
Health behaviour change among users of NHS Health Trainer Services Benjamin Gardner 1, James Cane 1,...
19
Health behaviour change among users of NHS Health Trainer Services Benjamin Gardner 1 , James Cane 1 , Nichola Rumsey 2 & Susan Michie 1 1: University College London; 2: University of the West of England 3 rd July 2012
-
Upload
gwendolyn-sherman -
Category
Documents
-
view
220 -
download
0
Transcript of Health behaviour change among users of NHS Health Trainer Services Benjamin Gardner 1, James Cane 1,...

Health behaviour change among users of NHS Health Trainer Services
Benjamin Gardner1,
James Cane1, Nichola Rumsey2 & Susan Michie1
1: University College London; 2: University of the West of England
3rd July 2012

This work was undertaken as part
of a BPS DHP consultancy to the
Department of Health
(2003-2010)
Evaluations of the NHS Health Trainer Service
• 2007-09: data from hub leads (‘hub reports’)• Yearly audits of workforce and clients
– Who are the HTs?– Is the workforce growing?– Who is using the HT service? (Wilkinson et al, 2007; D Smith et al, 2008)
• 2009: DCRS data• Evaluation of service effectiveness• Does behaviour change among users of the HT
service?

Questions
1) Who uses the HT service?- Are we reaching ‘hard to reach’ clients?
2) Does (diet and activity) behaviour change following use of HT service?
3) Do all clients benefit equally?

Data
• Drawn from DCRS– Period: 1st April 2008 – 31st March 2009– Data extracted from DCRS v2.4 by BPCSSA
• Final extraction for DCRS report: December 2009• Final extraction for paper mid-2010
– Data recording on DCRS then non-compulsory• At start of time period, estimated from hub report that 62% of
HTSs entered data into DCRS
• Paper accepted for publication in Dec 2011
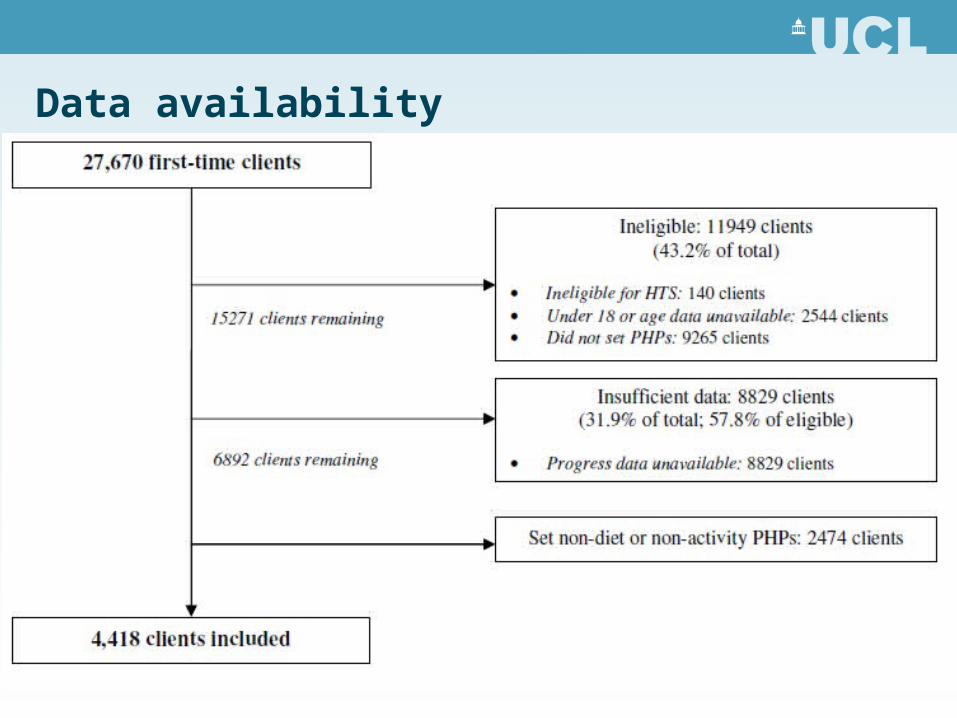
Data availability
Drop-out bias?
• Setting PHPs:– White clients (35%) and Asian clients (30%) more likely to set PHPs
than Black clients (25%)– More PHPs set in least deprived quintile (42%) than others (~36%)
• Pre-post HTS data availability:– White clients (35%) more likely to have pre-post than Asian (30%) or
Black clients (27%)– More data available in least deprived quintile (45%) than others
(~29%)

MeasuresPre- and post-HTS
- Baseline demographics
- Pre- and post-HTS:• Behaviour measures
– BMI (height, weight)– Self-reported behaviour (diet [snacks, fruit & veg],
activity [moderate/intensive sessions])

Results1) Who uses the HTS?
• 3503 female (79%) (UK population, 2001 = 51% female)
• Typical age 36-45 years (22.4%) (UK 2001 = 19%)
• Deprivation:– Q1 (most deprived): 1836 (43.2%)– Q2 1093 (25.7%)– Q3 688 (16.2%)– Q4 405 (9.5%)– Q5 (least deprived) 230 (5.4%)

Results1) Who uses the HTS?
• Ethnicity: (UK 2001 = 93% White)
– White 3647 (83.2%) – Asian 485 (11.1%) – Black 175 (4.0%) – Mixed or other 79 (1.8%)
Results1) Who uses the HTS – and for what purpose?
• Weight status:– Obese 2717 (72.3%)– Overweight 824 (22.4%)– Normal weight 218 (5.8%)
• PHP focus:– Diet 3346 (75.7%)– Physical activity 1072 (24.3%)

Results2) Diet change following diet PHP achievement
Outcome Number of clients
Pre-HTS mean
Post-HTS mean
% change
Daily fruit & veg
(portions)
2376 3.08 5.23 70% increase
No. of daily fried snacks
1869 1.99 0.79 60% decrease
BMI 3164 34.33 32.45 6% decrease

Results2) Activity change following activity PHP achievement
Outcome N Pre-HTS mean
Post-HTS mean
% change
Weekly moderate sessions
921 3.06 4.77 56% increase
Weekly intensive sessions
637 0.63 1.71 171% increase
BMI 595 32.46 31.24 4% decrease

3) Do all clients benefit equally?
• Ethnicity or deprivation differences?– All clients
• Deprivation & BMI:– Less BMI reduction in most deprived quintile vs all others (0.28 BMI points)
– Diet:• Deprivation & BMI:
– Less BMI reduction in most deprived quintile vs all others (0.24 BMI points)
• Ethnicity & BMI:– Less BMI reduction in Asian versus White clients (0.55 BMI points)

Conclusions
• HTS is reaching disadvantaged clients and changing behaviour
• Effects similar across demographic groups– But more PHPs set and more data recorded in less
deprived groups

Challenges and recommendations
• Missing data problematic– Pre- and post-HTS behaviour data essential
• Reliance on self-report– May overestimate behaviour change
– Ideally need objective measures, e.g. biochemical verification, objectively measured weight
• Whether data self-report or objective should be recorded
Challenges and recommendations
• Need to ensure continued fidelity to HTS as originally devised
• Qualitative data needed– Quantitative data allows for ‘birds eye view’ group-level
analyses– Qualitative data engages with contextualised individual
experiences– Would reveal ‘real-life’ benefits of HTS

Challenges and recommendations
• Qualitative data needed– Brief interviews with clients/feedback from clients?
• How do clients feel they have benefitted?
– Written case studies?• Description of individual client’s journey
– Need a DCRS repository for qualitative evidence storage
Acknowledgements:
Janet Andelin and Rachel Carse, Dept of Health
Jan Smith, CORE, UCL
Ertan Fidan & David Hopkinson, Birmingham Primary Care Shared Services Agency
For a copy of the published paper, contact me at
Thank you


















