HEALTH POLICY AND THE COMMUNITY AFETY …...HEALTH POLICY AND THE COMMUNITY SAFETY NET FOR...
8
HEALTH POLICY AND THE COMMUNITY SAFETY NET FOR INDIVIDUALS WITH INTELLECTUAL DISABILITY Harold A. Pollack * University of Chicago School of Social Service Administration, 969 East 60th Street, Chicago, Illinois This article explores social policy developments in the arena of in- tellectual and developmental disabilities. It begins by summarizing the challenges facing persons with intellectual disabilities and their caregivers in 1945. Families depended on a patchwork of over-crowded and under- funded large state institutions. Children with intellectual disabilities were marginalized from education and public services. Shame and stigma, along with the lack of community-based services, led many parents to institutionalize a child. The federal government provided almost no spe- cific assistance for disabled individuals or to their families. Postwar Amer- ica provided fertile ground for parents to act collectively through the emergence of the National Association of Retarded Children (NARC). Partly as a consequence of such organizing, the 1950s marked a surpris- ing turning-point, in which the federal government expanded income support to disabled persons through measures such as Social Security’s ‘‘Disabled Adult Child’’ program and, by the early 1970s, the advent of Supplemental Security Income (SSI). It also reviews the growth of Medic- aid as the dominant payer of medical and social services at the bounda- ries between personal medical services, case management, education, and other social services. The article ends by summarizing current chal- lenges in intellectual disability policy. It notes that the size, complexity, and expense of I/DD services poses inherent challenges, particularly to state and local governments in the current recession. Adjusting for infla- tion, 23 states actually reduced real spending on I/DD services between 2008 and 2009. Controlling for local conditions, politically conservative states enacted deeper cuts and spent a smaller fraction of state income on intellectual disability services than other states. ' 2012 Wiley Periodicals, Inc. Dev Disabil Res Rev 2011;17:44–51. Key Words: intellectual disability; medicaid; public policy; recession INTRODUCTION P olicy interventions for individuals with intellectual dis- ability predate the American Republic. As early as 1752, Benjamin Franklin assisted in the development of the colonies’ first general hospital that served individuals with intellectual and other mental disabilities [Braddock et al., 2005]. An adequate historical account would describe the rise of the asylum during the 19th century and early Progressive efforts. One might also note initiatives such as the Social Se- curity Act’s inclusion of Title V monies to provide services to disabled children [Braddock et al., 2005]. OUT OF THE SHADOWS: THE POSTWAR ERA From the perspective of public policy, World War II provides a sensible, though somewhat arbitrary starting point in considering social insurance and categorical assistance poli- cies to serve persons living with intellectual disabilities. The immediate postwar period also marks the emergence of family caregivers as an organized constituency making specific claims on public policy. 1945 provides a stark reminder of how far American public policies, law, and culture have moved. Before this point (and for a considerable period afterwards), families depended on a patchwork of over-crowded and under-funded large state institutions, forty of which housed more than 3,000 individuals [Braddock et al., 2005]. Forbidding realities of institutional care were far from public view [Rothman and Rothman, 1984]. The war engaged greater awareness of these conditions, partly because of Nazi crimes against people with disabilities, and also because of historical accident. Wartime legal authorities detailed conscientious objectors to institu- tions for the retarded. Some of these conscientious objectors went on to write scathing accounts of the poor conditions they had witnessed ([Richardson, 1946] cited in [Trent, 1994]). This was certainly not the last time that inhumane insti- tutional conditions caused a public outcry. In the early 1960s, Eunice Kennedy Shriver described equally forbidding institu- tional conditions in the pages of the Saturday Evening Post [Braddock, 2010]. In 1967, Look magazine published a series of graphic photos titled ‘‘Christmas in Purgatory’’ [Trent, 1994]. In 1972, young reporter Geraldo Rivera’s television ex- pose of conditions at Staten Island’s Willowbrook Institution produced even greater political and policy responses ([Rothman and Rothman, 1984]; Even in 2011, scandals regarding wrongful deaths and inhumane conditions continue *Correspondence to: Harold A. Pollack, University of Chicago School of Social Service Administration, 969 East 60th Street, Chicago, IL 60637. E-mail: [email protected] Received 6 December 2011; Accepted 11 December 2011 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/ddrr.138 DEVELOPMENTAL DISABILITIES RESEARCH REVIEWS 17: 44 – 51 (2011) ' 2012 Wiley Periodicals, Inc.
Transcript of HEALTH POLICY AND THE COMMUNITY AFETY …...HEALTH POLICY AND THE COMMUNITY SAFETY NET FOR...

HEALTH POLICY AND THE COMMUNITY
SAFETY NET FOR INDIVIDUALS WITH
INTELLECTUAL DISABILITY
Harold A. Pollack*University of Chicago School of Social Service Administration, 969 East 60th Street, Chicago, Illinois
This article explores social policy developments in the arena of in-tellectual and developmental disabilities. It begins by summarizing thechallenges facing persons with intellectual disabilities and their caregiversin 1945. Families depended on a patchwork of over-crowded and under-funded large state institutions. Children with intellectual disabilities weremarginalized from education and public services. Shame and stigma,along with the lack of community-based services, led many parents toinstitutionalize a child. The federal government provided almost no spe-cific assistance for disabled individuals or to their families. Postwar Amer-ica provided fertile ground for parents to act collectively through theemergence of the National Association of Retarded Children (NARC).Partly as a consequence of such organizing, the 1950s marked a surpris-ing turning-point, in which the federal government expanded incomesupport to disabled persons through measures such as Social Security’s‘‘Disabled Adult Child’’ program and, by the early 1970s, the advent ofSupplemental Security Income (SSI). It also reviews the growth of Medic-aid as the dominant payer of medical and social services at the bounda-ries between personal medical services, case management, education,and other social services. The article ends by summarizing current chal-lenges in intellectual disability policy. It notes that the size, complexity,and expense of I/DD services poses inherent challenges, particularly tostate and local governments in the current recession. Adjusting for infla-tion, 23 states actually reduced real spending on I/DD services between2008 and 2009. Controlling for local conditions, politically conservativestates enacted deeper cuts and spent a smaller fraction of state incomeon intellectual disability services than other states. '2012 Wiley Periodicals,Inc.Dev Disabil Res Rev 2011;17:44–51.
Key Words: intellectual disability; medicaid; public policy; recession
INTRODUCTION
Policy interventions for individuals with intellectual dis-ability predate the American Republic. As early as1752, Benjamin Franklin assisted in the development of
the colonies’ first general hospital that served individuals withintellectual and other mental disabilities [Braddock et al.,2005]. An adequate historical account would describe the riseof the asylum during the 19th century and early Progressiveefforts. One might also note initiatives such as the Social Se-curity Act’s inclusion of Title V monies to provide services todisabled children [Braddock et al., 2005].
OUT OF THE SHADOWS: THE POSTWAR ERAFrom the perspective of public policy, World War II
provides a sensible, though somewhat arbitrary starting pointin considering social insurance and categorical assistance poli-cies to serve persons living with intellectual disabilities. Theimmediate postwar period also marks the emergence of familycaregivers as an organized constituency making specific claimson public policy.
1945 provides a stark reminder of how far Americanpublic policies, law, and culture have moved. Before thispoint (and for a considerable period afterwards), familiesdepended on a patchwork of over-crowded and under-fundedlarge state institutions, forty of which housed more than3,000 individuals [Braddock et al., 2005]. Forbidding realitiesof institutional care were far from public view [Rothman andRothman, 1984]. The war engaged greater awareness of theseconditions, partly because of Nazi crimes against people withdisabilities, and also because of historical accident. Wartimelegal authorities detailed conscientious objectors to institu-tions for the retarded. Some of these conscientious objectorswent on to write scathing accounts of the poor conditionsthey had witnessed ([Richardson, 1946] cited in [Trent,1994]).
This was certainly not the last time that inhumane insti-tutional conditions caused a public outcry. In the early 1960s,Eunice Kennedy Shriver described equally forbidding institu-tional conditions in the pages of the Saturday Evening Post[Braddock, 2010]. In 1967, Look magazine published a seriesof graphic photos titled ‘‘Christmas in Purgatory’’ [Trent,1994]. In 1972, young reporter Geraldo Rivera’s television ex-pose of conditions at Staten Island’s Willowbrook Institutionproduced even greater political and policy responses([Rothman and Rothman, 1984]; Even in 2011, scandalsregarding wrongful deaths and inhumane conditions continue
*Correspondence to: Harold A. Pollack, University of Chicago School of SocialService Administration, 969 East 60th Street, Chicago, IL 60637.E-mail: [email protected] 6 December 2011; Accepted 11 December 2011Published online in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ddrr.138
DEVELOPMENTAL DISABILITIESRESEARCH REVIEWS 17: 44 – 51 (2011)
' 2012Wiley Periodicals, Inc.

to regularly surface [Hakim, 2011;Hopkins and Rose, 2011]). Withoutunderstating the impact of such laterdisclosures, revelations in the immediateaftermath of World War II initiatednational debate about topics that hadnot previously been the subject of opendiscussion.
Shame and stigma regarding theetiology of intellectual disability--coupled with the lack of realistic alter-natives or community-basedservices—led many parents to institu-tionalize a child, sometimes withouteven revealing that the child was born.In 1944, the psychologists Eric and JoanErickson had a child diagnosed withDown Syndrome. The Ericksons con-cealed the child from their other chil-dren, saying that he had died at birth([Jones, 2004]; As late as the 1960s,playwright Arthur Miller quietly institu-tionalized his son David, also born withDown Syndrome [Andrews, 2007]).
Even after the establishment ofthe New Deal, the federal governmentprovided almost no specific assistancefor disabled individuals or to their fami-lies. Aid to the aged, blind, and disabledwas regarded as a state or local responsi-bility which, which rare exceptions, laybeyond the purview of federal policy.Federal expenditures specifically identi-fied for intellectual disability servicesamounted to less than $1 million [Brad-dock, 2010].
1950 marked a watershed withthe publication of Pearl Buck’s best-seller, The child who never grew[Buck, 1950]. The child who nevergrew broke taboos by recounting Buck’sgradual discovery of her daughter Caro-lyn’s intellectual disability (which wasactually Phenylketonuria, or PKU).Buck describes her difficult decision toinstitutionalize Carolyn at 9 years ofage: ‘‘I realized then that I must findanother world for my child, one whereshe would not be despised and rejected,one where she could find her own leveland have friends and affection.’’
Buck’s account spurred publica-tion by other parents, most prominentlythe actress Dale Evans’ best-seller, Angelunaware [Rogers, 1953]. These booksand others [Frank, 1952; Tucker, 1954]frankly chronicled the struggle facingeven wealthy parents who sought toaccept and understand the reality oftheir child’s condition, obtain basic edu-cational services, create long-term cus-todial care arrangements that wouldensure reliable and attentive care evenafter these parents were gone. From thevantage point of 2011, it is striking that
these memoirists present caregiving as aprivate tragedy to be understood, a bur-den to be managed, with little expecta-tion of broader public policy interven-tions.
Titles such as The child whonever grew or Angel unaware framedissues of intellectual disability as a mat-ter of parents caring for children. Thisvocabulary and rhetoric was suited tothe times in which these books werewritten and read. It also matched thelife expectancy of many intellectuallydisabled persons. In 1929, the meanlifespan for an infant born with Down’sSyndrome was 9 years [Strauss andEyman, 1996]. As late as 1983, the me-dian age of death among Americansdiagnosed with Down’s syndrome wasonly 25 [Yang et al., 2002].
Mothers of intellectuallydisabled children began tofind each other. Manyfound that they facedcommon challengesranging from the
provision of social andemotional support tofinding appropriatesummer camps,comparing notesregarding specific
therapies and medicalproviders, sharing whatwould later be calledrespite care. Many
parents discovered a needand a capacity for
collective action to obtainservices and resources for
their children.
FAMILY ADVOCACY AND THEFOUNDING OF NARC
Aside from such epidemiologicalfactors, postwar America provided fer-tile ground for parents, especially moth-ers, to act collectively and to politicallymobilize on behalf of their children
with intellectual disabilities. (This sec-tion on parental activism draws uponand updates [Pollack, 2007]). Social his-torians describe the emergence of theNational Association of Retarded Chil-dren (NARC), and, relatedly, families’ambivalent decisions to embrace con-gregant care for disabled children out-side the family home [Castles, 2004;Jones, 2004].
Mothers of intellectually disabledchildren began to find each other.Many found that they faced commonchallenges ranging from the provision ofsocial and emotional support to findingappropriate summer camps, comparingnotes regarding specific therapies andmedical providers, sharing what wouldlater be called respite care. Manyparents discovered a need and a capacityfor collective action to obtain servicesand resources for their children.
Katherine Jones profiles the localactivism of New Jersey housewife LauraBlossfeld, who helped to found whatwould become the New Jersey ParentsGroup for Retarded Children [Jones,2004]. In 1946, Blossfeld placed a localnewspaper advertisement recruitingother parents to join the nascent orga-nization. Her pitch might have beendrawn from a political science textbook:
Each parent can ultimately helphis own child by doing something tohelp all children similarly affected. . .Therefore I suggest an organization forall parents of mentally retarded children,[one that] may well prove to be the firstchapter in a nationwide organization.
Similar appeals were undertakenin nearby states. In 1949, a New YorkCity housewife placed a similar newspa-per advertisement, writing ‘‘Surely theremust be other children like [her son],other parents like myself. Where areyou? Let’s band together and do some-thing for our children!’’ [Castles, 2004].
By 1950, Blossfeld’s New Jerseygroup had expanded to seven chapters.Two years later, parent groups in manystates had mobilized to form theNational Association for Retarded Chil-dren (NARC). NARC offered directservices, nursery school classes, recrea-tional and social groups, counseling andguidance for parents, and referrals tosocial service agencies. NARC chaptersalso conducting need-assessment, estab-lished local lobbying groups, provided orsubsidized training for service providers.By 1960, NARC had 681 local affiliatesand 62,000 members. By 1964, mem-bership exceeded 100,000 [Segel, 1974].
NARC materials emphasized thatintellectual disability crosses racial, eco-
Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK 45

nomic, and class lines. This rhetoricunderplayed actual socio-demographicdisparities in the actual incidence of in-tellectual disability. NARCs inclusiverhetoric also did not reflect the compo-sition of its own membership. A 1974survey indicated that 96% of NARCparents were white. Most were married,had attended college, and reported mid-dle-class incomes [Segel, 1974].
NARCs founding displayed manysimilarities to the founding of othersuccessful voluntary organizations thatfound broad appeal. As the scholar ofpolitical movements Theda Skocpoldescribes this process:
[O]rdinary Americans joined vol-untary membership federations not onlyfor political reasons but also in search ofsociability, recreation, cultural expres-sion, and social assistance. Recruitmentoccurred through peer networks, andpeople usually had a mix of reasons forjoining. Men and women could bedrawn in initially for nonpolitical rea-sons, yet later end up learning aboutpublic issues or picking up skills or con-tacts that could be relevant to legislativecampaigns, electoral politics, or com-munity projects [Skocpol, 2004].
In the case of NARC, this provedto be a potent combination. The orga-nization provided members with mutualsupport, with local chapters facilitatingsuch basic tasks as helping families planbeach vacations. Within the politicalrealm, NARC advocated what wouldbecome special education, and it sup-ported state bond issues to expand resi-dential treatment.
EXPANDING SOCIALINSURANCE
Partly as a consequence of suchorganizing, the 1950s marked a surpris-ing turning-point, in which the federalgovernment enacted major legislation toexpand income support to persons withdisability. Although the great increasesin public expenditures would occur inlater decades, the foundation was laid inseveral key items of legislation. In 1950,Congress authorized public benefits inthe form of ‘‘Aid to the Permanentlyand Totally Disabled (APTD).’’ In 1954,President Eisenhower declared the firstNational Retarded Children’s Week,reflecting the increased visibility of thispopulation [Segel, 1974; Trent, 1994].
By 1956, Social Security Amend-ments created the ‘‘Disabled AdultChild (DAC)’’ program, which author-ized payments to the surviving child ofa retired, disabled, or deceased workerpast the age of 18 if that survivor was
disabled [Braddock et al., 2005]. Underthe provisions of the DAC program, thechild of a retired or disabled worker canreceive up to 50% of the amount avail-able to the primary beneficiary. Thechild of a deceased worker can receiveup to 75% of the amount available tothe primary beneficiary.
The DAC program thus providedthe first pillar of entitlement security forintellectually disabled Americans whomight outlive their primary caregivers.By 1972, �176,000 adults receivedbenefits through the DAC program dueto a diagnosis of mental retardation. (In1972, another 155,000 adults with thesame diagnoses received assistancethrough the APTD program [Gettings,2011]). By 2010, almost a half-millionAmericans receive such benefits due toqualifying diagnoses of autistic disorders(16,684), developmental disorders(3,998) and intellectual disability(441,956) [SSA, 2010].
In 1958, then-RepresentativeGeorge McGovern sponsored the Edu-cation for Mentally Retarded ChildrenAct, which authorized modest federaltraining efforts for the teachers of intel-lectually disabled children [Braddock,2010]. This also blossomed intoexpanded educational supports in a va-riety of settings. Such legislation pro-vided a foundation for what eventuallybecame PL 94-142, the Education forAll Handicapped Children Act, enactedtwo decades later.
During the 1960s, NARC con-tinued to serve as a key constituency,allying itself with other organizations inthe ‘‘mind lobby’’ to advocate for theexpansion of community-based mentalhealth and mental retardation services.David Felicetti, in describing this his-tory, notes that: ‘‘The mind lobbies hearmany critics who will certainly helpshape legislation. . . but they confrontvirtually no political enemies in Con-gress [p. 124]’’ [Felicetti, 1975].
MEDICAID AND MEDICAREThe establishment of Medicare,
Medicaid, Title I education funding,and more during the 1960s providedthe largest components of federal fund-ing for intellectual and developmentaldisability (I/DD) services.
Medicaid in particular has becomethe dominant payer-- not only formedical and long-term care services,but also for a variety of school- andcommunity-based services at the boun-daries between personal medical serv-ices, case management, education, andother social services [Braddock et al.,
2011; Gettings, 2011]. Medicaid’s Inter-mediate Care Facility for Persons withMental Retardation (ICF/MR), and(after 1982) Medicaid’s Home andCommunity-Based Services (HCBS)waiver authority have provided the twoprincipal mechanisms through whichthe federal government supports I/DDservices.
Medicare receives less attention inconnection with the same services. Yetit has also proved important, since manyAmericans with intellectual and devel-opmental disabilities receive benefitsthrough the Social Security system.
The 1960s also saw the creationof an infrastructure for I/DD servicesand research sparked by the 1961-62President’s Panel on Mental Retarda-tion. The Panel issued 97 recommenda-tions, many of which were eventuallyenacted into federal law. Other legisla-tion, notably the 1970 DevelopmentalDisabilities Act and its subsequent reau-thorization, also proved important inbroadening the populations eligible forassistance based on intellectual and de-velopmental disabilities, and in further-ing efforts to move individuals fromlarge public institutions to community-based settings [Gettings, 2011].
Supplemental Security IncomeThe 1972 establishment of Supple-
mental Security Income (SSI) providedwhat may be the final pillar of entitle-ment security for persons living with in-tellectual disabilities [Daly and Bur-khauser, 2003; NRC, 2002] SSI estab-lished a federal assistance program to theaged, blind, and disabled, supplantingthe patchwork of state disability pro-grams and the 1950 APTD amendments.
SSI emerged as an outgrowth ofpolitical debate over the proposed nega-tive income tax of the late 1960s andearly 1970s. By December 2010, 1.5million Americans receive SSI benefitsdue to qualifying diagnoses of autisticdisorders (151,260), developmental dis-orders (271,506), or intellectual disabil-ities (1,077,484). Within these recipientgroups, average monthly benefits are�$549 [SSA, 2011]. Even when com-bined with Food Stamps and other in-kind aid, SSI provides only modest eco-nomic support. Low income remains akey challenge facing many individualswith intellectual disabilities. Even at thismodest level, SSI allows hundreds ofthousands of men, women, and childrento live within their family homes, or tootherwise reside in community settings.
Throughout the 1970s andbeyond, the ‘‘mind lobby’’ continued to
46 Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK

benefit from support that crossed eco-nomic and political boundaries. Forexample, in the early 1980s some offi-cials in the Reagan administrationsought to curtail the scope of benefitsprovided under PL 94-142. They wereopposed by a diverse network of influ-ential family caregivers that includedRepublican Senator Lowell Weickerand conservative columnist George Will[p. 313] [Melnick, 1994].
In large part as a consequence ofthis political change, public expendi-tures on I/DD services have steadilyincreased over the past four decades.Published tallies indicated expendituresof $52.9 billion spent on I/DD servicesby 2009; an inflation-adjusted increaseby a factor of four in such spendingsince 1977 ([Braddock et al., 2011]; Bycomparison, federal expenditures ontraditional welfare—cash assistance forlow-income families with dependentchildren through the TANF pro-gram—was $33.5 billion in FY2009[Schott, 2011]). This $52.9 billion fig-ure itself likely understates public andprivate expenditures on education,income maintenance, health, and socialservices.
The role of litigationThe same political dynamic
played a complementary role in litiga-tion pursued on behalf of intellectuallydisabled persons. Full accounting of theintricate legal history is beyond thescope of this paper. However, severalaspects of this history are especiallynoteworthy [Bazelon, 1973; Melnick,1994; Gettings, 2011].
Some political scientists and legalscholars presented litigation as a substi-tute for other forms of organizing andadvocacy—even at times a harmful sub-stitute that in the long-run proves polit-ically counterproductive [Silverstein,2009]. This critique may have merit insome policy domains; it does not appearto describe the history of I/DD serv-ices. Within this domain, litigation hasproved complementary to other formsof advocacy and to other efforts toimprove the quality and reach of I/DDservices. Such litigation resulted in asubstantial expansion of special educa-tion services, [Melnick, 1994] and theright to humane and decent treatment[Bazelon, 1973].
In accounting, for example, thehistory of litigation surrounding theWillowbrook scandal, Rothman andRothman [p. 353] note that litigationresulted in the transfer of most patientsto appropriate settings. Unlike the case
of severely mentally ill persons, thisdeinstitutionalization resulted in thetransfer of substantial resources acrosscare settings to promote improved out-comes.
Political advocacy complementedlitigation, as disability rights groupswere able to convince legislators to pro-vide the required resources to complywith court rulings. At the same time,litigation proved politically generative,as the discovery process brought to lightsubstandard or inhumane conditions atpublic care facilities.
Political advocacycomplemented litigation,as disability rights groupswere able to convincelegislators to provide therequired resources tocomply with courtrulings. At the sametime, litigation provedpolitically generative, asthe discovery processbrought to light
substandard or inhumaneconditions at public care
facilities.
More recent litigation has alsostrengthened the legal and program-matic foundation of community-basedservices. In the 1999 case, Olmstead v.L.C and E.W., the state of Georgiaappealed a lower-court ruling whichconcluded that the Americans with Dis-abilities Act (ADA) required Georgia toprovide services in the most integratedsetting appropriate to the needs of indi-viduals with disability. Georgia arguedthat the lower court’s ruling would leadto the closing of state hospitals and tothe disruption of important state serv-ices. Originally, 26 states had signed anAmicus Brief in support of Georgia.Many of these states, however, with-drew their support in response to thedisability rights community [Anony-mous, 1999]. Writing for a 6-3Supreme Court majority, Justice RuthBader Ginsberg affirmed the lower-court’s decision:
States are required to place per-sons with mental disabilities in commu-nity settings rather than in institutionswhen the State’s treatment professionalshave determined that community place-ment is appropriate, the transfer frominstitutional care to a less restrictive set-ting is not opposed by the affected indi-vidual, and the placement can be rea-sonably accommodated, taking intoaccount the resources available to theState and the needs of others with men-tal disabilities [Anonymous, 1999].
The shift to community-basedservices
Olmstead proved to be one of themost important decisions in the historyof American disability policy. In affirm-ing the right to community services, itspurred both state and federal provisionof home- and community-based serv-ices for children and adults living withdiverse disabilities.
In part because of these changes,there has been an enormous increase inthe proportion of persons with intellec-tual disabilities who are able to live inthe family home or in other commu-nity care settings. Indeed, the numberof people with intellectual and develop-mental disabilities living in large stateinstitutions declined by almost 85 per-cent between 1965 and 2009, from223,590 to 34,447.
Healthy People 2010 sought to‘‘reduce to zero the number of childrenage 17 and younger living in congregatecare facilities’’ [Larson et al., 2011]. Thenumber of children and youth in publicinstitutions declined by 98 percent, from92,000 to about 1,500. Between 1977and 2009, the number of Americansunder age 21 reported to live in congre-gate settings sharply declined. Mean-while, the proportion of those over theage of 21 living in such settings morethan doubled, from 156,854 to384,011--a trend which often reflectedgreater community care opportunitiesfor autonomy and personal developmentamong intellectually disabled adults.
That same period witnessed dra-matic declines in unit size of residentialsettings that housed individuals livingwith intellectual or developmental set-tings. In 1977, the average number ofpersons per residential setting was 22.5.By 1987, this had dropped to 7.5, andby 2009 had dropped to 2.5 persons persetting [Lakin et al., 2010].
Challenges looking aheadGiven these broad accomplish-
ments and the steady expansion of I/
Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK 47

DD services, several challenges remaincentral:
Public policies have yet to match theincreased life-span and physical well-being ofintellectually disabled persons.
The majority of individuals withmild or moderate intellectual disabilitieswill outlive their parents, who are oftentheir primary caregivers. Indeed731,000 individuals with intellectualdisabilities now live with caregivers overthe age of 60. Many of these older care-givers will themselves experience physi-cal and cognitive challenges.
This is an ironic but inevitableconsequence of the great progress inmedical and social services to the dis-abled themselves [Glasson et al., 2002,2003]. As noted, the median age ofdeath was 25 among Americans diag-nosed with Down’s syndrome. By 1997,median age at-death had nearly doubledto 49 years of age within this same pop-ulation [Yang et al., 2002].
Survival is strongly associated withthe severity of individuals’ intellectualdisability. In one Australian study, me-dian life expectancy was 74.0 yearsamong people with mild disability, 67.6years among those with moderate dis-abilities, and 58.6 years among thosewith severe disabilities [Bittles et al.,2002]. Thus individuals most likely tothrive in the family home or anothercommunity-environment are most likelyto outlive the men and women who aretheir direct caregivers.
Current public policies do notprovide families with the options andassistance required for proper transition
planning. The widely-cited 2010FINDS national survey documentssome of these gaps, as well as familyand individual needs for social support.FINDS data indicate that most familycaregivers do not have a plan for wheretheir loved one would go if they them-selves could no longer able to providecare (62%). Nearly two-thirds of allfamily caregivers worry that the personthey care for might have to go some-where they do not want to live[Anderson et al., 2011].
FINDS web-based dataset mayalso understate service difficulties andmaterial hardship among intellectually
disabled Americans. Ninety percent ofFINDS respondents reported that theywere non-Hispanic white. Fifty-six per-cent reported before-tax income of atleast $60,000 [Anderson et al., 2011].
The transition to a decentralized network ofhome- and community-based care placessignificant burdens on families to select andmonitor services.
The quality of such services is of-ten low. Services are often providedthrough a low-wage, high-turnoverdirect care workforces that requiresimproved training and work conditionsto provide effective care [Stancliffe andLakin, 2005]. In 2009, the medianhourly wage for all direct-care workerswas $10.58. One in four nursing homeworkers and more than a third of aidesworking in agency-based home carelacked health coverage [PHI, 2011].
The shift to decentralized home-and community-based services may alsoheighten economic, race/ethnic, andeducational disparities in access and uti-lization of key services. Communitiesvary in their provision of such services.Higher-income families may also havegreater resources and skills for self-ad-vocacy in successfully obtaining andmonitoring community-based care. Atthe same time, low-income commun-ities bear disproportionate burdens ofintellectual disability, even as these samecommunities often provide more lim-ited access to disability services[Emerson, 2012]. Although existingdata are unclear, research on California
Fig. 2. Changes in state-only funding 2008–2009. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
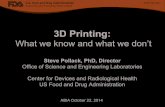
Fig. 1. Real percent change in I/DD expenditures 1978–2009. [Color figure can be viewedin the online issue, which is available at wileyonlinelibrary.com.]
48 Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK

services indicate that nonwhites wereless likely to obtain intellectual disabilityservices [Harrington and Kang, 2008].
The sheer size, complexity, and expense ofI/DD services poses inherent challenges tostate and local government, particularlyduring the current recession.
I/DD services comprise one ofthe largest line items in most statebudgets. Compared with K-12 educa-tion, general Medicaid expenses, andpublic employee retiree benefit obliga-tions, I/DD services may also be partic-ularly susceptible to retrenchment intimes of fiscal stress.
Trends in I/DD expenditures1977-2009
The impact of these state andlocal fiscal challenges is revealed in the2011 edition of State of the States inDevelopmental Disabilities, a periodiccompendium of state policies, servicepatterns, and spending across the UnitedStates. The 2011 edition extends previ-ously-available data from 2006 to fiscalyear 2009, and thus into the currentrecession ([Braddock et al., 2011]; thissection expands [Pollack, 2011b]).
I/DD services serve a politicallyappealing, vulnerable population. Yetthese services impose fiscal burdens onstates and localities experiencing sharpdeclines in tax revenue and sharpincreases in the demand for a variety ofpublic assistance and social services.States’ different approaches to preservingor to cutting these services in hard fiscal
times thus provide a signal of states’larger values and vision of government.
Reliable time-series data regard-ing state I/DD expenditures are avail-able since the late 1970s. As shown inFigure 1 [Braddock et al., 2011], infla-tion-adjusted growth in I/DD expendi-tures far outpaced inflation between1977 and 2002. Growth then precipi-tously dropped as states began to expe-rience the most serious fiscal stress. Bynumerous metrics, state budgetaryretrenchment is the deepest on record.
Between 2008 and 2009, 23 statesactually reduced real spending on I/DDservices. (See Fig. 2 below, reprinted bypermission from David Braddock.)
If one excludes federal dollars, 47states reduced I/DD service spendingbetween fiscal years 2008 and 2009.Nationally, the average spending reduc-tion was 12%, with Alabama, SouthCarolina, Idaho, and Rhode Islandreducing state expenditures by morethan one-quarter [Braddock et al.,2011; Pollack, 2011b].
These changes in federal and stateexpenditure are associated with tangiblechanges in service delivery. An esti-mated 123,000 persons with intellectu-ally disabilities are now on waiting listsfor publicly-funded residential services[Lakin et al., 2010]. Many states havealso curtailed Medicaid-funded ancillaryservices such as dental care, homehealth care, and even hospice servicesprovided under the ambit of Medicaid[Pollack, 2011a].
FINDS data reflects these pat-terns. Sixty-two percent of family care-givers, seventy percent of those caringfor individuals with severe intellectualor developmental disabilities, reportedthat services in their communities weredecreasing [Anderson et al., 2011]. AsAnderson and colleagues report:
Decreasing supports werereported to result in the person withID/DD losing services such as PT, OTand Speech provided by schools (43%),not being able to go outside the homeas much (29%), not seeing friends as
Fig. 3. State fiscal effort 2009. [Color figure can be viewed in the online issue, which isavailable at wileyonlinelibrary.com.]
Fig. 4. Changes in state I/DD spending 2008–2009. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK 49

much (24%), not making as many choices(23%), and not talking to as many people(18%) as they had in the past.
Changes and levels in I/DDexpenditures reflect state specific cir-cumstances. Yet these expenditurechanges also reflect partisan politicalalignment and ideological concerns.Figures 2 and 3 below illustrate thesepatterns.
In Figure 3, the vertical axis rep-resents states 2009 ‘‘fiscal effort’’ on in-tellectual and developmental disabilityservices. Here fiscal effort is operation-alized as dollars spent on I/DD servicesper $1,000 of state personal income.The horizontal axis provides an evensimpler measure of states’ political align-ment, simply operationalized as the pro-portion of state’s voters who cast theirvote for Barack Obama rather than forJohn McCain in the 2008 presidentialelection. The red line corresponds topredicted values, computed on the basisof linear regression weighted by statepopulation size.
As shown, traditionally Republi-can states such as Oklahoma, Utah, Ala-bama, and Texas are clustered in thelower left quadrant of the graph. Incontrast, traditional Democratic statessuch as New York, Connecticut, andMaine are clustered in the upper rightquadrant.
In fact, a one standard-deviation(8.44 percentage points in the popularvote) rise in Candidate Obama’s 2008voting share was associated with anaccompanying 0.54 standard deviationrise (about $1.15 per $1,000 in statepersonal income) in fiscal effort in sup-porting I/DD services. This is a largeobserved association-- corresponding to�27% of states’ mean expenditures.
Regression analysis of the changein state spending yields similar results.Figure 4 below shows the percentagechange in states’ spending on I/DDservices between 2008 and 2009, againgraphed against Barack Obama’s shareof the two-party presidential vote. Asabove, the red line represents predictedvalues based on weighted linear regres-sion.
The same general pattern held. Inthis analysis, a one standard-deviationrise in Barack Obama’s voting share wasassociated with an accompanying 0.47standard deviation rise in states’ fiscaleffort. Especially striking are the num-ber of states with the lowest fiscal effortgoing into the great recession—SouthCarolina, Oklahoma, Texas, and oth-ers—that also implemented the deepestcuts between 2008 and 2009.
Data are not yet available for fiscalyears 2010 and 2011. Subsequent budg-etary retrenchment may prove morepronounced. The 2009 federal stimuluspackage—more formally, the AmericanRecovery and Reinvestment Act of2009—provided key federal assistancethat has now ended. ARRA providedan enhanced federal matching rate forMedicaid services. This provided strongfinancial inducement for states to main-tain Medicaid services. ARRA alsoimposed maintenance of effort require-ments that constrained states’ ability tocut Medicaid or K-12 educational serv-ices. These requirements are no longeroperative, which may facilitate furtherbudget cuts.
CONCLUSIONBy chance, this article was sub-
mitted on the same day that the Obamaadministration announced that theCLASS (Community Living and SocialSupports) Act cannot be implementedas originally defined within the 2009Patient Protection and Affordable CareAct (ACA).
A complex long-term disabilityservices program, CLASS’s abortive tra-jectory exemplifies the continuing chal-lenge to American social insuranceposed by the cost and the complexity ofcare required to assist a diverse disabilitypopulation. This is a particular disap-pointment, especially given the particu-lar value of CLASS [Caldwell, 2010] forpersons with intellectual disabilities liv-ing in community settings.
ACA still provides many impor-tant benefits for citizens with intellec-tual disabilities. The new law establishesexpanded Medicaid benefits for low-income individuals who do not other-wise qualify for public aid, as well assubsidies to moderate-income familieswho obtain health coverage throughhealth insurance exchanges.
The new law institutes insuranceregulations of particular importance tointellectual disability. These include theremoval of lifetime expenditure capsand prohibitions against discriminationin coverage or premiums on the basis ofpreexisting conditions. Adults youngerthan age 26 can now receive coverageunder their parents’ employer-basedpolicies. ACA also supports demonstra-tion projects and initiatives to improveservices to dual-eligible Medicare-Med-icaid recipients. All of these provisionsare of particular value for children andadults with intellectual disabilities. ACAalso offers states valuable options in
addressing some challenges of long-termcare [Reinhard et al., 2011].
ACA does not address servicesthat are provided outside the ambit ofhealth care, many of which are financedat the local level. Policymakers face se-rious challenges in every area of servicedelivery, income maintenance, and clin-ical care. At one level, services for intel-lectual disability are often insulated fromefforts to promote management innova-tion, evidence-based practice, and pay-for-performance that have improvedmedical care systems such as the Veter-an’s Administration [Gettings, 2011].Service agencies are provided funds suf-ficient to provide custodial care. Theyoften accomplish this mission thoughlow labor costs in a low-skill workforce,with accompanying questions of em-ployee morale and turnover.
Policymakers also struggle to pro-vide families with the informationneeded to make wise choices within adecentralized network of communityservices. Few caregivers can scrutinizewhether their daughter or brother isreceiving the right mix of services.Recent scandals exemplify families’deepest fears of custodial care [Hakim,2011; Hopkins and Rose, 2011]. Manypersons with intellectual disability alsoexperience complex physical or psychi-atric comorbidities. Many are treated byphysicians and social service professio-nals who have limited experience inaddressing these concerns.
Notwithstanding these challenges,the arena of intellectual disabilitiesshould be recognized as a genuine,readily-overlooked triumph of Ameri-can social policy. Prodigious expendi-tures reveal the latent generosity of awelfare state which draws stark distinc-tions among recipients of public help.The same society that can stigmatizemillions of people deemed unworthy ofhelp behaves quite differently towardsthose it deems genuinely needy. A para-digmatic example of the worthy poor,persons with intellectual disability nowreceive substantial supports from federal,state, and local government.
Sixty years ago, the birth of achild living with intellectual disabilitieswas regarded as a private tragedy. Tothe extent attention was paid, it wasfocused on family caregivers and some-times on children. The life-course pos-sibilities and challenges facing the indi-vidual himself (or herself) was rarelyconsidered. Persons with intellectualdisabilities were excluded from publiceducation and the labor market,enjoyed no legal protections within the
50 Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK

labor market, had little access to basicincome support and health servicesrequired to enhance their well-being.
Not all of these burdens havebeen lifted. Yet intellectual disabilityservices are now recognized as a propertask of American social insurance. Legalprotections have greatly expanded. Theembrace of persons with intellectual dis-abilities within new media and popularculture has, if anything, been more dra-matic (e.g., [Diament, 2010; Matthews,2011]). Foremost credit for thesechanges belongs to persons with intel-lectual disabilities and their caregivers,who mobilized as a social and politicalforce to bring about needed policychanges.
These historic developments arenoteworthy; they do not merit compla-cency. America’s fragmented and con-tested welfare state often underminesour best efforts to help. I/DD servicesare delivered by state and local govern-ments that increasingly lack the fiscaland administrative capacity to imple-ment these programs well. As the cur-rent recession indicates, this brings areal price. n
ACKNOWLEDGMENTSKruti Acharya, Greg Anrig, Mi-
chael Msall, Veronica Perrone Pollack,and Lainie Friedman Ross provideduseful comments. The Century Foun-dation partially supported the prepara-tion of this manuscript through anadjunct fellowship.
REFERENCESAnderson L, Larson S, Wuorio A. 2011. 2010
FINDS National Survey: family and Individ-ual needs for disability supports. Available athttp://www.thearc.org/document.doc?id53141 (accessed October 18, 2011).
Andrews S. 2007. Arthur Miller’s missing act.Minneapolis, Minnesota: Vanity Fair.
Anonymous. 1999. Supreme Court UpholdsADA ‘Integration Mandate’ in Olmsteaddecision. Available at http://www.accessi-blesociety.org/topics/ada/olmsteadoverview.htm. Accessed on October 1, 2011.
Bazelon D. 1973. The judicial process—a tool forreform. Presented at the rights of the men-tally handicapped: proceedings from a bi-re-gional conference, San Francisco.
Bittles AH, Petterson BA, Sullivan SG, et al.2002. The influence of intellectual disabilityon life expectancy. J Gerontol Ser A: BiolSci Med Sci 57:M470–M472.
Braddock D. 2010. Honoring eunice Kennedyshriver’s legacy in intellectual disability. Intel-lect Dev Disabil 48:63–72.
Braddock D, Hemp R, Rizzolo MC, et al. 2011.State of the states in developmental disabil-ities 2011. Boulder: Coleman Institute forCognitive Disabilities.
Braddock D, Rizzolo MC, Hemp R, et al. 2005.Public spending for developmental disabil-
ities in the United States: an historical-com-parative perspective. In:Stancliffe R, LakinKC, editors. Costs and outcomes of commu-nity services for people with intellectualdisabilities. Baltimore, MD: Paul H Brookes.p 1–23.
Buck P. 1950. The child who never grew, 2nd ed.Bethesda, MD: Woodbine House.
Caldwell J. 2010. Implications of health carereform for individuals with disabilities. Intel-lect Dev Disabil 48:216–219.
Castles K. 2004. Nice average parents. In:Noll S,Trent JW, editors. Mental retardation inAmerica. New York: New York UniversityPress. p 351–370.
Daly M, Burkhauser R. 2003. The supplementalsecurity income program. In:Moffitt R, edi-tor. Means-tested transfer programs in theUnited States. Chicago: University of Chi-cago Press. p 79–139.
Diament M. 2010. ‘Glee’ actresses with down syn-drome to be honored. Available at http://www.disabilityscoop.com/2010/11/03/glee-actresses-honored/11036/ (accessed October18, 2011).
Emerson E. 2012. Deprivation, ethnicity and theprevalence of intellectual and developmentaldisabilities. J Epidemiol Commun Health 66:218–224.
Felicetti D. 1975. Mental health and retardationpolitics. New York: Praeger.
Frank J. 1952. My son’s story. New York: AlfredA. Knopf.
Gettings R. 2011. Forging a federal-state partner-ship: a history of federal developmental dis-abilities policy. Washington, DC: AmericanAssociation on Intellectual and Developmen-tal Disabilities.
Glasson EJ, Sullivan SG, Hussain R, et al. 2002.The changing survival profile of people withDown’s syndrome: implications for geneticcounselling. Clin Genet 62:390–393.
Glasson EJ, Sullivan SG, Hussain R, et al. 2003.Comparative survival advantage of maleswith Down syndrome. Am J Hum Biol15:192–195.
Hakim D. 2011. A disabled boy’s death, and a sys-tem in disarray, New York Times, p. 1.Available at http://www.nytimes.com/2011/06/06/nyregion/boys-death-highlights-crisis-in-homes-for-disabled.html?pagewanted5all.Accessed on October 1, 2011.
Harrington C, Kang T. 2008. Disparities in serv-ice utilization and expenditures for individu-als with developmental disabilities. DisabilHealth J 1:184–195.
Hopkins J, Rose S. 2011. 10 years, 13 deaths.Chicago: Tribune.
Jones KW. 2004. Education for children with men-tal retardation. In:Noll S, Trent JW, editors.Mental retardation in America. New York:New York University Press. p 322–350.
Lakin KC, Larson S, Salmi P, et al. 2010. Resi-dential services for persons with develop-mental disabilities: status and trends through2009. Available at http://rtc.umn.edu/docs/risp2009.pdf (accessed October 11, 2011).
Larson SA, Lakin KC, Salmi P, et al. 2011. Chil-dren and youth with intellectual or develop-mental disabilities living in congregate caresettings (1977 to 2009): healthy people 2010objective 6.7b outcomes (revised). IntellectDev Disabil 49:209–213.
Matthews AW. 2011. Feud over best setting for thedisabled. Wall Street J. Available at http://online.wsj.com/article/SB10001424052748704307404576079750072401830.html. Ac-cessed on October 1, 2011.
Melnick RS. 1994. Between the lines: interpret-ing welfare rights. Washington, DC: Brook-ings Institution Press.
NRC. 2002. Mental retardation: determining eli-gibility for Social Security Benefits. Wash-ington, DC: National Academy of Sciences.
PHI. 2011. [Who are direct-care workers?]. Para-professional Healthcare Institute, February2011 http://www.directcareclearinghouse.org/download/NCDCW%20Fact%20Sheet-1.pdf.
Pollack H. 2007. learning to walk slow: America’spartial policy success in the arena of intellec-tual disability. J Policy History 19:95–112.
Pollack H. 2011a. The real impact of cuttingmedicaid—just when we need it the most.Available at http://www.kaiserhealthnews.org/Columns/2011/May/050511pollack.aspx(accessed October 18, 2011).
Pollack H. 2011b. The state of the states in develop-mental disabilities: it’s not good, especially inred states. Available at http://www.tnr.com/blog/jonathan-cohn/90557/developmental-disabilities-states-obama (accessed October18, 2011).
Reinhard S, Kassner E, Houser A. 2011. How theaffordable care act can help move states to-ward a high-performing system of long-termservices and supports. Health Aff (Millwood)30:447–453.
Richardson C. 1946. A hundred-thousand defec-tives. Christian Century 63:110–111.
Rogers DE. 1953. Angel unaware. Westwood, NJ:Revell.
Rothman D, Rothman S. 1984. The Willow-brook wars. New York: Harper and Row.
Schott L. 2011. Policy basics: an introduction toTANF. Available at http://www.cbpp.org/cms/?fa5view&id5936 (accessed October18, 2011).
Segel R. 1974. The National association for re-tarded citizens. Available at http://www.thearc.org/history/segal.htm (accessed May29, 2006).
Silverstein G. 2009. Law’s allure: how law shapes,constrains, saves, and kills politics. Cam-bridge, UK: Cambridge University Press.
Skocpol T. 2004. The narrowing of civic life.Available at http://prospect.org/cs/articles?article5the_narrowing_of_civic_life (accessedOctober 18, 2011).
SSA. 2010. Annual statistical report on the social se-curity disability insurance program 2010—alldisabled beneficiaries (table 6). Available athttp://www.ssa.gov/policy/docs/statcomps/di_asr/2010/sect01b.html#table6. Accessedon October 1, 2011.
SSA. 2011.SSI Annual Statistical Report 2010,Vol. 13–11827. Washington, DC: SocialSecurity Administration.
Stancliffe R, Lakin KC. 2005. Context and issuesin research on expenditures and outcomes ofcommunity supports. In:Stancliffe R, LakinKC, editors. Costs and outcomes of commu-nity services for people with intellectualdisabilities. Baltimore, MD: Paul H Brookes.p 1–23.
Strauss D, Eyman R. 1996. Mortality of peoplewith mental retardation in California withand without Down syndrome, 1986–1991.Am J Mental Retard 100:643–653.
Trent JW. 1994. Inventing the feeble mind.Berkeley, CA: University of California Press.
Tucker CD. 1954. Betty Lee. New York: MacMil-lan.
Yang QH, Rasmussen SA, Friedman JM. 2002.Mortality associated with Down’s syndromein the USA from 1983 to 1997: a popula-tion-based study. Lancet 359:1019–1025.
Dev Disabil Res Rev � HEALTH POLICY AND THE COMMUNITY SAFETY NET � POLLACK 51