive
coo
per
atio
n w
ith
th
e ta
xad
min
istr
atio
n; i
nvo
lvem
ent
of
add
itio
nal
inco
me
cate
go
ries
in c
om
pu
lso
ryco
ntr
ibu
tio
n s
chem
es
(e.g
. sel
f-em
plo
yed
entr
epre
neu
rs a
nd
inve
stin
gp
artn
ers
in c
om
pan
ies)
.
In 2
009
the
NH
IFin
tro
du
ced
ch
ang
es
trea
tmen
t, c
erta
inm
edic
ines
, no
n-
urg
ent
amb
ula
nce
serv
ices
, den
tal
pro
sth
esis
, cer
tain
op
hth
alm
olo
gic
alap
plia
nces
). A
s a
resu
lt,
a h
igh
er p
erce
nta
ge
of
cost
s is
pai
d by
pat
ient
s(m
ost
of
wh
om
are
sub
seq
uen
tly
reim
-b
urs
ed b
y vo
lun
tary
hea
lth
insu
ran
ce).

Health policy responses to the financial crisis in Europe – Annexes
Spai
nTh
e h
ealt
h s
yste
m is
dec
entr
aliz
ed t
o t
he
leve
l o
f au
ton
om
ou
s re
gio
ns.
Th
ere
gio
ns
hav
e re
spo
nsi
bili
tyfo
r b
ud
get
s an
d a
pp
lyin
gco
st-c
on
tain
men
t m
easu
res.
To d
ate
the
on
ly r
egio
n t
hat
has
dra
fted
an
Act
ion
Pla
nfo
r b
uild
ing
su
stai
nab
ility
o
f th
e h
ealt
h s
yste
m is
Cat
alo
nia
(A
pri
l 201
1).
Un
der
th
e p
lan
, th
e 20
11h
ealt
h b
ud
get
is 1
0% lo
wer
com
par
ed t
o 2
010
(an
d,
in n
om
inal
ter
ms,
is e
qu
al
to t
he
2007
bu
dg
et).
Th
em
easu
res
are
just
ifie
d b
ased
on
th
e fo
llow
ing
init
ial
fin
anci
al s
itu
atio
n o
f th
eC
atal
an h
ealt
h s
yste
m:
bet
wee
n 2
003
and
201
0 th
e C
atal
an h
ealt
h b
ud
get
incr
ease
d b
y 76
.5%
an
d
the
def
icit
was
red
uce
d
by
EUR
2.6
1 m
illio
n.
Nev
erth
eles
s, 2
010
end
ed w
ith
a d
efic
it
of
EUR
850
mill
ion
.
65

Policy summary
66
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Swed
enIn
crea
sed
fu
nd
ing
(SE
K 7
bill
ion
) g
iven
by
the
stat
e to
mu
nic
ipal
itie
s/co
un
tyco
un
cils
in 2
009
toco
mp
ensa
te f
or
red
uce
dlo
cal t
ax r
even
ues
. Fro
m20
11 o
nw
ard
s th
e an
nu
alst
ate
gra
nts
are
incr
ease
db
y SE
K 5
bill
ion
. Ab
ou
t a
thir
d o
f th
ese
reve
nu
es
are
dir
ecte
d t
o t
he
cou
nty
cou
nci
ls, w
ho
se m
ain
expe
nses
con
cern
hea
lth
care
.
Swit
zerl
and
Du
e to
th
e fi
nan
cial
cri
sis,
HIF
s su
ffer
ed lo
sses
on
th
ein
vest
men
ts t
hey
mad
e w
ith
the
mo
ney
th
ey n
eed
to
hav
e in
res
erve
as
asse
ts;
to c
om
pen
sate
, pre
miu
ms
wo
uld
hav
e h
ad t
o b
e ra
ised
by
10–2
0% in
201
0 ra
ther
than
ab
ou
t 4%
as
in p
revi
ou
sye
ars.
As
a re
sult
, in
May
2009
th
e g
ove
rnm
ent
pro
po
sed
mea
sure
s to
low
erth
e h
ealt
h c
ost
s o
f h
ealt
hin
sure
rs. T
he g
over
nmen
t al
sop
lan
ned
to
incr
ease
pre
miu
msu
bsi
die
s fo
r lo
w-i
nco
me
ho
use
ho
lds
by
CH
F 20
0m
illio
n; h
ow
ever
aft
er m
any
deb
ates
bet
wee
n t
he
two
Ch
amb
ers
of
the
Swis
sPa
rlia
men
t th
ese
mea
sure
sw
ere
ult
imat
ely
refu
sed
in
A u
ser
char
ges
ref
orm
was
ag
reed
by
the
Parl
iam
ent
inSe
pte
mb
er 2
011:
th
eco
-in
sura
nce
rat
e w
asp
lan
ned
to
incr
ease
fro
m 1
0% t
o 1
5% f
or
peo
ple
wh
o o
pt
for
trad
itio
nal
pla
ns
(th
isen
cou
rag
es p
eop
le
to s
ub
scri
be
to a
man
aged
car
e m
od
elo
f in
sura
nce
).

Health policy responses to the financial crisis in Europe – Annexes
Oct
ob
er 2
010.
Mea
sure
s to
red
uce
hea
lth
insu
rers
’ co
sts
wer
e in
stea
d in
tro
du
ced
in20
11 (
see
nex
t co
lum
n).
The
form
erYu
go
slav
Rep
ub
lic o
fM
aced
on
ia
Des
pit
e fl
uct
uat
ion
s in
fun
din
g f
or
dif
fere
nt
pri
ori
ty a
reas
, th
e h
ealt
hb
ud
get
was
incr
ease
d f
or
2010
, 201
1 an
d 2
012,
wit
hEU
R 2
1.8
mill
ion
allo
cate
dfo
r h
ealt
h in
th
e 20
10b
ud
get
, EU
R 3
4 m
illio
n in
2011
an
d E
UR
36
mill
ion
in20
12. A
rou
nd
70–
80%
of
the
2012
hea
lth
bu
dg
etin
crea
ses
are
for
med
ical
equ
ipm
ent
and
tec
hn
olo
gy.
Ove
rall,
du
rin
g t
he
cris
is,
fun
ds
for
soci
al s
afet
y n
ets
wer
e p
rote
cted
wh
ile n
on
-p
rio
rity
exp
end
itu
res
wer
eel
imin
ated
.
Hea
lth
car
e co
ntr
ibu
tio
ns
hav
e b
een
red
uce
d f
rom
9.2%
to
7.5
% in
200
9 an
d
a fu
rth
er r
edu
ctio
n t
o 6
%
in 2
011
was
pla
nn
ed in
ord
er t
o in
crea
se f
ore
ign
inve
stm
ents
an
d e
con
om
icac
tivi
ty a
s w
ell a
s ta
xco
llect
ion
.
Turk
eyTh
e M
inis
try
of
Hea
lth
bu
dg
et in
crea
sed
fro
m
TRY
11,
994
mill
ion
(20
08)
to T
RY 1
4,59
4 m
illio
n(2
009)
, bu
t o
nly
slig
htl
y in
2010
to
TRY
14,
768
mill
ion
.H
ealt
h e
xpen
dit
ure
as
ash
are
of
the
go
vern
men
tb
ud
get
ro
se in
200
9 b
ut
fell
slig
htl
y in
201
0 (1
2.8%
in 2
008,
12.
8% in
200
9).
Glo
bal
bu
dg
ets
for
ho
spit
als
hav
e in
crea
sed
eve
ry y
ear
thro
ug
h 2
011,
alt
ho
ug
h
In e
arly
201
0, h
ealt
h c
are
pay
men
ts o
n t
he
par
t o
fg
ove
rnm
ent
emp
loye
es
and
th
eir
dep
end
ants
w
ere
tran
sfer
red
fro
m t
he
Min
istr
y o
f Fi
nan
ce t
o t
he
Soci
al S
ecu
rity
Inst
itu
tio
n.
Co
-pay
men
t fo
ro
utp
atie
nt
visi
ts(e
xcep
t p
rim
ary
care
vis
its)
beg
an in
the
last
qu
arte
r o
f20
08. C
o-p
aym
ents
for
ou
tpat
ien
tm
edic
ines
an
dp
rost
hes
is/o
rth
oti
csw
ere
un
chan
ged
as
a re
sult
of
the
cris
is.
67

Policy summary
68
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Turk
ey (
con
t.)
wh
ile t
he
2009
(9%
) an
d20
10 (
17%
) b
ud
get
sin
crea
sed
at
a h
igh
rat
e,
the
2011
bu
dg
et w
as s
late
dto
incr
ease
at
a m
uch
slo
wer
rate
(1%
).
Ukr
ain
ePu
blic
exp
end
itu
re o
nh
ealt
h a
s a
pro
po
rtio
n o
fto
tal e
xpen
dit
ure
incr
ease
dan
nu
ally
bet
wee
n 2
003
and
2007
. Ho
wev
er, i
n 2
008
itb
egan
to
dec
reas
e: it
was
57.2
% in
200
8 an
d 5
4.9%
in
200
9, w
hic
h c
orr
esp
on
ds
wit
h t
he
low
est
ind
ex f
or
the
pas
t se
ven
yea
rs. T
he
shar
e o
f p
riva
te r
eso
urc
es
in h
ealt
h f
inan
cin
g in
200
8–20
09 r
each
ed 4
2.5%
an
d45
.1%
, mo
st o
f w
hic
h
(~94
%)
is in
dir
ect
pay
men
tso
f h
ou
seh
old
s (o
ut
of
po
cket
).
Sin
ce 2
010
the
nat
ion
alb
ud
get
has
no
t b
een
set
ann
ual
ly, b
ut
is g
ove
rned
by
gen
eral
law
“Th
e B
ud
get
Co
de
of
Ukr
ain
e”. T
he
law
det
erm
ines
th
at t
he
amo
un
to
f p
rote
cted
exp
end
itu
res
can
no
t b
e ch
ang
ed b
yre
du
cin
g t
he
app
rove
db
ud
get
allo
cati
on
s. T
he
list
of
such
exp
end
itu
res
was
An
SH
I sys
tem
is
no
t u
sed
in U
krai
ne.
Ho
wev
er, s
ince
200
0,U
krai
ne
has
had
a
pro
gra
mm
e o
fvo
lun
tary
med
ical
insu
ran
ce f
or
railw
ay w
ork
ers.
Th
e p
rem
ium
s fo
rvo
lun
tary
hea
lth
insu
ran
ce in
crea
sed
du
rin
g t
he
cris
is:
in 2
007–
2008
th
em
on
thly
co
ntr
ibu
tio
nw
as U
AH
16
(UA
H 8
each
fro
m e
mp
loye
ean
d e
mp
loye
r); i
n20
09 it
was
UA
H 2
4(a
gai
n s
plit
eq
ual
lyb
etw
een
em
plo
yee
and
em
plo
yer)
; fro
mSe
pte
mb
er 2
010
itw
as U
AH
32
(UA
H 2
0fr
om
th
e em
plo
yee
and
UA
H 1
2 fr
om
th
e em
plo
yer)
. Th
ep
rem
ium
incr
ease
is
pri
mar
ily d
ue
to

Health policy responses to the financial crisis in Europe – Annexes
sig
nif
ican
tly
exp
and
ed a
nd
incl
ud
es: s
alar
ies
of
staf
fd
ealin
g w
ith
th
e b
ud
get
,d
rug
s an
d b
and
agin
gm
ater
ial p
rocu
rem
ent,
fo
od
pro
visi
on
, uti
litie
s an
d e
lect
rici
ty o
f fa
cilit
ies,
serv
icin
g t
he
stat
e d
ebt,
curr
ent
tran
sfer
s to
th
ep
op
ula
tio
n, c
urr
ent
tran
sfer
s to
loca
l bu
dg
ets,
fun
din
g in
stit
uti
on
s o
fh
igh
er e
du
cati
on
of
I–IV
accr
edit
atio
n le
vels
,p
rovi
din
g t
he
dis
able
d
wit
h t
ech
nic
al a
nd
oth
erre
hab
ilita
tio
n it
ems,
med
ical
pro
du
cts
for
per
son
al u
se, b
asic
res
earc
h,
app
lied
res
earc
h a
nd
tech
no
log
ical
dev
elo
pm
ent.
a sh
arp
ris
e in
th
ep
rice
of
dru
gs.
Info
rmal
pay
men
tsp
er c
apit
a (e
xclu
din
gco
sts
of
dru
gs
pu
rch
asin
g)
incr
ease
d b
y 70
%(f
rom
UA
H 9
4.4
in20
08 t
o U
AH
153
.6
in 2
009)
.
Un
ited
Kin
gd
om
(En
gla
nd
)
Aft
er y
ears
of
unpr
eced
ente
db
ud
get
gro
wth
(6.
6% p
erye
ar in
199
9–20
07),
th
e N
HS
has
en
tere
d a
new
era
of
aust
erit
y. In
Oct
ob
er 2
010
the
Dep
artm
ent
of
Hea
lth
pu
blis
hed
th
e Sp
end
ing
Rev
iew
set
tlem
ent
for
the
NH
S w
hic
h in
volv
es a
nav
erag
e 0.
1% r
eal t
erm
sin
crea
se o
ver
the
nex
t fo
ur
year
s an
d a
req
uir
emen
t to
fin
d u
p t
o G
BP
5 b
illio
np
rod
uct
ivit
y im
pro
vem
ents
a ye
ar t
hro
ug
h t
o 2
014/
2015
to m
eet
incr
ease
d d
eman
d
The
rece
ssio
n h
asre
sult
ed in
are
du
ctio
n in
exp
ecte
d r
ecei
pts
and
a li
mit
ed in
crea
sein
dis
cret
ion
ary
spen
din
g in
200
9–20
10 c
om
par
ed w
ith
pre
vio
us
year
s.C
on
seq
uen
tly,
wh
erea
s p
lan
ned
tota
l go
vern
men
tre
ceip
ts f
or
2008
–20
09 w
ere
GB
P 57
5b
illio
n, j
ust
GB
P 53
3.8
A p
rog
ram
me
toex
pan
d t
he
ran
ge
of
lon
g-t
erm
co
nd
itio
ns
that
ben
efit
fro
m
free
pre
scri
pti
on
s w
asan
no
un
ced
by
the
pre
vio
us
go
vern
men
tb
ut
no
t im
ple
men
ted
;th
is w
ill n
ow
no
lon
ger
be
take
nfo
rwar
d.
69

Policy summary
70
Co
un
try
Hea
lth
bu
dg
etFi
scal
po
licy
SHI c
on
trib
uti
on
sU
ser
char
ges
Oth
er
Un
ited
Kin
gd
om
(En
gla
nd
)(c
on
t.)
and
imp
rove
th
e q
ual
ity
of
its
serv
ices
.
Ove
rall,
NH
S sp
end
ing
will
incr
ease
by
0.4%
in r
eal
term
s o
ver
the
cou
rse
of
the
Spen
din
g R
evie
wp
erio
d; t
his
is t
he
low
est
incr
ease
sin
ce t
he
1950
s.H
ow
ever
, acc
ord
ing
to
m
any
com
men
tato
rs, t
he
Spen
din
g R
evie
w p
lan
s fo
rth
e N
HS
amo
un
t to
a d
efa
cto
cu
t in
NH
S sp
end
ing
inre
al t
erm
s. M
anag
ers
of
NH
So
rgan
izat
ion
s n
ow
hav
e to
pla
n f
or
wh
at, i
n e
ffec
t,am
ou
nts
to
a 2
0–30
%re
du
ctio
n in
NH
S sp
end
ing
for
the
five
-yea
r p
erio
dfr
om
201
1.
To m
eet
the
risi
ng
co
sts
of
hea
lth
car
e an
d in
crea
sin
gd
eman
d o
n it
s se
rvic
es, t
he
NH
S w
ill h
ave
to r
elea
se u
pto
GB
P 20
bill
ion
of
ann
ual
effi
cien
cy s
avin
gs
ove
r th
en
ext
fou
r ye
ars,
all
of
wh
ich
will
be
rein
vest
ed t
o m
eet
risi
ng
leve
ls o
f d
eman
d a
nd
to s
up
po
rt im
pro
vem
ents
inq
ual
ity
and
ou
tco
mes
.
bill
ion
was
rai
sed
. It
is e
stim
ated
th
atth
ere
was
a f
urt
her
red
uct
ion
in t
ota
lre
ceip
ts in
200
9–20
10to
GB
P 51
4.6
bill
ion
,o
f w
hic
h G
BP
95.6
bill
ion
was
gen
erat
ed f
rom
Nat
ion
al In
sura
nce
Co
ntr
ibu
tio
ns,
G
BP
145.
6 b
illio
nfr
om
inco
me
tax
and
the
rest
fro
m a
ran
ge
of
taxe
s, in
clu
din
gco
rpo
rati
on
, exc
ise,
VA
T an
d p
rop
erty
rate
s (c
ou
nci
l tax
an
d b
usi
nes
s ra
tes)
.
Uzb
ekis
tan

Health policy responses to the financial crisis in Europe – Annexes
Tab
le A
.2. P
olic
ies
targ
etin
g v
olu
me
and
qu
alit
y o
f ca
re in
th
e co
nte
xt o
f th
e ec
on
om
ic c
risi
s, W
HO
Eu
rop
ean
Reg
ion
No
tes:
No
info
rmat
ion
was
ava
ilabl
e fo
r A
ndor
ra, K
azak
hsta
n, L
uxem
bour
g, M
onac
o, M
onte
negr
o, S
an M
arin
o, T
ajik
ista
n an
d Tu
rkm
enis
tan.
Text
not
in it
alic
s in
dica
tes
a po
licy
whi
ch w
as d
efin
ed b
y th
e re
leva
nt a
utho
ritie
s in
the
cou
ntry
as
a re
spon
se t
o th
e cr
isis
. Tex
t in
ital
ics
indi
cate
s a
polic
y w
hich
was
eith
er p
artia
lly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed b
efor
e th
e cr
isis
but
impl
emen
ted
afte
r w
ithgr
eate
r/le
ss s
peed
/inte
nsity
tha
n pl
anne
d; o
r po
ssib
ly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed a
nd im
plem
ente
d si
nce
the
star
t of
the
cris
is, b
ut n
ot d
efin
ed b
y th
e re
leva
nt a
utho
ritie
s as
a r
espo
nse
to t
he c
risis
. A b
lank
cel
l ind
icat
es n
o po
licy
resp
onse
to
the
cris
is (n
ot n
ore
spon
se t
o th
e su
rvey
).
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Alb
ania
Arm
enia
Au
stri
a
Aze
rbai
jan
Bel
aru
sFr
om
200
9, c
itiz
ens
wit
h r
adia
tio
nsi
ckn
ess
as w
ell a
s ce
rtai
n d
isab
led
peo
ple
hav
e th
e ri
gh
t to
a 9
0%re
du
ctio
n in
th
e p
rice
of
med
icin
esp
resc
rib
ed b
y a
ph
ysic
ian
. Cit
izen
s w
ith
su
rgic
al d
isea
ses
also
hav
e th
eri
gh
t to
a 9
0% r
edu
ctio
n in
th
e p
rice
o
f b
and
agin
g m
ater
ials
.
Bel
giu
mSo
me
emp
has
is s
et o
n c
ance
rsc
reen
ing
, pro
mo
tio
n o
fh
ealt
h f
oo
d, p
hys
ical
act
ivit
yan
d p
reve
nti
on
of
fata
lac
cid
ents
sin
ce 2
007.
71

Policy summary
72
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Bo
snia
an
dH
erze
go
vin
aSi
nce
th
e st
art
of
the
cris
is, a
list
of
esse
nti
al d
rug
s th
at a
re p
rovi
ded
fre
eo
f ch
arg
e b
y th
e C
HIF
has
bee
n c
reat
ed.
Sin
ce t
he
star
t o
f th
e cr
isis
,am
end
men
ts t
o t
he
Law
on
Hea
lth
Insu
ran
ce p
rovi
ded
cove
rag
e fo
r ch
ildre
n (
even
if
th
eir
par
ents
do
no
t h
ave
cove
rag
e), t
ho
se o
ver
65 y
ears
of
age
and
th
e u
nin
sure
d.
The
Law
on
Hea
lth
Insu
ran
cew
as r
evis
ed a
s p
art
of
gen
eral
refo
rms,
bu
t vu
lner
able
gro
up
sb
ecam
e a
foca
l po
int
as a
resu
lt o
f th
e cr
isis
. Ho
wev
er,
a la
ck o
f re
liab
le s
ou
rces
of
fun
din
g h
as le
d t
o d
iffi
cult
ies
in im
ple
men
tin
g t
he
law
.
In 2
008
and
200
9, m
edia
cam
pai
gn
s an
d o
ther
hea
lth
pro
mo
tio
n a
nd
pre
ven
tio
nac
tivi
ties
wer
e ai
med
at
imp
rovi
ng
po
pu
lati
on
hea
lth
by
advo
cati
ng
hea
lth
ier
lifes
tyle
s. T
hes
e ca
mp
aig
ns
hav
e al
so p
rovi
ded
th
e p
ub
licw
ith
info
rmat
ion
on
hea
lth
sect
or
refo
rms.
Bu
lgar
iaTh
e M
inis
try
of
Hea
lth
is p
lan
nin
g
to d
evel
op
a p
osi
tive
list
of
med
ical
dev
ices
(si
mila
r to
th
e p
osi
tive
list
o
f d
rug
s).
Wit
h t
he
amen
dm
ent
of
the
Hea
lth
Act
in 2
010
tob
acco
smo
kin
g w
as p
roh
ibit
ed in
ind
oo
r p
ub
lic p
lace
s ex
cep
tis
ola
ted
“sm
oki
ng
ro
om
s”.
In c
afes
an
d r
esta
ura
nts
wit
har
ea o
f le
ss t
han
50
sq. m
, th
e o
wn
er c
an c
ho
ose
if t
he
wh
ole
est
ablis
hm
ent
is f
or
smo
kers
or
no
n-s
mo
kers
.B
ecau
se o
f th
e cr
isis
(res
tau
ran
ts’ f
inan
cial
pro
ble
ms)
th
e g
ove
rnm
ent
dec
ided
to
po
stp
on
e fu
llp
roh
ibit
ion
. In
200
9 th
eg
ove
rnm
ent
incr
ease
d t
he
pri
ce o
f ci
gar
ette
s b
y 25
%,
and
in 2
010
by
38%
.

Health policy responses to the financial crisis in Europe – Annexes
Cro
atia
Imp
rove
men
ts in
ph
arm
aceu
tica
lp
rici
ng
an
d r
eim
bu
rsem
ent
gen
erat
edsa
vin
gs
wh
ich
mad
e it
po
ssib
le t
o a
dd
64 n
ew d
rug
s to
th
e b
enef
it li
st a
t th
een
d o
f 20
10.
Cyp
rus
In 2
011
the
go
vern
men
t m
ade
the
deci
sion
to
agai
n po
stpo
neth
e im
ple
men
tati
on
of
the
new
Nat
ion
al H
ealt
h In
sura
nce
syst
em. C
ypru
s, w
hic
h d
oes
no
th
ave
a h
ealt
h c
are
syst
em t
hat
off
ers
un
iver
sal c
ove
rag
e, in
1991
vo
ted
fo
r th
e la
w t
hat
wo
uld
cre
ate
a n
ew N
atio
nal
Hea
lth
Insu
ran
ce S
chem
e b
ut
this
has
no
t b
een
imp
lem
ente
dto
dat
e. A
cco
rdin
g t
o M
inis
try
of
Hea
lth
est
imat
es, i
n 2
007
83%
of
the
po
pu
lati
on
had
com
pre
hen
sive
co
vera
ge
free
of
char
ge
at t
he
po
int
of
serv
ice.
Th
e re
st o
f th
ep
op
ula
tio
n h
as a
cces
s to
p
ub
lic h
ealt
h s
ervi
ces
eith
er
on
red
uce
d o
r fu
ll ra
tes
(2%
and
15%
of
the
po
pu
lati
on
,re
spec
tive
ly).
73

Policy summary
74
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Cze
ch R
epu
blic
Th
e b
asic
ben
efit
pac
kag
e an
d li
st o
fre
imb
urs
ed s
ervi
ces
will
be
asse
ssed
fro
m t
he
per
spec
tive
of
hea
lth
tech
no
log
y as
sess
men
t (u
sin
g e
vid
ence
fro
m a
bro
ad)
in 2
012/
2013
. In
form
atio
nto
pat
ien
ts o
n w
hic
h s
ervi
ces
are
reim
bu
rsed
will
be
imp
rove
d in
201
2.Th
is m
ay r
esu
lt in
a r
eallo
cati
on
of
pu
blic
an
d p
riva
te e
xpen
dit
ure
.M
and
ato
ry u
se o
f p
osi
tive
list
s o
f d
rug
s fo
r M
inis
try
of
Hea
lth
pro
vid
ers
(un
iver
sity
ho
spit
als,
rep
rese
nti
ng
50%
of
the
mar
ket)
intr
od
uce
d in
201
1(p
revi
ou
sly
the
list
was
vo
lun
tary
).Fu
rth
er li
sts
pla
nn
ed f
or
2012
.
Enti
tlem
ent
to p
ub
licly
fin
ance
d c
ove
rag
e fo
r h
igh
-ris
k co
nd
itio
ns
red
uce
dfo
r fo
reig
n c
itiz
ens
and
resp
on
sib
ility
fo
r co
vera
ge
tran
sfer
red
to
pri
vate
insu
ran
ce in
201
1 (r
esu
ltin
g
in h
igh
er p
rem
ium
s fo
r fo
reig
n c
itiz
ens)
.
Co
nsu
mp
tio
n t
axes
incr
ease
(to
bac
co, a
lco
ho
l) p
lan
ned
fo
r 20
12.
Den
mar
k
Esto
nia
EHIF
red
uce
d t
he
ben
efit
pac
kag
e in
tw
o w
ays.
Fir
st, t
he
syst
em f
or
tem
po
rary
sic
k le
ave
ben
efit
s w
asre
form
ed. F
rom
1 J
uly
200
9 n
o b
enef
itis
pai
d d
uri
ng
th
e fi
rst
thre
e d
ays
of
sick
nes
s o
r in
jury
(p
revi
ou
sly
firs
t d
ayo
nly
), t
he
emp
loye
r p
ays
the
ben
efit
fro
m d
ay f
ou
r to
day
eig
ht
(new
co
st-
shar
ing
mec
han
ism
, em
plo
yer
did
no
tp
arti
cip
ate
pre
vio
usl
y) a
nd
th
e EH
IFst
arts
to
pay
th
e b
enef
it f
rom
day
nin
e(p
revi
ou
sly
fro
m d
ay t
wo
). T
he
rate
of
sick
nes
s b
enef
it w
as r
edu
ced
fro
m 8
0%to
70%
of
the
insu
red
per
son
’s in
com
e.Th
e ra
te o
f si
ckn
ess
ben
efit
in t
he
case
of
cari
ng
fo
r a
child
un
der
12
year
s o
f
Max
imu
m w
aiti
ng
tim
es f
or
ou
tpat
ien
tsp
ecia
lists
’ vis
its
incr
ease
d in
Mar
ch20
09 b
y th
e d
ecis
ion
of
the
EHIF
su
per
viso
ryb
oar
d f
rom
fo
ur
to
six
wee
ks.
VA
T o
n a
lco
ho
l in
crea
sin
gsi
nce
200
5 b
ut
gre
ates
t ri
sew
as in
200
8 an
d t
ob
acco
VA
Tin
crea
sin
g s
ince
201
1.

Health policy responses to the financial crisis in Europe – Annexes
age
was
red
uce
d f
rom
100
% t
o 8
0%.
The
max
imu
m le
ng
th o
f m
ater
nit
yle
ave
was
red
uce
d f
rom
154
day
s to
140
day
s. E
xpec
ted
sav
ing
: EEK
50
mill
ion
. Sec
on
d, u
nti
l 1 J
anu
ary
2009
al
l in
sure
d p
erso
ns
of
at le
ast
19 y
ears
of
age
cou
ld a
pp
ly f
or
the
den
tal c
are
ben
efit
of
EEK
300
(EU
R 1
9.18
), b
ut
fro
m 2
009,
on
ly in
sure
d p
erso
ns
ove
r63
yea
rs o
f ag
e an
d p
erso
ns
elig
ible
fo
r a
pen
sio
n f
or
inca
pac
ity
for
wo
rk
or
an o
ld-a
ge
pen
sio
n r
etai
ned
th
isri
gh
t. E
xpec
ted
sav
ing
: EEK
4 m
illio
n.
The
Min
istr
y o
f So
cial
Aff
airs
was
dev
elo
pin
g a
co
mp
reh
ensi
ve h
ealt
hte
chn
olo
gy
asse
ssm
ent
syst
em in
201
1w
ith
th
e h
elp
of
Tart
u U
niv
ersi
ty.
Fin
lan
d
Fran
ceLe
Rev
enu
Min
imu
m d
’Inse
rtio
n(R
MI)
or
bas
ic b
enef
it w
asre
pla
ced
in J
un
e 20
09 b
y th
eR
even
u d
e So
lidar
ité
Act
ive
(RSA
), r
esu
ltin
g in
an
incr
ease
in t
he
nu
mb
er o
f o
vera
llre
cip
ien
ts. W
ith
th
is c
han
ge,
ben
efic
iari
es o
f th
e n
ew R
SAau
tom
atic
ally
hav
e th
e ri
gh
t to
rec
eive
sta
te-f
un
ded
C
MU
(C
ou
vert
ure
Mal
adie
Un
iver
selle
) –
un
iver
sal
hea
lth
insu
ran
ce –
an
dco
mp
lem
enta
ry in
sura
nce
CM
U-C
.
Fro
m 2
011,
tax
on
to
bac
co w
illin
crea
se b
y 6%
.
Ger
man
y
75

Policy summary
76
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Geo
rgia
Stat
e fu
nd
ing
fo
r in
sura
nce
cove
rag
e fo
r ce
rtai
n g
rou
ps
of
pu
blic
em
plo
yees
(te
ach
ers,
po
lice
forc
e an
d m
ilita
ry),
an
da
stat
e-su
bsi
diz
ed p
rog
ram
me
for
low
-inco
me
fam
ilies
(Med
ical
Insu
ran
ce f
or
the
Poo
r) w
ere
intr
od
uce
d (
2007
an
d 2
008
resp
ecti
vely
). T
his
was
acco
mp
anie
d b
y in
terv
enti
on
sto
incr
ease
aw
aren
ess
amo
ng
po
or
peo
ple
ab
ou
t su
bsi
diz
edh
ealt
h in
sura
nce
. In
201
0 M
IPco
vere
d 2
1% o
f p
op
ula
tio
n,
wh
ile in
200
7 o
nly
385
000
o
r 8.
8% h
ad t
his
insu
ran
ce.
An
exp
ansi
on
of
the
po
pu
lati
on
co
vere
d u
nd
erin
sura
nce
is e
xpec
ted
in 2
012
–ta
rget
ing
mo
stly
th
e el
der
lyan
d t
he
you
ng
.
Gre
ece
Un
ific
atio
n o
f b
enef
it p
acka
ges
am
on
gth
e va
rio
us
SHI f
un
ds
(in
Ju
ne
2011
).Fr
om
201
1, t
he
po
or
and
un
insu
red
are
on
ly a
llow
ed
to b
e tr
eate
d in
des
ign
ated
ho
spit
als
and
pre
scri
bed
gen
eric
s.
The
Mem
ora
nd
um
imp
ose
s a
limit
of
no
mo
re t
han
tw
om
on
ths
for
sub
mit
tin
g a
nin
voic
e fo
r re
imb
urs
emen
t fo
r h
osp
ital
ch
arg
es t
o s
oci
alin
sura
nce
fu
nd
s in
Gre
ece
as
For
the
per
iod
200
8–20
12,
hea
lth
pro
mo
tio
n in
itia
tive
s:ca
rdio
vasc
ula
r, ca
nce
r, o
bes
ity,
nu
trit
ion
, ora
l hea
lth
,m
ater
nal
an
d c
hild
hea
lth
,in
clu
din
g a
sm
oki
ng
law
ban
.

Health policy responses to the financial crisis in Europe – Annexes
wel
l as
oth
er E
U M
emb
erSt
ates
an
d p
riva
te H
ICs
for
no
n-n
atio
nal
s an
d n
on
-p
erm
anen
t re
sid
ents
.
Hu
ng
ary
In 2
009
sick
-pay
ben
efit
s w
ere
red
uce
d.
Prev
iou
sly
the
HIF
co
uld
pro
vid
e si
ck-
pay
fo
r u
p t
o o
ne
year
fo
r em
plo
yees
wit
h v
alid
insu
ran
ce. W
ith
ou
t in
sura
nce
it w
as o
nly
45
day
s. T
his
ch
ang
ed t
o
30 d
ays.
Wit
h a
min
imu
m t
wo
-yea
rp
erio
d o
f in
sura
nce
th
e am
ou
nt
was
70%
of
inco
me.
In c
ase
of
a sh
ort
erin
sura
nce
per
iod
or
inp
atie
nt
care
itw
as 6
0%. A
fter
th
e m
od
ific
atio
n t
hes
ew
ere
dec
reas
ed t
o 6
0% a
nd
50%
.
Icel
and
To m
inim
ize
the
effe
ct o
f th
e cr
isis
an
dcu
ts in
exp
end
itu
re o
n h
ealt
h s
ervi
ces,
a d
ocu
men
t w
as p
ub
lish
ed in
ear
ly 2
009
focu
sin
g o
n p
ub
lic h
ealt
h, e
qu
ity,
an
dla
bo
ur
issu
es. A
nu
mb
er o
f ac
tio
ns
hav
eb
een
tak
en a
s a
resu
lt, s
uch
as
pro
vid
ing
acce
ss t
o d
enta
l car
e fr
ee o
f ch
arg
e fo
rlo
w-i
nco
me
fam
ilies
sin
ce 2
009.
Ther
e h
as b
een
incr
ease
d e
mp
has
is
on
occ
up
atio
nal
reh
abili
tati
on
by
the
Icel
and
ic R
ehab
ilita
tio
n F
un
d t
osy
stem
atic
ally
dec
reas
e th
e p
rob
abili
tyo
f em
plo
yees
losi
ng
th
eir
job
s d
ue
toin
cap
acit
y an
d s
ickn
ess.
To
th
is e
nd
, th
e Ic
elan
dic
Reh
abili
tati
on
Fu
nd
w
as e
stab
lish
ed in
200
8 to
pro
vid
eco
nsu
ltin
g s
ervi
ces
to e
mp
loye
es w
ho
are
on
ext
end
ed s
ick
leav
e so
th
ey d
on
ot
lose
th
eir
job
s. S
ince
th
e fi
nan
cial
cris
is, a
ctiv
ity
at t
he
fun
d h
as in
crea
sed
.
77

Policy summary
78
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Irel
and
Fro
m 2
010,
a c
ut
of
EUR
30
mill
ion
to
den
tal c
are
for
med
ical
car
d h
old
ers.
Fro
m 2
009,
rem
ova
l of
med
ical
card
s fo
r th
e 12
100
wea
lth
iest
(3.4
%)
peo
ple
ag
ed o
ver
70.
Med
ical
car
ds
con
fer
free
acc
ess
to G
Ps a
nd
wai
ve h
osp
ital
inp
atie
nt
fees
fo
r th
ose
un
der
cert
ain
inco
me
thre
sho
lds.
New
go
vern
men
t el
ecte
d in
2011
has
pro
po
sed
a u
niv
ersa
lh
ealt
h in
sura
nce
sys
tem
.
Isra
el
Ital
y
Kyr
gyz
stan
Latv
iaA
n e
arly
can
cer
det
ecti
on
(cer
vica
l an
d b
reas
t ca
nce
r)p
rog
ram
me
star
ted
in 2
009.
Lith
uan
iaIn
200
9 so
me
chan
ges
wer
e im
plem
ente
dre
du
cin
g p
aym
ent
of
illn
ess
ben
efit
,w
hic
h is
pai
d f
or
soci
ally
insu
red
tem
po
rari
ly s
ick
peo
ple
fro
m t
he
Soci
alIn
sura
nce
Fu
nd
. Fo
r ex
amp
le, p
revi
ou
sly
illn
ess
ben
efit
was
85%
of
the
sala
ry o
fa
soci
ally
insu
red
per
son
in t
he
maj
ori
tyo
f ca
ses.
Aft
er t
he
chan
ges
wer
eim
ple
men
ted
, du
rin
g t
he
firs
t se
ven
day
sill
nes
s b
enef
it is
on
ly 4
0% o
f sa
lary
an
d,
afte
r th
e ei
gh
th d
ay, 8
0% o
f th
e sa
lary
.

Health policy responses to the financial crisis in Europe – Annexes
Mal
ta
Net
her
lan
ds
Fro
m 2
010,
lim
ited
rei
mb
urs
emen
t fo
rIV
F; p
hys
io s
essi
on
s to
be
pai
d f
or
by
the
pat
ien
t in
crea
sed
to
15;
co
vera
ge
of
care
ou
tsid
e th
e EU
rem
ove
d a
nd
req
uir
es b
ilate
ral a
dju
stm
ents
wit
hce
rtai
n c
ou
ntr
ies;
men
tal h
ealt
hse
rvic
es r
estr
icte
d a
nd
psy
cho
log
ical
care
rei
mb
urs
emen
t re
du
ced
fro
mei
gh
t to
fiv
e se
ssio
ns.
No
rway
Pola
nd
Port
ug
alFr
om
201
1, t
he
follo
win
g h
ealt
hse
rvic
es u
nd
er A
DSE
(th
e h
ealt
h s
yste
mfo
r p
ub
lic s
ecto
r w
ork
ers)
will
cea
se t
ob
e co
vere
d: s
ervi
ces
reg
ard
ing
wo
rkin
gac
cid
ents
an
d p
rofe
ssio
nal
dis
ease
s,cl
inic
al t
rial
s, u
nco
nve
nti
on
alth
erap
euti
cs a
nd
aes
thet
ic s
urg
ery.
AD
SE r
efor
m in
201
1: b
enef
itin
gfr
om
AD
SE b
eco
mes
op
tio
nal
.B
elo
ng
ing
to
th
is s
yste
m w
asal
read
y o
pti
on
al f
or
wo
rker
sen
teri
ng
pu
blic
ad
min
istr
atio
nfr
om
200
6, b
ut
un
til n
ow
was
still
man
dat
ory
fo
r w
ork
ers
wh
o h
ad e
nte
red
pu
blic
adm
inis
trat
ion
bef
ore
200
6.Sp
ecia
lists
th
ink
that
few
peo
ple
will
leav
e A
DSE
.
79

Policy summary
80
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Rep
ub
lic o
fM
old
ova
In 2
009
pri
mar
y h
ealt
h c
are
rece
ived
pri
ori
ty f
inan
cin
g f
rom
man
dat
ory
HIF
s,in
crea
sin
g t
he
com
pen
sate
d m
edic
ines
spec
tru
m a
nd
intr
od
uci
ng
gen
eric
dru
gs
aim
ed a
t tr
eati
ng
th
e m
ost
imp
ort
ant
dis
ease
s re
late
d t
o t
he
dis
ease
bu
rden
and
pu
blic
hea
lth
ris
ks.
The
hea
lth
car
e b
enef
it p
acka
ge
for
the
un
insu
red
was
ext
end
ed t
o t
he
pro
visi
on
of
emer
gen
cy c
are
and
fu
ll co
vera
ge
of
pri
mar
y ca
re, i
ncl
ud
ing
co
mp
ensa
ted
reim
bu
rsed
med
icin
es f
or
ou
tpat
ien
tca
re. (
Prev
iou
sly
all u
nin
sure
d c
itiz
ens
had
the
righ
t on
ly t
o cl
inic
al e
xam
inat
ion
wit
h r
eco
mm
end
atio
ns
for
asse
ssm
ent
and
tre
atm
ent
at t
he
pri
mar
y ca
rele
vel.)
Sin
ce 2
010,
ho
wev
er, t
he
leve
l of
com
pen
sate
d d
rug
s h
as b
een
red
uce
d.
Esse
nti
ally
th
is n
ew le
gis
lati
on
was
no
tb
acke
d u
p w
ith
ad
dit
ion
al b
ud
get
.
In 2
009
ther
e w
as a
rev
iew
of
Nat
ion
alH
ealt
h P
rog
ram
mes
res
ult
ing
in a
nex
ten
sio
n o
f th
e lis
t o
f p
rofi
le d
isea
ses
and
of
resp
ecti
ve p
atie
nt
cate
go
ries
.
Du
rin
g 2
009
and
201
0, t
he
Min
istr
y of
Hea
lth
in c
oope
rati
onw
ith
Nat
ion
al H
ealt
h In
sura
nce
Co
mp
any
mad
e se
vera
l am
end
-m
ents
to
th
e La
w o
n M
HI.
The
law
no
w e
nsu
res
that
mem
ber
so
f h
ou
seh
old
s el
igib
le f
or
soci
alb
enef
its
will
au
tom
atic
ally
be
insu
red
wit
h t
he
MH
I sys
tem
and
rec
eive
fu
lly s
ub
sid
ized
hea
lth
insu
ran
ce. T
wo
add
itio
nal
gro
up
s o
f p
erso
ns
wer
e al
so g
ran
ted
insu
ran
ce in
MH
I: m
oth
ers
of
fou
r o
r m
ore
child
ren
an
d f
ull-
tim
e d
oct
ora
lst
ud
ents
. Th
ese
exte
nsi
on
s in
cove
rag
e ar
e fu
nd
ed b
yin
crea
sed
tra
nsf
ers
fro
m t
he
stat
e b
ud
get
to
th
e m
and
ato
ryH
IFs.
As
a re
sult
, hea
lth
insu
ran
ce c
ove
rag
e, in
clu
din
gfo
r th
e m
ost
vu
lner
able
, has
incr
ease
d (
esti
mat
ed f
igu
res
sug
ges
t in
201
0 it
ro
se t
o 8
2%fr
om
72%
in 2
009)
.
Rev
iew
of
the
fin
anci
ng
of
pre
ven
tive
pro
gra
mm
es,
incr
easi
ng
th
e p
op
ula
tio
nim
mu
niz
atio
n c
ove
rag
e an
du
nd
erta
kin
g m
easu
res
for
pro
mo
tio
n o
f h
ealt
hy
lifes
tyle
edu
cati
on
, acc
ord
ing
to
Euro
pea
n s
tan
dar
ds.
Ro
man
ia

Health policy responses to the financial crisis in Europe – Annexes
Ru
ssia
nFe
der
atio
nPr
ior
to t
he
fin
anci
al c
risi
s in
200
7 th
ere
wer
e d
iscu
ssio
ns
of
com
pre
hen
sive
fr
ee p
har
mac
euti
cal p
rovi
sio
n f
or
ou
tpat
ien
ts in
th
e fr
amew
ork
of
com
pu
lso
ry m
edic
al in
sura
nce
; ho
wev
erth
ese
dis
cuss
ion
s w
ere
dis
con
tin
ued
,p
oss
ibly
bec
ause
of
the
rece
ssio
n.
In m
id 2
011
the
dis
cuss
ion
s w
ere
re-l
aun
ched
an
d a
rei
mb
urs
emen
tp
rog
ram
me
is s
ched
ule
d f
or
2013
–201
5.
Shar
p in
crea
ses
in a
lco
ho
l an
dto
bac
co e
xcis
e ta
xes
pro
po
sed
in 2
009,
to
be
imp
lem
ente
d in
2011
–201
2.
Serb
ia
Slo
vaki
a
Slo
ven
ia
Spai
nC
atal
on
ia: d
eman
ded
com
pen
sati
on
fo
r tr
eati
ng
pat
ien
ts r
esid
ing
in o
ther
auto
no
mo
us
reg
ion
s fr
om
2011
.
Cat
alan
pla
n: f
rom
2011
, ap
ply
a w
aiti
ng
list
man
agem
ent
syst
em a
nd
mak
ech
ang
es in
wai
tin
g li
stp
rio
riti
zati
on
cri
teri
a.
Fro
m A
pri
l 201
0, in
Cat
alo
nia
: red
uct
ion
in n
on
-urg
ent
care
(eye
su
rger
ies,
h
ip a
nd
kn
eere
pla
cem
ent)
.
Swed
en
81

Policy summary
82
Co
un
try
Ben
efit
s (c
ove
rag
e sc
op
e)Po
pu
lati
on
co
vera
ge
(co
vera
ge
bre
adth
)N
on
-pri
ce r
atio
nin
g(w
aiti
ng
tim
es)
Ch
ang
ing
ind
ivid
ual
s’b
ehav
iou
r (h
ealt
h p
rom
oti
on
and
pre
ven
tio
n)
Swit
zerl
and
Sin
ce t
he
beg
inn
ing
of
2011
, eye
gla
sses
are
no
lon
ger
co
vere
d b
y m
and
ato
ryh
ealt
h in
sura
nce
. Th
is is
on
e o
f se
vera
lm
easu
res
inte
nd
ed t
o s
low
wh
at h
ave
oth
erw
ise
bee
n c
on
sist
ent
ann
ual
incr
ease
s in
hea
lth
insu
ran
ce p
rem
ium
s.M
any
op
tici
ans
hav
e re
spo
nd
ed b
yre
du
cin
g e
yeg
lass
pri
ces
for
child
ren
.
The
form
erYu
go
slav
Rep
ub
lic o
fM
aced
on
ia
In J
anu
ary
2011
, th
e M
inis
try
of
Hea
lth
star
ted
a c
amp
aig
n f
or
peo
ple
inre
mo
te r
egio
ns
to h
ave
bet
ter
acce
ss
to c
are.
Th
is in
clu
des
fre
e ch
eck-
up
s in
so
me
villa
ges
.
Un
iver
sal c
ove
rag
e p
rovi
din
ges
sen
tial
ben
efit
s fo
r al
l cit
izen
sw
as in
tro
du
ced
in M
ay 2
009
and
fin
ance
d f
rom
th
e ce
ntr
alb
ud
get
. Th
e o
vera
ll n
um
ber
of
peo
ple
insu
red
has
incr
ease
das
a r
esu
lt. U
niv
ersa
l co
vera
ge
incl
ud
es p
reve
nti
ve c
hec
k-u
ps,
imm
un
izat
ion
, co
vera
ge
of
par
to
f th
e p
osi
tive
list
of
dru
gs
and
tre
atm
ent
for
a ra
ng
e o
f co
mm
un
icab
le d
isea
ses.
Turk
ey
Ukr
ain
eIn
Mar
ch 2
008
Parl
iam
ent
pas
sed
a la
w r
estr
icti
ng
th
ead
vert
isin
g o
f to
bac
co a
nd
alco
ho
l. In
ord
er t
o in
crea
sere
ven
ues
an
d r
edu
ce n
egat
ive
imp
acts
on
hea
lth
, du
rin
g 2
008
and
200
9 th
e g
ove
rnm
ent
and
Parl
iam
ent
reg
ula
rly
rais
edta
xes
on
to
bac
co a
nd
alc
oh
ol

Health policy responses to the financial crisis in Europe – Annexes
pro
du
cts.
As
a re
sult
, th
em
inim
um
exc
ise
du
ty o
nto
bac
co p
rod
uct
s h
as in
crea
sed
mo
re t
han
six
tim
es, t
he
aver
age
pri
ce o
f a
pac
k o
fci
gar
ette
s in
crea
sed
2.5
tim
es.
Smo
kin
g r
estr
icti
on
s w
ere
also
intr
od
uce
d in
pu
blic
pla
ces.
Pro
gra
mm
es a
nd
cen
tral
ized
mea
sure
s to
co
mb
attu
ber
culo
sis
and
on
imm
un
izat
ion
rec
eive
d
pri
ori
ty f
un
din
g in
200
9.
Un
ited
Kin
gd
om
(En
gla
nd
)
A p
rog
ram
me
of
on
e-to
-on
e n
urs
ing
for
can
cer
pat
ien
ts a
nd
a o
ne-
wee
kw
ait
for
can
cer
dia
gn
ost
ics
was
ann
ou
nce
d b
y th
e p
revi
ou
sg
ove
rnm
ent
bu
t n
ot
imp
lem
ente
d;
it w
ill n
ow
no
t b
e ta
ken
fo
rwar
d.
Var
iou
s re
po
rts
of
cuts
in s
ervi
ces
are
emer
gin
g, p
rob
ably
du
e to
less
sp
end
ing
po
wer
res
ult
ing
inso
me
form
of
rati
onin
go
r re
stri
ctio
n in
serv
ices
in t
he
NH
S,al
tho
ug
h m
ore
evid
ence
is n
eed
ed
to c
on
firm
th
is.
Uzb
ekis
tan
83

Policy summary
84
Tab
le A
.3. P
olic
ies
inte
nd
ed t
o a
ffec
t th
e co
sts
of
pu
blic
ly f
inan
ced
hea
lth
car
e in
th
e co
nte
xt o
f th
e ec
on
om
ic c
risi
s, W
HO
Euro
pea
n R
egio
n
No
tes:
No
info
rmat
ion
was
ava
ilabl
e fo
r A
ndor
ra, K
azak
hsta
n, L
uxem
bour
g, M
onac
o, M
onte
negr
o, S
an M
arin
o, T
ajik
ista
n an
d Tu
rkm
enis
tan.
Text
not
in it
alic
s in
dica
tes
a po
licy
whi
ch w
as d
efin
ed b
y th
e re
leva
nt a
utho
ritie
s in
the
cou
ntry
as
a re
spon
se t
o th
e cr
isis
. Tex
t in
ital
ics
indi
cate
s a
polic
y w
hich
was
eith
er p
artia
lly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed b
efor
e th
e cr
isis
but
impl
emen
ted
afte
r w
ithgr
eate
r/le
ss s
peed
/inte
nsity
tha
n pl
anne
d; o
r po
ssib
ly a
res
pons
e to
the
cris
is, t
hat
is, i
t w
as p
lann
ed a
nd im
plem
ente
d si
nce
the
star
t of
the
cris
is, b
ut n
ot d
efin
ed b
y th
e re
leva
nt a
utho
ritie
s as
a r
espo
nse
to t
he c
risis
. A b
lank
cel
l ind
icat
es n
o po
licy
resp
onse
to
the
cris
is (n
ot n
ore
spon
se t
o th
e su
rvey
).
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Alb
ania
Sala
ries
of
heal
th c
are
prof
essi
onal
s ha
ve s
tead
ilyin
crea
sed
in t
he p
ast
few
year
s, w
ith
heal
thw
orke
rsa
lari
es a
t le
vels
appr
oxim
atel
y tw
ice
ashi
gh a
s in
200
5. S
alar
ies
are
expe
cted
to
cont
inue
to in
crea
se, a
ccor
ding
to
appr
oved
bud
gets
.
Arm
enia
Dur
ing
2009
the
Arm
enia
n dr
am w
asfo
rced
to
floa
t as
a r
esul
tof
the
fin
anci
al c
risi
s,le
adin
g to
imm
edia
tein
crea
ses
in t
he c
osts
of
impo
rted
goo
ds,
incl
udin
g m
edic
ines
.
In 2
008,
cas
e-ba
sed
paym
ent
to h
ealt
hfa
cilit
ies
(pol
yclin
ics
and
mat
erni
ty c
linic
s)
for
mat
erni
ty s
ervi
ces
was
intr
oduc
ed b
ased
on
mar
ket
pric
es u
nder
the
Basi
c Be
nefi
t Pa
ckag
e(B
BP),
whi
ch id
enti
fies
Ong
oing
nat
iona
lpr
ogra
mm
espr
iori
tize
pr
imar
y ca
re
and
impr
ovem
ents
in m
ater
nal a
ndch
ild h
ealt
h.

Health policy responses to the financial crisis in Europe – Annexes
heal
th s
ervi
ces
that
shou
ld b
e pr
ovid
edw
itho
ut c
harg
e to
a li
stof
vul
nera
ble
grou
ps
or c
ateg
orie
s, s
uch
asdi
sabl
ed p
eopl
e, o
rpha
nsun
der
18, v
eter
ans
and
fam
ilies
of
war
vic
tim
s,fa
mili
es w
ith
mor
e th
anth
ree
child
ren,
and
child
ren
unde
r 18
wit
hon
e pa
rent
. Pre
viou
sly,
mat
erni
ty s
ervi
ces
had
been
fin
ance
d in
the
sam
e m
anne
r as
all
othe
rBB
P-co
vere
d se
rvic
es(lo
wer
tha
n ac
tual
cos
ts)
prov
idin
g in
cent
ives
for
info
rmal
pay
men
ts.
Aus
tria
The
Fede
rati
on o
f So
cial
Hea
lth
Insu
ranc
e Fu
nds
nego
tiat
ed w
ith
phar
ma -
ceut
ical
com
pani
es t
olo
wer
pri
cing
and
reim
burs
emen
t an
dre
duce
the
cos
t of
dru
gpr
escr
ibin
g by
phy
sici
ans.
Cost
sav
ings
of
EUR
132
mill
ion
in 2
010
and
proj
ecte
d EU
R 22
2m
illio
n by
201
3.
Long
-ter
m c
ontr
acts
wer
e es
tabl
ishe
d fo
rpu
rcha
sing
CT
and
MRI
scan
ners
and
for
med
ical
aids
. Tar
get
to r
educ
esp
endi
ng b
y 0.
5%an
nual
ly b
etw
een
2010
and
2013
. No
savi
ngs
have
yet
bee
n re
port
ed.
The
Fede
rati
on o
f So
cial
Hea
lth
Insu
ranc
e Fu
nds
nego
tiat
ed w
ith
the
Doc
tor’
s A
ssoc
iati
on o
ver
cost
-con
trol
mea
sure
spe
rmit
ting
HIF
s to
mon
itor
cos
t-co
ntro
lpr
acti
ces
and
revi
ew k
eyfi
gure
s. R
esul
ted
insa
ving
s of
EU
R 9
mill
ion
in 2
010.
Curr
ent
gove
rnm
ent
disc
ussi
ons
wit
h th
eLä
nder
are
dev
elop
ing
mod
els
of f
inan
cing
an
d de
liver
ing
care
to
enha
nce
effi
cien
cy a
ndqu
alit
y by
201
2/20
13.
The
Länd
er h
old
hosp
ital
budg
ets
whi
ch h
ave
incr
easi
ngly
gon
e in
to
85

Policy summary
86
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Aus
tria
(con
t.)
debt
; the
se d
ebt
leve
lsin
crea
sed
the
gros
sge
nera
l gov
ernm
ent
debt
by a
bout
EU
R 3
billi
on in
2010
; a f
isca
l equ
aliz
atio
nag
reem
ent
in 2
008
valid
thro
ugh
2014
sti
pula
tes
that
the
gov
ernm
ent
need
s to
dev
elop
ast
rate
gy f
or t
he n
ext
agre
emen
t du
e in
201
4to
alt
er g
over
nanc
e of
heal
th f
inan
cing
on
the
basi
s of
an
eval
uati
on
of t
he u
se o
f ad
diti
onal
mon
ies
the
Länd
erre
ceiv
e an
nual
ly
(EU
R 10
0 m
illio
n) t
ofi
nanc
e ho
spit
al c
are;
corr
ecti
ng im
bala
nces
in
the
sup
ply
chai
n.
Aze
rbai
jan
Ack
now
ledg
ing
the
very
low
leve
l of
sala
ries
, the
gove
rnm
ent
has
been
stea
dily
incr
easi
ng s
taff
sala
ries
for
pub
lic s
ecto
rem
ploy
ees.
Suc
h sa
lary
incr
ease
s w
ere
mad
e in
the
year
s pr
eced
ing
the
fina
ncia
l cri
sis
as w
ell a
sin
201
0. H
owev
er, i
n20
09, n
o re
sour
ces
wer
e
Dur
ing
2009
–201
1, t
hego
vern
men
t co
ntin
ued
to a
lloca
te s
ubst
anti
alre
sour
ces
to u
pgra
deph
ysic
al in
fras
truc
ture
and
equi
pmen
t in
the
publ
ic h
ealt
h se
ctor
,w
hich
suf
fere
d se
vere
lyfr
om u
nder
-inve
stm
ent
duri
ng t
he 1
990s
and
earl
y 20
00s.

Health policy responses to the financial crisis in Europe – Annexes
allo
cate
d to
rai
se s
alar
ies
of t
he h
ealt
h ca
repe
rson
nel;
this
mig
htha
ve b
een
rela
ted
to
the
decr
ease
in p
ublic
reve
nues
rel
ated
to
asi
gnif
ican
t dr
op in
oil
pric
es in
200
9.
Am
ong
the
maj
orch
ange
s im
plem
ente
d in
publ
ic h
ealt
h se
ctor
inre
cent
yea
rs w
as t
hecl
osur
e of
the
maj
orit
y of
sm
all r
ural
hos
pita
ls,
whi
ch r
esul
ted
in a
lmos
ta
50%
red
ucti
on in
the
num
ber
of b
eds
in t
heco
untr
y. O
ptim
izat
ion
of t
he p
ublic
hea
lth
care
netw
ork
is p
art
of t
hena
tion
al h
ealt
h se
ctor
refo
rm a
nd w
as p
lann
edbe
fore
the
cri
sis
bega
n.Th
is is
sup
port
ed t
hrou
gha
Wor
ld B
ank
proj
ect.
Bela
rus
From
200
9, m
edic
ines
whi
ch a
re n
ot n
orm
ally
reim
burs
ed c
an b
ere
gist
ered
and
pre
scri
bed
on p
refe
rent
ial t
erm
s to
indi
vidu
al p
atie
nts
deem
ed t
o be
inpa
rtic
ular
nee
d.
The
prop
orti
on o
fdo
mes
tica
lly p
rodu
ced
med
icin
es in
the
tot
alpu
rcha
sed
amou
nt is
stea
dily
incr
easi
ng (i
n20
09 –
26.
5%, i
n 20
10 –
28.2
%),
and
ther
e is
al
so a
n in
crea
se in
dom
esti
cally
pro
duce
dm
edic
al e
quip
men
t.
From
200
9, r
efor
ms
toin
crea
se t
he e
ffic
ienc
y of
role
s an
d di
stri
buti
on o
fhu
man
res
ourc
es f
orhe
alth
: elim
inat
ion
ofin
effe
ctiv
e po
siti
ons;
intr
oduc
tion
of
stan
dard
son
pop
ulat
ion-
to-s
taff
rati
os a
t ou
tpat
ient
heal
th c
are
inst
itut
ions
;in
trod
ucti
on o
f ne
wpo
siti
ons
wit
hin
exis
ting
staf
fing
leve
ls d
ue t
ofi
lling
vac
ant
orin
effi
cien
tly
used
posi
tion
s); c
onti
nued
incr
ease
s in
bas
ic s
alar
ies
for
heal
th w
orke
rs; t
hein
trod
ucti
on o
f th
epo
siti
on o
f do
ctor
’sas
sist
ant
at o
utpa
tien
tpr
imar
y he
alth
car
ein
stit
utio
ns c
onti
nued
in
Tran
siti
on t
o pe
r ca
pita
budg
ets
has
ensu
red
the
econ
omic
inde
pend
ence
and
incr
easi
ngre
spon
sibi
lity
of h
ealt
hca
re in
stit
utio
ns in
deliv
erin
g m
edic
al c
are.
From
200
9,re
duct
ion
ofov
erhe
ad c
osts
isbe
ing
carr
ied
out
(pri
mar
ily d
ue
to r
educ
tion
s of
adm
inis
trat
ive
cost
s). E
xpen
ditu
reon
fue
l and
ene
rgy
reso
urce
s, t
rans
port
,bu
sine
ss t
rips
,co
mm
unic
atio
nse
rvic
es, e
tc. h
asbe
en r
educ
ed.
Prop
orti
on o
f ex
pens
ive
inpa
tien
t se
rvic
es h
asde
crea
sed
and
reso
urce
sha
ve b
een
redi
rect
ed
to t
he o
utpa
tien
t le
vel
(a t
otal
of
35.0
% o
ut
of t
otal
exp
endi
ture
on
heal
th w
ere
allo
cate
d to
the
out
pati
ent
inst
itut
ions
in 2
009
asco
mpa
red
wit
h 31
.4%
in
200
8).
Plan
s fo
r in
vest
men
t in
exp
ensi
ve f
acili
ties
,co
nstr
ucti
on a
ndeq
uipm
ent,
etc
. hav
ebe
en d
efer
red.
Budg
etar
y fu
nds
have
been
allo
cate
d to
spe
cifi
cpr
ojec
ts a
ccor
ding
to
econ
omic
eva
luat
ions
by
exp
erts
.
87

Policy summary
88
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Bela
rus
(con
t.)
2010
(in
2010
a t
otal
of
732
posi
tion
s of
doc
tor’
sas
sist
ant
wer
e in
trod
uced
as c
ompa
red
wit
h 62
pos
itio
ns in
200
9).
Belg
ium
In 2
010,
a n
ew c
ost-
cont
ainm
ent
mea
sure
intr
oduc
ed a
bia
nnua
lap
plic
atio
n of
aco
mpu
lsor
y pr
ice
redu
ctio
n fo
r “o
ld”
drug
s: d
rugs
rei
mbu
rsed
for
over
12
year
s an
d le
ssth
an 1
5 ye
ars
had
thei
rex
-fac
tory
pri
ce a
ndre
imbu
rsem
ent
basi
sre
duce
d by
15%
, and
drug
s re
imbu
rsed
for
over
15
year
s un
derw
ent
a 17
% r
educ
tion
. New
rule
s in
pla
ce f
orre
imbu
rsem
ent
for
impl
ants
and
med
ical
devi
ces
sinc
e 20
08. P
rice
redu
ctio
ns h
ave
occu
rred
but
the
effe
ct o
n vo
lum
eis
unc
lear
.
Impr
oved
coo
rdin
atio
nof
car
e w
ith
grou
ping
of
GPs
and
the
fin
anci
ng o
fgl
obal
med
ical
rec
ords
.

Health policy responses to the financial crisis in Europe – Annexes
Bosn
ia a
ndH
erze
govi
naV
AT
spen
ding
by
heal
thca
re in
stit
utio
ns in
crea
sed
sign
ific
antl
y in
200
9be
caus
e, f
rom
200
9,fu
nds
to s
ubsi
dize
V
AT
for
heal
th c
are
inst
itut
ions
are
no
long
erin
clud
ed in
fed
eral
and
cant
onal
bud
gets
and
heal
th c
are
inst
itut
ions
no lo
nger
hav
e th
e ri
ght
to V
AT
refu
nds.
HIF
s in
trod
uced
addi
tion
al c
ontr
actu
alm
easu
res
to m
anag
e,re
duce
and
con
trol
cos
tsof
hea
lth
care
pro
vide
rs(t
arge
ting
cap
ital
inve
stm
ents
and
over
head
cos
ts s
uch
asw
ater
, ele
ctri
city
and
phar
mac
euti
cals
and
devi
ces)
and
qua
lity
(min
imum
req
uire
dam
ount
of
stoc
k) s
ince
the
star
t of
the
cri
sis.
As
part
of
gene
ral
refo
rms,
edu
cati
onca
mpa
igns
hav
eta
rget
ed h
ealt
hw
orke
rs (i
.e. f
amily
prac
titi
oner
s,he
alth
inst
itut
ion
and
fund
man
ager
s, e
tc.),
plac
ing
part
icul
arem
phas
is o
nim
prov
ing
heal
thin
stit
utio
nm
anag
emen
t,st
rate
gic
plan
ning
,ne
goti
atin
g sk
ills,
and
mon
itor
ing
and
eval
uati
on.
Bulg
aria
In 2
011
the
Min
istr
y of
Hea
lth
was
pre
pari
ng
to in
trod
uce
diag
nosi
s-re
late
d gr
oups
as p
aym
ent
met
hods
for
acu
teho
spit
al c
are
in 2
012.
In 2
010
the
Min
iste
r of
Hea
lth
intr
oduc
ed a
fee
ceili
ng f
or a
ll ho
spit
alco
ntra
ctor
s of
NH
IF. T
hem
axim
um f
ee f
or a
tea
mof
phy
sici
ans
is B
GN
900
and
BGN
700
for
one
phys
icia
n. P
revi
ousl
y th
e
In 2
009
the
new
gove
rnm
ent
anno
unce
d pl
ans
to r
educ
ead
min
istr
ativ
e an
dov
erhe
ad c
osts
inal
l gov
ernm
ent
inst
itut
ions
by
10%
. In
resp
onse
to t
his
in 2
010
ther
e w
as c
hang
eof
adm
inis
trat
ive
and
man
ager
ial
stru
ctur
e of
the
NH
IF w
hich
aim
ed
Seve
ral r
efor
ms
have
been
intr
oduc
ed in
the
hosp
ital
sec
tor.
In 2
009,
2010
and
201
1 th
e N
HIF
impl
emen
ted
capp
edho
spit
al b
udge
ts b
ylim
itin
g th
e nu
mbe
rs o
fpa
tien
ts f
unde
d. In
201
0a
new
law
and
sta
ndar
dsof
com
pete
nce
wer
ein
trod
uced
wit
h th
e ai
mof
red
ucin
g th
e ov
eral
lnu
mbe
r of
hos
pita
ls a
ndN
HIF
-fun
ded
med
ical
faci
litie
s. In
a r
efor
m
89

Policy summary
90
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Bulg
aria
(con
t.)
fees
wer
e se
t by
eve
ryho
spit
al w
itho
utre
gula
tion
.
In 2
011
the
gove
rnm
ent
was
pla
nnin
g to
ref
orm
purc
hasi
ng o
f m
edic
alde
vice
s by
cen
tral
izin
gce
rtif
icat
ion
of m
edic
aleq
uipm
ent,
labs
and
high
ly s
peci
aliz
edm
edic
al a
ctiv
itie
s an
din
trod
ucin
g a
posi
tive
lis
t of
med
ical
dev
ices
.Th
e go
vern
men
t w
aspl
anni
ng t
o de
cent
raliz
efu
ndin
g fo
r dr
ugs
for
rare
dis
ease
s an
d ca
ncer
from
the
Min
istr
y of
Hea
lth
to t
he N
HIF
.
An
amen
dmen
t of
the
Hea
lth
Insu
ranc
e A
ct
in 2
009
intr
oduc
edde
term
inat
ion
by t
heM
inis
try
of F
inan
ce o
fhe
alth
ser
vice
s pr
ices
fund
ed b
y th
e N
HIF
. The
Min
istr
y of
Fin
ance
was
init
iato
r of
thi
s po
licy.
Unt
il th
at t
ime
pric
esw
ere
nego
tiat
edbe
twee
n th
e N
HIF
and
doct
ors’
org
aniz
atio
ns
to r
educ
e ov
erhe
adco
sts
by s
ever
alth
ousa
nd B
GN
.Fu
rthe
rmor
e, in
2010
the
Min
iste
rof
Hea
lth
anno
unce
d pl
ans
to r
educ
ead
min
istr
ativ
eco
sts
of t
heM
inis
try
by
29.4
% a
mou
ntin
gto
a s
avin
g of
BG
N 4
mill
ion
annu
ally
.
fund
ed b
y BG
N 3
00m
illio
n fr
om t
heEu
rope
an C
omm
issi
onO
pera
tion
al P
rogr
amm
e“R
egio
nal d
evel
opm
ent”
,in
201
0 th
e go
vern
men
tpr
opos
ed: s
tabi
lizat
ion
and
mod
erni
zati
on
of s
tate
onc
olog
ical
hosp
ital
s an
d tr
eatm
ent
cent
res;
res
truc
turi
ng o
fso
me
mun
icip
alit
y an
dst
ate
acut
e an
d lo
ng-
term
car
e ho
spit
als;
clos
ure
of s
ome
smal
lho
spit
als;
mod
erni
zati
onof
sta
te a
nd m
unic
ipal
ity
hosp
ital
s; a
nd c
losu
re
of h
omes
for
soc
ial a
ndm
edic
al c
are
for
child
ren
repl
aced
by
new
day
cent
res.
In 2
011
the
heal
th m
ap w
as r
evis
edso
tha
t it
incl
udes
not
only
the
min
imum
, but
also
the
max
imum
num
ber
of b
eds,
doc
tors
and
heal
th e
stab
lishm
ents
for
each
reg
ion
ofBu
lgar
ia. T
he a
im o
f th
ere
form
was
to
real
loca
tere
sour
ces
acco
rdin
g to
nee
ds.

Health policy responses to the financial crisis in Europe – Annexes
and
incl
uded
in t
heN
atio
nal F
ram
ewor
kCo
ntra
ct. T
he r
efor
m
was
met
wit
h gr
eat
diss
atis
fact
ion
by t
hem
edic
al u
nion
. As
are
sult
a n
ew a
men
dmen
tw
as m
ade
to t
he H
ealt
hIn
sura
nce
Act
in 2
011
and
the
pric
ing
proc
ess
ison
ce a
gain
impl
emen
ted
by n
egot
iati
on b
etw
een
NH
IF a
nd d
octo
rsor
gani
zati
ons.
In 2
011
the
Min
iste
r of
Hea
lth
post
pone
d a
stim
ulus
pol
icy
for
acut
eho
spit
al c
are
due
to
a la
ck o
f re
sour
ces.
Croa
tia
In 2
010
Croa
tia
subs
tant
ially
ref
orm
ed
its
pric
ing
and
reim
burs
emen
tre
gula
tion
for
pres
crip
tion
med
icin
es.
The
who
lesa
le p
rice
s of
all
med
icin
es a
re s
etth
roug
h in
tern
atio
nal
pric
e co
mpa
riso
ns (b
ased
on F
ranc
e, It
aly,
Slo
veni
a,Sp
ain
and
Czec
hRe
publ
ic) a
nd in
tern
alre
fere
nce
pric
ing.
Inte
rnat
iona
l pri
ceco
mpa
riso
ns a
re u
sed
for
sett
ing
max
imum
who
lesa
le p
rice
s.Fi
nanc
ing
of d
rugs
is
reg
ulat
ed b
y cr
oss-
prod
uct
agre
emen
ts a
ndpa
y ba
ck a
gree
men
ts
(i.e.
def
ined
max
imum
expe
ndit
ure
limit
s,ov
ersp
ends
pai
d ba
ck
by p
harm
aceu
tica
l
Ther
e ha
s be
enre
orga
niza
tion
inpr
imar
y ca
re w
hich
incl
udes
cap
itat
ion
paym
ents
to
prim
ary
care
pro
vide
rs t
hat
are
divi
ded
into
"fi
xed"
and
"flo
atin
g" p
aym
ents
.Fi
xed
paym
ents
are
base
d on
fix
ed c
osts
and
floa
ting
pay
men
ts a
reba
sed
on t
he n
umbe
r of
pat
ient
ref
erra
ls t
osp
ecia
lists
, pre
scri
ptio
nco
sts,
pre
vent
ion
care
and
grou
p pr
acti
ce.
Glo
bal b
udge
ts f
orho
spit
als
have
incr
ease
dev
ery
year
up
to 2
010.
Whi
le t
he 2
009
budg
ets
for
hosp
ital
hea
lth
care
incr
ease
d at
rat
e of
3.37
%, t
he 2
010
budg
etw
as r
educ
ed b
y 3.
28%
com
pare
d to
200
9.
As
of F
ebru
ary
2009
pre
scri
ptio
nsfo
r ce
rtai
nm
edic
ines
bec
ame
valid
for
long
er
(six
mon
ths)
, whi
chle
ssen
s th
e bu
rden
on f
amily
med
icin
edo
ctor
s, r
educ
esun
nece
ssar
y vi
sits
and
decr
ease
sad
min
istr
ativ
eco
sts.
In J
anua
ry 2
011
the
Croa
tian
Hea
lth
Insu
ranc
e In
stit
ute
and
Hea
lth
Prot
ecti
on a
t W
ork
mer
ged
to c
reat
eth
e N
HIF
(Cro
atia
nIn
stit
ute
for
Hea
lth
Insu
ranc
e).
An
elec
tron
ic r
ecor
dspr
ojec
t (i.
e. e
-pre
scri
ptio
nan
d e-
refe
rral
s) w
aspi
lote
d in
201
0.
E-pr
escr
ipti
on w
as f
ully
impl
emen
ted
in J
anua
ry20
11. A
s a
resu
lt, t
head
min
istr
ativ
e w
orkl
oad
for
phar
mac
ists
dec
lined
by o
ver
90%
.
91

Policy summary
92
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Croa
tia
(con
t.)
com
pani
es o
r av
oide
d by
tim
ely
dona
tion
s, s
tric
tpe
nalt
ies
for
delib
erat
esh
orta
ges)
. The
sem
easu
res
decr
ease
d dr
ug e
xpen
ditu
re b
y 7%
.
Cypr
usTh
e sa
lari
es o
f al
l pub
licse
ctor
hea
lth
prof
essi
onal
sw
ere
redu
ced.
Inad
diti
on, t
he M
inis
try
of H
ealt
h ha
s ch
ange
ddo
ctor
s’ o
vert
ime
rem
uner
atio
n.
Czec
hRe
publ
icD
rugs
: sim
plif
ied
appr
oval
pro
cess
for
gene
ric
drug
s to
ent
erth
e Cz
ech
mar
ket
intr
oduc
ed in
201
0(f
urth
er m
easu
res
plan
ned
for
2012
).
Med
ical
equ
ipm
ent:
auct
ions
for
pur
chas
ing
new
med
ical
equ
ipm
ent
intr
oduc
ed in
201
1(f
urth
er m
easu
res
plan
ned
for
2012
).
Dec
reas
e of
10%
inex
pend
itur
e on
sal
arie
sof
pub
lic a
dmin
istr
atio
nem
ploy
ees,
incl
udin
gth
ose
wor
king
in h
ealt
hse
ctor
(exc
ept
heal
thpr
ofes
sion
als
such
as
phys
icia
ns, n
urse
s et
c.)
in 2
009.
Phy
sici
ans
wer
eth
reat
ened
wit
h sa
lary
cuts
res
ulti
ng f
rom
prop
osed
red
ucti
ons
of p
aym
ents
to
hosp
ital
sbu
t re
sist
ed (2
0% o
fth
em h
ande
d in
the
irno
tice
). A
s a
resu
ltin
sura
nce
fund
s di
d no
tre
duce
pay
men
ts a
nd
No
incr
ease
in b
udge
t fo
r re
imbu
rsem
ent
ofho
spit
als
by in
sura
nce
fund
s in
201
0. C
hang
e of
rei
mbu
rsem
ent
mec
hani
sms
in h
ospi
tals
from
glo
bal b
udge
tsto
war
ds d
iagn
osis
-re
late
d gr
oups
pla
nned
for
2012
.
Chan
ge in
law
to
enab
le m
ergi
ng
of S
HI f
unds
inor
der
to im
prov
eef
fici
ency
pla
nned
for
2012
.
Rest
ruct
urin
g of
inpa
tien
t be
ds is
bei
ngco
nsid
ered
(ana
lysi
sbe
ing
done
in 2
011)
in
ord
er t
o de
crea
senu
mbe
r of
acu
te c
are
beds
and
incr
ease
num
ber
of b
eds
for
follo
w-u
p ca
re.

Health policy responses to the financial crisis in Europe – Annexes
sala
ries
did
not
dec
reas
e.H
owev
er, p
art
of t
hene
goti
atio
n w
as t
hat
phys
icia
ns a
ccep
ted
othe
r re
form
s.Im
plem
ente
d in
201
1.
Den
mar
kA
s pa
rt o
f on
goin
gpo
licie
s ac
cele
rate
d af
ter
2008
, eff
orts
to
impr
ove
rati
onal
phar
mac
othe
rapy
.
Onl
y lim
ited
incr
ease
s in
sal
arie
s fo
r he
alth
prof
essi
onal
s as
a r
esul
tof
neg
otia
tion
s in
201
1.
As
part
of
ongo
ing
polic
ies
acce
lera
ted
afte
r20
08, i
ncre
ased
use
of
tend
er t
o st
reng
then
com
peti
tion
bet
wee
npr
ovid
ers
(pub
licho
spit
als
outs
ide
each
regi
on, p
riva
te h
ospi
tals
and
supp
liers
to
publ
icho
spit
als
in e
ach
regi
on).
Revi
ews
of h
ospi
tal
budg
ets
to id
enti
fypo
tent
ial s
avin
gs.
As
part
of
ongo
ing
polic
ies
acce
lera
ted
afte
r20
08, c
entr
aliz
atio
n(h
ospi
tal a
ndde
part
men
t cl
osur
es)
to a
chie
ve e
cono
mie
s of
sca
le a
nd r
educ
em
aint
enan
ce c
osts
.
IT im
prov
emen
ts m
ade
aspa
rt o
f on
goin
g po
licie
sac
cele
rate
d af
ter
2008
.
Esto
nia
In M
arch
201
0 th
eM
inis
try
of S
ocia
l A
ffai
rs (M
OSA
) ini
tiat
edam
endm
ents
to
the
min
iste
rial
dec
ree
ondr
ug p
resc
ript
ions
to
sup
port
act
ive
ingr
edie
nt-b
ased
pres
crib
ing
and
disp
ensi
ng. T
heam
endm
ent
did
not
chan
ge p
resc
ribi
ng r
ules
,bu
t do
es r
equi
reph
arm
acie
s to
pro
vide
pati
ents
wit
h th
e dr
ugw
ith
the
low
est
leve
l of
cost
sha
ring
and
to
note
if p
atie
nts
refu
se c
heap
eral
tern
ativ
es. I
n A
pril
2010
the
Hea
lth
EHIF
red
uced
hea
lth
serv
ices
pri
ces
by 6
%fr
om 2
009.
The
obj
ecti
vew
as t
o ba
lanc
e th
ehe
alth
insu
ranc
e bu
dget
wit
hout
dim
inis
hing
acce
ss t
o ca
re. B
efor
e th
e cr
isis
, hea
lth
serv
ice
expe
ndit
ures
(als
o pr
ices
)in
crea
sed
very
rap
idly
and
ther
efor
e th
at 6
%cu
t w
as n
ot a
big
econ
omic
sho
ck f
orpr
ovid
ers.
Sin
ce 2
011
the
pric
e of
hea
lth
serv
ices
has
redu
ced
by 5
%, w
ith
exce
ptio
n of
pri
mar
yca
re w
here
the
red
ucti
onra
te is
low
er (3
%).
93

Policy summary
94
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Esto
nia
(con
t.)
Insu
ranc
e A
ct w
asam
ende
d to
ext
end
the
appl
icat
ion
of
pric
e ag
reem
ents
and
refe
renc
e pr
icin
g to
med
icin
es in
the
low
est
(50%
) rei
mbu
rsem
ent
cate
gory
(som
e ef
fect
ive
drug
s an
d m
any
less
cos
t-ef
fect
ive
drug
s). P
rice
agre
emen
ts p
revi
ousl
yon
ly a
pplie
d to
dru
gsre
imbu
rsed
at
high
erra
tes
(100
%, 9
0% a
nd75
%).
In S
epte
mbe
r 20
10EH
IF la
unch
ed a
n an
nual
gene
ric
drug
pro
mot
ion
cam
paig
n on
tel
evis
ion
and
billb
oard
s in
coop
erat
ion
wit
h M
OSA
,th
e St
ate
Med
icin
esA
genc
y (S
AM
) and
the
Ass
ocia
tion
of
Fam
ilyPh
ysic
ians
(SFM
). A
t th
ebe
ginn
ing
of 2
010
EHIF
and
MO
SA la
unch
ed a
new
e-p
resc
ript
ion
syst
em, w
hich
cur
rent
lyop
erat
es a
long
side
pap
erpr
escr
ibin
g. T
he n
ewsy
stem
mak
es a
ctiv
ein
gred
ient
-bas
edpr
escr
ibin
g ea
sier
.

Health policy responses to the financial crisis in Europe – Annexes
Finl
and
Serv
ice
vouc
hers
intr
oduc
ed f
or s
ocia
lca
re: c
arin
g fo
r cl
ose
rela
tive
s; d
omes
tic
serv
ices
; sup
port
ser
vice
sto
hou
sing
ser
vice
s an
d ho
usin
g se
rvic
e fo
r di
sabl
ed p
eopl
e.In
trod
ucti
on f
or h
ealt
hse
rvic
es w
as p
lann
ed f
or20
11. U
se o
f vo
uche
rs
is in
tend
ed t
o m
itig
ate
publ
ic s
ecto
r pr
essu
res
and
incr
ease
fre
edom
of
cho
ice
of s
ervi
ces
user
s. T
wen
ty-s
even
mun
icip
alit
ies
use
them
; 32
to e
xpan
d or
intr
oduc
e th
em; 6
and
10
for
spe
cial
ized
car
e;
2 an
d 5
for
reha
bilit
atio
n;4
and
13 f
or d
enta
l car
e.
Sign
ific
ant
diff
eren
ces
exis
t ac
ross
mun
icip
alit
ies
due
to v
aria
tion
infi
nanc
ial r
esou
rces
and
avai
labi
lity
of h
ealt
hpr
ofes
sion
als.
Thi
s ha
sle
d to
a r
estr
uctu
ring
and
mer
gers
of
mun
icip
alit
ies
to p
ool
reso
urce
s. B
etw
een
2005
and
2011
the
num
ber
ofm
unic
ipal
itie
s de
crea
sed
from
432
to
336.
Fran
ceSa
ving
s an
tici
pate
d in
2011
due
to
decr
easi
ngco
st o
f he
alth
pro
duct
s,in
clud
ing
grea
ter
use
ofge
neri
c dr
ugs.
From
201
1, d
ecre
ase
in t
he f
ee f
or s
ervi
ces
of c
erta
in h
ealt
hpr
ofes
sion
als.
Five
-yea
r ho
spit
al s
ecto
rin
vest
men
t pl
an (2
008–
2012
) of
EUR
16 b
illio
n of
whi
ch o
nly
EUR
6 m
illio
n is
to b
e sp
ent
in 2
010–
2012
.
Geo
rgia
In 2
009
redu
ced
mar
ket
entr
y ba
rrie
rs a
nd
capi
tal r
equi
rem
ents
fo
r ph
arm
acy
netw
ork
to in
crea
se m
arke
tco
mpe
titi
vene
ss, w
hich
pote
ntia
lly c
ould
bri
ngpr
ices
dow
n. R
ecen
tan
alys
is s
how
s th
at p
rice
sha
ve c
ome
dow
n sl
ight
lyfo
r br
ande
d m
edic
ines
,bu
t no
t fo
r ge
neri
cs.
In r
elat
ion
to c
apit
al a
ndov
erhe
ad c
osts
, in
2007
the
gove
rnm
ent
aim
edto
incr
ease
inve
stm
ents
in u
pgra
ding
or
cons
truc
ting
hea
lth
care
faci
litie
s an
d op
tim
ize
exce
ss p
rovi
der
capa
city
thro
ugh
priv
atiz
atio
n. T
heH
ospi
tal D
evel
opm
ent
Plan
cal
led
for
the
com
plet
e re
plac
emen
t of
95

Policy summary
96
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Geo
rgia
(con
t.)
exis
ting
hos
pita
l inf
ra -
stru
ctur
e w
ithi
n a
thre
e-ye
ar p
erio
d (2
007–
2009
),by
tra
nsfe
rrin
g fu
llow
ners
hip
righ
ts f
rom
the
stat
e to
the
pri
vate
sect
or t
hrou
gh a
tend
erin
g pr
oces
s.H
owev
er, a
s a
resu
lt
of w
ar in
200
8 an
d th
egl
obal
fin
anci
al c
risi
s,in
vest
ors
and,
pri
mar
ily,
deve
lope
rs h
ave
face
dse
riou
s liq
uidi
ty p
robl
ems,
whi
ch h
ave
had
sign
ific
ant
cons
eque
nces
wit
h re
gard
to
fulf
illin
gth
eir
cont
ract
ual
oblig
atio
ns u
nder
thi
spr
ogra
mm
e. A
s a
resu
lt,
impl
emen
tati
on o
f th
eho
spit
al m
aste
r pl
anst
alle
d an
d m
any
orig
inal
inve
stor
s, w
ho p
artic
ipat
edin
the
ten
ders
, had
to
wit
hdra
w a
nd f
ace
fina
ncia
l pen
alti
es. T
hego
vern
men
t su
bseq
uent
lyre
solv
ed t
his
issu
e by
iden
tify
ing
new
inve
stor
san
d cu
rren
tly
a la
rge
num
ber
of h
ospi
tals
ar
e be
ing
cons
truc
ted.

Health policy responses to the financial crisis in Europe – Annexes
In 2
010,
the
way
the
Med
ical
Insu
ranc
e fo
r th
ePo
or is
impl
emen
ted
was
chan
ged.
A s
ingl
e co
ntra
ctpe
r re
gion
was
put
out
for
com
peti
tive
ten
der
by t
he g
over
nmen
t, t
hat
is, p
riva
te h
ealt
h in
sure
rsbi
d to
be
the
sole
insu
ranc
e pr
ovid
er o
f th
eM
IP in
any
giv
en r
egio
n.Pa
rt o
f th
e de
al f
orw
inni
ng t
he t
ende
r w
asth
at p
riva
te in
sure
rs h
adto
bui
ld n
ew h
ospi
tals
.Th
is p
rogr
amm
e fo
r ne
win
fras
truc
ture
sho
uld
befi
naliz
ed in
201
2.
Ger
man
y
Gre
ece
The
Mem
oran
dum
aim
sat
sav
ing
EUR
2 bi
llion
from
pha
rmac
euti
cal
prod
ucts
– E
UR
1 bi
llion
was
to
be s
aved
in 2
011
–re
duci
ng p
harm
aceu
tica
lex
pend
itur
e by
1%
of
GD
P.
From
201
1, p
osit
ive
list
of m
edic
ines
rei
ntro
duce
d(it
was
abo
lishe
d in
2006
), w
ith
a fo
cus
onge
neri
cs. R
educ
tion
inV
AT
for
med
icin
es
(11%
to
6.5%
); in
crea
sed
use
of g
ener
ics
(50%
of
med
icin
es in
pub
licho
spit
als
shou
ld b
ege
neri
cs);
max
imum
gene
ric
pric
e is
60%
From
201
1, s
alar
y cu
ts(e
.g. n
urse
s’ s
alar
y cu
t by
14%
com
pare
d w
ith
2009
). Te
mpo
rary
sta
ffem
ploy
ed u
nder
fix
ed-
term
con
trac
ts r
emov
ed.
Redu
ctio
n in
the
repl
acem
ent
of s
taff
w
ho a
re r
etir
ing
(for
fi
ve p
erso
ns w
ho a
rere
tiri
ng o
nly
one
is t
o be
app
oint
ed).
From
201
1, r
educ
tion
in
pha
rmac
ists
’ pro
fit
by15
–20%
. Lib
eral
izat
ion
of p
harm
acie
s: m
ore
than
one
pha
rmac
ist
can
wor
k at
the
sam
eph
arm
acy
and
phar
mac
ies
can
be e
stab
lishe
d in
clos
er p
roxi
mit
y to
ea
ch o
ther
. Ext
ensi
on
of h
ours
, dec
reas
e in
popu
lati
on t
hres
hold
for
sett
ing
up a
pha
rmac
y;re
bate
s av
aila
ble.
Dev
elop
men
t of
a p
rici
ngsy
stem
for
hos
pita
ls o
nba
sis
of m
edic
al c
ases
,w
hich
will
be
used
for
sett
ing
hosp
ital
bud
gets
from
201
3.
A n
ew h
ealt
h la
win
trod
uced
in 2
011
prov
ides
the
cons
titu
tion
of
a m
ain
prim
ary
heal
th c
are
body
nam
ed t
he N
atio
nal
Hea
lth
Serv
ice
Org
aniz
atio
n(E
OPY
Y),
unde
r th
e su
perv
isio
n of
the
Min
istr
ies
ofH
ealt
h an
d So
cial
Solid
arit
y an
dLa
bour
and
Soc
ial
Secu
rity
Ope
rati
on,
wit
h op
erat
ions
begi
nnin
g in
Jun
e20
11. T
he a
ims
ofth
e EO
PYY
are
to
In J
une
2010
, the
new
gov
ernm
ent
that
cam
e to
pow
er e
nact
ed
a la
w t
o es
tabl
ish
a ne
w a
rchi
tect
ure
for
mun
icip
alit
ies
and
regi
ons
(kno
wn
as t
he“K
allik
rati
s” P
lan)
.W
ith
the
Kal
likra
tis
Plan
, 13
regi
ons
have
bee
n cr
eate
din
pla
ce o
f 76
pref
ectu
res
and
the
1034
mun
icip
alit
ies
redu
ced
to f
ewer
than
370
. Und
erth
e re
orga
niza
tion
,
From
201
1, in
trod
ucti
onof
hos
pita
l mer
gers
and
clos
ures
, inc
ludi
ngm
ergi
ng s
ocia
l hea
lth
insu
ranc
e an
d na
tion
alhe
alth
ser
vice
hos
pita
ls.
Nat
iona
l hea
lth
serv
ice
hosp
ital
s’ o
peni
ng h
ours
have
bee
n ex
tend
ed.
Hea
lth
and
Wel
fare
Map
:fr
om 2
010,
a d
ata
and
inde
x sy
stem
is b
eing
deve
lope
d th
roug
hw
hich
(a) c
itiz
ens’
hea
lth
stat
us w
ill b
e re
cord
edan
d (b
) the
suf
fici
ency
,ef
fect
iven
ess
and
effi
cien
cy o
f he
alth
serv
ices
will
be
asse
ssed
.
97

Policy summary
98
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Gre
ece
(con
t.)
of b
rand
ed d
rugs
;ce
ntra
lized
pro
cure
men
tof
med
ical
ser
vice
s an
d go
ods;
pri
vate
indi
vidu
als
are
perm
itte
dto
pro
cure
con
trac
ts;
fine
s fr
om E
UR
500
toEU
R 50
000
if t
here
isde
viat
ion
from
the
appr
oved
bud
get
in a
proc
urem
ent
cont
ract
.
coor
dina
te p
rim
ary
care
, reg
ulat
eco
ntra
ctin
g of
heal
th c
are
prov
ider
s an
d se
t qu
alit
y an
d ef
fici
ency
stan
dard
s, w
ith
the
broa
der
goal
of
alle
viat
ing
pres
sure
on a
mbu
lato
ry a
ndem
erge
ncy
care
inpu
blic
hos
pita
ls.
The
heal
thdi
visi
ons
of t
hem
ain
SHI f
unds
are
tran
sfer
red
and
inte
grat
ed in
thi
sor
gani
zati
on.
regi
onal
hea
lth
auth
orit
ies
are
expe
cted
to
play
a
muc
h gr
eate
rro
le in
man
agin
gan
d or
gani
zing
the
hum
an r
esou
rces
of t
he n
atio
nal
heal
th s
ervi
ce.
New
mea
sure
s in
the
2011
hea
lth
law
allo
wth
e ex
pans
ion
of p
riva
tecl
inic
s in
the
bui
ldin
g of
infr
astr
uctu
re,
deve
lopi
ng n
ewde
part
men
ts, u
nits
an
d la
bora
tori
es, a
ndho
spit
al b
eds,
wit
hin
cert
ain
defi
ned
limit
s in
gro
wth
rat
es.
Expa
nsio
n of
the
elec
tron
ic p
resc
ript
ion
syst
em f
rom
201
1:
it s
houl
d be
use
d in
diag
nost
ic e
xam
inat
ions
and
in in
pati
ent
care
and
the
mai
n in
sura
nce
fund
sar
e ob
liged
to
use
it.
Hun
gary
From
201
0, f
inan
cial
rew
ards
wer
e in
trod
uced
for
the
rati
onal
use
of
dru
gs. D
octo
rs a
rere
war
ded
for
pres
crip
tion
of c
heap
er, b
utth
erap
euti
cally
equi
vale
nt s
ubst
itut
esan
d ph
arm
acie
s m
aypr
omot
e th
e us
e of
th
ese
drug
s by
alt
erin
gdo
ctor
s’ p
resc
ript
ions
. In
201
1 th
e go
vern
men
t
The
Sem
mel
wei
s Pl
anai
ms
at c
reat
ing
a ca
reer
pat
h m
odel
for
heal
th c
are
prof
essi
onal
sth
at, w
ith
chan
ges
inre
mun
erat
ion,
edu
cati
onan
d in
the
con
diti
ons
ofem
ploy
men
t, p
rovi
des
mot
ivat
ion
for
stay
ing
in t
he f
ield
and
wor
king
in H
unga
ry.
In 2
008
fina
ncin
gm
ulti
plie
rs (w
eigh
ting
fact
ors
for
Hom
ogen
eous
Dis
ease
Gro
ups,
HBC
S) f
orin
pati
ent
reha
bilit
atio
nw
ere
rais
ed. S
ince
200
8th
e H
ealt
h In
sura
nce
Fund
Adm
inis
trat
ion
is e
ntit
led
to a
brog
ate
a fi
nanc
ing
cont
ract
if q
ualit
y or
oth
ercr
iter
ia a
re n
ot m
et. I
nA
pril
2009
out
pati
ent
and
inpa
tien
t fi
nanc
ing
Adm
inis
trat
ive
cost
of
the
NH
IFad
min
istr
atio
n is
pla
nned
to
bere
duce
d fr
om
1.5%
to
1%.

Health policy responses to the financial crisis in Europe – Annexes
anno
unce
d pl
ans
tore
form
the
pre
scri
ptio
ndr
ug s
ubsi
dy s
yste
m.
chan
ged.
The
re h
ad b
een
a pr
e-de
term
ined
fee
up
to a
cer
tain
vol
ume
limit
.Th
e vo
lum
e lim
it w
asre
duce
d an
d a
floa
ting
fee
for
serv
ices
abo
veth
is li
mit
was
intr
oduc
ed.
How
ever
the
red
ucti
onin
and
unp
redi
ctab
ility
of
the
spe
cial
ist
prov
ider
s’ b
udge
ts w
asun
man
agea
ble
and
inO
ctob
er t
hey
wer
eco
mpe
nsat
ed w
ith
atr
ansf
er o
f an
ext
ra
HU
F 10
.5 b
illio
n (i.
e.
not
incl
uded
in b
udge
tpr
ovis
ions
), th
e re
form
was
rev
erse
d an
d th
eor
igin
al s
yste
m r
esto
red.
In 2
010,
inpa
tien
tpr
ovid
ers
agai
n re
ceiv
edex
tra
fund
ing
in o
rder
to
avoi
d ba
nkru
ptcy
(HU
F27
.5 b
illio
n). I
t w
as s
pent
mai
nly
on t
he d
ebts
of
inst
itut
ions
and
shor
teni
ng s
ome
wai
ting
lists
. By
acce
ptin
g th
ishe
lp, i
nsti
tuti
ons
agre
edto
mak
e a
cons
olid
atio
npl
an, t
o pa
rtic
ipat
e in
are
gula
r de
bt-m
onit
orin
gsy
stem
and
to
coop
erat
ein
ter
rito
rial
cap
acit
yre
stru
ctur
ing.
The
2010
gov
ernm
ent
Sem
mel
wei
s Pl
anen
visa
ged
the
cont
inua
tion
of
thes
ere
form
s in
201
0/20
11.
Extr
a fu
ndin
g w
ill b
e
99

Policy summary
100
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Hun
gary
(con
t.)
used
pri
mar
ily in
thr
eepr
iori
ty a
reas
: to
mod
erni
ze t
he f
leet
of
the
Nat
iona
l Am
bula
nce
Serv
ice,
to
stre
ngth
enpr
imar
y ca
re a
nd e
xten
dit
s fu
ncti
ons
(in o
rder
to
redu
ce t
he b
urde
n of
spec
ializ
ed c
are)
, and
to
red
uce
the
debt
of
hosp
ital
s an
d he
alth
car
epr
ovid
ers.
To
esta
blis
hfi
nanc
ial s
usta
inab
ility
,ef
fect
ive
and
tran
spar
ent
reso
urce
allo
cati
onm
echa
nism
s ar
e pl
anne
dth
at a
re a
djus
ted
tone
eds.
To
achi
eve
this
,th
e pl
an a
ims
to a
bolis
hth
e st
rict
vol
ume
limit
inin
pati
ent
and
outp
atie
ntca
re. T
reat
men
ts a
bove
the
volu
me
limit
are
plan
ned
to b
e re
imbu
rsed
acco
rdin
g to
the
var
iabl
eco
st o
f th
e ca
se. T
hepr
esen
t fe
e-fo
r-se
rvic
esy
stem
in a
mbu
lato
ryca
re w
ould
be
repl
aced
by a
syst
em o
f am
bula
tory
Hom
ogen
eous
Dis
ease
Gro
ups
(Hun
gari
anve
rsio
n of
dia
gnos
is-
rela
ted
grou
ps).

Health policy responses to the financial crisis in Europe – Annexes
Icel
and
As
of M
arch
200
9,
offi
cial
pre
scri
ptio
n ru
les
mus
t no
w b
e fo
llow
ed(i.
e. c
erta
in g
ener
ics
mus
t be
pre
scri
bed
befo
re t
ryin
g co
stlie
ral
tern
ativ
es),
othe
rwis
epa
tien
ts m
ust
pay
100%
of d
rug
cost
s. A
s a
resu
lt,
appl
icab
le d
rug
cost
sw
ere
redu
ced
by 1
0.7%
from
200
9 to
201
0.
In 2
009,
indi
vidu
al h
ealt
hca
re o
rgan
izat
ions
wer
eta
sked
wit
h cu
ttin
ghe
alth
wor
ker
sala
ries
. A
com
mon
app
roac
h w
as t
o cu
t ov
erti
me
and
nigh
t sh
ifts
, and
to
leng
then
shi
fts
that
requ
ire
few
er s
taff
,tr
avel
cos
ts, c
onti
nuin
ged
ucat
ion,
etc
. Thi
saf
fect
ed m
edic
al d
octo
rsan
d re
gist
ered
nur
ses,
as
wel
l as
othe
r he
alth
car
epr
ofes
sion
als
and
heal
thca
re s
taff
. A n
umbe
r of
the
se h
ealt
h ca
reem
ploy
ees
lost
the
ir jo
bs.
For
exam
ple,
ove
r 70
0pe
ople
hav
e lo
st t
heir
jobs
at
the
Nat
iona
lU
nive
rsit
y ho
spit
al in
th
e pe
riod
200
7–20
10(a
ppro
xim
atel
y 10
% o
fto
tal s
taff
). A
ccor
ding
to
surv
eys,
the
se c
uts
have
crea
ted
nega
tive
att
itud
esam
ong
staf
f. C
urre
ntly
ther
e ar
e ph
ysic
ian
vaca
ncie
s in
man
y he
alth
care
org
aniz
atio
nsar
ound
the
cou
ntry
. In
addi
tion
, the
ave
rage
age
of m
edic
al d
octo
rs
is in
crea
sing
dra
mat
ical
ly,
as m
edic
al d
octo
rsch
oose
not
to
retu
rn
to t
he c
ount
ry a
fter
obta
inin
g th
eir
spec
ializ
atio
n ab
road
.
In O
ctob
er 2
008,
the
Min
istr
y of
Hea
lth
and
Min
istr
yof
Soc
ial A
ffai
rsm
erge
d to
red
uce
adm
inis
trat
ive
cost
s an
d in
crea
seef
fici
ency
. The
rear
e in
tent
ions
to
mer
ge t
heD
irec
tora
te o
fH
ealt
h an
d th
ePu
blic
Hea
lth
Inst
itut
e of
Ic
elan
d in
201
1.
Ther
e ha
ve b
een
anu
mbe
r of
hea
lth
cent
re m
erge
rs.
For
exam
ple
ther
ew
ere
arou
nd 2
0ru
ral h
ealt
h ce
ntre
sin
200
7 bu
t by
2011
the
re w
ere
only
12.
101

Policy summary
102
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Irel
and
Rene
goti
atio
n of
dea
lsw
ith
phar
mac
euti
cal
com
pani
es f
rom
201
0.
In 2
009:
mor
ator
ium
on
rec
ruit
men
t an
dpr
omot
ion,
non
-re
plac
emen
t of
sta
ff
on le
ave,
end
ing
ofte
mpo
rary
con
trac
ts,
staf
f tr
ansf
er, v
olun
tary
redu
ndan
cy, c
utba
cks
ined
ucat
ion
and
trai
ning
.In
the
201
0 bu
dget
: low
erfe
es p
aid
to c
ontr
acte
dpr
ofes
sion
als
(GPs
and
othe
r hea
lth p
rofe
ssio
nals)
prod
ucin
g es
tim
ated
savi
ngs o
f EU
R 65
9 m
illio
n.In
the
201
1 bu
dget
:re
duce
d ag
ency
and
locu
m s
taff
ing,
red
uced
prof
essi
onal
fee
s, e
arly
reti
rem
ent
and
volu
ntar
yre
dund
ancy
pro
pose
d.
From
200
8, r
educ
edan
nual
fee
to
GPs
who
trea
t m
edic
al c
ard
hold
ers.
From
200
9, r
educ
tion
of
8% o
n al
l pro
fess
iona
lfe
es a
nd c
ut t
o ph
arm
acy
fees
of
24–3
4%. F
urth
ercu
ts in
fee
s of
5%
for
heal
th p
rofe
ssio
nals
wer
e in
trod
uced
in
2010
and
201
1.
HSE
com
mit
men
tin
200
9 to
red
uce
adm
inis
trat
ive,
man
agem
ent
and
adve
rtis
ing
cost
s by
at
leas
t 3%
.
Cuts
in a
dmin
istr
a -ti
ve s
pend
ing
intr
oduc
ed in
201
0bu
dget
, inc
ludi
ngre
duci
ng H
SE
staf
f by
600
0 (E
UR
300
mill
ion)
plus
add
itio
nal
effi
cien
cies
in t
heH
SE (E
UR
90 m
illio
n).
Cuts
inad
min
istr
atio
n(E
UR
43 m
illio
n)w
ere
prop
osed
inth
e 20
11 b
udge
t.
Mea
sure
s to
pro
vide
mor
e se
rvic
es w
ith
few
erre
sour
ces:
hos
pita
l day
care
incr
ease
d by
5%
inth
e fi
rst
six
mon
ths
of20
09 r
elat
ive
to 2
008
and
abov
e th
e 20
09ta
rget
. Out
pati
ent
(OPD
)ap
poin
tmen
ts in
crea
sed
by 3
% b
etw
een
the
firs
tsi
x m
onth
s of
200
8 an
d20
09, a
nd t
he n
umbe
r of
new
OPD
att
enda
nces
have
incr
ease
d by
6%
in
the
sam
e pe
riod
.H
ospi
tal c
apac
ity
redu
ced
by 5
19 b
eds
betw
een
Janu
ary
and
July
200
9.
Isra
el
Ital
yFr
om 2
010,
per
form
ance
mea
sure
men
t in
trod
uced
and
linke
d to
pay
men
t of
pro
vide
rs a
s a
cost
-co
ntai
nmen
t m
easu
re.
Kyr
gyzs
tan

Health policy responses to the financial crisis in Europe – Annexes
Latv
iaIn
200
9 ph
arm
aco-
ther
apeu
tic
refe
renc
egr
oups
wer
e ex
tend
edan
d m
ore
atte
ntio
n w
as g
iven
to
the
inte
rnat
iona
l com
pari
son
of p
harm
aceu
tica
l pri
ces.
The
Cent
re o
f H
ealt
hEc
onom
ics
re-e
valu
ated
the
cost
–eff
ecti
vene
ssan
d pr
ices
for
the
trea
tmen
t of
HIV
/AID
S in
200
9 an
d sp
ecif
ied
reco
mm
enda
tion
s fo
r th
e pr
escr
ibin
g of
phar
mac
euti
cals
.Pr
evio
usly
, the
phar
mac
euti
cals
for
HIV
/AID
S w
ere
purc
hase
dce
ntra
lly b
ut h
ave
been
incl
uded
in t
here
imbu
rsem
ent
syst
emsi
nce
2010
. On
the
basi
sof
an
eval
uati
on o
f co
st–e
ffec
tive
ness
and
nego
tiat
ions
wit
hco
mpa
nies
on
pric
ere
duct
ions
bas
ed o
nin
tern
atio
nal
com
pari
sons
, the
Cen
tre
of H
ealt
h Ec
onom
ics
mad
e si
gnif
ican
t pr
ice
redu
ctio
ns –
fro
m 3
%
to 4
9% –
com
pare
d to
pric
es in
200
9. T
his
enab
led
trea
tmen
t fo
r an
incr
easi
ng n
umbe
r of
pat
ient
s fo
r th
e sa
me
amou
nt o
f m
oney
.
In 2
009
apr
ogra
mm
e to
incr
ease
resp
onsi
bilit
ies
and
duti
es f
or f
amily
doct
ors,
incl
udin
gin
crea
sed
supp
ort
for
the
prov
isio
n of
hea
lth
care
at
hom
e w
asin
trod
uced
.
The
Publ
ic H
ealt
hA
genc
y w
as c
lose
din
200
9. M
any
publ
iche
alth
fun
ctio
nsw
ere
dist
ribu
ted
amon
g ot
her
inst
itut
ions
and
som
e w
ere
lost
. A
s pa
rt o
f a
reor
gani
zati
on
of t
he in
stit
utio
nw
hich
dev
elop
sst
ate
polic
y on
avai
labi
lity
ofhe
alth
car
e se
rvic
esan
d m
anag
es t
hest
ate
fina
ncin
g of
heal
th c
are
aim
edat
dim
inis
hing
stat
e ad
min
istr
ativ
eex
pens
es, t
heH
ealt
h Pa
ymen
tCe
ntre
(HPC
) was
esta
blis
hed
in 2
009.
This
cha
nge
was
asso
ciat
ed w
ith a
cut
in t
he p
rogr
amm
esbu
dget
of
LVL
127.
8m
illio
n or
24.
8% in
2009
com
pare
d to
2008
and
sta
ffre
dund
anci
es.
Furt
herm
ore,
th
e to
tal n
umbe
rof
em
ploy
ees
decr
ease
d fr
om31
3 (2
008)
to
139
(200
9). T
here
was
also
reo
rgan
izat
ion
of e
mer
genc
yse
rvic
es. I
n Fe
brua
ry20
09 in
stea
d of
The
num
ber
of p
ublic
lyfu
nded
hos
pita
ls w
ith
inpa
tien
t ca
re p
rovi
sion
in L
atvi
a de
crea
sed
from
88 in
200
8 to
72
in 2
009
and
39 in
201
0. T
henu
mbe
r of
hos
pita
ls p
er10
0 00
0 in
habi
tant
s in
2009
was
3.1
8, c
ompa
red
to 1
.73
in 2
010.
The
num
ber
of h
ospi
tal b
eds
decr
ease
d fr
om 7
46/1
0000
0 in
habi
tant
s in
200
8to
625
in 2
009
and
493
in20
10. I
n 20
09 c
ompa
red
wit
h 20
08 t
he n
umbe
r of
hosp
ital
adm
issi
ons
and
bed
days
in in
pati
ent
hosp
ital
s de
crea
sed
by27
.1%
. Ave
rage
cos
ts
per
sing
le h
ospi
tal s
tay
decr
ease
d by
1.2
% b
utth
e co
st o
f on
e in
pati
ent
day
incr
ease
d by
6.8
%.
The
aver
age
leng
th o
fst
ay in
hos
pita
ls in
200
8w
as 9
.5 d
ays,
com
pare
dto
8.7
in 2
009
and
8.5
days
in 2
010.
In 2
009,
due
to t
he c
losu
re o
fse
vera
l reg
iona
lho
spit
als,
the
act
ivit
y of
and
serv
ices
pro
vide
d by
day
clin
ics
incr
ease
dsi
gnif
ican
tly.
In 2
009
the
num
ber
of p
atie
nts
trea
ted
at d
ay h
ospi
tals
was
39
507,
but
in t
hefi
rst
eigh
t m
onth
s of
2010
it w
as 5
0 93
8. In
2009
the
re w
as a
tot
al o
f37
3 31
3 ho
spit
aliz
atio
ns.
103

Policy summary
104
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Latv
ia (c
ont.
)39
inst
itut
ions
on
e Em
erge
ncy
Med
icar
e Se
rvic
ew
as e
stab
lishe
d in
orde
r to
gra
dual
lyta
ke o
ver e
mer
genc
ym
edic
ine
func
tion
sfr
om M
edic
are
inst
itut
ions
, to
cent
raliz
e th
eem
erge
ncy
syst
eman
d to
sav
e ad
min
-is
trat
ive
cost
s. T
his
redu
ced
the
num
ber
of e
mer
genc
ym
edic
al c
alls
by
10%
in 2
009.
Lith
uani
aTh
e Pl
an f
or t
heIm
prov
emen
t of
Phar
mac
euti
cal
Acc
essi
bilit
y an
d Pr
ice
Redu
ctio
n w
as a
ppro
ved
in J
uly
2009
. Fro
m 2
010
ther
e w
ere
new
requ
irem
ents
for
gen
eric
pric
ing,
e.g
. the
fir
stge
neri
c ha
s to
be
pric
ed 3
0% b
elow
the
orig
inat
or, w
hile
the
seco
nd a
nd t
hird
gen
eric
sm
ust
be p
rice
d at
leas
t10
% le
ss t
han
the
firs
t
Dec
reas
e of
10%
insa
lari
es o
f m
edic
al s
taff
in 2
009
and
6% d
ecre
ase
in 2
010.
Mov
ing
from
the
cur
rent
nati
onal
cas
e-ba
sed
paym
ent
for
hosp
ital
s to
an
inte
rnat
iona
llyre
cogn
ized
sta
ndar
ddi
agno
sis-
rela
ted
grou
ps s
yste
m w
as in
prep
arat
ion
in 2
011.
In 2
009
apr
ogra
mm
e of
reor
gani
zati
on
of t
he n
etw
ork
ofm
edic
al in
stit
utio
nsin
to d
istr
ict,
regi
onal
and
nati
onal
leve
ls
was
intr
oduc
ed.
Uni
ting
hos
pita
lsin
to la
rger
lega
len
titi
es r
educ
edth
e nu
mbe
r of
inst
itut
ions
prov
idin
g he
alth
Hea
lth
care
sys
tem
refo
rms
of 2
009
have
apr
imar
y go
al t
o re
duce
the
volu
me
of in
pati
ent
serv
ices
, whi
le d
irec
ting
avai
labl
e fu
nds
topr
imar
y he
alth
car
e,ou
tpat
ient
aid
(inc
reas
eby
at
leas
t 5%
), as
wel
l as
day
inpa
tien
t (in
crea
seth
e vo
lum
e by
at
leas
t8%
) and
nur
sing
ser
vice
s,an
d to
red
irec
t he
alth
care
spe
cial
ists
to
outp
atie
nt a
nd d
ay

Health policy responses to the financial crisis in Europe – Annexes
gene
ric
to b
e re
imbu
rsed
.A
new
ly p
rice
d ca
talo
gue
of m
edic
ines
whi
ch a
rere
imbu
rsed
fro
m t
heCH
IF w
as e
nact
ed.
Med
icin
es s
tart
ed t
o be
reim
burs
ed a
ccor
ding
to
acti
ve s
ubst
ance
(IN
N) o
fth
e pr
oduc
t an
d pa
tien
tha
s th
e ri
ght
to c
hoos
em
edic
ine
for
whi
ch c
o-pa
ymen
t is
sm
alle
st. T
heba
se p
rice
of
mor
e th
an10
00 m
edic
ines
was
redu
ced.
Bef
ore
this
refo
rm, p
erso
nal e
xpen
ses
for
the
co-p
aym
ents
for
thes
e pr
oduc
ts c
ompr
ised
LTL
130
mill
ion
per
year
;it
is e
stim
ated
tha
t if
pati
ents
cho
ose
chea
per
med
icin
es f
rom
the
new
pric
e ca
talo
gue,
LTL
80
mill
ion
per
year
of
pers
onal
exp
ense
s w
ill
be s
aved
. Com
puls
ory
HIF
expe
ndit
ure
on d
rugs
and
med
ical
dev
ices
inth
e am
bula
tory
car
ese
ctor
dec
reas
ed f
rom
EUR
197.
88 m
illio
n in
200
8to
EU
R 20
1.64
mill
ion
in20
09 a
nd E
UR
189.
22m
illio
n in
201
0, w
hile
the
num
ber
of p
resc
ript
ions
rose
.
care
ser
vice
s by
24.
The
econ
omic
effe
ct is
ant
icip
ated
to b
e LT
L 13
7m
illio
n.
Rest
ruct
urin
g of
the
Min
istr
y of
Hea
lth
and
inst
itut
ions
acco
unta
ble
to
it w
as s
tart
ed in
2009
–201
0.
Reor
gani
zati
on
of p
ublic
hea
lth
–se
ven
publ
ic h
ealt
hin
stit
utio
ns w
ere
mer
ged
in 2
009–
2010
.
surg
ery
serv
ices
, as
wel
las
long
-ter
m c
are.
105

Policy summary
106
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Mal
taA
lega
l fra
mew
ork
to s
eta
max
imum
ref
eren
cepr
ice
at t
he p
oint
of
deci
sion
reg
ardi
ng e
ntry
into
the
for
mul
ary
was
esta
blis
hed
in 2
009.
Thi
sis
yie
ldin
g th
e de
sire
dre
sult
s. D
urin
g 20
10,
cert
ain
pric
es o
f m
edic
ines
decr
ease
d, r
esul
ting
inm
ore
favo
urab
le p
rice
sfo
r pu
blic
pro
cure
men
t.
Net
herl
ands
From
201
0, p
olic
ies
allo
win
g H
IFs
to h
ave
a gr
eate
r ro
le in
purc
hasi
ng c
are
acce
lera
ted,
pla
ying
an
impo
rtan
t ro
le in
the
redu
ctio
n of
pri
ces
of,
for
exam
ple,
med
icin
esan
d ex
ecut
ing
a“p
refe
rent
ial p
olic
y” t
oke
ep d
rug
pric
es u
nder
cont
rol.
From
201
0, a
s pa
rt o
f th
ech
ange
s to
pur
chas
ing
bySH
I fun
ds, p
harm
acis
tsre
ceiv
e a
pre-
defi
ned
fee
for
each
ser
vice
and
bonu
ses
are
rem
oved
.
From
201
0, g
reat
erin
tegr
atio
n of
pri
mar
yca
re a
t th
e co
mm
unit
yle
vel t
o re
duce
use
of
hosp
ital
car
e an
dpr
omot
ion
of e
-men
tal
heal
th t
o in
crea
se s
elf-
man
agem
ent.
In li
ne w
ith
the
refo
rm
of t
he D
utch
hea
lth
care
syst
em in
200
6, f
rom
2010
, the
pri
vate
mar
ket
was
fur
ther
sti
mul
ated
to
inve
st in
the
hea
lth
care
sec
tor.
Ther
efor
e a
syst
em o
f re
gula
ted
prof
it c
reat
ion
in h
ealt
hca
re w
as in
trod
uced
. Thi
ssh
ould
lead
to
exte
rnal

Health policy responses to the financial crisis in Europe – Annexes
(pri
vate
) cap
ital
for
car
ein
nova
tion
s, q
ualit
yim
prov
emen
ts, p
atie
ntlo
gist
ics
and
bett
erse
rvic
e. N
o pr
ofit
s fo
rca
re p
rovi
ders
will
be
allo
cate
d du
ring
the
fir
stth
ree
year
s af
ter
the
date
of in
vest
ing.
Inst
rum
ents
and
regu
lati
ons
are
desi
gned
to
ensu
re c
riti
cal
care
whe
n fi
nanc
ial
prob
lem
s ap
pear
inho
spit
als,
str
essi
ng t
here
spon
sibi
lity
of h
ospi
tals
thro
ugh
an “
earl
yw
arni
ng s
yste
m”.
Exi
tbo
nuse
s fo
r m
anag
ers
inth
e he
alth
car
e se
ctor
are
rest
rict
ed t
o a
max
imum
of E
UR
75 0
00.
Nor
way
Pola
ndA
new
law
was
pre
sent
edby
the
gov
ernm
ent
in20
11, t
o re
gula
te t
here
imbu
rsed
dru
gs m
arke
t.Th
e ke
y el
emen
ts o
f th
ere
gula
tion
s ar
e as
follo
ws:
max
imum
lim
itof
NH
F ex
pend
itur
es f
ordr
ugs
reim
burs
emen
tw
as e
stab
lishe
d at
the
leve
l of
17%
of
tota
lex
pend
itur
es –
whe
n th
e lim
it is
exc
eede
d,pr
oduc
ers
ofph
arm
aceu
tica
ls in
clud
edin
the
rei
mbu
rsem
ent
syst
em w
ill b
e ob
liged
to
New
law
intr
oduc
ed in
2011
to
allo
w h
ospi
tals
to b
e co
rpor
atiz
ed.
They
will
con
tinu
e to
be
publ
icly
ow
ned
but
will
be s
ubje
ct t
o ba
nkru
ptcy
law
s. T
his
is in
tend
ed
to im
prov
e fi
nanc
ial
man
agem
ent.
107

Policy summary
108
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Pola
nd(c
ont.
)pa
y ba
ck c
erta
in a
mou
nts;
max
imum
mar
gin
ondr
ugs
sold
by
who
lesa
lers
and
phar
mac
ies;
pri
ces
ofre
imbu
rsed
dru
gs in
phar
mac
ies
will
be
fixe
d;no
dis
coun
ts a
re a
llow
edbe
twee
n w
hole
sale
rs a
ndph
arm
acie
s. T
he la
w is
very
muc
h cr
itic
ized
by
the
phar
mac
euti
cal
indu
stry
, pha
rmac
ies
and
othe
r in
tere
sted
par
ties
,bu
t ha
s a
stro
ng s
uppo
rtfr
om t
he g
over
nmen
tan
d th
e Pa
rlia
men
t.
Port
ugal
From
201
1, c
entr
aliz
edpr
ocur
emen
t of
med
icin
esan
d di
agno
stic
tes
ts;
redu
ctio
ns in
pri
cing
and
reim
burs
emen
t; f
aste
rav
aila
bilit
y of
gen
eric
s,pr
escr
ibin
g by
act
ive
ingr
edie
nt, p
resc
ribi
nggu
idel
ines
, e-p
resc
ribi
ng.
Mea
sure
s in
clud
ed in
the
2011
nat
iona
l bud
get:
(1) P
rice
red
ucti
on o
nge
neri
c dr
ugs
that
hav
ehi
gh p
rice
s co
mpa
red
wit
h in
tern
atio
nal o
nes,
From
201
0, m
easu
res
rega
rdin
g pu
blic
wor
kers
incl
udin
g he
alth
wor
kers
:
(1) F
reez
ing
sala
ries
.
(2) F
reez
ing
prom
otio
nsan
d ca
reer
pro
gres
sion
inpu
blic
adm
inis
trat
ion.
(3) F
reez
ing
adm
issi
ons
and
redu
cing
the
num
ber
of h
ired
peo
ple
(esp
ecia
llyw
orke
rs w
ith
mor
epr
ecar
ious
con
trac
ts).
(4) R
educ
ing
som
eex
pens
es s
uch
as s
ome
Mov
e to
per
cap
ita
paym
ent
in 2
011.
From
Dec
embe
r20
10: e
limin
atin
gth
e pr
acti
ce o
f“i
ndis
crim
inat
e”ch
eck-
ups
and
rout
ine
exam
sw
itho
utte
chni
cal/s
cien
tifi
cfo
unda
tion
;in
trod
ucin
gm
easu
res
inin
form
atio
nsy
stem
s to
pre
vent
the
pres
crip
tion
of
exa
ms
wit
h no
Targ
et t
o sa
ve
5% o
n cu
rren
tex
pend
itur
e co
sts
inev
ery
depa
rtm
ent/
med
ical
ser
vice
,ex
clud
ing
pers
onne
lco
sts,
in 2
011.
The
Off
ice
of t
heH
igh
Com
mis
sion
erfo
r H
ealt
h is
sche
dule
d fo
rcl
osur
e af
ter
publ
ishi
ng t
heN
atio
nal H
ealt
hPl
an 2
011–
2016
.
Follo
win
g pa
st t
rend
s in
rece
nt y
ears
, the
re h
asbe
en a
red
ucti
on in
hosp
ital
bed
s an
d m
ore
rece
ntly
clo
sure
of
prim
ary
care
cen
tres
.D
ata
rega
rdin
g be
ds p
er10
0 00
0 in
habi
tant
s sh
owa
decr
ease
fro
m 3
36.7
beds
in h
ospi
tals
in 2
008
to 3
34.8
in 2
009
and
from
5.5
bed
s in
pri
mar
yhe
alth
cen
tres
in 2
008
to4.
6 in
200
9. R
egar
ding
the
num
ber
of p
rim
ary

Health policy responses to the financial crisis in Europe – Annexes
star
ting
wit
h th
e m
ost
sold
gen
eric
s om
epra
zol
and
sim
vast
atin
: pri
ces
shou
ld b
e at
leas
t 35
%lo
wer
tha
n th
e br
and
phar
mac
euti
cal d
rug.
(2) P
rice
red
ucti
on o
f7.
5% o
n bi
olog
ical
phar
mac
euti
cal d
rugs
.
(3) P
rice
red
ucti
on o
nsu
pple
men
tary
dia
gnos
tic
and
ther
apeu
tic
proc
edur
es: 5
% o
n cl
inic
aldi
agno
stic
tes
ts a
nd 3
%on
med
ical
imag
ing.
(4) P
rice
red
ucti
on o
f10
% o
n gl
ycae
mic
cont
rol c
onsu
mab
le
test
str
ips
for
diab
etic
s.
(5) P
rice
red
ucti
on o
nha
emod
ialy
sis.
(6) D
ecre
ase
the
pric
e of
phar
ma
good
s su
bsid
ized
by s
tate
by
6%.
trav
el a
nd e
atin
gex
pens
es, o
vert
ime
cost
s,el
imin
atin
g th
epo
ssib
ility
of
rece
ivin
gpu
blic
sal
arie
s w
hile
als
ore
ceiv
ing
pens
ions
. Thi
sle
d to
an
unex
pect
edin
crea
se in
ret
irem
ent
of d
octo
rs; n
earl
y 60
0do
ctor
s ha
d as
ked
for
reti
rem
ent
byN
ovem
ber
2010
.
adva
ntag
e to
th
e pa
tien
t;di
scip
linin
gco
nsum
ptio
n in
am
bula
tory
hosp
ital
; cha
rgin
ga
fina
ncia
l pen
alty
in c
ase
ofin
appr
opri
ate
use
of p
harm
aceu
tica
ldr
ugs.
heal
th c
entr
es, m
ore
rece
ntly
the
re h
as b
een
a sl
ight
dec
reas
e of
prim
ary
heal
th c
entr
es(f
or e
xam
ple
377
in 2
008
to 3
75 in
200
9), b
ut a
very
str
ong
decr
ease
inpr
imar
y he
alth
cen
tre
outp
osts
or
peri
pher
alun
its
(177
8 in
200
8 to
1318
in 2
009)
.
Repu
blic
of
Mol
dova
In 2
009,
dev
elop
men
t of
perf
orm
ance
ass
essm
ent
and
resu
lts-
base
dfi
nanc
ing,
aim
ing
atm
edic
al p
erso
nnel
mot
ivat
ion,
qua
lity
impr
ovem
ent
and
reso
urce
eff
icie
ncy.
Th
e he
alth
pro
vide
rsco
ntra
cted
wit
hin
man
dato
ry h
ealt
hin
sura
nce
are
paid
an
d re
imbu
rsed
in li
new
ith
tari
ffs
and
cost
The
Min
istr
y of
Hea
lth
has
draw
nup
a p
lan
of a
ctio
nto
com
bat
and
mit
igat
e th
eef
fect
s of
the
cri
sis
on p
ublic
hea
lth,
inac
cord
ance
wit
hth
e pr
ovis
ions
of
the
prog
ram
me
tost
abili
ze a
nd r
eviv
eth
e ec
onom
y of
the
coun
try
for
2009
–201
1. It
Des
pite
the
res
tric
tion
sin
trod
uced
by
the
Min
istr
y of
Fin
ance
on
capi
tal i
nves
tmen
ts, a
ndlim
itat
ions
on
staf
fing
and
trai
ning
exp
endi
ture
s,th
e M
inis
try
of H
ealt
hsu
ccee
ded
in m
aint
aini
ngan
d ev
en in
crea
sing
the
fina
ncin
g of
suc
h do
mai
nsby
pas
sing
a n
ewam
endm
ent
in t
he L
awon
Man
dato
ry H
ealt
hIn
sura
nce.
Thu
s a
law
109

Policy summary
110
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Repu
blic
of
Mol
dova
(con
t.)
of m
edic
al s
ervi
ces,
appr
oved
com
mon
ly b
yM
inis
try
of H
ealt
h an
dth
e N
atio
nal H
ealt
hIn
sura
nce
Com
pany
base
d on
a s
peci
alfo
rmul
a th
at in
clud
esca
ps o
n ov
erhe
ads
and
som
e ru
nnin
g co
sts,
and
adju
sted
eac
h ye
ar in
the
cont
ext
of t
he r
ate
ofin
flat
ion
and
tren
ds in
HIF
s’ a
ccum
ulat
ion
ofre
venu
e an
d sp
endi
ng.
envi
sage
sre
dist
ribu
ting
th
e fi
nanc
ing
ofdi
ffer
ent
type
s an
d le
vels
of
heal
th a
ssis
tanc
e,in
clud
ing
inpa
tien
tad
vanc
edte
chno
logy
and
expe
nsiv
e m
edic
alse
rvic
es. P
rior
ity
fund
ing
ofem
erge
ncy
and
prim
ary
heal
th c
are
(mor
e th
an 3
1% o
fth
e fu
nds
of C
MI)
perm
itte
d th
em
aint
enan
ce
of a
cces
s to
appr
opri
ate
med
ical
serv
ices
and
exte
nsio
n of
the
list
of c
ompe
nsat
edm
edic
atio
ns.
adop
ted
by t
hePa
rlia
men
t in
Jul
y 20
10le
giti
mat
ed t
he n
ew“f
und
for
deve
lopm
ent
and
mod
erni
zati
on o
f th
epu
blic
hea
lth
prov
ider
s”w
ithi
n th
e m
anda
tory
heal
th in
sura
nce
fram
ewor
k. T
he f
inan
cial
reso
urce
s co
llect
ed a
reus
ed p
redo
min
antl
y fo
rca
paci
ty d
evel
opm
ent
ofhe
alth
pro
vide
rs, i
nclu
ding
capi
tal i
nves
tmen
ts,
proc
urem
ent
of m
oder
nan
d ex
pens
ive
equi
pmen
t,sa
nita
ry t
rans
port
,in
form
atio
n te
chno
logi
es,
etc.
Inve
stm
ent
plan
s fo
rco
stly
equ
ipm
ent
wer
ere
view
ed a
nd p
ut o
nho
ld in
200
9.
Rom
ania
Und
er p
ress
ure
from
phar
mac
eutic
al c
ompa
nies
and
who
lesa
lers
, the
Min
istr
y of
Hea
lth
upda
ted
pric
es o
fph
arm
aceu
tica
ls t
o re
flec
tth
e ne
w e
xcha
nge
rate
In 2
010
the
gove
rnm
ent
cut
the
sala
ries
of
all
staf
f em
ploy
ed in
the
publ
ic s
ecto
r, in
clud
ing
hosp
ital
phy
sici
ans
and
othe
r ho
spit
al p
erso
nnel
by 2
5%. T
his
led
to
From
200
9 on
war
ds t
hepo
int
valu
e ba
se o
nw
hich
GPs
are
reim
burs
ed d
ecre
ased
as
per
the
fra
mew
ork
cont
ract
whi
ch s
tipu
late
sth
at a
ny f
luct
uati
on in
At
the
begi
nnin
gof
201
1 M
inis
try
ofH
ealt
h an
noun
ced
the
mer
ger
of
111
hosp
ital
s;
71 h
ospi
tals
will
be
con
vert
ed in
to
Befo
re t
he c
risi
s th
eM
inis
try
of H
ealt
han
noun
ced
a pl
an t
obu
ild a
bout
eig
ht n
ewho
spit
als
for
whi
ch a
prel
imin
ary
feas
ibili
tyst
udy
was
don
e. A
s a

Health policy responses to the financial crisis in Europe – Annexes
(it h
ad w
orse
ned
due
to in
flat
ion)
cau
sing
an
incr
ease
in p
rice
s in
200
9.
In 2
011
the
NH
IF c
hang
edth
e re
fere
nce
pric
esy
stem
for
rei
mbu
rsed
drug
s in
ord
er t
o co
ntai
nco
sts
by s
tim
ulat
ing
the
pres
crip
tion
of
med
icin
esw
ith
pric
es b
elow
the
refe
renc
e pr
ice.
A c
law
-bac
k m
echa
nism
for
phar
mac
euti
cal
com
pani
es w
asin
trod
uced
in 2
010
(aft
er V
AT
dedu
ctio
n a
perc
enta
ge f
rom
the
tota
l sal
es o
f re
imbu
rsed
drug
s ha
s to
be
paid
bac
kto
Min
istr
y of
Hea
lth;
the
claw
-bac
k ra
te is
on
asl
idin
g sc
ale
depe
ndin
gon
val
ue o
f to
tal s
ales
).
a de
crea
se in
the
cont
ribu
tion
for
hea
lth
(to
unde
rsta
nd t
he
scal
e of
thi
s it
is w
orth
men
tion
ing
that
in 2
010
wer
e ab
out
1.4
mill
ion
publ
ic e
mpl
oyee
s ou
t of
abo
ut 4
mill
ion
cont
ribu
tors
to
the
HIF
).
the
inco
me
of t
he N
HIF
can
be r
efle
cted
in t
hepa
ymen
t le
vel o
f th
epr
imar
y ca
re.
A n
ew s
yste
m o
f G
Ppa
ymen
t (r
educ
ing
the
per
capi
ta c
ompo
nent
of
GP
reve
nue
in f
avou
r of
fee-
for-
serv
ice
linke
dw
ith
som
e pe
rfor
man
ceev
alua
tion
) and
alim
itat
ion
of n
umbe
r of
hour
s w
orke
d pe
r w
eek
was
pro
pose
d as
par
t of
a re
vise
d G
P fr
amew
ork
cont
ract
in 2
010;
it w
asre
ject
ed b
y G
Ps a
nd w
asbe
ing
revi
sed
in 2
011.
nurs
ing
hom
es f
orth
e el
derl
y.
Incr
ease
dac
coun
tabi
lity
inth
e m
anag
emen
tof
hos
pita
ls w
astr
ansf
erre
d to
loca
lgo
vern
men
t as
part
of
an o
ngoi
ngpr
oces
s of
dece
ntra
lizat
ion.
Plan
to
intr
oduc
e a
new
hea
lth
info
rmat
ion
syst
eman
d an
“in
sure
rca
rd”
in o
rder
to
incr
ease
eff
icie
ncy
in t
he s
yste
m a
ndre
duce
bur
eauc
racy
anno
unce
d in
2010
.
resu
lt o
f th
e fi
nanc
ial
cris
is t
his
plan
was
aban
done
d. P
urch
ase
of e
quip
men
t w
as a
lso
redu
ced.
Russ
ian
Fede
rati
on
An
esse
ntia
l dru
gs li
stpr
icin
g re
gula
tion
,re
gist
erin
g pr
oduc
ers’
pric
es a
nd li
mit
ing
max
imum
who
lesa
le
and
reta
il m
ark-
ups
was
impl
emen
ted
in 2
010.
Libe
raliz
atio
n of
the
lega
l sta
tus
of s
tate
an
d m
unic
ipal
fac
iliti
es:
they
will
bec
ome
eith
er“a
uton
omou
s no
n-pr
ofit
-m
akin
g” “
budg
etar
y” o
r“g
over
nmen
t” f
acili
ties
.Th
e fo
rmer
tw
o ty
pes
will
hav
e th
e ri
ght
toch
arge
cit
izen
s fo
r pu
blic
serv
ices
and
will
be
perm
itted
to g
o ba
nkru
pt.
They
are
to
be p
aid
acco
rdin
g to
fix
ed b
lock
gran
ts f
or a
cer
tain
volu
me
of s
ervi
ces,
wit
h
Ove
rall
RUB
460
billi
on(U
SD 1
5 bi
llion
) is
expe
cted
to
be u
sed
for
a m
oder
niza
tion
pro
ject
over
tw
o ye
ars
(201
1–20
13).
The
split
of
the
addi
tion
al t
axes
col
lect
edis
ske
wed
tow
ards
cap
ital
inve
stm
ent
(bui
ldin
g an
dre
nova
tion
, med
ical
equi
pmen
t –
RUB
300
billi
on),
wit
h th
ein
form
atio
n sy
stem
sde
velo
pmen
t co
mpo
nent
rece
ivin
g RU
B 34
bill
ion
and
the
Med
ical
111

Policy summary
112
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Russ
ian
Fede
rati
on(c
ont.
)
care
pro
vide
d ab
ove
the
thre
shol
d at
the
exp
ense
of t
he c
itiz
ens.
The
cate
gori
zati
on o
ffa
cilit
ies
into
the
thr
eegr
oups
was
exp
ecte
d in
2011
, but
is s
till
ongo
ing,
wit
h ef
fect
as
of 2
013.
Stan
dard
izat
ion
proj
ect
(the
leas
t cl
ear
in t
erm
sof
con
tent
) get
ting
RU
B 13
6 bi
llion
.
Serb
iaTh
e pu
blic
HIF
ask
edph
arm
aceu
tica
lco
mpa
nies
to
redu
ceth
eir
pric
es, a
nd in
resp
onse
pha
rmac
euti
cal
com
pani
es w
aive
d 10
%of
tot
al s
ales
for
Mar
ch20
11 t
hrou
gh M
arch
2012
wit
h th
e po
ssib
ility
of a
n ex
tens
ion
of t
his
arra
ngem
ent.
In s
imila
rfa
shio
n, t
he H
IF is
try
ing
to r
educ
e ex
pend
itur
esfo
r m
edic
al d
evic
es b
ut it
is u
ncle
ar y
et w
heth
erth
is w
ill b
e su
cces
sful
.
Sinc
e 20
10, h
ouse
keep
ing
and
IT s
uppo
rt w
orke
rsin
hea
lth
care
inst
itut
ions
(who
are
pri
vate
lyco
ntra
cted
) hav
e ac
cept
edlo
wer
wag
es s
o th
at t
hey
have
bee
n ab
le t
o ke
epth
eir
cont
ract
s. O
ften
this
has
mea
nt t
hat
thei
rco
ntra
cts
stay
ed t
hesa
me
in d
inar
s (R
SD) b
utde
crea
sed
in r
eal t
erm
sdu
e to
infl
atio
n an
d th
edi
nar
to e
uro
exch
ange
rate
.

Health policy responses to the financial crisis in Europe – Annexes
Slov
akia
Re
fere
nce
base
d dr
ugpr
icin
g w
as in
trod
uced
in
200
9 an
d 20
10. I
t ha
sbe
en t
he k
ey p
olic
ych
ange
mit
igat
ing
the
impa
ct o
f th
e 20
09 c
risi
s.
Acu
te la
ck o
ffu
ndin
g in
the
Gen
eral
Hea
lth
Insu
ranc
e Co
mpa
nyle
d to
del
ayed
paym
ents
to
phar
mac
ies
and
prov
ider
s. T
hego
vern
men
tst
eppe
d in
to
resc
ueit
. Thi
s st
ep w
asdi
sgui
sed
by t
hem
erge
r w
ith
the
Com
mon
Hea
lth
Insu
ranc
e Co
mpa
ny(C
HIC
) on
1 Ja
nuar
y20
10. T
he m
erge
rse
cure
d EU
R 65
mill
ion
from
the
stat
e bu
dget
an
d an
othe
rap
prox
imat
ely
EUR
33 m
illio
n fr
om t
he f
inan
cial
rese
rves
of t
he C
HIC
.
Slov
enia
In
200
9 th
e N
HIF
rev
ised
lists
of
med
icin
es; r
educ
edpr
ices
of
med
icin
esth
roug
h ne
goti
atio
nw
ith
supp
liers
; pro
vide
din
form
atio
n to
the
pub
licre
gard
ing
prop
er u
se o
fm
edic
ines
; pro
vide
dtr
aini
ng in
rat
iona
lpr
escr
ibin
g fo
rph
ysic
ians
; and
red
uced
the
pric
e of
dia
lysi
s du
e to
low
er p
rice
s of
ery
thro
poie
tin.
Mea
sure
s ad
opte
d by
the
gove
rnm
ent
in t
he f
ield
of p
ublic
sec
tor
sala
ries
(tot
al s
avin
gs E
UR
23m
illio
n ea
ch y
ear)
: in
2009
the
re h
as b
een
noad
just
men
t of
bas
ic s
alar
yto
infl
atio
n; in
201
0 th
isad
just
men
t w
as lo
wer
than
infl
atio
n ra
te;
dela
ying
fur
ther
elim
inat
ion
of w
age
disp
arit
ies
(unt
ilec
onom
ic g
row
thim
prov
es s
ubst
anti
ally
);
In 2
009
the
NH
IF r
educ
edth
e pr
ice
of h
ealt
hse
rvic
es (g
ener
ally
) by
2.5%
and
impl
emen
ted
pena
ltie
s fo
r he
alth
car
epr
ovid
ers
rela
ted
to t
hebr
each
of
the
cont
ract
betw
een
the
fund
and
the
prov
ider
.
In 2
009:
sel
ecti
vere
duct
ion
inm
ater
ial c
osts
by
the
NH
IF, r
educ
tion
of d
irec
t co
sts
ofN
HIF
.
In 2
009
the
NH
IF r
educ
edex
pend
itur
e on
ter
tiar
yse
rvic
es b
y 5%
.
113

Policy summary
114
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Slov
enia
(con
t.)
abol
itio
n of
the
allo
wan
cefo
r ov
er-p
erfo
rman
cefr
om A
pril
2009
onw
ards
.N
HIF
intr
oduc
edm
easu
res
to r
educ
eab
sent
eeis
m:
stre
ngth
enin
g th
e la
yco
ntro
l of
abse
nce
from
wor
k; t
rain
ing
inas
sess
men
t m
etho
dsre
gard
ing
abse
nce
from
wor
k fo
r G
Ps.
Spai
nN
atio
nal l
evel
: att
empt
sto
red
uce
phar
mac
euti
cal
expe
ndit
ures
(thr
ough
mor
e fa
vour
able
nego
tiat
ion
wit
h th
e ph
arm
aceu
tica
lpr
ovid
ers,
but
not
thro
ugh
mor
e ef
fici
ent
use
of m
edic
ines
).
Cata
lan
plan
: fro
m
2011
, dev
elop
eff
icie
ntpr
escr
ibin
g st
rate
gies
base
d on
cos
tef
fect
iven
ess,
co
-res
pons
ibili
ty a
mon
gpr
ovid
ers
and
pati
ents
,us
e of
gen
eric
s or
low
er-
cost
alt
erna
tive
.
Nat
iona
l lev
el: s
hort
-te
rm r
educ
tion
of
sala
ries
to
all c
ivil
serv
ants
(hea
lth
pers
onne
l inc
lude
d)in
itia
ted
by t
he T
reas
ury
from
201
0.
Cata
loni
a: n
egot
iati
on o
fco
ntra
cts
wit
h pr
ovid
ers
and
redu
ctio
n in
pric
e pa
idpe
r m
edic
al a
ct r
educ
edby
2%
fro
m 2
011.
Cata
loni
a: f
rom
2011
, dev
elop
prio
riti
zati
onst
rate
gies
in c
linic
alpr
acti
ce; g
uara
ntee
bett
er p
roce
ssor
gani
zati
on;
impr
ove
the
qual
ity
and
effe
ctiv
enes
s of
clin
ical
man
agem
ent
of p
harm
aceu
tica
lpr
escr
ibin
g;m
onit
orin
g qu
alit
yan
d kn
owle
dge
ofhe
alth
pro
fess
iona
ls;in
terv
enti
ons
topr
omot
e re
spon
sible
use
of h
ealt
hse
rvic
es a
mon
g th
e po
pula
tion
.
Cata
loni
a: f
rom
2011
, int
rodu
ctio
nof
adm
inis
trat
ive
sim
plif
icat
ion
rule
s(e
xpec
ted
impa
ct is
to in
crea
se s
avin
gsby
25%
), in
clud
ing
aust
erit
y m
easu
res,
to t
he m
anag
emen
tof
hea
lth
cent
res
and
grea
ter
use
of e
lect
roni
cm
anag
emen
t.
From
201
1, in
Cat
alon
ia:
mor
e us
e of
IT s
yste
man
d e-
heal
th. P
rior
itiz
ein
vest
men
t in
repl
acem
ent
of e
xist
ing
infr
astr
uctu
re (r
athe
rth
an n
ew in
fras
truc
ture
).

Health policy responses to the financial crisis in Europe – Annexes
Swed
enM
any
coun
ty c
ounc
ils a
repl
anni
ng r
educ
tion
s in
hum
an r
esou
rces
thr
ough
an e
mpl
oym
ent
free
ze,
e.g.
by
not
repl
acin
gre
tire
d st
aff
or n
ot u
sing
stan
d-in
s w
hen
pers
onne
lar
e on
sic
k le
ave.
Swit
zerl
and
The
form
erYu
gosl
avRe
publ
ic o
fM
aced
onia
In 2
010,
for
the
fir
st t
ime
the
HIF
use
d re
fere
nce
pric
es f
or d
rugs
on
apo
siti
ve li
st t
hat
isad
just
ed b
ased
on
drug
pri
ces
in S
love
nia,
Croa
tia,
Ser
bia,
Bul
gari
a.Th
is a
llow
ed t
he H
IF t
opu
rcha
se m
ore
new
drug
s w
ithi
n th
e sa
me
budg
et a
nd m
ore
drug
sfo
r th
e in
sure
d w
itho
utco
-pay
men
t (in
crea
se
of 7
6%).
In J
anua
ry 2
011,
to
try
to c
ompe
nsat
e fo
r th
eem
igra
tion
of
heal
thw
orke
rs, t
he M
inis
try
of H
ealt
h ap
prov
ed t
heem
ploy
men
t of
an
addi
tion
al 2
00 d
octo
rs,
60 n
urse
s, 2
0 X
-ray
and
lab
tech
nici
ans
in p
ublic
heal
th o
rgan
izat
ions
,w
hich
will
cos
t EU
R 2–
2.5
mill
ion
annu
ally
. Thi
s is
inte
nded
to
impr
ove
qual
ity
and
acce
ss in
publ
ic h
ealt
h in
stit
utio
ns,
as w
ell a
s to
pre
vent
qual
ifie
d m
edic
al s
taff
from
leav
ing
the
publ
icse
ctor
.
The
HIF
pai
d of
f al
l deb
tsof
hea
lth
inst
itut
ions
in
200
8, c
osti
ngap
prox
imat
ely
EUR
80m
illio
n. A
s a
resu
lt,
tran
sfer
s to
pub
lic h
ealt
hin
stit
utio
ns w
ere
redu
ced
in 2
009
by 6
.1%
.
In A
pril
2010
, the
val
ueof
a c
apit
atio
n po
int
was
dec
reas
ed b
y 10
%
(MK
D 5
) for
pri
mar
yhe
alth
car
e do
ctor
s fo
rsi
x m
onth
s, a
ltho
ugh
this
was
rev
erse
d af
ter
doct
ors
prot
este
d.
To in
crea
se t
he q
ualit
y of
heal
th s
ervi
ces
sinc
e th
ecr
isis
, the
re h
ave
been
mis
cella
neou
s he
alth
sect
or c
hang
es, i
nclu
ding
a re
orga
niza
tion
of
emer
genc
y m
edic
alse
rvic
es, t
hees
tabl
ishm
ent
of a
com
mit
tee
dedi
cate
d to
the
impr
ovem
ent
ofth
e he
alth
sec
tor,
and
impl
emen
tati
on o
f an
inte
grat
ed h
ealt
hm
anag
emen
tin
form
atio
n sy
stem
and
elec
tron
ic h
ealt
h ca
rd.
Turk
eyA
s of
200
9, t
here
imbu
rsem
ent
cap
in t
here
fere
nce
pric
e sy
stem
for
phar
mac
euti
cals
has
been
red
uced
(fro
m22
%) t
o 15
% o
f th
e pr
ice
of t
he m
ost
inex
pens
ive
med
icin
e th
at c
ould
be
pres
crib
ed f
or t
he s
ame
indi
cati
on. A
s a
resu
lt,
115

Policy summary
116
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Turk
ey (c
ont.
)so
me
phar
mac
euti
cal
com
pani
es w
hose
dru
gsw
ere
not
prev
ious
lyco
vere
d ha
ve v
olun
tari
lycu
t th
eir
pric
es in
ord
erto
be
cove
red
agai
n; t
his
has
led
to s
ubst
anti
alsa
ving
s, a
roun
dap
prox
imat
ely
TRY
1 b
illio
n.
Ukr
aine
In O
ctob
er 2
008
pric
esfo
r dr
ugs
and
med
ical
prod
ucts
incr
ease
ddr
amat
ical
ly d
ue t
ocu
rren
cy f
luct
uati
ons.
The
gove
rnm
ent
set
limit
s of
sup
ply
and
sale
sal
low
ance
s fo
r th
e dr
ugs
on t
he e
ssen
tial
dru
gsan
d m
edic
al p
rodu
cts
list
(not
hig
her
than
12%
of
who
lesa
le p
rice
s an
d no
tm
ore
than
25%
of
the
proc
urem
ent
pric
e;
for
drug
s an
d m
edic
alpr
oduc
ts, p
urch
ased
from
bud
geta
ry f
unds
–no
t ex
ceed
ing
10%
for
both
the
who
lesa
le a
ndpr
ocur
emen
t pr
ice)
. Th
e at
tem
pt o
f pr
ice
rete
ntio
n w
as n
otsu
cces
sful
and
res
ulte
d in
As
sala
ry f
alls
und
erpr
otec
ted
expe
ndit
ure,
in 2
009
sala
ryex
pend
itur
e ro
se a
tal
mos
t 3%
(the
n it
slig
htly
dec
reas
ed in
2010
). A
t th
e sa
me
tim
e, t
he g
over
nmen
t's
deci
sion
s re
late
d to
publ
ic s
ecto
r em
ploy
ees
adop
ted
in 2
009
(incr
ease
of
min
imal
an
d ba
sic
sala
ry) a
llow
edit
to
mai
ntai
n an
d ev
ensl
ight
ly r
aise
sal
arie
s (b
y4–
7%) f
or a
ll ca
tego
ries
of m
edic
al p
erso
nnel
.Th
e go
vern
men
tin
trod
uced
an
incr
ease
for
seni
orit
y (n
umbe
r of
wor
king
yea
rs) f
ordo
ctor
s an
d nu
rses
at
a ra
te o
f 10
% t
o 30
%
In 2
009,
des
pite
the
cris
is, t
heM
inis
try
of H
ealt
hde
velo
ped
ave
rtic
ally
org
aniz
edsy
stem
(ran
ging
from
the
Min
istr
yto
hea
lth
care
prov
ider
s) o
fm
anag
emen
t an
dco
ntro
l of
med
ical
care
qua
lity,
w
hich
incl
uded
mon
itor
ing
and
com
plia
nce
wit
hcl
inic
al p
roto
cols
and
med
ical
stan
dard
s.H
owev
er, n
osa
ncti
ons
for
non-
com
plia
nce
wit
hm
edic
al s
tand
ards
or m
otiv
atio
ns t
o
In 2
008
the
gove
rnm
ent
adop
ted
a pr
ogra
mm
e“O
verc
omin
g th
e im
pact
of t
he g
loba
l fin
anci
alcr
isis
and
ong
oing
deve
lopm
ent”
. A s
peci
alse
ctio
n w
as d
evot
ed t
oen
suri
ng t
he p
rovi
sion
of
hig
h-qu
alit
y an
dav
aila
ble
med
ical
serv
ices
, whe
re, i
npa
rtic
ular
, cer
tain
mea
sure
s to
opt
imiz
e th
ene
twor
k of
hea
lth
care
faci
litie
s w
ere
stip
ulat
ed.
In f
act,
the
pro
gram
me
was
not
impl
emen
ted.
In20
09, t
he n
umbe
r of
med
ical
fac
iliti
es h
ad n
otch
ange
d, t
he n
umbe
r of
beds
dec
reas
ed b
y 7%
due
to r
estr
uctu
ring
,in
itia
ted
by lo
cal

Health policy responses to the financial crisis in Europe – Annexes
a re
duct
ion
of t
he r
ange
of d
rugs
ava
ilabl
e. It
als
oin
crea
sed
the
prop
orti
onof
hig
h-co
st d
rugs
,br
ough
t ab
out
are
duct
ion
in t
he n
etw
ork
of p
harm
acie
s, c
ause
d a
rise
of
unem
ploy
men
tin
thi
s se
ctor
and
cont
ribu
ted
to t
hegr
owth
of
soci
al t
ensi
on.
The
gove
rnm
ent,
hav
ing
resp
onde
d to
cri
tici
sm,
impl
emen
ted
a so
fter
and
mor
e m
arke
t-or
ient
ed m
echa
nism
of
pri
ce c
ontr
ol b
yin
trod
ucin
g a
form
ula
that
tak
es in
to a
ccou
ntcu
rren
cy f
luct
uati
ons.
In20
08 d
rug
pric
es r
ose
by15
% c
ompa
red
to t
hepr
evio
us y
ear,
in 2
009
by 4
2%, b
ut in
201
0 by
6.4%
. The
slo
wer
gro
wth
rate
of
pric
es w
as d
ue t
oth
e re
plac
emen
t of
dru
gspu
rcha
sed
in c
ount
ries
wit
h hi
gh c
osts
(Ger
man
yan
d Sw
itze
rlan
d) w
ith
drug
s fr
om c
ount
ries
wit
h lo
wer
cos
ts, i
npa
rtic
ular
fro
m In
dia,
as
wel
l as
drug
s pr
oduc
edlo
cally
.
of s
alar
y, s
igni
fica
ntly
rais
ing
the
sala
ry o
fm
edic
al s
taff
in 2
010
(by
24–5
3%).
Whi
le in
200
8in
USD
equ
ival
ent
the
sala
ries
of
med
ical
pers
onne
l hav
e be
enre
duce
d by
alm
ost
30%
,in
201
0 th
ey a
lmos
tre
turn
ed t
o th
e pr
e-20
08 le
vel.
follo
w t
hem
had
been
sti
pula
ted.
Ther
efor
e th
ispo
licy
had
nopr
acti
cal e
ffec
t on
the
act
ivit
ies
ofm
edic
al p
erso
nnel
.
auth
orit
ies,
whi
ch d
idno
t ha
ve s
uffi
cien
t fu
nds
for
the
mai
nten
ance
of
heal
th f
acili
ties
. As
are
sult
, the
num
ber
ofsm
all r
ural
hos
pita
lsde
crea
sed
by 5
0% a
sth
ey c
hang
ed t
heir
prof
ile t
o am
bula
tory
clin
ics.
Jud
ging
by
the
dyna
mic
s of
the
tot
alex
pend
itur
es, t
he m
ost
affe
cted
fun
ctio
ns a
rein
pati
ent
care
(red
ucti
onof
rea
l exp
endi
ture
s by
13%
, in
USD
equ
ival
ent
by 3
3.6%
), pr
ovis
ion
ofdr
ugs
(by
2.5%
and
25.5
% r
espe
ctiv
ely)
,pr
even
tion
ser
vice
s (9
% a
nd 3
0.3%
), bu
tm
ost
of a
ll, f
ixed
cap
ital
expe
ndit
ures
(by
22.4
%an
d 40
.7%
).
Dur
ing
the
cris
is t
here
have
bee
n ch
ange
s in
the
stru
ctur
e of
bud
geta
ryex
pend
itur
es f
or u
tilit
ies
of f
acili
ties
(gro
wth
in20
09 a
t 2%
wit
h so
me
decl
ine
in 2
010)
. Sha
re
of d
rug
and
food
expe
ndit
ure
has
stay
edre
lati
vely
sta
ble,
whi
leth
e sh
are
of f
ixed
cap
ital
expe
ndit
ures
tha
t do
no
t re
late
to
prot
ecte
dex
pend
itur
e de
clin
edsh
arpl
y in
200
8 (b
y m
ore
than
thr
ee t
imes
) and
in20
10 c
onti
nue
to r
emai
nlo
w (3
.7%
of
tota
l).
117

Policy summary
118
Coun
try
Pric
es o
f m
edic
al
good
sSa
lari
es a
nd m
otiv
atio
nof
hea
lth
sect
or w
orke
rsPa
ymen
ts t
o pr
ovid
ers
Prio
rity
set
ting
or
pro
toco
ls t
och
ange
acc
ess
to t
reat
men
ts,
coor
dina
tion
of
care
and
pat
tern
sof
use
Ove
rhea
d co
sts:
rest
ruct
urin
g th
eM
inis
try
of H
ealt
han
d pu
rcha
sing
agen
cies
Prov
ider
infr
astr
uctu
rean
d ca
pita
l inv
estm
ent
Uni
ted
Kin
gdom
(Eng
land
)
From
Apr
il 20
11, a
t le
ast
two-
year
pay
fre
ezes
for
heal
th p
rofe
ssio
nals
at
a ti
me
of r
isin
g in
flat
ion.
Plan
ned
mea
sure
s to
incr
ease
eff
icie
ncy
incl
ude
cont
inuo
usly
impr
ovin
g w
orkf
orce
prod
ucti
vity
.
Plan
ned
mea
sure
sto
incr
ease
effi
cien
cy in
clud
e:ap
plyi
ng b
est
prac
tice
thro
ugho
ut
the
NH
S in
the
man
agem
ent
of lo
ng-t
erm
cond
itio
ns;
driv
ing
dow
nin
cons
iste
ncie
s in
adm
issi
ons
and
outp
atie
ntap
poin
tmen
ts.
The
adm
inis
trat
ion
budg
et h
as b
een
redu
ced
by 3
3%
in t
he S
pend
ing
Revi
ew f
or t
hepe
riod
Apr
il 20
11 –
Mar
ch 2
014.
One
plan
ned
mea
sure
isa
redu
ctio
n in
the
num
ber
of a
rm’s
-le
ngth
bod
ies
(e.g
.H
ealt
h Pr
otec
tion
Age
ncy,
the
Foo
dSt
anda
rds
Age
ncy
and
the
Nat
iona
lTr
eatm
ent
Age
ncy
for
Subs
tanc
eM
isus
e) f
rom
18
to a
max
imum
of
10
by 2
014.
The
capi
tal s
pend
ing
budg
et h
as b
een
redu
ced
by 1
7% in
the
Spe
ndin
gRe
view
for
the
per
iod
Apr
il 20
11 –
Mar
ch 2
014.
Uzb
ekis
tan

Joint policy summaries
1. Addressing financial sustainability in health systemsSarah Thomson, Tom Foubister, Josep Figueras, Joseph Kutzin, Govin Permanand,Lucie Bryndová
2. Assessing future health workforce needsGilles Dussault, James Buchan, Walter Sermeus, Zilvinas Padaiga
3. Using audit and feedback to health professionals to improve the quality and safety of health careSigne Agnes Flottorp, Gro Jamtvedt, Bernhard Gibis, Martin McKee
4. Health system performance comparison: an agenda for policy, information and researchPeter C. Smith, Irene Papanicolas
HEN produces synthesis reports and summaries (available at http://www.euro.who.int/en/what-we-do/data-and-evidence/health-evidence-network-hen).

The Health Evidence Network (HEN) of theWHO Regional Office for Europe is a trustworthysource of evidence for policy-makers in the53 Member States in the WHO European Region.HEN provides timely answers to questions onpolicy issues in public health, health care andhealth systems through evidence-based reports orpolicy briefs, summaries or notes, and easy accessto evidence and information from a number ofweb sites, databases and documents on its website (http://www.euro.who.int/en/what-we-do/data-and-evidence/health-evidence-network-hen).
The European Observatory on Health Systemsand Policies is a partnership that supports andpromotes evidence-based health policy-makingthrough comprehensive and rigorous analysisof health systems in the European Region. Itbrings together a wide range of policy-makers,academics and practitioners to analyse trendsin health reform, drawing on experience fromacross Europe to illuminate policy issues. TheObservatory’s products are available on its website (http://www.healthobservatory.eu).
ISSN 2077-1584