Health Information Exchange in Oregon Preparing for the Future Building from the Present Striving...
22
Health Information Exchange in Oregon Preparing for the Future Building from the Present Striving for the Triple Aim
-
Upload
amy-beasley -
Category
Documents
-
view
220 -
download
0
Transcript of Health Information Exchange in Oregon Preparing for the Future Building from the Present Striving...
Health Information Exchange in Oregon
Preparing for the Future
Building from the Present
Striving for the Triple Aim

American Recovery and Reinvestment Act
President Obama signed the American Recovery and Reinvestment ACT in February 2009. The goals relating to Health Information Exchange:
“To improve the quality of our health care while lowering its cost, we will make the immediate investments necessary to ensure that, within five years, all of America’s medical records are computerized.
This will cut waste, eliminate red tape, and reduce the need to repeat expensive medical tests. But it just won’t save billions of dollars and thousands of jobs; it will save lives by reducing the deadly but preventable medical errors that pervade our health care system.”
President Barack Obama

3
Health Information Exchange:More than Technology
To encourage the adoption and use of certified electronic health record (EHR) technology by the States and providers to improve health care outcomes
The EHR technology is not an end in itself but a means to achieve the goals of improving care, ensuring quality, permitting greater access to care, and reducing costs.
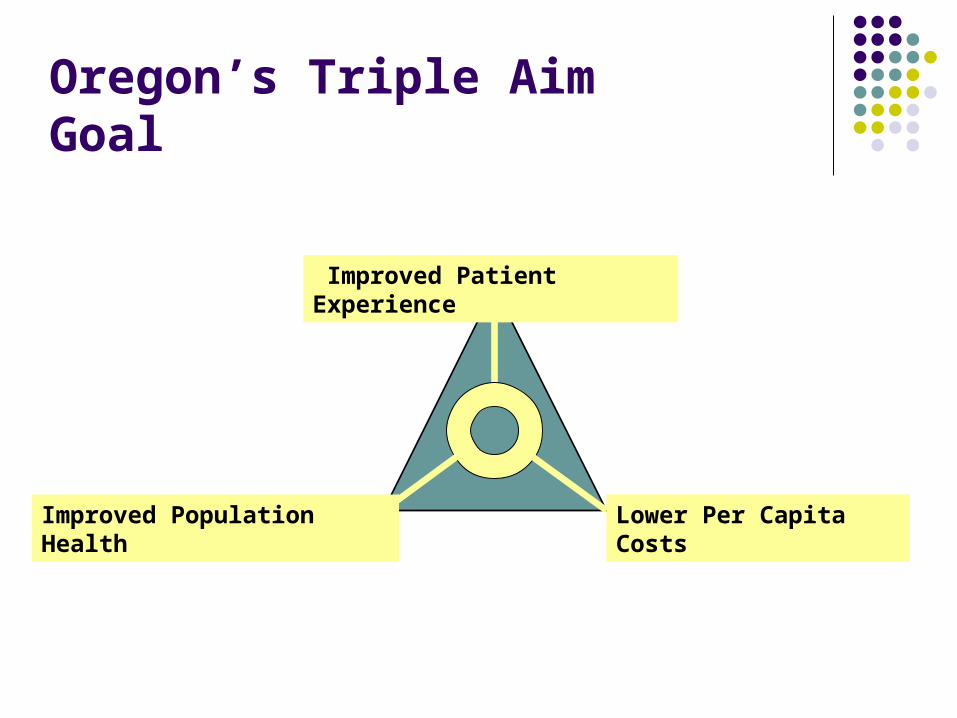
Lower Per Capita CostsImproved Population Health
Oregon’s Triple Aim Goal
Improved Patient Experience

One Small Step . . . Appropriated Funds: $2 billion
Cooperative agreement programs for developing interoperable health information exchange in each state
Grant programs for developing regional extension centers for technical assistance and support to providers
Entitlement Funds: $34 billion Medicare and Medicaid payment
incentives

One Giant Leap . . .
Developing a statewide interoperable system for the exchange of health information will serve as a critical tool for implementing and measuring state and national health care reform.

Appropriated Funds
$2 billion Health Information Exchange Grants
Electronic Health Record Adoption Loan Program (no details currently)
Regional Extension Centers
Workforce Training Grants
New Technology Research and Development Grants
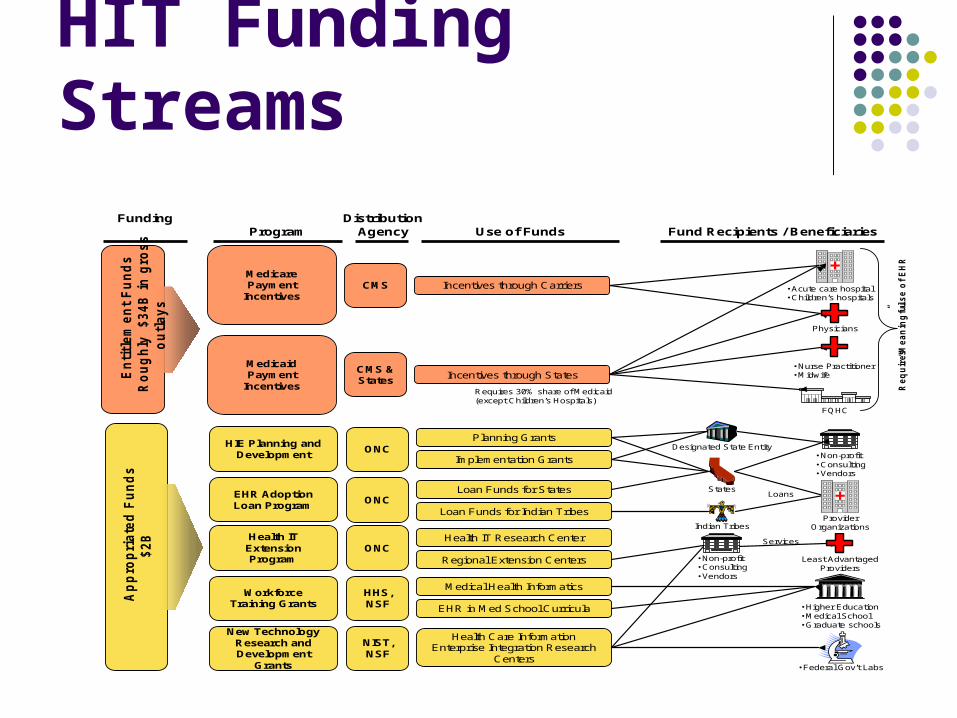
HIT Funding Streams
En
titl
em
en
t F
un
ds
Ro
ug
hly
$34
B i
n g
ros
s
ou
tlay
s
Medicare Payment
Incentives
Medicaid Payment
Incentives
Physicians
• Acute care hospital • Children’s hospitals
Incentives through Carriers
Incentives through States• Nurse Practitioner• Midwife
FQHC
Requires 30% share of Medicaid (except Children’s Hospitals)
Re
qu
ire
s
“Me
an
ing
ful
”u
se
of
EH
R
CMS
CMS & States
ProgramFunding Distribution
Agency Use of Funds Fund Recipients / Beneficiaries
Ap
pro
pri
ate
d F
un
ds
$2B
Workforce Training Grants
New Technology Research and Development
Grants
Medical Health Informatics
EHR in Med School Curricula • Higher Education• Medical School• Graduate schools
Health Care Information Enterprise Integration Research
Centers• Federal Gov’t Labs
HHS, NSF
NIST, NSF
Health IT Extension Program
Health IT Research Center
Regional Extension Centers Least Advantaged Providers
• Non-profit• Consulting• Vendors
ServicesONC
HIE Planning and Development
EHR Adoption Loan Program
Planning Grants
Implementation Grants
Loan Funds for States
Loan Funds for Indian Tribes
Designated State Entity
States
Indian TribesProvider
Organizations
Loans
• Non-profit• Consulting• Vendors
ONC
ONC

Health Information Exchange Cooperative Agreements
What we know: FROM: Office of the National Coordinator for HIT TO: States or Qualified State-Designated Entities FOR: Grants for both planning and implementation WHEN: Application due October 16, 2009
Planning funds beginning January 2010 Strategic and Operational Plan due July
15, 2010 Implementation funds after Plan is
approved HOW MUCH: $8.58 million over 4 years

Regional Extension Centers
What we know: FROM: Office of the National Coordinator for HIT TO: Regional Extension Centers FOR: Supporting the centers as research and
consulting organizations that assist least-advantaged providers.
Funding will be up to 50 percent of capital and annual operating budget for two years
OCHIN has been invited to submit grant application and will be partnering with OHSU
Grant application due November 3, 2009 Award selection announcement December 11,
2009

Workforce Training Grants
What we know: FROM: HHS, National Science Foundation TO: Higher education institutions FOR: Promote HIT workforce development
New Technology Research and Development Grants
What we know: FROM: National Institute of Standards and
Technology, National Science Foundation TO: Higher education, government labs, non-
profits FOR: promoting research and innovation

Entitlement Funds
$34 billionDedicated to Medicare and Medicaid as incentives for
physician
and hospitals who purchase and use Electronic Health Records

Medicaid Incentives
States may make payments to Medicaid providers to encourage adoption and use of certified EHR technology
No duplicative Medicare and Medicaid Payments to medical providers but Childrens and Acute Care Hospitals may receive both
Medicaid providers include: Physicians, dentists, certified nurse midwives, nurse practitioners,
physicians assistants that are practicing in rural health clinics or FQHCs Children and acute hospitals
Requires a percentage of patient volume allocated to either individuals receiving medical assistance, or to needy individuals

Medicare, physicians, EHR
Funds will be available commencing in calendar year 2011
Compensation for “meaningful EHR users” in an equal amount, or up to 75% of allowable charges for professional services furnished by physicians
Incentives are for 5 years, with a declining schedule each year
Phasedown for physicians adopting after CY 2013
Beginning CY 2015, reductions in Medicare reimbursements by 1 to 3% annually will impact physicians that are not “meaningful EHR users”
Incentives are available to physicians of qualified Medicare Advantage organizations
No incentives will be available after CY 2016 when disincentives begin
Certain hospital-based professionals such as pathologists, anesthesiologists, and emergency room physicians are specifically mentioned as being ineligible.

Defining Terms - The Health IT Policy Advisory Committee:Meaningful Use [mee-ning-fuh l yoos] –
“ultimate goal of meaningful use of an Electronic Health Record is to enable significant and measurable improvements in population health through a transformed health care delivery system. The ultimate vision is one in which all patients are fully engaged in their healthcare, providers have real-time access to all medical information and tools to help ensure the quality and safety of the care provided while also affording improved access and elimination of health care disparities.”

Medicare and Medicaid Timeline
2009 2010 2011 2012 2013 2014 2015 2016 2017….. 2021
Medicare Incentives begin Jan 2011 for
non-hospital based physicians
Medicaid: non-hospital basedphysicians no payments after
2021 or more than 5 yrs.
Medicare penalties begin for non-meaningful users
FY15 for hospitalscalendar 2015 for physicians
HHS develop interoperability standards end of 2009
Medicare (FY2011)Incentives begin Oct. 2010
for hospitals
Medicaid: hospitals that adopt after 2017 not eligible for incentives
Medicaid Incentives beginMedicaid: non-hospital
based physicians1st yr cost no later than 2016
Medicare IncentivesEnd 2016
Medicare phase down incentive payments for physicians
Medicare: Physicians who 1st paymentIs after 2014 receive no incentives
Setting of standards complete
Sources: HIMSS http://www.himss.org/ASP/index.asp and AHIMA http://www.ahima.org/

“The Authority establishes a Health Information Technology Oversight Council charged with focusing state, federal and private sector resources and activities to accelerate the adoption of personal health records (PHR), electronic health records (EHR) and electronic data exchange among healthcare providers, patients and consumers.”
HITOC charter and mission18

States will play a critical leadership role by determining a unified path and a model for exchange of health information. States will be expected to use their authority, programs, and resources to:
Determine roles and responsibilities of State Designated Entity (SDE), (if desired) Develop and implement Strategic and Operational Plans Develop state level directories and enable technical services for HIE within and across states. Remove barriers and create enablers for HIE, particularly those related to interoperability across
laboratories, hospitals, clinician offices, health plans and other health information trading partners
Convene health care stakeholders to ensure trust in and support for a statewide approach to HIE Ensure that an effective model for HIE governance and accountability is in place Coordinate an integrated approach with Medicaid and state public health programs to enable
information exchange and support monitoring of provider participation in HIE as required for Medicaid meaningful use incentives.
Develop or update privacy and security requirements for HIE within and across state borders.
Federal Grant Opportunity requirements
19

September 2009-HITOC nominations announced September 2009-States Letter of Intent filed September 2009-OHSU and OCHIN file application for Regional
Extension Center September 2009-State systems environmental scan complete September 2009-Contingent attends National Governors
Association education conference October 2009-HITOC appointees confirmed October 2009 HITOC launch October 2009 ONC Cooperative Agreement application submitted
Progress to date20

HITOC Members
Chair:Steve Gordon, M.D., Eugene, VP, Chief Quality Officer, PeaceHealthVice Chair:Rick Howard, Salem, CIO, Oregon Department of Human Services & Oregon Health Authority
Bob Brown, Portland, Retired, Board member, Oregon Health Action CampaignBrian DeVore, Hillsboro, Director of Industry Affairs, IntelGreg Fraser, Sublimity, Medical Director of Information Systems and Informatics, Mid-Valley IPABridget Haggerty, Portland, VP, CIO, Oregon Health & Sciences UniversityBill Hocket, Portland, Director, Web Strategy, ODS Marie Laper, Corvallis, Coordinator of Quality Improvement & Clinical Care, Benton County Health ServicesRobert Rizk, Hermiston, Director, Information Technology, Good Shepherd Health System Sharon Stanphill, Roseburg, Clinic Director, Cow Creek Band of Umpqua Tribe of IndiansDave Widen, Dayton, Director of Pharmacy, Safeway

“If information is the lifeblood of this effort, then IT infrastructure is the circulatory system.”
“Translating thoughts into a concrete plan and paying for it in a politically charged environment is difficult to do.”
From the NGA e-health Learning Conference September 2009
22