Health and Productivity as a Business Strategy: A...
18
FAST TRACK ARTICLE Health and Productivity as a Business Strategy: A Multiemployer Study Ronald Loeppke, MD, MPH Michael Taitel, PhD Vince Haufle, MPH Thomas Parry, PhD Ronald C. Kessler, PhD Kimberly Jinnett, PhD Objective: To explore methodological refinements in measuring health-related lost productivity and to assess the business implications of a full-cost approach to managing health. Methods: Health-related lost productivity was measured among 10 employers with a total of 51,648 employee respondents using the Health and Work Performance Ques- tionnaire combined with 1,134,281 medical and pharmacy claims. Regression analyses were used to estimate the associations of health conditions with absenteeism and presenteeism using a range of models. Results: Health-related productivity costs are significantly greater than medical and pharmacy costs alone (on average 2.3 to 1). Chronic conditions such as depression/anxiety, obesity, arthritis, and back/neck pain are especially important causes of productivity loss. Comorbidities have significant non-additive effects on both absenteeism and presen- teeism. Executives/Managers experience as much or more monetized productivity loss from depression and back pain as Laborers/Operators. Testimonials are reported from participating companies on how the study helped shape their corporate health strategies. Conclusions: A strong link exists between health and productivity. Integrating produc- tivity data with health data can help employers develop effective workplace health human capital investment strategies. More research is needed to understand the impacts of comorbidity and to evaluate the cost effectiveness of health and productivity interventions from an employer perspective. (J Occup Environ Med. 2009;51:411– 428) B usinesses face a host of critical chal- lenges impacting their profitability and viability. Chronic health condi- tions are on the rise across all age groups, and these conditions create a significant economic burden, costing employers heavily as they provide medical benefits for employees and absorb the costs of sickness absence and long- and short-term disability claims. 1,2 One study found that more than 80% of medical spending goes toward care for chronic conditions. 3 Moreover, nearly 50% of Americans have one or more chronic health con- ditions. 4 Employers are the ultimate purchasers of health care for the ma- jority of Americans, spending approx- imately $13,000 per employee per year on total direct and indirect health- related costs. 3,5 U.S. Department of Labor statistics indicate that there are approximately 137 million non-farm employees and the overall annual cost impact of poor health on the workplace is estimated at $1.8 trillion. 6 Although many employers now are concerned about workforce health, their efforts to address this problem have tended to focus on medical costs without considering the impact of health on workforce productivity. After identifying their major medical and pharmacy cost drivers, many employers have attempted to relieve their cost burden by shifting a por- tion of these costs to employees through higher copays and deduct- ibles and other managed care ap- proaches. But these strategies do not address the cost of reduced produc- tivity, which can be substantial. The approaches that many employers have taken may have actually created From the Alere (Dr Loeppke), Brentwood, Tenn; Alere (Dr Taitel, Mr Haufle), Rosemont, Ill; Integrated Benefits Institute (Dr Parry, Dr Jinnett), San Francisco, Calif; and Department of Health Care Policy (Dr Kessler), Harvard Medical School, Boston, Mass. Address correspondence to: Dr Ron Loeppke, MD, MPH, 5166 Remington Dr. Brentwood, TN 37027; E-mail: [email protected]. Copyright © 2009 by American College of Occupational and Environmental Medicine DOI: 10.1097/JOM.0b013e3181a39180 JOEM • Volume 51, Number 4, April 2009 411
Transcript of Health and Productivity as a Business Strategy: A...

FAST TRACK ARTICLE
Health and Productivity as a Business Strategy:A Multiemployer Study
Ronald Loeppke, MD, MPHMichael Taitel, PhDVince Haufle, MPHThomas Parry, PhDRonald C. Kessler, PhDKimberly Jinnett, PhD
Objective: To explore methodological refinements in measuringhealth-related lost productivity and to assess the business implications ofa full-cost approach to managing health. Methods: Health-related lostproductivity was measured among 10 employers with a total of 51,648employee respondents using the Health and Work Performance Ques-tionnaire combined with 1,134,281 medical and pharmacy claims.Regression analyses were used to estimate the associations of healthconditions with absenteeism and presenteeism using a range of models.Results: Health-related productivity costs are significantly greater thanmedical and pharmacy costs alone (on average 2.3 to 1). Chronicconditions such as depression/anxiety, obesity, arthritis, and back/neckpain are especially important causes of productivity loss. Comorbiditieshave significant non-additive effects on both absenteeism and presen-teeism. Executives/Managers experience as much or more monetizedproductivity loss from depression and back pain as Laborers/Operators.Testimonials are reported from participating companies on how thestudy helped shape their corporate health strategies. Conclusions: Astrong link exists between health and productivity. Integrating produc-tivity data with health data can help employers develop effectiveworkplace health human capital investment strategies. More research isneeded to understand the impacts of comorbidity and to evaluate the costeffectiveness of health and productivity interventions from an employerperspective. (J Occup Environ Med. 2009;51:411–428)
B usinesses face a host of critical chal-lenges impacting their profitabilityand viability. Chronic health condi-tions are on the rise across all agegroups, and these conditions create asignificant economic burden, costingemployers heavily as they providemedical benefits for employees andabsorb the costs of sickness absenceand long- and short-term disabilityclaims.1,2 One study found that morethan 80% of medical spending goestoward care for chronic conditions.3
Moreover, nearly 50% of Americanshave one or more chronic health con-ditions.4 Employers are the ultimatepurchasers of health care for the ma-jority of Americans, spending approx-imately $13,000 per employee per yearon total direct and indirect health-related costs.3,5 U.S. Department ofLabor statistics indicate that there areapproximately 137 million non-farmemployees and the overall annual costimpact of poor health on the workplaceis estimated at $1.8 trillion.6
Although many employers now areconcerned about workforce health,their efforts to address this problemhave tended to focus on medical costswithout considering the impact ofhealth on workforce productivity.After identifying their major medicaland pharmacy cost drivers, manyemployers have attempted to relievetheir cost burden by shifting a por-tion of these costs to employeesthrough higher copays and deduct-ibles and other managed care ap-proaches. But these strategies do notaddress the cost of reduced produc-tivity, which can be substantial. Theapproaches that many employershave taken may have actually created
From the Alere (Dr Loeppke), Brentwood, Tenn; Alere (Dr Taitel, Mr Haufle), Rosemont, Ill;Integrated Benefits Institute (Dr Parry, Dr Jinnett), San Francisco, Calif; and Department of HealthCare Policy (Dr Kessler), Harvard Medical School, Boston, Mass.
Address correspondence to: Dr Ron Loeppke, MD, MPH, 5166 Remington Dr. Brentwood, TN37027; E-mail: [email protected].
Copyright © 2009 by American College of Occupational and Environmental Medicine
DOI: 10.1097/JOM.0b013e3181a39180
JOEM • Volume 51, Number 4, April 2009 411

the opposite of their intended effect:By shifting costs to employees theyhave created barriers to access thatlead to delay of care, which in theend worsens clinical outcomes andnegatively impacts productivity.5
This view of employee health as acost to be reduced, rather than aninvestment to be managed, needs tobe reconsidered in light of the over-whelming demographic trends towardan older workforce and growing re-search evidence documenting substan-tial costs of worker health problems onwork performance. Some forward-thinking employers have become re-ceptive to a new model that focuseson health-related productivity—notmere medical and pharmacy spend-ing—as their most compelling costissue related to worker health. This isa comprehensive view of health inthe workplace, which places a truebusiness value on health and viewshuman capital as an investment. Itrecognizes that, to date, employershave given inadequate attention tofactors such as presenteeism, ab-sence and disability as they haveattempted to understand the impactof poor health. It acknowledges thatthe business community needs a newand improved methodology to mea-sure the relationship between healthand productivity, as well as a newlexicon to help articulate its value toall stakeholders.
In an effort to advance betterunderstanding of these emergingconcepts, the American College ofOccupational and EnvironmentalMedicine (ACOEM) and IntegratedBenefits Institute (IBI) initiated aprogram of research aimed at assess-ing the full impact of health condi-tions in the workplace, factoring innot only medical or pharmacy costbut also health-related productivitycosts such as absenteeism and pre-senteeism. ACOEM and IBI, work-ing in strategic collaboration withAlere (formerly Matria Healthcare)and faculty from Harvard MedicalSchool, focused this “Health andProductivity as a Business Strategy”study on identifying leading chronic
health conditions that drive health-related costs. In phase 1 of this study,Loeppke et al7 identified the totalcost impact of health on the financialbottom line for four employers witha total of 57,000 employees. Thismultiemployer study integrated med-ical and pharmacy claims data withemployee self-reported health-re-lated absenteeism and presenteeismdata from the validated Health andWork Performance Questionnaire(HPQ) survey to determine the “fullcost” of health.
The results of phase 1 providedimportant new insights into the healthconditions which have the greatestproductivity-related impact on em-ployers included in the study. In addi-tion, the true value of health-relatedlost productivity was found to ex-ceed the direct medical and phar-macy costs for most of the healthconditions studied. The first phase ofthis study confirmed what other pub-lished studies have suggested—thaton average, for every 1 dollar em-ployers spend on worker medical orpharmacy costs, they absorb at least2 to 4 dollars of health-related pro-ductivity costs.7,8
Health-related productivity costsin the study were manifested in theform of absenteeism and presenteeismassociated with 25 chronic conditionsselected for study. Even without dis-ability costs being included, thestudy found that when looking at thecombined medical, pharmacy, absen-teeism and presenteeism costs ofthese health problems, some condi-tions such as back or neck pain,depression, and fatigue are far morecostly than employers have previ-ously realized. Furthermore, the costranking of health conditions thathave been measured through the lensof productivity loss is significantlydifferent from the more traditionalcost ranking of medical or pharmacycosts alone.7 Phase 1 of our studyconcluded that an integrated ap-proach of combining medical orpharmacy costs with lost productiv-ity costs provides a more complete
and actionable financial assessmentof health for employers.
This article presents an overview ofresults from all 10 companies partici-pating in our study, with a more de-tailed focus on the results of phase 2.In phase 2, we increased the powerof the analysis by increasing thenumber of employers and employeesmeasured and investigated more sub-tle aspects of the relationship be-tween the targeted health problemsand productivity. We explored a num-ber of methodological refinements inmeasuring productivity, estimatingthe lost productivity associated withhealth problems and blending pro-ductivity costs with medical and phar-macy claims costs to create estimatesof total health-related workplace costs.We also provide significant new find-ings about the workplace effects ofcomorbidities. In addition, we presentresults that continue to support theneed for a new, productivity-focusedhealth model in the workplace and anew language and methodology tohelp determine the true business valueof health. We also offer insights fromparticipating companies on how thestudy helped shape their corporatehealth strategies.
Methods
SampleTen participating companies were
identified based on size, availabilityof medical and pharmacy claims dataand either availability of HPQ surveydata or a willingness to implement anHPQ survey in their workforce, alongwith an agreement to allow the merg-ing of these data sources. For each ofthe 10 companies in the study, Table 1shows the phase, industry type, num-ber of eligible employees, number ofHPQ respondents, and response rate.The companies ranged in size from1407 to 38,413 eligible employeesand had response rates from 11.5%to 65.0%; the combined responserate was 34.3%. Company C wasdropped from subsequent analysisbecause it did not include the absen-teeism measure used in the phase 2
412 Health and Productivity as a Business Strategy • Loeppke et al

analysis. The phase 1 HPQ surveyswere administered in 2005–2006;phase 2 surveys were administered in2007–2008. The analysis included49,576 valid HPQ respondents, with14,954 in phase 1 and 34,622 inphase 2.
MeasuresHealth Conditions. Health condi-
tions were assessed by self-reportwith a standard chronic conditionschecklist based using WHO HPQ.9,10
The HPQ conditions checklist isbased on US National Health Inter-view Survey (http://www.hcp.med.harvard.edu/hpq/) and (http://www.cdc.gov/nchs/nhis.htm).11,12 Checklists ofthis sort have been widely used inprior population-based studies andhave been shown to yield more com-plete and accurate reports than esti-mates derived from responses toopen-ended questions.13 Method-ological studies in both the US andUK have documented good concor-dance between such condition re-ports and medical records.14–16
In the surveys carried out in phase1, the HPQ was administered as anindependent on-line instrument inthree companies and integrated intoan on-line health risk assessment(HRA) in one company; we used thestandard HPQ question series to askrespondents “Do you have any of the
following conditions” and, if yes,“mark whether you never, previously,or currently receive professional treat-ment.” For all the companies in phase2, the survey process was changed inseveral ways. The HPQ survey wasintegrated into an existing on-lineHRA instrument and administered aspart the companies’ annual assess-ment. This was a practical changereflective of companies’ desire tointegrate productivity measures intotheir wellness programs, as well as,simplify data collection and reducethe administrative burden of popula-tion assessment. As a trade off, thequestion about health condition wasasked in a more restrictive mannercommon to many HRAs. In phase 2,respondents were asked “has yourdoctor ever told you that you have orhave had any of the following healthproblems.” If yes, then indicate “yes,I am receiving treatment and I amtaking medication; yes, I am receiv-ing treatment but I am not takingmedication; No, I am not currentlyreceiving treatment.” This change al-lows us to see the impact of instrumentvariation on condition and treatmentprevalence as well as on health-relatedproductivity assessment. Individualsfrequently misclassify their per-ceived weight status relative to theircalculated body mass index (BMI)based on self-reported height and
weight.17 Because we had self-reported height and weight available,we calculated BMI (BMI ! weightkg/[height meter2]; if BMI !30 thenobese) to determine a more accurateassessment of obesity. However, thischange also eliminated the self-report of treatment for this healthcondition.
Workplace Outcomes. The HPQmeasures absenteeism through a self-report assessment of sickness ab-sence days in the month (28 days)before the survey, which was definedfor purposes of this article as theamount of time the respondent re-ported missing work due to theirhealth conditions. These results weremultiplied by 13 to project to anannual absenteeism value. An alter-native would have been to assesstotal amount of time of missed workfor any reason, which is the methodused for estimating absenteeism inour earlier article.7 We chose thenarrower focus for phase 2 of thestudy because it reduces variabilityin lost time from work due to vaca-tion and other reasons. However, thisapproach may not capture any losttime from work that the respondentfails to recognize as due to healthreasons, such as “vacation” days as-sociated with low-level physical (eg,fatigue) or psychological (eg, depres-sion) symptoms. Separate questions
TABLE 1Sample Details
Phase Company Industry TypeNo. of Eligible
EmployeesNo. of Valid HPQ
RespondentsResponseRate (%)
Phase 1 Company A Chemical Manufacturer 12,000 3,929 32.7Company B Computer Hardware Manufacturer 1,407 347 24.7Company C* Tele-Communication Information Technology 6,000 2,072 34.5Company D Tele-Communication Information Technology 38,413 10,678 27.8
Phase 1 sub-total 57,820 17,026 29.4Phase 2 Company E Hospitality and Entertainment 20,100 2,311 11.5
Company F Energy Corporation 9,184 4,377 47.7Company G Aerospace and Defense 22,237 10,928 49.1Company H Industrial Manufacturer 16,349 3,434 21.0Company I Healthcare Consulting 22,000 11,809 53.7Company J Insurance 2,712 1,763 65.0
Phase 2 sub-total 92,582 34,622 37.4Total 150,402 51,648 34.3Combined (9 employers) 144,402 49,576 34.3
*Dropped from final analysis due to missing data.
JOEM • Volume 51, Number 4, April 2009 413

were asked about number of fulldays (which we assigned 8 hours ofmissed time) or partial days (whichwe assigned 4 hours of missed time)the respondent missed “because ofproblems with your physical or men-tal health.” Also, unlike the unre-stricted approach to assessing hoursof missed work, this more restrictedapproach does not account for work-ers coming in early or leaving late onother days to make up for hours ofmissed work.
The HPQ measures presenteeismthrough a self-report assessment ofon-the-job work performance. The sur-vey asked “On a scale from 0 to 10,where 0 is the worst job performanceand 10 is the top job performance, howwould you rate your overall perfor-mance on the days you worked in thepast 4 weeks (28 days).” The resultswere converted to a percentage andannualized by assuming a 250 daywork year. Furthermore, we adjustedthe presenteeism score by the amountof absenteeism so that we did notallocate presenteeism for time the em-ployee was absent. Validation studieshave documented significant associa-tions (r ! 0.61 to 0.87) between HPQabsenteeism reports and objective em-ployer payroll records,9 significant as-sociations between HPQ presenteeismreports and supervisor assessments(r ! 0.52),10 and significant associa-tions between HPQ reports and otheradministrative indicators of perfor-mance (r ! 0.58 to 0.72).9
Control Variables. All of the re-gression analyses described belowcontrolled for respondent gender,age, and occupation. Occupation wasdivided into eight self-reported cate-gories used in the HPQ to approximatethe categories specified in the first digitof the 2000 Census Classified Index ofOccupations (http://www.census.gov/hhes/www/ioindex/overview.html).These include: executive, administra-tor, or senior manager; professional;technical support; sales; clerical oradministrative support; service; pre-cision production of crafts; and op-erator or laborer.
Medical Claims. We analyzed paidmedical claims incurred during the12 months before each respondent’sHPQ completion date. We matchedthe medical claims to the HPQ re-sults by mapping the claims’ primaryInternational Classification of Dis-eases, Version 9, Clinical Modifica-tion (ICD-9-CM) diagnoses to theHPQ medical conditions. We firstapplied the identification algorithmsdeveloped by Alere to map most ofthe chronic health conditions. Be-cause the HPQ includes only chronicconditions, we recognize that thereare many expensive acute or trau-matic health conditions that are notcurrently measured by the HPQ andothers that are vague and difficult todetermine a match. For example, ab-dominal pain could be attributed toindigestion, bladder, gynecological, ormany other sources and general symp-toms could be any or no condition.
This study used primary diagnosiscodes from ICD-9-CM to map themedical claims into the HPQ condi-tion and allocate medical costs. Thelater are defined as the actual costs theemployer paid on that claim. Althoughthe paid amount is influenced by otherfactors such as benefit plan designelements (eg, network discounts, em-ployee deductibles, coinsurance andcopays) and does not include costspaid by the employee, we focus on thepaid claim because it represents theemployers’ cost burden.
Pharmacy Claims. We also ana-lyzed pharmacy paid claims incurredduring the 12 months before eachrespondents HPQ completion date.To map pharmacy claims to HPQhealth conditions, we used the Na-tional Drug Data File Plus from FirstDatabank, Inc. Pharmacists, physi-cians, nurses, and analysts fromAlere collaborated on the develop-ment of an algorithm that groupsNational Drug Codes (NDC) intodrug categories associated withcertain health conditions for the pur-poses of standardizing NDC identifi-cation. The team used several druginformation indicators (TherapeuticDrug Group, First Databank Class,
Generic Code Number, and Route) tohelp facilitate the categorization ofNDCs.
These drug categories are thefoundation on which pharmacyclaims are matched to HPQ condi-tions. Many of the drug categorieshave one to one indication relation-ships with the HPQ conditions. Forexample, insulin medications aredirectly associated with diabetes.Alere researchers also recognizedthat these categories are not com-pletely sufficient to account for themultiple indications of certaindrugs classes. We therefore devel-oped a process to systematicallydistribute the corresponding claimdollars to the appropriate condi-tions by matching the individual’spharmacy claims to the HPQ con-ditions identified from the medicalclaims.
For example, beta blockers likeCarvedilol are typically prescribedfor heart condition management.Carvedilol can be prescribed to pa-tients with Congestive Heart Failure(CHF), Coronary Heart Disease(CHD), and hypertension. To prop-erly distribute the pharmacy claimsdollars among the multiple condi-tions, we matched each pharmacyclaim to the individual’s HPQ condi-tions identified in their medicalclaims. If an individual’s medicalclaims indicate they have CHF anddo not have CHD or hypertension,then all the dollars for that claimwill be allocated to CHF. If anindividual’s medical claims indicatesimultaneous condition prevalenceof CHF and hypertension, then 50%of the claim dollars will be allocatedto CHF and 50% will be allocated tohypertension. In instances where allthree conditions are indicated, 33%of the claim dollars would be allo-cated to each of the three conditions.
Impact Survey. Once we analyzedthe data collected in the HPQ sur-veys and medical or pharmacyclaims, we presented the results tohealth benefit decision-makers ineach of the participating companies.We then developed and subsequently
414 Health and Productivity as a Business Strategy • Loeppke et al

administered a semi-structured inter-view to gather information fromthese decision-makers about howthey were influenced by their com-pany’s results.
Analysis MethodsSimple cross-tabulations and cal-
culations of means were used to ex-amine the demographic distributionof the sample, to estimate the preva-lence of individual health conditionsand comorbidities, and to estimatethe magnitudes of absenteeism andpresenteeism in the sample. Linear re-gression analyses were used toestimate the effects of health condi-tions on absenteeism and presentee-ism, controlling for respondent gender,age, and occupation.
For the various analyses, the datawere segmented into three groups: 1.Respondents with a specific focalhealth condition selected from thechronic conditions checklist (withcondition); 2. Respondents with noneof the measured health conditions onthe chronic conditions checklist (noconditions); and 3. Respondents whodo not have a specific focal healthcondition (without focal condition).The without focal condition groupincludes respondents who may haveother chronic health conditions onthe checklist but not the specificfocal condition and respondents whodo not have any health conditions onthe checklist.
A number of different bivariate(only one condition included in eachequation) regression equations wereestimated. They examined the focalconditions compared to the no con-dition group or the without focalcondition group, difference amongthe treatment groups and differencesamong occupation groups. The biva-riate equations additionally varieddepending on whether they com-pared workers with single condition(ie, those with the focal conditionwho had none of the other condi-tions) and comorbid conditions (ie,those with the focal condition whoalso had at least one of the otherconditions) versus all those with the
focal condition (ie, whether single orcomorbid) to other workers. A finalset of regression equations examinedthe associations between the numberof conditions and the outcomes. Thecontrols for gender, age and occupa-tion were included in all the regressionequations. Statistical significance inthe regression equations was consis-tently evaluated using 0.05-level,two-sided tests without correctionsfor design effects.
Although most of the regressionanalysis results are examined at theindividual level, we also carried outsome analyses that made projectionsto the workforce. This was done bymultiplying the estimated effect ofthe condition on absenteeism or pre-senteeism at the level of the individ-ual worker by the prevalence of thecondition to arrive at an estimate ofthe number of sickness absence daysor presenteeism day-equivalents per1000 workers in the workforce dueto the condition.
To monetize the impact of losttime we multiplied the absenteeismand presenteeism estimates of daysof work lost per year by the averagedaily salary-plus-fringe equivalentsof workers with the condition. Inaddition, we multiplied the result byan industry-specific worker absencemultiplier. This last step is used torecognize that simple “replacementcosts” of absent employees signifi-cantly underestimates the real cost tothe employer. Nicholson et al18
found that these opportunity costsare a function of three factors: 1) theease with which replacement work-ers can be found, 2) the time value ofoutput (eg, can the employer sell tothe market all the goods and servicesit produces as soon as they are avail-able) and 3) the degree to whichemployees work in teams. In re-sponse, they also developed a seriesof industry and occupational multi-pliers to represent additional em-ployer financial lost productivitycosts. These multipliers are used inthe analysis of absenteeism and pre-senteeism.
In the case of presenteeism, the ratioscores were converted to day-equiva-lents by assuming that a presenteeismscore of X can be interpreted as indi-cating (100-X) percent lost productiv-ity on days at work (ie, taking intoconsideration the decrease in total daysat work due to the effects of the focalcondition on absenteeism).
To observe the total cost of healthconditions, we aggregated phase 2companies’ medical claims, phar-macy claims, absenteeism and pre-senteeism costs for each of the healthconditions. We used the methodol-ogy as described above to monetizethe productivity results. All the costswere converted into a per 1000 FTEmetric which allowed us to combinethe medical, pharmacy, absenteeismand presenteeism costs.
Results
Demographic DistributionsTable 2 shows the distribution of gen-
der, age, and occupation segmented bystudy phase and comparison group.There are several differences in thedemographic composition betweenphases. This can be attributed to themix of companies and respondentsincluded in the study. Phase 1 em-ployee respondents had a larger pro-portion of males and professionals(72.4%, 80.1%) than phase 2 (58.1%,48.7%). Also, phase 2 employee re-spondents included more Executives/Managers (8.4%), Technical Supportstaff (12.3%), and Clerical Supportstaff (12.7%) than phase 1 (1.1%,3.6%, and 3.0%). Both phase 1 andphase 2 employee respondents hadthe same percentage (7.9%) of Oper-ator/Laborers.
The difference between phase 1and phase 2 on the percent of respon-dents with a condition is consider-ably larger than we would expectbased on the demographic differ-ences between the samples in the twophases. It is noteworthy in this regardthat there was a difference in thequestion relating to whether a doctortold someone that they had the con-dition(s) or the individual thought
JOEM • Volume 51, Number 4, April 2009 415

they had the condition(s). In phase 1,only 3.5% indicated having no con-ditions. However, in phase 2, 29.4%indicated they had no conditions, asdefined by whether or not a doctortold them they have a health con-dition. Within phase 2 we are ableto observe the differences betweenthe with condition group and the noconditions group. The subsequentanalyses control for gender, age,and occupation.
Health Condition PrevalenceFrom HPQ Survey
Table 3 displays a comparison ofthe estimated prevalences of thehealth conditions for phase 1 andphase 2 respondents adjusted for theage, gender, and occupation differ-ences. Adjusting the prevalences al-lows us to consider explanationsother than demographics for the sim-ilarities and differences between thecondition prevalences in the phases.
Wide variation exists in the adjustedprevalence of the conditions consid-ered here, from a maximum of morethan one third of respondents in bothphases who reported having seasonalallergies to a minimum of less than
TABLE 3Health Condition Prevalence From HPQ Survey and Rank Order
Phase 1 Phase 2
% Difference P*
AdjustedPrevalence
(%) Rank
AdjustedPrevalence
(%) Rank
Allergy 48.1 1 34.0 1 14.1 "0.001Anxiety 8.0 15 11.1 7 #3.1 "0.001Arthritis 14.9 6 16.2 4 #1.3 "0.001Asthma 9.3 13 7.9 8 1.4 "0.001Back/neck pain 27.4 2 7.5 9 19.9 "0.001Bladder/urinary 8.8 14 4.5 16 4.3 "0.001Chronic bronchitis/
emphysema2.8 21 0.5 23 2.3 "0.001
Congestive heartfailure
1.2 23 0.3 24 0.9 "0.001
COPD 0.4 25 0.2 25 0.2 "0.001Coronary heart
disease1.0 24 2.0 20 #1.1 "0.001
Depression 12.6 9 11.2 6 1.5 "0.001Diabetes 4.7 18 4.7 15 0.1 0.725Fatigue 13.3 7 5.3 13 8.0 "0.001GERD 15.5 5 12.6 5 2.8 "0.001Headache 12.2 10 5.2 14 7.0 "0.001Hypertension 17.4 3 18.0 3 #0.6 0.116Irritable bowel 10.3 12 5.5 12 4.8 "0.001Migraine 13.1 8 7.2 10 5.9 "0.001Obesity 17.0 4 29.3 2 #12.3 "0.001Osteoporosis 2.8 20 1.6 21 1.2 "0.001Other cancer 2.4 22 2.1 19 0.3 0.076Other chronic pain 7.3 16 3.1 17 4.2 "0.001Skin cancer 3.2 19 0.7 22 2.5 "0.001Sleeping problem 11.4 11 5.7 11 5.7 "0.001Ulcer 5.0 17 2.4 18 2.6 "0.001
*T-test for pairwise differences between adjusted prevalences rs ! 0.89, P " 0.001.
TABLE 2Demographic Distributions
Phase 1 Phase 2
With Condition No Conditions Total With Condition No Conditions Total
N 14,434 520 14,954 24,439 10,183 34,622% 96.5% 3.5% 70.6% 29.4%Gender
Male 72.3% 76.0% 72.4% 56.0% 63.2% 58.1%Female 27.7% 24.0% 27.6% 44.1% 36.8% 41.9%
Age18–29 7.0% 7.1% 7.0% 12.7% 20.9% 15.1%30–44 58.3% 44.2% 57.8% 38.4% 44.4% 40.2%45–59 33.3% 47.9% 33.8% 42.9% 32.3% 39.8%!60 1.5% 0.8% 1.4% 6.0% 2.5% 4.9%
OccupationExecutive, administrator, senior
manager0.8% 6.9% 1.1% 8.3% 8.7% 8.4%
Professional 81.6% 39.6% 80.1% 47.1% 52.6% 48.7%Technical support 3.4% 8.5% 3.6% 12.1% 12.2% 12.3%Sales 0.5% 1.9% 0.6% 5.2% 6.1% 5.5%Clerical or administrative support 2.8% 8.3% 3.0% 14.1% 9.3% 12.7%Service occupation 0.3% 0.6% 0.3% 1.8% 1.5% 1.7%Precision production or craft workers 3.2% 8.9% 3.4% 2.9% 2.6% 2.8%Operator or laborer 7.3% 25.4% 7.9% 8.3% 7.0% 7.9%
416 Health and Productivity as a Business Strategy • Loeppke et al

1% who report such severe, but com-paratively uncommon conditions aschronic obstructive pulmonary dis-ease and CHF. The rank-order ofprevalence estimates is very similarin the two phases (rs ! 0.89, P "0.001). Four of the five most com-monly reported conditions are thesame in both phases. Seasonal aller-gies are reported to be the single mostprevalent condition in both phase 1(48.1%) and phase 2 (34.0%), withGastroesophageal Reflux Disease(GERD) (15.5% and 12.6%), hyper-tension (17.4% and 18.0%), and obe-sity (17.0% and 29.3%) also amongthe top five most common conditionsin both phases. The only discrepancyin the top five is arthritis, which is inthe top five in phase 2 (16.2%) butnot phase 1 (14.9%), and back orneck pain, which is in the top five inphase 1 (27.4%) but not phase 2(7.5%).
A plausible interpretation of thedifferences in the reported conditionprevalences between the phases isdue to the fact that, as noted above,respondents in phase 1 were asked ifthey experienced the condition,whereas respondents in phase 2 wereasked if a doctor ever told them theyhad the condition. For example, backor neck pain has a dramaticallyhigher prevalence in phase 1 thencompared with phase 2. As back orneck pain often goes undiagnosed, itwould not be surprising to find thatmany more people report having thiscondition than reporting being toldby a doctor they have the condition.
Consistent with this interpretation,prevalence estimates are higher inphase 1 than phase 2 for almost threequarters (18/25) of the conditions inthe checklist. Furthermore, thehigher prevalence in phase 1 has thegreatest magnitude for symptom-based conditions (ie, conditions thatare apparent to people who havethem without a doctor’s diagnosis)that are often not diagnosed ortreated by a physician, most notablyfatigue, irritable bowel and migraine,along with back or neck pain. Thedifference in the prevalence of obe-
sity between the phases (17.0% and29.3%) is in large part due to a differ-ence in methodology in which phase 1was based on self-reported obesity andphase 2 was calculated based on self-reported height and weight.
Table 3 also highlights similaritiesin the prevalences of certain conditionsconsistent with our expectations ofcondition reporting. The betweenphase prevalences of diabetes, hyper-tension, and other cancer are notsignificantly different from eachother. These conditions are often di-agnosed only by a doctor and there-fore we would not expect respondentto report these conditions without adoctor diagnosis.
It needs to be noted, though, thatthe differences in prevalence be-tween the two phases could also bedue to differences in any number ofother unmeasured variables that dif-fer between the two groups.
Estimates of AggregateBivariate Associations
The most basic regression equa-tions we estimated were bivariateequations that compared absenteeismand presenteeism scores of respon-dents with and without each condi-tion, one condition at a time, usingtwo kinds of comparisons. The firstcompared employees with the focalcondition to employees of the samegender, age and occupation who re-ported none of the conditions in ourchecklist. The second compared em-ployees with the focal condition toemployees of the same gender, ageand occupation who did not reportthe focal condition (but who mighthave reported other conditions).These comparisons were made sepa-rately in phase 1 and phase 2 forabsenteeism and presenteeism. Theregression coefficients for presentee-ism were converted into day-equiva-lents ($ ! days lost per year) so as tofacilitate comparison of coefficientsin the absenteeism and presenteeismequations. With 25 conditions, twosamples, and two outcomes (ie, ab-senteeism and presenteeism), we had
exactly 100 coefficients for each ofthe two comparison methods.
Several broad patterns can be seenon inspection of these coefficients(Table 4). First, the vast majority ofthe coefficients (98.5%) are positiveand statistically significant (88.5%)at the 0.05 level, documentingclearly that the conditions consideredhere are significantly associated withelevated absenteeism and presentee-ism. Second, every one of the coef-ficients in the model that comparesrespondents with condition to re-spondents with no conditions islarger than the parallel coefficient inthe model that compares respondentswith condition to respondents with-out focal condition. Third, roughlytwo thirds of the coefficients in themodel predicting presenteeism arelarger than in the parallel model pre-dicting absenteeism, although thispattern is confined in the modelswhere the comparison is with re-spondents with no conditions (76%)rather than the models where thecomparison is with respondentswithout focal condition (54%).Fourth, the coefficients based onanalysis of phase 2 are almost en-tirely (96%) larger than those basedon analysis of phase 1 when wefocus on absenteeism but for themost part smaller than those basedon phase 1 when we focus on pre-senteeism (80%).
The median value of the regres-sion coefficients for absenteeism are3.6 (phase 1) and 6.4 (phase 2) daysper year in models that comparerespondents with condition to re-spondents with no conditions. Thecomparable coefficients in modelsthat compare respondents with con-dition to respondents without focalcondition are 1.7 (phase 1) and 5.1(phase 2). The inter-quartile range(IQR; 25th–75th percentiles) of thecoefficients in absenteeism modelsthat make the first type of compari-son are 2.9 to 4.7 (phase 1) and 5.3 to10.8 (phase 2), whereas the IQR ofthe coefficients in models that makethe second kind of comparison are1.2 to 3.2 (phase 1) and 3.9 to 9.2
JOEM • Volume 51, Number 4, April 2009 417

TABL
E4
Estim
ates
ofA
ggre
gate
Biv
aria
teA
ssoc
iatio
nsby
Pha
sean
dC
ompa
rison
Gro
upP
hase
1P
hase
2
With
Con
ditio
nvs
No
Con
ditio
nsW
ithC
ondi
tion
vsW
ithou
tFo
calC
ondi
tion
With
Con
ditio
nvs
No
Con
ditio
nsW
ithC
ondi
tion
vsW
ithou
tFo
calC
ondi
tion
Abs
ente
eism
Pre
sent
eeis
mA
bsen
teei
smP
rese
ntee
ism
Abs
ente
eism
Pre
sent
eeis
mA
bsen
teei
smP
rese
ntee
ism
!S
E!
SE
!S
E!
SE
!S
E!
SE
!S
E!
SE
Alle
rgy
2.1*
0.7
7.0*
1.4
0.4
0.3
1.8*
0.5
2.3*
0.3
3.7*
0.4
1.1*
0.3
1.3*
0.4
Anx
iety
5.0*
1.0
13.2
*2.
03.
2*0.
67.
9*1.
15.
7*0.
59.
4*0.
64.
4*0.
47.
1*0.
5A
rthr
itis
3.6*
1.0
8.9*
1.6
1.8*
0.5
3.4*
0.9
5.3*
0.5
6.0*
0.6
4.1*
0.4
3.1*
0.5
Ast
hma
3.6*
1.2
9.1*
1.8
1.6*
0.5
3.3*
0.9
4.0*
0.5
4.4*
0.7
2.6*
0.5
1.6*
0.6
Bac
k/ne
ckpa
in2.
9*0.
89.
7*1.
61.
4*0.
35.
1*0.
67.
2*0.
66.
9*0.
75.
8*0.
54.
0*0.
7B
ladd
er/u
rinar
y4.
6*0.
910
.1*
1.9
1.8*
0.6
3.9*
1.0
5.3*
0.7
7.9*
0.9
3.4*
0.7
4.7*
0.9
Chr
onic
bron
chiti
s/em
phys
ema
3.9*
0.8
7.0*
2.2
1.7
1.0
1.5
1.7
19.2
*2.
513
.0*
3.4
16.1
*2.
88.
7*3.
6
Con
gest
ive
hear
tfa
ilure
3.0*
0.9
7.6*
2.6
1.1
1.3
1.1
2.5
28.4
*2.
316
.8*
3.0
25.7
*2.
512
.9*
3.2
CO
PD
6.7*
2.0
10.0
*4.
24.
52.
62.
84.
721
.1*
2.7
9.8*
3.8
18.7
*3.
16.
04.
0C
oron
ary
hear
tdi
seas
e6.
7*1.
911
.5*
3.8
4.5
2.9
2.4
3.7
14.6
*1.
14.
9*1.
312
.2*
1.0
1.3
1.3
Dep
ress
ion
5.9*
1.1
16.8
*1.
94.
0*0.
512
.9*
0.9
6.9*
0.5
12.9
*0.
65.
6*0.
410
.8*
0.6
Dia
bete
s2.
5*1.
07.
8*2.
00.
70.
82.
41.
46.
3*0.
74.
2*0.
94.
4*0.
60.
70.
8Fa
tigue
4.6*
0.9
15.4
*1.
83.
0*0.
510
.3*
0.9
10.8
*0.
712
.8*
1.0
9.2*
0.7
9.5*
0.9
GER
D2.
7*0.
69.
6*1.
71.
2*0.
43.
9*0.
85.
2*0.
56.
3*0.
63.
8*0.
43.
6*0.
5H
eada
che
3.8*
0.9
10.8
*1.
82.
2*0.
54.
8*0.
96.
6*0.
79.
6*0.
95.
1*0.
76.
6*0.
9H
yper
tens
ion
2.6*
1.0
8.2*
1.5
0.8
0.4
1.8*
0.8
3.7*
0.4
4.6*
0.5
2.2*
0.4
1.4*
0.5
Irrita
ble
bow
el3.
0*0.
712
.3*
1.8
1.1*
0.5
6.1*
0.9
5.6*
0.6
7.7*
0.8
3.9*
0.6
4.9*
0.7
Mig
rain
e3.
6*0.
88.
3*1.
71.
6*0.
52.
5*0.
96.
3*0.
66.
0*0.
84.
9*0.
63.
0*0.
7O
besi
ty3.
7*1.
29.
3*1.
62.
4*0.
54.
3*0.
93.
1*0.
45.
1*0.
52.
1*0.
33.
1*0.
4O
steo
poro
sis
2.5*
0.9
9.7*
2.6
#0.
41.
22.
52.
27.
5*1.
25.
7*1.
74.
2*1.
20.
31.
6O
ther
canc
er7.
6*2.
210
.1*
2.4
5.6*
1.1
3.2
1.9
9.8*
0.9
5.4*
1.2
7.6*
0.9
1.4
1.2
Oth
erch
roni
cpa
in6.
7*1.
514
.0*
1.9
5.3*
0.7
8.4*
1.2
12.9
*0.
910
.9*
1.2
11.1
*0.
97.
6*1.
2S
kin
canc
er1.
4*0.
65.
7*1.
8#
0.6
0.9
#0.
61.
612
.2*
1.7
8.5*
2.3
9.9*
1.8
5.1*
2.3
Sle
epin
gpr
oble
m3.
9*0.
912
.8*
1.7
2.5*
0.5
7.9*
0.9
6.2*
0.6
8.9*
0.8
4.4*
0.6
6.2*
0.7
Ulc
er3.
9*1.
09.
5*1.
91.
8*0.
73.
0*1.
37.
1*0.
94.
2*1.
25.
3*0.
90.
91.
2
*Sig
nific
ant
atth
e0.
05le
vel,
two-
side
dte
st.
418 Health and Productivity as a Business Strategy • Loeppke et al

(phase 2). The median value of theregression coefficients for presentee-ism, in comparison, are 8.8 (phase 1)and 6.9 (phase 2) days per year inmodels that compare respondentsWith condition to respondents withno conditions. The comparable coef-ficients in models that comparerespondents with conditions to re-spondents without focal conditionare 2.4 (phase 1) and 4.0 (phase 2).The IQR (25th to 75th percentiles) ofthe coefficients in presenteeismmodels that make the first type ofcomparison are 2.4 to 5.1 (phase 1)and 5.3 to 9.6 (phase 2), whereasthe IQR of the coefficients in mod-els that make the second kind ofcomparison are 2.4 to 5.1 (phase 1)and 1.3 to 6.6 (phase 2).
There is little consistency acrossthe two phases in the conditions thatare estimated to have the strongestadverse effects on work perfor-mance. This is perhaps not surprisinggiven the differences in sample com-position and in the assessment ofconditions. However, several consis-tencies in the results are especiallynoteworthy in light of this generallack of consistency. First, chronicobstructive pulmonary disease andCHD are found in both phases to beamong the strongest predictors ofabsenteeism but not among the stron-gest predictors of presenteeism. Sec-ond, depression and fatigue arefound in both phases surveys to beamong the strongest predictors ofpresenteeism but not among thestrongest predictors of absenteeism.Third, other chronic pain is found inboth phases to be among the stron-gest predictors of both absenteeismand presenteeism.
Estimates of DisaggregatedBivariate Associations Based onTreatment Status in Phase 2
We noted earlier that informationwas obtained in our surveys aboutwhether respondents received treat-ment for each of the conditions as-sessed in the checklist. The existenceof selection biases into treatment on
the basis of severity makes it impossi-ble to make inferences about treatmenteffects by comparing the outcomes ofpeople who did receive treatment tothe outcomes of people who did notreceive treatment. However, compar-ison of the effects of conditions inthe presence versus absence of treat-ment can nonetheless be helpful inconsidering potentially useful inter-vention targets.
If it turns out that the significantpositive association between the con-dition and reduced work perfor-mance is confined to respondentswho are in treatment for the focalcondition, then the most plausibleinterpretation is that severity of thecondition motivates people who aremost impaired by the condition toseek treatment. Any intervention toreduce the impairment caused bythe condition, in such a case, wouldhave to focus on treatment qualityimprovement.
In addition, a potential impact oftreatment on presenteeism andabsenteeism is when a physician pre-scribes work restrictions, work limi-tations or modified duty and whetherthe manager at the employer allowsthe employee to return to work be-fore they are fully recovered. How-ever, that typically is more relevantto injuries or acute illnesses ratherthan chronic illnesses.
If, however, it turns out that thesignificant positive association be-tween the condition and reducedwork performance is confined to re-spondents who are not in treatmentfor the focal condition, then the mostplausible interpretation is that treat-ment is effective and that furtherintervention should focus on increas-ing the proportion of cases that seektreatment. In the more typical casewhere the significant positive associ-ation between the condition and re-duced work performance is foundboth among those who are in treat-ment and those not in treatment,information about the relative sizesof the coefficients in the treatmentsub-samples and not-in-treatmentsub-samples can be used to evaluate
the opportunities associated withquality improvement versus screen-ing and outreach interventions.
Based on Treatment Status inPhase 2
Some indication of the complexi-ties encountered in carrying out dis-aggregated analyses of this sort canbe seen by considering the results ofbivariate analyses that compare re-spondents with focal conditions to re-spondents with no conditions in phase2 as a function of treatment status(Table 5). We see that all the coeffi-cients that are significant in the totalsample remain positively significantin the sub-sample of respondents notin treatment in predicting both ab-senteeism and presenteeism, that thevast majority of these same coeffi-cients remain positively significantin the sub-sample of respondentswho are in treatment with medication(92%), and that two thirds of thecoefficients remain positively signif-icant in the sub-sample of respon-dents who are in treatment withoutmedication.
Focusing on absenteeism, we seethat two thirds of the coefficients inthe sub-sample of respondents whoare not in treatment are smaller thanthose in one or both sub-samples ofrespondents who are in treatment.This pattern does not hold, though,for presenteeism, where there is nooverall difference in the coefficientsas a function of treatment (54% ofthe time the coefficient in the sub-sample not in treatment is larger thanthe sub-sample in treatment). Com-parative analyses of similar dataacross a number of different samplesmight find more subtle patterns ofconsistency related to particular dis-orders, possibly depending on partic-ular modalities of treatment.
Caution is needed in interpretingthese results, as treatment is not ran-domly assigned. It is likely thatworkers whose conditions are seri-ously impairing are more likely thanothers with the same condition toobtain treatment, leading to an up-
JOEM • Volume 51, Number 4, April 2009 419

ward bias in the estimate of theproductivity loss due to treated con-ditions. With this kind of underlyingselection process in mind, the mainconclusion we can draw from thesedata is that the significant positiveassociations of conditions with theoutcomes exist for the vast majorityof conditions regardless of treatmentstatus. Further, there is reason toassess the quality of care received bythose in treatment and try to identifyopportunities for improvement thatincludes reducing work impairment.
Estimates of DisaggregatedBivariate Associations Basedon Occupation
Another consideration is whetherpositive associations of health condi-tions with work performance vary by
employee socio-demographic char-acteristics, such as their gender, age,or occupation. We examine one suchpossibility here by focusing on occu-pation. As in the last section, weconsider the results of bivariate anal-yses that compare respondents withfocal condition to respondents withno conditions. Only two conditionsare considered, back or neck pain anddepression, as the analysis is per-formed only for illustrative purposes.Back or neck pain has its lowest prev-alence among Executives and Profes-sionals and its highest prevalenceamong Clerical and Services Workers.Depression, in comparison, has itslowest prevalence among Executivesand Precision Craft Workers and itshighest prevalence among ClericalWorkers and Laborers.
The slopes of absenteeism andpresenteeism on back or neck painand depression also vary signifi-cantly across the eight occupationsub-samples (F7,34,615 ! 3.7 and 6.9,P " 0.001). In the case of back orneck pain, the coefficient predictingabsenteeism is highest by far amongLaborers, whereas the coefficientpredicting presenteeism is highestamong Sales Workers and Laborers.The situation is different for depres-sion, where the coefficient predictingabsenteeism is highest among Ser-vice Workers and the coefficient pre-dicting presenteeism is highestamong Executives/Senior Managers.
When we monetized the sum ofslopes (ie, total days lost per year)for absenteeism and presenteeismcombined, though, we see an inter-
TABLE 5Estimates of Disaggregated Bivariate Associations Based on Treatement Status in Phase 2
Not Currently ReceivingTreatment
Currently Treated andMedication
Currently TreatedNo Medication
Absenteeism Presenteeism Absenteeism Presenteeism Absenteeism Presenteeism
! SE ! SE ! SE ! SE ! SE ! SE
Allergy 1.8* 0.3 4.1* 0.5 3.3* 0.4 3.2* 0.6 3.6* 0.8 2.7* 1.1Anxiety 4.0* 0.5 9.4* 0.8 7.5* 0.6 9.4* 0.8 8.8* 1.7 9.5* 2.4Arthritis 3.6* 0.5 6.1* 0.6 9.6* 0.9 5.8* 1.0 10.3* 1.1 7.3* 1.6Asthma 2.9* 0.6 4.9* 0.9 5.4* 0.7 3.7* 0.9 3.5* 1.3 5.1* 1.9Back/neck pain 3.6* 0.6 6.0* 0.9 15.9* 1.1 9.0* 1.4 9.5* 1.0 7.9* 1.4Bladder/urinary 3.6* 0.7 7.4* 1.0 9.8* 1.3 12.4* 1.9 12.5* 2.1 3.0 3.0Chronic bronchitis/
emphysema25.9* 2.8 17.9* 4.0 #1.0 5.1 #5.5 7.6 #2.7 9.9 12.0 14.6
Congestive heartfailure
30.9* 3.7 14.6* 5.2 29.2* 2.8 18.3* 3.8 #0.9 10.0 9.4 14.6
COPD 15.9* 3.5 11.2* 5.0 36.6* 4.7 7.6 6.7 2.6 8.1 8.9 11.9Coronary heart
disease11.2* 1.4 5.3* 1.9 17.4* 1.3 5.3* 1.7 7.7 4.8 #7.8 7.1
Depression 4.0* 0.6 11.2* 0.8 9.2* 0.6 14.3* 0.8 8.6* 1.7 13.3* 2.4Diabetes 8.4* 1.6 7.6* 2.3 6.4* 0.7 3.6* 1.0 2.9 1.9 5.3 2.7Fatigue 9.3* 0.8 12.2* 1.1 14.6* 1.4 13.2* 2.0 15.9* 2.3 17.1* 3.3GERD 4.7* 0.6 7.3* 0.8 5.8* 0.6 5.9* 0.7 4.6* 1.4 4.9* 2.1Headache 5.2* 0.8 9.4* 1.1 8.8* 1.1 9.1* 1.5 8.2* 1.8 12.1* 2.6Hypertension 2.5* 0.6 7.4* 0.9 4.2* 0.5 3.5* 0.6 1.8 1.7 5.6* 2.5Irritable bowel 5.8* 0.7 9.0* 0.9 6.1* 1.0 6.0* 1.4 2.3 1.5 4.7* 2.3Migraine 4.3* 0.7 5.0* 1.0 9.4* 0.9 8.1* 1.2 5.7* 1.4 4.8* 2.1Obesity†Osteoporosis 9.1* 1.8 7.5* 2.6 6.0* 1.5 4.9* 2.1 4.0 4.0 1.2 5.9Other cancer 5.3* 1.0 3.4* 1.4 26.1* 2.1 9.2* 2.8 13.8* 2.2 10.9* 3.3Other chronic pain 7.0* 1.2 8.2* 1.7 20.9* 1.4 14.4* 1.9 11.9* 1.8 10.8* 2.6Skin cancer 8.5* 1.8 8.3* 2.5 73.5* 7.7 23.0* 11.1 18.2* 4.6 4.8 6.7Sleeping problem 6.2* 0.8 8.1* 1.1 9.5* 1.4 10.8* 1.9 5.2* 0.8 9.0* 1.1Ulcer 6.6* 0.9 4.2* 1.3 7.4* 1.9 2.2 2.7 24.1* 5.2 18.3* 7.6
*Significant at the 0.05 level, two-sided test.†Treatment not available for obesity.
420 Health and Productivity as a Business Strategy • Loeppke et al

esting correlation. The average mon-etized lost productivity per year dueto depression is highest for Execu-tives ($15,889 compared with $3903to $11,646 for other occupationgroups). This reflects both the highsalaries of Executives and the highcoefficient associated with presen-teeism among Executives.
The average monetized lost pro-ductivity per year due to back orneck pain per employee with thatcondition is also found to be highestfor Executives.
Estimates of DisaggregatedBivariate Associations Basedon Comorbidity
Up to now we have consideredonly the aggregated associations in-volving individual conditions. Weknow, though, that many of the peo-ple with individual conditions alsohave comorbidities. It is conse-quently not clear from the resultsreported so far if the coefficientsassociated with individual conditionsare associated with those conditionsthemselves or with commonly occur-ring comorbid conditions. The healthand productivity literature has notdone a good job of distinguishingthese two possibilities. Given thelarge number of respondents in oursurveys, we are able to make a firstattempt at distinguishing associa-tions involving single and comorbidconditions. For this analysis, we de-fine a Single Condition as respon-dents having a single focal conditionand none of the other health condi-tions considered here; and a Comor-bid Condition as respondents havinga focal condition and at least oneother health condition. We estimateda series of bivariate models that com-pare respondents with single condi-tions and comorbid conditions torespondents with no conditions.
Two clear patterns emerge fromthese results (Table 6). First, the highprevalence of comorbidity is strik-ing, with over 90% of respondentswith a focal condition having one or
TABLE 6Estimates of Disaggregated Bivariate Associations Based on Comorbidity
Condition N
Absenteeism Presenteeism
! SE ! SE
AllergySingle 3,159 0.0 0.4 0.1 0.6Comorbid 8,655 3.2* 0.3 5.1* 0.5
AnxietySingle 257 #0.8 1.2 3.0 1.9Comorbid 3,383 6.2* 0.5 10.0* 0.6
ArthritisSingle 470 #1.1 0.9 1.5 1.4Comorbid 4,171 6.1* 0.6 6.7* 0.6
AsthmaSingle 184 #0.3 1.5 1.7 2.2Comorbid 2,452 4.3* 0.5 4.7* 0.7
Back/neck painSingle 170 2.0 1.5 4.8* 2.3Comorbid 2,070 7.6* 0.6 7.3* 0.8
Bladder/urinarySingle 140 #0.1 1.7 6.9* 2.5Comorbid 1,210 6.0* 0.7 8.1* 1.0
Chronic bronchitis/emphysemaSingle 8 #1.6 7.0 17.9 10.5Comorbid 68 21.6* 2.6 12.6* 3.7
Congestive heart failureSingle 5 #3.9 8.9 15.1 13.2Comorbid 91 30.2* 2.3 17.1* 3.2
COPDSingle 2 #2.6 14.0 #3.7 20.9Comorbid 58 22.0* 2.8 10.3* 3.9
Coronary heart diseaseSingle 60 12.0* 2.6 3.6 3.9Comorbid 529 14.9* 1.1 5.1* 1.4
DepressionSingle 254 1.9 1.3 12.2* 1.9Comorbid 3,302 7.2* 0.5 13.1* 0.7
DiabetesSingle 168 #0.1 1.5 #3.8 2.3Comorbid 1,285 7.3* 0.7 5.4* 0.9
FatigueSingle 35 #1.6 3.4 8.8 5.0Comorbid 1,190 11.2* 0.7 13.0* 1.0
GERDSingle 397 #0.6 1.0 0.2 1.5Comorbid 3,675 5.8* 0.5 7.1* 0.6
HeadacheSingle 60 0.7 2.6 7.6* 3.8Comorbid 1,324 6.9* 0.7 9.8* 0.9
HypertensionSingle 920 #0.4 0.7 1.1 1.0Comorbid 4,858 4.5* 0.5 5.3* 0.6
Irritable bowelSingle 195 #0.4 1.4 2.2 2.1Comorbid 1,619 6.4* 0.6 8.5* 0.8
MigraineSingle 170 2.2 1.5 6.4* 2.3Comorbid 1,884 6.7* 0.6 6.0* 0.8
ObesitySingle 2,196 #0.3 0.5 1.6* 0.7Comorbid 6,911 4.3* 0.4 6.4 0.5
OsteoporosisSingle 49 #2.5 2.9 0.6 4.3Comorbid 359 8.7* 1.3 6.4* 1.8
(continued)
JOEM • Volume 51, Number 4, April 2009 421

more comorbidities for 14 of the 25conditions considered here and atleast 75% of respondents with a focalcondition having one or more comor-bidities for the 11 other conditions.Second, there is a generally consis-tent pattern for the coefficients asso-ciated with the comorbid cases to behigher than those for the single con-ditions. This is true in 92% of thecomparisons in the table, the onlyexceptions being cancer in predictingabsenteeism and skin cancer, migraine,and ulcer in predicting presenteeism.In all four of these exceptions, thecoefficients associated with single andcomorbid conditions are very similarin magnitude.
For the vast majority of conditions,comorbid conditions are significantpredictors of either absenteeism (23 of25 conditions) or presenteeism (19 of25 conditions). The exceptions, wheresingle conditions are significant pre-dictors, are cancer and CHD in predict-ing absenteeism and back or neck pain,bladder or urinary infections, depres-sion, migraine, headache, and obesityfor presenteeism. This conjunction of ahigh proportion of cases being comor-bid and the associations of most con-ditions being confined to comorbidcases complicates efforts to pinpointthe source of the aggregate associa-tions of individual conditions withwork performance.
Estimates of MultivariateAssociations Basedon Comorbidity
Our investigation of the effects ofcomorbidity in the last section fo-cused on single versus comorbidconditions without considering thenumber or type of comorbidities. Wecan learn more by investigating theimplications of the extent of comor-bidity; that is, by considering theassociations between number of con-ditions and work performance. Re-sults of such an analysis are examinedhere as an extension of the expandedbivariate models considered in the lastsection. As in those models, we focuson the phase 2 sample, but this time weestimate a multivariate model that in-cludes a separate predictor that definesthe total number of conditions eachrespondent has out of those in thechecklist.
The distribution of the number ofconditions is highly skewed in thephase 2 sample. Among respondentswho reported having any of the 25health conditions more than threefourths had between one and threeconditions (37.7% one, 25.0% two,and 15.0% three); and the majority ofothers had either four (9.1%) or five(5.4%) (Table 7). Only 7.9% of re-spondents with conditions reportedsix or more of the 25 conditions. Theassociations between number of con-ditions and the outcomes are gener-ally monotonic.
The coefficients are consistentlyhigh for respondents with a largenumber of comorbid conditions. Infact, these coefficients are so highthat a substantial proportion of all thework impairment associated withthese conditions is concentratedamong respondents with high comor-bidity. This can be seen by focusingon absenteeism and multiplying thenumber of respondents with a givennumber of conditions by the coeffi-cient associated with that number ofconditions and summing that productacross number of conditions to arriveat the total number of annual absen-teeism days due to the conditions.
TABLE 6(Continued)
Condition N
Absenteeism Presenteeism
! SE ! SE
Other cancerSingle 120 11.5* 1.9 0.1 2.7Comorbid 585 9.4* 1.0 6.5* 1.3
Other chronic painSingle 14 7.8 5.3 9.9 7.9Comorbid 669 13.0* 0.9 11.1* 1.2
Skin cancerSingle 25 1.3 4.0 9.7 5.9Comorbid 149 14.0* 1.8 8.3* 2.5
Sleeping problemSingle 79 3.8 2.3 5.6 3.3Comorbid 1,729 6.3* 0.6 9.1* 0.8
UlcerSingle 65 #0.7 2.5 6.8 3.7Comorbid 632 8.0* 0.9 4.0* 1.2
*Significant at the 0.05 level, two-sided test.
TABLE 7Estimates of Multivariate Associations Based on Comorbidity
No. ofConditions N
Absenteeism Presenteeism
! SE ! SE
1 9,202 0.1 0.3 1.5* 0.42 6,102 1.4* 0.3 3.5* 0.53 3,666 3.1* 0.4 4.7* 0.64 2,217 4.4* 0.5 7.5* 0.75 1,322 5.9* 0.7 6.8* 0.96 807 6.6* 0.8 7.6* 1.17 470 8.0* 1.0 11.5* 1.58 280 8.7* 1.3 17.8* 1.99 157 14.7* 1.7 14.7* 2.510 or more 216 27.5* 1.6 9.9* 2.1
*Significant at the 0.05 level, two-sided test.
422 Health and Productivity as a Business Strategy • Loeppke et al

This sum is equal to roughly 57,300days of absenteeism. More than 33%of all these absenteeism days areconcentrated in the 7.9% of respon-dents with six or more conditions.Close to 50% of all absenteeism daysare concentrated among the 13.3% ofrespondents with five or more condi-tions. Similar, but somewhat less ex-treme, concentrations are found inexamining the associations of num-ber of conditions with presenteeism.
It should be noted that this modelassumes that all combinations ofconditions will be associated withthe same levels of absenteeism asany other. This assumption is almostcertainly incorrect, as we have al-ready seen that the effects of singleconditions vary substantially. SingleCHD and single other cancer, forexample, are each associated withmore than 2 weeks of absenteeismper year compared with 0 days asso-ciated with single allergies and sin-gle chronic bronchitis. It is difficultto imagine that a combination of twoconditions consisting of heart diseaseand cancer would be associated with
the same average number of absen-teeism days as a combination ofallergies and chronic bronchitis. Fur-ther analysis is consequently neededto develop a more realistic model ofthe effects of comorbidity. Such amodel would presumably include in-formation about both number of con-ditions and types of conditions,although the most reasonable specifi-cation of these joint effects remains tobe determined.
Top 10 Health Conditions byTotal Cost
To further explore findings fromour previous research7 that rankedthe health conditions with the great-est health-related workplace costs wereplicated portions of phase 1 with alarger sample of companies and em-ployees using an improved methodfor mapping medical and pharmacyclaims and an alternative method ofmeasuring productivity.
The results from combining medicaland pharmacy claim costs to absentee-ism and presenteeism costs found that
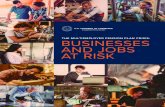
the following are the top 10 healthconditions in terms of total workplacecosts: depression, obesity, arthritis,back or neck pain, anxiety, GERD,allergy, other cancer, other chronicpain, and hypertension (Fig. 1).
When looking at the ratio of health-related productivity costs to medicaland pharmacy costs at a specific health-condition level across the 25 healthconditions, the ratios range widely—from greater than 20 to 1 to less than 1to 1. Combining costs across the 25health conditions show that on aver-age, for every 1 dollar of medical pluspharmacy costs there are 2.3 dollars ofhealth-related productivity costs in ab-senteeism and presenteeism. This find-ing falls in a range typically reported inprevious studies7,8 using alternativemethodologies.
Insights FromParticipating Companies
A company-specific health andproductivity report was provided andreviewed with every participatingcompany. This report documented
0 50000 100000 150000 200000 250000 300000 350000 400000
Depression
Obesity
Arthritis
Back/Neck Pain
Anxiety
GERD
Allergy
Other Cancer
Other Chronic Pain
Hypertension
Medical Drug Absenteeism Presenteeism
Fig. 1. Top 10 health conditions by annual medical, drug, absenteeism and presenteeism costs per 1000 FTEs for phase 2 companies.
JOEM • Volume 51, Number 4, April 2009 423

the health conditions driving thebroader medical, drug, absenteeismand presenteeism costs within theirworkforce. Some of the companiessubsequently provided us informationas to how they utilized their health andproductivity report in designing theircorporate health strategies.
Common themes from employers inthis study of what insights were gainedand how this integrated workforcehealth and productivity informationwas used include the following:
• Integration of their corporate healthstrategies is very important to them.Companies are seeking integratedsolutions that span the health contin-uum from wellness to complex care.Therefore this integrated informa-tion was used as the foundation forthe business case of justifying thecontinuation of current health-re-lated strategies as well as the blue-print for action of future initiatives.
• This integrated health and produc-tivity information was shared withmembers of their senior manage-ment and leadership teams oftenincluding members of their C-Suite(CEO, CFO, and COO).
• Employers found that the produc-tivity of their employees at work(presenteeism) was significantly im-pacted by behavioral health issues(eg, depression, anxiety, GERD, fa-tigue, sleep disorders etc.), height-ening the need for more integratedfocus in this area. In several casesthis led to integrating behavioralhealth resources through their Em-ployee Assistance Programs moreeffectively with their chronic condi-tion management providers.
• The study findings confirmed theneed to focus on obesity and cardio-metabolic risk reduction. Therefore,they increased efforts with workplace-based as well as on-line, phone-basedand community-based weight man-agement programs. In addition, someemployers communicated with localhealth care providers so they couldbetter leverage the provider-patientrelationship and one employer evenhelped providers establish diabetic
clinics and lipid clinics to reducemetabolic syndrome.
• Several employers are changingtheir benefit plan design to focusmore on health improvement bytrying to increase participation andmore active engagement of theiremployees in their wellness, healthmanagement, and condition man-agement programs.
• The companies with internationalworkforces are keenly interestedin health improvements and theirlink to productivity improvements.Therefore, even though in manycountries the employer does notdirectly pay for the medical andpharmacy costs of health care, thecosts of health-related productivityloss are compelling them to investin global health and productivityenhancement strategies.
• They also expressed interest inseeing a more broad based adop-tion of health-related productiv-ity metrics in the industry. Theywould like to see absenteeism andpresenteeism as additional outcomemeasurements for evidence basedmedicine and provider pay for per-formance criteria. They think theevidence used to determine bestpractices needs to go beyond clini-cal outcomes or financial outcomesand include functional outcomes—impacts on health and productivity.
• They realize that the impact of ahealthier, more productive workforceis quantifiable; when combinedwith other business measures ithelps determine the overall eco-nomic value of an enterprise. Theywould like to see the businesscommunity, ranging from finan-cial analysts to investors, developand institutionalize additional ac-counting and valuation methodsthat include health and productivitymetrics to more accurately deter-mine the business value of work-force health assets in a company.
• They would like to foster a sharingof findings and innovations amongthe employer community so theycan enjoy the economies of intel-lect and harness the collective con-sciousness of thought leadership inhealth and productivity strategies.
Employers want to have a con-sistent, ongoing approach formeasuring and benchmarkingtheir results as they design andimplement integrated health andproductivity improvement initiatives.Therefore, they are encouraging thedevelopment of benchmarking com-parison data sets and tools to helpevaluate their total health-related costsso they can make the business case fornecessary change as well as assess theimpact of their programs.
DiscussionAs noted in the introduction, the
purpose of the “Health and Produc-tivity as a Business Strategy” studywas to assess the full impact ofhealth conditions in the workplace,factoring in not only medical andpharmacy cost but also health-relatedproductivity costs such as absentee-ism and presenteeism. Phase 1 of thestudy supported the value of integrat-ing medical and pharmacy claimswith self-reported productivity to-ward understanding the full cost ofhealth conditions. In phase 2, weexpanded the power of the analysisby increasing the number of employ-ers and employees measured; furtherinvestigated observations regardingthe relationship of health and pro-ductivity; and explored a number ofmethodological refinements in de-termining health-related lost pro-ductivity and the full cost of healthconditions. We examined the impacton productivity of a more restrictivemethod of determining health condi-tions; two different comparisongroups; treatment status; occupa-tional differences; and comorbidities.We also offered insights from partic-ipating companies on how the studyhelped shape their corporate healthstrategies.
Overall in phase 2, we observedthat there are many factors that influ-ence the assessment of health-relatedlost productivity. When measuringthe magnitude of lost productivity itis important to understand the com-position of the comparison group. Acomparison group with no health
424 Health and Productivity as a Business Strategy • Loeppke et al

conditions will likely show greaterproductivity loss than a comparisongroup without the focal condition butwho may have other health condi-tions. Furthermore, analyses that fo-cus on employees with a specifichealth condition (which includesthose who may other comorbid con-ditions) show effect sizes to be largerthan when we focus on employeeswho exclusively have only that sin-gle focal condition. We know thatsome conditions are more likely tobe part of comorbid clusters thanothers merely by virtue of their highprevalence (eg, obesity, seasonal al-lergies), whereas other conditions aremore likely to be significantly inter-correlated with each other eventhough they are less prevalent in thetotal population (eg, depression—anxiety and back or neck pain—arthritis). These findings need to beconsidered when developing and re-fining measures of health-related lostproductivity.
This research gives employers apreliminary estimate of the likelyeffects of particular health conditionson work performance. This informa-tion can be used to help target specifichealth conditions for interventioneven though they are clearly imper-fect models. We can also developtailored models that focus on partic-ular conditions if we have reason tobelieve that these conditions are im-portant or if new interventions exist.A good case in point is the modelthat was recently developed to eval-uate the possible workplace effectsof interventions to detect and treatworkers with adult ADHD.19 Modelswith a specific focus will inevitablybe easier to develop than general-purpose models that consider all co-morbidities among all conditions. Inthe ideal case, these interventionsshould be evaluated experimentally,but this will seldom be practical incommercial applications. Nonethe-less, it should be feasible to obtainquasi-experimental evidence basedon before-after case-control compar-isons that closely approximate thekinds of evidence one can obtain
from experimental studies. Thisstudy is an intermediate phase in theprogression to those quasi-experi-mental studies.
Our study demonstrated that a sub-stantial proportion of the productiv-ity loss due to health conditions isfound in people with other comorbidconditions, it poses a challenge forfuture non-experimental research onthe effects of health problems onwork performance. A sound ap-proach is needed to investigate thejoint effects of comorbid conditionson full health-related costs. Thiswould be important where the medi-cal conditions have insignificant as-sociations with work performanceand where it is likely that effects ofcomorbid condition clusters arefound to be a joint function of bothnumber of conditions in the clusterand types of conditions in the cluster.Therefore, future research should ex-plore several aspects related to comor-bidity such as which health conditionstend to cluster together in people, howdo different combinations of condi-tions impact productivity, do certainconditions have a greater synergisticimpact and what are the best methodsto allocate lost productivity cost tohealth conditions?
Moreover, research should im-prove the understanding of potentialconfounding variables such as sever-ity of condition, treatment and healthbehavior variations, and the relation-ship of lifestyle health risks to pro-ductivity loss. Finally, as this andother studies have demonstrated thevalue of integrating data from multi-ple sources, data sources should beexpanded to include health-relatedproductivity impacts when consider-ing value based benefit plan design,time off policies and measures ofcorporate culture.
In addition to the methodologicalcontributions, the results of thisstudy continue to support the needfor a new, productivity-focusedhealth model in the workplace and anew language and methodology tohelp determine the true business valueof health. Based on the quantitative
findings from the measurement ofhealth-related lost productivity and thequalitative findings from interviewswith participating employers we offerinsights that employers can consider asthey evolve their employee healthstrategies.
1. Health conditions have impact be-yond medical and pharmacy costs.For several years, the focus on ap-propriate approaches to preventionand treatment of chronic conditionshas focused entirely on potentialgains in medical and pharmacycost savings. This research em-phasizes that health-related lostproductivity (absenteeism andpresenteeism) are costs employerscannot ignore. At an aggregatepopulation level across the 25health conditions assessed in phase2, the results show that on average,for every 1 dollar of medical andpharmacy costs there are 2.3 dollarsof health-related productivity costsin lost work time from absenteeismand presenteeism. Employers needto explore new ways of integratingabsence and presenteeism data intotheir current data collection andevaluation strategies.
2. Presenteeism relative to absencelost time is not trivial. For em-ployers, absence has always beena tangible—and observable—consequence of poor health. Thisresearch, consistent with severalresearch studies published overthe past several years, emphasizesthat presenteeism is typically ofgreater consequence to the em-ployer than absence. This realitypresents challenges to employersthat are skeptical of employeeself-reports as valid sources ofdata. However, with the growingnumber of validation studies ofself-reporting tools, employersmust find ways to integrate pre-senteeism management into theirhealth strategy approaches. Be-cause employers are hesitant toundertake multiple surveys of em-ployees, they may want to integratevalid absence and presenteeism
JOEM • Volume 51, Number 4, April 2009 425

self-reporting questions into thehealth-risk assessments and otherself-reporting tools.
3. Opportunities to improve produc-tivity may be found both in thestrategies for delivering medicalcare and in access to treatment.The research suggests that peoplewith chronic conditions undertreatment still have work impair-ments manifesting as absence andpresenteeism lost time. The datado not inform us as to whetherthis is due to sub-optimal care.However, research published inthe New England Journal of Med-icine in 2003 suggests that onlyabout half of people gettingtreatment receive recommendedcare.20 This finding indicates thatthere are opportunities to improvehealth-related lost productivitythrough more effective medicalcare to those in treatment—whether through improved qual-ity, more effective plan designs ormore active patient engagement.At the same time, those withchronic conditions not beingtreated also experience lost timefrom absence and presenteeismsuggesting that employers oughtto consider screening and out-reach interventions to encourageemployees to seek treatment. Em-ployers will need to address howbest to distribute scarce healthmanagement resources betweenimproving strategies for care andimproving access to treatment.
4. The complexity and impact ofcomorbidities must be recog-nized in any health managementapproach. Employers are in tran-sition in their approach toworkforce health management.Employers started with a singu-lar focus on controlling medicalcosts, transitioned to managingindividual diseases and havebroadened to population healthmanagement. Whatever the ap-proach individual employersand their supplier partners take,they must account for the impactof comorbidities. This research
shows that, for the sample stud-ied, employees with one comor-bid condition comprise nearly40% of comorbid cases and gen-erate about 15,600 lost days fromabsence and presenteeism. Em-ployees with six or more comor-bidities make up about 8% of thegroup but contribute more than36,000 lost days. Although morecomorbidities generally are asso-ciated with more lost time, thetypes of conditions grouped to-gether matter just as much if notmore. An important next step is toinvestigate groupings of comor-bidities and whether managementapproaches can be developed tominimize full costs of these co-morbid condition groups.
5. What information is important toemployers? Employers can usetheir medical and pharmacyclaims data as a window intomedical care expenses but theyalso need to integrate employeeself-reported data on health con-ditions and their associated lost-time implications for the morecomplete view of the impact ofhealth conditions on health-re-lated costs. Employees reportingtheir own medical conditions tendto show higher condition preva-lence over a variety of conditionscompared to a more limited viewof having a physician diagnosethe problem. Yet both sources ofinformation show significantamounts of absence and presen-teeism lost productivity.
6. Analysis of non-experimentaldata is limiting. Cross-sectional,non-experimental data such asthose reported here are a goodstarting point for employers todevelop intervention strategies,particularly around whether tar-gets should focus on conditionsassociated with high prevalenceor low average lost time or lowprevalence or high average losttime. However, cost-effective-ness of the intervention is key inthis decision: high-cost strate-gies aimed at conditions with
high prevalence or low time willhave limited cost-effectiveness.
7. Not all lost time is equal. Theresearch also indicates that em-ployers need to look beyond sim-ply the amount of lost time butalso to the occupations and com-pensation of those losing time tounderstand the true productivityloss costs. Highly compensatedindividuals with concomitant highopportunity costs of lost time maybe good targets for interventionseven when condition prevalencemay be low.
8. Primary, secondary, and tertiaryprevention are all critical needs.Examples include: 1) Primaryprevention of obesity and otherhealth risks through wellness, 2)Secondary prevention of earlierdiagnosis of conditions throughscreening, and 3) Tertiary preven-tion of disabling and high totalcost conditions through earlierand higher quality of care withevidence based medicine.
We realize there may be selectionbias in the employers that partici-pated in this study by the mere factthey were interested in measuring theimpacts of health conditions on theproductivity of their workforce. Assuch, these employers may be moreattuned to advanced corporate healthstrategies. However, we see an in-creasing number of employers of allsizes interested in how to leveragetheir investments in the health oftheir workforce as a key businessstrategy with economic value to theirenterprise.
As an example, Eastman Chemi-cal Company, one of the employersthat participated in this study, sum-marizes its health strategy verysuccinctly:
“Our health strategy is about the value ofhealth. There are two broad categories offocus: improving the health of our people,and improving the quality of health careoutcomes.
The first component is changing the waypeople think about their health; motivatingpeople to become more engaged in activelymanaging their health; increased focus on
426 Health and Productivity as a Business Strategy • Loeppke et al

prevention, identifying and addressing healthrisks, and managing chronic conditions.
The second component is improving thequality of health care in the U.S. by helpingdrive systemic change in the way care isdelivered. This involves more transparencywith regard to cost and quality of care;achieving consensus on consistent measure-ment standards for quality care; advancingthe use of health information technology toenable clinicians to provide better and moretimely medical decisions; and revamping thereimbursement process to pay for resultsrather than activity.
If we focus on these two areas, ie, if weare successful in improving the health of ourpeople and the quality of care they receive,then cost improvement will follow.
In summary:IF . . . . .
• Health: prevention & managing healthrisks
• Quality: health care outcomes & delivery
THEN . . . . .
Cost improvement will follow”
LimitationsWe recognize there may be selec-
tion bias that cannot be accounted forin both the employers that volun-teered to participate in this study aswell as the employees within theparticipating companies that volun-tarily completed the HRA that in-cluded the HPQ. Survey responserates for some employers in the studywere less than optimal. Consequently,those employees that did respond maybe a unique group and not representa-tive of the employee population as awhole. However, when total employeepopulation eligibility data was ana-lyzed, we found the age, gender, andoccupation distribution demographicsof the respondents were reasonablyconsistent with the total employeepopulation demographics of the partic-ipating companies. Furthermore, thecontrols for age, gender, and occupa-tion were included in all the regressionequations used in our analysis of thedata for this article. Even with therefinements in the methodology to al-locate pharmacy costs, it is still possi-ble some of the pharmacy costs aremisallocated among conditions.
Annualizing absenteeism and pre-senteeism assumes that the 1 monthmeasured is representative of thewhole year. This may not be the case
due to seasonal variation, especiallyas HPQ surveys are typically carriedout at a point in time rather thanthroughout the year. This problemcould be addressed by administeringHPQ surveys of workers’ birthdaysor anniversary date of being hired orin some other way that spreads outthe surveys throughout the year, butour experience is that employers pre-fer one-short administration thatleaves us with the problem of possi-ble seasonal variation in associa-tions. The coefficients associatedwith some conditions (eg, seasonalallergies) are more likely to be af-fected than others, but the problemhas to be recognized as of potentialimportance in evaluating the associ-ations involving all conditions andcomorbidities.
ConclusionsAs employers assess their em-
ployee health strategies, they willfind that their most compelling costissue is the link between poor healthand reduced productivity. Findingsfrom phase 1 of this study showedthat on average, for every 1 dollaremployers spend on worker medicalor pharmacy costs, they absorb 2 to 4dollars of health-related productivitycosts. These costs are manifestedlargely in the form of presenteeismabsence. Our earlier research alsoshowed that in addition to commonchronic conditions such as cancer,heart disease and diabetes, a host ofother conditions—ranging from mus-culoskeletal or pain, depression, andfatigue to anxiety and obesity—are themost significant drivers of total health-related costs in the workplace.7
Phase 2 of this study refines thosemethods and examines variations bytreatment, comorbidities and occupa-tions, providing further validation tothe concept of health and productiv-ity as a business strategy.
Employers of all sizes and types canuse strategies based on the relationshipbetween health and productivity tolower health risks, reduce the burdenof illness, improve wellness and hu-man performance, and enhance the
quality of life for workers and theirfamilies, while reducing total health-related costs. Such programs help em-ployers more accurately determinewhich health conditions have thegreatest impact on overall productivityand then design strategies to help theiremployees prevent or better managethese conditions.
As employers seek to gain a betterunderstanding of key medical careissues, they struggle with sources ofinformation on workforce health.Traditionally, employers and theirsupplier partners have relied uponmedical and pharmacy claims data astheir window into employee health.As employers have broadened theirattention to health risks and “busi-ness-relevant outcomes” such as pro-ductivity, they are looking to newsources of information. Employeeself-reported data, such as found inHRAs and absence and presenteeismmeasurement tools are becoming animportant part of the employer’s toolchest of information.
In an environment in which healthcosts are skyrocketing, health pro-motion and health protection measuresaimed at the nation’s workforce couldhave significant long-term impact,potentially saving billions in costs.Furthermore, the positive impact ofreaching large populations throughthe workplace extends beyondthose currently employed. Familiesof the employed, retirees and otherbeneficiaries could also benefitfrom integrated health and produc-tivity strategies implemented bythe nation’s employers.
The fundamental philosophy driv-ing the adoption of these strategies isthat health is not only of great valueto individuals and populations, butalso of great value to business andindustry. It is important for all em-ployers—whether small, medium orlarge—to look beyond health carebenefits as a cost to be managed andrather to the benefits of good healthas an investment to be leveraged.Ultimately, a healthier, more produc-tive workforce can help drive greater
JOEM • Volume 51, Number 4, April 2009 427

profitability for employers as well asa healthier economy for our nation.
AcknowledgmentWe want to thank Gary Persinger and
Jeffrey Warren, MPA, of the National Phar-maceutical Council as well as Dr PamelaHymel, Corporate Medical Director of CiscoSystems and Paul Larson of ACOEM for theirassistance in providing review and commentduring the study and the development of thismanuscript. We also thank David Sensibaugh,Director of Integrated Health at EastmanChemical Company for participating in thestudy and sharing his company’s health strat-egy to be included in this paper.
The study is funded by the National Phar-maceutical Council, a research and educationorganization supported by more than 20 of thenation’s leading research-based pharmaceuti-cal companies.
References1. Blumenthal D. Employer-sponsored in-
surance—riding the Health Care Tiger.N Engl J Med. 2006;355:195–202.
2. Thorpe KE. Factors accounting for therise in health-care spending in the UnitedStates: the role of rising disease preva-lence and treatment intensity. PublicHealth. 2006;120:1002–1007.
3. Partnership for Solutions National ProgramOffice. Chronic Conditions: Making theCase for Ongoing Care: September 2004Update. Baltimore, MD: Partnership forSolutions, John Hopkins University; 2004.
4. Loeppke RR. The value of health and the
power of prevention. Int J WorkplaceHealth Manage. 2008;1:95–108.
5. Fronstin P, Collins SR. Findings From the2007 EBRI/Commonwealth Fund Consum-erism in Health Survey. New York, NY:The Commonwealth Fund; 2008.
6. Bureau of Labor Statistics. The Employ-ment Situation: December 2008. Washing-ton, DC: US Department of Labor; 2009.
7. Loeppke RR, Taitel M, Richling DE, etal. Health and productivity as a businessstrategy. J Occup Environ Med. 2007;49:712–721.
8. Edington DW, Burton WN. Health andProductivity. A Practical Approach toOccupational and Environmental Medi-cine. Philadelphia: Lippincott Williams& Wilkins; 2003:140–152.
9. Kessler RC, Barber C, Beck A, et al. TheWorld Health Organization Health andWork Performance Questionnaire (HPQ).J Occup Environ Med. 2003;45:156–173.
10. Kessler RC, Ames M, Hymel PA, et al.Using the World Health OrganizationHealth and Work Performance Question-naire (HPQ) to evaluate the indirectworkplace costs of illness. J Occup En-viron Med. 2004;46:S23–S37.
11. Schoenborn C, Adams P, Schiller J.Summary health statistics for the U.S.population: National Health InterviewSurvey, 2000. Vital Health Stat 10.2003;(214):1– 83.
12. National Center for Health Statistics. Na-tional Health Interview Survey. Hyatts-ville, MD: United States Department ofHealth and Human Services; 2004.
13. Knight M, Stewart-Brown S, Fletcher L.Estimating health needs: the impact of a
checklist of conditions and quality of lifemeasurement on health information de-rived from community surveys. J PublicHealth Med. 2001;23:179–186.
14. Baker M, Stabile M, Deri C. What doself-reported, objective measures of healthmeasure? Cambridge, MA: National Bu-reau of Economic Research; 2001.
15. Edwards W, Winn D, Kurlantzick V, etal. Evaluation of National Health Inter-view Survey Diagnostic Reporting. VitalHealth Stat 2. 1994;120:1–116.
16. Revicki DA, Rentz AM, Dubois D, et al.Gastroparesis Cardinal Symptom Index(GCSI): development and validation of apatient reported assessment of severity ofgastroparesis symptoms. Qual Life Res.2004;13:833–844.
17. Villanueva EV. The validity of self-reported weight in US adults: a popula-tion based cross-sectional study. BMCPublic Health. 2001;1.
18. Nicholson S, Pauly MV, Polsky D,Sharda C, Szrek H, Berger ML. Measur-ing the effects of work loss on productiv-ity with team production. Health Econ.2006;15:111–123.
19. Kessler RC, Adler L, Ames M, et al. Theprevalence and effects of adult attentiondeficit/hyperactivity disorder on workperformance in a nationally representa-tive sample of workers. J Occup EnvironMed. 2005;47:565–572.
20. McGlynn EA, Asch SM, Adams J, Kee-sey J, DeCristofaro AH, Kerr EA. Thequality of health care delivered to adultsin the United States. N Engl J Med.2003;348:2635–2645.
428 Health and Productivity as a Business Strategy • Loeppke et al