
Health IT Summit Denver 2014 - "Anatomy of a Health System"
31
Anatomy of a Health System July 23, 2014 Marc Lassaux, CTO, Quality Health Network Justin Aubert, CFO, Quality Health Network Kevin Fitzgerald, MD, CMO, Rocky Mountain Health Plans
-
Upload
health-it-conference-iht2 -
Category
Education
-
view
556 -
download
2
Transcript of Health IT Summit Denver 2014 - "Anatomy of a Health System"

Anatomy of a Health SystemJuly 23, 2014
Marc Lassaux, CTO, Quality Health Network
Justin Aubert, CFO, Quality Health Network
Kevin Fitzgerald, MD, CMO, Rocky Mountain Health Plans

Agenda for this session
Quick Overview
Technology to support Pop. Health
Sustainability consideration
Operationalizing Clinically
General Discussion

Formed in 2004
Two Hospitals, Physician Organization
Payer, Community Resource Organization
Over 200 organizations and 850 providers
HIE, HISP, eHealth Exchange participant
Data Aggregation and Applications
Incorporated as Non-profit 501 (c) 3 - August 2004
“Trusted, non-exclusive, and apolitical Organization”
Live Operations: October 2005Private Capital $2.75 million
Cash Flow Positive from Operations - 2007
The Start:

QHN’s Regional Connectivity - 2013
Including Providers
Copyright Quality Health Network
Connections In Development• The Memorial Hospital, Craig
• Yampa Valley Medical Center, Steamboat Springs
• VA Medical Center, Grand Junction
• CORHIO – Colorado eastern slope
Hospital & Lab Connections • St. Mary’s Regional MC
• Community Hospital
• Family Health West
• Aspen Valley
• Montrose Memorial
• Rangely District
• Delta County Memorial
• Gunnison Valley
• Grand River Health (Hospital)
• Valley View/Glenwood
• Pioneers/Meeker
• LabCorp
• Quest Diagnostics
• Grand Junction Diagnostics
• Internal Medicine Assoc.
• DCI
Hospice
PACE (Senior
Community Care)
Care Transitions
Home Care
DME
Respiratory &
Physical Therapy
Long-Term Care
Assisted Living
Connected
Providers.
.
.
..
...
.
...
.
.............
..............................................................................................................................................
...... .......... ......... .......
..
.
.
.

RMHP and QHN RMHP one of QHN’s five founding members
Colorado Beacon Consortium
• Rocky Lead, QHN Sub recipient
Practice Redesign and Quality Improvement
Population Health Tools
• Disease, Wellness, Risk
Care Coordination


Sustainability Considerations
Justin Aubert CPHIT, CPEHR
CFO, Quality Health Network
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.
7

Historical Funding of QHN
Initial Funding from Private Capital
Core Operations are Funded by Subscription Fees
Everybody Connected Pays
Self Sustaining Since 2007
Development Fund• QHN initially Mesa County initiative
• New neighborhoods contribute to infrastructure
8
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.

Historical Funding of Technology
Grant from The Colorado Health Foundation• Expand HIT through out western Colorado
• Defray one-time costs to connect to the HIE
Colorado Beacon Consortium ONC ARRA Grant• Federal funding to procure technology
• Capital investment vs. operational
Increase Value to Participants• Population Health
• Quality Improvement Initiatives
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.
9

Considerations
New Technology is Expensive and Changing Fast
Open Source vs. Proprietary
Contracting Issues
• Vendor pricing typically ASP
• QHN negotiated contracts for perpetual licenses with
annual maintenance vs. ASP model
- Larger up front costs with lower recurring
- Sustainability plan for post grant funds
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.
10

Considerations
Population Based Pricing
• Western Colorado’s population less than 500K
• First tier pricing typically up to 1M lives
- Non-starter in rural areas
- Not economically feasible unless partnering or revised tiers
Partnering with Other Organizations
• Cheaper to incrementally increase existing license
• Take advantage of economies of scale
• Create similar initiatives across geographic areas
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.
11

Looking Forward
Value Add to Participants of HIE
• Data delivery moving towards a commodity
• Longitudinal patient record is key value
• Use the data to increase value to providers and patients
What Role Does the HIE Play
• EHR’s will/could have functionality
• Workflow, workflow, workflow
©2014 Quality Health Network (QHN) – All rights reserved, QHN proprietary and confidential not for further redistribution.
12

Clinical Aspects When Operationalizing QI and PH- 7/22/14 Anatomy of Health System Panel Presentation
- Institute for Health Technology Transformation (IHT )
Kevin R. Fitzgerald, MD
Chief Medical Officer
Rocky Mountain Health Plans
2

Disclaimers
• Family Doc
• RMHP CMO
• Doctors On Call
14

Anatomy of a Health System- Where We’re Focused
Focus Region
- Approximately 850,000
Residents
- RMHP Key Markets
- RCCO Service Area
- QHN Footprint
- Distinct Patterns of Care
(Dartmouth Atlas)

RMHP Initiatives
• Office Record Review (ORR) since the 90’s
• Chronic Disease Management since the early 2000’s
• Beacon 2009
• CPCi/Practice Transformation 2013 and ongoing
• Medicaid RCCO (ACO) Region 1 2013 and ongoing

Primary Care Practice Transformation
• Top RMHP Priority and Investment Area
• Maximize Primary Care Population Management Capacity− Data Use and QI Competencies
– Adopt New Tools
– Integrate New Staff
– Team Based Care
• Five Active Learning Tracks– Foundations
– Masters 1
– Masters 2
– PCMH Recognition
– CPCi

Barriers To Change
• Non-integrated delivery system
• Frontier communities (IPA’s)
• Evolution of their delivery systems
• Improve communication in their communities
• Create a culture of innovation in the medical community

Accountable, Population-Focused Care- Technology is a Cog in the Machine
Population-Focused Care
Payment
19
Measurement

Boots on the Ground
- Practice Transformation
20
A Rising Tide
• 2012: 51 Practices (Beacon).
• 2013: 102 Practices -- 50% growth or doubling of the number of
practices we supported in 2012.
• 2014: 95 Practices to date -- with 50 practices in queue for
recruiting into any one of the program tracks.

Our Goals
Small tests of change emphasizing the triple aim through
population health management:
• Population management through registries
• Practice case management
• Risk rating and patient stratification
• Referral systems/continuity in transitions
• Community care management of the person
• Community care plans
• Community surveillance models

Whole Person Support
22
• Comprehensive Assessments
• Health, Behavioral, Social, Functional Domains
• Coordinating the Coordinators

RMHP Statewide RCCO Report
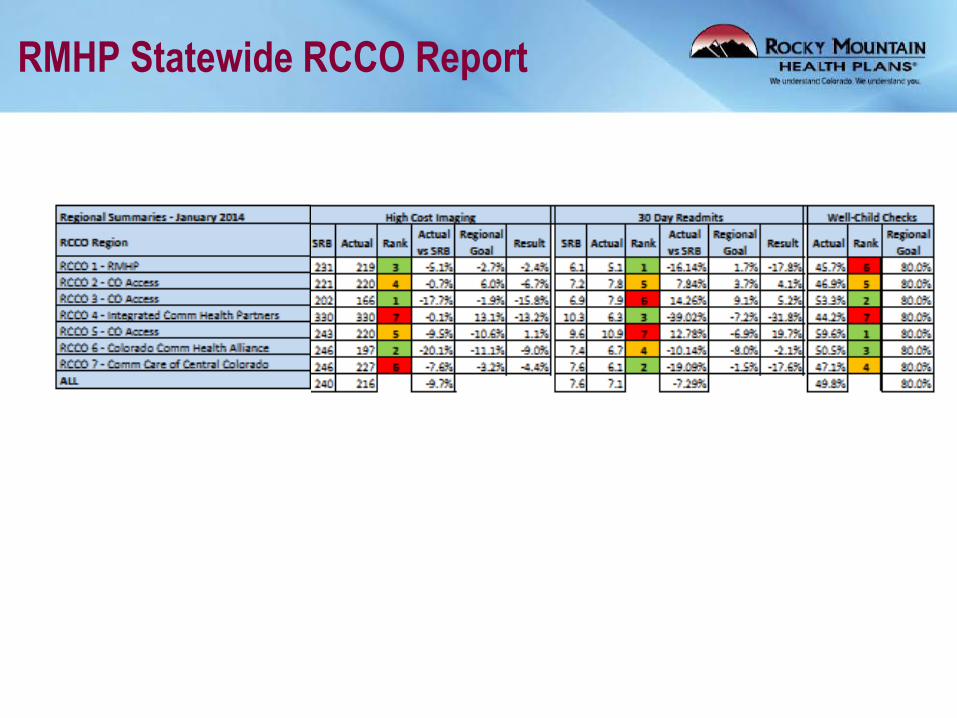
RMHP Statewide RCCO Report
• Practice Transformation
• Measurement & Feedback
• Workforce (Human Capital)
• Payment
• Technology
25
Anatomy of a Health System- Key Drivers in an Accountable Community

Global Outcomes Score
(“GO Score”)
1. Comprehensive and Continuous
2. Guidelines and Predicted Risks
3. Net Benefit Focus - Counterintuitive Results

What is the“GO Score”
Predicted # events prevented by PCP
Opportunity BenchmarkGO Score =
• In example above GO Score = 100/180 = 55
•The opportunity captured is 55% of total
benchmark
0
20
40
60
80
100
120
140
160
180
200
Opportunity Benchmark Current Treatment
5-Year CVD Events Prevented
180 events
100 events

How is the GO Score different?
28
The Global Outcomes Score measures CVD risk reduction in populations
• Credits providers for reducing risk not just meeting a treatment target or process measure
Corrects problems with current simple performance measures such as the blood pressure guidelines:
• Credit is given to reduced SBP from 142 to 138
• No credit is given for reducing SBP from 200 to 142
• Other patient risk factors are largely ignored
• Leaves little room for physician discretion
NCQA is testing the GO Score as a performance measure
• PCP will be one of the first groups in the country to test this new approach

Oversimplified guidelines impact care
29
Mrs.
Smith
Mr. Jones
SBP = 142 SBP = 138age = 45age = 42
LDL = 116 LDL = 178
HDL = 35HDL = 61
FPG = 116FPG = 89
weight = 244 weight = 345
height = 5’6’’ height = 5’11’’
GO Score will give more credit for treating Mr. Jones
1.2%Risk of MI or stroke in 5
years7.1%
0.4%Absolute risk reduction if
lower BP2.1%

What actions increase your GO Score?
Prescriptions (15 month grace period for incentive)
• Statins
• Thiazides
• ACE/ARB
• CCBs
• Beta Blockers
Smoking (cessation during the year)
Weight loss >5% during the year (BMI>25 at
outset)
30
Future versions may include other interventions and
other diseases provided data quality is sufficient

Contact
Kevin Fitzgerald, MD
Chief Medical Officer
Rocky Mountain Health Plans
31


















