Health Assessment by Dr. Hala Yehia. Objectives At the end of this lecture the student will be able...
115
Health Assessment Health Assessment by by Dr. Hala Yehia Dr. Hala Yehia
-
date post
19-Dec-2015 -
Category
Documents
-
view
214 -
download
0
Transcript of Health Assessment by Dr. Hala Yehia. Objectives At the end of this lecture the student will be able...
Health Health AssessmentAssessment
by by Dr. Hala YehiaDr. Hala Yehia

Objectives
At the end of this lecture the student will be able to:Define health assessmentList purpose of H.E.Identify types of HE.Describe methods of data collection.Explain component of nursing history.

Objectives
Define physical assessmentDiscuss principles of Physical assessment.Discuss preparation for physical examination.Identify physical assessment methodsApply physical examination from head to toe.
Health Assessment Systematic and continuous collection,organization, validation and
documentation of data.
The first step in the nursing process It is focus on a client’s response to a
health problem.

Purposes of Assessment
To create a data base of the client’s response to health and illnessTo determine the nursing care needs of the patient.To evaluate physiologic outcomes of health care and thus client progressTo screen for presence of risk factors

FOUR TYPES OF ASSESSMENT
Initial Assessment
Focus Assessment or On-going Assessment
Emergency Assessment
Time-Lapsed Assessment

FOUR TYPES OF ASSESSMENT
1. Initial AssessmentWhen performed:At specified time after admission
Where done:Done at the ward
Purpose of Initial Assessment:•To create a data base for problem identification• For reference and future comparison
FOUR TYPES OF ASSESSMENT
2. Focus Assessment or On-going AssessmentWhen performed:Integrated throughout the nursing process
Purpose of On-going Assessment:•To identify problems overlooked earlier
•To determine the status of a health problem (i.e. hypertension status every fifteen minutes

FOUR TYPES OF ASSESSMENT
3.Emergency AssessmentWhen done:During acute physiologic and psychological crisis
Where done:Emergency Room Comfort RoomAnywhere!!! On site!!!
Purpose of Emergency AssessmentTo identify life-threatening condition

TYPES OF ASSESSMENT
4. Time-Lapsed AssessmentWhen done:Several months after initial
assessmentPurpose of Time-Lapsed Assessment
To compare current status of patient with base line data (initial assessment)
What is the initial output of the Assessment Phase?
Data or Recorded Data:
process of gathering information about the client’s health status
TYPES OF DATA
1. Subjective or Covert Data:
Information (data) apparent only to the person affected that can be described or verified only by that person.
During the recording of data, this should be stated using the patient’s own wordsThese are the symptoms felt by the patient.Fever “ I felt of hotness
TYPES OF DATA
2. Objective or Overt Data
signs or overt data; detectable by an observer or can be tested against an accepted standardThese are the signs which are observableFever skin is warm to touch; temp. is 38.9.
SOURCES OF DATA
1. Primary SourcePatient himself except when:•He is unconscious•Patient is a baby•Patient is insane
SOURCES OF DATA
2. SecondarySupport peopleClients recordsHealth care professionalsLiteratureResults of laboratory and diagnostic testsMedical history and physical examination

Assessment
Observation +Interview +Examination =
Assessment (Data Collection)

METHODS OF DATA COLLECTION
Observing
Interviewing
Examining
METHODS OF DATA COLLECTION
1-Observation – to gather data by:
using the five senses; a conscious deliberate skill that is developed only through effort and with an organized approach.
METHODS OF DATA COLLECTION
2-Interview – a planned communication or
conversation with a purpose.Preparation:
1. review the client’s medical records2. conversations with other health team
members3. research of the presenting medical
diagnosis
METHODS OF DATA COLLECTION: INTERVIEWING
Two types of Interview
Directive Type of InterviewNon-directive Type of Interview or
Rapport building Interview.

DIRECTIVE TYPE OF INTERVIEW
StructuredUses closed-ended questions
calling for specific data• When used:
When you need to elicit specific dataWhen there is little time availableoften begin with when, where, who, what, do, does, did
NON-DIRECTIVE TYPE ORRAPPORT-BUILDING INTERVIEW
Uses more open-ended questionsAdvantage is that it allows the patient to volunteer information
TYPES OF INTERVIEW QUESTIONS
Open-Ended Questionse.g. Explain ----
Closed-Ended Questionse.g. did --------
Stages of Interview
1. Introduction/Opening2. Working/Body3. Closure/Closing



Social dataFamily relationshipEducational history Occupational historyEconomic status

Physical Examinations
Is the process which investigate the body of a patient for sign of disease.It generally follows the taking of the medical history.

Purposes of Physical Assessment
Gather baseline data about the client’s current health status.Supplement, confirm or refute data obtained from history taking.Confirm and identify health problems.Make clinical judgment about the client’s changing health status.Decide on an intervention based on data obtained.Evaluate The Physiologic Outcome Of Care.

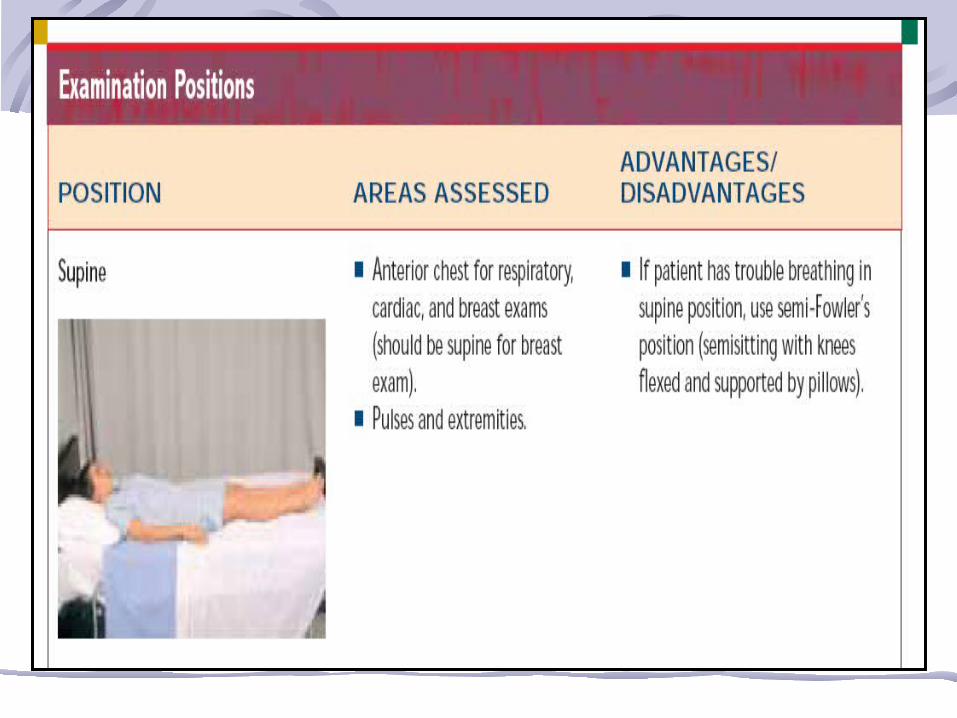
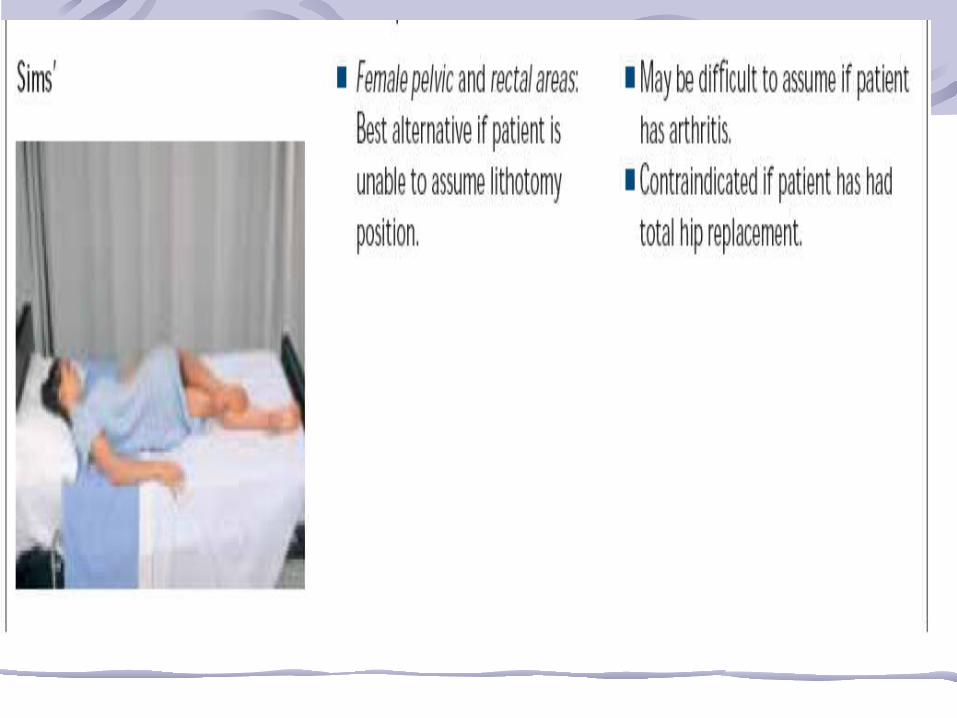
Principles in Performing Physical Assessment
Order of examination Preparation of environmentPreparation of equipmentsPhysical preparation of the clientPsychological preparation of the client





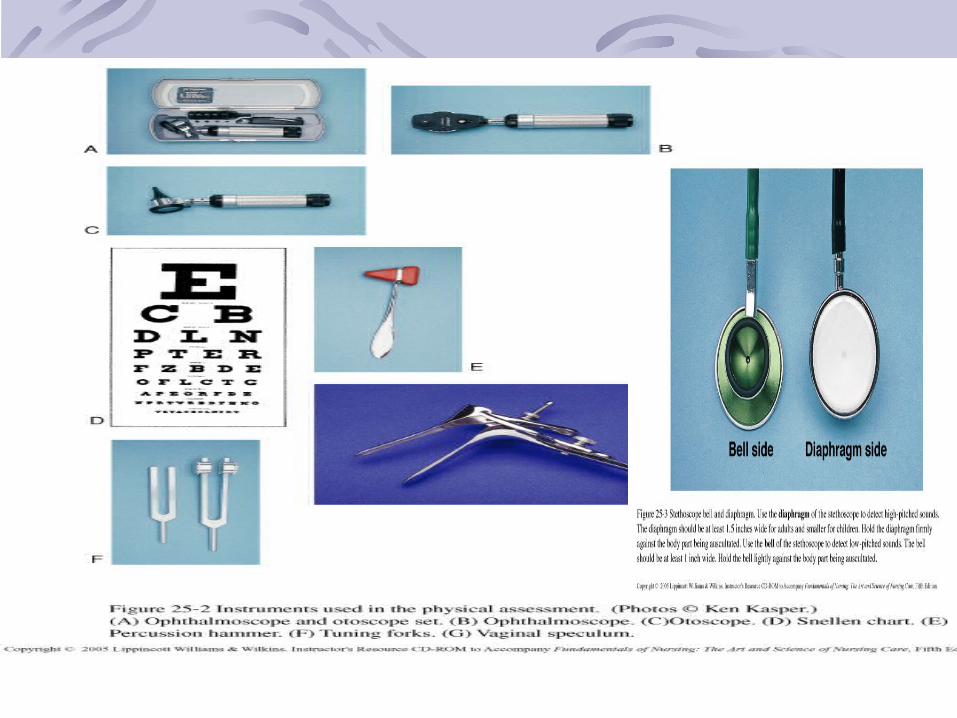



Physical Assessment Methods
InspectionPalpationAuscultationPercussion

Inspection
Assessment process during which the nurse observes the client
InspectionIs the visual examination, that is assessing by using the sense of sight. It should be deliberate, purposeful, and symmetric.Done By:
Naked eye. Otoescope.To assess:
Moisture, color, and texture of body surface as well as shape, position, size, and symmetry of the body parts.

Palpation
The use of the hands and the sense of touch to gather data

Different parts of the hand are best suited for specific purposes For example, the dorsal aspect of the hand is best for assessing temperature changes , the ball of the hand on the palm and ulnar surface is best for detecting vibration, and the finger pads and tips are the most discriminating for detecting fine sensations, such as pulsations

PalpationIs the examination of the body using the sense of touch. The pads of the fingers are used.
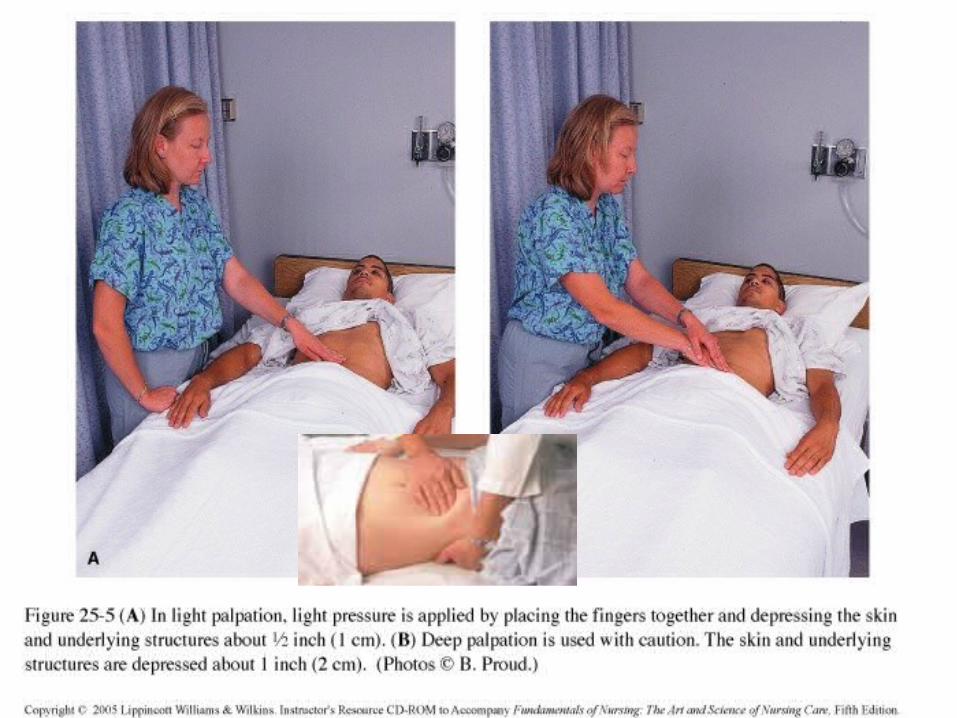
Types of palpation: Light palpation. Deep palpation.Bimanual PalpationTo assess: Texture, temperature, and size. Distention, pulsation, and mobility of organs or masses.
Guidelines for palpation
The nurse’s hands should be clean and warm, and finger nail short. Area of tenderness should be palpated last. Deep palpation should be done after superficial palpation.
.
PercussionTapping of various body organs and structures to produce vibration and sound.

PercussionPercussion
Is the act of striking the body surface to elicit sounds that can be heard or vibration that can be felt.
Types of percussion:Direct percussion.Indirect percussion.
It is indicate: tissue is fluid filled, air filled or solid.

Auscultation
The act of listening to sounds within the body to evaluate the condition of body organs(stethoscope)

Auscultation
Quiet environmentKnow landmarksKnow “normal”PRACTICE! PRACTICE! PRACTICE!Requires concentration, practice, and application of knowledge
Auscultation of the sounds described according to their:
Pitch: is the frequency of the vibrations( ranging from high to low)
Intensity: the loudness or softness of a sound.
Duration: the sound length( short, medium, or long)
Quality: a subjective description of a sounds( gurgling, swishing)

Organization of Physical Assessment
1- General appearance Mood and affectSigns of distressPostureBody movementHygiene and groomingType of clothing
2- MeasurementsHeight and weightVital signs

3- Head to toe examination
Head Neck Skull Anterior thorax Scalp BreastHair Abdomen Face Posterior thorax Eyes Upper extremitiesEars Lower extremities NoseMouth

General AppearanceAffect is the person’s feelings as they
appear to othersMood or emotional state is expressed
verbally and non verballySign of distress is signs and symptoms
of pain, difficulty in breathing or anxiety
Hygiene and grooming observe the appearance of hair, skin or fingernails and clothes
Type of clothing observe if the type of clothing worn is appropriate for temperature and weather conditions

SkinMethod of assessment:
Inspection palpation
Normal skin is:
varies from light to deep brown, from ruddy pink to light pink and from yellow overtones to olive. Intact surfaces.

Abnormal findings
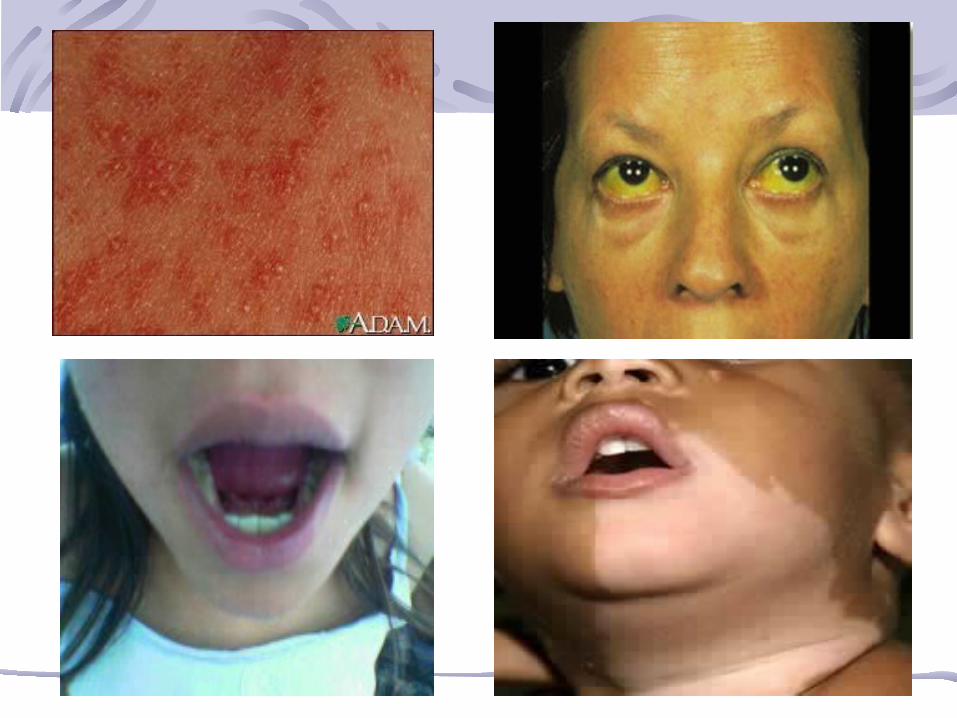
Pallor: is the result of inadequate circulating blood or hemoglobin and subsequent reduction in tissue oxygenation. Cyanosis: a bluish color is most evident in the nail beds, and lips. Jaundice: a yellowish color observed in the sclera of the eyes, mucosa membrane and the skin. Erythema: is a redness associated a Varity of rashes. Vitiligo: patches of hypo pigmented skin.
Assessment of the hair
Method:Inspection palpationNormal hair is: well distributed, thick hair, silky, resilient hair.
Abnormal finding: Alopecia: hair loss. Protein deficiency: the hair color is reddish or bleached. Hypothyroidism: cause very thin and brittle hair.

Assessment of the nails
Method: Inspection- Palpation.
Assess: the nails plate shape, angel between the nail and the nail bed, nail bed color, and the intactness of the tissue around the nail.
Normal nail: convex curvature, angel of nail plate about 160, smooth texture, highly vascular, and intact epidermis.


The head
Method: inspection - palpation.Assess: Skull- Face
Normal skull: rounded, smooth skull contour, absences of masses or nodules.
Normal face: symmetric facial features, equal in size, and symmetric facial movement.
Abnormal finding:Edema of the eyelids.Moon face: round face with reddened cheeks

Assessment of the eyes and vision
Method: inspection- palpation.
Assess: External eye structure, vision, lacrimal gland, lacrimal sac, nasolacrimal duct.
Normal eyes: Eye structure: symmetrical eyes, eyebrows symmetrically aligned, equal movement, skin intact, with shiny smooth and pink or red conjunctiva, pupils equal in color, size and diameter.Lacrimal glands: No edema or tenderness over lacrimal gland.

Assessment of the ear and hearing
Method: inspection –palpationAssess: the external ear- internal ear canal- tympanic membrane.
Normal ear and hearing: Color of the ear as same of facial skin, symmetrical, and the auricle aligned with outer canthus of eye.Mobile, firm, and not tender.Normal tympanic membrane is grayish color.

Pulling the ear pinna up and backPulling the ear pinna up and back Inserting the otoscopeInserting the otoscope

Watch tick test.
Tuning fork tests.
Hearing Test

A- Weber’s testA- Weber’s test
B1-(Rinne test) Place the tuning fork on the mastoid process
B1-(Rinne test) Place the tuning fork on the mastoid process
B2-(Rinne test) Place the tuning fork in front of the ear
B2-(Rinne test) Place the tuning fork in front of the ear
Assessment of the nose and sinuses
Method: inspection- palpation.Assess: the nose, nasal cavity patency, sinuses.
Normal nose : symmetric and straight, no discharge and flaring, , no tender or lesions.
Nasal cavity patency: the air moves freely as the client breath, mucosa pink and watery discharge.
Sinuses: no tenderness in the maxillary and frontal sinuses.


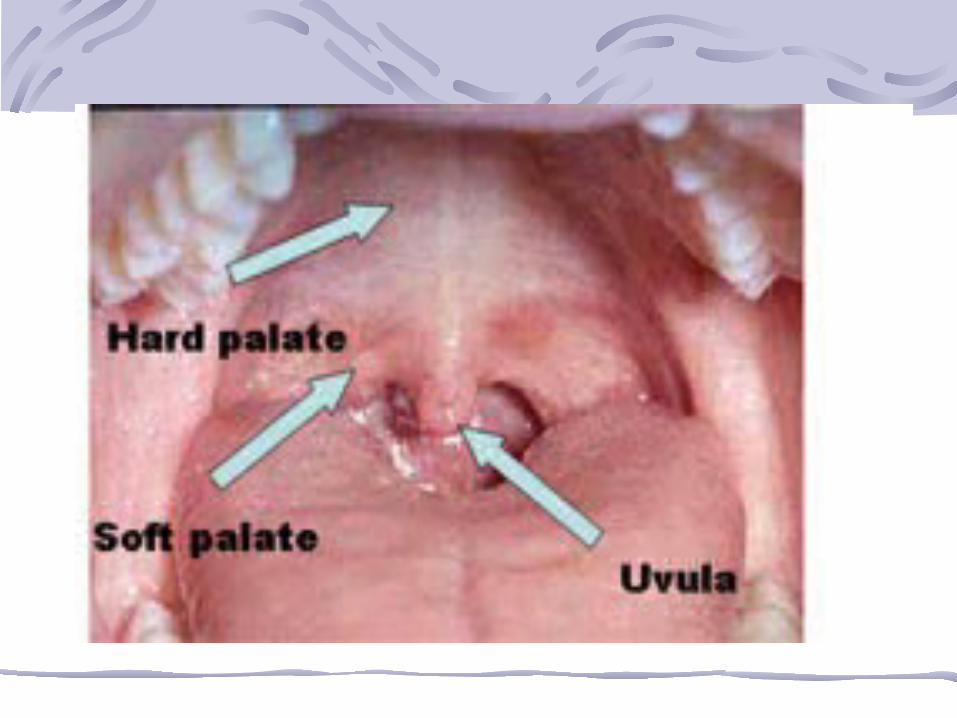
Assessment of the Mouth and pharynx
Method: inspection- palpation.Assess: the lips and buccal mucosa, teeth, gum, tongue, floor of the mouth, salivary gland, palate, uvula, tonsils.
Normal Mouth and pharynx:Lips and buccal mucosa: pink color, soft, moist, smooth texture, symmetry of contour, ability to purse lips.Teeth and gums: 32 adult teeth, smooth, white, shiny tooth enamel, pink gums and intact.

Tongue/floor of the mouth: central position for the tongue, moves freely, no tenderness, smooth with no palpable nodules in the tongue or in the floor.
Silvery glands: same color of the buccal mucosa, no nodules or tenderness, and secret the saliva in the oral cavity.
Palates and uvula: light pink, smooth, soft intact palate, the uvula positioned in the midline and mobile.

pharynx and tonsils: pink and smooth posterior wall, pink and smooth tonsils within normal size and no discharge.
Abnormal findings: Dental caries: cavities.Glossitis: inflammation of the tongue.Stomatitis: inflammation of the oral mucosa.
Assessment of the neck
Method: inspection- palpationAssess : the muscles, lymph nodes, trachea, thyroid gland, carotid arteries, and jugular vein.
Assessment of thorax and lungs
Method: inspection- Auscultation- percussion.Assess: chest shape and size, Breathing sounds, chest sounds.
Chest shape and size: the thorax is oval.

Abnormal chest shape: in older adult kyphosis and osteoporosis alter the size of the chest cavity as the ribs move downward and forward.Pigeon chest.Permanent deformity ( caused by rickets).Funnel chest.
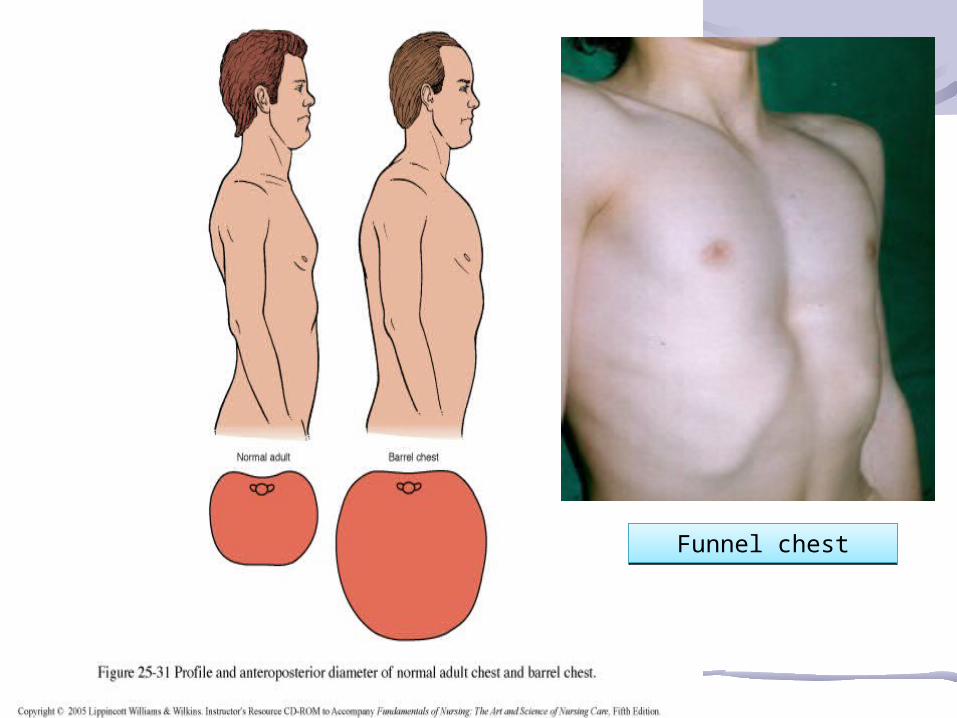
Funnel chestFunnel chest
Chest landmarks:
Front: anterior axilla line, midclavicular line, midsternal line.
Back: Vertebral line, right scapular line


Assessing the thorax and lungs:
Anterior thorax: Assess respiratory excursion .
Percussion sounds on the anterior chest.
Posterior thoraxAssess respiratory excursion


Assessment of cardiovascular and peripheral system
Heart
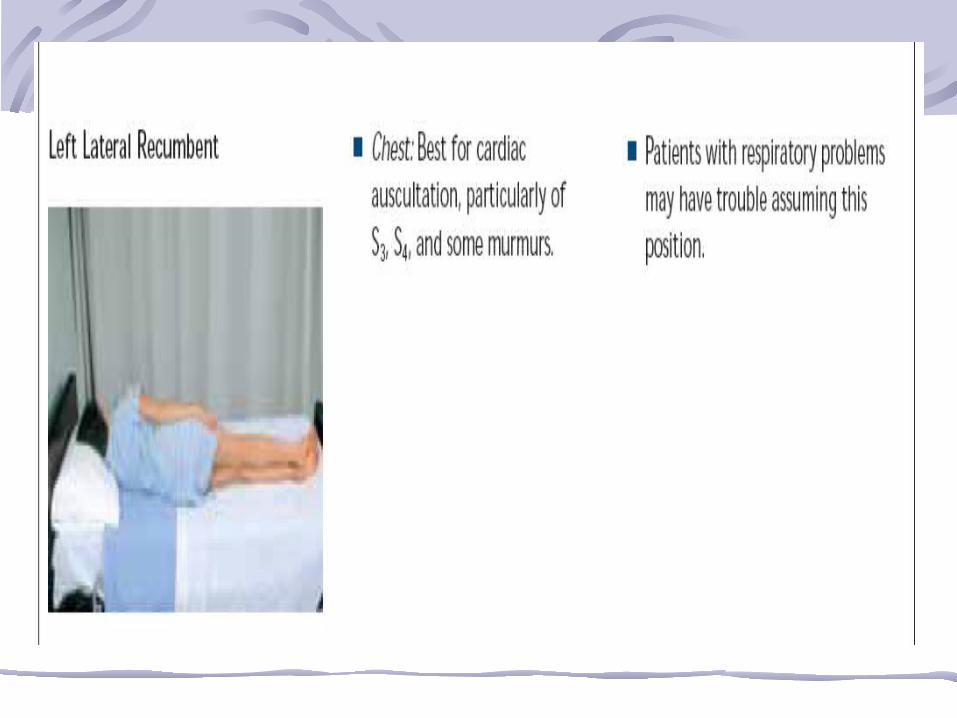
Auscultation is more meaningful method.Heart examination are usually performed when the client is a symmetrical position.
The normal heart sounds:
Systole: Ventricles contract S1.Diastole: Ventricles relax S2.
S1 (Lub) ….. occur when atrioventricular valves close (A-V), valve close when the ventricles have been filled.
S2 ( Dub) …. after the ventricles empty their blood into the aorta and pulmonary arteries, has a higher pitch than S1 and also Shorter.
S1 and S2 are (Lub-Dub) sounds.

Abnormal heart sounds:
S3….. is normal in children and young adults, in older adults its indicate heart failure.
S4…. may be heard in many elderly clients and can be signs of hypertension.
CAROTID ARTERY Palpation Palpate carotid artery with extreme caution -auscultation
JUGULAR VEIN Inspection Client is placed in a semi fowlers position

BREAST AND AXILLAEInspection Inspect the breast for size, symmetry, and contour or shape.Inspect the skin of the breast for localized discoloration
Normal;Female: rounded shape; slightly unequal in size; generally symmetricMale; breast even with chest wall Abnormal:Recent change in breast size; swellings; marked asymmetry.Localized discoloration
Abdomen
Inspection Inspect the abdomen for skin integrity.Inspect the abdomen for contour and symmetry.movements associated with respirations, peristalsis or aortic pulsations

AuscultationAuscultate the abdomen for bowel soundsPercussion Percuss several areas in each of the four quadrants to determine the presence of tympany (gas in the stomach and intestines) and dullness (decrease, absence or flatness of resonance over solid masses or fluid).

Palpation
Perform light palpation first to detect areas of tenderness and/or muscle guarding.Perform deep palpation over all four quadrants

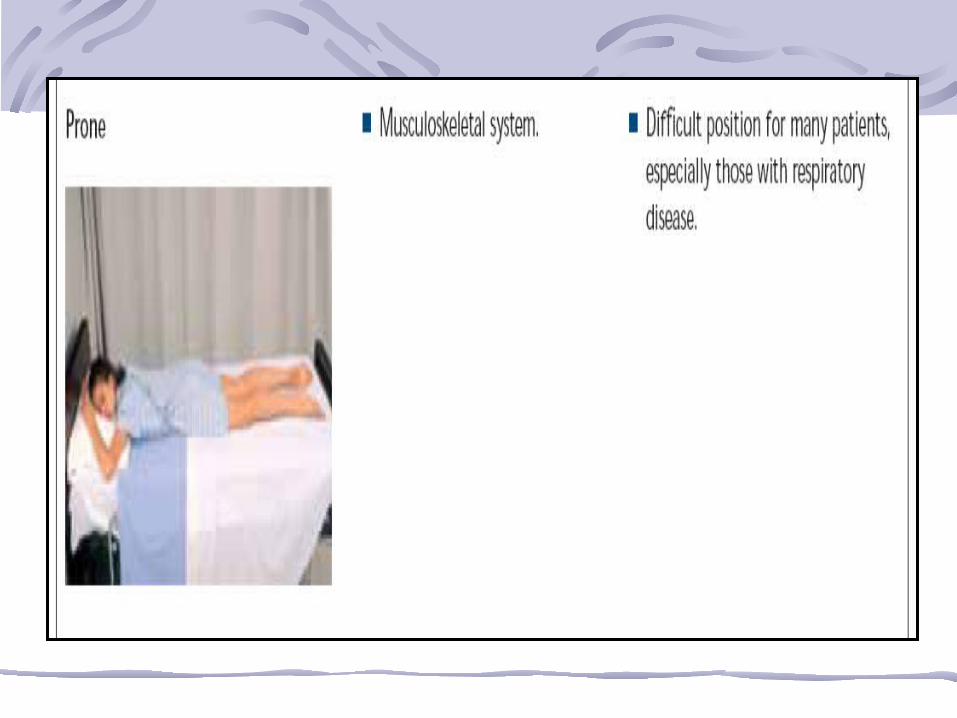
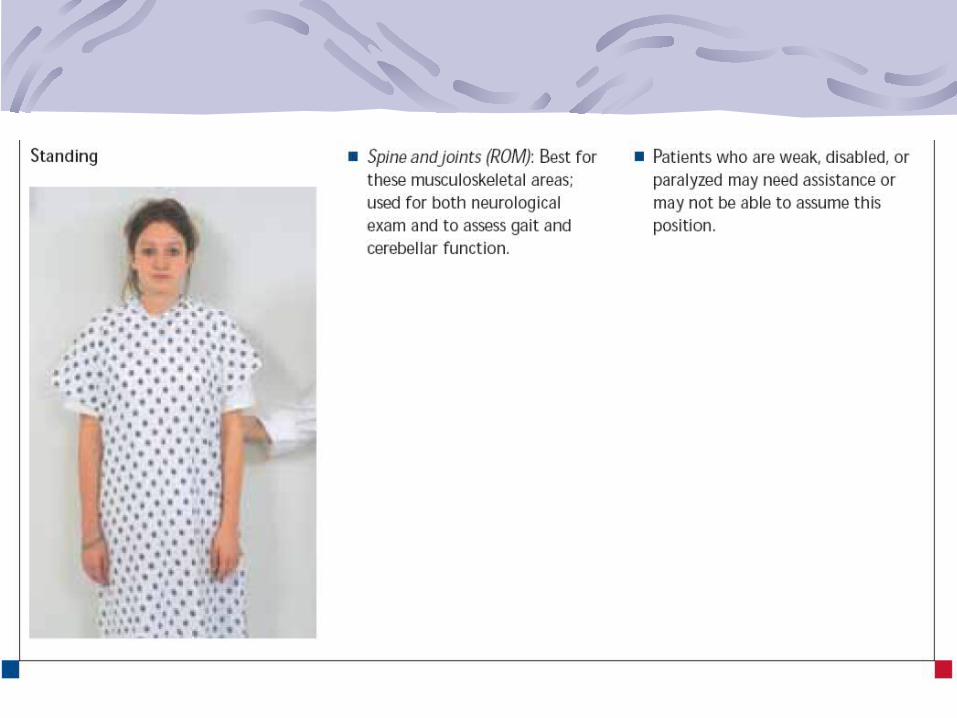
Musculoskeletal System
Muscles, bones and jointsObjective assessment of musculoskeletal systemPurpose
To assess function of ADL (activities of daily living)Screen for abnormalities
Screening examsInspection (look)Palpation (feel)ROM with movement active or passiveCompare with the opposite
Muscles
Inspect for muscle size – equal size on both sides of the bodyInspect the muscles and tendons for contractures – there should be no contracturesInspect the muscles for fasciculation and tremors – there should be no fasciculation and tremors

Palpate muscles at rest to determine muscle tonicity – normally firmPalpate muscles while the client is active and passive for flaccidity, plasticity & smoothness of movement – there should be smooth coordinated movements

Bones
Inspect the skeleton for normal structure and deformities – there should be no deformitiesPalpate the bones to locate any areas of edema or tenderness – no tenderness or swelling
Joints
Palpate each joint for tenderness, smoothness of movement, swelling, crepitating, and presence of nodule – no tenderness, swelling, crepitating or nodules
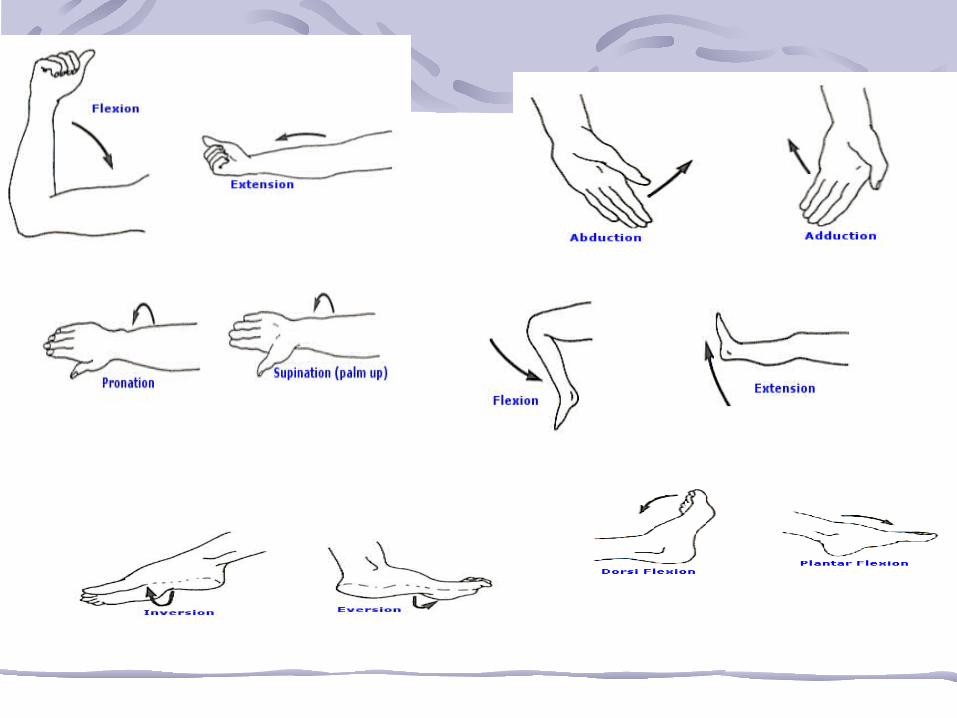
Types of joint movementFlexion – bendingExtension – straighteningAdduction – toward – further straighteningAbduction –the midlineRotation – around its central axisCircumduction – circularEversion – foot outwardInversion – foot inwardPronation – palm downSupination – palm up