Health Education England London and South East Accreditation in Medicines Management ... · Health...
28
Health Education England London and South East Accreditation in Medicines Management (AIMM) scheme for Pharmacy Technicians Portfolio Paperwork Course leads contact details: Tracey Tisley HEE LaSE 3rd Floor, Red Wing, Crawley Hospital, West Green Drive, Crawley, RH11 7DH Tel: 01293 227144 Email: [email protected]
Transcript of Health Education England London and South East Accreditation in Medicines Management ... · Health...

Health Education England London and South East
Accreditation in Medicines Management (AIMM) scheme for Pharmacy Technicians
Portfolio Paperwork
Course leads contact details:
Tracey Tisley
HEE LaSE
3rd Floor, Red Wing, Crawley Hospital, West Green Drive, Crawley, RH11 7DH
Tel: 01293 227144 Email: [email protected]

Appendix 1
Health Education England - LaSE AIMM scheme 2015
Accreditation in Medicines Management (AIMM) Observed Holistic Practice Based Assessment
Candidate name: Facilitator’s Name: Facilitator’s Signature:
Holistic Assessment where the pharmacy technician has identified patients for the following:
Assessment of Patient’s Own Drugs (PODs) Supply: Accurately supplying medicines to individual patients Medicines Reconciliation
Candidates should consistently demonstrate they have met each assessment criterion. A tick (√) should be used to demonstrate if criteria has been met and a cross (x) if criteria has not been met.
The underpinning skills are used to assess the pharmacy technicians communication and consultation skills.
If a candidate has not demonstrated they have met an underpinning skill this must be assessed by assessment discussion (AD) and recorded on page 4.
Assessment criteria Date of Ob 1
Date of Ob 2
Date of Ob 3
Date of Ob 4
Date of Ob 5
The pharmacy technician must successfully demonstrate they:
Complete the date each observation (Ob) completed in the columns above
1. visit the ward at an appropriate time
2. observe ‘Infection Prevention and Control Measures’ in place on the ward as per local SOPs
3. notify ward staff of their presence and purpose on the ward
4. communicate with ward staff to establish any requirements
5. introduces him/herself to the patient
6. confirm details of the patient (ie Name & DOB)
7. explain purpose of visit/discussion
8. check and document allergy status of patient and nature of reaction
9. obtain patient consent/agreement as per local SOPs where necessary
10. always consider barriers to communication
11. responds to patient/carers questions appropriately and provides accurate information regarding their medications and storage
12. encourage the individual/carer to ask questions, raise concerns and seek information or advice
13. maintains patient confidentiality

Appendix 1
Health Education England - LaSE AIMM scheme 2015
14. deal with any problems and refer any issues outside personal limitations appropriately
Assessment of Patient’s Own Drugs (PODs)
15. accurately check the PODs against the prescription/kardex
16. check the following and make an appropriate decisions regarding the suitability for use of the PODs (as per local SOPs)
label and contents quality details of medication with the
patient/carer (where appropriate)
17. identifies PODs not suitable for use and processes as per local SOPs
18. conduct the POD assessment in a timely manner
19. complete all relevant Trust documentation (patient consent/re-use/destruction – where appropriate)
Supply: Accurately supplying medicines to individual patients
20. check patient/ward details are accurate on charts
21. ensure that all charts where possible are checked for supply requirements
22. confirm that the prescriptions/drug charts are clear and signed by the prescriber to ensure it is valid.
23. ensure that all prescribed medicines are clinically screened prior to supply
24. identify when supplies are available from ward stock and document according to local SOPs
25. complete the appropriate documentation ensuring that all patient and medicine details are completed clearly and accurately according to local SOPs
26. self check documentation to ensure that it clearly and accurately reflects supplies required
27. conduct the order requests in a timely manner
28. monitor existing supplies including quantity, incorrect storage and stock rotation
29. forwards the order for processing as per local SOPs
Medicines Reconciliation
30. uses case notes for background information such as reason for admission, past medical history, social factors and medication history
31. use effective questioning to confirm medication history (where appropriate)

Appendix 1
Health Education England - LaSE AIMM scheme 2015
32. use probing questions to clarify vague or incomplete responses (where appropriate)
33. introduce self to healthcare professional (e.g.
receptionist at GP surgery)
34. record details of all medications being taking (inc.
OTC, complimentary or borrowed medication’
35. identify and refer any compliance or non- compliance issues
36. identify lifestyle issues (e.g. diet, smoking etc) that may relate to medicines being used or medical conditions (where appropriate)
37. accurately identify and document discrepancies between chart/prescription and completed medicines reconciliation using the most recent chart/prescription available
38. accurately conduct medicine reconciliation using a minimum of 2 sources
39. obtain information from a 3rd source or refer appropriately if discrepancies found
40. document the outcome/resolution of any queries as per local SOPs
41. complete the appropriate documentation ensuring all patient and medicine details are completed clearly and accurately according to local SOPs and filed in the correct location
42. communicate any outcomes of the medicines reconciliation
Underpinning Communication and Consultation Skills
The pharmacy technician must have successfully demonstrated they have used the following skills
43. Verbal communication
44. Non-verbal communication
45. Active listening
46. Effective questioning techniques
47. Effective negotiation skills
48. Appropriate use of communication (i.e. avoiding
jargon) and clear explanation where needed
49. Assessment of understanding
50. Ensures any discussion with the patient is kept on track and is closed appropriately
Barriers to communication
The pharmacy technician must demonstrate the ability to identify and resolve barriers to effective communication
51. Describe barriers to effective communication and possible actions to overcome these
52. Cover a range of patient types/needs e.g.: hearing impaired, sight impaired, confused, elderly, etc. Please specify:-

Appendix 1
Health Education England - LaSE AIMM scheme 2015
Accreditation in Medicines Management Observed Holistic Practice Based Assessment
Assessment Discussion
Candidate name: Date:
Facilitator’s Name: Facilitator’s Signature:
If a candidate has not demonstrated they have met an underpinning skill this must be assessed by assessment discussion (AD).
The facilitator should document below what was discussed, any questions asked along with the candidate’s response and any feedback given.

Health Education England – London and South East AIMM scheme
Appendix 3 Accreditation in Medicines Management (AIMM)
Learning Agreement
This agreement outlines the responsibilities required to achieve the Accreditation in Medicines Management (AIMM) for Pharmacy Technicians.
It is the AIMM candidate’s responsibility to:
fulfil work responsibilities as outlined in their job description be familiar with and work consistently within the Trust’s SOPs successfully complete the pre-course workbook attend the AIMM candidate study days complete the work that is set on Day 1 and submit it on Day 2 record ALL his/her evidence using the current LPEandT recording forms provided by
the AIMM facilitator
meet deadlines mutually agreed with the candidate’s AIMM facilitator meet deadlines as detailed on the AIMM time frame guidance must notify the AIMM facilitator each time they make an error discuss any difficulties as soon as they arise, which will be treated as confidential
unless this conflicts with departmental or training requirements
meet with the facilitator following the 2nd study and then on a regular basis todiscuss and document progress
undertake responsibility for self-directed learning in their own time as necessary andproactively seek learning opportunities
respect and be prepared to learn from colleagues at all levels
It is expected of the AIMM candidate that any time lost as a result of annual leave or short sickness should have no impact on the progress or successful completion of the AIMM accreditation.
It is the AIMM facilitator’s responsibility to:
attend the AIMM facilitator study day in order to have a working knowledge of theAIMM scheme and be aware of their responsibilities
inform the Pharmacy Technician Training Manager & Training Specialist of the nameof the candidate they will be facilitating
ensure the correct and current recording paperwork is used facilitate the local implantation of the AIMM scheme ensure that they keep up to date with and implement any revised changes to the
AIMM scheme
confirm the candidate has a clear understanding of all the relevant local SOPs andthat the candidate works consistently within them
provide the candidate with the pre-course workbook assess the candidate’s pre-course workbook once completed

Health Education England – London and South East AIMM scheme
It is the AIMM facilitator’s responsibility to:
forwards the nomination form for the AIMM scheme and the pre-course workbook to HEE London and South East Pharmacy Team
meet with the candidate on a regular basis to provide (verbal and written) support,guidance and feedback
number and sign each of the log forms for quality assurance purposes before givingthem to the candidate
be responsible for nominating suitable colleagues to act as ‘witnesses’ of thecandidates performance during work based activities
contact the Pharmacy Technician Training Manager & Training Specialist forguidance when errors are made by the candidate and the appropriate action to take
nominate the candidate for the AIMM scheme assessment ensuring the nominationform is counter signed by the Chief Pharmacist or designated deputy
maintain confidentiality unless this conflicts with training or departmentalrequirements, informing the candidate if this is the case
AIMM candidate’s name: (Please print)
AIMM candidate’s signature: Date:
AIMM facilitator’s name: (Please print)
AIMM facilitator’s signature: Date:

Health Education England – London and South East AIMM scheme
Appendix C
Printed names and samples of signatures of designated witness as designated by AIMM
facilitator
A copy of the signatories should be kept by the candidate for reference purposes with their portfolio
Print name Signature
Witness List

Appendix D
Health Education England London and South East
AIMM Scheme
Suggested Preparation for Candidate Prior to Meeting with your Facilitator
What are you doing well as a ward based pharmacy technician?
What do you find particularly challenging about being a ward based pharmacytechnician?
Are you comfortable working in the ward environment?
Are there any factors that have had a negative effect on your performance?
Have you received any feedback from dispensary or ward staff about yourperformance?
What are your weaknesses as a ward based pharmacy technician?(How are you going to develop your skills to eliminate this?)
Have you made any referrals? (In this review period)o If yes what were they?o What action was taken?
Have you made any errors? (In this review period)o If yes what were they?o What do you think caused you to make an error?o How would you prevent this from happening again?
Have you found any difficulties whilst in the transition of your role?
Do you feel you are receiving sufficient support?
Are there any other comments that you feel may be relevant?
Here are some suggested points you may wish to consider before meetings with your facilitator. This would also prove useful reflective record for your
CPD Portfolio.

Appendix E
Health Education England London and South East
AIMM Scheme
Suggested Preparation for Facilitators when meeting with Candidates
How is the candidate progressing through the scheme?
What is the candidate doing well in their extended role?
Are there any features of the candidate’s performance that you are concernedabout?
Does the candidate have any areas for improvement where you can offersupport?
Is the candidate’s level of confidence appropriate?
Have you had any feedback from dispensing/ward staff about this candidate?
Would you recommend that the candidate continue with this scheme?
Are there any other comments that you feel may be relevant?
Here are some suggested points you may wish to consider before meetings with the candidate.

Appendix F
Health Education England London and South East
AIMM Scheme
AIMM Accreditation Progress Meeting Paperwork
NAME________________________________________
This documentation can be used as part of your CPD Portfolio
Points discussed
Action plan
Candidate Comments on Performance
Facilitator Comments on Candidate’s Performance
Signed by Candidate Date
Signed by Facilitator Date

H e a l t h E d u c a t i o n E n g l a n d L o n d o n a n d S o u t h E a s t Appendix G
Accreditation in Medicines Management for Pharmacy Technicians
Assessment of Patient’s Own Medicines Log Form
Pharmacy Technician’s Name .................................................................... Trust: ........................................................ 2015
Item No
Date Patient’s Initials
Medicine You must detail
medicine name & strength
Drug Form
Suitable for use
Yes or No &
Suitability Code
Referral Action Taken
Pharmacy Technicians
initials
Checkers initials
Errors Detected by
Checker
Drug Form Codes Suitability
SO Solid Oral, LO Liquid Oral I inhaler TOP Topical SP spray Ij Inject OC Eye Ointment, AD Ear Drops, ND Nose Drops, ED eye drops PR Suppository, PV Pessary, EN Enema
a) Contents cannot be identified b) Label not appropriate/no label c) Container not appropriate d) Medicines have not been stored properly e) Medicines do not match prescription chart f) Medicines that are not on the prescription g) Medicines with limited expiry or expired h) Medicines have been dispensed/labelled incorrectly i) Insufficient quantity j) Medication in compliance device (local policy) k) Discontinued medication l) Borrowed medicines m) Dispensed over 6 months ago
Referral to 1 pharmacist 2 doctor 3 ward staff 4 Other Action Taken D Destroy R Re label N New supply O Other
Facilitator’s Signature
Sheet No. Date

H e a l t h E d u c a t i o n E n g l a n d L o n d o n a n d S o u t h E a s t
Accreditation in Medicines Management for Pharmacy Technicians
Assessment of Patient’s own medicines Log Form
Details of Intervention/Referral – POD Assessment
Item no.
Date Details of Referral (include medicine name and a description of the referral)
Action Taken (Include who you spoke to, what was done and the outcome)

Pharmacy Technician's Name Trust 2015
Item
no
Date
Cost Code
Type of Supply
Ward
Patient Initials
Medicine Name
State Brand where appropriate
Form
Strength
Dose/
Frequency
Quantity
Pharmacy
Technician’s initials
Checker’s
initials
Error
Detected
Type of Supply IP In patient supply OSD One Stop Dispensing TTA Take home medication TS Temp Stock NF Non Formulary or not approved for use
R Repeat supply
N Newly prescribed items
Medicine Form Codes SO Solid Oral, LO Liquid Oral I inhaler TOP Topical SP spray IJ Inject OC Eye Ointment, AD Ear Drops, ND Nose Drops, ED eye drops PR Suppository, PV Pessary, EN Enema
Transcription errors a) Ward / Department b) Patients name c) Medicines generic name d) Medicine brand name if appropriate e) Medicine form f) Medicine strength g) Dose h) Frequency i) Quantity j) Patient allergic to medicine supplied k) Previously supplied l) Not intended for re-supply m) Stock item supplied n) Medicine stopped
# Candidate must follow trust policy on whether the chart must have had a full clinical check prior to transcribing the order Log must show a variety of initial and/or repeat supply issues
Facilitator’s Signature
Sheet No. Date
H e a l t h E d u c a t i o n E n g l a n d L o n d o n a n d S o u t h E a s t Appendix Hi
Accreditation in Medicines Management for Pharmacy Technicians
Transcription Log

Health Education England London and South East Appendix Hi Accreditation in Medicines Management for Pharmacy Technicians
Transcription Log Form - Details of Referral
Item no.
Date Details of Referral (include medicine name and a description of the referral)
Action Taken (Include who you spoke to, what was done and the outcome)

Health Education England London and South East Appendix Ii Medication Consultation - Log Form
Pharmacy Technician __________ Date
Trust Record number
To be completed by the pharmacy technician
Location Pharmacy / Clinic* / Ward* (please delete) * give details i.e. Ward Name, Which Clinic:
Patient type Paediatric / non-English speaker / Sensory impairment*/ Carer / Patient representative / Elderly / Other* (please delete)* give details:
Allergy Status
Drug form (please tick) Solid oral Liquid oral Inhaler device/nebules
Topical Ear, Eye or nasal drops/ointment
Injectables Pessary or suppository/enema
Other give details;
List all medicines on prescription
Reason for counselling
List all main counselling points.

Detail any written information given to the patient e.g. steroid card
Outcome
Include referral details, if applicable
Comments/ Reflection
Include learning points, and areas for improvement
Signature of Pharmacy Technician
To be completed by the witness
Areas covered well
Areas for development
General Comments
Name & title of witness
Signature of witness

Observation checklist for Medication Consultations
To be completed by the witness
Enter YES, NO
or NA Comments
Identifies self
Identifies patient
Explains purpose of the visit
Confirms allergies
Confirms whether patient has had medication before
Confirms if patient takes any other medication, including OTC/herbal
States name of medication
Confirms the indications for the drug(s)
Correctly explains dosage, directions & duration
Correctly explains all main counselling points
Correctly explains warnings/side effects when necessary
Gives appropriate PIL or other written information
Explores manual dexterity/ability to see and read label
Correctly explains how to obtain further supply
Allows patient to ask questions and addresses patients concerns
Confirms patient understands information given
Appropriate referral made (if applicable)
Pharmacy Technician has remained professional and has recognised own limitations
Rounds off session professionally

Pharmacy Technician’s Name: Trust: Patients Initials: Date of Birth:
Management of medicines (Please circle as appropriate)
Self District Nurse Carer Medicine Reminder Device
1. Prescribed Medicines on admission to hospital including any recently prescribed acute medicine or short courses (To be completed by the Pharmacy Technician)
Medicine, Strength and Form Dose & Frequency
Repeat or Acute
Medicines
Date started
Indication Specific Requirements e.g. Clic loc compliance aids
Any problems experienced
Facilitator’s Signature:
Page No: Date:
Health Education England London and South East Medicines Reconciliation
Recording Form
Page 1 of 4
Appendix Ji

Page 2 of 4
2. Over the counter preparations purchased
Medicine, Strength and Form
Dose & Frequency Date started Indications Any problems experienced
3. Complementary medicines (inc. herbal products/homeopathy/Chinese herbs etc)
Medicine & Strength Form, Dose & Frequency
Date started Indications Any problems experienced
4. Details of Allergies & previous ADRs
5. Social history
i) Units of alcohol a week? ____________
ii) Cigarettes smoked a day? ____________
iii) Any drugs of abuse? – DO NOT ASK THE PATIENT DIRECTLY (explore alternative sources of information e.g. case notes, nursing staff etc) ________________________________________________________________________
Health Education England London and South East Medicines Reconciliation
Recording Form

Page 3 of 4
6. Record here any discrepancies between the medication history and the current prescription/medication chart E.g. how you reconciled the medication history, who you spoke to (section 7), what you
documented and where
7. Minimum of 2 sources used to obtain information (please tick which used) Patient_____ Patient’s Carer/Relative______ Repeat prescription request/documentation_________
Medicine containers_______ Nursing notes______ Previous Patients notes_____
Contacting GP_____ Community Pharmacy_____ Nursing/Care Home_____
Other, give details_____________________________________________________
8. Document any problems/issues the patient is experiencing with their medicines or concerns around compliance that needs to be referred E.g. side effects experienced by the patient, adverse drug reactions,
previous prescribed medication stopped or changed recently and reasons for change/discontinuing medication.
Health Education England London and South East Medicines Reconciliation
Recording Form


Health Education England London and South East Page 4 of 4
Medicines Reconciliation Recording Form
To be completed by the witness
Areas covered well
Areas for development
General Comments
Name & Title of witness
Signature of witness
Signature of Pharmacy
Technician
Date

Appendix K Health Education England London and South East
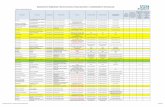
AIMM Facilitators and Course Participants Final Summary Report
The facilitator/ Educational Supervisor should complete sections 1 – 6. Comment on if and to what extent the course participant has improved or developed in these areas during the course. The course participant should complete and sign section 7. Both should sign the form stating that the portfolio meets the specified criteria. 1. Application to work – the course participants’ willingness to take on
these responsibilities, the level of interest shown in extending knowledge and skill
2. Quality of work – the standard of work and whether this is variable or
consistent, awareness of time available/patient’s time commitments
3. Attitude to patients and colleagues – level of tact and
courteousness, communication skills, level of confidence in dealing with patients, ability to deal with constructive criticism, diversity and ethnicity
Answer
Answer
Answer

4. Eliciting patients’ needs – ability to find out and understand a patient’s needs, ability to show empathy
5. Identifying, Solving problems and Referral skills – ability to
identify, solve problems or refer on to an appropriate colleague where necessary, way in which referral process is handled, understanding of own limitations
6. Responsibilities – indicate your level of confidence in the ability of the technician to take on the responsibilities associated with accreditation
Answer
Answer

7. Reflection (to be completed by the course participant) please indicate how the course has or will change your practice and how (if at all) departmental practices have changed during the course. Please continue on a separate sheet if necessary
Candidates Signature
Facilitator Signature
Date
Answer

Appendix O
AIMM Portfolio Progress Report Form
To be faxed or emailed to HEE London and South East as per dates on timeline guidance
Candidates Name
Workplace
Facilitators Name
Documentation Completed Facilitator’s Comments
Pre-course workbook YES/NO
Witness List (appendix C) YES/NO
4 Continuing Professional Development records
(If you complete on line with the GPhC please print
off the relevant records for inclusion in your portfolio)
YES/NO
A Minimum of 4 Progress Reports with facilitator (appendix F)
YES/NO
100 PODs (appendix Gi) YES/NO
If no, how many?
100 Transcriptions (appendix Hi) YES/NO
If no, how many?
15 Patient Consultations observed & documented by
Witness (appendix Ii) – the facilitator must witness a minimum of 5 consultations
YES/NO If no, how many?
15 Medicine Reconciliation observed & documented by
Witness (appendix Ii)
YES/NO
If no, how many?
5 Observed Holistic Practice Based Assessment of Assessment of Patient’s Own Drugs (appendix 1)
YES/NO
5 Observed Holistic Practice Based Assessment of
Supply (appendix 2) YES/NO
5 Observed Holistic Practice Based Assessment of
Medicine Reconciliation (appendix 3) YES/NO
Observed Holistic Practice Based Assessment Discussion (appendix 4) – if applicable
YES/NO
General comments from Facilitator/Educational Supervisor
Signature: Date:
Please email to Tracey Tisley @ [email protected] following progress meetings with your candidates as per dates on timeline guidance.

Appendix Q
AIMM Portfolio Content List
Candidates Name
Workplace
Facilitators Name
Documentation Completed Facilitator’s Comments
LEPT’s Comments
Portfolio Content List YES/NO
Homework YES/NO
Current Job Description YES/NO
Learning Agreement YES/NO
Pre-course workbook or Online
Trust SOP questions and answers
YES/NO
YES/NO
Witness List (appendix C) YES/NO
4 Continuing Professional Development records
(If you complete on line with the GPhC please print off the relevant records for inclusion in your portfolio)
YES/NO
A Minimum of 4 Progress Reports with facilitator
(appendix F) YES/NO
100 PODs (appendix Gi) YES/NO
100 Transcriptions (appendix Hi) YES/NO
15 Patient Consultations observed & documented by
Witness (appendix Ii)
YES/NO
15 Medicine Reconciliation observed & documented by Witness (appendix Ii)
YES/NO
5 Observed Holistic Practice Based Assessment of
Assessment of Patient’s Own Drugs, supply and Medicines Reconciliation (appendix 1)
YES/NO
Observed Holistic Practice Based Assessment Discussion (appendix 4) – if applicable
YES/NO
Facilitator and Participant Final Report Form (appendix K)
YES/NO
OSCE Assessment Nomination Form (appendix L) YES/NO
General comments from Facilitator/Educational Supervisor
Signature: Date:
HEE LaSE
Name: Signature: Date: