
Healing of apical tissues after root canal...
117
Healing of apical tissues after root canal treatment Domenico Ricucci MD, DDS Dansk Endodontiforening Hindsgavl Slot d. 8. -9. januar 2016
Transcript of Healing of apical tissues after root canal...
Healing of apical tissues after root
canal treatment
Domenico Ricucci MD, DDS
Dansk EndodontiforeningHindsgavl Slot d. 8. -9. januar 2016
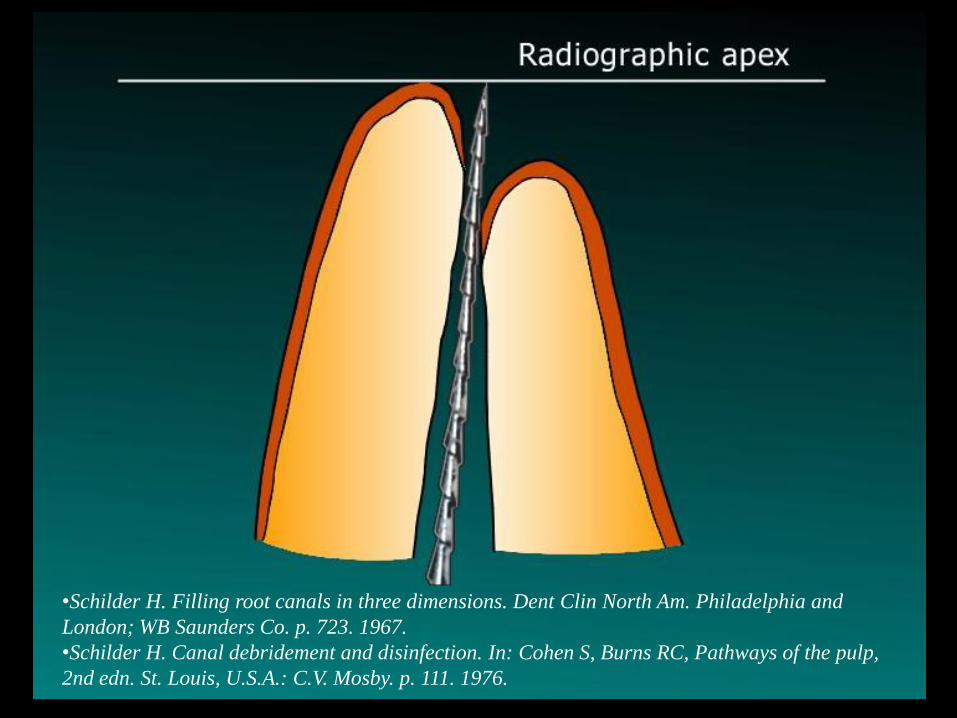
•Schilder H. Filling root canals in three dimensions. Dent Clin North Am. Philadelphia and
London; WB Saunders Co. p. 723. 1967.
•Schilder H. Canal debridement and disinfection. In: Cohen S, Burns RC, Pathways of the pulp,
2nd edn. St. Louis, U.S.A.: C.V. Mosby. p. 111. 1976.
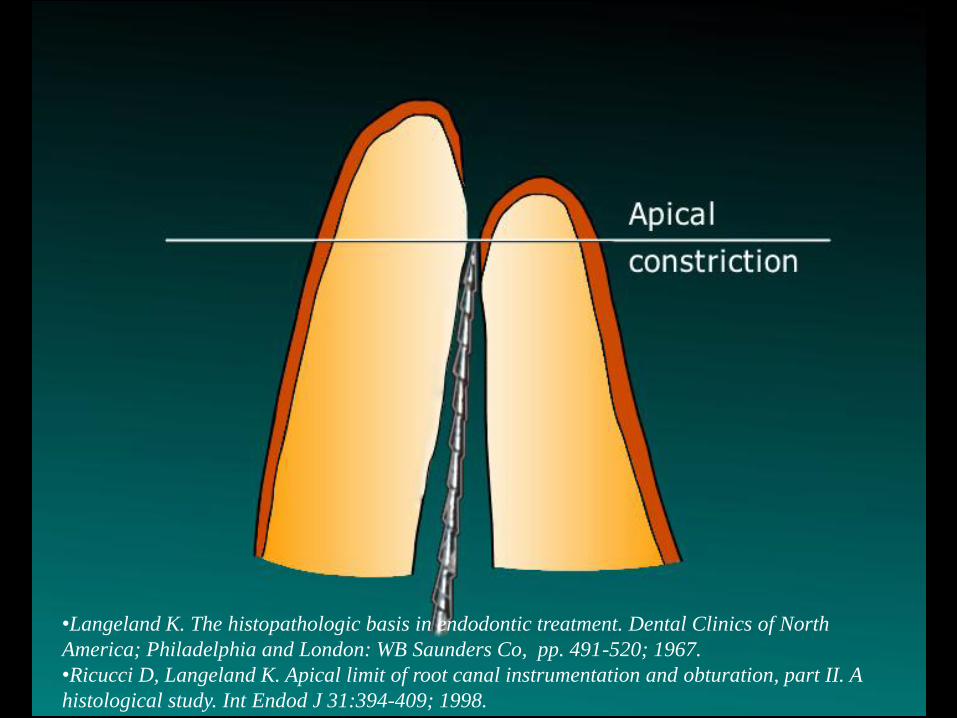
•Langeland K. The histopathologic basis in endodontic treatment. Dental Clinics of North
America; Philadelphia and London: WB Saunders Co, pp. 491-520; 1967.
•Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation, part II. A
histological study. Int Endod J 31:394-409; 1998.
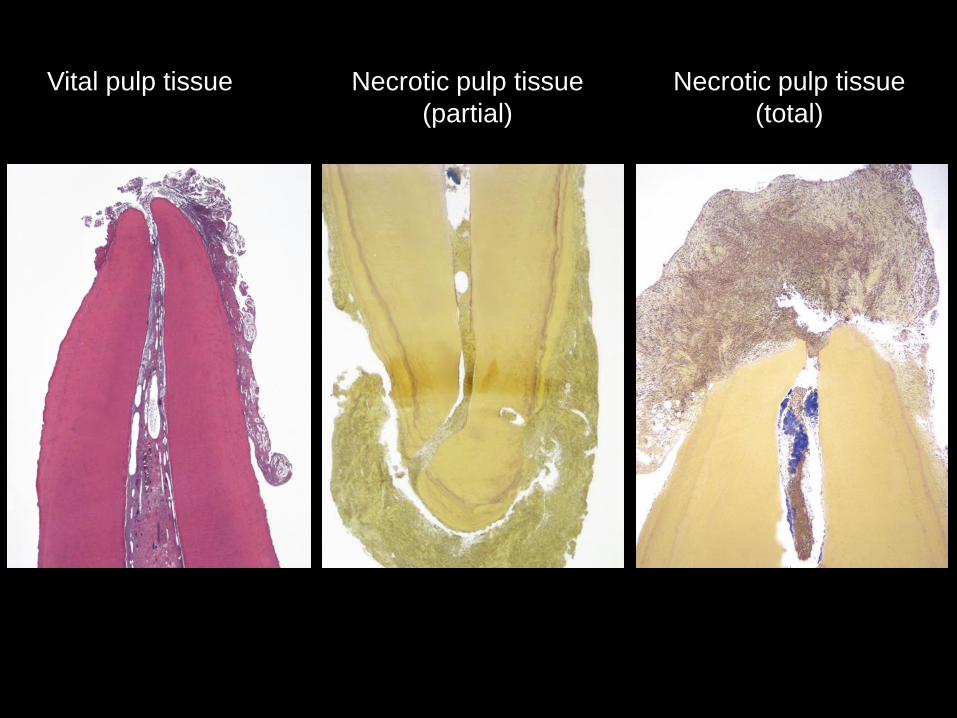
Vital pulp tissue Necrotic pulp tissue
(partial)
Necrotic pulp tissue
(total)
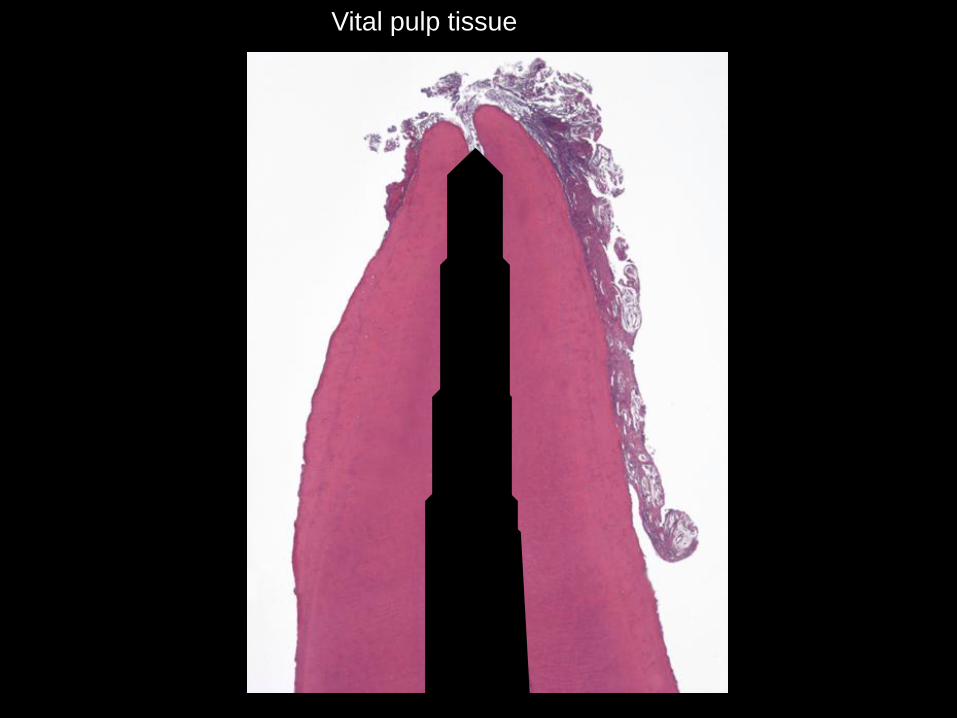
Vital pulp tissue
“To leave the apical and foraminal part of the pulp tissue and to retain
its vitality will play a decisive role for the success in the treatment of
the vital pulp.” “In cases where the pulp is vital before treatment, no
matter whether the diagnosis be clinically intact pulp, acute or chronic
pulpitis, partial extirpation seems to give the most favourable
prognosis. By appropriate treatment, in the majority of cases, the
vitality of the residual pulp may be conserved, the result being a
normal apical periodontal ligament and fibrous connective tissue in
the apical portion of the root canal.”
NYGAARD-ØSTBY B (1944) Om vevsforandringer i det apikale
paradentium hos mennesket ved rotbehandling. Nye kliniske,
røntgenologiske og histopatologiske studier. Det Norske
Videnskaps-Akademi. 2, 57; Oslo.
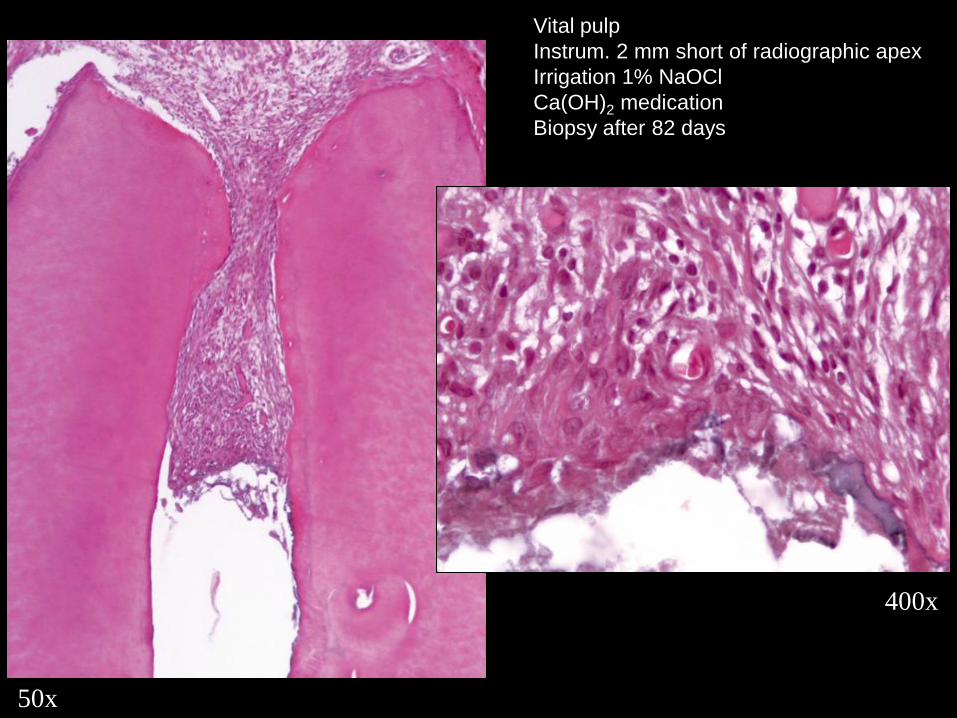
50x
400x
Vital pulp
Instrum. 2 mm short of radiographic apex
Irrigation 1% NaOCl
Ca(OH)2 medication
Biopsy after 82 days
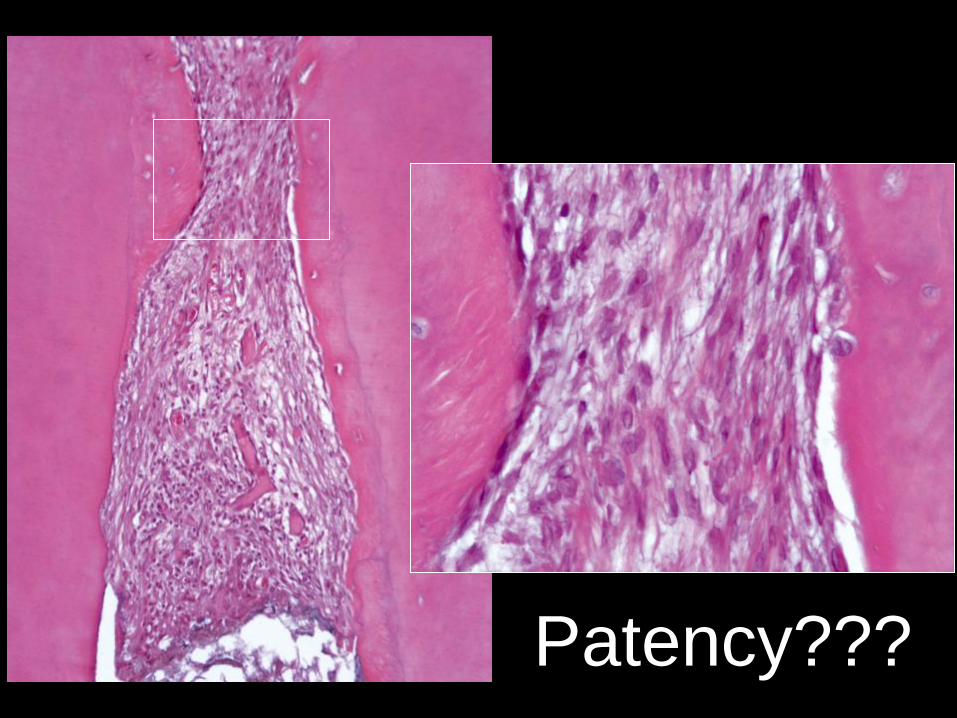
Patency??? Patency???
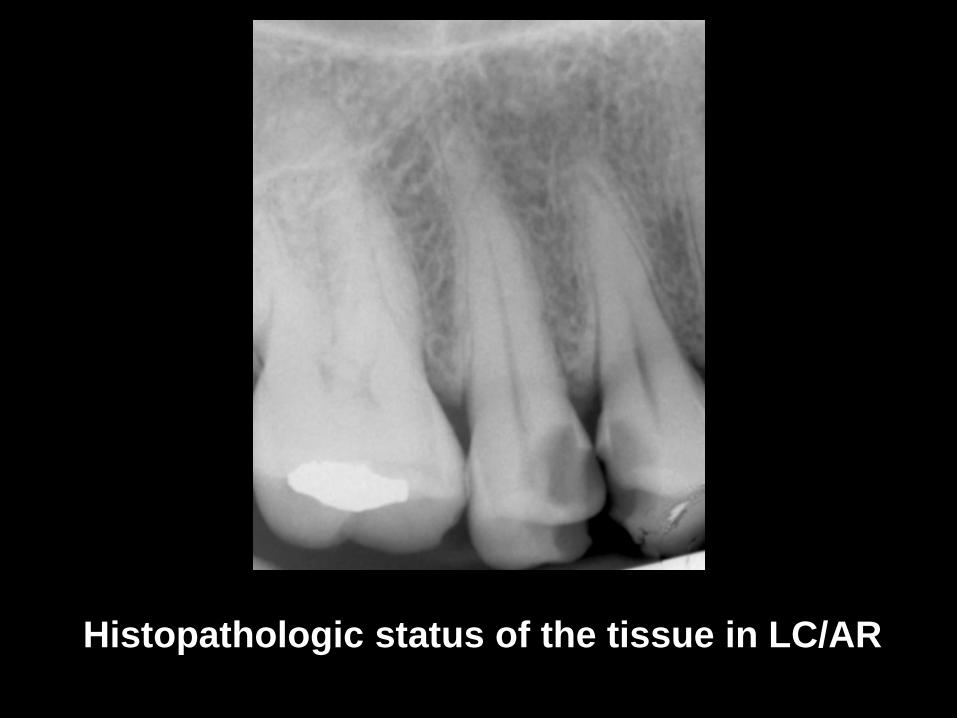
Histopathologic status of the tissue in LC/AR
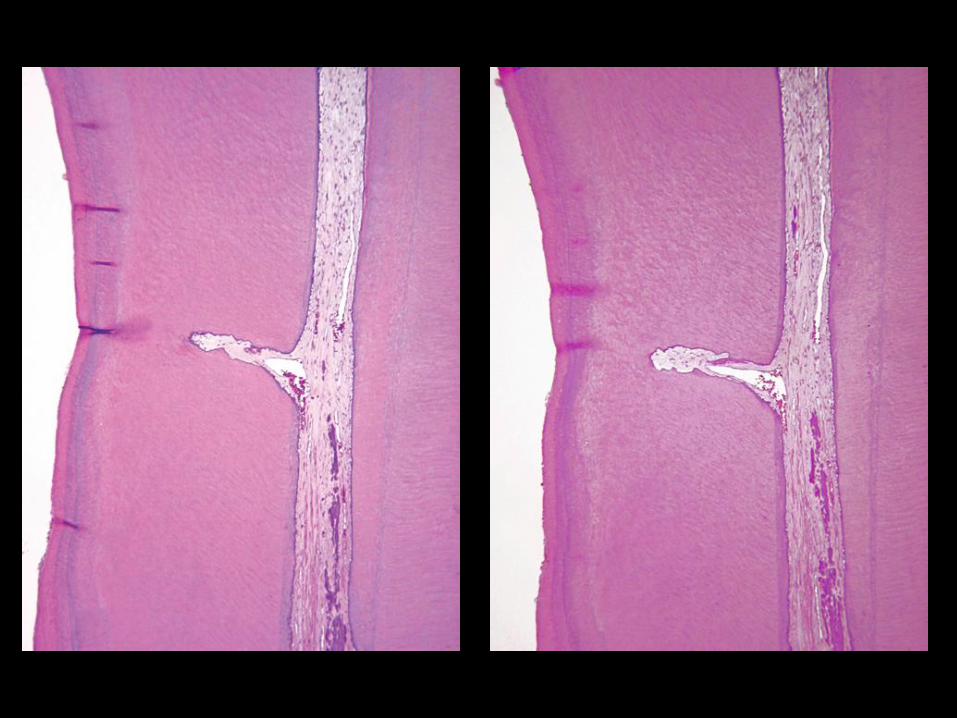
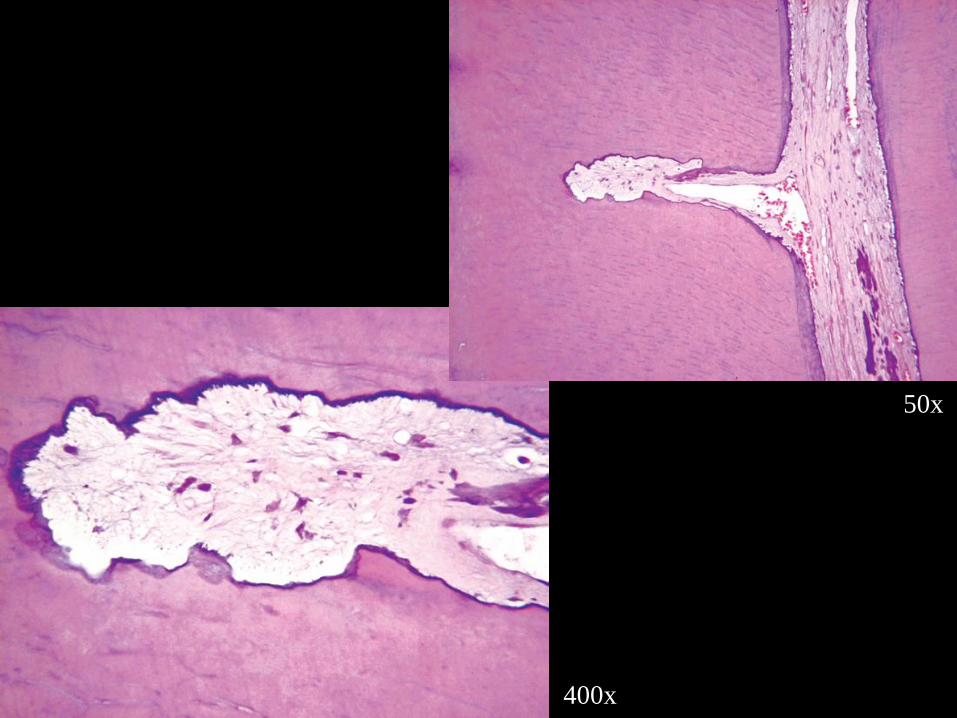
50x
400x
1
2
3
1
2
3
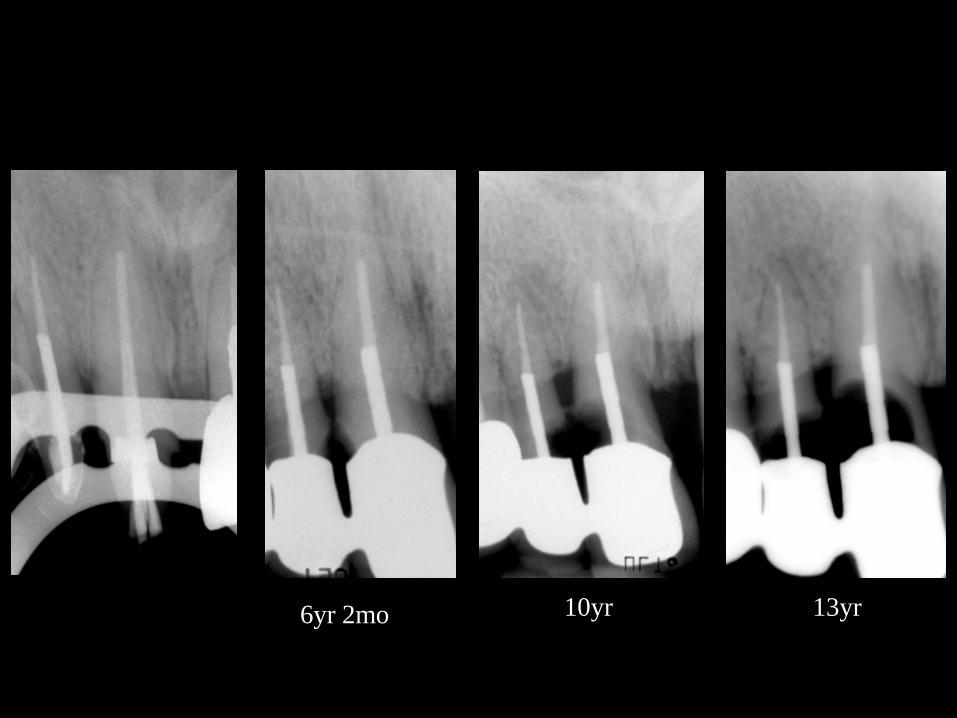
13yr6yr 2mo 10yr
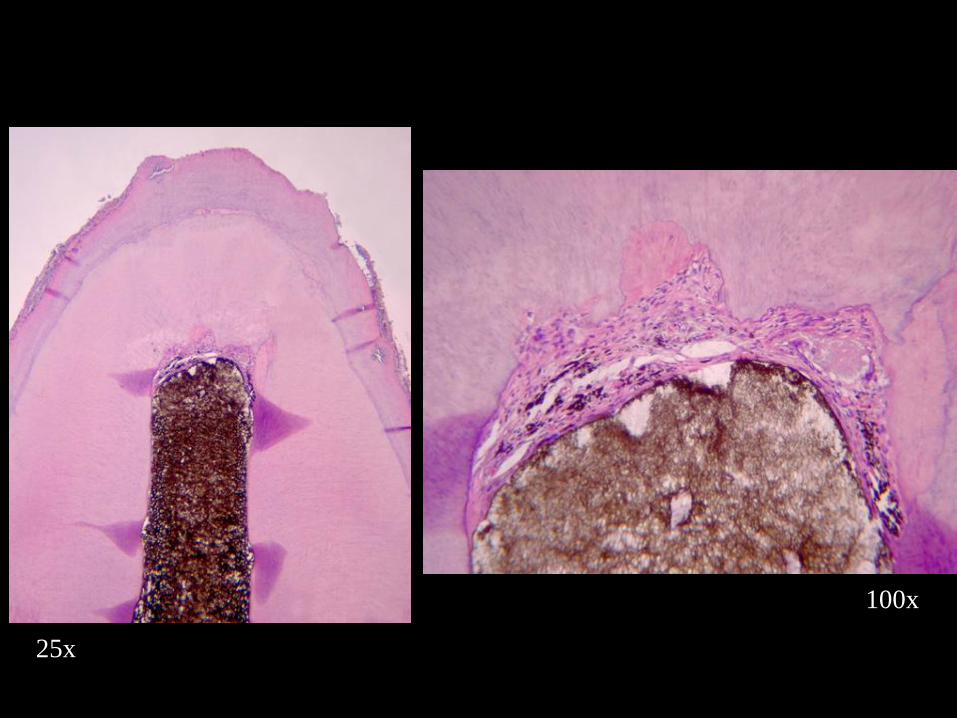
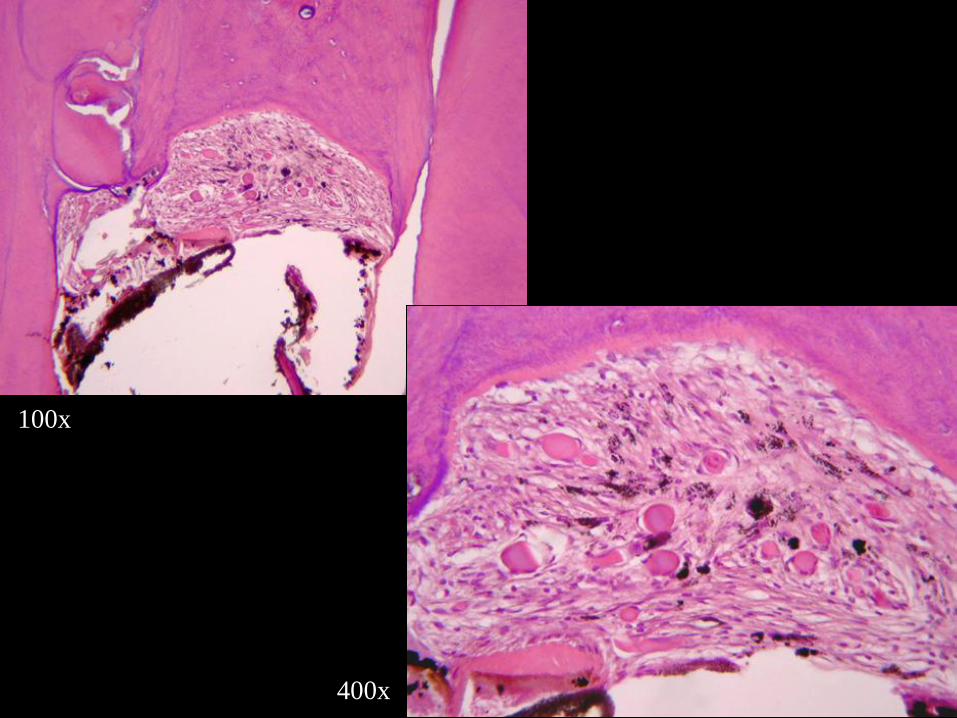
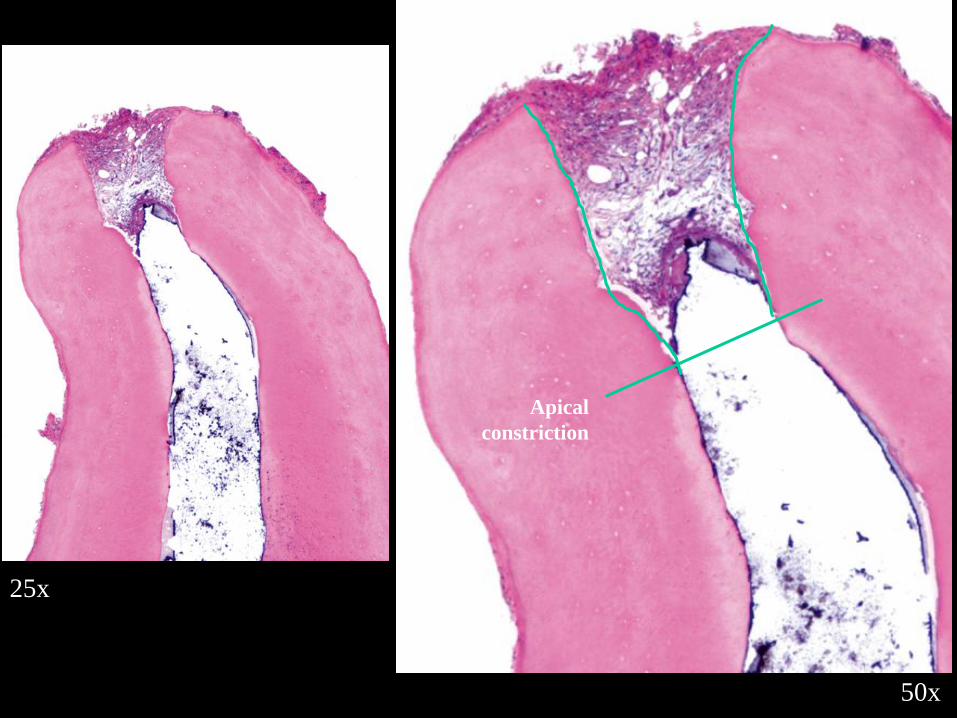
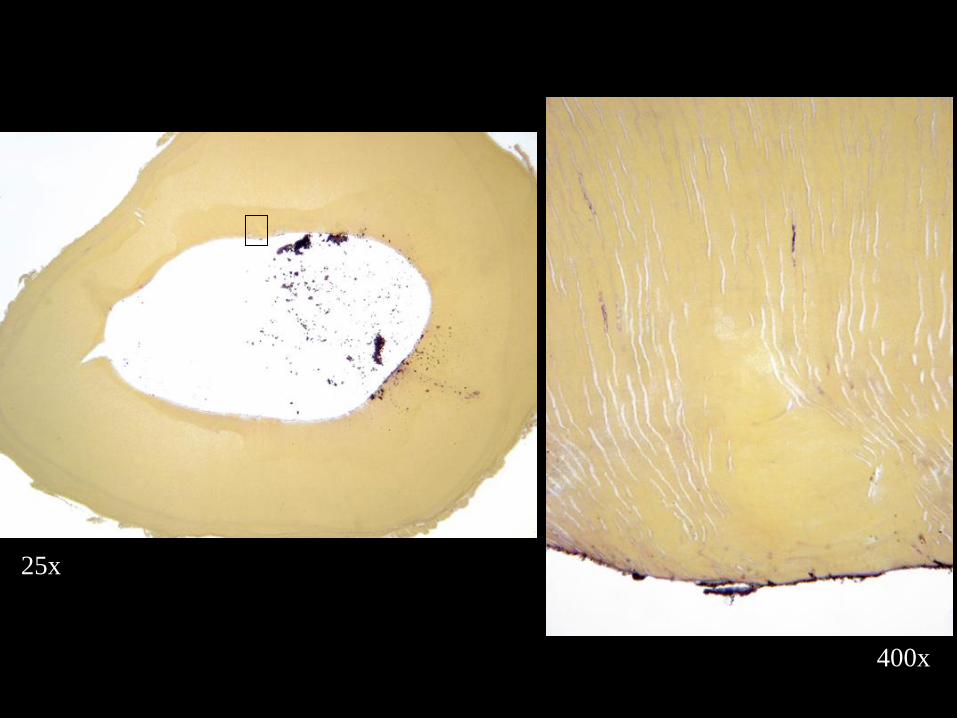
25x
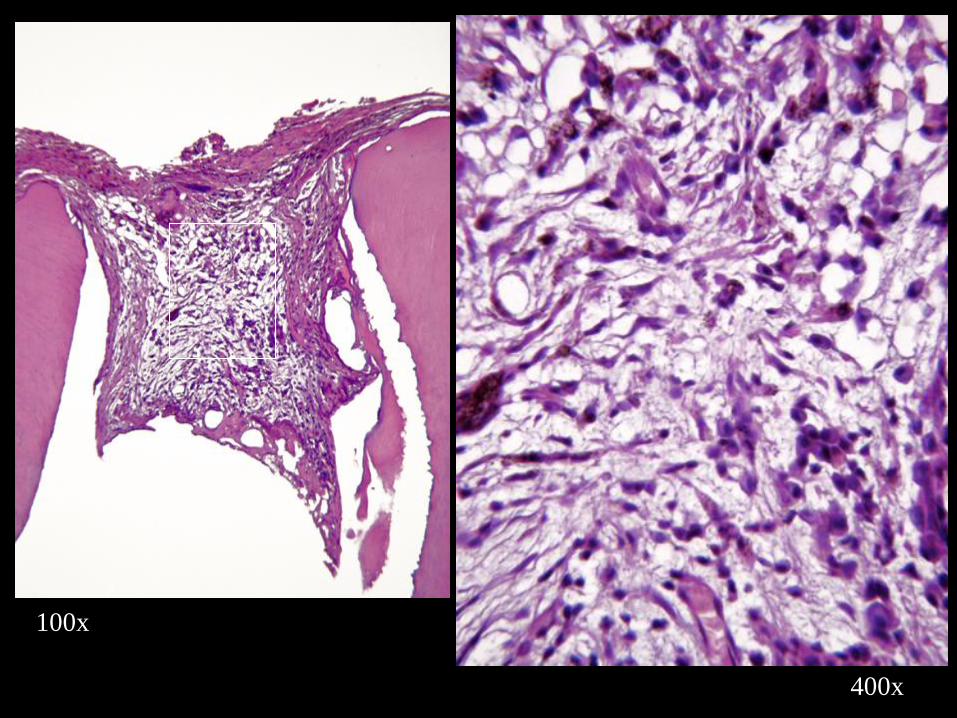
100x
400x
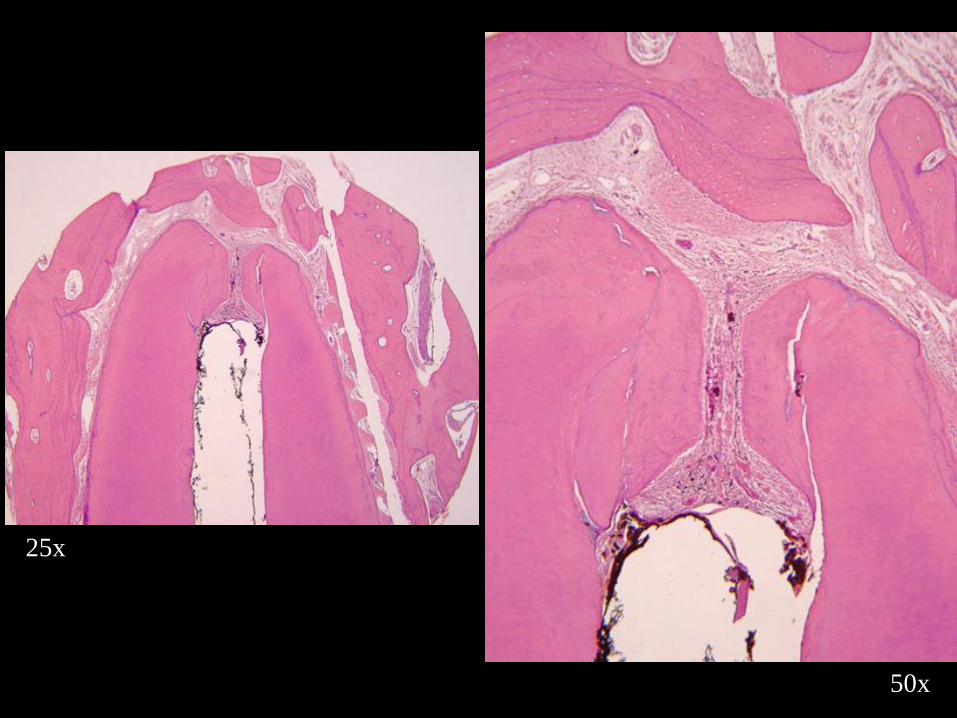
25x
50x
50x
400x
50x
400x
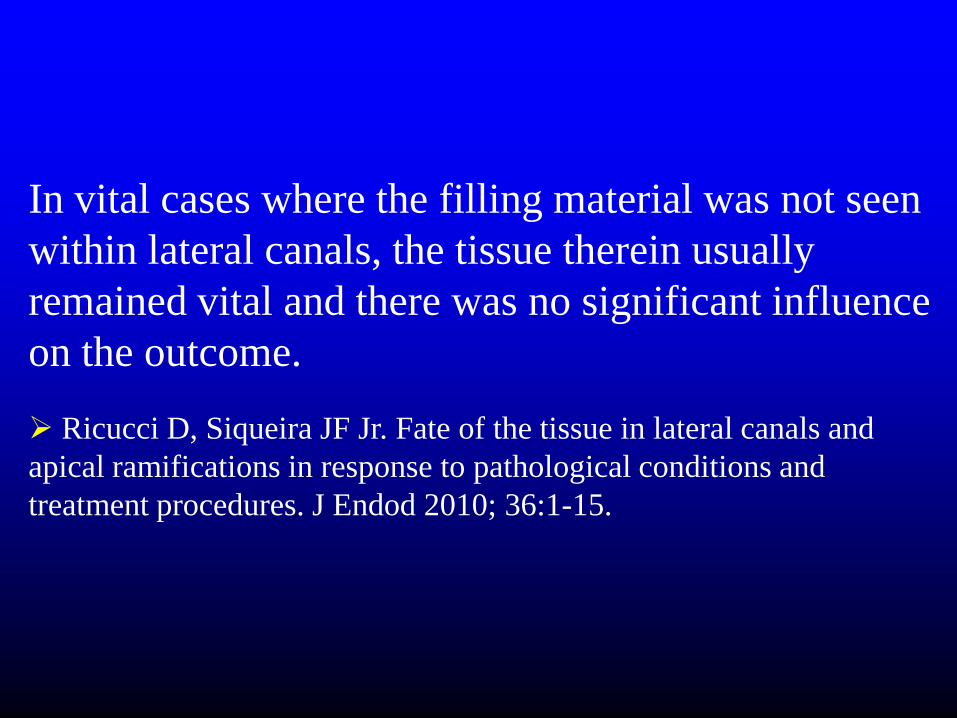
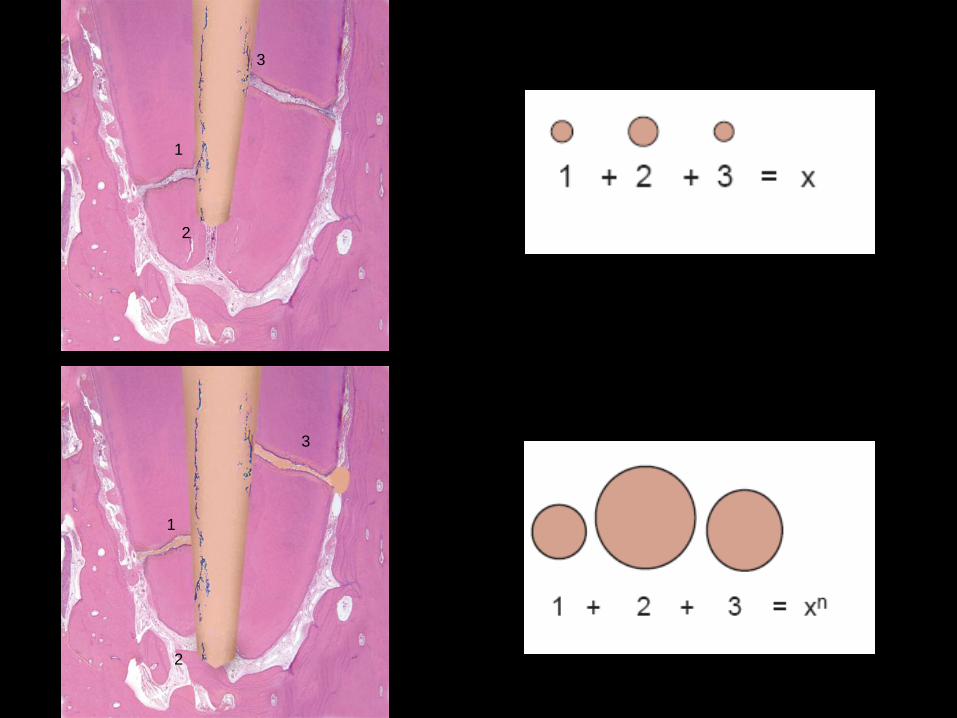
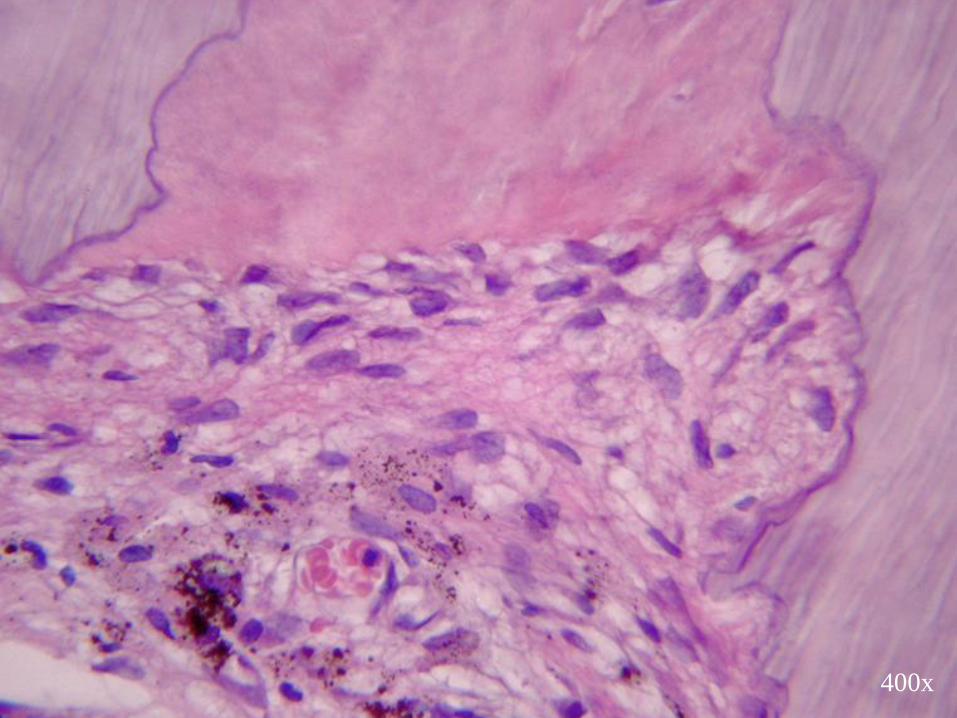
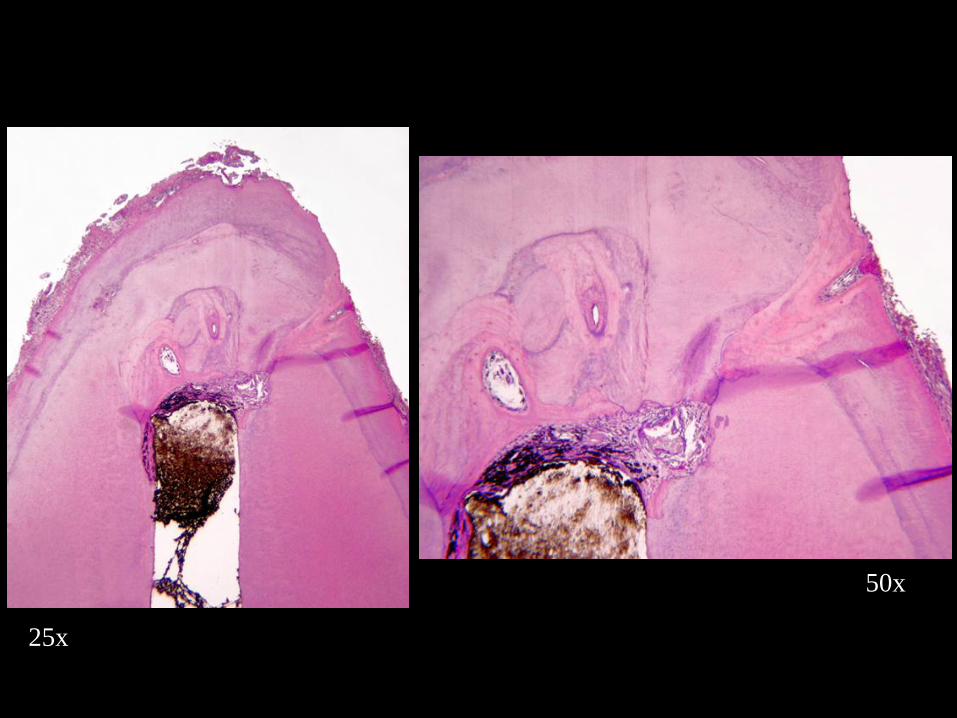
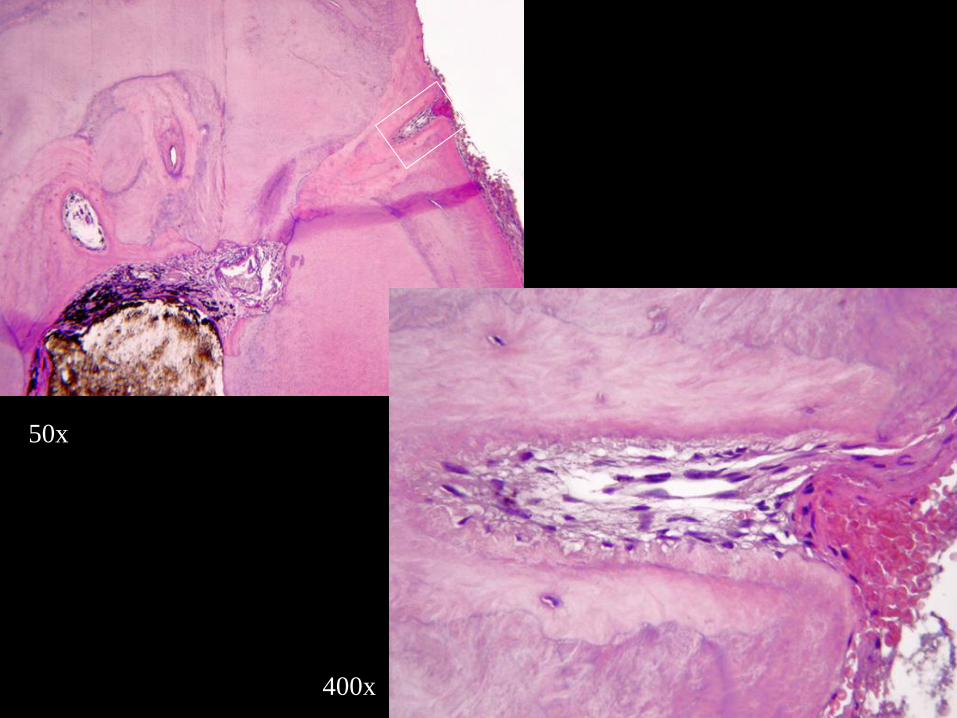
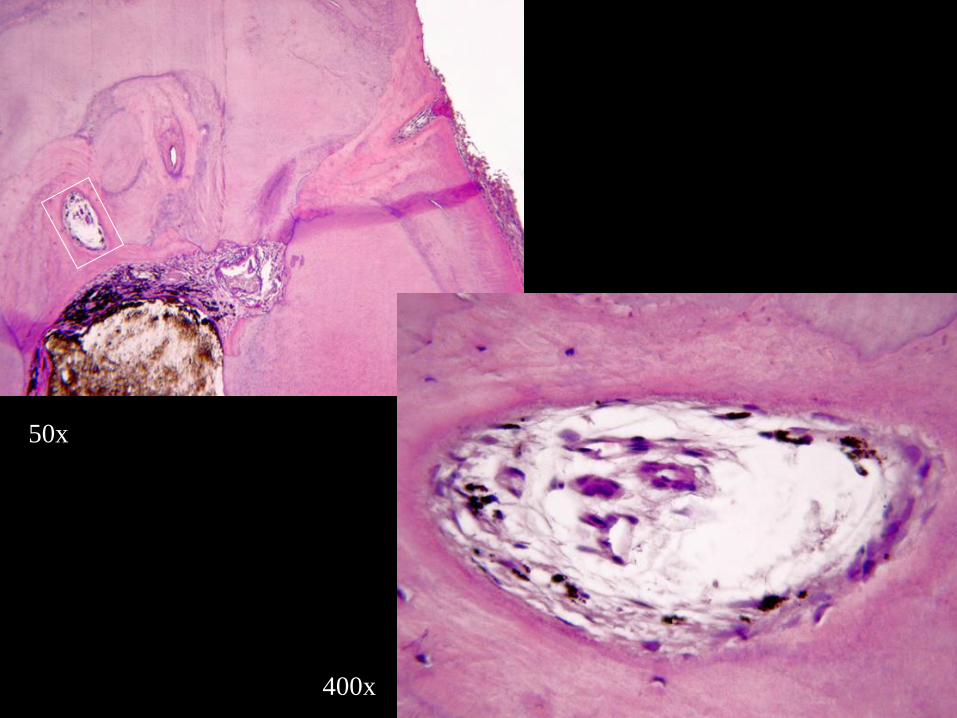
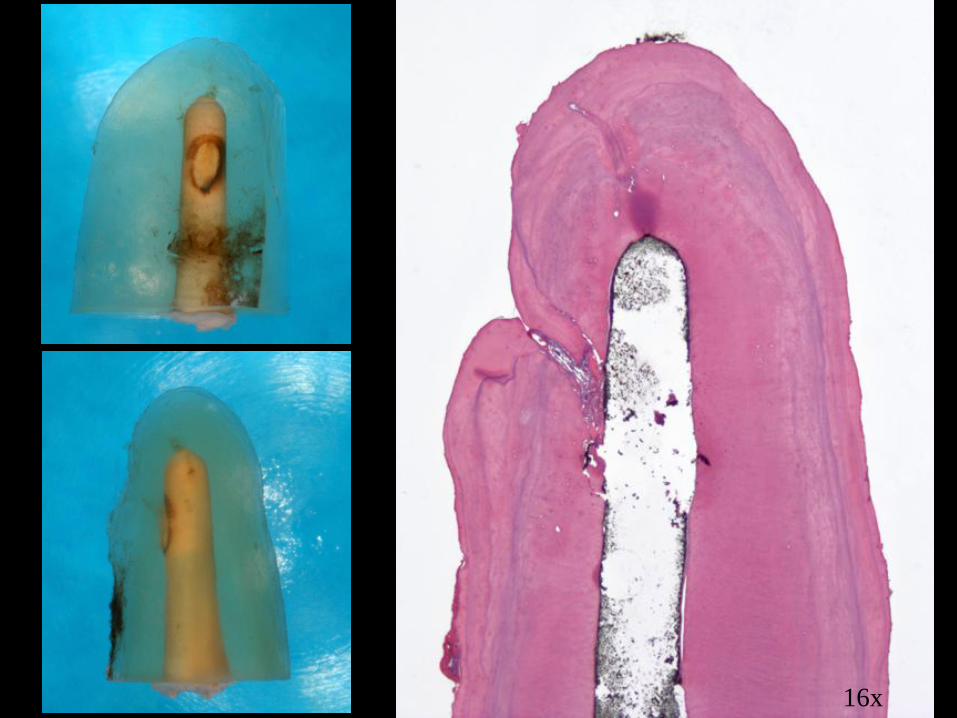
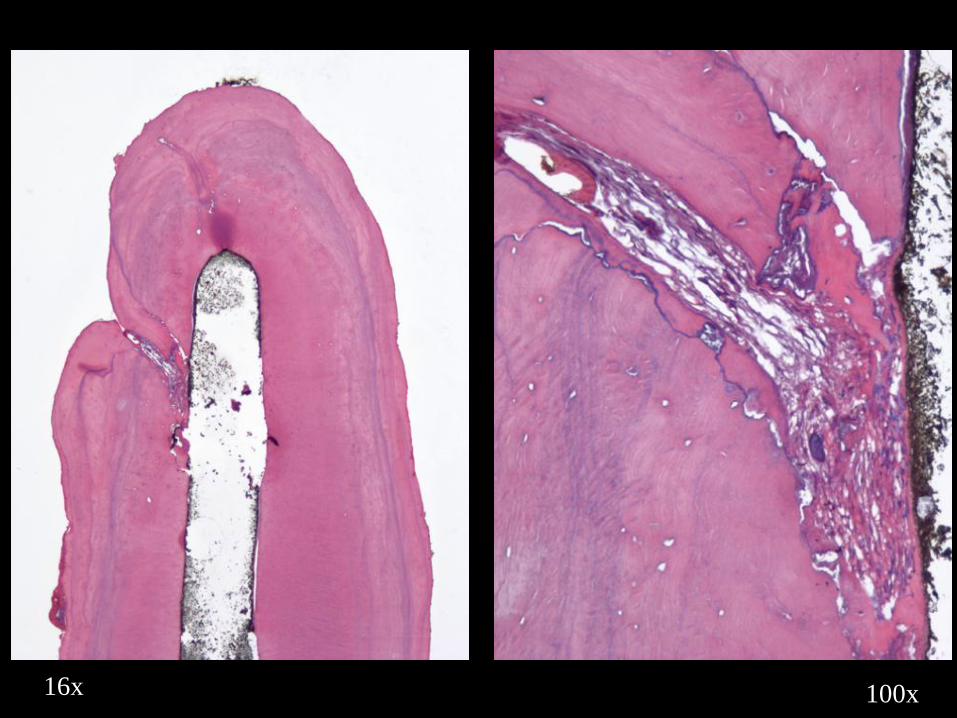
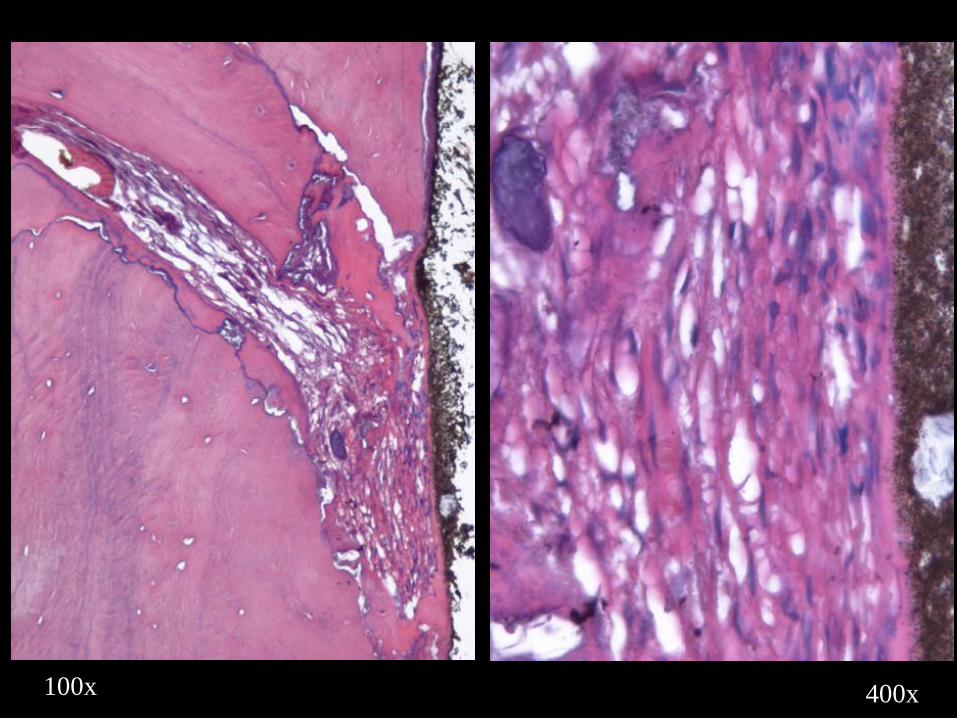
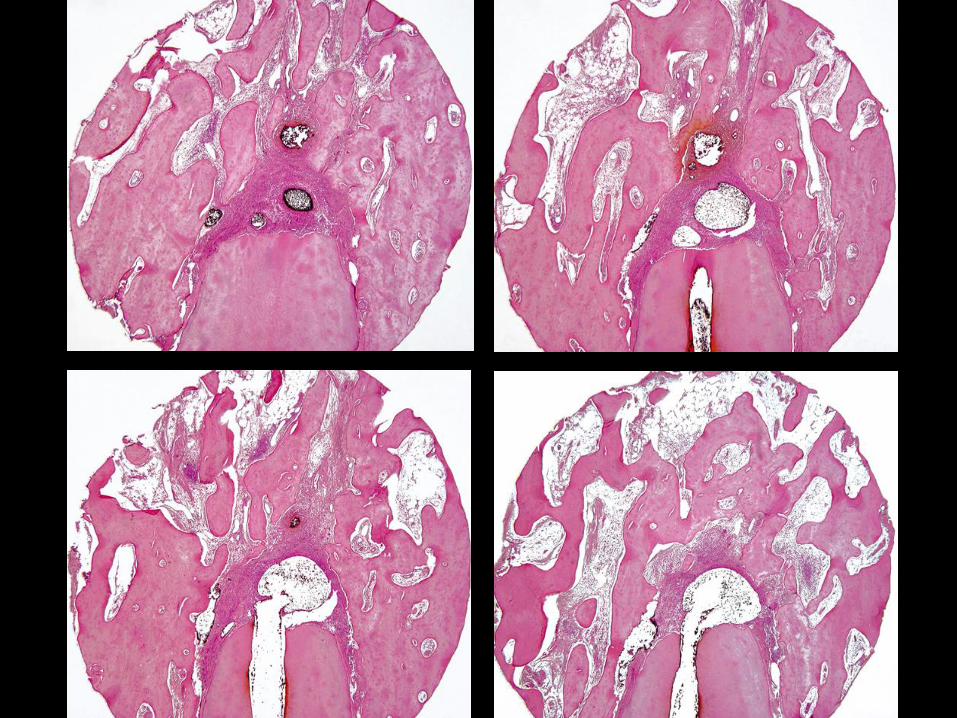
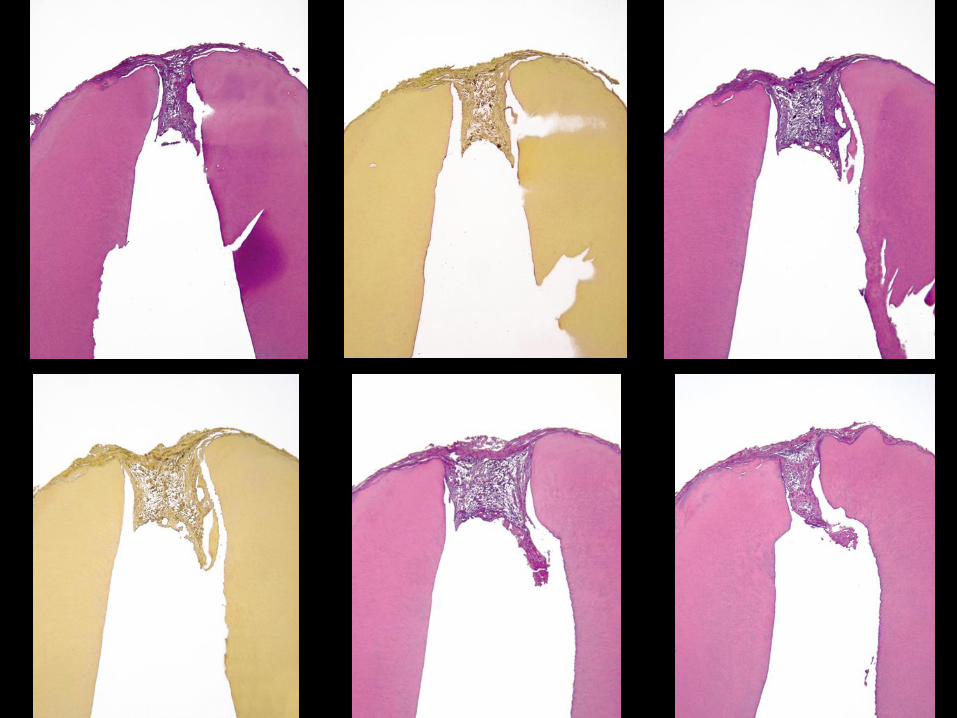
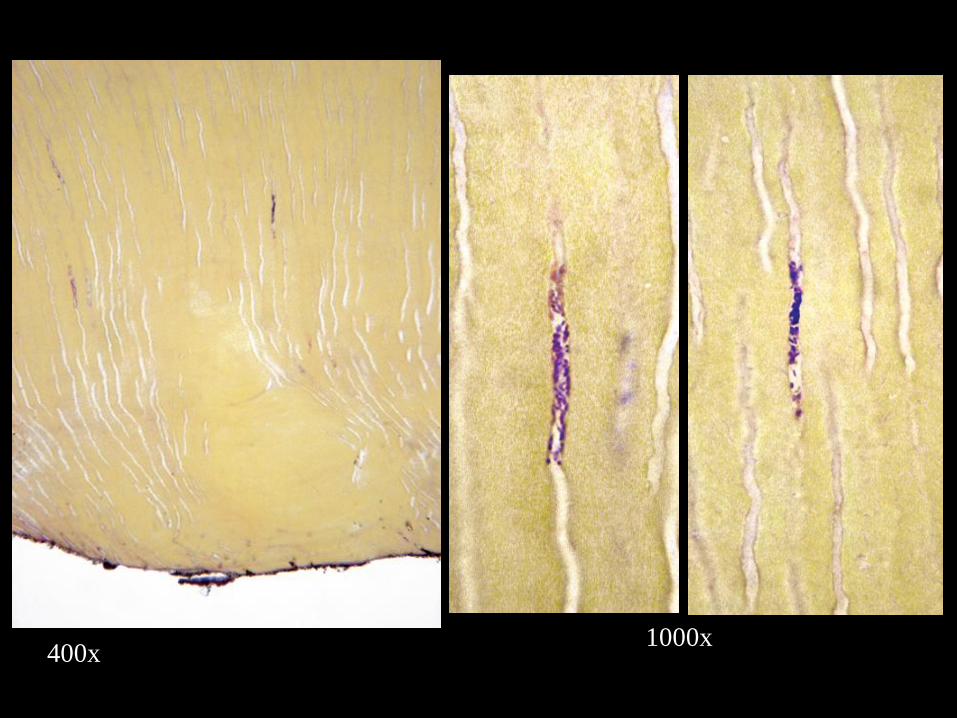
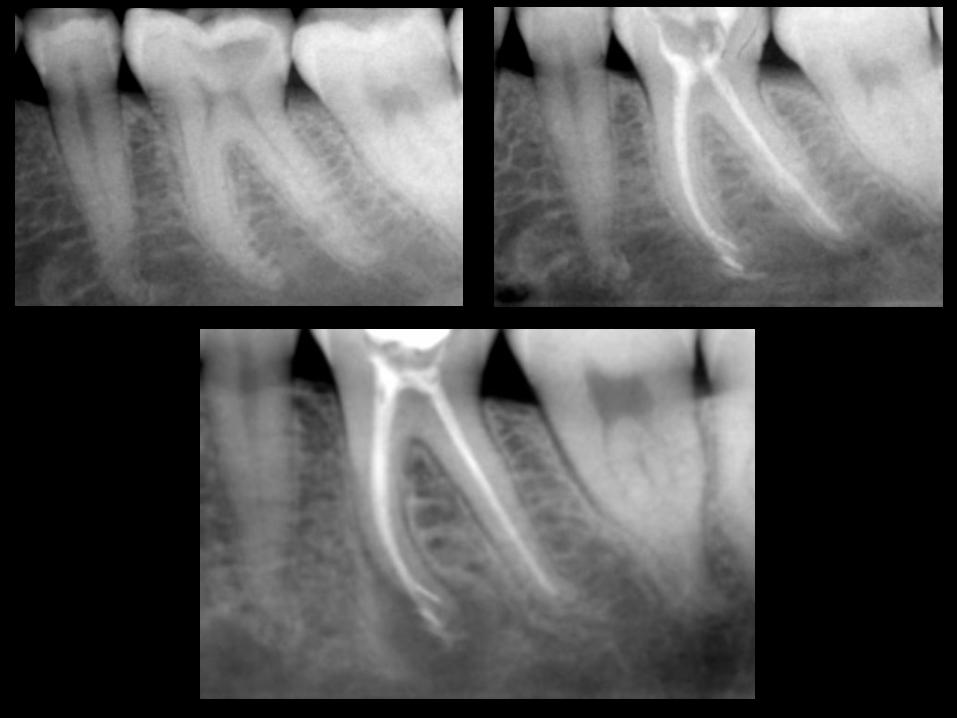
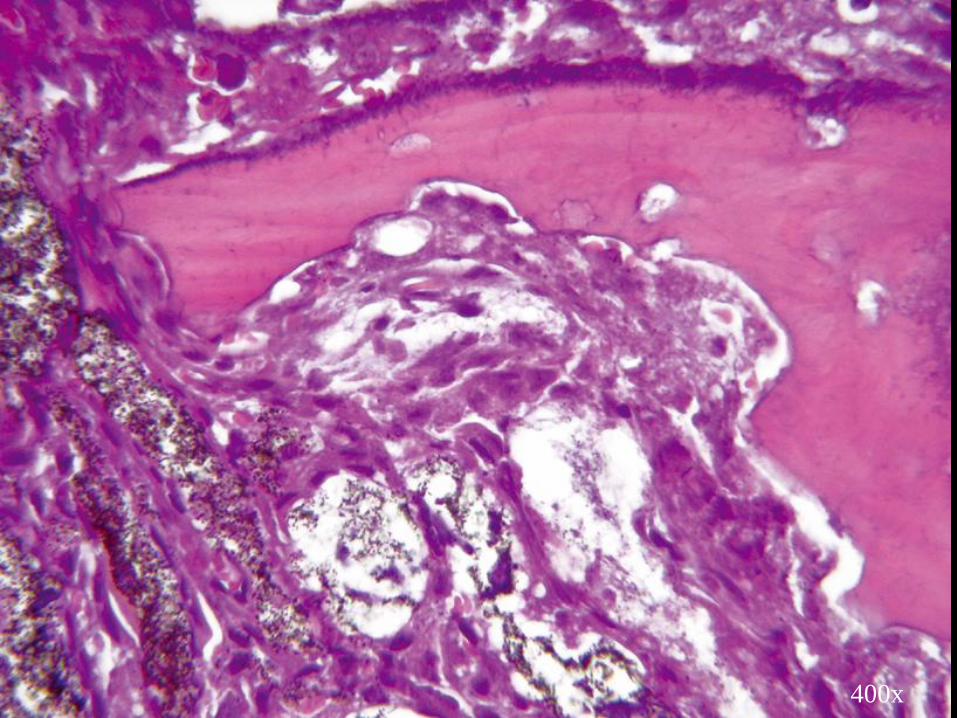
In vital cases where the filling material was not seen
within lateral canals, the tissue therein usually
remained vital and there was no significant influence
on the outcome.
Ricucci D, Siqueira JF Jr. Fate of the tissue in lateral canals and
apical ramifications in response to pathological conditions and
treatment procedures. J Endod 2010; 36:1-15.

9yr 5mo
16x
16x 100x
100x 400x

2mo

25x
100x

100x
400x

25x16x
400x100x
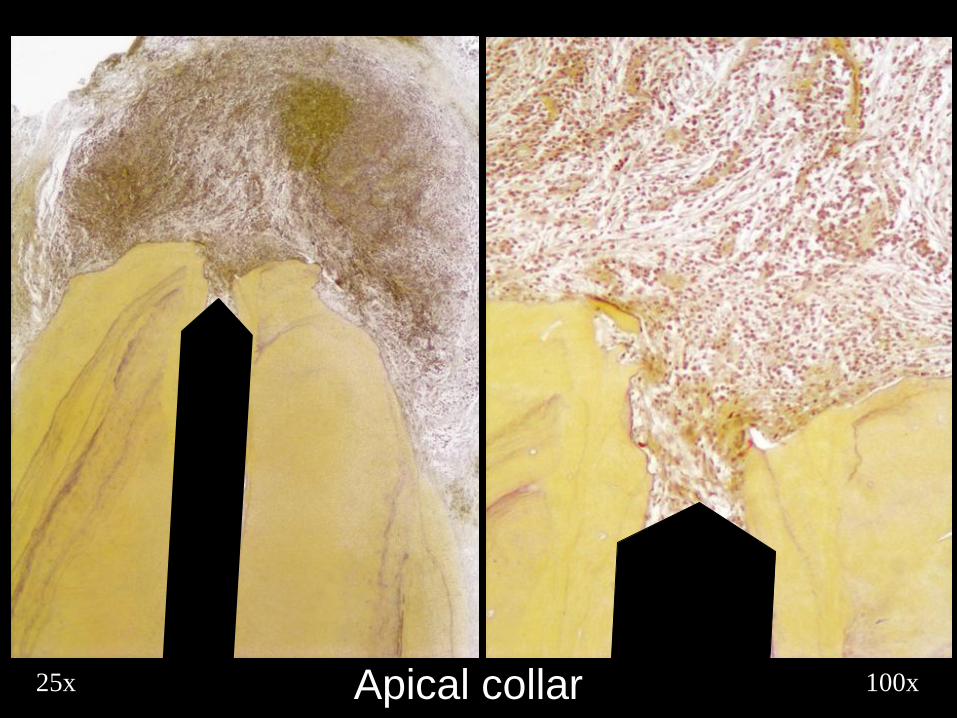
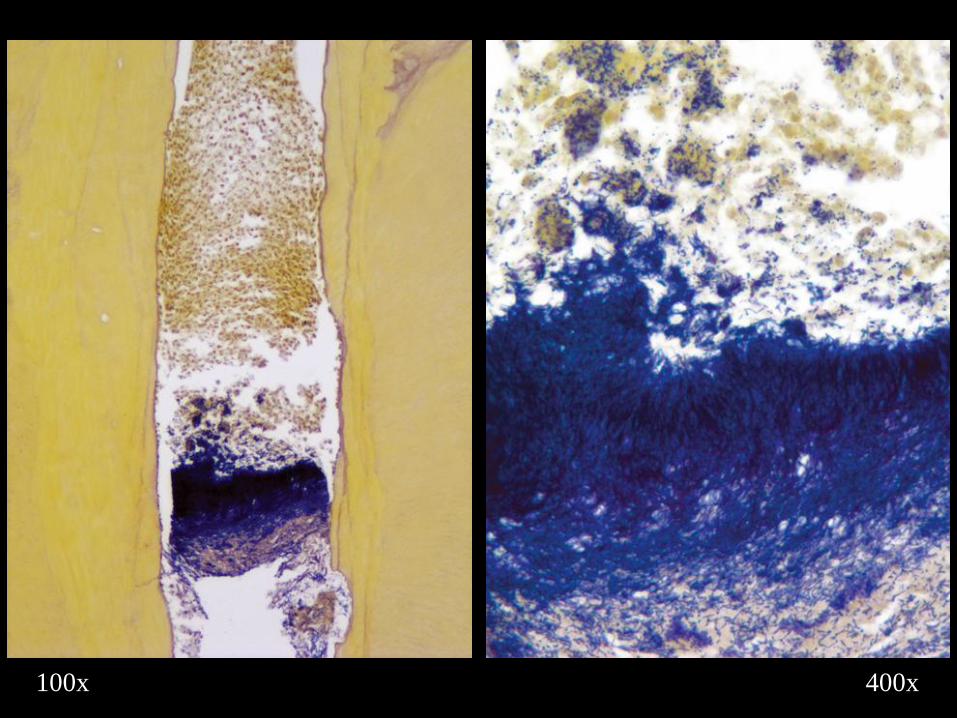
100x25x Apical collar

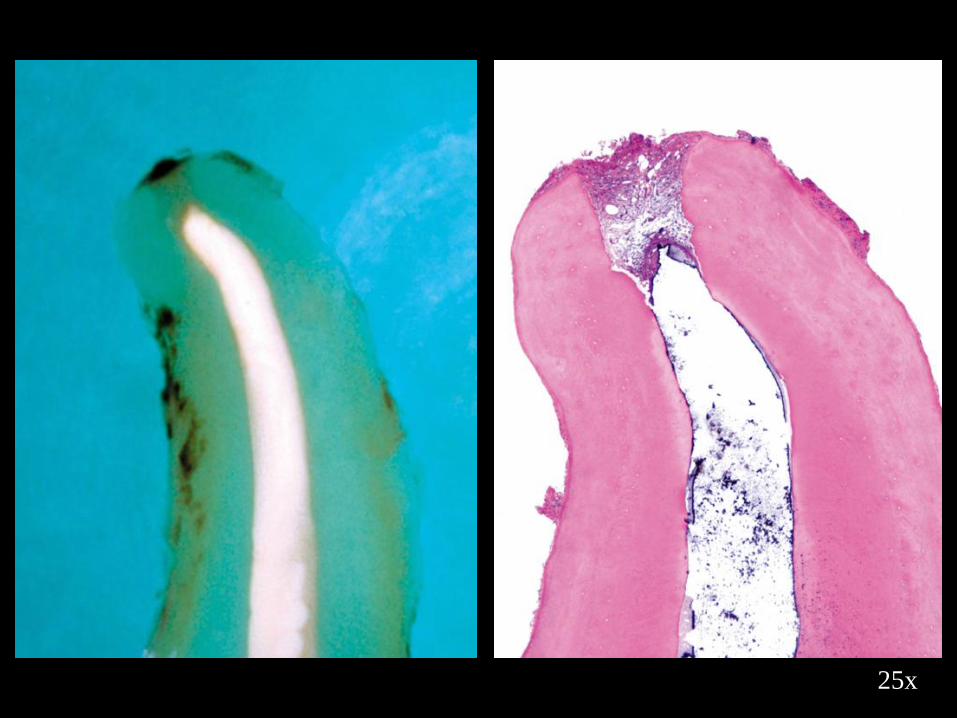
25x
50x
100x
400x
25x
50x
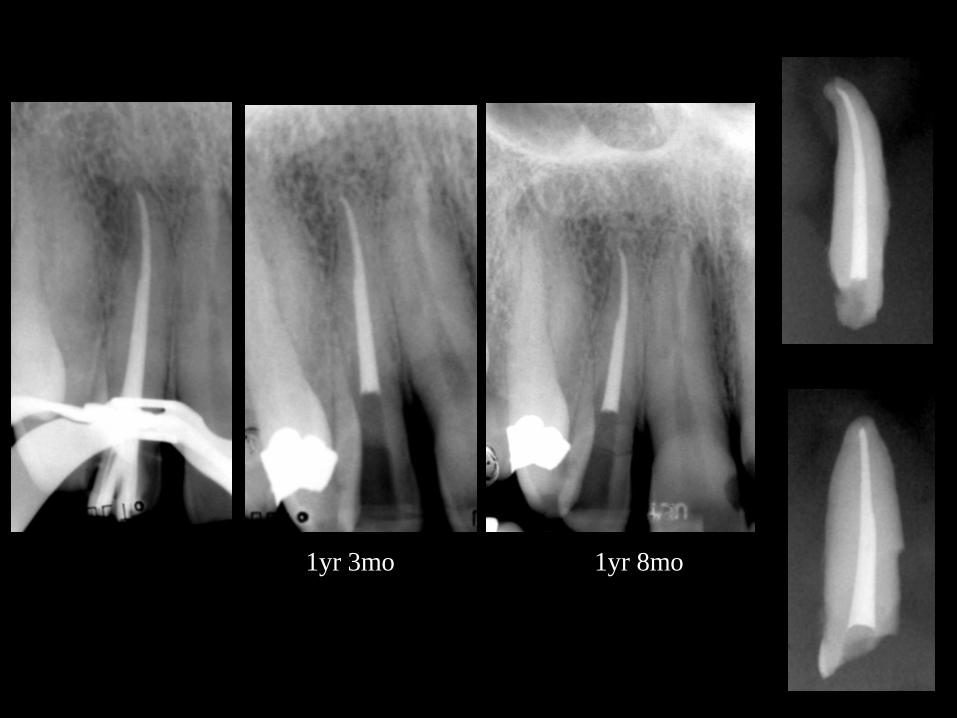
1yr 3mo 1yr 8mo
25x
25x
50x
Apical
constriction
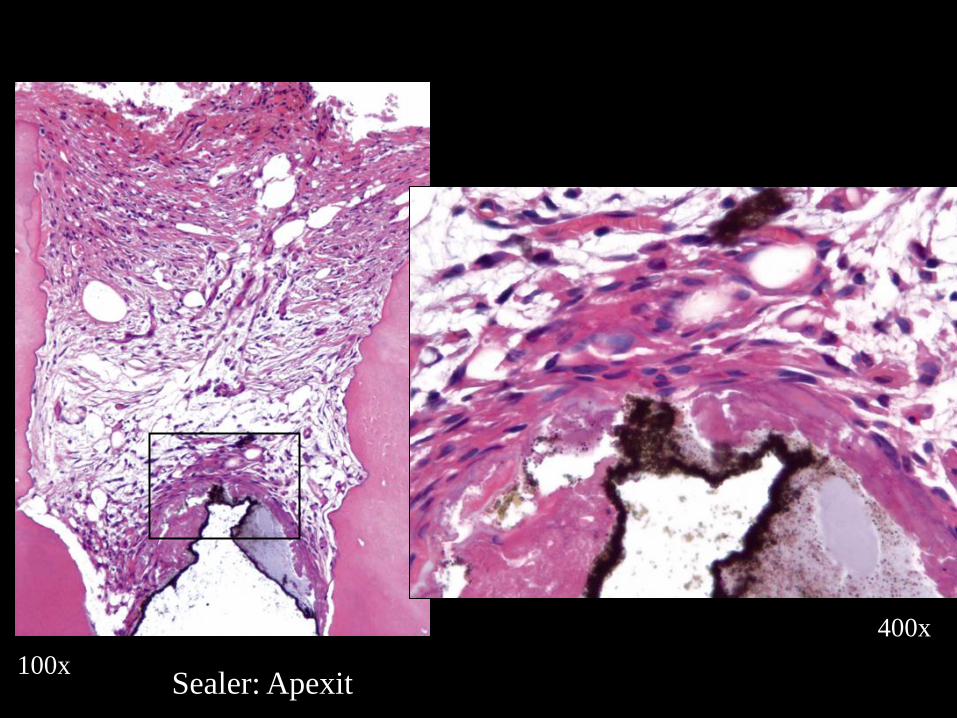
100x
400x
Sealer: Apexit
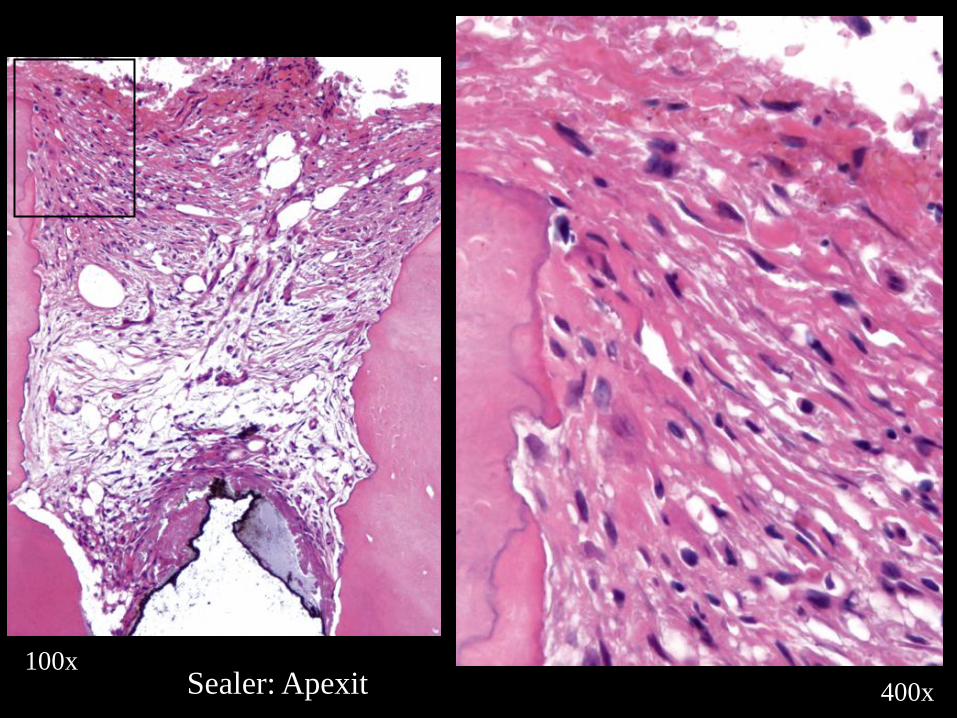
100x
400xSealer: Apexit
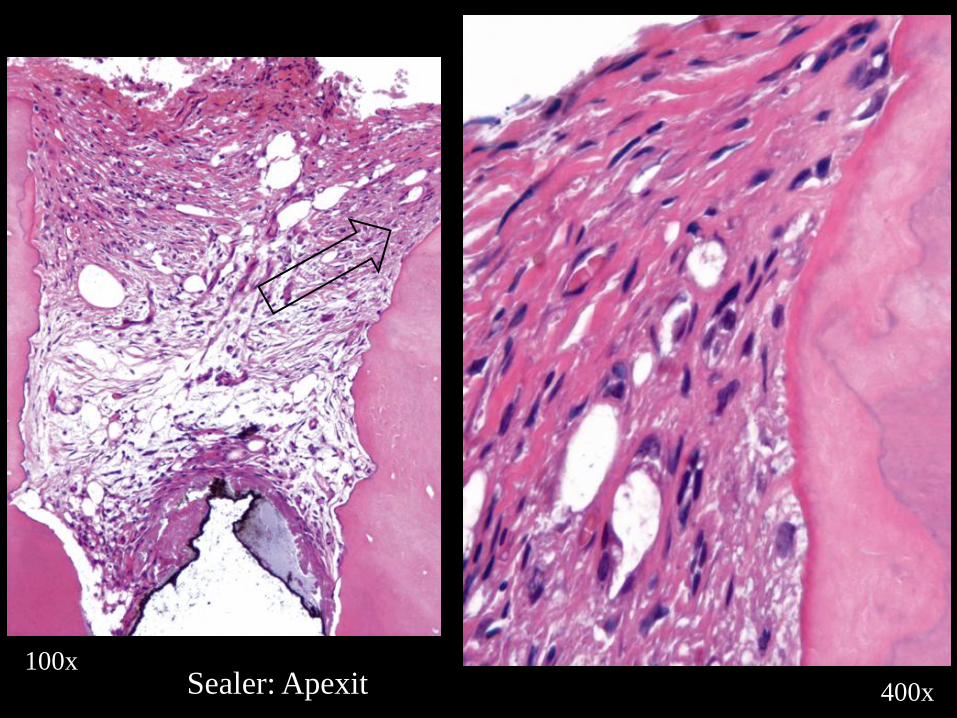
100x
400xSealer: Apexit
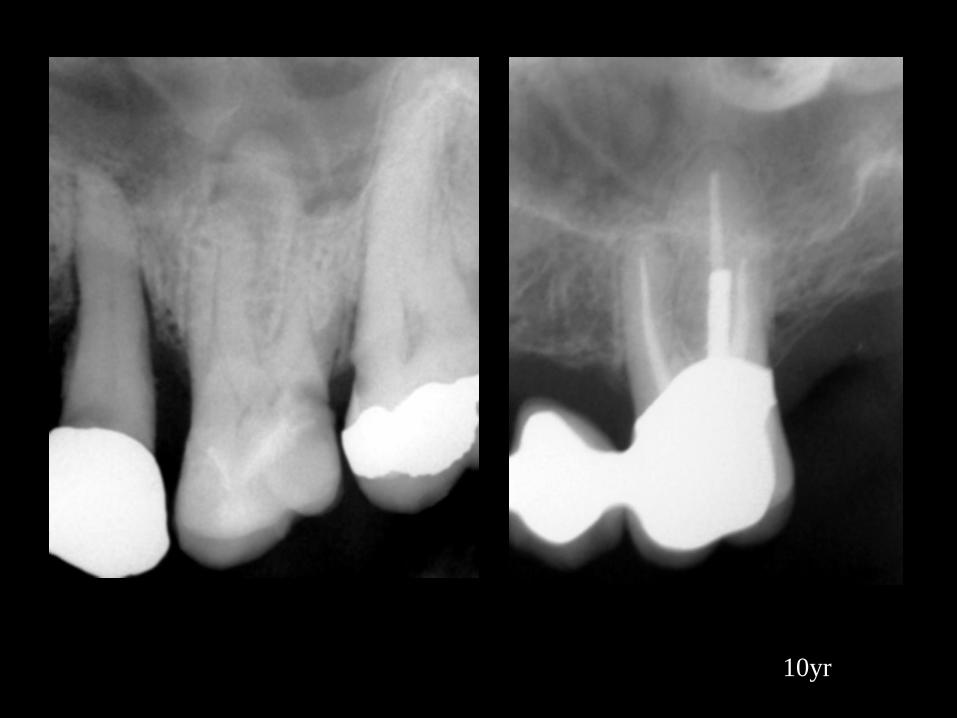
10yr

13yr 5mo
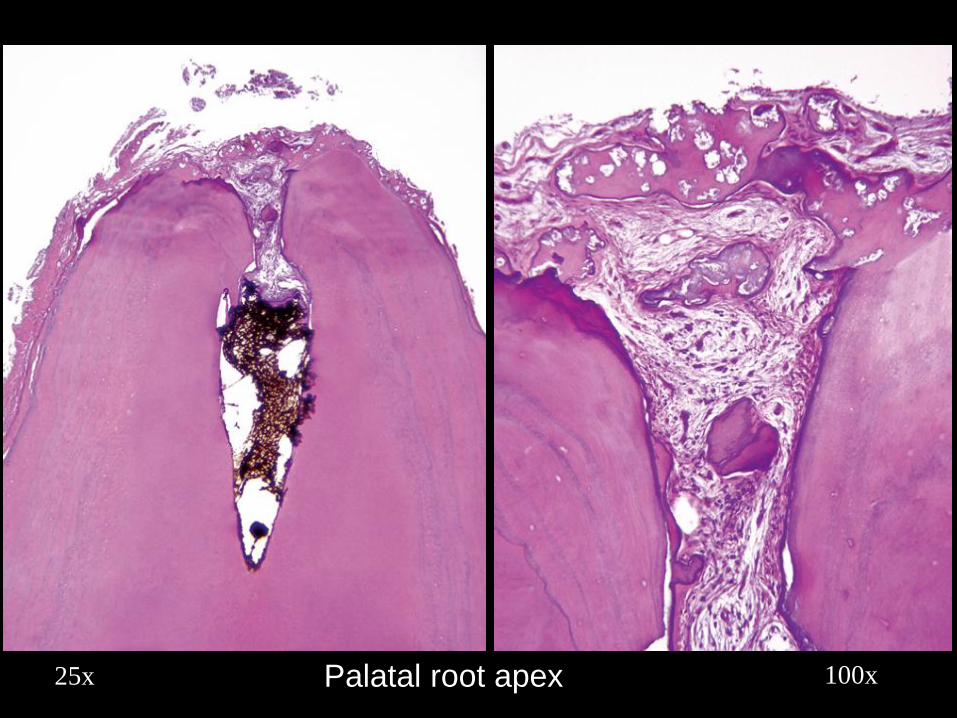
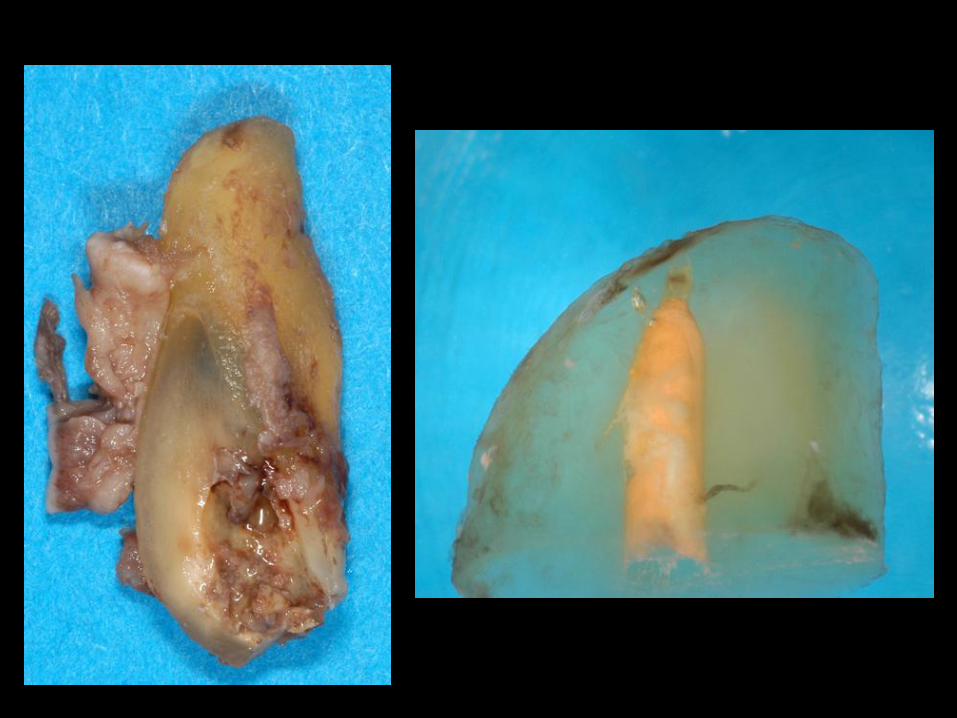
25x 100xPalatal root apex
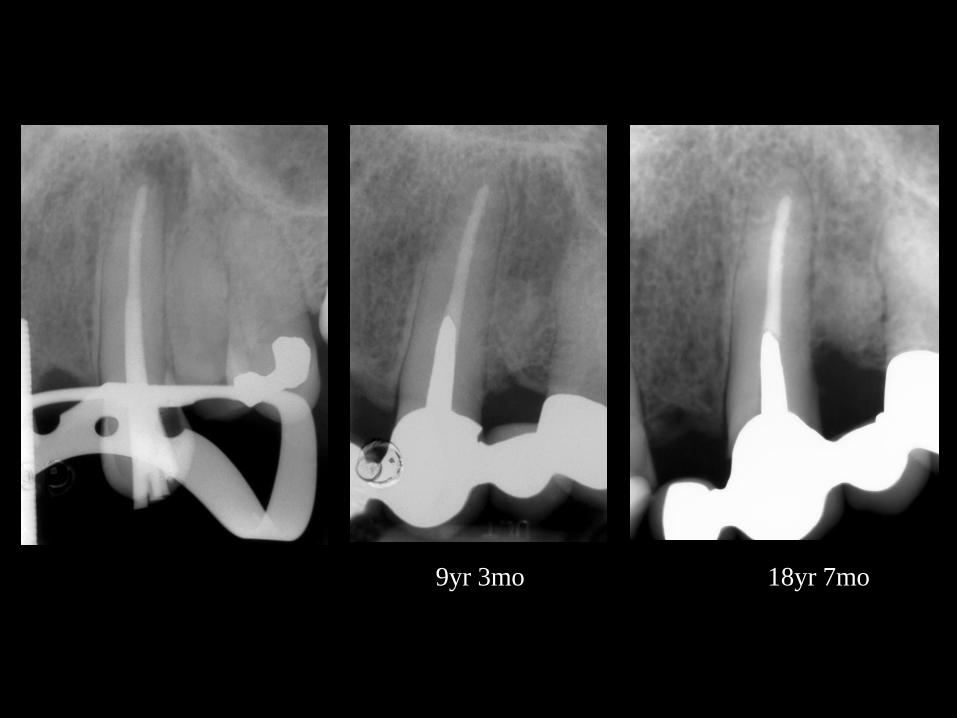
18yr 7mo9yr 3mo
50x
100x
100x 400x
100x 400x
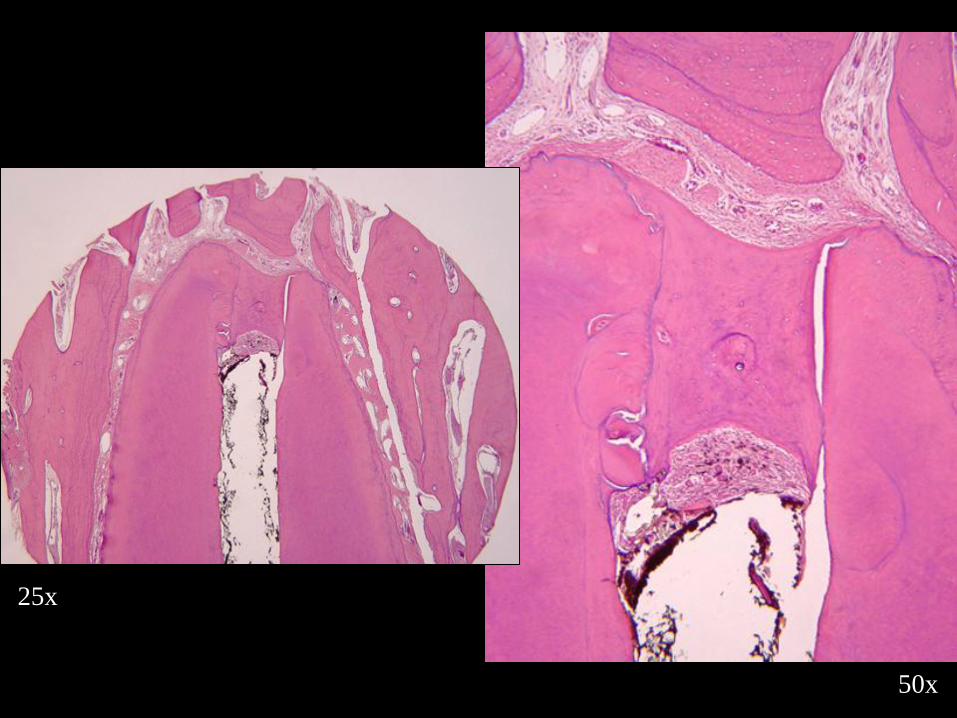
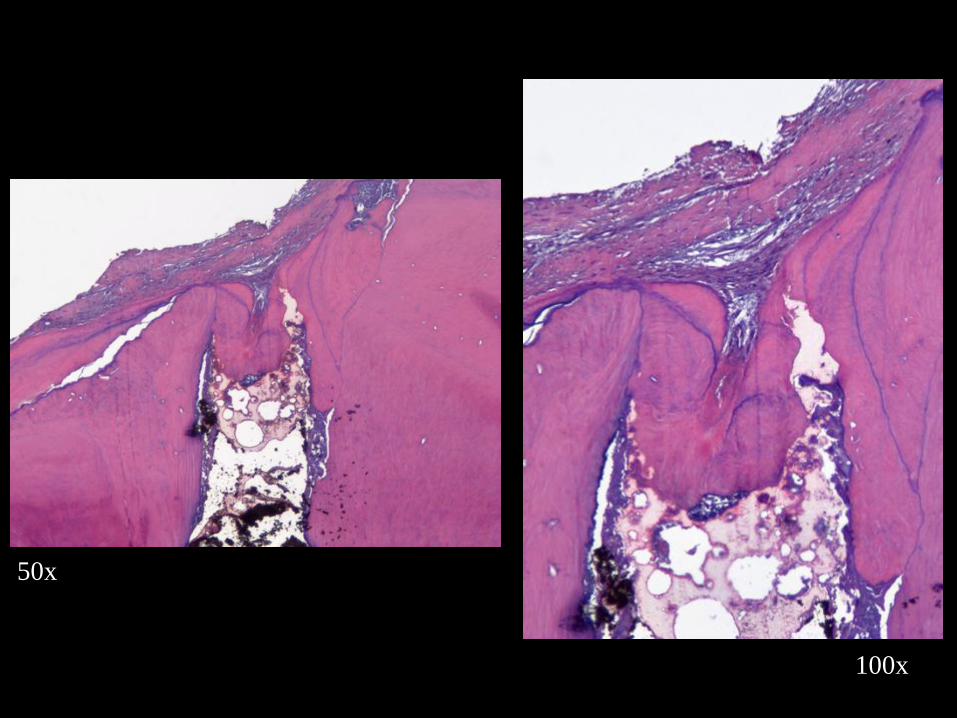
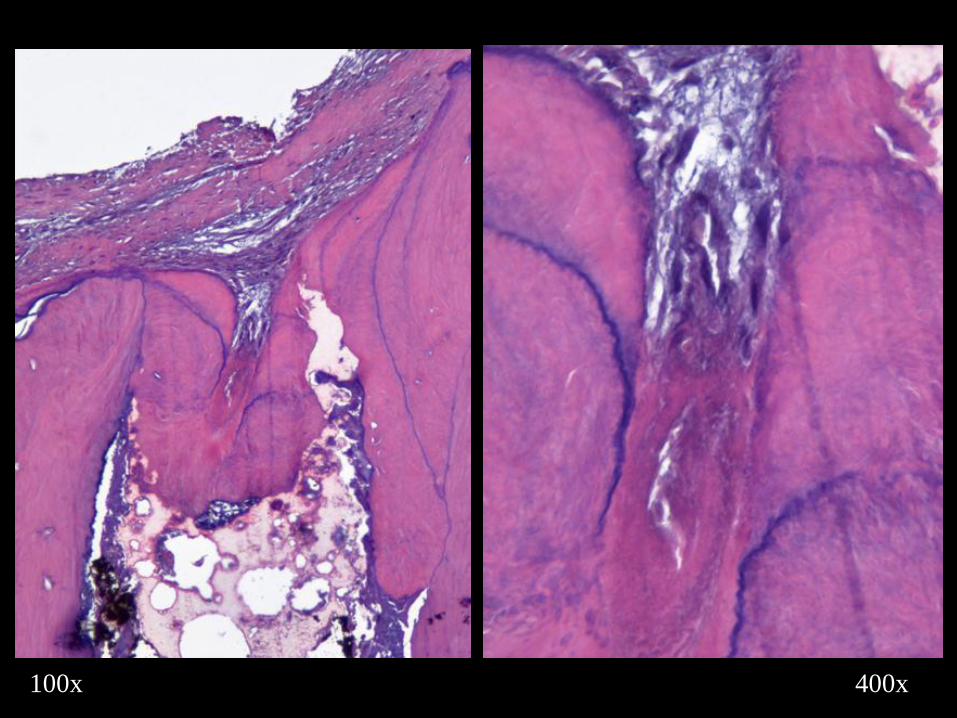
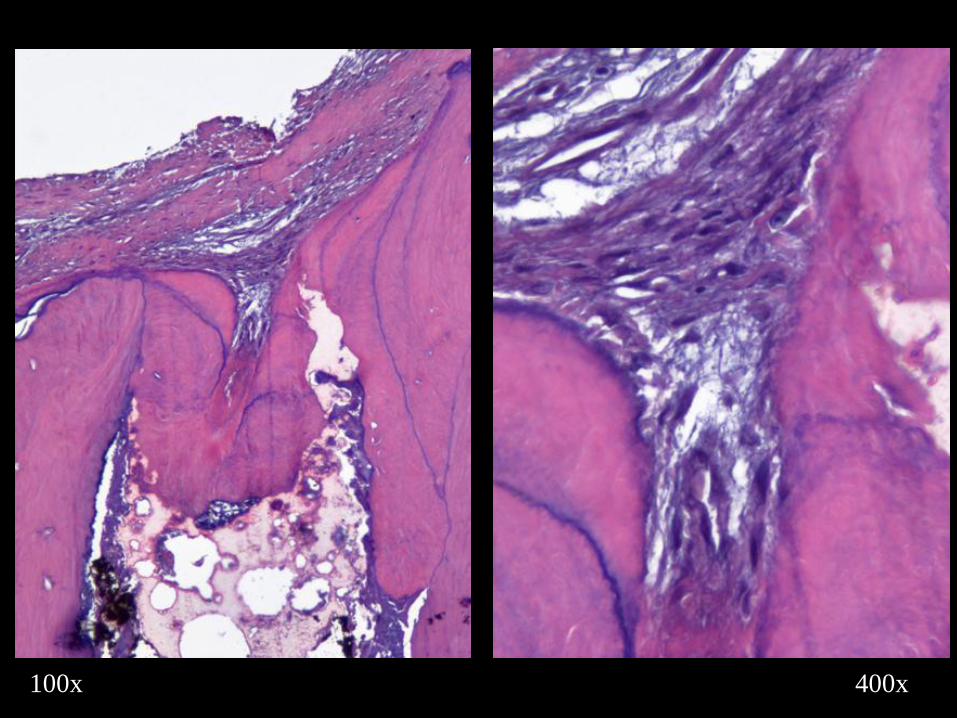
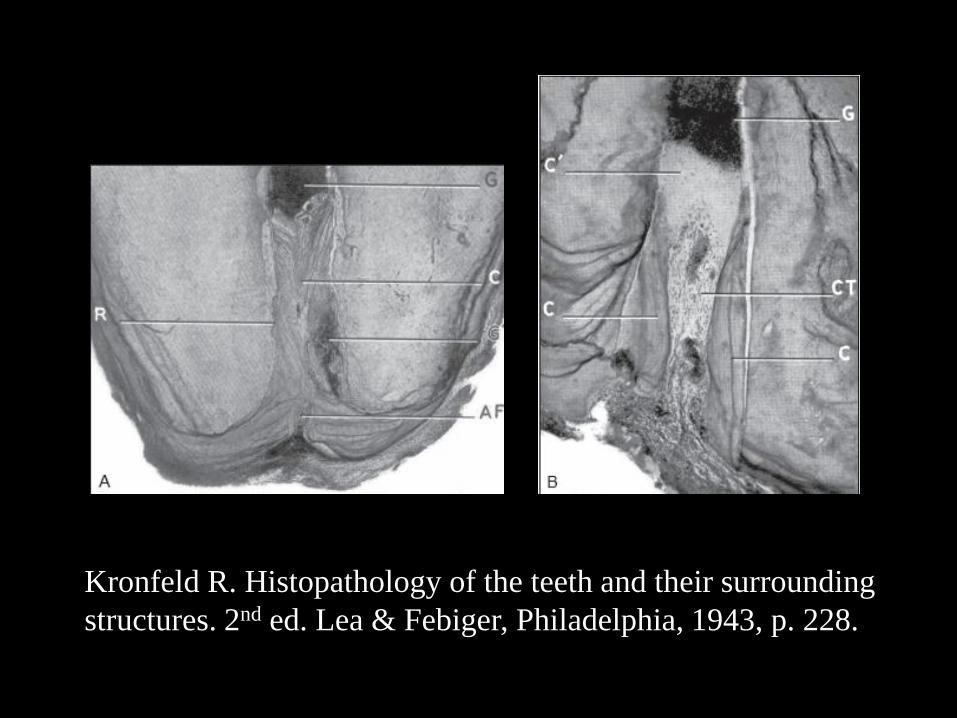
Kronfeld R. Histopathology of the teeth and their surrounding
structures. 2nd ed. Lea & Febiger, Philadelphia, 1943, p. 228.
“Most roots are slightly underfilled…and containing fibrous
connective tissue, which may be either a remnant of the original
pulp tissue or periodontal connective tissue that proliferated into
the open apical portion of the root canal. The connective tissue has
a tendency to form cementum, which is deposited in layers on the
wall of the pulp canal.”
Kronfeld R. Histopathology of the teeth and their surrounding
structures. 2nd ed. Lea & Febiger, Philadelphia, 1943, p. 228.
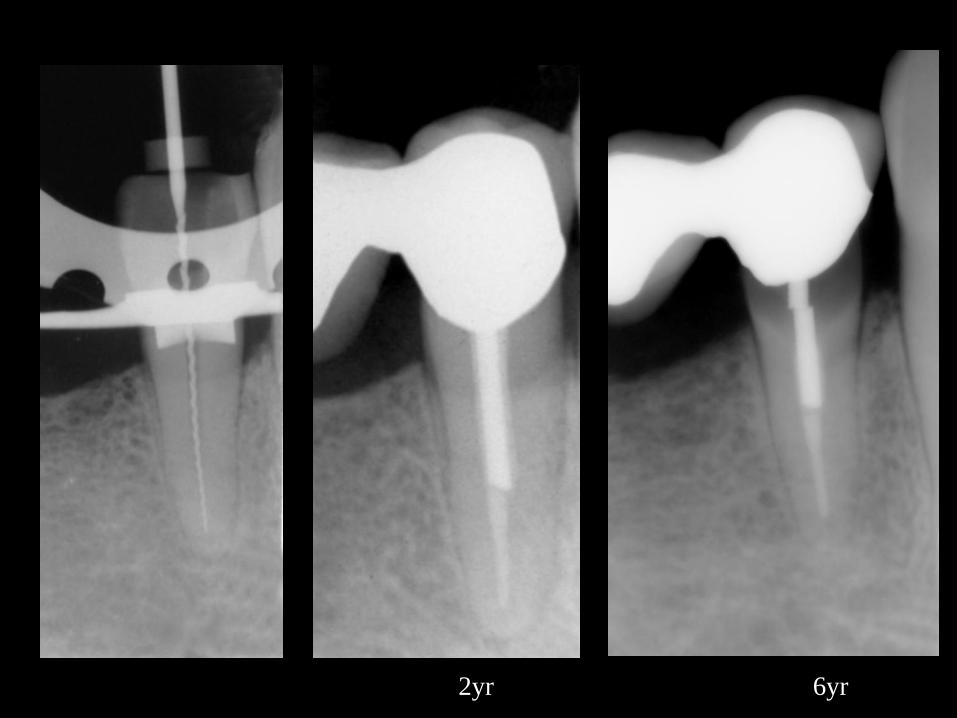
2yr 6yr

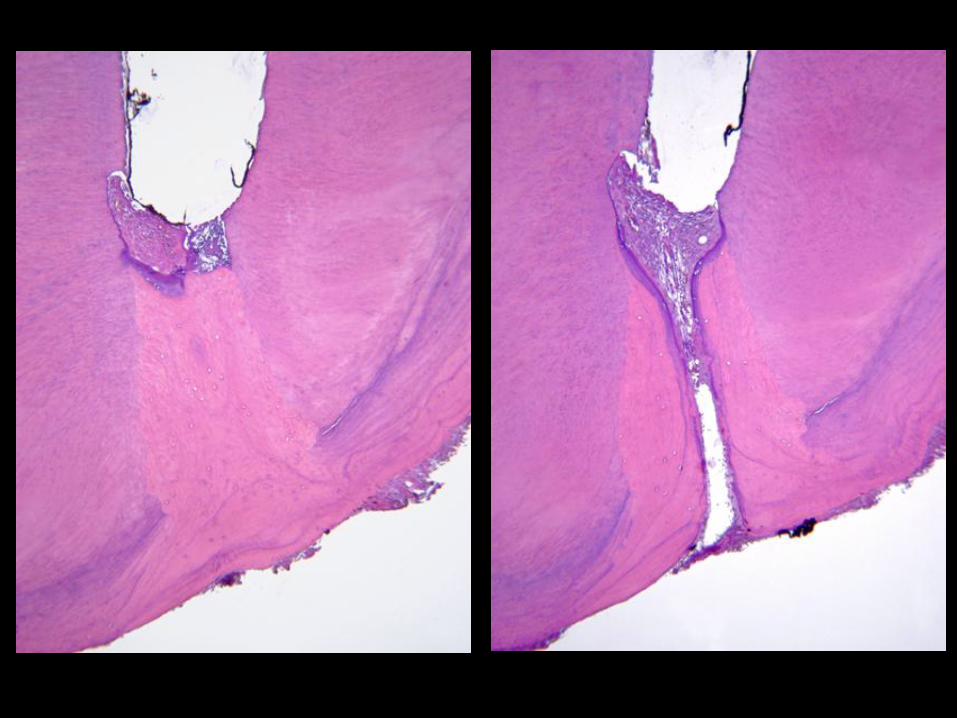
25x 50x
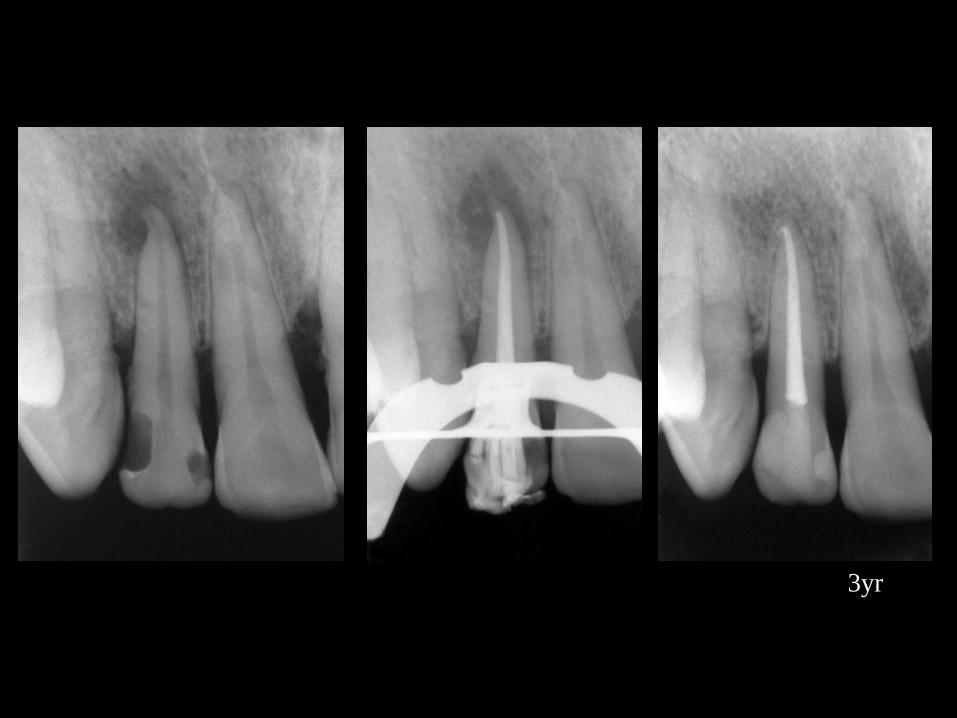
3yr
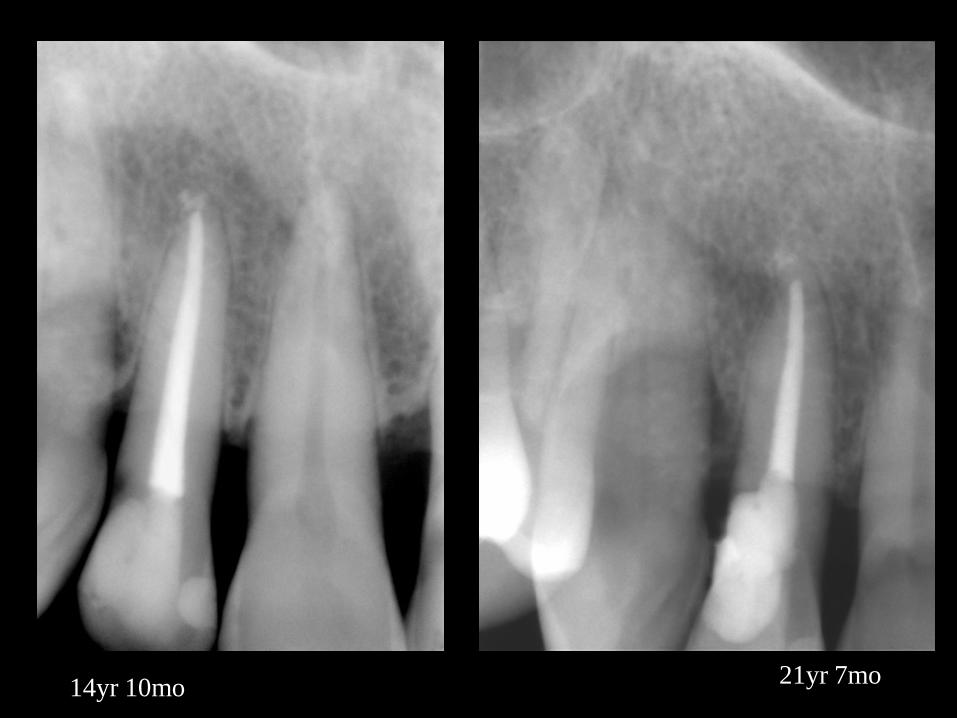
14yr 10mo21yr 7mo

25yr24yr 5mo
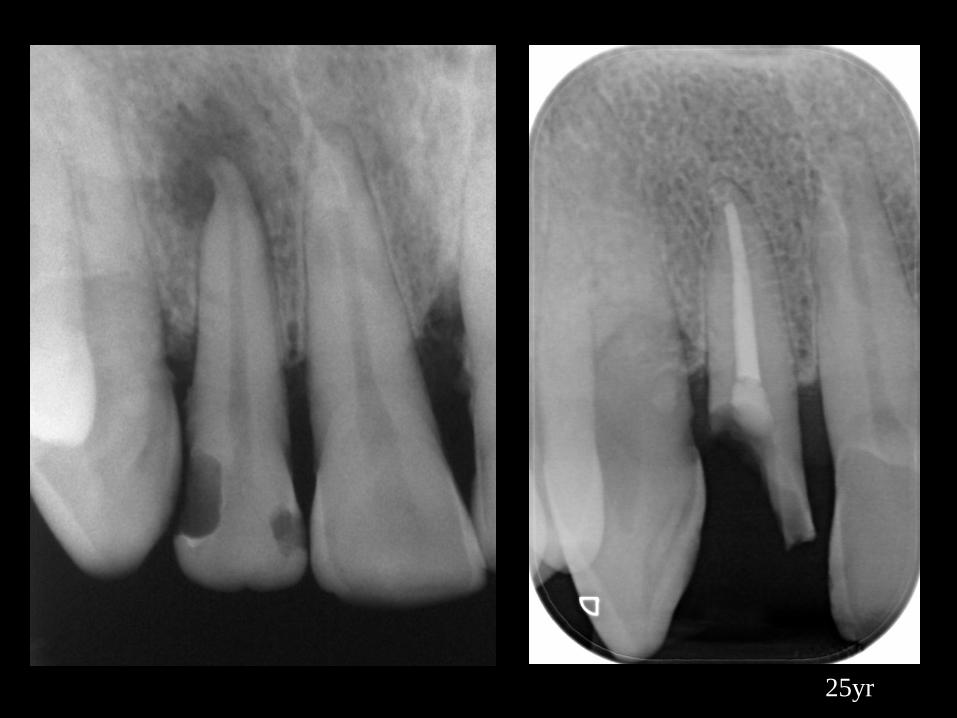
25yr

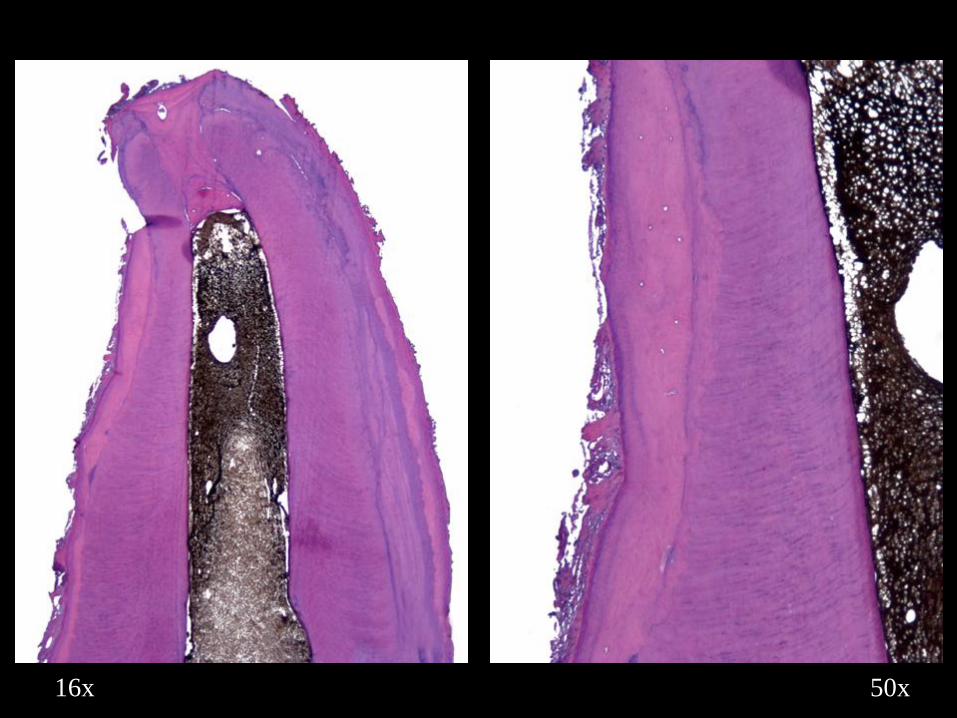
50x16x
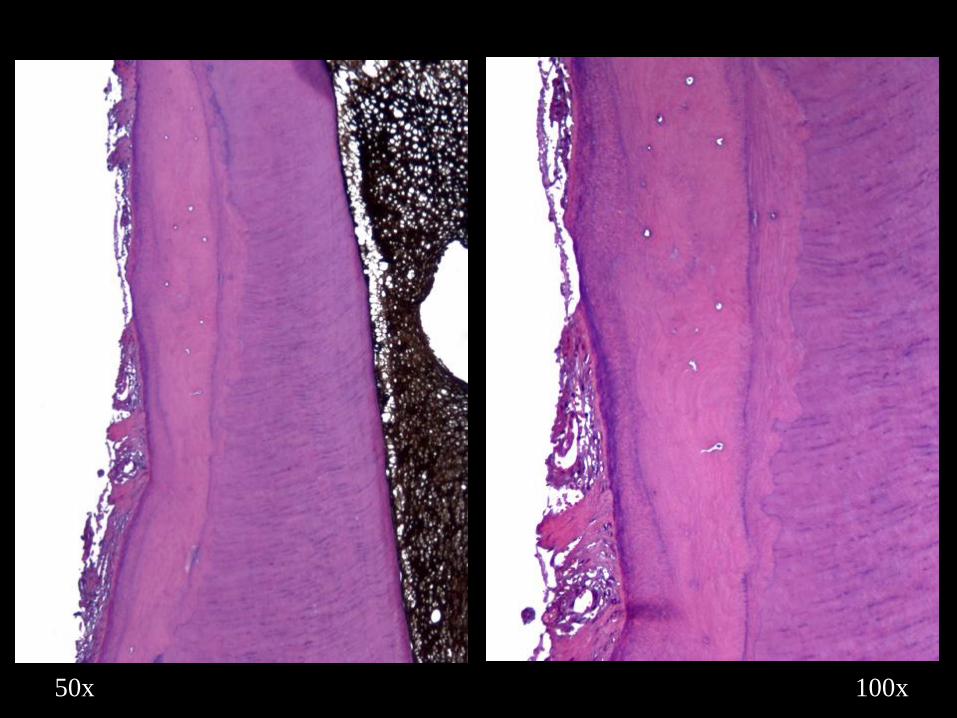
100x50x
100x
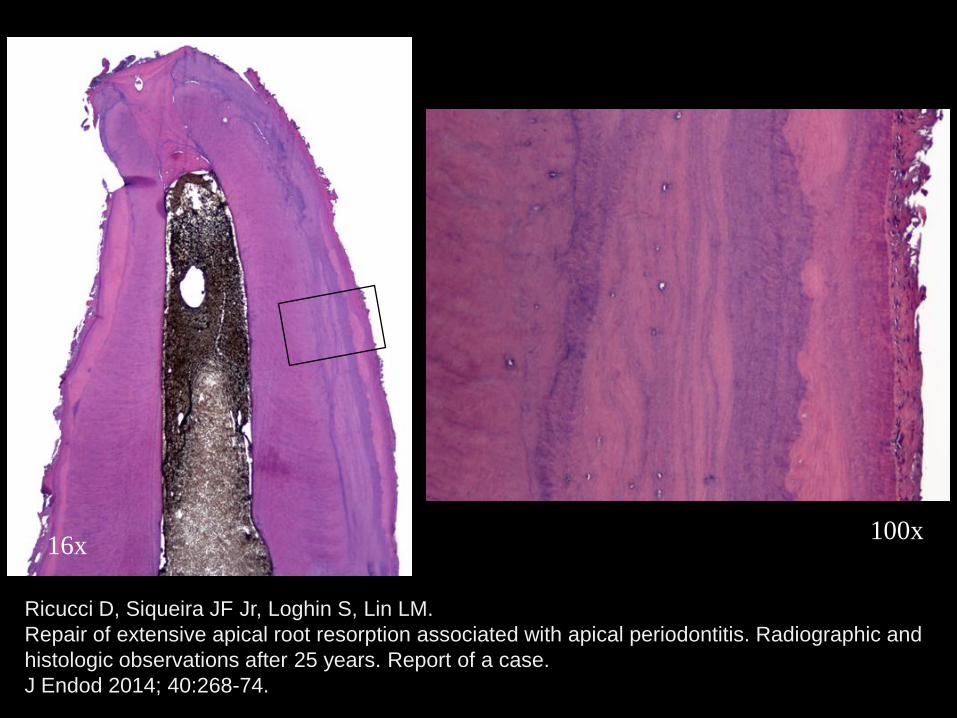
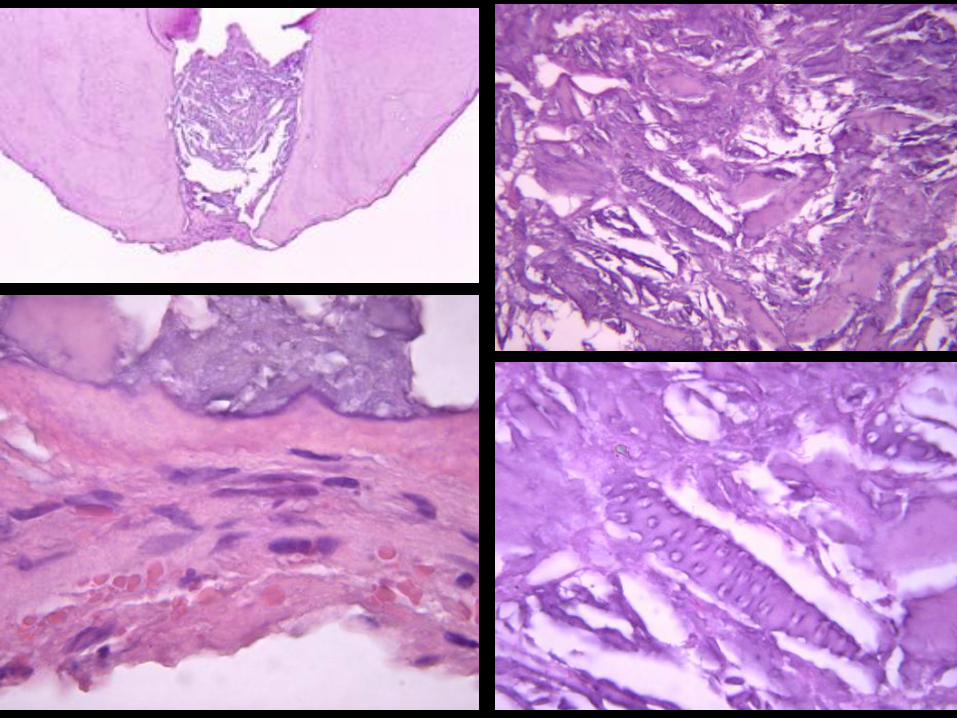
Ricucci D, Siqueira JF Jr, Loghin S, Lin LM.
Repair of extensive apical root resorption associated with apical periodontitis. Radiographic and
histologic observations after 25 years. Report of a case.
J Endod 2014; 40:268-74.
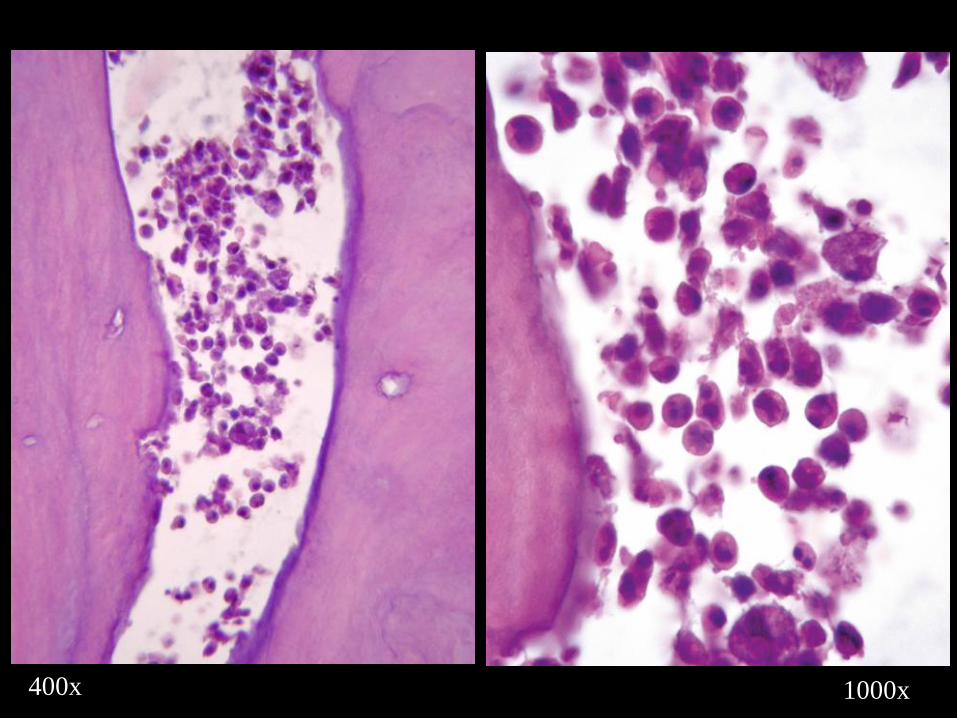
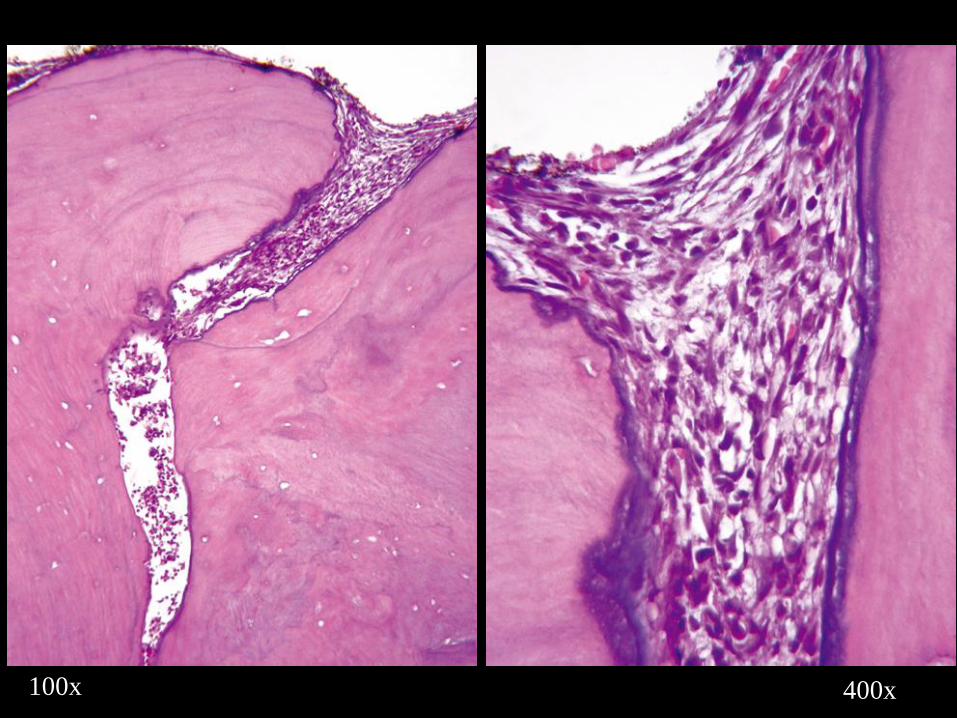
16x


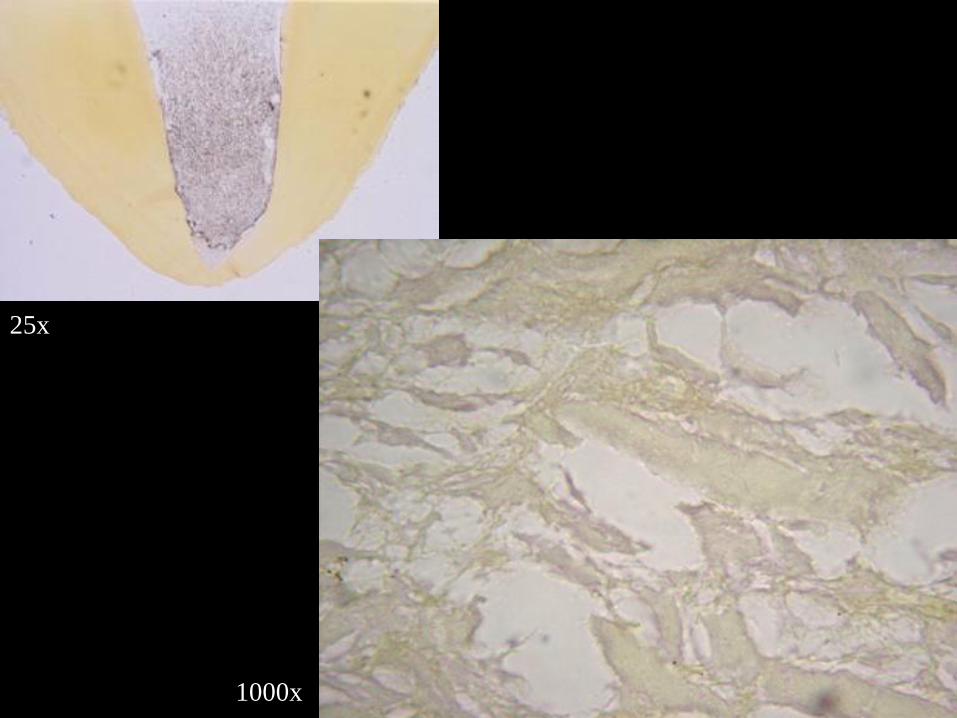
25x
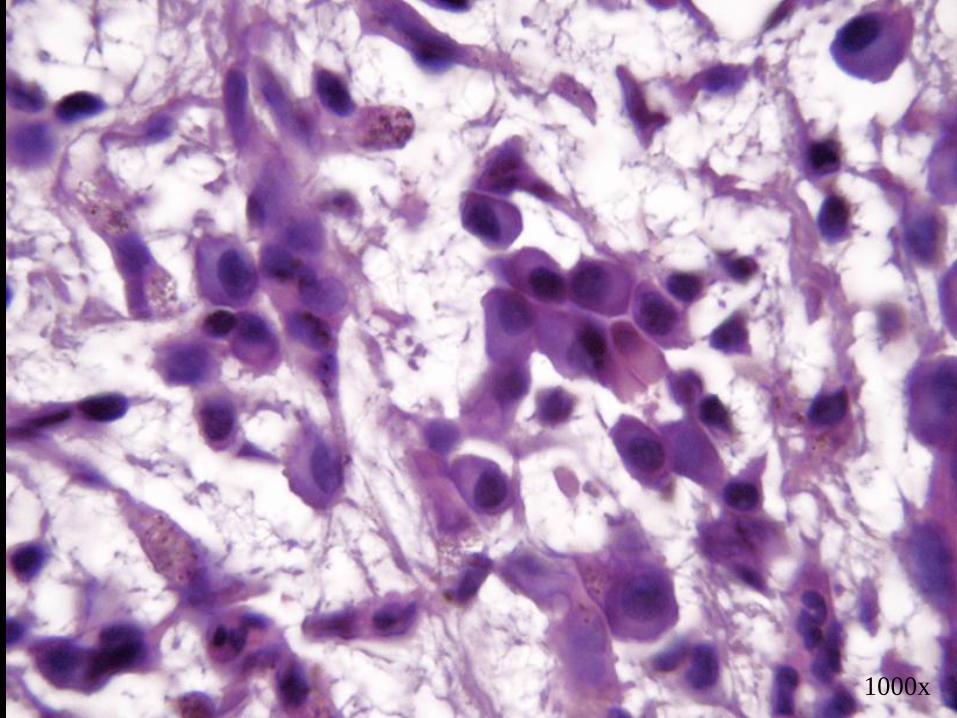
1000x
Brynolf I. A histological and roentgenological study of the periapical region
of human upper incisors. Odont Revy 18 (supp. 11):1-176; 1967.
Only 6% of root filled teeth could be considered histologically healthy.
Green TL, Walton RE, Yaylor JK, Merrel P. Radiographic and histologic
periapical findings of root canal treated teeth in cadaver. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 83:707-711; 1997.
Barthel CR, Zimmer S, Trope M. Relationship of radiologic and histologic
signs of inflammation in human root-filled teeth. J Endod 30:75-79; 2004.

3yr 9mo3yr 9mo
6yr 8mo
100x
100x 400x
100x 400x1000x1000x
25x
400x
400x1000x

8yr 8mo3yr7mo
25x 50x
50x 100x
50x 100x
400x 1000x
100x 400x
25x 100x
100x 1000x

2
Can overfilling impair treatment outcome?

1yr 4yr 4mo
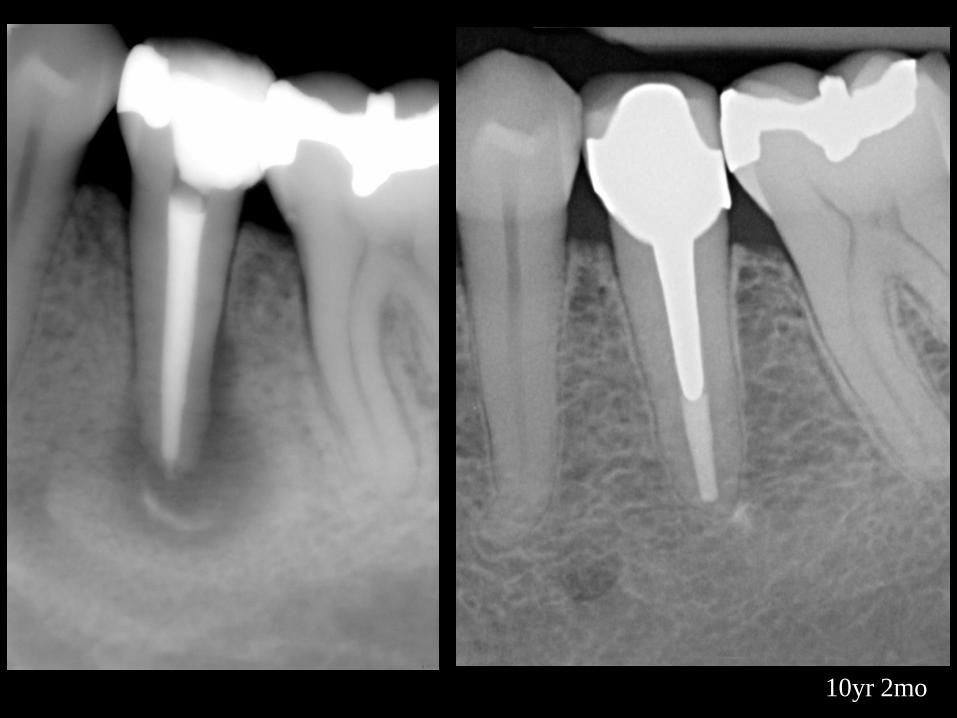
10yr 2mo
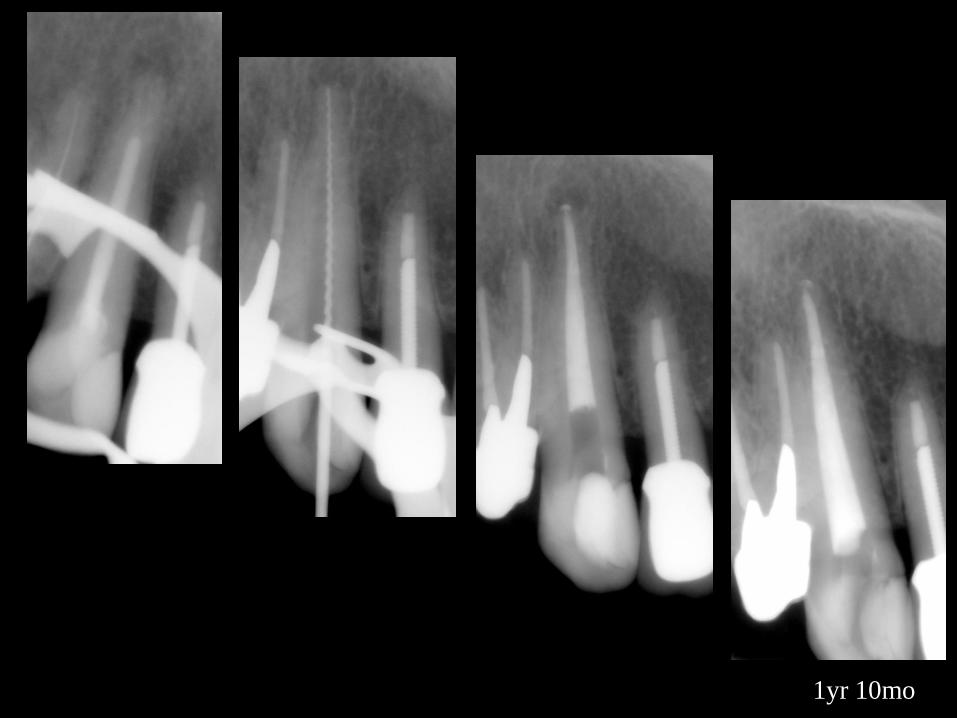
1yr 10mo
Spångberg LSW, Haapasalo M. Rationale and efficacy of root canal
medicaments and root filling materials with emphasis on treatment
outcome. Endodontic Topics 2:35-58; 2002.
“The majority of root canal filling materials are relatively inert after
setting...No commonly used material, however, can by itself cause a
progressively growing bone lesion. Therefore, it is logical to
question the wisdom of the negative effect observed on treatment
outcome of excess filling material. It appears that the increased rate
of failures associated with excess of materials also has some
association with failure to obtain a completely disinfected pulp
space before obturation.”

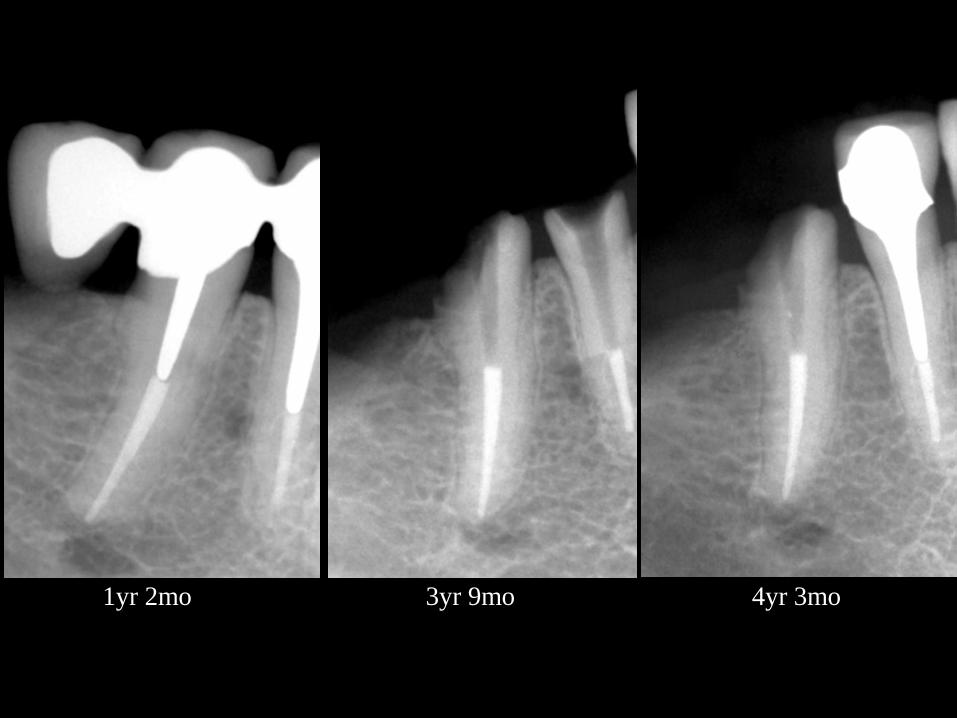
1yr 2mo 3yr 9mo 4yr 3mo
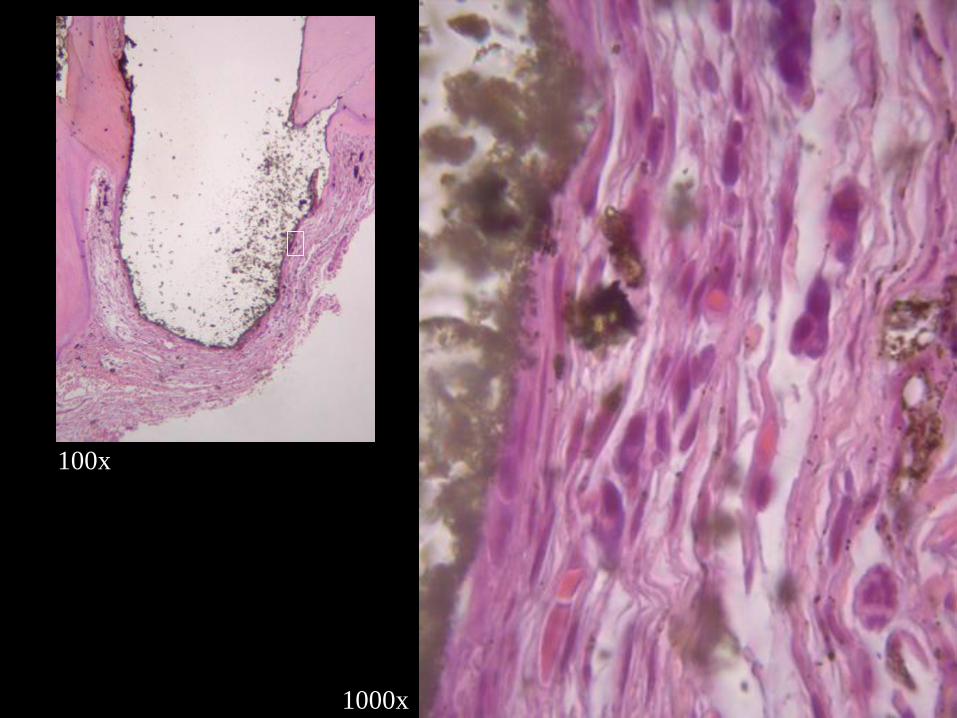
100x
1000x
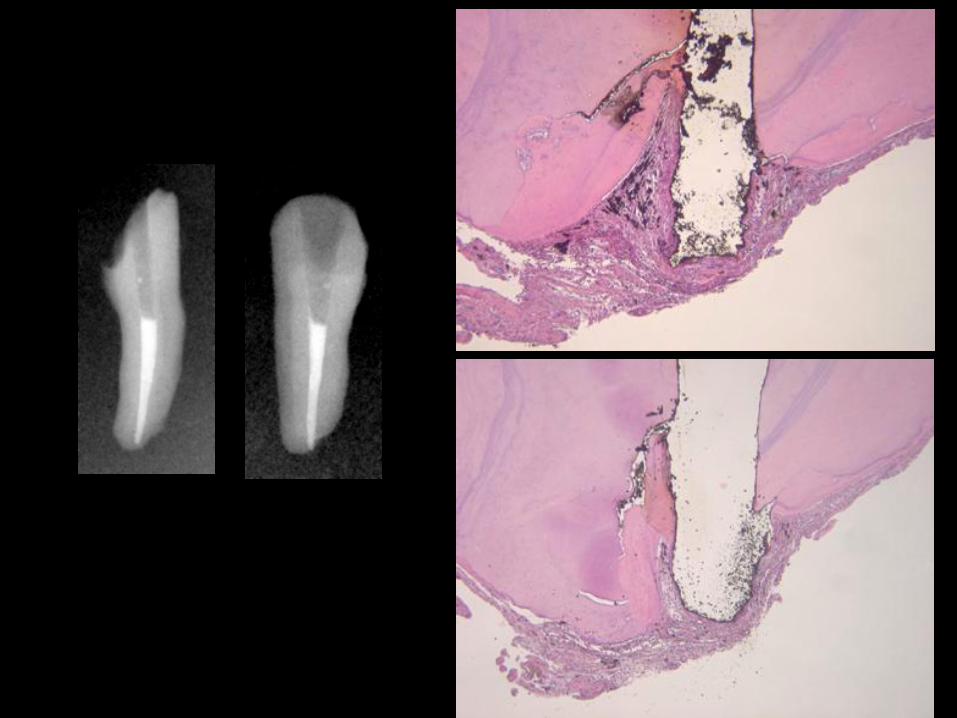
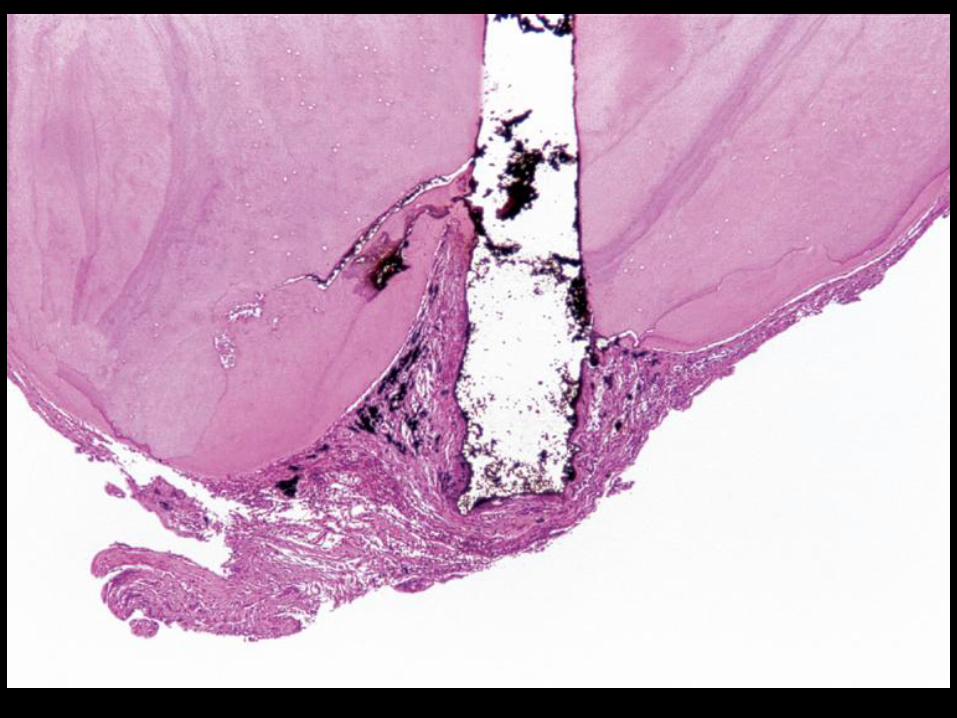
Ricucci D, Lin LM, Spångberg LSW. Wound healing of apical tissues after root
canal therapy: A long-term clinical, radiographic, and histopathologic observation
study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108:609-621; 2009.
51 human teeth
Observation periods ranged from 2 years to 22 years and 4 months
(mean 10 years 3 months).
Various sealers were used in a random fashion during this study. Most
commercially available sealers become practically inert after some
time. As the observation periods in this study was very long it is very
unlikely that any material toxicity would be discernible as tissue
changes. No clinical association with outcome could be observed
when comparing the long term treatment results of the sealer used
here.
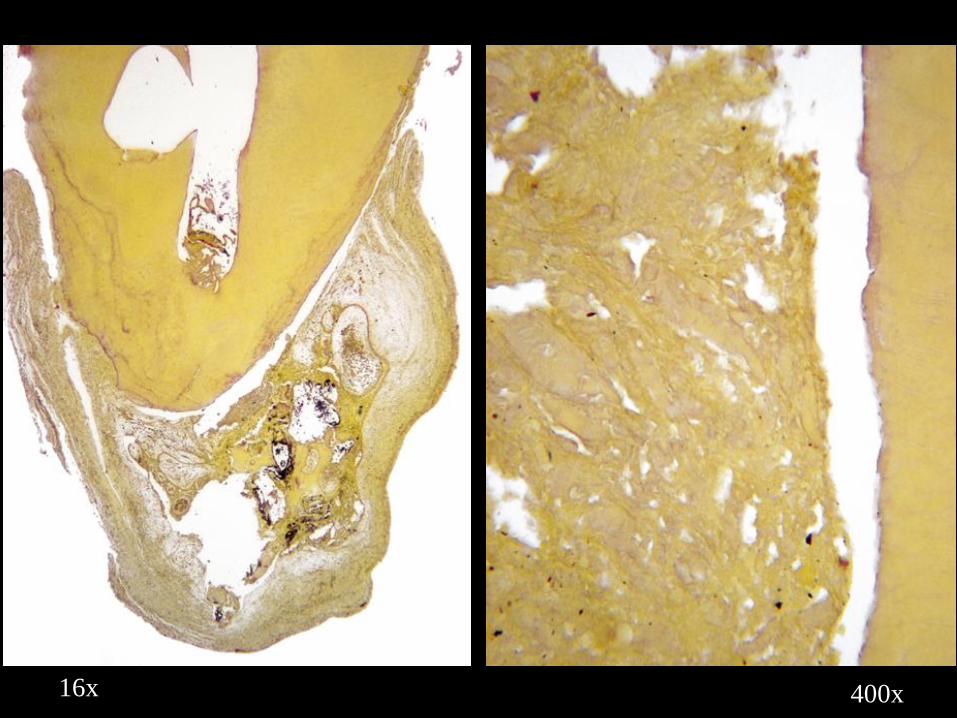
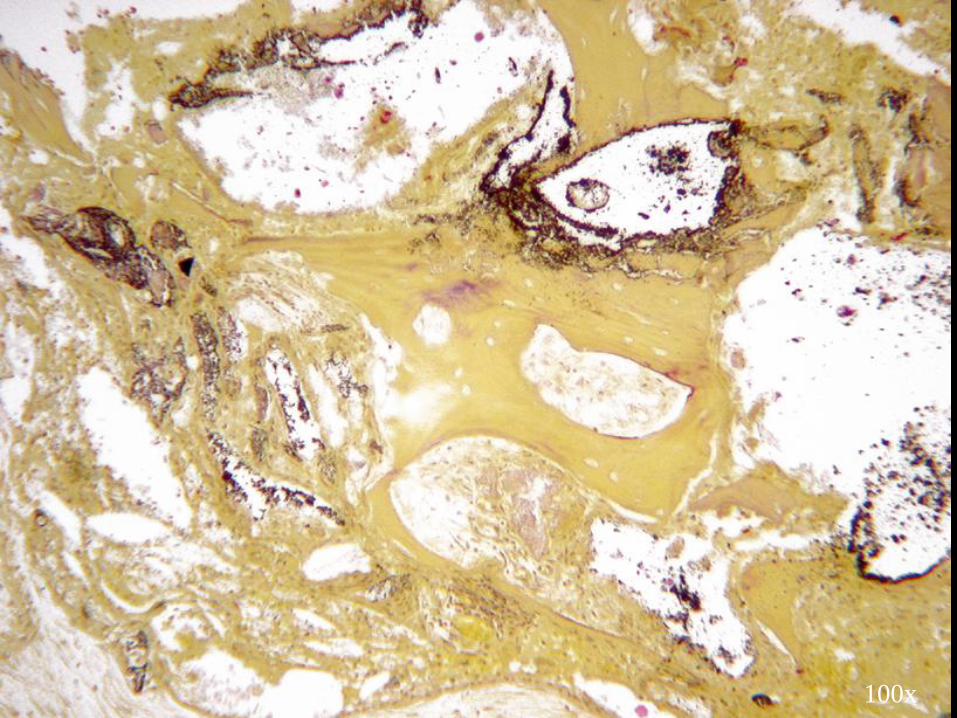
Ricucci D, Rôças IN, Alves FRF, Loghin S, Siqueira JF Jr.
Apically extruded sealers: fate and influence on treatment outcome.
Journal of Endodontics 2016. In press.
105 teeth treated by a single operator (75 of which showing apical
periodontitis lesions) and exhibiting overfillings in the postobturation
radiograph were included in the study.
Sealer included:
Pulp Canal Sealer (PCS), PCS Extended Working Time-EWT, Tubli-
Seal, Endomethasone, AH Plus, and Apexit.
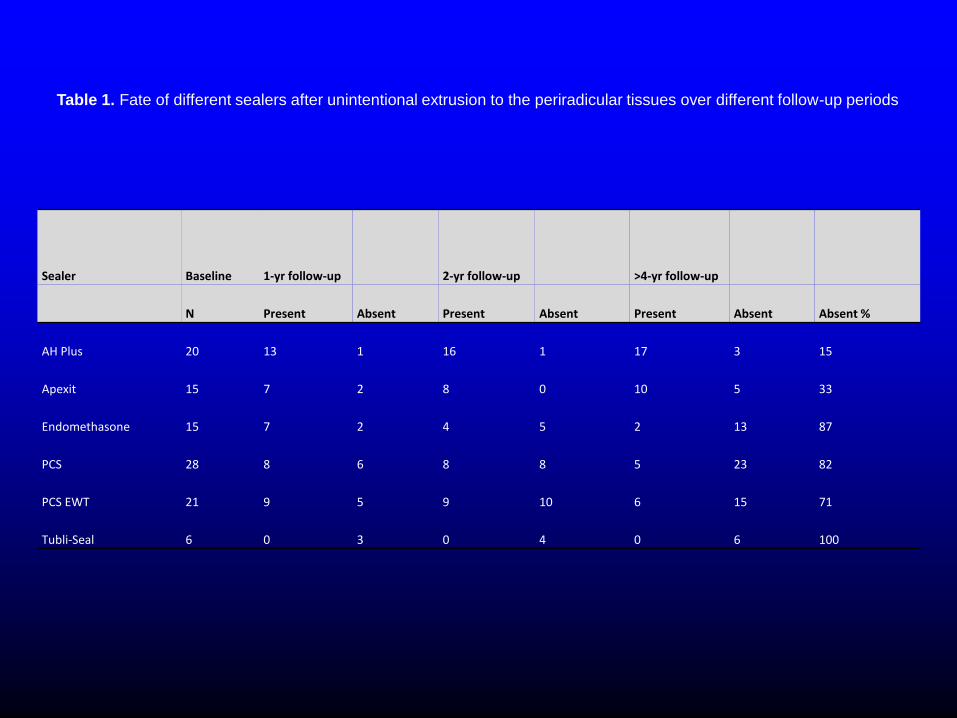
Sealer Baseline 1-yr follow-up 2-yr follow-up >4-yr follow-up
N Present Absent Present Absent Present Absent Absent %
AH Plus 20 13 1 16 1 17 3 15
Apexit 15 7 2 8 0 10 5 33
Endomethasone 15 7 2 4 5 2 13 87
PCS 28 8 6 8 8 5 23 82
PCS EWT 21 9 5 9 10 6 15 71
Tubli-Seal 6 0 3 0 4 0 6 100
Table 1. Fate of different sealers after unintentional extrusion to the periradicular tissues over different follow-up periods

4yr 7yr
PCS EWT
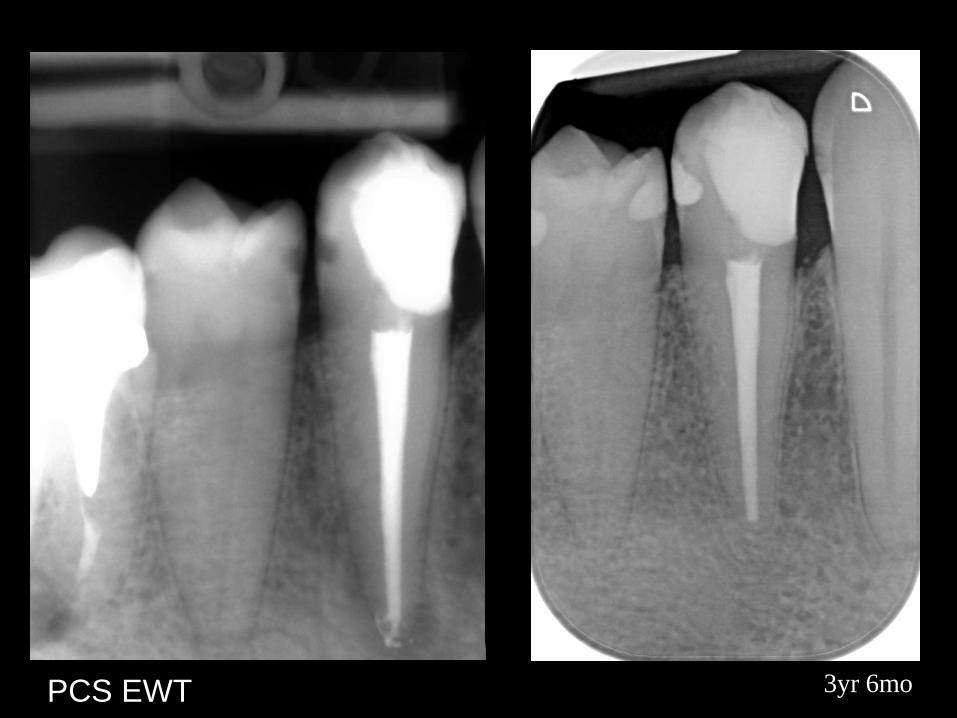
3yr 6moPCS EWT
5yr
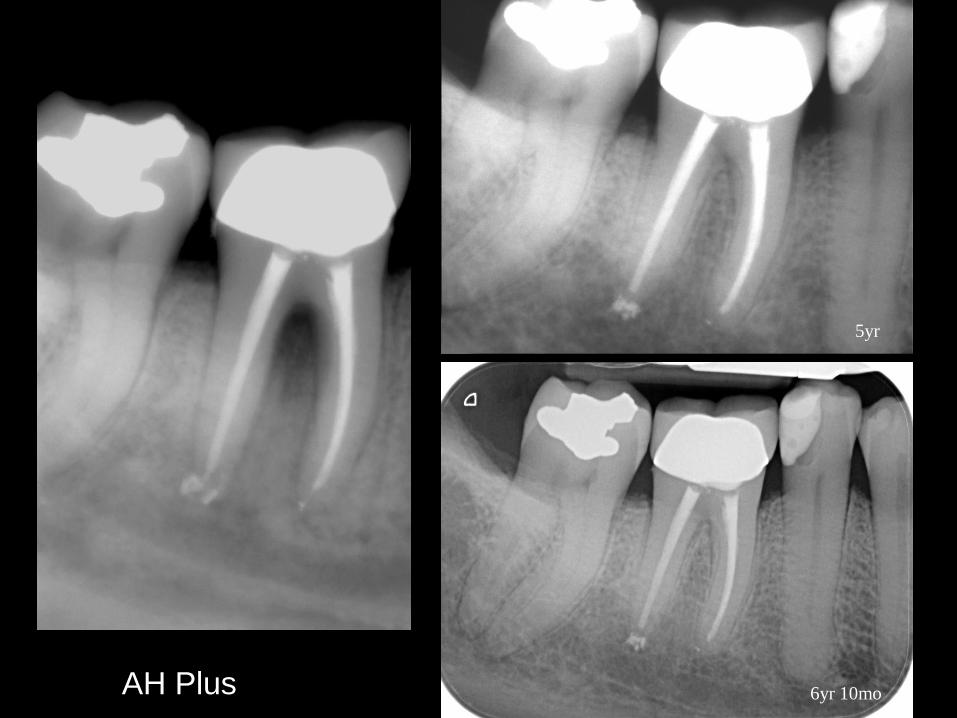
6yr 10mo AH Plus
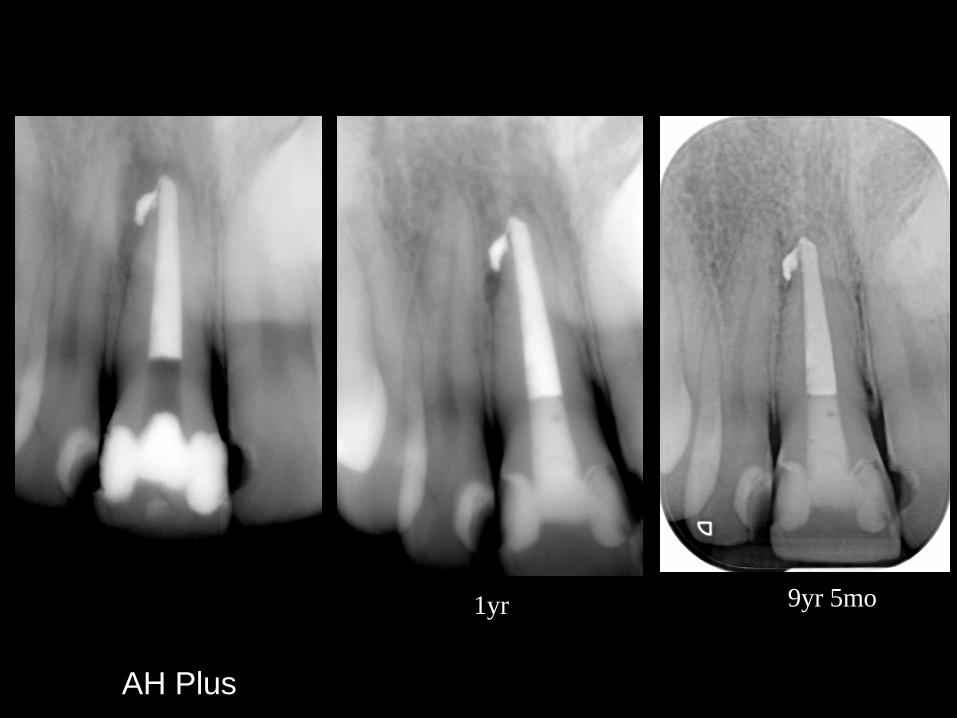
1yr 9yr 5mo
AH Plus

4yr 9mo
Apexit
16yr
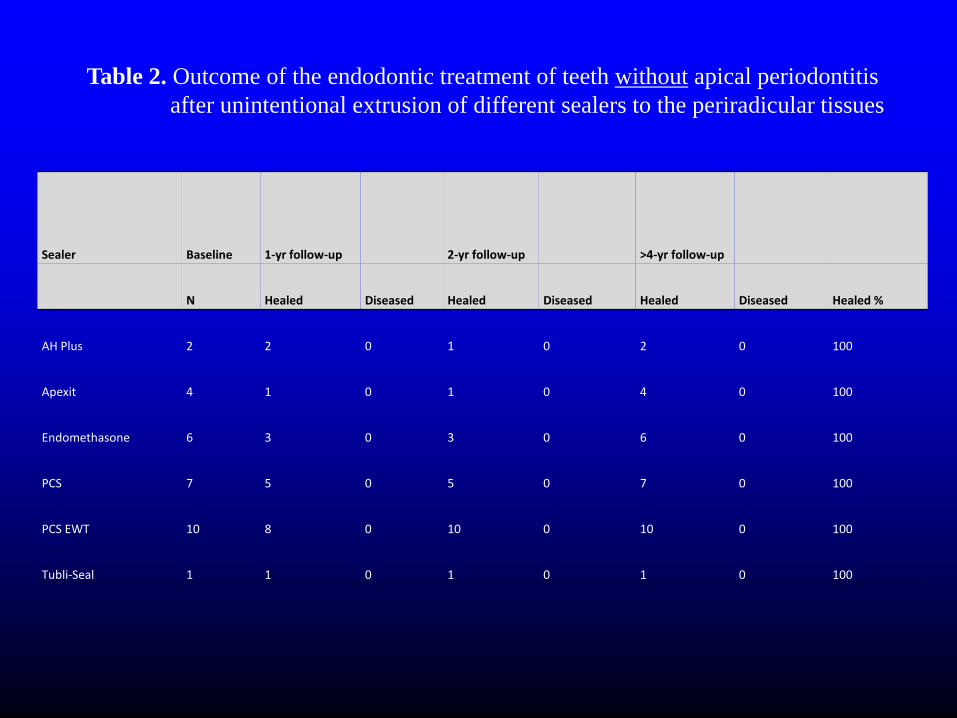
Table 2. Outcome of the endodontic treatment of teeth without apical periodontitis
after unintentional extrusion of different sealers to the periradicular tissues
Sealer Baseline 1-yr follow-up 2-yr follow-up >4-yr follow-up
N Healed Diseased Healed Diseased Healed Diseased Healed %
AH Plus 2 2 0 1 0 2 0 100
Apexit 4 1 0 1 0 4 0 100
Endomethasone 6 3 0 3 0 6 0 100
PCS 7 5 0 5 0 7 0 100
PCS EWT 10 8 0 10 0 10 0 100
Tubli-Seal 1 1 0 1 0 1 0 100
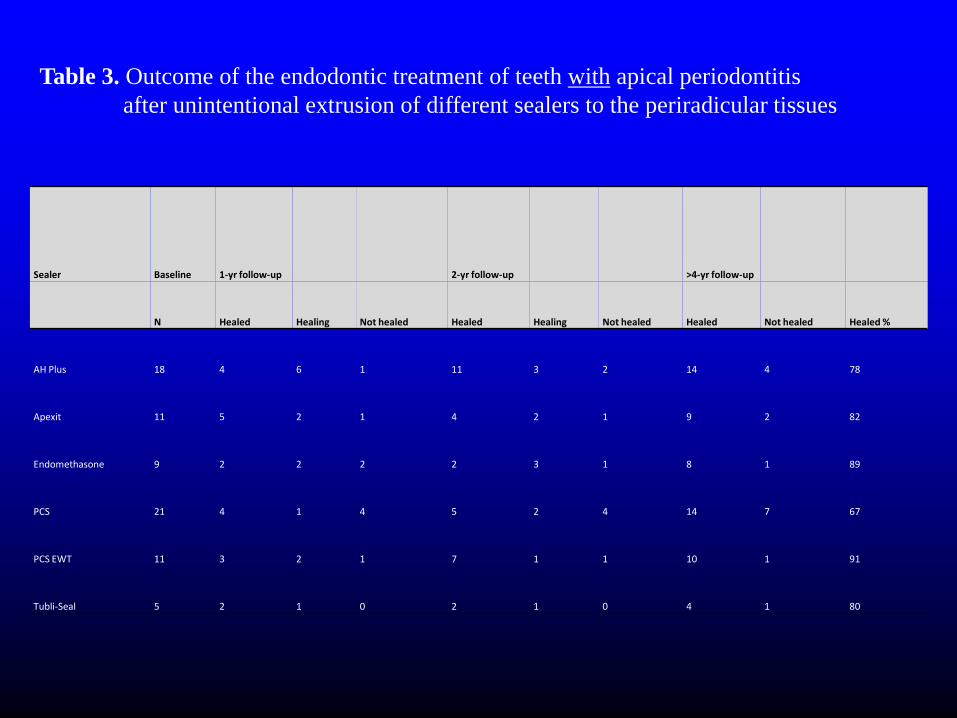
Table 3. Outcome of the endodontic treatment of teeth with apical periodontitis
after unintentional extrusion of different sealers to the periradicular tissues
Sealer Baseline 1-yr follow-up 2-yr follow-up >4-yr follow-up
N Healed Healing Not healed Healed Healing Not healed Healed Not healed Healed %
AH Plus 18 4 6 1 11 3 2 14 4 78
Apexit 11 5 2 1 4 2 1 9 2 82
Endomethasone 9 2 2 2 2 3 1 8 1 89
PCS 21 4 1 4 5 2 4 14 7 67
PCS EWT 11 3 2 1 7 1 1 10 1 91
Tubli-Seal 5 2 1 0 2 1 0 4 1 80

16x
50x
100x
400x
16x 400x
100x


10yr

13yr
10yr

13yr 23yr
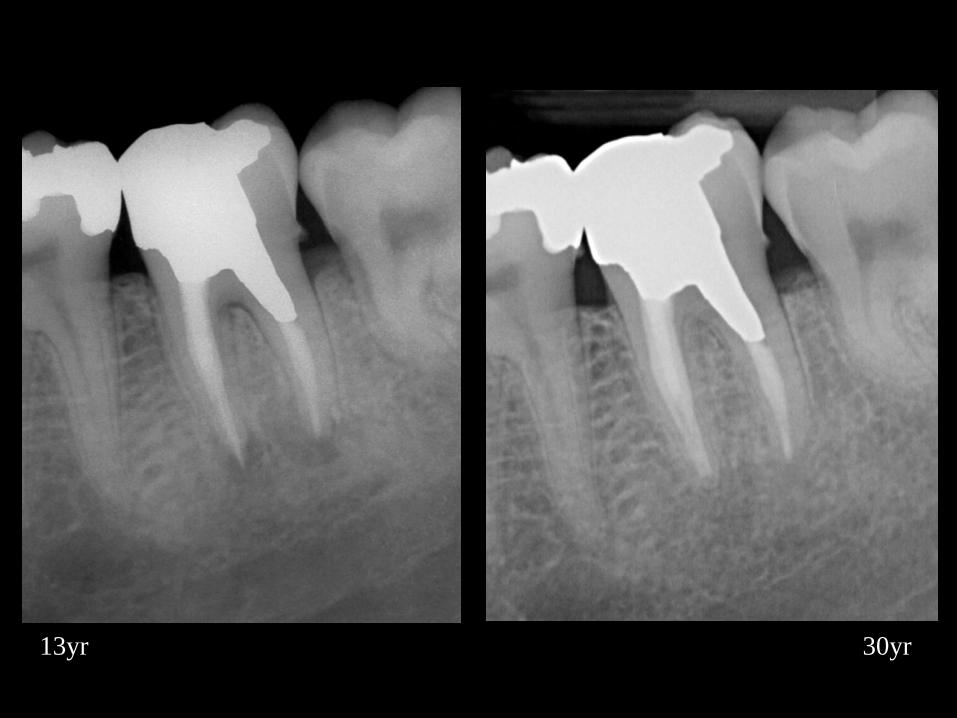
13yr 30yr
“14 of the 17 roots with late signs of periapical healing had been
filled with surpluss material extruding into the periapical area in
necrotic cases. These cases can, therefore, be explained as healing
processes disturbed by a foreign-body reaction.”
Molven O, Halse A, Fristad L, MacDonald-Jankowski D. Periapical changes
following root-canal treatment observed 20-27 years postoperatively. Int Endod J
35:784-790; 2002.
Fristad L, Molven O, Halse A. Nonsurgically retreated root-filled teeth –
radiographic findings after 20-27 years. Int Endod J 37:12-18; 2004.


















