Health Behaviour Change Competency Framework · responsible for delivering behaviour change. The...
46
Page | 0 Foundation Competences: examples capacity to adapt interventions to client need ability to foster and maintain a good intervention alliance knowledge of professional and ethical guidelines Behaviour Change Competences: examples capacity to implement models in a flexible manner capacity to select and apply the most appropriate intervention method ability to take a generic assessment Behaviour Change Techniques: number for each route M = 7 BTCs A = 11 BCTs P = 39 BCTs M = 9 BTCs A = 13 BCTs P = 5 BCTs M = 5 BTCs A = 6 BCTs P = 3 BCTs Low Intensity Interventions Medium Intensity Interventions High Intensity Interventions Health Behaviour Change Competency Framework: Competences to deliver interventions to change lifestyle behaviours that affect health 10/11/2010 Diane Dixon and Marie Johnston
Transcript of Health Behaviour Change Competency Framework · responsible for delivering behaviour change. The...

P a g e | 0
Foundation Competences:examples
capacity to adapt
interventions to client need
ability to foster and maintain
a good intervention alliance
knowledge of professional and
ethical guidelines
Behaviour Change
Competences:examples
capacity to implement models
in a flexible manner
capacity to select and apply the
most appropriate intervention
method
ability to take a generic
assessment
Behaviour Change Techniques:number for each route
M = 7 BTCs A = 11 BCTs P = 39 BCTs
M = 9 BTCs A = 13 BCTs P = 5 BCTs
M = 5 BTCs A = 6 BCTs P = 3 BCTs Low Intensity
Interventions
Medium Intensity
Interventions
High Intensity
Interventions
Health Behaviour Change
Competency Framework: Competences to deliver interventions to change
lifestyle behaviours that affect health 10/11/2010
Diane Dixon and Marie Johnston

P a g e | 1
Contents
page
Executive Summary 2
Background 4
Development of the HBCC Framework 5
The Health Behaviour Change Competency Framework (HBCC) 7
Delivering Behaviour Change 9
Low Intensity Interventions 9
Medium Intensity Interventions 10
High Intensity Interventions
11
Mapping the Health Behaviour Change Competency Framework to the
Knowledge and Skills Framework 13
Competences Described in the Training Manual For Alcohol Brief
Interventions 14
Future Directions 15
Acknowledgements 16
Appendix 1 17
The HBCC Hierarchy and KSF Mapping
Appendix 2 39
Competences described in Alcohol Brief Interventions: Training
Manual NHS Health Scotland, 2009
Appendix 3
How the HBCC was developed 44

P a g e | 2
Foundation Competences:examples
capacity to adapt
interventions to client need
ability to foster and maintain
a good intervention alliance
knowledge of professional and
ethical guidelines
Behaviour Change
Competences:examples
capacity to implement models
in a flexible manner
capacity to select and apply the
most appropriate intervention
method
ability to take a generic
assessment
Behaviour Change Techniques:number for each route
M = 7 BTCs A = 11 BCTs P = 39 BCTs
M = 9 BTCs A = 13 BCTs P = 5 BCTs
M = 5 BTCs A = 6 BCTs P = 3 BCTs Low Intensity
Interventions
Medium Intensity
Interventions
High Intensity
Interventions
Executive Summary
This report builds on earlier work described in the document Generic Health Behaviour
Change: a Comprehensive Competency Framework (GHBC-CF). The GHBC-CF described a
comprehensive list of competences required by workers delivering health behaviour change
across different health behaviours and to different clients and client groups. This report
orders those competences into a hierarchical framework: The Health Behaviour Change
Competency Framework (HBCC), designed to support a tiered approach to interventions for
health behaviour change.
The competency framework describes three competency domains:
• Foundation Competences
• Behaviour Change Competences
• Behaviour Change Techniques
Competences within the three domains are organised into three levels characterised by the
intensity of the health behaviour change intervention being delivered:
1. Low intensity interventions
Interventions delivered per protocol (i.e. following an agreed ‘script’) with restricted
flexibility for change by the practitioner. Interventions will primarily be brief and will
include opportunistic delivery. Clients may present with few or mild (but not
moderate or severe) physical co-morbidities (i.e. few of those additional illnesses
which often occur together).
2. Medium intensity
Interventions for which there is a manual but which offer the practitioner some
flexibility in delivery. Interventions might be of longer duration, either in the form of
a longer single session or multiple sessions. Interventions could be delivered
opportunistically or via self-referral or referral from other services. Clients may
present with mild to moderate (but not severe) physical co-morbidities.
3. High intensity
Flexible interventions delivered to match the assessed needs of the client. Typically
interventions will be of longer duration on referral from other services. Clients may
present with moderate or complex physical co-morbidities and may present with
moderate mental health co-morbidities.

P a g e | 3
How has the HBCC been Used? The competences described in the Health Behaviour Change Competency Framework
(HBCC) have been mapped to the competences described in the Knowledge and Skills
Framework (KSF). In addition, competences described in NHS Health Scotland’s training
manual for alcohol brief interventions (2009) have been mapped to the competences
described in the HBCC.

P a g e | 4
Background
The shift from an acute to a chronic model of health puts human health behaviour at the
centre of health policy and health care delivery. Health behaviours such as smoking, alcohol
consumption, diet and physical activity make a significant contribution to the health status
of individuals, communities and populations. Social patterning of these key health
behaviours also contributes to health inequalities. The Scottish Government has expressed
a commitment to improving the health and wellbeing of the population as a whole and to
reducing Scotland’s health inequalities in particular. Government recognises that changing
the health behaviours of a population will require interventions delivered at individual,
household, community and population levels1. These interventions will vary in scope,
design and the behaviour change techniques employed, but all will benefit from the
application of the science of behaviour change. This science employs theoretical models of
behaviour and behaviour change that have been subjected to rigorous testing and extensive
evaluation.
A model of health that recognises the central role of behaviour and behaviour change has
significant implications for the training of health professionals and other workers
responsible for delivering behaviour change. The Health Behaviour Change Competency
Framework (HBCC) described here orders the competences described in the document
Generic Health Behaviour Change: A Comprehensive Competency Framework into a
hierarchy, to be used to develop training programs for health and other professionals. The
competency hierarchy enables a cumulative approach to training in health behaviour
change. A wide range of staff could receive the basic training required to deliver low
intensity interventions, but this basic training can be built upon to enable staff to acquire
the competences required to deliver more intensive interventions to clients with more
complex needs.
The competency hierarchy has been developed to describe the competences required to
deliver interventions of differing intensity. Three levels of intervention intensity are
described: low, medium and high intensity interventions. The competences required to
deliver each level of intervention have been mapped to the Knowledge and Skills
Framework (KSF). This will enable the HBCC-training framework to be integrated into
current competency frameworks used in the NHS.
The HBCC will be of use to:
• Educators: to develop training programmes to skill the workforce to deliver
interventions at different levels of intensity.
• Employers of frontline staff: to describe competences required for advertised posts
and to assess the competences of applicants.
• Frontline workers: to identify their current skill level within the HBCC training
framework.
• Policy workers: to analyse current training provision.
1 National Institute for Health and Clinical Excellence (2007). Public Health Guidance 6: Behaviour change
at population, community and individual levels. Available at: www.nice.org.uk/PH6

P a g e | 5
Development of the HBCC Framework
The competences within the HBCC were identified by examining the published evidence
base. Several sources of information were consulted2.
• Relevant professional competency frameworks
• Systematic reviews of interventions for behaviour change
• Manuals for behaviour change interventions
• NHS and Health Scotland Skills for Health and competency frameworks for alcohol
brief interventions
Competencies identified in the published evidence base were ordered into three
competency domains: foundation, behaviour change and behaviour change techniques.
Then, competencies within each domain were ordered into the three level hierarchy;
competencies relevant to the delivery of low, medium or high intensity interventions. The
ordering of competencies was carried out independently3 by the authors of this report, who
were aided by their collaborative network of research active and practicing health and
clinical psychologists.
Developed to be Consistent with Behaviour Change Models In addition, the HBCC was developed to take account of the latest work on models of
behaviour and behaviour change. Numerous modals of human behaviour are available. The
question therefore arose as to which model was most suitable for a competency framework
for the delivery of health behaviour change. Unfortunately, there is little evidence available
to determine the use of one model in preference to any other. Indeed, the National
Institute for Health and Clinical Excellence, in its review, Behaviour Change at Population,
Community and Individual Levels indicates that the evidence does not support any one
model in particular4. Rather, NICE suggests that training programmes should be based on
competencies and skills, rather than focussed on specific models. The HBCC, therefore,
does not employ any one model of behaviour change; rather, it describes a route MAP to
behaviour change, which includes many of the concepts identified by NICE to be used to
structure and inform interventions.
The route MAP is a useful tool to summarise the central tenets of multiple models of
behaviour change. The MAP describes three routes to behaviour: MOTIVATION
development; ACTION on motivation and PROMPTED or cued routes. Within the HBCC
behaviour change is initiated and maintained through the development of strategies to
increase and maintain motivation and to improve and broaden skills that enable that
motivation to be translated into action. In addition, the HBCC includes a third route, the
prompted or cued route, and this route supports behaviour change without the need for the
constant cognitive effort required by the other routes. The effectiveness of the prompted
2 See Appendix 3 for full details of information sources used in the development of the HBCC
3 Colleagues ordered the competencies independently. This enabled the level of agreement between
colleagues to be calculated. The level of agreement was above 0.7 in both cases (ordering competencies
into domains and ordering into the hierarchy), which is the accepted level for reliability in judgement tasks
such as this. This means the HBCC is not simply a consensus document. 4 Behaviour Change at Population, Community and Individual Levels (2007) National Institute for Health
and Clinical Excellence, Public Health Guidance 6.

P a g e | 6
route is strongly supported by the evidence base. The current fashion for ‘nudging’
behaviour change would largely be accounted for by the prompted route.
Developed to be Useful to a Variety of Audiences The HBCC identifies the competencies required to deliver behaviour change interventions
generically, i.e. across different behaviours and via each of the three routes. In addition, it
also identifies behaviour change techniques that promote change via each of the three
routes. As a consequence, the HBCC was developed to provide a tool for:
• Practitioners to structure their work to ensure their clients receive interventions that
target the route(s) most appropriate for them. The HBCC is also consistent with the
model of behaviour change that currently has greatest currency with practitioners,
namely the Stages of Change model. This consistency will ensure the HBCC has face
validity for practitioners.
• Educators to plan training programmes to skill workers to deliver interventions that
exploit all three routes.
• Managers to specify and describe the competences required for particular roles.
• Policy workers to develop policy that employs all routes to promote behaviour change
and to avoid over reliance on any one particular route.
Developed to be Consistent with an Asset Based Approach to Health The HBCC is consistent with an asset based approach to health. The HBCC describes three
competency domains, each of which are designed to deliver the professional skills required
for a collaborative model of health and health behaviour change. Foundation competences
describe communication skills that enable the practitioner to learn from their clients. This
collaborative approach enables a client to speak about the issues that are of greatest
concern to them and what they want to change (as opposed to what the professional thinks
should be of concern and should be changed). The behaviour change competences and the
behaviour change techniques employ and build on these collaborative communication skills
to develop an understanding of a client’s existing skills and abilities and the environment in
which they live their daily life. They build on these existing skills to enable the client to
develop behaviour change strategies suitable for their needs in their environment. For
example, clients identify those skills they already possess which can be garnered to support
their behaviour change activity and the professional and client work together to explore
ways in which any barriers might realistically be overcome. The HBCC is an asset based
approach to health behaviour change.

P a g e | 7
Foundation
Competencies
Behaviour
Change
Competencies
Behaviour
Change
Techniques
The Health Behaviour Change Competency
Framework (HBCC)
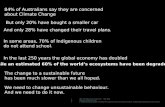
General Structure of the HBCC Framework The HBCC is organised into three competency domains: foundation,
behaviour change and behaviour change techniques (BCTs). The foundation
and behaviour change competency domains are organised into twelve
competency topics. The BCTs are organised into a MAP of behaviour change,
which is composed of three routes to behaviour change: motivation
development, action on motivation and prompted behaviour.
The competences in each domain are organised into a three level hierarchy.
This hierarchy describes the competences relevant to the delivery of low,
medium and high intensity interventions. The hierarchy is cumulative, in that
competency to work at any given level assumes possession of the
competences described at all lower levels.
Foundation competences The foundation competency domain is described by twelve competency topics. At its core
are the communication skills required to develop an effective intervention alliance.
Additional topics cover the professional and ethical guidelines required for effective practice
with different clients and client groups.
Behaviour change competences The behaviour change competency domain is composed of twelve topics. These topics
cover knowledge of the relationship between behaviour and health status. This domain
requires knowledge of models and theories of behaviour and how these have been used to
develop behaviour change interventions. It describes the general assessment and core
intervention skills required to implement theory based interventions for behaviour change
in practice.
Behaviour Change Techniques This domain delivers the full breadth of behaviour change techniques to the HBC
framework. The 89 techniques relevant to health behaviour change identified in the
literature have been organised into three routes to behaviour and behaviour change:
Motivation development (e.g. motivational interviewing, recording the consequences of
behaviour); Action on motivation (e.g. setting behavioural goals, providing feedback on
performance) and Prompted or cued behaviour (e.g. change the environment to facilitate
the target behaviour, provide rewards contingent on target behaviour being performed).
This MAP of behaviour change can be used to ensure that interventions and training
programmes exploit each route to behaviour change.
The organisation of the HBCC, including the hierarchy of competences, is shown in Figure 1
overleaf and used in simplified form on the cover.

Pa
ge
| 8
Fo
un
da
tio
n C
om
pe
ten
cie
s
F8
: c
ap
ac
ity
to
ad
ap
t in
terv
en
tio
ns
to c
lie
nt
ne
ed
F1
1:
ca
pa
cit
y t
o s
tru
ctu
re a
nd
pa
ce
co
nsu
lta
tio
ns
F6
: a
bil
ity
to
wo
rk w
ith
gro
up
s o
f c
lie
nts
F7
: a
bil
ity
to
fo
ste
r a
nd
ma
inta
in a
go
od
inte
rve
nti
on
all
ian
ce
F9
: a
bil
ity
to
ma
na
ge
ex
pe
cta
tio
ns
F1
2:
ca
pa
cit
y t
o d
ea
l wit
h b
arr
iers
to
an
d
fac
ilit
ato
rs o
f in
terv
en
tio
ns
F1
: k
no
wle
dg
e o
f p
rofe
ssio
na
l an
d e
thic
al
gu
ide
lin
es
F2
: a
bil
ity
to
ma
ke
use
of
sup
erv
isio
n
F3
: k
no
wle
dg
e o
f a
nd
ab
ilit
y t
o w
ork
wit
h
dif
fere
nce
F4
: a
bil
ity
to
co
mm
un
ica
te a
nd
wo
rk w
ith
dif
fere
nce
F5
: a
bil
ity
to
en
ga
ge
cli
en
t
F1
0:
ab
ilit
y t
o d
eli
ve
r in
form
ati
on
Be
ha
vio
ur
Ch
an
ge
Co
mp
ete
nci
es
BC
1:
kn
ow
led
ge
of
he
alt
h b
eh
avi
ou
r a
nd
he
alt
h
be
ha
vio
ur
pro
ble
ms
BC
3:
kn
ow
led
ge
of
mo
de
ls o
f b
eh
av
iou
r c
ha
ng
e a
nd
ab
ilit
y t
o u
se t
he
m in
pra
cti
ce
BC
5:
ca
pa
cit
y t
o im
ple
me
nt
mo
de
ls in
a f
lex
ible
ma
nn
er
BC
6:
ca
pa
cit
y t
o s
ele
ct
an
d a
pp
ly m
ost
ap
pro
pri
ate
inte
rve
nti
on
me
tho
d
BC
11
: c
ap
ac
ity
to
ma
na
ge
ob
sta
cle
s to
ca
rry
ing
ou
t
be
ha
vio
ur
ch
an
ge
BC
12
: a
bil
ity
to
en
d in
terv
en
tio
n a
nd
pla
n f
or
lon
g-t
erm
ma
inte
na
nc
e
BC
7:
ca
pa
cit
y t
o im
ple
me
nt
be
ha
vio
ur
ch
an
ge
in a
ma
nn
er
co
nso
na
nt
wit
h it
s u
nd
erl
yin
g p
hil
oso
ph
y
BC
8:
ca
pa
cit
y t
o s
ele
ct
an
d a
pp
ly t
he
mo
st a
pp
rop
ria
te
inte
rve
nti
on
me
tho
d
BC
9:
ab
ilit
y t
o u
se m
ea
sure
s a
nd
se
lf-m
on
ito
rin
g
BC
12
: a
bil
ity
to
en
d in
terv
en
tio
n a
nd
pla
n f
or
lon
g-t
erm
ma
inte
na
nc
e
BC
1:
kn
ow
led
ge
of
he
alt
h b
eh
avi
ou
r a
nd
he
alt
h
be
ha
vio
ur
pro
ble
ms
BC
2:
ab
ilit
y t
o t
ak
e a
ge
ne
ric
ass
ess
me
nt
BC
3:
kn
ow
led
ge
of
mo
de
ls o
f b
eh
av
iou
r c
ha
ng
e a
nd
ab
ilit
y t
o u
se t
he
m in
pra
cti
ce
BC
4:
ab
ilit
y t
o a
gre
e in
terv
en
tio
n g
oa
ls
BC
9:
ab
ilit
y t
o u
se m
ea
sure
s a
nd
se
lf-m
on
ito
rin
g t
o
gu
ide
inte
rve
nti
on
s a
nd
ou
tco
me
s
BC
10
: h
ea
lth
be
ha
vio
ur
pro
ble
m s
olv
ing
ab
ilit
y
BC
12
: a
bil
ity
to
en
d in
terv
en
tio
n a
nd
pla
n f
or
lon
g-
term
ma
inte
na
nc
e
Be
ha
vio
ur
Ch
an
ge
Te
chn
iqu
es
M=
7 B
TC
s
A=
11
BC
Ts
P=
39
BC
Ts
M=
9 B
TC
s
A=
13
BC
Ts
P=
5 B
CT
s
M=
5 B
TC
s
A=
6 B
CT
s
P=
3 B
CT
s
Low Intensity
Interventions
Medium Intensity
Interventions
High Intensity
Interventions
F
igu
re 1
: H
iera
rch
ica
l S
tru
ctu
re o
f th
e H
BC
C F
ram
ew
ork
NB
: T
his
is
a s
um
ma
ry s
tru
ctu
re.
Co
mp
ete
ncy
do
ma
ins
ha
ve
be
en
ass
ign
ed
to
a p
art
icu
lar
lev
el o
f in
terv
en
tio
n b
ase
d o
n a
su
bst
an
tive
pro
po
rtio
n o
f
com
pe
ten
ces
wit
hin
th
at
do
ma
in b
ein
g r
ele
va
nt
to a
sin
gle
in
ten
sity
le
ve
l. In
mo
st c
ase
s co
mp
ete
ncy
do
ma
ins
con
tain
sp
eci
fic
com
pe
ten
ces
rele
va
nt
to
mo
re t
ha
n o
ne
in
ten
sity
le
ve
l.
For
a f
ull
er
de
scri
pti
on
of
the
sp
eci
fic
com
pe
ten
ces
rele
va
nt
to e
ach
le
ve
l of
inte
nsi
ty p
lea
se s
ee
be
low
an
d A
pp
en
dix
1.

P a g e | 9
Delivering Behaviour Change
Competences within the HBCC are organised into a 3 level hierarchy. This hierarchy
describes the competences relevant to the delivery of low, medium and high intensity
interventions. This 3 level hierarchy should be considered a developing rather than
definitive structure for the promotion of health behaviour change.
NHS Scotland recognises that all NHS sectors have a contribution to make to health
improvement. The concept of a health promoting health service, which aims to support the
development of a health promoting culture will require input from the whole workforce. A
change of culture will only be achieved if all staff feel they have a role to play in the
promotion of health. Staff need not necessarily be trained to deliver behaviour change
interventions to make a significant contribution, rather, all staff should have the ability to
identify opportunities to promote health behaviour change, for example through a general
awareness of the role of behaviour in health and an ability to signpost people to suitable
services.
Low Intensity Interventions5
The health promoting health service views every healthcare contact as a health
improvement opportunity. Low intensity interventions represent a skill set that will enable
frontline staff to identify opportunities for brief interventions and to deliver those
interventions as each opportunity for health improvement presents itself.
The term ‘low intensity’ is used to describe interventions that are delivered as described in
an intervention manual, with little or no flexibility to deviate from the described protocol.
Clients receiving low intensity interventions are likely to have few physical co-morbidities
that could be problematic in relation to behaviour change interventions. Low intensity
interventions are exemplified by alcohol brief interventions. The competences required for
delivery of low level interventions can be considered as a core set of competences for
generic health behaviour change. These competences are required by everyone delivering
interventions to change health behaviours.
Competences for Delivery of Low Intensity Interventions
Foundation: Competences from nine of the twelve foundation competency topics are
required for the delivery of low intensity interventions (F1, F2, F3, F4, F5, F7, F9, F10, F12).
In five of the nine topics the majority of individual competences described are required for
delivery of low level interventions.
• F1: knowledge of professional and ethical guidelines.
• F2: ability to make use of supervision.
• F3: knowledge of and ability to work with difference.
• F5: ability to engage client.
• F10: ability to deliver information.
5 Full details of the individual competences within each topic and each domain required for delivery of low level
interventions are provided in Appendix 1

P a g e | 10
Behaviour Change: Competences from nine of the twelve behaviour change
competency topics are required for the delivery of low intensity interventions (BC1, BC2,
BC3, BC4, BC7, BC8, BC9, BC10, BC12). In five of the nine a large proportion of the
individual competences are required for delivery of low level interventions.
• BC1: knowledge of health behaviour and health behaviour problems.
• BC2: ability to undertake a generic assessment.
• BC3: knowledge of a model of behaviour change and the ability to employ the model
in practice.
• BC4: ability to agree goals for the intervention.
• BC10: health behaviour problem solving ability.
Behaviour Change Techniques: Competency to deliver 13 behaviour change
techniques is required for the delivery of low intensity interventions. These 13 BCTs
represent each of the three routes to change as follows.
• 5 BCTs via Motivation development.
• 6 BCTs via Action on motivation.
• 3 BCTs via Prompted or cued route to behaviour.
Medium Intensity Interventions6
Medium intensity interventions will primarily be delivered to clients referred from other
services or clients who self-refer. Practitioners at this level will be skilled to deliver
interventions to clients with more complex needs, for example the presence of multiple
physical co-morbidities and/or mild mental health morbidity. Medium intensity
interventions may involve some flexibility in the delivery of an intervention manual. This
flexibility might typically take the form of the practitioner identifying, from a range of BCTs,
those that are best suited to the assessed needs of an individual client. Medium intensity
interventions will generally be of longer duration, and might involve multiple sessions.
These competences are in addition to those required to deliver low intensity interventions.
Competences for Delivery of Medium Intensity Interventions
Foundation: Competences from ten of the twelve foundation topics are required for
delivery of medium level interventions (F1, F2, F3, F4, F5, F6, F7, F9, F10, F12). Delivery of
medium level interventions requires the majority of individual competences in six
competency topics. In addition to the five topics listed above for low intensity
interventions, the majority of competences in topic G6 are also required for delivery of
medium level interventions.
• F6: ability to work with groups of clients.
Behaviour Change: Competences from nine of the twelve behaviour change
competency topics are required for the delivery of medium intensity interventions (BC1,
BC2, BC3, BC4, BC7, BC8, BC9, BC10, BC12). In all nine a large proportion of the individual
competences are required for delivery of medium level interventions. In addition, to the
five topics listed above for low intensity interventions, a large proportion of the individual
6 Full details of the individual competences within each topic and each domain required for delivery of
medium level interventions are provided in Appendix 1

P a g e | 11
competences within the following topics are required for delivery of medium level
interventions:
• BC7: capacity to implement behaviour change in a manner that is consonant with its
underlying philosophy.
• BC8: ability to structure consultations.
• BC9: ability to use measures and self-monitoring to guide interventions and to
monitor outcome.
• BC12: ability to end the intervention in a planned manner and to plan for long-term
maintenance of gains.
Behaviour Change Techniques: An additional 27 BCTs have been identified as
relevant to the delivery of medium intensity interventions. These additional BCTs operate
primarily through the Motivation development and Action on motivation routes, although
BCTs that operate via the Prompted or cued route are also included.
• 9 BCTs via Motivation development.
• 13 BCTs via Action on motivation.
• 5 BCTs via Prompted or cued route to behaviour.
High Intensity Interventions7
High intensity interventions are typically flexible interventions that can be tailored to
address the assessed needs of the client. Typically interventions will be of longer duration
and will include multiple sessions. High intensity interventions will be delivered on referral
from other services. Clients might present with moderate or complex physical co-
morbidities and may present with moderate mental health co-morbidities.
These competences are in addition to the competences required to deliver low and medium
intensity interventions.
Competences for Delivery of High Intensity Interventions Foundation: The delivery of high intensity interventions requires additional
competences in five of the foundation competency topics, already required for delivery of
low and medium intensity interventions (F2, F3, F4, F5, F7). In addition, two competency
topics are unique to the delivery of high intensity interventions, namely:
• F8: capacity to adapt interventions in response to client feedback.
• F11: capacity to structure consultations and maintain appropriate pacing.
Behaviour Change: Additional competences are required in four behaviour change
competency topics, which also include competences required for delivery of lower
intensity interventions (BC1, BC3, BC7, BC9). In addition, three competency topics are
unique to the delivery of interventions at the high intensity level:
• BC5: capacity to implement behaviour change models in a flexible but coherent
manner.
• BC6: capacity to select and skilfully apply the most appropriate behaviour change
intervention method.
7 Full details of the individual competences within each topic and each domain required for delivery of high level
interventions are provided in Appendix 1

P a g e | 12
• BC11: capacity to manage obstacles to carry out behaviour change.
Behaviour Change Techniques: An additional 57 BCTs have been identified as
relevant to the delivery of high intensity interventions. These additional BCTs operate
primarily through the Prompted or cued route, but BCTs that operate via the Motivation
development and Action on motivation routes are also included.
• 7 BCTs via Motivation development.
• 11 BCTs via Action on motivation.
• 39 BCTs via Prompted or cued route to behaviour.

P a g e | 13
Mapping the HBCC Framework to the Knowledge and
Skills Framework (KSF)8
The KSF consists of five competency dimensions: Core, Health & Wellbeing, Estates &
Facilities, Information & Knowledge and General, each of which is composed of sub-
dimensions. The HBCC competences are described by three KSF dimensions:
• Core
• Health & Wellbeing
• Information & Knowledge
KSF Core Dimension
The Core dimension is composed of 6 sub-dimensions; five are relevant to the HBCC:
• Communication
• Personal & people development
• Service improvement
• Quality
• Equality & diversity
KSF Health and Wellbeing Dimension
Health and Wellbeing is largest KSF dimension being composed of 10 sub-dimensions,
four of which are relevant to the HBCC:
• Protection of health & wellbeing
• Enablement to address health & wellbeing needs
• Assessment & treatment planning
• Interventions & treatments
KSF Information & Knowledge Dimension
Two of the three sub-dimensions within the Information and Knowledge dimension are
relevant to the HBCC:
• Information collection & analysis
• Knowledge & information resources
Each KSF sub-dimension is described at four levels of competency, level 1 to level 4. Higher
levels represent more advanced competency within that sub-dimension. The HBCC
competences were also matched to KSF competency levels within the relevant sub-
dimension. For example, the HBCC foundation competency F1.1 describes the national and
local codes of practice which apply to all staff involved in the delivery of healthcare, this
competency matches to KSF Core Communication dimension at competency level 1. The
HBCC as a whole contains competences up to KSF level 3.
8 The complete mapping of each HBCC competency to the KSF is described in Appendix 1.

P a g e | 14
Competences Described in the Training Manual
for Alcohol Brief Interventions9
The competency hierarchy at the core of the HBCC has been developed, in part, to facilitate
the development and assessment of training programmes to skill the workforce to deliver
interventions of differing levels of intensity and complexity across all health behaviours. In
addition, the HBCC can be used to identify which competences are being delivered in
existing training programmes for health behaviour change. Currently, health behaviour
change training tends to be delivered within topic silos. However, the competences
described in the HBCC are those required for the delivery of generic health behaviour
change, therefore the HBCC can also be used to identify the competences within training
programmes for particular health behaviours.
The HBCC has been used to analyse the content of the training manual for alcohol brief
interventions (ABIs) used by NHS Health Scotland to train the workforce to deliver ABI’s10
.
The ABI training programme is a 10 unit programme designed to be delivered over an 11
hour period, either as a two-day course or via four shorter sessions.
Table 1 below provides a brief summary of the competency domains delivered in each ABI
training unit. A detailed description of the competences delivered in each unit can be found
in Appendix 2.
Table 1: Competences being delivered in each Alcohol Brief Intervention training unit
ABI Training Unit
HBCC Competency Domain Delivered In
Each Training Unit
Foundation Behaviour
Change BCTs
a
(& route MAP)
M A P
1. Brief interventions: what and why �
2. Attitudes to alcohol � �
3. Barriers and concerns � �
4. Brief intervention observation � � � �
5. Units and drinking limits �
6. Raising the issue of alcohol � �
7. Screening and feedback � � � �
8. Referral: when, where and how? � �
9. Brief interventions delivery: key skills � � � � �
10. Brief interventions delivery: putting it all together competences not described in detail aBCTs = Behaviour Change Techniques and the route to change targeted by the techniques delivered in a particular training unit
Table 1 suggests a focus on foundation and behaviour change competences. As the
workforce is likely to be trained in the majority of foundation competences already, it may
be possible to increase training in behaviour change techniques within the current ABI
training timetable.
9 Alcohol Brief Interventions: Training Manual. NHS Health Scotland, 2009
10 The content analysis is described in full in Appendix 2

P a g e | 15
Future Directions
Developing the Evidence Base
Currently we do not have a complete understanding of the effective and necessary
components of behaviour change interventions. That said this evidence base is rapidly
progressing. Two recent meta-analyses11
of interventions to change eating and physical
activity have highlighted the following:
• Less might be more � the use of a larger number of BCTs in interventions is not necessarily related
to better outcomes
• Use of theory based BCTs is associated with more successful outcomes � self-monitoring as a key behaviour change technique
� self-monitoring plus one other behaviour change technique relevant to self-
regulation is additionally effective
To date this work has established the effectiveness of a small number of techniques.
However, that is not to say only a few techniques are effective; at present we lack the
research evidence concerning whether other techniques are or are not effective. Therefore,
there is a need for evidence that can establish the effectiveness or not of a much wider
range of BCTs.
This work focuses on identifying the behaviour change techniques to be included in
interventions. It could usefully be combined with evidence and experience from other
sources that addresses how best complex interventions can be implemented effectively.
Integrating evidence from multiple sources should facilitate the development of
interventions that contain behaviour change techniques of known effectiveness and that are
designed to ensure they can be delivered to clients effectively and efficiently by workers
with the relevant competences.
Using the HBCC In its current form the HBCC is a very comprehensive description of the competences
relevant to the delivery of behaviour change across a wide range of client need. This
introduces a level of complexity into the HBCC that, in its current form, makes it most
suitable for use by policy makers and educators. However, the HBCC could be developed
further.
Development of a Self-Assessment Tool
The HBCC provides a platform for the development of a self-assessment tool for use by
managers and the frontline workforce. Any review of current training provision or
assessment of future training needs would benefit from an understanding of the
knowledge and skills already possessed by the workforce. It is likely that health
professionals already have the majority of the Foundation Competences and may also be
11
Michie, S., C. Abraham, et al. (2009). Effective Techniques in Healthy Eating and Physical Activity Interventions: A
Meta-Regression. Health Psychology 28(6): 690-701. Dombrowski, S., F. F. Sniehotta, et al. (in press). Identifying
active ingredients in complex behavioural interventions for obese adults with obesity-related comorbidities or
additional risk factors for co-morbidities: A systematic review. Health Psychology Review.

P a g e | 16
using other the competences described by the HBCC. The HBCC may be used to develop
a simple online self-assessment tool to enable individual workers and managers to
identify:
• the competences currently employed in practice and the level of those competences
• the competences addressed in training already delivered
• additional competences that require training
• new or additional training to increase the level of competence
Development of Competency Based Training Programmes
Competency based training programmes would improve training efficiency because staff
could identify the competences they already possess and seek additional training only in
those competences they currently lack. The Foundation Competences and Behaviour
Change Techniques Competences are largely generic, i.e. they apply equally across
different health behaviours. However, staff could only move between health behaviours
if they also had the competences that are specific to those particular health behaviours.
For example, competency to identify and use appropriate measures of behaviour is
behaviour specific; the measures used to assess alcohol consumption are specific to
alcohol and different from those used to measure smoking. These behaviour specific
competences are primarily described by competences within the Behaviour Change
Competency domain. For example, staff trained in the generic competences (foundation,
behaviour change and behaviour change techniques) at low intensity and low intensity
alcohol specific behaviour change competences could transfer to also deliver low
intensity smoking interventions if they acquired training in low intensity smoking specific
behaviour change competences. A competency focussed approach to training, therefore,
enables training to be delivered very efficiently. It also simplifies the landscape, which
should make learning and delivering health behaviour change easier.
Acknowledgements
We would like to thank Professor Ronan O’Carroll (University of Stirling), Dr Vivien Swanson
(University of Stirling), Dr Susan Rasmussen (University of Strathclyde), Dr Zoe Chouliara
(Queen Margaret University) and Professor Pauline Adair (University of Salford) for their
input into the development of the HBCC. We would also especially like to thank Tim Warren
(Scottish Government) for his help, patience and continual support throughout the
development of the HBCC and the GHBC-CF. Finally, we would like to thank colleagues in
NHS-Education Scotland, especially Jane Cantrell; NHS-Health Scotland, in particular Wilma
Reid and Bethan Mitchell; all in the Health Improvement Strategy Division, we are
particularly indebted to Fergus Millan (Healthy Living and Screening Policy Team), Amanda
Adams (Alcohol Policy Team) and Lora Powrie (Drugs Policy Unit); Dr Nicky Thomas
(Consultant Health Psychologist, Guy’s Hospital, London), Oliver Harding (Public Health
Consultant, NHS Forth Valley), Ann Dunbar (PHRU) and Grace Moore (NHS, Ayrshire and
Arran) who provided insightful and helpful input to and feedback on the GHBC-CF and the
first draft of the HBCC.

Pa
ge
| 1
7
Ap
pe
nd
ix 1
H
iera
rch
y o
f h
ea
lth
be
ha
vio
ur
cha
ng
e c
om
pe
ten
ces
an
d K
SF
ma
pp
ing
12
Th
e t
ab
les
be
low
de
scri
be
th
e in
div
idu
al co
mp
ete
nce
s w
ith
in e
ach
co
mp
ete
ncy
to
pic
, w
ith
in e
ach
co
mp
ete
ncy
do
ma
in (
fou
nd
ati
on
, b
eh
avio
ur
cha
ng
e a
nd
be
ha
vio
ur
cha
ng
e t
ech
niq
ue
s).
Ea
ch c
om
pe
ten
cy i
s co
lou
r co
de
d f
or
its
pla
ce i
n t
he
hie
rarc
hy.
Th
e c
olo
ur
ind
ica
tes
the
le
ve
l o
f
inte
rve
nti
on
in
ten
sity
ap
pro
pri
ate
fo
r th
at
com
pe
ten
cy.
Co
mp
ete
nce
s re
lev
an
t to
:
•
Low
in
ten
sity
in
terv
en
tio
ns
ha
ve n
o c
olo
ur
•
Me
diu
m i
nte
nsi
ty i
nte
rve
nti
on
s a
re c
olo
ure
d p
ale
gre
y
•
Hig
h i
nte
nsi
ty i
nte
rve
nti
on
s a
re c
olo
ure
d d
ark
gre
y
KS
F M
ap
pin
g
Th
e K
SF d
ime
nsi
on
, su
b-d
ime
nsi
on
an
d l
eve
l o
f co
mp
ete
ncy
are
lis
ted
fo
r e
ach
HB
CC
co
mp
ete
ncy
. T
he
KS
F m
ap
pin
g i
s d
esc
rib
ed
in
th
e
foll
ow
ing
se
qu
en
ce:
dim
en
sio
n c
od
e;
sub
-dim
en
sio
n n
um
be
r; le
ve
l o
f co
mp
ete
ncy
Fo
r e
xam
ple
HW
B4
L3 d
en
ote
s K
SF
He
alt
h a
nd
We
llb
ein
g D
ime
nsi
on
(H
WB
), s
ub
-dim
en
sio
n 4
(e
na
ble
me
nt
to a
dd
ress
he
alt
h a
nd
we
llb
ein
g
ne
ed
s),
leve
l o
f co
mp
ete
nce
3.
Th
e K
SF d
ime
nsi
on
s a
re c
od
ed
in
th
e t
ab
les
as
follo
ws:
•
C =
Co
re d
ime
nsi
on
;
•
HW
B =
He
alt
h a
nd
We
llb
ein
g d
ime
nsi
on
;
•
IK =
In
form
ati
on
an
d K
no
wle
dg
e d
ime
nsi
on
.
12In
tra
cla
ss c
orr
ela
tio
n c
oe
ffic
ien
t w
as
use
d a
s a
me
asu
re o
f re
lia
bil
ity
(a
gre
em
en
t b
etw
ee
n j
ud
ge
s p
erf
orm
ing
th
e l
eve
l o
f in
ten
sity
ma
pp
ing
ta
sk).
IC
C=
0.7
1,
ICC
valu
es
of
0.7
or
ab
ov
e i
nd
ica
te a
n a
cce
pta
ble
le
vel
of
ag
ree
me
nt

Pa
ge
| 1
8
Fo
un
da
tio
n C
om
pe
ten
cy D
om
ain
F1
. P
rofe
ssio
na
l a
nd
eth
ica
l g
uid
eli
ne
s
KS
F
1.
Kn
ow
led
ge
of
na
tio
na
l a
nd
lo
cal
cod
es
of
pra
ctic
e w
hic
h a
pp
ly t
o a
ll s
taff
in
volv
ed
in
th
e d
eli
ve
ry o
f h
ea
lth
care
, a
s w
ell
as
an
y c
od
es
of
pra
ctic
e w
hic
h a
pp
ly
to t
he
he
alt
h p
rofe
ssio
na
l a
s a
me
mb
er
of
a s
pe
cifi
c p
rofe
ssio
n
C5
L1
2.
Kn
ow
led
ge
of
leg
isla
tio
n r
ele
va
nt
to a
rea
s o
f p
rofe
ssio
na
l p
ract
ice
in
wh
ich
th
e h
ea
lth
pro
fess
ion
al
is e
ng
ag
ed
(sp
eci
fica
lly
in
clu
din
g t
he
Hu
ma
n R
igh
ts A
ct,
Da
ta P
rote
ctio
n A
ct)
C5
L1
3.
Kn
ow
led
ge
of
rele
van
t co
de
s o
f p
rofe
ssio
na
l a
nd
eth
ica
l co
nd
uct
an
d p
ract
ice
in
ord
er
to a
pp
ly t
he
ge
ne
ral
pri
nci
ple
s e
mb
od
ied
in
th
ese
co
de
s to
ea
ch
pie
ce o
f w
ork
be
ing
un
de
rta
ke
n,
in t
he
are
as
of:
C
5L1
3.1
. o
bta
inin
g i
nfo
rme
d c
on
sen
t fo
r in
terv
en
tio
ns
fro
m c
lie
nts
C
1L3
C5
L1
3.2
. m
ain
tain
ing
co
nfi
de
nti
ali
ty,
an
d k
no
win
g t
he
co
nd
itio
ns
un
de
r w
hic
h c
on
fid
en
tia
lity
ca
n b
e b
rea
che
d
C1
L1
C5
L1
3.3
. k
ee
pin
g a
ccu
rate
re
cord
s
C1
L1
C5
L1
IK2
L1
3.4
. sa
feg
ua
rdin
g t
he
cli
en
t’s
inte
rest
s w
he
n c
o-w
ork
ing
wit
h o
the
r p
rofe
ssio
na
ls a
s p
art
of
a t
ea
m,
incl
ud
ing
go
od
pra
ctic
e r
eg
ard
ing
in
terw
ork
er/
inte
r-
pro
fess
ion
al
com
mu
nic
ati
on
C1
L3
C5
L1
3.5
. co
mp
ete
nce
to
pra
ctic
e,
an
d m
ain
tain
ing
co
mp
ete
nt
pra
ctic
e t
hro
ug
h a
pp
rop
ria
te t
rain
ing
/pro
fess
ion
al
de
velo
pm
en
t C
2L3
C5
L1
3.6
. re
cog
nit
ion
of
the
lim
its
of
com
pe
ten
ce a
nd
ta
kin
g a
ctio
n t
o e
nh
an
ce p
ract
ice
th
rou
gh
ap
pro
pri
ate
tra
inin
g/p
rofe
ssio
na
l d
eve
lop
me
nt
C2
L1
C5
L1
3.7
. p
rote
ctin
g c
lie
nts
fro
m a
ctu
al
or
po
ten
tia
l h
arm
fro
m p
rofe
ssio
na
l m
alp
ract
ice
by
co
lle
ag
ue
s b
y i
nst
itu
tin
g a
ctio
n i
n a
cco
rda
nce
wit
h n
ati
on
al
an
d
pro
fess
ion
al
gu
ida
nce
C5
L3
HW
B3
L1
4.
Ma
inta
inin
g a
pp
rop
ria
te s
tan
da
rds
of
pe
rso
na
l co
nd
uct
fo
r se
lf:
C5
L1
4.1
. a
ca
pa
city
to
re
cog
nis
e a
ny
po
ten
tia
l p
rob
lem
s in
re
lati
on
to
po
we
r a
nd
“d
ua
l re
lati
on
ship
s” w
ith
cli
en
ts,
an
d t
o d
esi
st a
bso
lute
ly f
rom
an
y a
bu
ses
in
the
se a
rea
s C
5L1
4.2
. re
cog
nis
ing
wh
en
pe
rso
na
l im
pa
irm
en
t co
uld
in
flu
en
ce f
itn
ess
to
pra
ctic
e,
an
d t
ak
ing
ap
pro
pri
ate
act
ion
(e
.g.
see
kin
g p
ers
on
al
an
d p
rofe
ssio
na
l
sup
po
rt a
nd
/or
de
sist
ing
fro
m p
ract
ice
) C
5L1
5.
Kn
ow
led
ge
of
an
d a
pp
rop
ria
te r
efe
rra
l to
oth
er
ag
en
cie
s w
he
n r
eq
uir
ed
C
5L1
6.
Ide
nti
fyin
g p
rob
lem
s o
r o
pp
ort
un
itie
s fo
r im
pro
vin
g a
ny
asp
ect
of
serv
ice
(in
clu
din
g f
rom
cli
en
t fe
ed
ba
ck)
C4
L1
7.
Re
po
rtin
g a
pp
rop
ria
tely
pro
ble
ms
or
op
po
rtu
nit
ies
for
imp
rovi
ng
an
y a
spe
ct o
f se
rvic
e
C4
L1

Pa
ge
| 1
9
F2
. S
up
erv
isio
n
K
SF
1.
Kn
ow
led
ge
th
at
the
pri
ma
ry p
urp
ose
of
sup
erv
isio
n a
nd
le
arn
ing
is
to e
nh
an
ce t
he
qu
ali
ty o
f th
e i
nte
rve
nti
on
cli
en
ts r
ece
ive
C
2L1
2.
An
ab
ilit
y t
o w
ork
co
lla
bo
rati
vely
wit
h t
he
su
pe
rvis
or
C1
L2
C2
L2
2.1
. A
n a
bil
ity
to
wo
rk w
ith
th
e s
up
erv
iso
r in
ord
er
to g
en
era
te a
n e
xpli
cit
ag
ree
me
nt
ab
ou
t th
e p
ara
me
ters
of
sup
erv
isio
n (
e.g
. se
ttin
g a
n a
ge
nd
a,
be
ing
cle
ar
ab
ou
t th
e r
esp
ect
ive
ro
les
of
sup
erv
iso
r a
nd
su
pe
rvis
ee
, th
e g
oa
ls o
f su
pe
rvis
ion
an
d a
ny
co
ntr
act
s w
hic
h s
pe
cify
th
ese
fa
cto
rs)
C1
L2
C2
L2
2.2
. A
n a
bil
ity
to
he
lp t
he
su
pe
rvis
or
be
aw
are
of
yo
ur
curr
en
t st
ate
of
com
pe
ten
ce a
nd
yo
ur
tra
inin
g n
ee
ds
C1
L2
C2
L2
2.3
. A
n a
bil
ity
to
pre
sen
t a
n h
on
est
an
d o
pe
n a
cco
un
t o
f cl
ien
t w
ork
un
de
rta
ke
n
C1
L2
C2
L2
2.4
. A
n a
bil
ity
to
dis
cuss
cli
en
t w
ork
wit
h t
he
su
pe
rvis
or
as
an
act
ive
an
d e
ng
ag
ed
pa
rtic
ipa
nt,
wit
ho
ut
be
com
ing
pa
ssiv
e o
r a
void
an
t, o
r d
efe
nsi
ve o
r
ag
gre
ssiv
e
C1
L2
C2
L2
3.
A c
ap
aci
ty f
or
act
ive
le
arn
ing
C
2L2
3.1
. A
n a
bil
ity
to
act
on
su
gg
est
ion
s re
ga
rdin
g r
ele
van
t re
ad
ing
ma
de
by
th
e s
up
erv
iso
r, a
nd
to
in
corp
ora
te t
his
ma
teri
al
into
wo
rk w
ith
cli
en
ts
C2
L2
3.2
. A
n a
bil
ity
to
ta
ke
th
e i
nit
iati
ve i
n r
ela
tio
n t
o l
ea
rnin
g,
by
id
en
tify
ing
re
leva
nt
pa
pe
rs,
bo
ok
s, o
r w
eb
-ba
sed
re
sou
rce
s b
ase
d o
n (
bu
t in
de
pe
nd
en
t o
f)
sup
erv
iso
r su
gg
est
ion
s, a
nd
to
in
corp
ora
te t
his
ma
teri
al
into
wo
rk w
ith
cli
en
ts
C2
L2
IK3
L1
4.
An
ab
ilit
y t
o r
efl
ect
on
th
e q
ua
lity
of
sup
erv
isio
n a
s a
wh
ole
, a
nd
(in
acc
ord
an
ce w
ith
na
tio
na
l a
nd
pro
fess
ion
al
gu
ide
lin
es)
to
se
ek
ad
vic
e f
rom
oth
ers
wh
ere
:
C1
L3
C2
L3
4.1
. th
ere
is
con
cern
th
at
sup
erv
isio
n i
s b
elo
w a
n a
cce
pta
ble
sta
nd
ard
C
1L3
C2
L3
4.2
. w
he
re t
he
su
pe
rvis
or’
s re
com
me
nd
ati
on
s d
evi
ate
fro
m a
cce
pta
ble
pra
ctic
e
C1
L3
C2
L3
4.3
. w
he
re t
he
su
pe
rvis
or’
s a
ctio
ns
bre
ach
na
tio
na
l a
nd
pro
fess
ion
al
gu
ida
nce
(e
.g.
ab
use
s o
f p
ow
er
an
d/o
r a
tte
mp
ts t
o c
rea
te d
ua
l (s
exu
al)
re
lati
on
ship
s)
C1
L3
C2
L3
F3
. K
no
wle
dg
e o
f a
nd
ab
ilit
y t
o w
ork
wit
h d
iffe
ren
ce
K
SF
1.
Kn
ow
led
ge
of
the
po
ten
tia
l si
gn
ific
an
ce f
or
pra
ctic
e o
f so
cia
l a
nd
cu
ltu
ral
dif
fere
nce
, a
cro
ss a
ra
ng
e o
f d
om
ain
s, i
ncl
ud
ing
: C
1L2
C6
L2
1.1
. eth
nic
ity
C
1L2
C6
L2
1.2
. cu
ltu
re
C1
L2
C6
L2
1.3
. ed
uca
tio
n
C1
L2
C6
L2

Pa
ge
| 2
0
1.4
. de
pri
vati
on
le
vel/
SE
S
C1
L2
C6
L2
1.5
. re
lig
ion
C
1L2
C6
L2
1.6
. ge
nd
er
C1
L2
C6
L2
1.7
. ag
e
C1
L2
C6
L2
1.8
. dis
ab
ilit
y
C1
L2
C6
L2
1.9
. se
xua
l o
rie
nta
tio
n
C1
L2
C6
L2
2.
Kn
ow
led
ge
of
the
re
leva
nce
an
d p
ote
nti
al
imp
act
of
soci
al
an
d c
ult
ura
l d
iffe
ren
ce o
n t
he
eff
ect
ive
ne
ss a
nd
acc
ep
tab
ilit
y o
f a
n i
nte
rve
nti
on
fo
r a
ll c
lie
nts
C6
L2
C6
L3
HW
B7
L2
3.
Ab
ilit
y t
o m
ak
e a
pp
rop
ria
te a
dju
stm
en
ts t
o t
he
in
terv
en
tio
n,
wit
h t
he
aim
of
ma
xim
isin
g i
ts p
ote
nti
al
be
ne
fit
to t
he
cli
en
t w
he
re s
oci
al
an
d c
ult
ura
l
dif
fere
nce
im
pa
cts
on
th
e a
cce
ssib
ilit
y o
f in
terv
en
tio
n
HW
B7
L3
F4
. A
bil
ity
to
co
mm
un
ica
te a
nd
wo
rk w
ith
dif
fere
nt
ind
ivid
ua
ls,
gro
up
s a
nd
co
mm
un
itie
s
K
SF
1.
Ab
ilit
y t
o w
ork
an
d c
om
mu
nic
ate
eff
ect
ive
ly w
ith
: C
1L2
1.1
. in
div
idu
als
C
1L2
1.2
. g
rou
ps
C1
L2
1.3
. si
gn
ific
an
t o
the
rs (
incl
ud
ing
: sp
ou
ses,
pa
rtn
ers
, re
lati
ve
, fa
mil
ies,
oth
er
soci
al
gro
up
s)
C1
L2
1.4
. p
eo
ple
in
ow
n a
nd
oth
er
ag
en
cie
s C
1L2
F5
. A
bil
ity
to
en
ga
ge
cli
en
t
K
SF
1.
Ab
ilit
y t
o i
nit
iate
a d
iscu
ssio
n a
bo
ut
po
ten
tia
l h
ea
lth
be
ha
vio
ur
pro
ble
ms
C1
L3
1.1
. a
bil
ity
to
cre
ate
an
en
viro
nm
en
t su
ita
ble
fo
r fr
an
k,
con
fid
en
tia
l d
iscu
ssio
n
C1
L2
1.2
. a
bil
ity
to
exp
lain
wh
y t
he
cli
en
t’s
he
alt
h b
eh
avi
ou
r is
of
inte
rest
C
1L3
1.3
. a
bil
ity
to
in
itia
te d
iscu
ssio
ns
ab
ou
t ri
sky
he
alt
h b
eh
avi
ou
r a
nd
re
spo
nd
to
cli
en
ts w
ho
exp
ress
co
nce
rns
ab
ou
t th
eir
he
alt
h b
eh
avi
ou
r C
1L3
2.
Wh
ile
ma
inta
inin
g p
rofe
ssio
na
l b
ou
nd
ari
es,
an
ab
ilit
y t
o s
ho
w a
pp
rop
ria
te l
ev
els
of
wa
rmth
, co
nce
rn,
con
fid
en
ce a
nd
ge
nu
ine
ne
ss,
ma
tch
ed
to
cli
en
t n
ee
d
C1
L3
3.
An
ab
ilit
y t
o e
ng
en
de
r tr
ust
C
1L2
4.
An
ab
ilit
y t
o d
eve
lop
ra
pp
ort
C
1L2
5.
An
ab
ilit
y t
o a
da
pt
pe
rso
na
l st
yle
so
th
at
it m
esh
es
wit
h t
ha
t o
f th
e c
lie
nt
C1
L3
6.
An
ab
ilit
y t
o a
dju
st t
he
le
vel
an
d s
tru
ctu
re o
f th
e s
ess
ion
to
th
e c
lie
nt’
s n
ee
ds
C1
L3

Pa
ge
| 2
1
7.
An
ab
ilit
y t
o c
on
vey
an
ap
pro
pri
ate
le
ve
l o
f co
nfi
de
nce
an
d c
om
pe
ten
ce
C1
L2
8.
An
ab
ilit
y t
o a
void
ne
ga
tive
in
terp
ers
on
al
be
ha
vio
urs
(su
ch a
s im
pa
tie
nce
, a
loo
fne
ss,
or
insi
nce
rity
) C
1L2
F6
. A
bil
ity
to
wo
rk w
ith
gro
up
s o
f cl
ien
ts
K
SF
1.
Kn
ow
led
ge
of
an
d a
bil
ity
to
dra
w o
n t
his
kn
ow
led
ge
in
pra
ctic
e o
f p
rofe
ssio
na
l a
nd
eth
ica
l fa
cto
rs i
n r
ela
tio
n t
o w
ork
ing
wit
h g
rou
ps
C1
L3
2.
Ab
ilit
y t
o a
pp
ly p
rofe
ssio
na
l a
nd
eth
ica
l st
an
da
rds
wh
en
wo
rkin
g w
ith
gro
up
s C
1L3
3.
Ab
ilit
y t
o e
nsu
re t
he
gro
up
ad
op
ts a
pp
rop
ria
te e
thic
al
sta
nd
ard
s, e
.g.
con
fid
en
tia
lity
an
d r
esp
ect
C
1L3
4.
Ab
ilit
y t
o e
ng
ag
e t
he
gro
up
(se
e a
bil
ity
to
en
ga
ge
cli
en
t a
bo
ve)
C1
L3
5.
Ab
ilit
y t
o r
ep
ort
on
mis
sin
g m
em
be
rs
C1
L3
6.
Ab
ilit
y t
o e
nco
ura
ge
gro
up
dis
cuss
ion
s/d
ida
ctic
pre
sen
tati
on
s C
1L3
7.
Ab
ilit
y t
o c
om
mu
nic
ate
ru
les
go
vern
ing
th
e g
rou
p
C1
L3
8.
Ab
ilit
y t
o e
mp
ha
sis
tha
t e
ach
in
div
idu
al
ha
s a
re
spo
nsi
bil
ity
to
th
e g
rou
p
C1
L3
9.
Ab
ilit
y t
o e
sta
bli
sh a
clo
sed
gro
up
C
1L3
10
. A
bil
ity
to
co
mm
un
ica
te g
rou
p m
em
be
r id
en
titi
es
C1
L3
11
. A
bil
ity
to
co
mm
un
ica
te a
nd
ma
inta
in r
ule
s o
f g
rou
p b
eh
av
iou
r C
1L3
F7
. A
bil
ity
to
fo
ste
r a
nd
ma
inta
in a
go
od
in
terv
en
tio
n a
llia
nce
, a
nd
to
gra
sp t
he
cli
en
t’s
pe
rsp
ect
ive
*
Kn
ow
led
ge
of
the
co
nce
pt
of
the
in
terv
en
tio
n a
llia
nce
K
SF
1.
Kn
ow
led
ge
th
at
the
th
era
pe
uti
c a
llia
nce
is
usu
all
y s
ee
n a
s h
avi
ng
th
ree
co
mp
on
en
ts:
HW
B7
L3
1.1
. th
e r
ela
tio
nsh
ip o
r b
on
d b
etw
ee
n h
ea
lth
pro
fess
ion
al
an
d c
lie
nt
HW
B7
L3
1.2
. co
nse
nsu
s b
etw
ee
n t
he
he
alt
h p
rofe
ssio
na
l a
nd
cli
en
t re
ga
rdin
g t
he
go
als
of
inte
rve
nti
on
H
WB
7L3
1.3
. co
nse
nsu
s b
etw
ee
n t
he
he
alt
h p
rofe
ssio
na
l a
nd
cli
en
t re
ga
rdin
g t
he
te
chn
iqu
es/
me
tho
ds
em
plo
ye
d i
n t
he
in
terv
en
tio
n
HW
B7
L3
1.4
. A
n a
bil
ity
to
dra
w o
n k
no
wle
dg
e t
ha
t a
ll t
hre
e c
om
po
ne
nts
co
ntr
ibu
te t
o t
he
ma
inte
na
nce
of
the
all
ian
ce
HW
B7
L3
Ca
pa
city
to
de
ve
lop
an
d m
ain
tain
th
e a
llia
nce
K
SF
2.
An
ab
ilit
y t
o l
iste
n t
o t
he
cli
en
t’s
con
cern
s in
a m
an
ne
r w
hic
h i
s n
on
jud
gm
en
tal,
su
pp
ort
ive
an
d s
en
siti
ve,
an
d w
hic
h c
on
vey
s a
co
mfo
rta
ble
att
itu
de
wh
en
th
e c
lie
nt
de
scri
be
s th
eir
be
ha
vio
ur
an
d e
xpe
rie
nce
C1
L3
3.
An
ab
ilit
y t
o e
nsu
re t
ha
t th
e c
lie
nt
is c
lea
r a
bo
ut
the
ra
tio
na
le f
or
the
in
terv
en
tio
n b
ein
g o
ffe
red
C
1L3
HW
B7
L3
4.
An
ab
ilit
y t
o g
au
ge
wh
eth
er
the
cli
en
t: a
) u
nd
ers
tan
ds
the
ra
tio
na
le f
or
the
in
terv
en
tio
n,
b)
ha
s q
ue
stio
ns
ab
ou
t it
, o
r c)
is
ske
pti
cal
ab
ou
t th
e r
ati
on
ale
,
an
d t
o r
esp
on
d t
o t
he
se c
on
cern
s o
pe
nly
an
d n
on
-de
fen
siv
ely
C1
L3
HW
B7
L3
5.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
exp
ress
an
y c
on
cern
s o
r d
ou
bts
th
ey
ha
ve a
bo
ut
the
in
terv
en
tio
n a
nd
/or
the
he
alt
h p
rofe
ssio
na
l, e
spe
cia
lly
wh
ere
th
is r
ela
tes
to m
istr
ust
or
ske
pti
cism
C1
L3
HW
B7
L3
6.
An
ab
ilit
y t
o r
esp
on
d a
pp
rop
ria
tely
to
in
terv
en
tio
ns
in r
esp
on
se t
o d
isa
gre
em
en
ts a
bo
ut
task
s a
nd
go
als
: C
1L3
HW
B7
L3

Pa
ge
| 2
2
6.1
. A
n a
bil
ity
to
ch
eck
th
at
the
clie
nt
is c
lea
r a
bo
ut
the
ra
tio
na
le f
or
the
in
terv
en
tio
n a
nd
to
re
vie
w t
his
wit
h t
he
m a
nd
/or
cla
rify
an
y
mis
un
de
rsta
nd
ing
s
C1
L3
HW
B7
L3
6.2
. A
n a
bil
ity
to
he
lp c
lie
nts
un
de
rsta
nd
th
e r
ati
on
ale
fo
r th
e i
nte
rve
nti
on
th
rou
gh
usi
ng
/dra
win
g a
tte
nti
on
to
co
ncr
ete
exa
mp
les
C
1L3
HW
B7
L3
7.
An
ab
ilit
y t
o u
se h
um
ou
r ju
dic
iou
sly
, u
nd
ers
tan
din
g h
ow
it
can
be
use
d a
s a
n a
id t
o h
elp
cli
en
ts (
e.g
. to
no
rma
lise
th
e c
lie
nt’
s e
xpe
rie
nce
or
to r
ed
uce
ten
sio
n),
bu
t a
lso
re
cog
nis
ing
its
ris
ks
(e.g
. o
f in
vali
da
tin
g t
he
cli
en
t’s
fee
lin
gs,
act
ing
as
a d
istr
act
ion
to
/ a
void
an
ce o
f fe
eli
ng
s, o
r cr
ea
tin
g “
bo
un
da
ry
vio
lati
on
s”)
C1
L3
8.
An
ab
ilit
y t
o r
esp
on
d t
o c
lie
nt’
s h
um
ou
r in
a m
an
ne
r th
at
is c
on
gru
en
t w
ith
its
in
ten
t, a
nd
re
spo
nsi
ve t
o a
ny
im
pli
ed
me
an
ing
s
C1
L3
F8
. C
ap
aci
ty t
o a
da
pt
inte
rve
nti
on
s in
re
spo
nse
to
cli
en
t fe
ed
ba
ck
K
SF
1.
An
ab
ilit
y t
o a
cco
mm
od
ate
iss
ue
s th
e c
lie
nt
rais
es
exp
lici
tly
or
imp
lici
tly
, o
r w
hic
h b
eco
me
ap
pa
ren
t a
s p
art
of
the
pro
cess
of
the
in
terv
en
tio
n:
H
WB
4L3
HW
B7
L3
2.
An
ab
ilit
y t
o r
esp
on
d t
o,
an
d o
pe
nly
to
dis
cuss
, e
xpli
cit
fee
db
ack
fro
m t
he
cli
en
t w
hic
h e
xpre
sse
s co
nce
rns
ab
ou
t im
po
rta
nt
asp
ect
s o
f th
e i
nte
rve
nti
on
C
1L3
HW
B4
L3
3.
An
ab
ilit
y t
o d
ete
ct a
nd
re
spo
nd
to
im
pli
cit
fee
db
ack
wh
ich
in
dic
ate
s th
at
the
cli
en
t h
as
con
cern
s a
bo
ut
imp
ort
an
t a
spe
cts
of
the
in
terv
en
tio
n (
e.g
. a
s
ind
ica
ted
by
no
n-v
erb
al
be
ha
vio
ur,
ve
rba
l co
mm
en
ts o
r si
gn
ific
an
t sh
ifts
in
re
spo
nsi
ve
ne
ss)
HW
B7
L1
F9
. A
bil
ity
to
Ma
na
ge
Exp
ect
ati
on
s o
f th
e I
nte
rve
nti
on
K
SF
1.
Ab
ilit
y t
o c
om
mu
nic
ate
th
e f
req
ue
ncy
an
d d
ura
tio
n o
f co
nsu
lta
tio
ns
C1
L3
HW
B7
L3
2.
Ab
ilit
y t
o c
om
mu
nic
ate
wh
at
is e
xpe
cte
d o
f cl
ien
t b
etw
ee
n c
on
sult
ati
on
s C
1L3
HW
B7
L3
3.
Ab
ilit
y t
o m
an
ag
e e
nd
ing
s C
1L3
HW
B7
L3
3.3
. A
n a
bil
ity
to
sig
na
l th
e e
nd
ing
of
the
in
terv
en
tio
n a
t a
pp
rop
ria
te p
oin
ts d
uri
ng
th
e i
nte
rve
nti
on
(e
.g.
wh
en
ag
ree
ing
th
e i
nte
rve
nti
on
co
ntr
act
, a
nd
esp
eci
all
y a
s th
e i
nte
rve
nti
on
dra
ws
to c
lose
) in
a w
ay
wh
ich
ack
no
wle
dg
es
the
po
ten
tia
l im
po
rta
nce
of
this
tra
nsi
tio
n f
or
the
cli
en
t
C1
L3
HW
B7
L3
3.4
. A
n a
bil
ity
to
re
vie
w t
he
wo
rk u
nd
ert
ak
en
to
ge
the
r C
1L3
HW
B7
L3
3.5
. A
n a
bil
ity
to
sa
y g
oo
db
ye
C
1L3
HW
B7
L3

Pa
ge
| 2
3
F1
0.
Ab
ilit
y t
o d
eli
ve
r in
form
ati
on
KS
F
1.
An
ab
ilit
y t
o d
eli
ver
info
rma
tio
n i
n a
ma
nn
er
tha
t ca
n b
e u
nd
ers
too
d b
y t
he
cli
en
t C
1L3
2.
An
ab
ilit
y t
o g
ive
in
stru
ctio
n i
n a
ma
nn
er
clie
nt
can
fo
llo
w
C1
L3
3.
Ab
ilit
y t
o g
ive
ad
vice
in
a m
an
ne
r th
at
en
ab
les
clie
nt
to c
ho
se w
he
the
r o
r n
ot
to t
ak
e a
dvi
ce
C1
L3
4.
Ab
ilit
y t
o g
ive
ad
vice
ab
ou
t a
dd
itio
na
l re
sou
rce
s (i
ncl
ud
ing
me
dic
ati
on
) a
nd
su
pp
ort
re
leva
nt
to t
he
he
alt
h b
eh
avi
ou
r p
rob
lem
C
1L3
HW
B7
L3
F1
1.
Ca
pa
city
to
str
uct
ure
co
nsu
lta
tio
ns
an
d m
ain
tain
ap
pro
pri
ate
pa
cin
g
K
SF
1.
An
ab
ilit
y t
o m
ain
tain
ad
he
ren
ce t
o a
n a
gre
ed
ag
en
da
an
d t
o ‘
pa
ce’
the
co
nsu
lta
tio
n i
n a
ma
nn
er
wh
ich
en
sure
s th
at
all
ag
ree
d i
tem
s ca
n b
e g
ive
n
ap
pro
pri
ate
att
en
tio
n (
i.e
. e
nsu
rin
g t
ha
t si
gn
ific
an
t is
sue
s a
re n
ot
rush
ed
)
HW
B7
L3
2.
An
ab
ilit
y t
o b
ala
nce
th
e n
ee
d t
o m
ain
tain
ad
he
ren
ce a
nd
pa
cin
g w
hil
e b
ein
g a
pp
rop
ria
tely
re
spo
nsi
ve t
o c
lie
nt
ne
ed
:
HW
B7
L3
2.1
. A
n a
bil
ity
to
str
uct
ure
th
e s
ess
ion
in
a m
an
ne
r w
hic
h i
s co
ng
rue
nt
wit
h s
pe
cifi
c is
sue
s (e
.g.
the
cli
en
t’s
cap
aci
ty t
o c
on
cen
tra
te)
H
WB
7L3
3.
An
ab
ilit
y t
o b
ala
nce
th
e n
ee
d t
o m
ain
tain
an
ap
pro
pri
ate
pa
ce v
fo
llo
win
g u
p i
mp
ort
an
t is
sue
s ra
ise
d b
y t
he
cli
en
t:
HW
B7
L3
3.1
. A
n a
bil
ity
to
use
pro
fess
ion
al
jud
gm
en
t to
de
cid
e w
he
n i
ssu
es
ne
ed
s to
be
pu
rsu
ed
an
d w
he
n t
he
y c
ou
ld a
ct t
o d
ive
rt a
tte
nti
on
fro
m t
he
pri
ma
ry
(an
d a
gre
ed
) fo
cus
of
the
in
terv
en
tio
n
HW
B7
L3
F1
2.
Ab
ilit
y t
o r
eco
gn
ise
ba
rrie
rs t
o a
nd
fa
cili
tato
rs o
f im
ple
me
nti
ng
in
terv
en
tio
ns
K
SF
1.
Ab
ilit
y t
o r
eco
gn
ize
ba
rrie
rs t
o a
nd
fa
cili
tato
rs o
f im
ple
me
nti
ng
in
terv
en
tio
ns
at
the
le
ve
l o
f:
C4
L3
1.1
. O
rga
nis
ati
on
al
ba
rrie
rs a
nd
fa
cili
tato
rs:
C4
L3
1.1
.1.
ava
ila
bil
ity
of
tim
e a
nd
re
sou
rce
s to
en
ab
le i
mp
lem
en
tati
on
of
inte
rve
nti
on
s C
4L3
1.1
.2.
org
an
iza
tio
na
l a
ttit
ud
es
C
4L3
1.1
.3.
pro
visi
on
of
sup
erv
isio
n a
nd
on
go
ing
su
pp
ort
to
pra
ctic
e
C4
L3
1.2
. In
div
idu
al
he
alt
h p
rofe
ssio
na
l b
arr
iers
an
d f
aci
lita
tors
: C
5L3
1.2
.1.
ow
n b
eli
efs
an
d a
ttit
ud
es
to h
ea
lth
be
ha
vio
r a
nd
be
ha
vio
ur
cha
ng
e
C5
L3
1.2
.2.
com
pe
ten
ces
req
uir
ed
to
im
ple
me
nt
inte
rve
nti
on
s C
5L3
1.2
.3.
ad
eq
ua
te p
ost
in
wh
ich
to
de
live
r in
terv
en
tio
ns
C4
L3
C5
L3
1.3
. C
lie
nt
ba
rrie
rs a
nd
fa
cili
tato
rs:
HW
B6
L3
1.3
.1.
be
lie
fs,
att
itu
de
s, h
ea
lth
co
nd
itio
n
HW
B6
L3
1.3
.2.
soci
al
an
d p
hy
sica
l e
nvi
ron
me
nt
HW
B6
L3

Pa
ge
| 2
4
Be
ha
vio
ur
Ch
an
ge
Co
mp
ete
ncy
Do
ma
in
BC
1.
Kn
ow
led
ge
of
He
alt
h b
eh
av
iou
r a
nd
he
alt
h b
eh
av
iou
r p
rob
lem
s
KS
F
Kn
ow
led
ge
of:
1.
Co
mm
on
he
alt
h b
eh
avi
ou
r p
rob
lem
s d
uri
ng
ass
ess
me
nt
an
d w
he
n c
arr
yin
g o
ut
inte
rve
nti
on
s, i
ncl
ud
ing
kn
ow
led
ge
of
na
tio
na
l g
uid
eli
ne
s fo
r h
ea
lth
be
ha
vio
urs
, e
.g.
alc
oh
ol
con
sum
pti
on
lim
its,
re
com
me
nd
ed
ph
ysi
cal
act
ivit
y l
eve
ls e
tc
HW
B6
L3
HW
B7
L3
2.
Fa
cto
rs a
sso
cia
ted
wit
h t
he
de
ve
lop
me
nt
an
d m
ain
ten
an
ce o
f h
ea
lth
be
ha
vio
urs
H
WB
7L3
3.
Th
e u
sua
l p
att
ern
s o
f h
ea
lth
be
ha
vio
ur
pro
ble
ms
HW
B7
L3
4.
Th
e w
ay
s in
wh
ich
he
alt
h b
eh
avi
ou
r p
rob
lem
s ca
n i
mp
act
on
he
alt
h a
nd
fu
nct
ion
ing
H
WB
7L3
5.
Th
e u
sua
l k
no
wle
dg
e a
nd
mis
info
rma
tio
n t
ha
t p
eo
ple
ma
y h
ave
ab
ou
t h
ea
lth
be
ha
vio
ur
pro
ble
ms
HW
B7
L3
6.
Ma
in t
erm
s a
nd
co
nce
pts
use
d i
n e
pid
em
iolo
gy
an
d t
he
ba
sis
of
calc
ula
tio
ns
rela
ted
to
th
ese
te
rms
HW
B7
L3
7.
Dif
fere
nt
mo
de
ls,
pri
nci
ple
s a
nd
ap
pro
ach
es
to m
an
ag
ing
ris
k
HW
B7
L3
8.
Dif
fere
nt
mo
de
ls,
pri
nci
ple
s a
nd
ap
pro
ach
es
to p
reve
nti
ng
ris
k a
nd
th
rea
ts t
o p
op
ula
tio
n h
ea
lth
H
WB
7L3
9.
Dif
fere
nt
mo
de
ls,
pri
nci
ple
s a
nd
ap
pro
ach
es
to i
mp
rovi
ng
th
e h
ea
lth
of
ind
ivid
ua
ls
HW
B7
L3
BC
2.
Ab
ilit
y t
o u
nd
ert
ak
e a
ge
ne
ric
ass
ess
me
nt
K
SF
1.
An
ab
ilit
y t
o o
bta
in a
ge
ne
ral
ide
a o
f th
e n
atu
re o
f th
e c
lie
nt’
s p
rob
lem
C
1L3
HW
B6
L3
2.
An
ab
ilit
y t
o e
lici
t in
form
ati
on
re
ga
rdin
g h
ea
lth
be
ha
vio
ur
pro
ble
ms
an
d d
iag
no
sis
C1
L3
HW
B6
L3
3.
Ab
ilit
y t
o e
lici
t in
form
ati
on
ab
ou
t p
ast
his
tory
an
d p
rese
nt
life
sit
ua
tio
n
C1
L3
HW
B6
L3
4.
Ab
ilit
y t
o e
lici
t in
form
ati
on
ab
ou
t b
eh
avi
ou
ral
an
d o
the
r ri
sk f
act
ors
fo
r d
ise
ase
C
1L3
HW
B6
L3
5.
Ab
ilit
y s
cre
en
cli
en
t fo
r su
ita
bil
ity
fo
r g
rou
p b
ase
d s
up
po
rt w
he
re a
pp
rop
ria
te
C1
L3
HW
B6
L3
6.
Ab
ilit
y t
o s
cre
en
cli
en
t fo
r su
ita
bil
ity
fo
r b
eh
avi
ou
r ch
an
ge
or
refe
rra
l to
sp
eci
ali
st h
elp
C
1L3
HW
B6
L3
7.
An
ab
ilit
y t
o g
au
ge
th
e c
lie
nt’
s m
oti
vati
on
fo
r a
be
ha
vio
ur
cha
ng
e i
nte
rve
nti
on
C
1L3
HW
B6
L3

Pa
ge
| 2
5
BC
3.
Kn
ow
led
ge
of
a m
od
el
of
be
ha
vio
ur
cha
ng
e a
nd
th
e a
bil
ity
to
un
de
rsta
nd
an
d e
mp
loy
th
e m
od
el
in p
ract
ice
K
SF
1.
Kn
ow
led
ge
of
the
fa
cto
rs c
om
mo
n t
o a
ll b
eh
avi
ou
r ch
an
ge
mo
de
ls a
nd
me
tho
ds:
H
WB
6L3
1.1
. S
up
po
rt f
act
ors
: H
WB
6L3
1.1
.1.
a p
osi
tive
wo
rkin
g r
ela
tio
nsh
ip b
etw
ee
n h
ea
lth
pro
fess
ion
al
an
d c
lie
nt
cha
ract
eri
sed
by
wa
rmth
, re
spe
ct,
acc
ep
tan
ce a
nd
em
pa
thy
, a
nd
tru
st
HW
B6
L3
1.1
.2.
the
act
ive
pa
rtic
ipa
tio
n o
f th
e c
lie
nt
HW
B6
L3
1.1
.3.
he
alt
h p
rofe
ssio
na
l e
xpe
rtis
e
HW
B6
L3
1.1
.4.
op
po
rtu
nit
ies
for
the
cli
en
t to
dis
cuss
ma
tte
rs o
f co
nce
rn
HW
B6
L3
1.2
. Le
arn
ing
fa
cto
rs:
HW
B6
L3
1.1
.1.
info
rma
tio
n
HW
B6
L3
1.1
.2.
ad
vice
H
WB
6L3
1.1
.3.
fee
db
ack
H
WB
6L3
1.1
.4.
cha
ng
ing
exp
ect
ati
on
s o
f p
ers
on
al
eff
ect
ive
ne
ss
HW
B6
L3
1.1
.5.
ass
imil
ati
on
of
pro
ble
ma
tic
exp
eri
en
ces
HW
B6
L3
1.3
. A
ctio
n f
act
ors
: H
WB
6L3
1.3
.1.
be
ha
vio
ura
l re
gu
lati
on
H
WB
6L3
1.3
.2.
cog
nit
ive
ma
ste
ry
HW
B6
L3
1.3
.3.
exp
eri
en
ce o
f su
cce
ssfu
l co
pin
g
HW
B6
L3
2.
Kn
ow
led
ge
of
the
pri
nci
ple
s w
hic
h u
nd
erl
ie t
he
in
terv
en
tio
n b
ein
g a
pp
lie
d,
usi
ng
th
is t
o i
nfo
rm t
he
ap
pli
cati
on
of
the
sp
eci
fic
tech
niq
ue
s w
hic
h
cha
ract
eri
se t
he
mo
de
l
HW
B6
L3
3.
Kn
ow
led
ge
of
th
e p
rin
cip
les
of
the
be
ha
vio
ur
cha
ng
e m
od
el
in o
rde
r to
im
ple
me
nt
the
in
terv
en
tio
n i
n a
ma
nn
er
wh
ich
is
fle
xib
le a
nd
re
spo
nsi
ve
to
cli
en
t
ne
ed
, b
ut
wh
ich
als
o e
nsu
res
tha
t a
ll r
ele
van
t co
mp
on
en
ts a
re i
ncl
ud
ed
HW
B6
L3
4.
Kn
ow
led
ge
of
the
evi
de
nce
ba
se f
or
the
eff
ect
ive
ne
ss o
f b
eh
avi
ou
r ch
an
ge
mo
de
ls
HW
B6
L3
BC
4.
Ab
ilit
y t
o a
gre
e g
oa
ls f
or
the
in
terv
en
tio
n
1.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
ge
ne
rate
th
eir
ow
n g
oa
ls f
or
the
in
terv
en
tio
n,
an
d t
o r
ea
ch a
sh
are
d a
gre
em
en
t a
bo
ut
the
se,
by
he
lpin
g t
he
m:
H
WB
4L3
HW
B7
L3
1.1
. to
tra
nsl
ate
va
gu
e/a
bst
ract
go
als
in
to s
pe
cifi
c a
nd
co
ncr
ete
go
als
H
WB
4L3
1.2
. to
id
en
tify
go
als
wh
ich
wil
l b
e s
ub
ject
ive
ly a
nd
ob
ject
ive
ly o
bse
rva
ble
an
d p
ote
nti
all
y m
ea
sura
ble
(i.
e.
to e
nsu
re t
ha
t if
ch
an
ge
ta
ke
s p
lace
it
wil
l b
e
no
tice
ab
le t
o t
he
cli
en
t a
nd
to
oth
ers
)
HW
B4
L3
2.
An
ab
ilit
y t
o w
ork
wit
h t
he
cli
en
t to
en
sure
th
at
go
als
are
re
ali
stic
, a
tta
ina
ble
an
d t
ime
ly
HW
B4
L3

Pa
ge
| 2
6
BC
5.
Ca
pa
city
to
im
ple
me
nt
be
ha
vio
ur
cha
ng
e m
od
els
in
a f
lex
ible
bu
t co
he
ren
t m
an
ne
r
K
SF
1.
An
ab
ilit
y t
o i
mp
lem
en
t a
mo
de
l o
f b
eh
avi
ou
r ch
an
ge
in
a m
an
ne
r w
hic
h i
s fl
exi
ble
an
d w
hic
h i
s re
spo
nsi
ve t
o t
he
iss
ue
s th
e c
lie
nt
rais
es,
bu
t w
hic
h a
lso
en
sure
s th
at
all
re
leva
nt
com
po
ne
nts
of
the
mo
de
l a
re i
ncl
ud
ed
HW
B7
L3
2.
An
ab
ilit
y t
o m
ain
tain
ad
he
ren
ce t
o a
mo
de
l w
ith
ou
t in
ap
pro
pri
ate
sw
itch
ing
be
twe
en
mo
da
liti
es
in r
esp
on
se t
o m
ino
r d
iffi
cult
ies
(i.e
. d
iffi
cult
ies
wh
ich
can
be
re
ad
ily
acc
om
mo
da
ted
by
th
e m
od
el
be
ing
ap
pli
ed
)
HW
B6
L3
BC
6.
Ca
pa
city
to
se
lect
an
d s
kil
lfu
lly
to
ap
ply
th
e m
ost
ap
pro
pri
ate
be
ha
vio
ur
cha
ng
e i
nte
rve
nti
on
me
tho
d
1.
An
ab
ilit
y d
raw
on
kn
ow
led
ge
of
be
ha
vio
ur
cha
ng
e m
od
els
an
d m
eth
od
s a
nd
on
pro
fess
ion
al
exp
eri
en
ce i
n o
rde
r to
se
lect
fro
m t
he
co
mp
lete
ra
ng
e o
f
be
ha
vio
ur
cha
ng
e t
ech
niq
ue
s, a
nd
sk
illf
ull
y a
pp
ly t
he
m i
n a
ma
nn
er
wh
ich
is:
HW
B7
L3
HW
B6
L3
1.1
. m
atc
he
d t
o t
he
ne
ed
s a
nd
ca
pa
citi
es
of
the
cli
en
t
HW
B7
L3
HW
B6
L3
1.2
. a
pp
lie
d a
t th
e a
pp
rop
ria
te l
eve
l o
f p
rog
ress
ion
in
th
e p
roce
ss o
f b
eh
avi
ou
r ch
an
ge
H
WB
7L3
HW
B6
L3
BC
7.
Ca
pa
city
to
im
ple
me
nt
be
ha
vio
ur
cha
ng
e i
n a
ma
nn
er
con
son
an
t w
ith
its
un
de
rly
ing
ph
ilo
sop
hy
Ba
sic
ori
en
tati
on
1.
An
ab
ilit
y t
o b
ase
all
he
alt
h p
rofe
ssio
na
l/cl
ien
t co
nta
ct a
nd
co
nd
uct
on
a p
ers
pe
ctiv
e w
hic
h s
ee
s th
e w
orl
d,
incl
ud
ing
in
tera
ctio
ns
wit
h t
he
he
alt
h
pro
fess
ion
al,
fro
m t
he
pe
rsp
ect
ive
of
the
cli
en
t’s
be
lie
fs a
nd
ab
ilit
ies
C1
L3
HW
B7
L3
Ca
pa
city
to
fo
rm a
nd
ma
inta
in a
co
lla
bo
rati
ve
sta
nce
2.
A c
ap
aci
ty t
o f
orm
a c
oll
ab
ora
tive
re
lati
on
ship
wit
h t
he
cli
en
t, b
ase
d o
n a
n a
ctiv
e s
tan
ce w
hic
h f
ocu
ses
on
en
ab
lin
g t
he
cli
en
t a
nd
th
e h
ea
lth
pro
fess
ion
al
to w
ork
as
a t
ea
m
HW
B4
L3
HW
B7
L3
3.
An
ab
ilit
y t
o b
ala
nce
th
e n
ee
d t
o s
tru
ctu
re c
on
sult
ati
on
s a
s a
ga
inst
th
e n
ee
d t
o a
llo
w t
he
cli
en
t to
ma
ke
ch
oic
es
an
d t
ak
e r
esp
on
sib
ilit
y
HW
B7
L3
4.
An
ab
ilit
y t
o a
void
im
ple
me
nti
ng
be
ha
vio
ur
cha
ng
e i
n a
ma
nn
er
wh
ich
be
com
es
did
act
ic,
dir
ect
ive
, in
tell
ect
ua
l o
r co
ntr
oll
ing
H
WB
4L3
HW
B7
L3
Ma
inta
inin
g a
pro
ble
m s
olv
ing
pe
rsp
ect
ive
5.
An
ab
ilit
y t
o a
void
se
ein
g t
he
cli
en
t th
em
selv
es
as
a p
rob
lem
, b
ut
to m
ain
tain
a p
rob
lem
-so
lvin
g a
pp
roa
ch t
o t
he
cli
en
t’s
he
alt
h b
eh
avi
ou
r p
rob
lem
s H
WB
4L3
HW
B7
L3
6.
An
ab
ilit
y t
o m
ain
tain
a p
rob
lem
-so
lvin
g a
ttit
ud
e i
n t
he
fa
ce o
f d
iffi
cult
ies
an
d f
rust
rati
on
s H
WB
4L3
HW
B7
L3

Pa
ge
| 2
7
BC
8.
Ab
ilit
y t
o s
tru
ctu
re c
on
sult
ati
on
s
K
SF
1.
An
ab
ilit
y t
o s
tru
ctu
re c
on
sult
ati
on
s H
WB
7L3
2.
An
ab
ilit
y t
o s
ha
re r
esp
on
sib
ilit
y f
or
con
sult
ati
on
str
uct
ure
& c
on
ten
t
HW
B7
L3
2.1
. A
n a
bil
ity
to
be
ap
pro
pri
ate
ly s
tru
ctu
red
(e
spe
cia
lly
in
th
e i
nit
ial
sta
ge
s o
f th
e i
nte
rve
nti
on
), b
ut
als
o t
o a
void
be
com
ing
in
ap
pro
pri
ate
ly d
ida
ctic
H
WB
7L3
3.
An
ab
ilit
y t
o a
gre
e a
nd
ad
he
re t
o a
n a
gre
ed
ag
en
da
H
WB
7L3
3.1
. A
n a
bil
ity
to
wo
rk c
oll
ab
ora
tive
ly w
ith
th
e c
lie
nt
to s
et
a m
utu
all
y a
gre
ed
ag
en
da
at
the
sta
rt o
f e
ach
co
nsu
lta
tio
n
HW
B7
L3
3.2
. A
n a
bil
ity
to
se
t a
n a
ge
nd
a t
ha
t is
: H
WB
7L3
3.2
.1.
ap
pro
pri
ate
to
th
e c
lie
nt’
s h
ea
lth
be
ha
vio
ur
pro
ble
m
HW
B7
L3
3.2
.2.
ap
pro
pri
ate
fo
r th
e l
ev
el
of
pro
gre
ssio
n i
n t
he
pro
cess
of
be
ha
vio
ur
cha
ng
e
HW
B7
L3
3.2
.3.
con
sist
en
t w
ith
th
e s
ha
red
un
de
rsta
nd
ing
of
the
cli
en
t’s
pro
ble
m
HW
B7
L3
3.2
.4.
an
ab
ilit
y t
o p
rio
riti
se a
ge
nd
a i
tem
s, a
nd
se
t a
n a
ge
nd
a w
hic
h f
its
wit
h t
he
tim
e a
vail
ab
le
HW
B7
L3
3.2
.5.
an
ab
ilit
y t
o a
dh
ere
to
th
e a
ge
nd
a
HW
B7
L3
3.3
. A
n a
bil
ity
to
pa
ce t
he
co
nsu
lta
tio
n a
nd
use
tim
e e
ffic
ien
tly
H
WB
7L3
3.3
.1.
an
ab
ilit
y t
o ‘
tim
e m
an
ag
e’
the
co
nsu
lta
tio
n i
n r
ela
tio
n t
o t
he
ag
en
da
H
WB
7L3
3.3
.2.
an
ab
ilit
y t
o p
ace
th
e c
on
sult
ati
on
in
re
lati
on
to
th
e c
lie
nt’
s n
ee
ds
an
d l
ea
rnin
g s
pe
ed
H
WB
7L3
4.
An
ab
ilit
y t
o m
ak
e a
nd
re
vie
w a
ctio
n p
lan
s
HW
B4
L3
4.1
. A
bil
ity
to
pla
n a
ctio
n p
lan
s
HW
B4
L3
4.1
.1.
an
ab
ilit
y t
o w
ork
wit
h t
he
cli
en
t to
ag
ree
ap
pro
pri
ate
an
d m
an
ag
ea
ble
act
ion
pla
ns
H
WB
4L3
4.1
.2.
an
ab
ilit
y t
o w
ork
wit
h c
lie
nt
to i
de
nti
fy s
tra
teg
ies
wh
ich
wil
l h
elp
en
sure
th
at
act
ion
pla
ns
are
ca
rrie
d o
ut
H
WB
4L3
4.2
. A
bil
ity
to
re
vie
w a
ctio
n p
lan
s H
WB
6L3
4.2
.1.
an
ab
ilit
y t
o e
nsu
re t
ha
t a
ctio
n p
lan
s th
at
the
cli
en
t h
as
un
de
rta
ke
n a
re c
are
full
y d
iscu
sse
d a
nd
re
vie
we
d w
ith
th
em
in
th
e n
ext
se
ssio
n,
wit
h
the
aim
of
he
lpin
g t
he
m i
de
nti
fy w
ha
t th
ey
ha
ve l
ea
rne
d
HW
B6
L3
4.2
.2.
An
ab
ilit
y t
o h
elp
cli
en
ts a
pp
rais
e t
he
ou
tco
me
s o
f a
ctio
n p
lan
s:
HW
B6
L3
4.2
.2.1
. w
he
n o
utc
om
es
are
in
lin
e w
ith
th
e p
rio
r e
xpe
cta
tio
ns
of
the
he
alt
h p
rofe
ssio
na
l a
nd
cli
en
t
HW
B6
L3
4.2
.2.2
. w
he
n t
he
re i
s a
dif
fere
nt
ou
tco
me
fro
m t
ha
t w
hic
h h
as
be
en
pre
dic
ted
H
WB
6L3
4.2
.3.
an
ab
ilit
y t
o i
nte
gra
te l
ea
rnin
g f
rom
act
ion
pla
ns
into
th
e s
ess
ion
, a
nd
to
bu
ild
on
th
is l
ea
rnin
g i
n i
de
nti
fyin
g f
urt
he
r a
ctio
n p
lan
s
HW
B4
L3
HW
B6
L3
5.
An
ab
ilit
y t
o u
se s
um
ma
rie
s a
nd
fe
ed
ba
ck t
o s
tru
ctu
re t
he
co
nsu
lta
tio
n
HW
B4
L3
5.1
. A
n a
bil
ity
to
str
uct
ure
th
e c
on
sult
ati
on
by
re
gu
larl
y g
ivin
g f
ee
db
ack
to
th
e c
lie
nt,
an
d b
y e
licit
ing
re
gu
lar
fee
db
ack
fro
m t
he
cli
en
t
HW
B6
L3
5.2
. A
n a
bil
ity
to
eli
cit
an
d r
esp
on
d b
oth
to
ve
rba
l a
nd
no
n-v
erb
al
fee
db
ack
fro
m t
he
cli
en
t th
rou
gh
ou
t th
e c
on
sult
ati
on
(i.
e.
to t
ak
e i
nto
acc
ou
nt
exp
lici
t
sta
tem
en
ts m
ad
e b
y t
he
cli
en
t a
nd
th
eir
em
oti
on
al
rea
ctio
ns)
H
WB
6L3
5.3
. A
n a
bil
ity
to
giv
e v
erb
al
fee
db
ack
to
th
e c
lie
nt
thro
ug
ho
ut
the
se
ssio
n,
by
off
eri
ng
‘ca
psu
le’
sum
ma
rie
s a
nd
by
‘ch
un
kin
g’
imp
ort
an
t (s
ali
en
t)
info
rma
tio
n a
nd
/or
top
ics
HW
B4
L3
HW
B6
L3

Pa
ge
| 2
8
5.4
. A
n a
bil
ity
to
in
vite
su
mm
ari
es
fro
m t
he
cli
en
t (t
o c
he
ck t
ha
t th
e h
ea
lth
pro
fess
ion
al
un
de
rsta
nd
s th
e c
lie
nt’
s h
ea
lth
be
ha
vio
ur
pro
ble
ms
an
d t
ha
t th
e
clie
nt
un
de
rsta
nd
s w
ha
t th
e h
ea
lth
pro
fess
ion
al
is s
ay
ing
)
C1
L3
HB
W4
L3
5.5
. A
n a
bil
ity
to
off
er
sum
ma
rie
s a
t th
e s
tart
of
con
sult
ati
on
s (e
.g.
a r
ev
iew
of
pri
or
wo
rk)
an
d a
t th
e e
nd
of
the
se
ssio
n (
cove
rin
g t
he
ma
in p
oin
ts o
f th
e
con
sult
ati
on
)
HW
B4
L3
HW
B6
L3
BC
9.
Ab
ilit
y t
o u
se m
ea
sure
s a
nd
se
lf-m
on
ito
rin
g t
o g
uid
e b
eh
av
iou
r ch
an
ge
in
terv
en
tio
ns
an
d t
o m
on
ito
r o
utc
om
e
K
SF
1.
Kn
ow
led
ge
of
com
mo
nly
use
d q
ue
stio
nn
air
es
an
d r
ati
ng
sca
les
HW
B6
L3
2.
Ab
ilit
y t
o s
ele
ct a
nd
in
terp
ret
me
asu
res:
H
WB
6L3
2.1
. A
bil
ity
to
se
lect
me
asu
res
rele
van
t to
th
e c
lie
nt’
s h
ea
lth
be
ha
vio
ur
pro
ble
m
HW
B6
L3
2.2
. A
n a
bil
ity
to
in
terp
ret
me
asu
res:
H
WB
6L3
2.2
.1.
An
ab
ilit
y t
o i
nte
rpre
t sc
ore
s o
n s
tan
da
rd m
ea
sure
s re
leva
nt
to c
lie
nt’
s h
ea
lth
be
ha
vio
ur
pro
ble
m
HW
B6
L3
2.2
.2.
An
ab
ilit
y t
o d
raw
on
kn
ow
led
ge
re
ga
rdin
g t
he
in
terp
reta
tio
n o
f m
ea
sure
s (e
.g.
ba
sic
pri
nci
ple
s o
f te
st c
on
stru
ctio
n,
no
rms
an
d c
lin
ica
l cu
t-
off
s, r
eli
ab
ilit
y,
vali
dit
y,
fact
ors
wh
ich
co
uld
in
flu
en
ce (
an
d p
ote
nti
all
y i
nva
lid
ate
) te
st r
esu
lts)
HW
B6
L3
2.2
.3.
An
ab
ilit
y t
o b
e a
wa
re o
f th
e w
ay
s in
wh
ich
th
e r
ea
ctiv
ity
of
me
asu
res
an
d s
elf
-mo
nit
ori
ng
pro
ced
ure
s ca
n b
ias
clie
nt
rep
ort
H
WB
6L3
3.
Kn
ow
led
ge
of
self
-mo
nit
ori
ng
:
HW
B6
L3
3.1
. A
n a
bil
ity
to
dra
w o
n k
no
wle
dg
e o
f se
lf-m
on
ito
rin
g f
orm
s d
ev
elo
pe
d f
or
use
in
sp
eci
fic
inte
rve
nti
on
s (a
s p
ub
lish
ed
in
art
icle
s, t
ext
bo
ok
s, m
an
ua
ls o
r
we
b-b
ase
d r
eso
urc
es)
HW
B6
L3
3.2
. K
no
wle
dg
e o
f th
e a
dva
nta
ge
s o
f u
sin
g s
elf
-mo
nit
ori
ng
(to
ga
in a
mo
re a
ccu
rate
co
ncu
rre
nt
de
scri
pti
on
of
be
ha
vio
urs
(ra
the
r th
an
re
lyin
g o
n r
eca
ll),
to h
elp
ad
ap
t th
e i
nte
rve
nti
on
in
re
lati
on
to
cli
en
t p
rog
ress
, a
nd
to
pro
vid
e t
he
cli
en
t w
ith
fe
ed
ba
ck a
bo
ut
the
ir p
rog
ress
)
HW
B6
L3
3.3
. K
no
wle
dg
e o
f th
e r
ole
of
self
-mo
nit
ori
ng
in
be
ha
vio
ur
cha
ng
e (
a m
ea
ns
of
he
lpin
g t
he
cli
en
t to
be
com
e a
n a
ctiv
e,
coll
ab
ora
tive
pa
rtic
ipa
nt
in t
he
ir
ow
n b
eh
avi
ou
r ch
an
ge
by
id
en
tify
ing
an
d a
pp
rais
ing
ho
w t
he
y r
ea
ct t
o e
ve
nts
(in
te
rms
of
the
ir o
wn
ph
ysi
olo
gic
al
rea
ctio
ns,
be
ha
vio
urs
, fe
eli
ng
s a
nd
cog
nit
ion
s))
HW
B6
L3
3.4
. A
n a
bil
ity
to
dra
w o
n k
no
wle
dg
e o
f m
ea
sure
me
nt
to e
nsu
re t
ha
t p
roce
du
res
for
self
-mo
nit
ori
ng
are
re
leva
nt
(i.e
. re
late
d t
o t
he
qu
est
ion
be
ing
ask
ed
), v
ali
d (
me
asu
rin
g w
ha
t is
in
ten
de
d t
o b
e m
ea
sure
d)
an
d r
eli
ab
le (
i.e
. re
aso
na
bly
co
nsi
ste
nt
wit
h h
ow
th
ing
s a
ctu
all
y a
re)
HW
B6
L3
4.
Ab
ilit
y t
o i
nte
gra
te m
ea
sure
s in
to t
he
in
terv
en
tio
n:
H
WB
6L3
4.1
. A
n a
bil
ity
to
use
an
d t
o i
nte
rpre
t re
leva
nt
me
asu
res
at
ap
pro
pri
ate
po
ints
th
rou
gh
ou
t th
e i
nte
rve
nti
on
, w
ith
th
e a
im o
f e
sta
bli
shin
g b
oth
a b
ase
lin
e
an
d i
nd
ica
tio
ns
of
pro
gre
ss
HW
B6
L3
4.2
. A
n a
bil
ity
to
sh
are
in
form
ati
on
gle
an
ed
fro
m m
ea
sure
s w
ith
th
e c
lie
nt,
wit
h t
he
aim
of
giv
ing
th
em
fe
ed
ba
ck a
bo
ut
pro
gre
ss
HW
B6
L3
4.3
. A
n a
bil
ity
to
est
ab
lish
an
ap
pro
pri
ate
sch
ed
ule
fo
r th
e a
dm
inis
tra
tio
n o
f m
ea
sure
s, a
void
ing
ove
r-te
stin
g,
bu
t a
lso
aim
ing
to
co
lle
ct d
ata
at
mo
re t
ha
n
on
e t
ime
po
int
HW
B6
L3
5.
Ab
ilit
y t
o h
elp
cli
en
ts u
se s
elf
-mo
nit
ori
ng
pro
ced
ure
s:
HW
B6
L3
5.1
. A
n a
bil
ity
to
co
nst
ruct
in
div
idu
ali
sed
se
lf-m
on
ito
rin
g f
orm
s, o
r to
ad
ap
t ‘s
tan
da
rd’
self
-mo
nit
ori
ng
fo
rms,
in
ord
er
to e
nsu
re t
ha
t m
on
ito
rin
g i
s
rele
van
t to
th
e c
lie
nt
HW
B6
L3

Pa
ge
| 2
9
5.2
. A
n a
bil
ity
to
wo
rk w
ith
th
e c
lie
nt
to e
nsu
re t
ha
t m
ea
sure
s o
f th
e t
arg
ete
d p
rob
lem
are
me
an
ing
ful
to t
he
cli
en
t (i
.e.
are
ch
ose
n t
o r
efl
ect
th
e c
lie
nt’
s
pe
rce
pti
on
s o
f th
e p
rob
lem
or
issu
e)
HW
B6
L3
5.3
. A
n a
bil
ity
to
en
sure
th
at
self
-mo
nit
ori
ng
in
clu
de
s ta
rge
ts w
hic
h a
re c
lea
rly
de
fin
ed
an
d d
eta
ile
d,
in o
rde
r th
at
the
y c
an
be
mo
nit
ore
d/r
eco
rde
d
reli
ab
ly
HW
B6
L3
5.4
. A
n a
bil
ity
to
en
sure
th
at
the
cli
en
t u
nd
ers
tan
ds
ho
w t
o u
se s
elf
-mo
nit
ori
ng
fo
rms
(usu
all
y b
y g
oin
g t
hro
ug
h a
wo
rke
d e
xam
ple
du
rin
g t
he
con
sult
ati
on
)
HW
B6
L3
6.
Ab
ilit
y t
o i
nte
gra
te s
elf
-mo
nit
ori
ng
in
to t
he
in
terv
en
tio
n
HW
B6
L3
6.1
. A
n a
bil
ity
to
en
sure
th
at
self
-mo
nit
ori
ng
is
inte
gra
ted
in
to t
he
in
terv
en
tio
n,
bo
th i
n t
he
co
nsu
lta
tio
n a
nd
as
pa
rt o
f a
ctio
n p
lan
s, e
nsu
rin
g t
ha
t th
e
ag
en
da
fo
r th
e c
on
sult
ati
on
in
clu
de
s re
gu
lar
an
d c
on
sist
en
t re
vie
w o
f se
lf-m
on
ito
rin
g f
orm
s
HW
B6
L3
6.2
. A
n a
bil
ity
to
gu
ide
an
d t
o a
da
pt
the
in
terv
en
tio
n i
n t
he
lig
ht
of
info
rma
tio
n f
rom
se
lf-m
on
ito
rin
g
HW
B6
L3
BC
10
. A
bil
ity
to
ca
rry
ou
t h
ea
lth
be
ha
vio
ur
pro
ble
m s
olv
ing
K
SF
1.
An
ab
ilit
y t
o i
de
nti
fy h
ea
lth
be
ha
vio
ur
pro
ble
ms
faci
ng
th
e c
lie
nt,
wh
ich
ma
y b
e a
pp
rop
ria
te f
or
a p
rob
lem
so
lvin
g a
pp
roa
ch
HW
B4
L3
2.
An
ab
ilit
y t
o e
xpla
in t
he
ra
tio
na
le f
or
pro
ble
m-s
olv
ing
to
th
e c
lie
nt
C
1L3
HW
B7
L3
3.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
to s
ele
ct p
rob
lem
s, u
sua
lly
on
th
e b
asi
s th
at
pro
ble
ms
are
re
leva
nt
for
the
cli
en
t a
nd
are
on
es
for
wh
ich
ach
ieva
ble
go
als
ca
n
be
se
t
HW
B4
L3
4.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
spe
cify
th
e p
rob
lem
(s),
an
d t
o b
rea
k d
ow
n l
arg
er
pro
ble
ms
into
sm
all
er
(mo
re m
an
ag
ea
ble
) p
art
s
HW
B4
L3
5.
An
ab
ilit
y t
o i
de
nti
fy a
chie
vab
le g
oa
ls w
ith
th
e c
lie
nt,
be
ari
ng
in
min
d t
he
cli
en
t’s
reso
urc
es
an
d l
ike
ly o
bst
acl
es
H
WB
4L3
6.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
ge
ne
rate
(“b
rain
sto
rm”)
po
ssib
le s
olu
tio
ns
H
WB
4L3
7.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
sele
ct a
pre
ferr
ed
so
luti
on
H
WB
4L3
8.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
pla
n a
nd
im
ple
me
nt
pre
ferr
ed
so
luti
on
s
HW
B4
L3
9.
An
ab
ilit
y t
o h
elp
th
e c
lie
nt
ev
alu
ate
th
e o
utc
om
e o
f im
ple
me
nta
tio
n,
wh
eth
er
po
siti
ve
or
ne
ga
tive
H
WB
6L3
BC
11
. C
ap
aci
ty t
o m
an
ag
e o
bst
acl
es
to c
arr
yin
g o
ut
be
ha
vio
ur
cha
ng
e
K
SF
1.
An
ab
ilit
y t
o w
ork
co
lla
bo
rati
vely
wit
h c
lie
nt
be
ha
vio
urs
th
at
are
po
ten
tia
lly
co
un
ter-
pro
du
ctiv
e –
fo
r e
xam
ple
, cl
ien
ts w
ho
:
C1
L3
1.1
. fi
nd
it
dif
ficu
lt t
o t
alk
H
WB
6L3
1.2
. te
nd
to
ta
lk t
oo
mu
ch a
nd
/or
fin
d i
t h
ard
to
sta
y f
ocu
sed
H
WB
6L3
1.3
. in
ven
t o
r d
isto
rt m
ate
ria
l
HW
B6
L3
1.4
. a
re p
ers
iste
ntl
y l
ate
H
WB
6L3

Pa
ge
| 3
0
BC
12
. A
bil
ity
to
en
d t
he
in
terv
en
tio
n i
n a
pla
nn
ed
ma
nn
er
an
d t
o p
lan
fo
r lo
ng
-te
rm m
ain
ten
an
ce o
f g
ain
s a
fte
r in
terv
en
tio
n e
nd
s
K
SF
1.
An
ab
ilit
y t
o t
erm
ina
te t
he
in
terv
en
tio
n i
n a
ma
nn
er
wh
ich
is
pla
nn
ed
, a
nd
to
sig
na
l p
lan
s fo
r te
rmin
ati
on
at
ap
pro
pri
ate
po
ints
th
rou
gh
ou
t th
e
inte
rve
nti
on
HW
B7
L3
2.
An
ab
ilit
y t
o p
lan
fo
r m
ain
ten
an
ce o
f b
eh
avi
ou
r ch
an
ge
aft
er
the
en
d o
f th
e i
nte
rve
nti
on
:
HW
B7
L3
2.1
. A
n a
bil
ity
to
he
lp c
lie
nts
id
en
tify
an
d e
lab
ora
te t
he
ir c
on
cern
s a
bo
ut
term
ina
tio
n (
e.g
. w
orr
y t
ha
t th
at
the
y n
ee
d s
up
po
rt t
o m
an
ag
e o
n t
he
ir o
wn
, o
r
tha
t th
ey
wil
l re
lap
se)
HW
B7
L3
2.2
. a
bil
ity
to
he
lp c
lie
nts
id
en
tify
oth
er
reso
urc
es
tha
t m
igh
t h
elp
th
em
ma
inta
in t
he
ir b
eh
avi
ou
r ch
an
ge
(e
.g.
we
igh
twa
tch
ers
, w
eb
site
s, g
ym
me
mb
ers
hip
)
HW
B7
L3

Pa
ge
| 3
1
Behaviour Change Techniques
BC
T
cod
ea
Na
me
of
BC
T
Be
ha
vio
ur
Ch
an
ge
Te
chn
iqu
e D
esc
rip
tio
n
KS
F
T
ech
niq
ue
s fo
r M
oti
va
tio
n D
ev
elo
pm
en
t
Lo
w I
nte
nsi
ty I
nte
rve
nti
on
s
M2
0
Re
ass
ura
nce
E
nco
ura
ge
cli
en
t to
be
lie
ve
in
he
rse
lf/h
imse
lf a
nd
th
e p
oss
ibil
itie
s o
f im
pro
vem
en
t (e
.g.
by
no
n-
spe
cifi
c su
pp
ort
ive
co
mm
en
ts e
.g.
‘yo
u’l
l d
o f
ine
’)
C1
L3
M1
7
Ge
ne
ral
info
rma
tio
n
Pro
vid
e g
en
era
l in
form
ati
on
ab
ou
t th
e b
eh
av
iou
r a
nd
be
ha
vio
ur
cha
ng
e
HW
B4
L3
M1
2
So
cia
l su
pp
ort
(em
oti
on
al)
Pro
vid
e &
/or
id p
ote
nti
al
sou
rce
s o
f e
mp
ath
y a
nd
giv
e g
en
era
lise
d p
osi
tive
fe
ed
ba
ck
HW
B4
L3
M1
0
Info
rma
tio
n a
bo
ut
the
be
ha
vio
ur
Pro
vid
e i
nfo
rma
tio
n a
bo
ut
an
tece
de
nts
or
con
seq
ue
nce
s o
f th
e b
eh
av
iou
r, o
r co
nn
ect
ion
s b
etw
ee
n
the
m,
or
be
ha
vio
ur
cha
ng
e t
ech
niq
ue
s
HW
B4
L3
M1
1
Ve
rba
l p
ers
ua
sio
n /
pe
rsu
asi
ve
com
mu
nic
ati
on
Pre
sen
tati
on
of
arg
um
en
ts in
fa
vo
ur
of
the
be
ha
vio
ur
by
a c
red
ible
so
urc
e (
NB
: th
ere
mu
st b
e
ev
ide
nce
of
pre
sen
tati
on
of
arg
um
en
ts;
ge
ne
ral
pro
-be
ha
vio
ur
com
mu
nic
ati
on
do
es
no
t co
un
t)
HW
B4
L3
M
ed
ium
Le
ve
l In
terv
en
tio
ns
M1
(a
lso
A4
)
An
tece
de
nts
&
con
seq
ue
nce
s
Re
cord
an
tece
de
nts
an
d c
on
seq
ue
nce
s o
f b
eh
av
iou
r (e
.g.
soci
al a
nd
en
vir
on
me
nta
l si
tua
tio
ns
an
d
ev
en
ts,
em
oti
on
s, c
og
nit
ion
s)
HW
B4
L3
M8
B
eh
av
iou
ral
exp
eri
me
nts
Ide
nti
fy a
nd
te
st h
yp
oth
ese
s a
bo
ut
the
be
ha
vio
ur,
its
ca
use
s a
nd
co
nse
qu
en
ces,
by
co
lle
ctin
g a
nd
inte
rpre
tin
g d
ata
HW
B4
L3
HW
B6
L3
M1
3
De
cisi
on
-ma
kin
g
Ge
ne
rate
alt
ern
ati
ve c
ou
rse
s o
f a
ctio
n,
an
d p
ros
an
d c
on
s o
f e
ach
, a
nd
we
igh
th
em
up
H
WB
4L3
M1
5
Mo
tiv
ati
on
al
inte
rvie
win
g
Eli
cit
self
-mo
tiv
ati
ng
sta
tem
en
ts &
eva
lua
tio
n o
f o
wn
be
ha
vio
ur
to r
ed
uce
re
sist
an
ce t
o c
ha
ng
e
HW
B4
L3
M2
1
Re
fra
min
g
En
cou
rag
e c
lie
nt
to a
do
pt
a d
iffe
ren
t p
ers
pe
ctiv
e o
n b
eh
av
iou
r in
ord
er
to c
ha
ng
e a
ttit
ud
e (
e.g
. b
y
ask
ing
ho
w p
art
ne
r w
ou
ld s
ee
th
e b
eh
av
iou
r o
r h
ow
th
ey
mig
ht
see
it
wh
en
th
ey
we
re i
ll o
r o
lde
r)
HW
B4
L3
M5
(als
o A
7)
Co
ntr
act
G
en
era
te a
co
ntr
act
of
ag
ree
d p
erf
orm
an
ce o
f ta
rge
t b
eh
av
iou
r w
ith
at
lea
st o
ne
oth
er,
wri
tte
n
an
d s
ign
ed
or
ve
rba
l
HW
B4
L3

Pa
ge
| 3
2
M2
(als
o A
6)
Co
mp
ari
son
P
rov
ide
co
mp
ara
tiv
e d
ata
(cf
sta
nd
ard
be
ha
vio
ur,
pe
rso
n’s
ow
n p
ast
be
ha
vio
ur,
oth
ers
’ b
eh
av
iou
r)
HW
B4
L3
M3
S
oci
al
com
pa
riso
n
Pro
vid
e o
pp
ort
un
itie
s fo
r so
cia
l co
mp
ari
son
, i.
e.
com
pa
riso
n b
etw
ee
n s
elf
an
d o
the
r p
eo
ple
(e
.g.
con
test
s a
nd
gro
up
le
arn
ing
)
HW
B4
L3
M1
6
(als
o A
21
)
So
cia
l S
up
po
rt (
no
n-
spe
cifi
c)
Pro
vid
e a
nd
/or
ide
nti
fy s
ou
rce
s o
f n
on
-sp
eci
fic
soci
al s
up
po
rt
HW
B4
L3
H
igh
In
ten
sity
In
terv
en
tio
ns
M4
D
iscr
ep
an
cy
ass
ess
me
nt:
Hig
hli
gh
t n
atu
re o
f d
iscr
ep
an
cy (
dir
ect
ion
an
d a
mo
un
t) b
etw
ee
n s
tan
da
rd,
ow
n o
r o
the
rs’
be
ha
vio
ur
(go
es
be
yo
nd
sim
ple
se
lf-m
on
ito
rin
g)
HW
B4
L3
M6
F
ea
r a
rou
sal
Ind
uce
ne
ga
tive
(a
ve
rsiv
e)
em
oti
on
al
sta
te a
sso
cia
ted
wit
h t
he
be
ha
vio
ur
H
WB
4L3
M7
A
nti
cip
ate
d r
eg
ret
Ind
uce
exp
ect
ati
on
s o
f fu
ture
re
gre
t a
bo
ut
no
n-p
erf
orm
an
ce o
f b
eh
av
iou
r
HW
B4
L3
M9
C
og
nit
ive
rest
ruct
uri
ng
Ch
an
ge
co
gn
itio
ns
ab
ou
t ca
use
s a
nd
co
nse
qu
en
ces
of
be
ha
vio
ur
HW
B4
L3
M1
9
Pa
rad
oxi
cal
Inst
ruct
ion
s
Inst
ruct
th
e c
lie
nt
to d
o p
reci
sely
th
e o
pp
osi
te o
f w
ha
t co
mm
on
se
nse
wo
uld
dic
tate
in
ord
er
to
sho
w t
he
ab
surd
ity
or
self
-de
fea
tin
g n
atu
re o
f th
e c
lie
nt’
s o
rig
ina
l in
ten
tio
n (
e.g
. sm
ok
ing
ma
ny
mo
re c
iga
rett
es
tha
n t
he
clie
nt
wo
uld
no
rma
lly)
HW
B4
L3
M1
4
Co
pin
g s
tra
teg
ies
Ide
nti
fy b
eh
av
iou
rs t
o b
e u
nd
ert
ak
en
to
avo
id o
r re
du
ce s
tre
sso
rs
HW
B4
L3
M1
8
Ass
ert
ion
Tra
inin
g
A c
om
bin
ati
on
of
tech
niq
ue
s u
sed
to
te
ach
cli
en
t in
terp
ers
on
al
com
mu
nic
ati
on
to
he
lp t
he
m
exp
ress
em
oti
on
s, o
pin
ion
s, a
nd
pre
fere
nce
s (p
osi
tiv
e a
nd
ne
ga
tiv
e)
cle
arl
y,
dir
ect
ly,
an
d i
n a
n
ap
pro
pri
ate
ma
nn
er
(e.g
. fo
r a
cli
en
t w
ho
ea
ts o
r sm
ok
es
foll
ow
ing
in
terp
ers
on
al c
on
flic
t)
HW
B4
L3
T
ech
niq
ue
s fo
r A
ctio
n o
n M
oti
va
tio
n
Lo
w I
nte
nsi
ty I
nte
rve
nti
on
s
A3
S
elf
-Mo
nit
ori
ng
of
be
ha
vio
ur
Re
cord
th
e s
pe
cifi
ed
be
ha
vio
ur
(pe
rso
n h
as
acc
ess
to
re
cord
ed
da
ta o
f b
eh
av
iou
ral
pe
rfo
rma
nce
,
e.g
. fr
om
dia
ry)
HW
B4
L3
A1
G
oa
l se
ttin
g
Ide
nti
fy a
nd
se
t a
be
ha
vio
ura
l g
oa
l
HW
B4
L3
A1
2
Inst
ruct
ion
T
ea
ch n
ew
be
ha
vio
ur
req
uir
ed
fo
r p
erf
orm
an
ce o
f ta
rge
t b
eh
av
iou
r (n
ot
as
pa
rt o
f g
rad
ed
hie
rarc
hy
or
as
pa
rt o
f m
od
ell
ing
) (e
.g.
giv
e c
lea
r in
stru
ctio
ns)
HW
B4
L3
A9
C
op
ing
pla
nn
ing
Id
en
tify
an
d p
lan
wa
ys
of
ov
erc
om
ing
ba
rrie
rs (
no
te,
this
mu
st i
ncl
ud
e i
de
nti
fica
tio
n o
f sp
eci
fic
ba
rrie
rs e
.g.
“pro
ble
m s
olv
ing
ho
w t
o f
it i
nto
we
ek
ly s
che
du
le”
wo
uld
no
t co
un
t)
HW
B4
L3

Pa
ge
| 3
3
A8
A
ctio
n P
lan
nin
g
Ma
ke
a d
eta
ile
d p
lan
of
wh
at
the
cli
en
t w
ill
do
in
clu
din
g,
as
a m
inim
um
, w
he
n,
an
d w
he
re t
o a
ct
HW
B4
L3
A1
0
Go
al
rev
iew
A
sse
ss e
xte
nt
to w
hic
h t
he
go
al/
targ
et
be
ha
vio
ur
is a
chie
ve
d,
ide
nti
fy t
he
fa
cto
rs in
flu
en
cin
g t
his
an
d a
me
nd
go
al
if a
pp
rop
ria
te
HW
B4
L3
M
ed
ium
In
ten
sity
In
terv
en
tio
ns
A4
(a
lso
M1
)
An
tece
de
nts
an
d
con
seq
ue
nce
s
Re
cord
an
tece
de
nts
an
d c
on
seq
ue
nce
s o
f b
eh
av
iou
r (e
.g.
soci
al a
nd
en
vir
on
me
nta
l si
tua
tio
ns
an
d
ev
en
ts,
em
oti
on
s, c
og
nit
ion
s)
HW
B4
L3
A2
S
tan
da
rd
De
cid
e o
n t
he
ta
rge
t st
an
da
rd o
f b
eh
av
iou
r (s
pe
cifi
ed
an
d o
bse
rva
ble
) H
WB
4L3
A5
F
ee
db
ack
P
rov
ide
fe
ed
ba
ck o
f m
on
ito
red
(in
c. s
elf
-mo
nit
ore
d)
be
ha
vio
ur
HW
B6
L3
A6
(a
lso
M5
) C
om
pa
riso
n
Pro
vid
e c
om
pa
rati
ve
da
ta (
cf s
tan
da
rd b
eh
av
iou
r, p
ers
on
’s o
wn
pa
st b
eh
av
iou
r, o
the
rs’
be
ha
vio
ur)
H
WB
4L3
A7
(a
lso
M5
) C
on
tra
ct
Ge
ne
rate
a c
on
tra
ct o
f a
gre
ed
pe
rfo
rma
nce
of
targ
et
be
ha
vio
ur
wit
h a
t le
ast
on
e o
the
r, w
ritt
en
an
d s
ign
ed
or
ve
rba
l
HW
B4
L3
A1
5
Se
lf t
alk
M
ak
e p
lan
ne
d s
elf
-sta
tem
en
ts (
alo
ud
or
sile
nt)
to
im
ple
me
nt
be
ha
vio
ur
cha
ng
e t
ech
niq
ue
s H
WB
4L3
A1
8
Re
laxa
tio
n
Pro
vid
e s
yst
em
ati
c in
stru
ctio
n i
n p
hy
sica
l an
d c
og
nit
ive
str
ate
gie
s to
re
du
ce s
ymp
ath
eti
c a
rou
sal,
an
d t
o i
ncr
ea
se m
usc
le r
ela
xati
on
an
d a
fe
eli
ng
of
calm
HW
B4
L3
A1
9
Tim
e m
an
ag
em
en
t A
pp
ly a
ctio
n p
lan
nin
g t
o t
he
pe
rce
ive
d p
rob
lem
of
sho
rta
ge
of
tim
e
HW
B4
L3
A2
0
Ho
me
wo
rk
Se
t h
om
ew
ork
ta
sks
tha
t re
pe
at
or
bu
ild
on
wo
rk d
on
e w
ith
clie
nt
e.g
. p
erf
orm
me
nta
l re
he
ars
al o
r
oth
er
BC
Ts
HW
B4
L3
A2
1
(als
o M
16
)
So
cia
l S
up
po
rt (
no
n-
spe
cifi
c)
Pro
vid
e a
nd
/or
ide
nti
fy s
ou
rce
s o
f n
on
-sp
eci
fic
soci
al s
up
po
rt
HW
B4
L3
A2
2
Ge
ne
ral
pro
ble
m-
solv
ing
En
ga
ge
cli
en
t in
ge
ne
ral
pro
ble
m-s
olv
ing
H
WB
4L3
A2
4
Av
oid
an
ce
Ide
nti
fy a
nd
ad
vis
e c
lie
nt
to a
vo
id t
ho
se p
art
icu
lar
situ
ati
on
s, a
ctiv
itie
s, e
nv
iro
nm
en
ts,
ind
ivid
ua
ls,
thin
gs,
or
sub
ject
s o
f th
ou
gh
t o
r co
nv
ers
ati
on
th
at
ha
ve a
nti
cip
ate
d n
eg
ati
ve
co
nse
qu
en
ces
HW
B4
L3
A1
1
(a
lso
P8
) G
rad
ed
ta
sks
Se
t e
asy
ta
sks
to p
erf
orm
, m
ak
ing
th
em
in
cre
asi
ng
ly d
iffi
cult
un
til
targ
et
be
ha
vio
ur
is p
erf
orm
ed
H
WB
4L3
H
igh
In
ten
sity
In
terv
en
tio
ns
A1
3
(als
o P
11
) B
eh
av
iou
ral
reh
ea
rsa
l P
rov
ide
or
ide
nti
fy o
pp
ort
un
itie
s fo
r cl
ien
t to
pe
rfo
rm b
eh
av
iou
r (r
ep
ea
ted
ly)
HW
B4
L3
A1
4
(als
o P
14
) R
ole
pla
y P
rov
ide
op
po
rtu
nit
ies
for
clie
nt
to p
erf
orm
be
ha
vio
ur
in s
imu
late
d s
itu
ati
on
s H
WB
4L3

Pa
ge
| 3
4
A1
6
(als
o P
17
) Im
ag
ery
U
se p
lan
ne
d im
ag
es
(vis
ua
l, m
oto
r, s
en
sory
) to
im
ple
me
nt
BC
Ts
(in
c. m
en
tal r
eh
ea
rsa
l)
HW
B4
L3
A1
7
Re
lap
se p
reve
nti
on
Id
en
tify
sit
ua
tio
ns
tha
t in
cre
ase
th
e l
ike
lih
oo
d o
f th
e b
eh
av
iou
r n
ot
be
ing
pe
rfo
rme
d a
nd
ap
ply
cop
ing
str
ate
gie
s to
th
ose
sit
ua
tio
ns
HW
B4
L3
A2
3
Bio
fee
db
ack
Use
an
ext
ern
al m
on
ito
rin
g d
ev
ice
to
pro
vid
e a
n i
nd
ivid
ua
l w
ith
in
form
ati
on
re
ga
rdin
g h
is o
r h
er
ph
ysi
olo
gic
al
sta
te,
wh
ich
ma
ny
en
ab
le v
olu
nta
ry c
on
tro
l ove
r a
uto
no
mic
bo
dy
fu
nct
ion
s e
.g.
he
art
rate
fe
ed
ba
ck i
n i
ncr
ea
sin
g p
hy
sica
l a
ctiv
ity
HW
B6
L3
A2
5
Dis
tra
ctio
n
Ide
nti
fy a
lte
rna
tiv
e f
ocu
s fo
r cl
ien
t’s
att
en
tio
n t
o a
void
att
en
tio
n t
o t
rig
ge
rs f
or
pro
ble
ma
tic
be
ha
vio
ur
an
d i
nst
ruct
on
usi
ng
in
pro
ble
ma
tic
situ
ati
on
s.
HW
B4
L3
A2
6
Ra
tio
na
l Em
oti
ve
Th
era
py
Te
ach
th
e c
lie
nt,
usi
ng
a v
ari
ety
of
cog
nit
ive
, e
mo
tive
an
d b
eh
av
iou
ral t
ech
niq
ue
s, t
o m
od
ify
an
d
rep
lace
se
lf-d
efe
ati
ng
th
ou
gh
ts t
o a
chie
ve
ne
w a
nd
mo
re e
ffe
ctiv
e w
ay
s o
f fe
eli
ng
an
d b
eh
av
ing
.
HW
B4
L3
A2
7
So
cia
l S
kil
ls T
rain
ing
T
ea
ch e
ffe
ctiv
e s
oci
al
inte
ract
ion
in
sp
eci
fic
situ
ati
on
s (e
.g.
job
in
terv
iew
s,),
ma
y in
clu
de
te
chn
iqu
es
such
as:
be
ha
vio
ur
reh
ea
rsa
l, c
og
nit
ive
re
he
ars
al,
an
d a
sse
rtiv
en
ess
tra
inin
g
HW
B4
L3
A2
8
(als
o P
37
)
Str
ess
In
ocu
lati
on
Pro
gra
m
Fo
r cl
ien
ts e
xpe
rie
nci
ng
str
ess
co
nsi
de
r u
sin
g S
tre
ss-I
no
cula
tio
n T
rain
ing
(S
IT):
A f
ou
r-p
ha
se
tra
inin
g p
rog
ram
fo
r st
ress
ma
na
ge
me
nt
oft
en
use
d i
n c
og
nit
ive
be
ha
vio
ur
the
rap
y.
HW
B4
L3
A2
9
(als
o P
37
)
An
ge
r C
on
tro
l
Tra
inin
g
A c
om
bin
ati
on
of
tech
niq
ue
s th
at
are
use
d t
o e
na
ble
th
e c
lie
nt
to c
on
tro
l an
ge
r
HW
B4
L3
A3
0
(als
o M
18
) A
sse
rtio
n T
rain
ing
A c
om
bin
ati
on
of
tech
niq
ue
s u
sed
to
te
ach
cli
en
t in
terp
ers
on
al
com
mu
nic
ati
on
to
he
lp t
he
m
exp
ress
em
oti
on
s, o
pin
ion
s, a
nd
pre
fere
nce
s –
po
siti
ve a
nd
ne
ga
tiv
e –
cle
arl
y,
dir
ect
ly,
an
d i
n a
n
ap
pro
pri
ate
ma
nn
er
HW
B4
L3
P
rom
pte
d o
r cu
ed
ro
ute
Lo
w I
nte
nsi
ty I
nte
rve
nti
on
s
P1
5
Mo
de
llin
g
Pro
mp
t o
bse
rva
tio
n o
f th
e b
eh
av
iou
r o
f o
the
rs
HW
B4
L3
P1
8
So
cia
l su
pp
ort
(in
stru
me
nta
l)
Pro
vid
e o
r a
rra
ng
e f
or
oth
ers
to
pe
rfo
rm c
om
po
ne
nt
task
s o
f b
eh
av
iou
r o
r ta
sks
tha
t w
ou
ld
com
pe
te w
ith
be
ha
vio
ur
(e.g
. o
ffe
rin
g c
hil
dca
re)
HW
B4
L3
P2
P
rom
pt
Ide
nti
fy a
sti
mu
lus
tha
t e
lici
ts b
eh
av
iou
r (i
nc.
te
lep
ho
ne
ca
lls
or
po
sta
l re
min
de
rs d
esi
gn
ed
to
pro
mp
t th
e b
eh
av
iou
r)
HW
B7
L3
M
ed
ium
In
ten
sity
In
terv
en
tio
ns
P3
C
on
tin
ge
nt
Re
wa
rd
Ide
nti
fy a
nd
pro
vid
e a
co
nti
ng
en
t v
alu
ed
co
nse
qu
en
ce o
f th
e t
arg
et
be
ha
vio
ur
if a
nd
on
ly i
f th
e
targ
et
be
ha
vio
ur
is p
erf
orm
ed
(re
wa
rds
can
in
clu
de
so
cia
l a
pp
rov
al)
HW
B7
L3

Pa
ge
| 3
5
P8
(a
lso
A1
1)
Gra
de
d t
ask
s S
et
ea
sy t
ask
s to
pe
rfo
rm,
ma
kin
g t
he
m i
ncr
ea
sin
gly
dif
ficu
lt u
nti
l ta
rge
t b
eh
av
iou
r is
pe
rfo
rme
d
HW
B7
L3
P1
6
Vic
ari
ou
s
rein
forc
em
en
t
Pro
mp
t o
bse
rva
tio
n o
f th
e c
on
seq
ue
nce
s o
f o
the
rs’
be
ha
vio
ur
HW
B4
L3
P2
1
En
vir
on
me
nta
l ch
an
ge
C
ha
ng
e t
he
en
vir
on
me
nt
in o
rde
r to
fa
cili
tate
th
e t
arg
et
be
ha
vio
ur
(oth
er
tha
n p
rom
pts
, re
wa
rds
an
d p
un
ish
me
nts
, e
.g.
cho
ice
of
foo
d p
rov
ide
d)
HW
B4
L3
P3
9
Tim
e O
ut
Mo
ve
th
e c
lie
nt
aw
ay
fro
m t
he
are
a t
ha
t is
re
info
rcin
g t
he
be
ha
vio
ur,
e.g
. in
stru
ct c
lie
nt
no
t to
go
into
th
e l
oca
l sh
op
fro
m w
hic
h t
he
y b
uy
th
eir
cig
are
tte
s H
WB
4L3
H
igh
In
ten
sity
In
terv
en
tio
ns
P1
D
iscr
imin
ati
ve
(le
arn
ed
) cu
e
Ide
nti
fy a
n e
nv
iro
nm
en
tal s
tim
ulu
s th
at
ha
s b
ee
n r
ep
ea
ted
ly a
sso
cia
ted
wit
h c
on
tin
ge
nt
rew
ard
fo
r
spe
cifi
ed
be
ha
vio
ur
HW
B7
L3
P4
P
un
ish
me
nt
Ide
nti
fy a
nd
pro
vid
e a
co
nti
ng
en
t a
vers
ive
co
nse
qu
en
ce,
if a
nd
on
ly i
f th
e b
eh
av
iou
r is
no
t
pe
rfo
rme
d
HW
B7
L3
P5
O
mis
sio
n
Ide
nti
fy a
nd
re
mo
ve a
co
nti
ng
en
t v
alu
ed
co
nse
qu
en
ce,
if a
nd
on
ly i
f th
e b
eh
av
iou
r is
no
t
pe
rfo
rme
d
HW
B7
L3
P6
N
eg
ati
ve
rein
forc
em
en
t
Ide
nti
fy a
nd
re
mo
ve a
n a
ve
rsiv
e c
on
seq
ue
nce
of
the
be
ha
vio
ur,
if
an
d o
nly
if
the
be
ha
vio
ur
is
pe
rfo
rme
d
HW
B7
L3
P7
T
hre
at
Off
er
futu
re p
un
ish
me
nt
or
rem
ov
al o
f re
wa
rd c
on
tin
ge
nt
on
pe
rfo
rma
nce
H
WB
7L3
P9
S
ha
pin
g
Bu
ild
up
be
ha
vio
ur
by
in
itia
lly
re
info
rcin
g b
eh
av
iou
r cl
ose
st t
o r
eq
uir
ed
be
ha
vio
ur
an
d
syst
em
ati
call
y a
lte
rin
g b
eh
av
iou
r re
qu
ire
d t
o a
chie
ve c
on
tin
ge
nt
rein
forc
em
en
t H
WB
7L3
P1
0
Ch
ain
ing
B
uil
d u
p b
eh
av
iou
r b
y s
tart
ing
wit
h f
ina
l co
mp
on
en
t; g
rad
ua
lly
ad
d c
om
po
ne
nts
ea
rlie
r in
se
qu
en
ce
HW
B7
L3
P1
1
(als
o A
13
) B
eh
av
iou
ral
reh
ea
rsa
l P
rov
ide
or
ide
nti
fy o
pp
ort
un
itie
s fo
r cl
ien
t to
pe
rfo
rm b
eh
av
iou
r re
pe
ate
dly
H
WB
7L3
P1
2
Me
nta
l re
he
ars
al
Pro
vid
e o
pp
ort
un
itie
s fo
r cl
ien
t to
ima
gin
e p
erf
orm
ing
th
e b
eh
av
iou
r re
pe
ate
dly
H
WB
7L3
P1
3
Ha
bit
fo
rma
tio
n
Pro
vid
e o
r id
en
tify
op
po
rtu
nit
ies
for
clie
nt
to p
erf
orm
sa
me
be
ha
vio
ur
in t
he
sa
me
co
nte
xt
rep
ea
ted
ly
HW
B7
L3
P1
4
(als
o A
14
) R
ole
pla
y P
rov
ide
op
po
rtu
nit
ies
for
clie
nt
to p
erf
orm
be
ha
vio
ur
in s
imu
late
d s
itu
ati
on
H
WB
7L3
P1
7
(als
o A
16
) Im
ag
ery
U
se p
lan
ne
d im
ag
es
(vis
ua
l, m
oto
r, s
en
sory
) to
im
ple
me
nt
be
ha
vio
ur
cha
ng
e t
ech
niq
ue
s (i
ncl
.
me
nta
l re
he
ars
al)
HW
B4
L3

Pa
ge
| 3
6
P1
9
De
sen
siti
sati
on
Id
en
tify
an
d p
rov
ide
exp
osu
re t
o t
hre
ate
nin
g e
xpe
rie
nce
s
HW
B7
L3
P2
0
Sy
ste
ma
tic
de
sen
siti
sati
on
Pro
vid
e g
rad
ed
exp
osu
re t
o i
ncr
ea
sin
gly
th
rea
ten
ing
exp
eri
en
ces
H
WB
7L3
P2
2
Dif
fere
nti
al
Re
info
rce
me
nt
Arr
an
ge
fo
r re
info
rce
me
nt
of
on
ly s
ele
cte
d b
eh
av
iou
r (e
.g.
pro
vid
e r
ew
ard
of
con
sum
pti
on
of
low
fat
foo
ds
bu
t n
ot
con
sum
pti
on
of
hig
h f
at
foo
ds)
HW
B7
L3
P2
3
Esc
ap
e L
ea
rnin
g
Arr
an
ge
fo
r th
e t
erm
ina
tio
n o
f a
n a
ve
rsiv
e s
tim
ulu
s T
he
pri
nci
ple
is
ide
nti
cal
to t
ha
t o
f n
eg
ati
ve
rein
forc
em
en
t H
WB
7L3
P2
4
Ext
inct
ion
D
isco
nti
nu
e r
ein
forc
em
en
t o
f ta
rge
t b
eh
av
iou
r e
.g.
red
uce
am
ou
nt
of
soci
al
att
en
tio
n t
o s
mo
kin
g
be
ha
vio
urs
H
WB
7L3
P2
5
Flo
od
ing
Exp
ose
cli
en
t d
ire
ctly
to
a m
axi
mu
m-i
nte
nsi
ty a
nxi
ety
-pro
vok
ing
sit
ua
tio
n o
r st
imu
lus,
eit
he
r in
th
e
ima
gin
ati
on
or
in r
ea
lity
. F
loo
din
g t
ech
niq
ue
s a
im t
o r
ed
uce
an
xie
ty t
ha
t is
in
terf
eri
ng
wit
h d
esi
red
be
ha
vio
ur
e.g
. ta
kin
g c
lie
nt
to a
gym
to
ov
erc
om
e a
nxi
ety
ab
ou
t e
ng
ag
ing
in
ph
ysi
cal
act
ivit
y
HW
B7
L3
P2
7
Co
un
ter-
con
dit
ion
ing
Re
wa
rd c
lie
nt
for
resp
on
din
g t
o a
sti
mu
lus
in a
ma
nn
er
tha
t is
in
com
pa
tib
le w
ith
th
eir
pre
vio
us
resp
on
se t
o t
ha
t st
imu
lus,
(e
.g.
rew
ard
cli
en
t fo
r o
rde
rin
g a
so
ft d
rin
k w
he
n t
he
y f
irst
go
to
th
e b
ar
rath
er
tha
n a
n a
lco
ho
lic
dri
nk
)
HW
B7
L3
P2
8
Exp
osu
re
Pro
vid
e s
yst
em
ati
c co
nfr
on
tati
on
wit
h a
fe
are
d s
tim
ulu
s, e
.g.
a p
eri
od
of
wit
hd
raw
al
fro
m n
ico
tin
e
for
a c
lie
nt
wh
o w
an
ts t
o s
top
sm
ok
ing
, e
ith
er
live
or
in t
he
ima
gin
ati
on
(m
ay
en
com
pa
ss a
ny
of
a
nu
mb
er
of
be
ha
vio
ura
l in
terv
en
tio
ns,
in
clu
din
g s
yste
ma
tic
de
sen
siti
zati
on
, fl
oo
din
g,
imp
losi
ve
the
rap
y a
nd
ext
inct
ion
-ba
sed
te
chn
iqu
es)
HW
B7
L3
P2
9
Fa
din
g
Pro
vid
e a
gra
du
al
cha
ng
ing
of
on
e s
tim
ulu
s to
an
oth
er
(oft
en
use
d t
o t
ran
sfe
r st
imu
lus
con
tro
l).
Sti
mu
li c
an
be
fa
de
d o
ut
or
fad
ed
in
, e
.g.
gra
du
ally
in
cre
asi
ng
th
e r
an
ge
of
foo
ds
off
ere
d t
o a
clie
nt
wh
o i
s tr
yin
g t
o c
ho
ose
he
alt
hy
fo
od
s
HW
B7
L3
P3
0
Th
inn
ing
P
rov
ide
a g
rad
ua
l in
cre
ase
in t
he
in
term
itte
ncy
of
rein
forc
em
en
t, (
e.g
. g
rad
ua
lly
in
cre
ase
th
e t
ime
be
twe
en
re
wa
rds)
H
WB
7L3
P3
1
Ha
bit
re
vers
al
Pro
vid
e o
pp
ort
un
itie
s fo
r re
pe
ate
d r
eh
ea
rsa
l of
a n
ew
co
rre
ct r
esp
on
se t
o a
sti
mu
lus
an
d s
top
resp
on
din
g t
o a
pre
vio
usl
y le
arn
ed
cu
e,
(e.g
. cl
ien
t re
spo
nd
s to
a m
orn
ing
co
ffe
e b
rea
k b
y e
ati
ng
a
pie
ce o
f fr
uit
in
ste
ad
of
a p
iece
of
cho
cola
te)
HW
B7
L3
P3
2
Ne
ga
tiv
e p
un
ish
me
nt
Re
mo
ve
a r
ew
ard
as
a c
on
seq
ue
nce
of
a r
esp
on
se.
(e.g
., s
ub
tra
ct m
on
ey
fro
m a
pre
pa
id r
efu
nd
ab
le
de
po
sit
wh
en
clie
nt
smo
ke
s a
cig
are
tte
.
HW
B7
L3

Pa
ge
| 3
7
P3
3
No
nco
nti
ng
en
t
rein
forc
em
en
t
Pro
vid
e a
re
wa
rd i
nd
ep
en
de
ntl
y o
f a
ny
pa
rtic
ula
r ta
rge
t b
eh
av
iou
r.
HW
B7
L3
P3
4
Ov
erc
orr
ect
ion
W
he
n a
clie
nt
exh
ibit
s in
ap
pro
pri
ate
be
ha
vio
ur
ask
th
e c
lie
nt
to r
ep
ea
t th
e b
eh
av
iou
r in
an
ap
pro
pri
ate
bu
t e
xag
ge
rate
d w
ay
HW
B7
L3
P3
6
Re
spo
nse
co
st
Wit
hd
raw
a v
alu
ed
co
mm
od
ity
fro
m t
he
cli
en
t a
s a
re
sult
of
the
ir p
erf
orm
ing
an
un
wa
nte
d
be
ha
vio
ur,
e.g
. lo
ss o
f a
cce
ss t
o d
esi
red
act
ivit
y e
.g 1
hr
of
TV
vie
win
g f
or
ea
ch i
na
pp
rop
ria
te
be
ha
vio
ur
HW
B7
L3
P4
7
Sti
mu
lus
Ge
ne
rali
zati
on
Gu
ide
cli
en
t to
sp
rea
d o
f e
ffe
cts
of
lea
rnin
g a
be
ha
vio
ur
in o
ne
sit
ua
tio
n t
o o
the
r si
mil
ar
situ
ati
on
s
e.g
. e
xerc
ise
s le
arn
ed
in
gym
re
pe
ate
d w
he
n w
ea
rin
g in
form
al c
loth
es
HW
B7
L3
P3
7
Sa
tia
tio
n
Exp
ose
th
e c
lie
nt
to r
ep
ea
ted
exp
osu
re t
o a
re
info
rce
r e
.g.
cho
cola
te,
in o
rde
r to
re
du
ce i
ts
eff
ect
ive
ne
ss o
f a
re
info
rce
H
WB
7L3
P4
0
To
ken
Eco
no
my
Re
info
rce
th
e d
esi
red
be
ha
vio
ur
by
off
eri
ng
to
ken
s th
at
can
be
exc
ha
ng
ed
fo
r sp
eci
al
foo
ds,
tele
vis
ion
tim
e,
pa
sse
s, o
r o
the
r re
wa
rds
HW
B7
L3
P4
2
Cla
ssic
al
Co
nd
itio
nin
g
Pre
sen
t a
ne
utr
al
stim
ulu
s jo
intl
y w
ith
a s
tim
ulu
s th
at
alr
ea
dy
eli
cits
a r
esp
on
se r
ep
ea
ted
ly u
nti
l th
e
ne
utr
al
stim
ulu
s e
lici
ts t
ha
t re
spo
nse
(P
av
lov
ian
Co
nd
itio
nin
g)
e.g
. re
pe
ate
dly
pa
irin
g f
att
y f
oo
ds
wit
h a
dis
like
d f
lav
ou
red
sa
uce
HW
B7
L3
P4
3
Co
vert
Co
nd
itio
nin
g
Pro
vid
e o
pp
ort
un
itie
s fo
r cl
ien
t to
ima
gin
e p
erf
orm
ing
a d
esi
red
be
ha
vio
ur
in a
pro
ble
ma
tic
rea
l-
life
sit
ua
tio
n,
an
d t
o r
ew
ard
him
self
or
he
rse
lf f
or
me
nta
lly
en
ga
gin
g i
n t
he
be
ha
vio
ur.
A
lso
ca
lle
d
cove
rt b
eh
av
iou
ral
rein
forc
em
en
t
HW
B7
L3
P4
4
Co
vert
Se
nsi
tiza
tio
n
Pro
vid
e o
pp
ort
un
itie
s fo
r cl
ien
t to
ima
gin
e p
erf
orm
ing
th
e u
nd
esi
red
be
ha
vio
ur
(e.g
. o
ve
rea
tin
g)
an
d t
he
n i
ma
gin
e a
n u
np
lea
san
t co
nse
qu
en
ce (
e.g
. v
om
itin
g)
HW
B7
L3
P4
5
Dis
crim
ina
tio
n
Tra
inin
g
Re
wa
rd t
he
be
ha
vio
ur
in o
ne
sit
ua
tio
n b
ut
no
t in
an
oth
er
(e.g
. re
wa
rd f
or
ea
tin
g s
we
et
foo
ds
at
me
alt
ime
s b
ut
no
t b
etw
ee
n m
ea
ls
HW
B7
L3
P4
6
Em
eti
c T
he
rap
y P
rov
ide
cli
en
t w
ith
dru
gs
tha
t p
rod
uce
ave
rsiv
e s
ide
eff
ect
s w
he
n c
om
bin
ed
wit
h p
rob
lem
e.g
. th
e
use
of
An
tab
use
in
re
du
cin
g a
lco
ho
lism
H
WB
7L3
P3
8
(als
o A
28
)
Str
ess
In
ocu
lati
on
Pro
gra
m
Fo
r cl
ien
ts e
xpe
rie
nci
ng
str
ess
co
nsi
de
r u
sin
g S
tre
ss-I
no
cula
tio
n T
rain
ing
(S
IT)
HW
B4
L3
P4
1
(als
o A
29
)
An
ge
r C
on
tro
l
Tra
inin
g
A c
om
bin
ati
on
of
tech
niq
ue
s th
at
are
use
d t
o e
na
ble
th
e c
lie
nt
to c
on
tro
l an
ge
r (e
.g.
a c
lie
nt
wh
o
use
s a
lco
ho
l in
re
spo
nse
to
an
ge
r m
igh
t b
e t
rain
ed
to
co
ntr
ol
an
ge
r in
ord
er
to r
ed
uce
alc
oh
ol
con
sum
pti
on
.)
HW
B4
L3

Pa
ge
| 3
8
P2
6
Imp
losi
ve
Th
era
py
Re
pe
ate
dly
en
cou
rag
e c
lie
nt
to i
ma
gin
e a
n a
nxi
ety
-aro
usi
ng
sit
ua
tio
n,
an
d t
o e
xpe
rie
nce
an
xie
ty a
s
inte
nse
ly a
s p
oss
ible
wh
ile
do
ing
so
. S
ince
th
ere
is
no
act
ua
l d
an
ge
r in
th
e s
itu
ati
on
, th
e a
nxi
ety
resp
on
se i
s n
ot
rein
forc
ed
an
d t
he
refo
re i
s g
rad
ua
lly
ext
ing
uis
he
d
HW
B7
L3
P3
5
Ra
tio
na
l Em
oti
ve
Th
era
py
Te
ach
th
e c
lie
nt,
usi
ng
a v
ari
ety
of
cog
nit
ive
, e
mo
tive
an
d b
eh
av
iou
ral t
ech
niq
ue
s, t
o m
od
ify
an
d
rep
lace
se
lf-d
efe
ati
ng
th
ou
gh
ts t
o a
chie
ve
ne
w a
nd
mo
re e
ffe
ctiv
e w
ay
s o
f fe
eli
ng
an
d b
eh
av
ing
. In
the
pro
cess
th
e i
rra
tio
na
l b
eli
efs
an
d f
ee
lin
gs
are
fir
st u
nm
ask
ed
th
en
alt
ere
d b
y
HW
B4
L3
aco
de
nu
mb
er
for
BC
T t
ak
en
fro
m t
he
Ge
ne
ric
He
alt
h B
eh
avio
ur
Ch
an
ge
Co
mp
ete
ncy
Fra
me
wo
rk.
M=
mo
tiva
tio
n d
ev
elo
pm
en
t ro
ute
; A
=a
ctio
n o
n
mo
tiv
ati
on
ro
ute
; P
=p
rom
pte
d o
r cu
ed
ro
ute
KS
F n
ota
tio
n a
s fo
llow
s: C
=co
re d
ime
nsi
on
; H
WB
=h
ea
lth
an
d w
ell
be
ing
dim
en
sio
n;
IK=
info
rma
tio
n a
nd
kn
ow
led
ge
dim
en
sio
n.
Th
e f
irst
nu
mb
er
refe
rs t
o
the
su
b-d
ime
nsi
on
wit
hin
th
at
dim
en
sio
n.
L=
lev
el o
f co
mp
ete
nce
. T
he
se
con
d n
um
be
r re
fers
to
th
e le
vel o
f co
mp
ete
nce
. F
or
exa
mp
le:
HW
B4
L3 d
en
ote
s
KS
F H
ea
lth
an
d W
ell
be
ing
Dim
en
sio
n,
sub
-dim
en
sio
n 4
(e
na
ble
me
nt
to a
dd
ress
he
alt
h a
nd
we
llb
ein
g n
ee
ds)
, le
ve
l of
com
pe
ten
ce 3
.
Su
mm
ary
of
the
HB
CC
Co
mp
ete
ncy
To
pic
s M
atc
he
d t
o K
SF
Co
mp
ete
ncy
Dim
en
sio
ns
KS
F D
ime
nsi
on
(su
b-d
ime
nsi
on
) H
BC
C C
om
pe
ten
cy T
op
ics
Fo
un
da
tio
n
Be
ha
vio
ur
Ch
an
ge
B
CT
Ro
ute
Co
re D
ime
nsi
on
Co
mm
un
ica
tio
n
F1
- F
10
B
C2
, B
C7
, B
C8
, B
C1
0,
BC
11
n
a
Pe
rso
na
l &
pe
op
le d
eve
lop
me
nt
F2
n
a
na
Se
rvic
e i
mp
rov
em
en
t F
1,
F2
n
a
na
Qu
ali
ty
F1
n
a
na
Eq
ua
lity
& d
ive
rsit
y
F3
n
a
na
He
alt
h &
We
llb
ein
g D
ime
nsi
on
Pro
tect
ion
of
he
alt
h &
we
llb
ein
g
F1
n
a
na
En
ab
lem
en
t to
ad
dre
ss h
ea
lth
& w
ell
be
ing
ne
ed
s F
8
BC
4,
BC
7,
BC
8,
BC
10
M
, A
, P
Ass
ess
me
nt
& t
rea
tme
nt
pla
nn
ing
F
12
B
C1
-BC
3,
BC
5,
BC
6,
BC
8-
BC
11
M
, A
Inte
rve
nti
on
s &
tre
atm
en
ts
F3
, F
7-
F1
1
BC
1,
BC
4,
BC
5,
BC
6-
BC
10
, B
C1
2
P
Info
rma
tio
n &
Kn
ow
led
ge
Dim
en
sio
n
Info
rma
tio
n c
oll
ect
ion
& a
na
lysi
s F
1
na
n
a
Kn
ow
led
ge
& i
nfo
rma
tio
n r
eso
urc
es
F2
n
a
na
na
= K
SF
su
b-d
ime
nsi
on
no
t a
pp
lica
ble
to
th
is H
BC
C c
om
pe
ten
cy d
om
ain
. M
= B
CT
to
de
ve
lop
mo
tiv
ati
on
fo
r ch
an
ge
, A
= B
CT
to
en
ab
le a
ctio
n o
n m
oti
va
tio
n,
P=
BC
T t
o p
rom
pt
or
cue
be
ha
vio
ur

P a g e | 39
Appendix 2 Competences described in Alcohol Brief Interventions: Training Manual
NHS Health Scotland, 2009
The table below lists the HBCC competency topics described in NHS Health Scotland’s
training manual for ABIs. The behaviour change techniques (BCTs) described in the training
manual are listed according to the route(s) to behaviour change targeted by each BCT
(Motivation development route; Action on motivation route, Prompted or cued route to
change). The content of each ABI training unit is described in detail on the pages that follow
the table below.
Training Unit
HBCC competency used in each ABI training unita
Foundation
Topics
Behaviour Change
Topics
behaviour change technique
(route to behaviour change)
M A P
1. Brief interventions:
what and why
BC1; BC3
2. Attitudes to
alcohol
F3; F12 BC1
3. Barriers and
concerns
F1; F5; F12 BC3
4. Brief intervention
observation
F5; F7; F10 BC2; BC3; BC4; BC6;
BC7; BC8; BC9; BC12
M1; M2; M10;
M12; M13;
M14; M15;
M16; M17
A5; A6;
A9, A17;
A21; A22
5. Units and drinking
limits
BC1; BC9
6. Raising the issue of
alcohol
F5 BC1; BC9
7. Screening and
feedback
F3; F5; F10 BC1; BC2; BC7; BC8;
BC9
M5 A6
8. Referral: when,
where and how?
F1; F10 BC2; BC9
9. Brief interventions
delivery: key skills
F5; F7; F10 BC2; BC6; BC7; BC8;
BC9; BC10; BC12
M1; M2; M10;
M11; M12;
M14; M16;
M15; M17;
M18; M20
A1; A3;
A4; A5;
A6; A8;
A9; A10;
A13; A17;
A21; A25;
A28
P3;
P15;
P21
10. Brief interventions
delivery: putting it
all together
competences not described in detail in the training manual
afor foundation and behaviour change domains, competences are matched at the level of competency topic, it
is not necessarily the case that all individual competences within a topic are described in a training unit

P a g e | 40
Competences described in Alcohol Brief Interventions: Training Manual NHS Health
Scotland, 2009
Unit 1: Brief Interventions: what and why (20mins)
This unit is an information giving session. Data pertaining to alcohol as a public
health problem are presented and the nature of and evidence base for ABIs are
detailed. This unit delivers information relevant to two behaviour change
competency topics: BC1 (health behaviour and health behaviour problems) and
BC3 (knowledge of a model of behaviour change and the ability to understand and
employ the model in practice).
Unit 2: Attitudes to alcohol (45mins)
This unit delivers information and employs a practical session to enable trainees
to elicit and understand their own attitudes to alcohol consumption and a debrief
session to reinforce the practical session. The unit is primarily focussed on the
attitudes of the trainees to alcohol but the unit does suggest this is an opportunity
to discuss misinformation about alcohol, stereotypes associated with alcohol and
population subgroups, including different cultures. As a consequence, this unit is
an important training opportunity in relation to foundation competency F3
(knowledge of and ability to work with difference), which underpins the ability to
deliver interventions equitably to different types of clients, e.g. gender, religion,
age, deprivation, ethnicity and sexuality. Competency topic F12 (barriers to and
facilitators of implementing interventions) is also an important component of this
unit, as is behaviour change topic BC1 (health behaviour and health behaviour
problems).
Potential for development of Unit 2: this unit could include information about
alcohol and different sections of the community as a core component to ensure
the use of alcohol in relation to different groups, e.g. gender, religion, age,
deprivation, ethnicity, sexuality, is always covered by the training.
Unit 3: Barriers and concerns (40mins)
This unit enables trainees to express and discuss their concerns about and identify
possible barriers to delivering ABIs as part of their routine practice. The aim
appears to be to promote and generate positive beliefs towards ABIs within the
trainees. The unit elicits four types of beliefs: beliefs about role legitimacy, role
adequacy, role support and the trainee’s motivation to deliver ABIs. As such it
potentially covers all competences within competency topic F12 (barriers to and
facilitators of implementing interventions). In addition, it addresses professional
issues such as confidentiality within practice and knowledge of referral to other
services, both of which are covered by competences within foundation
competency topic F1 (professional and ethical guidelines).
Unit 4: Brief intervention observation (40mins +)
Video clips are used to illustrate three important skills required for the delivery of
an ABI: establishing rapport and an empathic approach, emphasising personal
responsibility, and listening for readiness to change. These competences are
described in foundation competency topics F5 (ability to engage client) and F7

P a g e | 41
(ability to foster and maintain a good intervention alliance, and to grasp the
client’s perspective). This unit also introduces and discusses the theoretical
framework used by the training programme, namely the Stages of Change or
trans-theoretical model. As such this unit addresses behaviour change
competency topic BC3 (knowledge of a model of behaviour change and the ability
to understand and employ the model in practice).
Potential for development of Unit 4: Knowledge of Behaviour Change Theory
The Stages of Change Model provides the theoretical model of behaviour change.
The training model describes the Model in full. There are two potential problems
with this approach: i). the Stages of Change model does not reflect current
models of behaviour change; ii). the Stages of Change Model, as described in the
training manual, presents information to trainees that they will not use in their
practice. As a consequence, there is an opportunity to improve the presentation
of behaviour theory within ABI training. First, behaviour theory now highlights
two pathways to behaviour. One is a conscious path that generates behaviour
through the development of motivation and enabling action on motivation. The
other path is more automatic and recognises a role for the environment, both
physical and social, and a role for emotional factors in the generation of
behaviour. These two pathways are encompassed by the MAP of behaviour
change used in the HBCC. Therefore, the MAP provides a simplified, but more
comprehensive, model of behaviour for training for brief interventions. Second,
the MAP is a closer match to the practical delivery of ABIs. It is likely that MAP
would provide trainees with a theory based structure to guide their practice.
Further, the MAP might give trainees a better understanding of the prompted or
cued route to behaviour change.
Unit 5: Units and drinking limits (40mins)
This unit focuses on measurement of alcohol consumption and national guidance
on alcohol limits for different groups. It addresses the behaviour change
competency topics BC9 (ability to use measures and self-monitoring to guide
behaviour change interventions and to monitor outcome) and BC1 (health
behaviour and health behaviour problems)
Unit 6: Raising the issue of alcohol (30mins)
Competences described in foundation competence topic F5 (ability to engage
client) are core to this unit. In addition, competences in relation to understanding
issues and illnesses associated with alcohol consumption are also delivered in this
unit. These competences are described in behaviour change competency topic
BC1 (health behaviour and health behaviour problems).
Unit 7: Screening and feedback (60mins)
This unit delivers information and uses role play to enable trainees to experience
the screening for an ABI from the perspective of the practitioner and the client. It
involves skills in relation to client assessment and the measurement of their
alcohol consumption, which are addresses by behaviour competency topics BC2
(ability to undertake a generic assessment) and BC9 (ability to use measures and
self-monitoring to guide behaviour change interventions and to monitor outcome).
In addition, this unit describes competences in relation to the ability to engage a
client, including the ability to work with different populations and to deliver

P a g e | 42
information effectively. These competences are contained within three
foundation topics F3 (knowledge of and ability to work with difference), F5 (ability
to engage client) and F10 (ability to deliver information).
Unit 8: Referral: when, where and how? (15mins)
This unit focuses on how to identify and respond to clients with possible alcohol
dependence. As such it describes competences required for screening in relation
to dependence and suitability for an ABI. These competences are described in
behaviour change topics BC2 (ability to undertake a generic assessment) and BC9
(ability to use measures and self-monitoring to guide behaviour change
interventions and to monitor outcome). These assessment and measurement
competences are complemented by knowledge about local referral pathways and
additional resources available for clients, which are described in foundation
competences F1 (professional and ethical guidelines) and F10 (ability to deliver
information).
Unit 9: Brief intervention delivery: key skills (150mins)
This unit identifies key components of ABIs and how practitioners can identify the
most appropriate brief intervention approach for each client. It brings together
the information gained from units 5, 6 and 7 and builds on these units to identify
behaviour change techniques relevant to the client’s stage of change. The focus is
on generic communication skills, provision of information following measurement
of client alcohol consumption, enhancing motivation and building confidence in
ability to change. As a consequence this unit described multiple competences
from the HBCC. The foundation competency topics F7 (ability to foster and
maintain a good intervention alliance, and to grasp the client’s perspective) and
F10 (ability to deliver information) are central to this unit. Multiple behaviour
change competency topics are described in this unit, including BC2 (ability to
undertake a generic assessment), BC6 (capacity to select and skillfully apply the
most appropriate behaviour change intervention method), BC8 (ability to structure
consultations), BC9 (ability to use measures and self-monitoring to guide
behaviour change interventions and to monitor outcome), BC10 (health behaviour
problem solving) and BC12 (ability to end the intervention in a planned manner
and to plan for long-term maintenance of gains after intervention ends). This unit
is the first to describe behaviour change techniques (BCTs) in any detail. Multiple
BCTs are described, the majority of which are aimed at the motivation
development and action on motivation routes to behaviour change. Client
motivation to change is developed using techniques from motivational
interviewing (BCT M15: motivational interviewing), including listing positive and
negative aspects of alcohol consumption (BCT M1 and A4: record antecedents and
consequences of behaviour). Motivated clients are helped to translate that
motivation into action primarily through action (BCT A1: identify and set a
behavioural goal) and coping planning (BCT A9: identify and plan ways of
overcoming barriers).
Potential for development of Unit 9: Using Behaviour Change Theory to Support
Practice
Unit 9 describes numerous BCTs. Trainees’ practice might benefit from an
understanding of how these techniques influence behaviour. For example, the

P a g e | 43
BCT of Action Planning is underpinned by a general principle that plans are more
effective if the plan details when, where and what behaviour will be performed.
For example, a client who wants to reduce their alcohol consumption might make
the following action plan: I will drink a soft drink between alcoholic drinks, when
I am out with my friends in the pub on Saturday night. The current training
manual tends to describe lots of behaviours that, if enacted, would reduce alcohol
consumption, e.g. drink soft drinks, avoid rounds, put my glass down between
sips. However, these behaviours are more likely to be performed if they are part
of an action plan, i.e. part of a plan that details when and where the behaviour
will be performed. Providing trainees with an understanding of these theory-
based, general principles of behaviour change is likely to result in improved
outcomes.
Unit 10: Brief interventions delivery: putting it all together (135mins)
This unit provides trainees with an opportunity to practice delivering an ABI based
on their own case studies. As a consequence the training manual does not
describe any specific competences within Unit 10. However, it can be anticipated
that trainees will employ the majority of competences delivered in the earlier
units. Precisely which competences are used by trainees in this Unit will depend
on the nature of the case studies described by the trainees to be used to practice
delivering ABIs. Unit 10 also includes a reflective practice log in which each
trainee records details of occasions on which they delivered an ABI and what
components of the ABI were delivered. This reflective practice log is likely to be
very useful. Feedback from practitioners and trainers in response to the GHBC-CF
highlighted the need to ensure that trainees were supported to implement their
training within their usual practice. A reflective practice log might work to
support the implementation of the ABI training.

P a g e | 44
Appendix 3 How the Framework was Developed
The HBCC is based on the Generic Health Behaviour Change: A Comprehensive Competency
Framework (GHBC-CF). The competences within the GHBC-CF were identified by examining
the published evidence base.
Several sources of information were consulted.
• Relevant professional competency frameworks
• Systematic reviews of interventions for behaviour change
• Manuals for behaviour change interventions
• NHS and Health Scotland Skills for Health and competency frameworks for alcohol
brief interventions
The competency framework for the delivery of cognitive behaviour therapy13
was identified
as the professional competency framework of most relevance for the delivery of health
behaviour change as; a) it describes competencies for delivery of personal change
interventions and, b) it is a clear, well-developed framework. This framework was adapted
to provide a framework for generic health behaviour change. An iterative process of
adaptation was employed. Other relevant documentation (detailed below) was analysed in
relation to the existing competency framework. These analyses enabled the framework to
be modified to exclude irrelevant competencies and to include health behaviour change
specific competencies.
Of particular importance was the need to identify specific behaviour change techniques to
be included in the GHBC competency framework as these did not form any part of the
competency framework for cognitive behavioural therapy. The most comprehensive review
of specific behaviour change techniques was included in the analyses14
. The GHBC-CF
identified 89 behaviour change techniques, from that review, which were of potential
relevance to health behaviour change. In order to make such a large number of techniques
usable by and useful for policy makers, managers and frontline staff, we mapped each
technique to one or more of three identified routes to behaviour change, namely,
motivation development, action on motivation, prompted or cued behaviour.
Feedback on the GHBC-CF The GHBC-CF was presented to representatives from:
• Health Improvement Strategy Division
• NHS Health Scotland
• NHS Education Scotland
and at meetings:
• British Psychological Society, Division of Health Psychology-Scotland, annual research
meeting
13
Roth AD, Pilling S. The competencies required to deliver effective cognitive behavioural therapy for
people with depression and anxiety disorders. Improving Access to Psychological Therapies (IAPT)
Programme. London: Department of Health, 2007. 14
Michie M, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping
theoretically derived behavioural determinants to behaviour change techniques. Applied Psychology: An
International Review 2008;57(4):660-80.

P a g e | 45
• Health Scotland: Helping People Change launch event for this new web-based
resource
Feedback was very positive but three issues were highlighted:
1. The GHBC-CF contained language that was considered too technical and a request was
made to revise the GHBC-CF using non-technical language throughout
2. Feedback requested we order the competences into a hierarchy, which would identify
the competences required at different levels of working
3. Colleagues suggested that it would be useful to map the GHBC-CF to the competences
described in relevant dimensions of the Knowledge and Skills Framework.
Use of Non-technical language We have attempted to use lay language wherever possible. Whilst this report has been
written in lay language it has been necessary to retain some technical terminology in the
descriptions of the behaviour change techniques. However, an understanding of this
terminology is not required to understand this report and each technical term used to label
a behaviour change technique is accompanied by a description in the vernacular.
Establishing a Competency Hierarchy The request to develop a hierarchy within the GHBC-CF was addressed by our collegiate
network. Colleagues, who were all chartered psychologists (health and/or clinical),
identified competences required to deliver low, medium, and high intensity health
behaviour change interventions. The hierarchy within the HBCC framework is based on
intensity of intervention15
rather than on the nine career framework levels described in
Skills for Health. The Skills for Health career framework was not adopted as we could not
reliably identify the job titles currently tasked with delivering health behaviour change nor is
there an established career structure for health behaviour change. As a consequence we
adopted a level of intervention approach and described the competences required to
deliver interventions at each level.
Mapping the HBCC Framework to the Knowledge and Skills Framework (KSF) Each competency described in the HBCC was compared to the indicators and descriptors of
each competency dimension described in the KSF. This process identified the competency
dimension(s) and level of competency within a KSF dimension that was the best match to
each HBCC competency.
Identifying Competences in Current Training Programmes for Health Behaviour
Change In addition, we have used the HBCC to identify the competences described in NHS Health
Scotland’s training manual for the delivery of alcohol brief interventions in Scotland. A
standard method16
of identifying competences for behaviour change was applied to NHS
Health Scotland’s Alcohol Brief Interventions: Training Manual (2009). Competences
identified within the Training Manual were mapped to competency topics and behaviour
change techniques within the HBCC.
15
The levels of intervention were informed by The matrix: a guide to delivering evidence based psychological therapies
in Scotland, December 2008. 16
Abraham, C. and S. Michie (2008). A Taxonomy of Behavior Change Techniques Used in Interventions. Health
Psychology 27(3): 379-387. Michie, S., S. Churchill, et al. (in press). Identifying evidence-based competences required
to deliver individual and group-based behavioural support for smoking cessation. Annals of Behavioral Medicine.