
Hazardous metals in mineral processing plants in South … · Facilitating safety and health...
273
Facilitating safety and health research in the South African mining industry Hazardous metals in mineral processing plants in South Africa The risk of occupational exposure SIMRAC Project Support Services September 2000 SIMRAC Project Health 603
Transcript of Hazardous metals in mineral processing plants in South … · Facilitating safety and health...

Facilitating safety and health research in the South African mining industry
Hazardous metals in mineral processingplants in South Africa
The risk of occupational exposure
SIMRAC Project Support ServicesSeptember 2000
SIMRAC Project Health 603


Executive SummaryThe presence of heavy metals and exposure of employees thereto in mineral processing plantsin South Africa have not been studied and described in a format that can be used as a generalreference document. This document provides a review of different process steps in mineralprocessing and the associated health hazards from heavy metals. It should be particularlyuseful for those who are new in the field, and for the relatively uninformed who have to performduties that require some understanding of the processes and background to health riskassessment. In providing these perspectives, the following aspects were considered to be ofprimary importance:
• To provide an understanding of the paradigm of human health risk assessment in theoccupational environment;
• To identify heavy metals that would be of interest in mineral processing plants;• To review the context of target-organ toxicity of heavy metals in the quantification of
exposure and health risks, taking into account the concepts of speciation and bioavailability;• To provide information on the elements of occupational health risk management, providing
general principles for survey design, sampling philosophies, and interpretation methods.• To put the principles listed above in context with selected mineral processing plants in
South Africa.
The overall paradigm of health risk assessment was followed in the investigations, i.e.according to the steps of hazard assessment, dose-response assessment, exposureassessment, and risk characterisation.
The first step in the investigation was to select those metals that could be placed in thecategory of "heavy metals". A list was compiled on the basis of toxicological properties of theelements, and comprised of 33 elements. The elements were chosen with the objective ofhealth risk management in mind, rather than on the basis of the classical definition of "metals".
To assess the potential for exposure to heavy metals, the various industries must be wellunderstood. This study therefore reviewed fifteen selected industrial processes to identify unitoperations, potential toxicants, and exposure zones where hazards might be posed. Theinformation is presented in generic flow diagrams. The diagrams were developed to representthe general process steps, rather than detailed descriptions that were not essential forunderstanding the basic concepts and associated hazards. The process information wasverified by means of visits to typical plants and discussions with specialists in the various fields.This work formed the hazard assessment part of the investigation.
The following types of mineral processing plants were studied:• Carbon steel process with blast and basic oxygen furnace;• Carbon steel process with direct reduced iron and electric arc furnace;• Typical copper recovery circuit;• Typical ferrochromium production process;• Typical ferromanganese production process;• Bacterial oxidation circuit for the pre-oxidation of refractory gold ores;• Carbon-in-pulp circuit for gold recovery;• Nickel, copper, and cobalt refining process;• Typical phosphate rock production process;• Platinum group metal refining;• Typical stainless steel process;• Typical titanium dioxide production process;• Vanadium pentoxide production: the salt-roast process;• Vanadium slag production process; and• Typical circuit for zinc recovery from concentrate.

The dose-response assessment (toxicological assessment) was based on literatureinformation reviewed for the various metals. The primary routes of exposure to toxicants in theoccupational environment are via inhalation, ingestion, and dermal contact. Most metalliccompounds occur as solids, fumes, or in mists, and are frequently associated with particulates inthe occupational exposure scenario. Particle size determines where in the respiratory tractinhaled particles are deposited and hence can exert their toxic effects. Metals seldom interfacewith biological systems in the elemental form. They occur as compounds that vary with the easewith which they can pass through biological membranes. An extensive literature review wasconducted, covering surveys of the most prominent international publications on the subject. The large volume of data is summarised in tables. To place the information in context, concisedescriptions of the target organs of the body that are relevant to metal toxicity are alsopresented. Because several of the metals are present in more than one processing plant,toxicological information is presented together in one section of the report. The most relevantinformation is however highlighted in the sections that deal separately with each plant.
The exposure assessment part of the studies is also handled in the descriptions of the 15selected mineral processing plants. The approach however does not follow the conventionaloccupational hygiene process of sampling and chemical analysis. It is limited to theidentification of zones of exposure, and recommendations for monitoring. Because theprotocols for occupational exposure monitoring are more related to the substances of interestthan the particular processing plants, the methodologies for monitoring are presented togetherin one section in the report. Reference has however been made to appropriate monitoring inthe sections that deal separately with each plant.
Risk characterisation is presented in the paradigm for quantitative human health riskassessment. Risks were not quantified for the various exposure scenarios, but the overallapproach to risk assessment is presented. It indicates in which areas the highest risks mightbe expected, and consequently, where risk management should be applied. Human health riskcharacterisation is generally divided into the evaluation of carcinogenic and non-carcinogenicrisks. Carcinogenic risks are interpreted in terms of excess lifetime cancer risks. In theoccupational exposure range the estimated cancer risk is assumed to be linear and proportionalto dose. Risks are assumed to be additive per target organ across chemicals and pathways,unless data are available that would support synergistic or antagonistic effects. Risks areexpressed as excess cancer risk, i.e. risk not taking into account any existing risk as a result ofbackground exposure to substances that have the same carcinogenic properties. Noncarcinogenic risks are evaluated by comparison with reference concentrations. If the ratioof the air concentration to the reference concentration (hazard quotient) exceeds one, there is apotential that adverse health effects may occur. For multiple chemical exposures, hazardquotients are summed per target organ, unless data are available to demonstrate synergistic orantagonistic effects. This is based on the assumption that the response of a target organ tomultiple toxic agents is additive in a linear relationship. It is measured in terms of a hazardindex, which is the sum of the hazard quotients for the individual substances.

Table of contentsPage
Executive Summary...................................................................................................... 1List of Figures.......................................................................................................................11List of Tables ........................................................................................................................13Glossary of abbreviations, symbols and terms .................................................................17
1 Introduction ....................................................................................................231.1 Research problem statement .....................................................................231.2 Objectives and aims of this study .............................................................241.2.1 Main objective.......................................................................................................241.2.2 Goals .....................................................................................................................241.3 Research context and design.....................................................................241.3.1 Research context .................................................................................................241.3.2 Research design ..................................................................................................251.4 Deployment of the study...............................................................................25
2 Research methodology...........................................................................27
3 Literature review .........................................................................................293.1 Principles of health risk assessment .......................................................293.2 Hazard assessment .......................................................................................293.2.1 Criteria for selection.............................................................................................293.2.1.1 The classification of heavy metals ..........................................................................293.2.1.2 Regulatory classification .........................................................................................303.2.2 Use of the list of hazardous metals....................................................................313.3 Dose-response assessment .......................................................................313.3.1 Basic concepts in toxicology ...............................................................................313.3.2 Mechanisms of metals toxicity ............................................................................333.3.3 Target organ systems and toxic responses.......................................................363.3.3.1 Renal system..........................................................................................................363.3.3.2 Nervous system......................................................................................................363.3.3.3 Liver........................................................................................................................373.3.3.4 Gastrointestinal tract...............................................................................................373.3.3.5 Respiratory tract .....................................................................................................383.3.3.6 Haematopoietic system ..........................................................................................393.3.3.7 Bone.......................................................................................................................393.3.3.8 Endocrine system ...................................................................................................403.3.3.9 Muscle ....................................................................................................................403.3.3.10 Eye .........................................................................................................................403.3.3.11 Skin ........................................................................................................................403.3.3.12 Cardiovascular system ...........................................................................................413.3.3.13 Immune system ......................................................................................................413.3.3.14 Reproductive system ..............................................................................................423.3.4 Toxicology of the elements .................................................................................433.3.4.1 Antimony (Sb).........................................................................................................433.3.4.2 Arsenic (As) ............................................................................................................453.3.4.3 Barium (Ba) ............................................................................................................483.3.4.4 Beryllium (Be) .........................................................................................................50

3.3.4.5 Bismuth (Bi) ............................................................................................................523.3.4.6 Cadmium (Cd) ........................................................................................................543.3.4.7 Calcium (Ca)...........................................................................................................573.3.4.8 Chromium (Cr)........................................................................................................593.3.4.9 Cobalt (Co) .............................................................................................................613.3.4.10 Copper (Cu)............................................................................................................633.3.4.11 Indium (In) ..............................................................................................................653.3.4.12 Iron (Fe)..................................................................................................................673.3.4.13 Lead (Pb)................................................................................................................693.3.4.14 Manganese (Mn).....................................................................................................713.3.4.15 Mercury (Hg)...........................................................................................................743.3.4.16 Molybdenum (Mo)...................................................................................................763.3.4.17 Nickel (Ni) ...............................................................................................................783.3.4.18 Osmium (Os) ..........................................................................................................803.3.4.19 Platinum (Pt)...........................................................................................................823.3.4.20 Rhodium (Rh) .........................................................................................................843.3.4.21 Selenium (Se).........................................................................................................863.3.4.22 Silver (Ag)...............................................................................................................883.3.4.23 Tantalum (Ta).........................................................................................................903.3.4.24 Tellurium (Te) .........................................................................................................923.3.4.25 Thallium (Tl) ...........................................................................................................943.3.4.26 Tin (Sn)...................................................................................................................963.3.4.27 Titanium (Ti) ...........................................................................................................983.3.4.28 Tungsten (W) .......................................................................................................1003.3.4.29 Uranium (U) ..........................................................................................................1023.3.4.30 Vanadium (V)........................................................................................................1043.3.4.31 Yttrium (Y) ............................................................................................................1063.3.4.32 Zinc (Zn) ...............................................................................................................1083.3.4.33 Zirconium (Zr) .......................................................................................................1103.4 Exposure assessment: General guidelines for occupational
health risk assessment and management...........................................1123.4.1 Context ................................................................................................................1123.4.2 The relationship between dust and heavy metals in exposure
assessment.........................................................................................................1123.4.3 Physical monitoring of the workplace...............................................................1143.4.3.1 Direct-reading instruments....................................................................................1143.4.3.2 Detector-tube measurements ...............................................................................1143.4.3.3 Air sampling and analysis .....................................................................................1143.4.3.4 Selection of appropriate positions for monitoring ..................................................1153.4.3.5 Personal sampling ................................................................................................1183.4.3.6 Sampling and analytical methods for exposure assessment.................................1203.4.4 Medical evaluation .............................................................................................1243.4.4.1 Medical surveillance..............................................................................................1243.4.4.2 Biological effect monitoring...................................................................................1253.4.4.3 Biological monitoring.............................................................................................1253.4.4.4 Medical evaluation summary: procedures relevant to the various heavy metals ...1273.5 Risk characterisation ...................................................................................1343.6 References ......................................................................................................134
4 Carbon steel process with blast furnace and basicoxygen furnace ..........................................................................................141
4.1 Introduction......................................................................................................141

4.2 Process description......................................................................................1414.2.1 Coke preparation................................................................................................1414.2.2 Sintering ..............................................................................................................1424.2.3 Storage/blending/material handling..................................................................1434.2.4 Blast furnace treatment .....................................................................................1434.2.5 Basic oxygen furnace treatment .......................................................................1444.2.6 Further refining, casting, rolling, pickling, galvanising....................................1454.3 Process diagram ...........................................................................................1464.4 Process assessment....................................................................................1464.4.1 Hazard identification ..........................................................................................1464.4.2 Toxicological assessment .................................................................................1484.4.3 Exposure assessment .......................................................................................1484.4.4 Risk quantification..............................................................................................1484.5 References ......................................................................................................148
5 Carbon steel process with direct reduced iron andelectric arc furnace..................................................................................151
5.1 Introduction......................................................................................................1515.2 Process description......................................................................................1515.2.1 Grinding...............................................................................................................1515.2.2 Pelletisation ........................................................................................................1525.2.3 Direct reduction ..................................................................................................1525.2.4 Electric arc furnace ............................................................................................1535.2.5 Casting, rolling, pickling, galvanising ...............................................................1545.3 Flow diagram ..................................................................................................1545.4 Process assessment....................................................................................1565.4.1 Hazard identification ..........................................................................................1565.4.2 Toxicological assessment .................................................................................1565.4.3 Exposure assessment .......................................................................................1565.4.4 Risk quantification..............................................................................................1575.5 References ......................................................................................................157
6 Typical copper recovery circuit ........................................................1596.1 Introduction......................................................................................................1596.2 Process description......................................................................................1596.2.1 Crushing and milling ..........................................................................................1596.2.2 Flotation and magnetic separation ...................................................................1596.2.3 Liquid/solid separation/drying ...........................................................................1606.2.4 Smelting and converting....................................................................................1606.2.5 Refining and rod casting....................................................................................1616.3 Flow diagram ..................................................................................................1616.4 Process assessment....................................................................................1626.4.1 Hazard identification ..........................................................................................1626.4.2 Toxicological assessment .................................................................................1626.4.3 Exposure assessment .......................................................................................1626.4.4 Risk quantification..............................................................................................1646.5 References ......................................................................................................164
7 Typical ferrochrome production process ...................................1657.1 Introduction......................................................................................................1657.2 Process description......................................................................................1657.2.1 Beneficiation .......................................................................................................1657.2.2 Material Handling ...............................................................................................1667.2.3 Smelting ..............................................................................................................1677.2.4 Alloy casting and sizing .....................................................................................1697.2.5 Metal recovery from slag ...................................................................................1697.3 Flow diagram ..................................................................................................1707.4 Process assessment....................................................................................1707.4.1 Hazard identification ..........................................................................................1707.4.2 Toxicological assessment .................................................................................1707.4.3 Exposure assessment .......................................................................................1707.4.4 Risk quantification..............................................................................................1707.5 References ......................................................................................................172
8 Typical ferromanganese production process..........................1738.1 Introduction......................................................................................................1738.2 Process description......................................................................................1738.2.1 Beneficiation .......................................................................................................1738.2.2 Sintering ..............................................................................................................1748.2.3 Material handling................................................................................................1748.2.4 8.2.4 Smelting ....................................................................................................1758.2.5 Alloy casting, crushing and sizing.....................................................................1768.2.6 Metal recovery from slag ...................................................................................1778.3 Flow diagram ..................................................................................................1778.4 Process assessment....................................................................................1778.4.1 Hazard identification ..........................................................................................1778.4.2 Toxicological assessment .................................................................................1778.4.3 Exposure assessment .......................................................................................1798.4.4 Risk quantification..............................................................................................1798.5 References ......................................................................................................179
9 Bacterial oxidation circuit for the pre-oxidation ofrefractory gold ores .................................................................................181
9.1 Introduction......................................................................................................1819.2 Process description......................................................................................1819.2.1 Crushing, Screening and Milling.......................................................................1819.2.2 Gravity concentration.........................................................................................1819.2.3 Flotation ..............................................................................................................1819.2.4 Bacterial oxidation and gold recovery ..............................................................1829.2.5 Bioliquor neutralisation/thickening and disposal .............................................1839.3 Flow diagram ..................................................................................................1849.4 Process assessment....................................................................................1849.4.1 Hazard identification ..........................................................................................1849.4.2 Toxicological assessment .................................................................................1849.4.3 Exposure assessment .......................................................................................184

9.4.4 Risk quantification..............................................................................................1869.5 References ......................................................................................................186
10 Carbon-in-pulp circuit for gold recovery.....................................18710.1 Introduction......................................................................................................18710.2 Process description......................................................................................18710.2.1 Crushing..............................................................................................................18710.2.2 Milling ..................................................................................................................18710.2.3 Thickening...........................................................................................................18810.2.4 Leaching..............................................................................................................18810.2.5 Adsorption...........................................................................................................18910.2.6 Stripping and carbon regeneration...................................................................19010.2.7 Electrowinning ....................................................................................................19110.2.8 Smelting ..............................................................................................................19210.2.9 Residue disposal................................................................................................19210.3 Flow diagram ..................................................................................................19210.4 Process assessment....................................................................................19410.4.1 Hazard identification ..........................................................................................19410.4.2 Toxicological assessment .................................................................................19410.4.3 Exposure assessment .......................................................................................19410.4.4 Risk quantification..............................................................................................19410.5 References ......................................................................................................194
11 Nickel, copper, cobalt refining processes .................................19511.1 Introduction......................................................................................................19511.2 Process description: option 1 ...................................................................19511.2.1 Matte grinding.....................................................................................................19511.2.2 Atmospheric Pressure Leach and Nickel Sulphate Crystallisation ...............19611.2.3 Pressure leach ...................................................................................................19711.2.4 Selenium removal ..............................................................................................19811.2.5 Copper electrowinning.......................................................................................19811.3 Flow diagram: option 1................................................................................19811.4 Process assessment: option 1.................................................................20011.4.1 Hazard identification ..........................................................................................20011.4.2 Toxicological assessment .................................................................................20011.4.3 Exposure assessment .......................................................................................20011.4.4 Risk quantification..............................................................................................20111.5 References: option 1....................................................................................20111.6 Process description: option 2 ...................................................................20211.6.1 Slow cool/crush/mill/magnetic concentration ..................................................20211.6.2 Copper cementation ..........................................................................................20211.6.3 Primary pressure leach......................................................................................20311.6.4 Secondary pressure leach ................................................................................20311.6.5 Copper electrowinning.......................................................................................20311.6.6 Cobalt removal ...................................................................................................20411.6.7 Nickel electrowinning .........................................................................................20411.6.8 Sulphur removal .................................................................................................20511.7 Flow diagram: option 2................................................................................205

11.8 Process assessment: option 2.................................................................20511.8.1 Hazard identification ..........................................................................................20511.8.2 Toxicological assessment .................................................................................20511.8.3 Exposure assessment .......................................................................................20711.8.4 Risk quantification..............................................................................................20711.9 References: option 2....................................................................................207
12 Typical phosphate rock production process............................20912.1 Introduction......................................................................................................20912.2 Process description......................................................................................20912.2.1 Crushing and Milling ..........................................................................................20912.2.2 Flotation of copper sulphide..............................................................................20912.2.3 Magnetic separation of magnetite ....................................................................21012.2.4 Phosphate flotation ............................................................................................21012.2.5 Phosphate rock concentrate treatment............................................................21012.2.6 Phosphoric acid production...............................................................................21112.3 Flow diagram ..................................................................................................21212.4 Process assessment....................................................................................21212.4.1 Hazard identification ..........................................................................................21212.4.2 Toxicological assessment .................................................................................21412.4.3 Exposure assessment .......................................................................................21412.4.4 Risk quantification..............................................................................................21412.5 References ......................................................................................................214
13 Platinum group metal refining...........................................................21513.1 Introduction......................................................................................................21513.2 Process description......................................................................................21513.2.1 Leaching..............................................................................................................21513.2.2 Gold extraction ...................................................................................................21613.2.3 Palladium extraction ..........................................................................................21613.2.4 Base metal separation.......................................................................................21713.2.5 Ruthenium separation .......................................................................................21713.2.6 Rhodium/iridium/osmium separation................................................................21713.2.7 Platinum recovery ..............................................................................................21813.3 Flow diagram ..................................................................................................21813.4 Process assessment....................................................................................21813.4.1 Hazard identification ..........................................................................................21813.4.2 Toxicological assessment .................................................................................22013.4.3 Exposure assessment .......................................................................................22013.4.4 Risk quantification..............................................................................................22213.5 References ......................................................................................................222
14 Typical stainless steel process........................................................22514.1 Introduction......................................................................................................22514.2 Process description......................................................................................22514.2.1 Raw material receipts and charge preparation ...............................................22514.2.2 Furnace charging and melting ..........................................................................227

14.2.3 Stainless steel refining.......................................................................................22814.2.4 Continuous casting ............................................................................................22914.2.5 Hot rolling............................................................................................................23014.2.6 Annealing and pickling.......................................................................................23014.2.7 Cold rolling and bright annealing......................................................................23114.2.8 Cutting to length, slitting, packing and despatching .......................................23114.2.9 Effluent treatment plant .....................................................................................23214.2.10 Water treatment/handling..................................................................................23214.3 Flow diagram ..................................................................................................23214.4 Process assessment....................................................................................23514.4.1 Hazard identification ..........................................................................................23514.4.2 Toxicological assessment .................................................................................23514.4.3 Exposure assessment .......................................................................................23514.4.4 Risk quantification..............................................................................................23714.5 References ......................................................................................................237
15 Typical titanium dioxide production process ...........................23915.1 Introduction......................................................................................................23915.2 Process description......................................................................................23915.2.1 Milling ..................................................................................................................23915.2.2 Digestion/production of digester residue byproduct .......................................23915.2.3 Hydrolysis/leaching/washing.............................................................................24015.2.4 Production of gypsum byproduct......................................................................24115.2.5 Calcining .............................................................................................................24215.2.6 Pigment finishing................................................................................................24215.3 Flow diagram ..................................................................................................24315.4 Process assessment....................................................................................24315.4.1 Hazard identification ..........................................................................................24315.4.2 Toxicological assessment .................................................................................24315.4.3 Exposure assessment .......................................................................................24515.4.4 Risk quantification..............................................................................................24515.5 References ......................................................................................................246
16 The salt-roast process for vanadium pentoxideproduction .....................................................................................................247
16.1 Introduction......................................................................................................24716.2 Process description......................................................................................24716.2.1 Crushing and milling ..........................................................................................24716.2.2 Magnetic separation and de-watering..............................................................24716.2.3 Roasting ..............................................................................................................24816.2.4 Leaching..............................................................................................................24816.2.5 Precipitation and vanadium pentoxide production..........................................24916.3 Flow diagram ..................................................................................................25016.4 Process assessment....................................................................................25016.4.1 Hazard identification ..........................................................................................25016.4.2 Toxicological assessment .................................................................................25016.4.3 Exposure assessment .......................................................................................25216.4.4 Risk quantification..............................................................................................252

16.5 References ......................................................................................................253
17 Vanadium slag production process...............................................25517.1 Introduction......................................................................................................25517.2 Process description......................................................................................25517.2.1 Crushing, screening and magnetic separation................................................25517.2.2 Pre-reduction ......................................................................................................25517.2.3 Electric arc smelting...........................................................................................25617.2.4 Shaking ladles/vanadium slag upgrading ........................................................25717.3 Flow diagram ..................................................................................................25817.4 Process assessment....................................................................................26017.4.1 Hazard identification ..........................................................................................26017.4.2 Toxicological assessment .................................................................................26017.4.3 Exposure assessment .......................................................................................26017.4.4 Risk quantification..............................................................................................26117.5 References ......................................................................................................261
18 Typical circuit for zinc recovery from concentrate ...............26318.1 Introduction......................................................................................................26318.2 Process description......................................................................................26318.2.1 Roasting ..............................................................................................................26318.2.2 Leaching and precipitation ................................................................................26418.2.3 Purification ..........................................................................................................26518.2.3 Electrowinning ....................................................................................................26618.2.4 Effluent treatment...............................................................................................26618.3 Flow diagram ..................................................................................................26718.4 Process assessment....................................................................................26718.4.1 Hazard identification ..........................................................................................26718.4.2 Toxicological assessment .................................................................................26918.4.3 Exposure assessment .......................................................................................26918.4.4 Risk quantification..............................................................................................27118.5 References ......................................................................................................271

List of FiguresPage
Figure 3.2.1.1 Periodic table of the elements, showing those elements that wereselected for investigation...........................................................................30
Figure 3.4.4.3 Types of monitoring in occupational health protection (afterLauwerys and Hoet, 1993: 9) ..................................................................126
Figure 4.3 Process diagram for the carbon steel process with blast furnaceand basic oxygen furnace. ......................................................................147
Figure 5.3 Process diagram for the carbon steel process with with directreduced iron and electric arc furnace. .....................................................155
Figure 6.3 Process diagram for the copper recovery circuit .....................................163Figure 7.3 Process diagram for the ferrochrome recovery circuit .............................171Figure 9.3 Process diagram for the bacterial oxidation circuit for the pre-
oxidation of refractory gold ores..............................................................185Figure 10.3 Process diagram for the carbon-in-pulp circuit for gold recovery.............193Figure 11.3 Process diagram for the Ni, Cu, Co refining process – option 1 ..............199Figure 11.7 Process diagram for the Ni, Cu, Co refining process – option 2 ..............206Figure 12.3 Process diagram for the phosphate rock production process..................213Figure 13.3 Process diagram for a platinum group metal refining process.................219Figure 14.3.1 Process diagram for a typical stainless steel process, sheet 1 of 2.........233Figure 14.3.2 Process diagram for a typical stainless steel process, sheet 2 of 2.........234Figure 15.3 Process diagram for a typical titanium dioxide production process .........244Figure 16.3 Process diagram for the vanadium pentoxide production circuit..............251Figure 17.3 Process diagram for the vanadium slag production process ...................259Figure 18.3 Process diagram for a typical circuit for zinc recovery from
concentrate .............................................................................................268


List of TablesPage
Table 3.2.1.2 List of elements selected for assessment .................................................31Table 3.3.1 The IARC classification for carcinogenicity ...............................................32Table 3.3.4.1 Antimony: Toxicological properties and target-organ effects .....................44Table 3.3.4.2 Arsenic: Toxicological properties and target-organ effects........................46Table 3.3.4.3 Barium: Toxicological properties and target-organ effects ........................49Table 3.3.4.4 Beryllium: Toxicological properties and target-organ effects .....................51Table 3.3.4.5 Bismuth: Toxicological properties and target-organ effects.......................53Table 3.3.4.6 Cadmium: Toxicological properties and target-organ effects.....................55Table 3.3.4.7 Calcium: Toxicological properties and target-organ effects .......................58Table 3.3.4.8 Chromium: Toxicological properties and target-organ effects ...................60Table 3.3.4.9 Cobalt: Toxicological properties and target-organ effects .........................62Table 3.3.4.10 Copper: Toxicological properties and target-organ effects ........................64Table 3.3.4.11 Indium: Toxicological properties and target-organ effects .........................66Table 3.3.4.12 Iron: Toxicological properties and target-organ effects..............................68Table 3.3.4.13 Lead: Toxicological properties and target-organ effects............................70Table 3.3.4.14 Manganese: Toxicological properties and target-organ effects .................72Table 3.3.4.15 Mercury: Toxicological properties and target-organ effects .......................75Table 3.3.4.16 Molybdenum: Toxicological properties and target-organ effects................77Table 3.3.4.17 Nickel: Toxicological properties and target-organ effects ..........................79Table 3.3.4.18 Osmium: Toxicological properties and target-organ effects ......................81Table 3.3.4.19 Platinum: Toxicological properties and target-organ effects ......................83Table 3.3.4.20 Rhodium: Toxicological properties and target-organ effects......................85Table 3.3.4.21 Selenium: Toxicological properties and target-organ effects .....................87Table 3.3.4.22 Silver: Toxicological properties and target-organ effects...........................89Table 3.3.4.23 Tantalum: Toxicological properties and target-organ effects.....................91Table 3.3.4.24 Tellurium: Toxicological properties and target-organ effects .....................93Table 3.3.4.25 Thallium: Toxicological properties and target-organ effects ......................95Table 3.3.4.26 Tin: Toxicological properties and target-organ effects...............................97Table 3.3.4.27 Titanium: Toxicological properties and target-organ effects ......................99Table 3.3.4.28 Tungsten: Toxicological properties and target-organ effects...................101Table 3.3.4.29 Uranium: Toxicological properties and target-organ effects ....................103Table 3.3.4.30 Vanadium: Toxicological properties and target-organ effects..................105Table 3.3.4.31 Yttrium (and rare earth elements): Toxicological properties and
target-organ effects.................................................................................107Table 3.3.4.32 Zinc: Toxicological properties and target-organ effects ...........................109Table 3.3.4.33 Zirconium: Toxicological properties and target-organ effects ..................111Table 3.4.2 Maximum concentrations of heavy metals that can be tolerated at
the maximum permissible dust loads in the occupationalenvironment ............................................................................................112
Table 3.4.3.2 Some detector tubes for screening assessment of exposure ..................114Table 3.4.3.4a Size of partial sample for the top 10 % potential release points at a
confidence level of 90 % .........................................................................116Table 3.4.3.4b Table of random numbers after NIOSH (1977) .......................................117Table 3.4.3.5 Size of partial sample for the top 10 % exposure subgroup at a
confidence level of 90 % .........................................................................119Table 3.4.3.6 List of NIOSH and OSHA sampling and analytical methods for air
monitoring ...............................................................................................120Table 3.4.4.3 Analytical methods for biological monitoring............................................127Table 3.4.4.4 Summary of medical surveillance, biological effects monitoring, and
biological monitoring ...............................................................................129Table 4.2.1 Coke preparation ....................................................................................142Table 4.2.2 Sintering..................................................................................................142

Table 4.2.3 Storage, blending and material handling .................................................143Table 4.2.4 Blast furnace treatment...........................................................................144Table 4.2.5 Basic oxygen furnace treatment..............................................................144Table 4.2.6 Further refining, casting, rolling, pickling, galvanising .............................146Table 5.2.1 Grinding ..................................................................................................151Table 5.2.2 Pelletisation.............................................................................................152Table 5.2.3 Direct reduction.......................................................................................152Table 5.2.4 Electric arc furnace .................................................................................153Table 5.2.5 Casting, rolling, pickling, galvanising.......................................................154Table 6.2.1 Crushing and milling................................................................................159Table 6.2.2 Flotation and magnetic separation ..........................................................160Table 6.2.3 Liquid/solid separation/drying..................................................................160Table 6.2.4 Smelting and converting..........................................................................161Table 6.2.5 Refining and rod casting .........................................................................161Table 7.2.1 Beneficiation ...........................................................................................166Table 7.2.2 Material handling.....................................................................................166Table 7.2.3 Smelting..................................................................................................168Table 7.2.4 Alloy casting and sizing...........................................................................169Table 8.2.1 Beneficiation ...........................................................................................174Table 8.2.2 Sintering..................................................................................................174Table 8.2.3 Material handling.....................................................................................175Table 8.2.4 Smelting..................................................................................................176Table 8.2.5 Alloy casting, crushing and sizing ...........................................................177Table 8.2.6 Metal recovery from slag.........................................................................177Table 9.2.1 Crushing, screening, wet milling..............................................................181Table 9.2.3 Flotation ..................................................................................................182Table 9.2.4 Bacterial oxidation and gold recovery......................................................183Table 9.2.5 Bioliquor neutralisation/thickening and disposal ......................................184Table 10.2.1 Crushing .................................................................................................187Table 10.2.3 Milling......................................................................................................188Table 10.2.3 Thickening ..............................................................................................188Table 10.2.4 Leaching .................................................................................................188Table 10.2.5 Adsorption...............................................................................................190Table 10.2.6 Stripping and carbon regeneration ..........................................................191Table 10.2.7 Electrowinning.........................................................................................191Table 10.2.8 Smelting..................................................................................................192Table 10.3.9 Residue disposal.....................................................................................192Table 11.2.1 Matte grinding .........................................................................................196Table 11.2.2 Atmospheric pressure leach and nickel sulphate crystallisation ..............197Table 11.2.3 Pressure leach ........................................................................................197Table 11.2.4 Selenium removal ...................................................................................198Table 11.2.5 Copper electrowinning ............................................................................198Table 11.6.1 Slow cool/crush/mill/magnetic concentration ...........................................202Table 11.6.4 Secondary pressure leach.......................................................................203Table 11.6.5 Copper electrowinning ............................................................................204Table 11.6.6 Cobalt removal........................................................................................204Table 11.6.7 Nickel electrowinning ..............................................................................205Table 12.2.1 Crushing and milling................................................................................209Table 12.2.2 Flotation of copper sulphide ....................................................................210Table 12.2.3 Magnetic separation of magnetite ...........................................................210Table 12.2.5 Phosphate rock concentrate treatment ...................................................211Table 12.2.6 Phosphoric acid production .....................................................................211Table 13.2.1 Leaching .................................................................................................216Table 13.2.2 Gold extraction........................................................................................216Table 13.2.3 Palladium extraction................................................................................217Table 13.2.4 Base metal separation ............................................................................217

Table 13.2.5 Ruthenium separation .............................................................................217Table 13.2.6 Rhodium/iridium/osmium separation .......................................................218Table 13.2.7 Platinum recovery ...................................................................................218Table 14.2.1 Raw material receipts and charge preparation ........................................225Table 14.2.2 Furnace charging and melting.................................................................228Table 14.2.3 Stainless steel refining ............................................................................229Table 14.2.4 Continuous casting .................................................................................229Table 14.2.5 Hot rolling................................................................................................230Table 14.2.6 Annealing and pickling ............................................................................231Table 14.2.7 Cold rolling and bright annealing.............................................................231Table 14.2.8 Cutting to length, slitting, packing and despatching ................................232Table 15.2.1 Milling......................................................................................................239Table 15.2.2 Digestion.................................................................................................240Table 15.2.3 Hydrolysis/Leaching/Washing .................................................................241Table 15.2.4 Production of Gypsum Byproduct............................................................241Table 15.2.5 Calcining .................................................................................................242Table 15.2.6 Pigment Finishing ...................................................................................242Table 16.2.1 Crushing and milling................................................................................247Table 16.2.2 Magnetic separation and de-watering .....................................................248Table 16.2.3 Roasting..................................................................................................248Table 16.2.4 Leaching .................................................................................................249Table 16.2.5 Precipitation and V2O5 production ...........................................................250Table 17.2.1 Crushing, screening and magnetic separation ........................................255Table 17.2.2 Pre-reduction ..........................................................................................256Table 17.2.3 Electric arc smelting................................................................................256Table 17.2.4 Shaking ladles.........................................................................................257Table 18.2.1 Roasting..................................................................................................263Table 18.2.2 Leaching and precipitation ......................................................................264Table 18.2.3 Purification ..............................................................................................265Table 18.2.4 Electrowinning.........................................................................................266Table 18.2.5 Effluent treatment ...................................................................................266


Glossary of abbreviations, symbols and terms
AbbreviationsAmerican Conference of Governmental Industrial Hygienists ACGIHAtomic absorption spectrometry AAAtomic absorption spectrometry, flame AA-FAtomic absorption spectrometry, graphite furnace AA-GFAtomic emission spectrometry AESBiological exposure index BEIBiological limit value BLVChronic beryllium disease CBDElectro-cardiography ECGGravimetric analysis GRInductively coupled plasma ICPInternational Agency for Research on Cancer IARCNational Institute for Occupational Safety and Health NIOSHOccupational exposure limit - control limit OEL-CLOccupational exposure limit - recommended limit OEL-RLOccupational exposure limit - time-weighted average OEL-TWAOccupational Safety and Health Administration OSHAPolarography POLThreshold limit value TLVUS Environmental Protection Agency USEPAX-ray diffraction X DIF
SymbolsExposure concentration CiHazard index HIHazard quotient HQiOriginal equal risk group size. NSample size or subgroup size. nUnit risk factor URFn
TerminologyAir spargeA technique used to add air in a distillation process.
AstheniaWant of strength.
AtherosclerosisA form of arterio-sclerosis, in which there is fatty degeneration of the middle coat of the arterialwall.
AutoimmunityA reaction to an individual’s own tissues (self-antigens) to which tolerance has been lost.
BioaccumulationThe retention and concentration of a chemical by an organism. It is a build-up of a chemical ina living organism, which occurs when the organism takes in more of the chemical than it can riditself of in the same length of time and stores the chemical in its tissue, etc.

BioavailabilityThe proportion of a substance reaching the systemic circulation after a particular route ofexposure.
CardiomyopathyDisease of the heart muscle of unknown cause.
CentrilobularTerm used to indicate the central part of soft tissues, for example in the hepatic system.
CompartmentalisationSeparation into different compartments, for example different organs or tissue, orenvironmental systems.
CortexThe outer layer of an organ or other body structure, as distinguished from the internalsubstance.
Cortical cellsCells pertaining to or of the nature of a cortex.
CyanosisA bluish discoloration, especially of the skin and mucous membranes due to excessiveconcentration of deoxyhemoglobin in the blood.
DartosAlso called musculus dartos or dartos muscle, the subcutaneous tissue underlying the skin ofthe scrotum.
EnterohepaticReabsorption instead of excretion by the liver cells into the small intestine.
EuchromatinThe condensed form of chromatin in which it stains lightly, is genetically active, and is partiallyof fully uncoiled, being the interphase form of the chromosome or the material of mostchromosome arms during metaphase.
FumeAerosol of solid particles resulting from condensation of the vapour given off from the heating ofmetals.
GlomerulusA cluster composed of blood vessels or nerve fibres.
GlycoproteinsA conjugated protein containing one or more covalently linked carbohydrate residues.
GranulomaAn imprecise term applied to an aggregation of inflammatory cells, initiated by variousinfectious or noninfectious agents.
HaematopoieticReferring to the blood system.

HaemosiderinAn intracellular storage form of iron, found in the form of pigmented yellow to brown granulesconsisting of a complex of ferric hydroxides, polysaccharides, and proteins.
Hazard index (HI)The sum of several hazard quotients for multiple substances and/or multiple exposure.pathways.
Hazard quotient (HQ)The ratio of a single substance exposure level for a specified time period to a reference dose ofthat substance derived from a similar exposure period.
Heavy metalsMembers of a group of metallic elements which are recognized as toxic and generallybioaccumulative. The term arises from the relatively high atomic weights of these elements.
HepatotoxicToxic to the liver.
HomeostaticallyControlled by the level in the human body.
IdiotopeAn antigenic determinant on a variable domain of an immunoglobulin molecule.
IdiotypeA set of one or more idiotopes that distinguish a clone of immunoglobin-producing cells fromother clones.
ImmunoglobulinsAny of the structurally related glycoproteins that function as antibodies.
ImmunoregulatoryControl of the immune response by mechanisms such as suppressor and contrasuppressorlymphocyte circuits and the immunoglobulin idiotype-anti-idiotype network.
ImmunosuppressionThe suppression of harmful immune responses.
IschaemiaDeficiency of blood in a part, usually due to functional constriction or actual obstruction of ablood vessel.
LacrimationProduction of tears.
LanguorFaintness, fatique.
LymphocytesA variety of white blood corpuscle produced in the lymphoid tissues and lymphatic glands of thehuman body.
LymphocytosisAn increase in the number of lymphocytes in the blood.

MedullaGeneral term for the most inner portion of an organ or structure.
Metabolic activationActivated by the physical and chemical processes by which the body is maintained, and thoseby which energy is made available for various forms of work.
MetaphaseThe second stage of cell division during which the contracted chromosomes are arranged in theequatorial plane of the spindle prior to separation.
MidzonalTerm used to indicate the intermediate part of soft tissues, for example in the hepatic system.
MistFinely divided liquid droplets suspended in air, formed by bubbling, boiling, foaming, spraying,splashing or otherwise agitating a liquid that contains heavy metals.
MutagenicThe property of a substance to increase the rate of mutation among cells.
NeoplasiaThe formation of a neoplasm.
NeoplasmAny new and abnormal growth, specifically a new growth of tissue in which the growth isuncontrolled and progressive.
NephrotoxicToxic or destructive to kidney cells.
NephrotoxinA toxin which has a specific destructive effect on kidney cells.
NeuroendocrinePertaining to interactions between the nervous and endocrine systems and to hormones suchas vasopressin and gastrin that are elaborated in the neurons and neuron-like cells.
NeuronsAny of the conducting cells of the nervous system.
NeurotoxicToxic or destructive to cells of the neurosystem.
OocyteA developing egg cell.
OogenesisThe process of formation of female egg cells.
OsteodystrophyDefective bone formation.
OVM badgesPassive samplers to measure exposure to hazardous chemicals, under the label OVM.

PeriportalSituated around the portal vein
PortalPertaining to a porta, or entrance, especially to the portal hepatis (liver).
RadiographicallyUsing radiology, X-rays.
Reference concentration (RfC)A concentration of a chemical substance in an environmental medium to which exposure canoccur over a prolonged period without an expected adverse effect. The medium in this case isusually air, with the concentration expressed in mg of chemical per m3 of air.
Reference dose (RfD)The maximum amount of a chemical that the human body can absorb without experiencingchronic health effects, expressed in mg of chemical per kg body weight per day. It is theestimate of lifetime daily exposure of a noncarcinogenic substance for the general humanpopulation (including sensitive receptors) which appears to be without an appreciable risk ofdeleterious effects, consistent with the threshold concept.
ResponseThe reaction of a body or organ to a chemical substance or other physical, chemical, orbiological agent.
Reticulo-endothelial systemHighly specialised cells scattered throughout the body, but mostly in the spleen, bone marrow,liver, and lymph glands. Their main function is the ingestion of red blood cells and theconversion of haemoglobin to bilirubin.
RhinitisInflammation of the mucous membrane of the nose.
SeminiferousProducing or conveying semen.
SensitisersTerm used for substances that cause a higher-than-normal response when repeatedly exposedto.
Sertoli cellsElongated cells in the seminiferous tubules to which the spermatids become attached.
SpeciationThe chemical form in which a substance exists, relating to its oxidation state.
SpermatogoniaPlural of spermatogonium.
SpermatogoniumAn undifferentiated germ cell of a male.
TeratogenesisThe production of birth defects in embryos and fetuses.

ThresholdThe lowest dose or exposure of a chemical at which a specified measurable effect is observedand below which such effect is not observed. Threshold dose is the minimum exposure dose ofa chemical that will evoke a stipulated toxicological response. Toxicological threshold refers tothe concentration at which a compound exhibits toxic effects.
Threshold limitThe concentration of a chemical above which adverse health and/or environmental effects mayoccur.
ToxicHarmful, or deleterious with respect to the effects produced by exposure to a chemicalsubstance.
ToxicantAny synthetic or natural chemical with an ability to produce adverse health effects. It is apoisonous contaminant that may injure an exposed organism.
ToxicityThe harmful effects produced by a chemical substance. It is the quality or degree of beingpoisonous or harmful to human or ecological receptors. It represents the property of asubstance to cause any adverse physiological effects (on living organisms).
Toxicity assessmentEvaluation of the toxicity of a chemical based on all available human and animal data. It is thecharacterization of the toxicological properties and effects of a chemical substance, with specialemphasis on the establishment of dose-response characteristics.
Toxic substanceAny material or mixture that is capable of causing an unreasonable threat to human health orthe environment.
TransductionThe transforming of one form of energy to another, such as by sensory mechanisms of thebody.
Transient histological changesEpisodes of changes in the minute structure of tissues, followed by complete recovery.
Tunica albugineaA dense, white fibrous sheath, enclosing a part or organ.
VapourThe gaseous form of a substance that is normally in the liquid or solid state at roomtemperature and pressure.
VascularisedTo supply with vessels.
XenobioticsA chemical foreign to the biologic system.

23
1 IntroductionThe toxicology and therapeutic properties of metals have been subjects of interest for centuries.For example, mercury has been used for medicinal purposes since early civilisations, yetmercury is also one of the most toxic substances known to man. Manganese is an essentialelement that has been shown to be important for growth and reproduction in animals andhumans. However, manganese is also neurotoxic, and sustained occupational exposuresabove certain levels have been shown to lead to a condition known as manganism, withsymptoms that resemble Parkinson's disease. Lead is also neurotoxic, but the manifestation ofeffects is not the same as for manganese. The uptake of manganese in the human body isinfluenced by the body burden of iron, and there are differences between the health effectsassociated with inhalation and ingestion. Several human hereditory diseases have been relatedto imbalances in metal metabolism. Hexavalent chromium compounds are believed to becarcinogenic, but no evidence exists that has linked trivalent chromium compounds to cancer. Many other examples exist to illustrate the complexity of metal toxicology. The toxic outcomesof exposure to metals cover virtually every adverse effect from the cellular to the whole bodylevel. Effects vary from sensory irritation to disabling systemic disease, including cancer ofvirtually every organ of the body. As one of the oldest areas of study, metal toxicology is alsoone of the most rapidly developing disciplines.
Epidemiological studies of occupational exposure to metals over many years have formed thebasis for setting exposure guidelines for the protection of employees, and also to developtolerable exposure levels for the public at environmental levels. In the absence of human data,animal studies form the basis for toxicological assessment. A whole new discipline has evolvedin health risk management over the past three decades, involving many branches of science.
Generally, occupational hygiene measurements to quantify exposure to metals are interpretedin a relatively simplistic manner. What is referred to as a "health risk assessment" inoccupational hygiene terms is often better described as a hazard assessment, because theactual risk is not quantified. Air concentrations of toxic substances are compared to someguideline concentrations that represent a "safe" dose concept. The ratio of the airconcentration of an occupational toxicant to its guideline or threshold concentration isexpressed as a hazard quotient. If the hazard quotient for a particular substance exceeds one,the exposure may lead to an unacceptable health risk and requires further investigation. In thecase of multiple chemical exposure, hazard quotients are added to get an overall hazard index,which also should not exceed one. Various agencies in the world use different terminology, butall these guideline values are based on the same philosophy. The underlying assumption isthat nearly all employees may be repeatedly exposed to concentrations up to the thresholdlevels without developing health effects. Because of the wide variation in susceptibility ofpeople to environmental toxicants, it may however be possible that a small percentage of theindividuals could experience some discomfort or aggravation of a pre-existing condition, or maydevelop an occupational illness in exceptional cases.
1.1 Research problem statementThe presence of heavy metals and exposure of employees thereto in mineral processing plantsin South Africa have not been studied and described in a format that can be used as a generalreference document. The intention has been to provide a concise review of different processsteps in mineral processing and the associated health hazard for those who are new in the field,and for the relatively uninformed who have to perform duties that require some understandingof the processes and background to health risk assessment. In providing these perspectives,the following aspects were considered to be of primary importance:
• To provide an understanding of the paradigm of human health risk assessment in theoccupational environment;
• To identify heavy metals that would be of interest in mineral processing plants;

24
• To review the context of target-organ toxicity of heavy metals in the quantification ofexposure and health risks, taking into account the concepts of speciation and bioavailability;
• To provide information on the elements of occupational health risk management, providinggeneral principles for survey design, sampling philosophies, and interpretation methods.
• To put the principles listed above in context with selected mineral processing plants inSouth Africa.
1.2 Objectives and aims of this study
1.2.1 Main objectiveThe main objective of the studies was to acquire and document all the background informationthat is necessary for an understanding of health risks associated with heavy metals in variousmineral-processing plants. This involves descriptions of unit processing steps and operationalparameters, identification of sources of chemical hazards, descriptions of toxicology, guidelinesfor sampling and chemical analysis for exposure assessment, and a framework for health riskmanagement. This information should assist persons who are not specialists in the field inrecognising health hazards relating to heavy metals, and should facilitate the review,implementation and management of appropriate monitoring and medical health surveillanceprogrammes.
1.2.2 GoalsProcess descriptions and exposure assessmentProcess flow sheets were developed to show the unit operations, materials, identified heavymetals, and potential exposure locations in the mineral processing plants.
Toxicological reviewsAll the metals of interest were reviewed for their toxic effects on target organs, to put exposuresand health risks into context.
Guidelines for health risk managementGuidelines for health risk management included consideration of regulatory requirements, aswell as criteria for monitoring and medical surveillance.
1.3 Research context and design
1.3.1 Research contextThe study was not intended to provide a manual with step-by-step guidance that could be usedfor health risk management in the various industries. Specialists in health risk management inthe industries have many such reference documents to assist in the implementation and controlof occupational health risk management programmes. It was the intention to develop adocument that would be useful for persons who are not familiar with all the industries, but havefunctions or an interest relating to occupational health across several of the industries. Thedocument may also be useful for persons who are specialists in some of the mineral processingplants, but wish to get an idea of the health risk status in other facilities. Whilst the research incertain respects has been generic, it provided specialist information on metal toxicology andtarget organ effects, which are not always considered in detail in the interpretation ofoccupational hygiene information. In this respect, it may assist in adding some scientific depthto health risk interpretations.

25
1.3.2 Research designThere is no universal definition of heavy metals. It appears that the concept of "heavy metals"did not have its origin only in molecular weight classification, but more in the fact that the metalsthat are relatively more toxic to humans and animals also have relatively high molecularweights. The first step in the current investigation was to select those metals that could beplaced in the category of "heavy metals". A list was compiled on the basis of toxicologicalproperties of the elements, and comprises 33 elements. The elements were chosen with theobjective of health risk management in mind, rather than on the basis of the classical definitionof "metals". For example, antimony and arsenic are classified as semi-metals, and selenium isnot a metal, but it does have some suggestion of metallic behaviour. These elements arehowever of toxic concern and were included in the overall assessment of human exposure.
In order to understand target organ effects of heavy metals, the studies included a review of thetarget organ systems of the body, and how these systems are affected by exposure to heavymetals. The toxicology of the metals and metal compounds is covered in a subsequent section. This information was used to identify health hazards in mineral processing plants.
To assess the potential for exposure to heavy metals, the various industries must be wellunderstood. This study therefore reviewed fifteen selected industrial processes to identify unitoperations, potential toxicants, and exposure zones where hazards may be posed. Theinformation is presented in generic flow diagrams. The diagrams were developed to representthe general process steps, rather than detailed descriptions that were not essential forunderstanding the basic concepts and associated hazards.
The following types of mineral processing plants were studied:
• Carbon steel process with blast furnace and basic oxygen furnace;• Carbon steel process with direct reduced iron and electric arc furnace;• Typical copper recovery circuit;• Typical ferrochromium production process;• Typical ferromanganese production process;• Bacterial oxidation circuit for the pre-oxidation of refractory gold ores;• Carbon-in-pulp circuit for gold recovery;• Nickel, copper, and cobalt refining process;• Typical phosphate rock production process;• Platinum group metal refining;• Typical stainless steel process;• Typical titanium dioxide production process;• Vanadium pentoxide production: the salt-roast process;• Vanadium slag production process; and• Typical circuit for zinc recovery from concentrate.
1.4 Deployment of the studyThe project focussed on the characterisation of occupational exposure to heavy metals in 15types of mineral processing plants. Many of the substances of interest occur in more than oneprocess, and similar health effects may be observed in the various plants. To avoid duplicationin the assessment of the 15 production plants, the rationale for selection of the 33 elements ofinterest and general toxicological aspects are presented together in one section. Exposureassessment, which covers monitoring and certain aspects of health risk management, is alsocommon to the various processes, and is therefore, presented in one section. These sectionswere grouped into the literature review section, according to the logical steps of health riskassessment, i.e. hazard assessment, dose-response (toxicological) assessment, and exposureassessment. The basis for health risk characterisation is also presented in this section. The 15

26
processing plants are discussed separately in subsequent sections. Literature references aregiven in the sections pertinent to the information.
Section 1: Introduction and background.Section 2: Research methodologySection 3: Literature review.Sections 4 to 18: Discussion of the mineral processing plants.
27
2 Research methodologyThe overall paradigm of health risk assessment was followed in the investigations, i.e.according to the steps of hazard assessment, dose-response assessment, exposureassessment, and risk characterisation.
As a first step, the 15 selected mineral processing plants were described in generic format,using documented information on the processes, materials, and products. Engineers who werefamiliar with the processes compiled process flow diagrams. The diagrams show processsteps, reagents, process conditions, discharge streams, hazard identification, and positionswhere it would be appropriate to quantify human exposure. More information is presented inprocess descriptions. The process information was verified through visits to typical plants anddiscussions with specialists in the various fields. This work covers the hazard assessmentpart of the investigation.
The dose-response assessment (toxicological assessment) was based on literatureinformation reviewed for the various metals. An extensive literature review was conducted,covering searches of the most prominent international publications on the subject. The largevolume of data is summarised in tables. To place the information in context, concisedescriptions of the target organs of the body that are relevant to metal toxicity are alsopresented. Because several of the metals are present in more than one processing plant,toxicological information is presented together in one section of the report. The most relevantinformation is however highlighted in the sections that deal separately with each plant.
The exposure assessment part of the studies was also handled in the descriptions of the 15selected mineral processing plants. The approach did however not follow the conventionaloccupational hygiene process of sampling and chemical analysis. It was limited to theidentification of zones of exposure, and recommendations for monitoring. Because theprotocols for occupational exposure monitoring are more related to the substances of interestthan the particular processing plants, the methodologies for monitoring have been presentedtogether in one section in the report. Reference has however been made to appropriatemonitoring in the sections that deal separately with each plant.
Risk characterisation was limited to descriptions of the paradigm for quantitative humanhealth risk assessment.

28

29
3 Literature review
3.1 Principles of health risk assessmentThe term risk assessment in general describes the process of data interpretation in order toassess the potential consequences of risks from human activities and natural events. In theoccupational and environmental protection context, risk assessment examines the potentialenvironmental and human health consequences related to the release of chemicals to theenvironment. It is an interdisciplinary process that encompasses such diverse fields asenvironmental chemistry, statistics, toxicology, air physics and chemistry, analytical technologyand engineering.
There are three basic concepts that are important in understanding the risk assessmentprocess:
Risk can be defined as the probability that a given hazard will cause harm of a specific natureto a human population or an ecosystem.A hazard is a source of risk and refers to the inherent capacity of heavy metals to cause harm.Exposure is defined as the amount of chemical or physical agent available for adsorption orinteraction at the exchange boundaries of the organism at risk.
As outlined above, environmental and occupational health risk assessments include the stepsof hazard identification, dose-response assessment, exposure assessment, and health riskcharacterisation. These are followed by a statement of risk options for decision-making on thebasis of financial, political or other relevant factors. Risk assessment provides the input datafor the implementation of a risk management programme.
3.2 Hazard assessmentThe project terms of reference did not specify a particular list of hazardous heavy metals forinvestigation. It was therefore necessary to develop a list of metals of interest to use as aguideline in the review of potential health hazards in the selected mineral processing plants. The rationale for selection of metals for assessment is presented below.
3.2.1 Criteria for selection
3.2.1.1 The classification of heavy metalsHeavy metals are defined as:Members of a group of metallic elements which are recognised as toxic and generallybioaccumulative. The term arises from the relatively high atomic weights of these elements. [Asante-Duah, 1996]. Elements in Period 4 onwards in the Periodic Table are considered in thecategory “heavy”. Beryllium is not a heavy element, but was nevertheless included because ofits carcinogenicity. Potassium is not relevant, because it is not toxic. Any toxicity of the salts ofpotassium is due to the anion thereof, for example where it is associated with cyanide. Cyanideis of prominent interest in certain mineral processing plants, but as a result of its associationwith many metals, also those that are not classifiable as heavy metals, it was not included inthis investigation. The occurrence and health consequences of cyanides should be consideredin a separate study, not only in the context of exposure to heavy metals.
Calcium compounds should be considered toxic only when they contain toxic compounds (suchas arsenic), or as calcium oxide or hydroxide. For completeness, however, calcium is includedfor possible exposures to calcium oxide or hydroxide. The other elements to consider are fromSc and the higher molecular weights under Transition Elements, and Group III onwards.
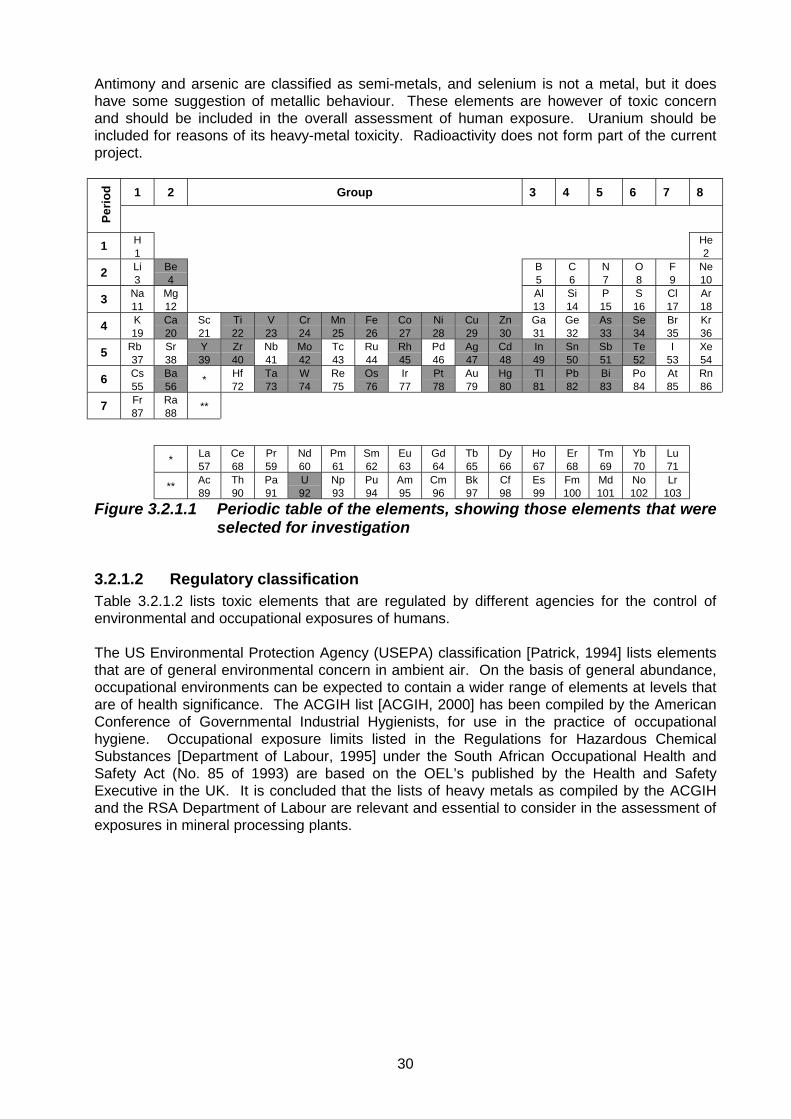
30
Antimony and arsenic are classified as semi-metals, and selenium is not a metal, but it doeshave some suggestion of metallic behaviour. These elements are however of toxic concernand should be included in the overall assessment of human exposure. Uranium should beincluded for reasons of its heavy-metal toxicity. Radioactivity does not form part of the currentproject.
1 2 Group 3 4 5 6 7 8
Perio
d
1 H1
He2
2 Li3
Be4
B5
C6
N7
O8
F9
Ne10
3 Na11
Mg12
Al13
Si14
P15
S16
Cl17
Ar18
4 K19
Ca20
Sc21
Ti22
V23
Cr24
Mn25
Fe26
Co27
Ni28
Cu29
Zn30
Ga31
Ge32
As33
Se34
Br35
Kr36
5 Rb37
Sr38
Y39
Zr40
Nb41
Mo42
Tc43
Ru44
Rh45
Pd46
Ag47
Cd48
In49
Sn50
Sb51
Te52
I53
Xe54
6 Cs55
Ba56 * Hf
72Ta73
W74
Re75
Os76
Ir77
Pt78
Au79
Hg80
Tl81
Pb82
Bi83
Po84
At85
Rn86
7 Fr87
Ra88 **
* La57
Ce68
Pr59
Nd60
Pm61
Sm62
Eu63
Gd64
Tb65
Dy66
Ho67
Er68
Tm69
Yb70
Lu71
** Ac89
Th90
Pa91
U92
Np93
Pu94
Am95
Cm96
Bk97
Cf98
Es99
Fm100
Md101
No102
Lr103
Figure 3.2.1.1 Periodic table of the elements, showing those elements that wereselected for investigation
3.2.1.2 Regulatory classificationTable 3.2.1.2 lists toxic elements that are regulated by different agencies for the control ofenvironmental and occupational exposures of humans.
The US Environmental Protection Agency (USEPA) classification [Patrick, 1994] lists elementsthat are of general environmental concern in ambient air. On the basis of general abundance,occupational environments can be expected to contain a wider range of elements at levels thatare of health significance. The ACGIH list [ACGIH, 2000] has been compiled by the AmericanConference of Governmental Industrial Hygienists, for use in the practice of occupationalhygiene. Occupational exposure limits listed in the Regulations for Hazardous ChemicalSubstances [Department of Labour, 1995] under the South African Occupational Health andSafety Act (No. 85 of 1993) are based on the OEL’s published by the Health and SafetyExecutive in the UK. It is concluded that the lists of heavy metals as compiled by the ACGIHand the RSA Department of Labour are relevant and essential to consider in the assessment ofexposures in mineral processing plants.

31
Table 3.2.1.2List of elements selected for assessment
USEPA hazardous airpollutants (HAPs)
List of metals assigned TLV’sby the ACGIH
List metals assigned OEL’saccording to South African
regulationsAntimonyArsenic
Beryllium
Cadmium
ChromiumCobalt
LeadManganeseMercury
Nickel
Selenium
AntimonyArsenicBariumBerylliumBismuthCadmiumCalciumChromiumCobaltCopperIndiumIronLeadManganeseMercuryMolybdenumNickelOsmiumPlatinumRhodiumSeleniumSilverTantalumTelluriumThalliumTinTitaniumTungstenUraniumVanadiumYttriumZincZirconium
AntimonyArsenicBariumBerylliumBismuthCadmiumCalciumChromiumCobaltCopperIndiumIronLeadManganeseMercuryMolybdenumNickelOsmiumPlatinumRhodiumSeleniumSilverTantalumTelluriumThalliumTinTitaniumTungstenUraniumVanadiumYttriumZincZirconium
3.2.2 Use of the list of hazardous metalsIt can be expected that different elements will be relevant in the various processes, and someof the elements listed in the table may not be present in significant concentrations in any of themineral processing plants. Furthermore, some of the elements may not be in a chemical formthat would be toxic. It is not inferred that sampling and chemical analyses would include all theelements in the table. Nevertheless, the entire list of elements in the table above had to beconsidered in the description and assessment of each mineral processing plant, and the overallhazard identification.
3.3 Dose-response assessment
3.3.1 Basic concepts in toxicologyDose-response assessment is based on the toxicological response to a dose in target tissuesto predict, for example, the non-cancer health risks resulting from human inhalation of an airpollutant, or the level of exposure associated with a one-in-a-million risk of cancer. Riskestimation in the low-dose region where human exposures normally occur, often depends on

32
extrapolation of dose-response information from studies using high-dose exposures inlaboratory animals.
Acute toxicity refers to the development of symptoms of poisoning or the occurrence of adversehealth effects after exposure to a single dose or multiple doses of a chemical within a short periodof time. Sensory irritation may be considered in short-term exposures, because it isconcentration-dependent rather than time-dependent.
Chronic toxicity refers to the occurrence of symptoms, diseases, or other adverse health effectsthat develop and persist over time, as a result of exposure to a single dose or multiple doses of achemical over a relatively long period of time (months to years).
Carcinogenicity describes the ability of a chemical to cause cancer in a living organism. Theclassification of carcinogens according to the International Agency for Research on Cancer(IARC) was used in this report. This is presented in Table 3.3.1.
Table 3.3.1The IARC classification for carcinogenicity
Group 1Human carcinogenSufficient evidence of carcinogenicity in humans.Group 2AProbable human carcinogenLimited human data and sufficient animal data.Only limited human data, or only sufficient animal data in the presence of other supporting data.Group 2BPossible human carcinogenLimited human data in the absence of sufficient evidence in animals.Sufficient animal data with inadequate or no human data.Limited animal data with other supporting data, and inadequate or no data in humans.Group 3Not classifiableData do not fit into any of the above groups.Group 4Probably not a human carcinogenEvidence suggests lack of carcinogenicity in humans and animals.
Developmental toxicity refers to adverse effects on the developing organism that may resultfrom exposure prior to conception (either parent), during prenatal development, or postnatal to thetime of sexual maturation. Adverse developmental effects may be detected at any point in the lifespan of the organism.
Sensitisation is the result of exposure to substances that have the ability to sensitise theorganism to subsequent exposures. This leads to severe responses at exposure concentrationsthat are normally below the threshold for manifestation of the typical effects.
Bioavailability is a term generally used to describe the extent and rate of absorption for a toxicsubstance that enters the systemic circulation in the unaltered form from the exposure site. Theconcept is more complex, however, because a substance may not be bioavailable in its parentform, but after metabolism may be converted into a form that can enter the systemic circulation.

33
Reproductive toxicity is divided into male and female reproductive toxicity. Male reproductivetoxicity is defined as the occurrence of adverse effects on the male reproductive system thatmay result from exposure to toxic substances. It may be expressed as alterations to the malereproductive organs and/or the related endocrine system, manifested as alteration in sexualbehaviour, fertility, pregnancy outcomes or modifications in other functions that are dependenton the integrity of the male reproductive system. Female reproductive toxicity refers to adverseeffects observed in the female reproductive system that may result from exposure to toxicsubstances. It includes, but is not limited to, adverse effects in sexual behaviour, onset ofpuberty, fertility, gestation, parturition, lactation or premature reproductive senescence.
3.3.2 Mechanisms of metals toxicityThe primary routes of exposure to toxicants in the occupational environment are via inhalation,ingestion, and dermal contact. Most metallic compounds occur as solids, fumes or in mists, andare frequently associated with particulates in the occupational exposure scenario. Particle sizedetermines where in the respiratory tract inhaled particles are deposited and hence can exert theirtoxic effects. Only a few metals and metal compounds are liquids at room temperature andpressure, e.g. mercury (Hg), nickel tetracarbonyl [Ni(CO)4], and arsenic trichloride (AsCl3). Liquids are in equilibrium with vapours above them, characterised by the vapour pressure of theliquid phase. If not contained, liquid metals and compounds release vapours to which employeesmay be exposed. A limited number of metal compounds exist as gases at room temperature andpressure, e.g. arsine (AsH3) and stibine (SbH3). Metals seldom interface with biological systemsin the elemental form. They occur as compounds that vary in the ease with which they can passthrough biological membranes.
Metabolism of metals refers to all the processes by which the body handles metals. Absorption,distribution, biochemical modification, storage, and excretion are the most important processesin the metabolism of metals.
Absorption refers to the process where xenobiotics cross body boundaries and reach thesystemic circulation.
Distribution is the process whereby the absorbed xenobiotics are transported by the bloodcirculation system to various organs and tissues.
Biochemical modification includes processes in the human body where chemical properties ofsubstances are modified, such as changes in oxidation state and complex and radical formation.
Storage of toxicants refers to the deposition and retention of toxicants in different organs of thebody.
Excretion is the process whereby xenobiotics are eliminated from the body through such routesas urine, faeces and the lungs.
Organ-specific toxicity reflects the principle of compartmentalisation. The target organ receivingthe exposure is highly susceptible to injury. Both uptake and toxicity may be linked to uniquemetabolic processes. For example, cadmium is known to accumulate in the kidneys as a result ofits association with the cadmium-scavenging protein metallothionin. On the other hand, lead isdistributed as a systemic toxicant throughout the entire body before being deposited in the bone. There is often little correlation between the reaction of a target organ to the toxic effects of a metaland the concentration of the metal in that tissue. For example, 90 per cent of the lead in thehuman body is found in the skeleton, but its toxic effects are manifested primarily in the nervoussystem, renal system, and haematopoietic system. It is not possible to generalise principles thatgovern the mechanisms of action of toxic metals. A variety of biological effects are produced indifferent organ systems, and in no case can the multiple manifestations of toxicity be assigned to
34
a single biochemical process. The mechanisms of metals toxicity can be classified into thefollowing categories:
Enzyme inhibitionToxic metals normally have a high affinity for amino-acid side chains such as sulphydryl, histidyl,or carboxyl groups, and can react directly with proteins to alter enzymatic or structural function.
Indirect effectsMetals may bind to cofactors, vitamins, and substrates, thereby altering the availability of theseessential cell constituents for biological function.
Substitution for essential metalsSeveral metals are essential to the human body, playing a role in protein structure, enzymecatalysis, osmotic balance, and transport processes. Toxic metals that are chemically andphysically similar to some of the essential metals may replace the essential metals, therebyexerting toxic effects through alteration of biological processes.
Table 2.3.2 shows an overview of target-organ toxicity of metals and metalloids.
Metal imbalanceExcessive exposure to a particular metal may lead to depletion or repletion of an essentialmetal in biological systems. For example, large exposures to zinc may lead to copperdeficiency. On the other hand, sufficient zinc prevents cadmium intoxication that is manifestedas necrosis in the intestine. Lead alters tissue levels of many essential elements, includingiron, zinc, copper, and calcium.

35
Table 2.3.2Overview of target-organ toxicity of metals and metalloids
TARGET ORGAN SYSTEM
SUBSTANCER
enal
sys
tem
Ner
vous
sys
tem
Live
r
Gas
troin
test
inal
trac
t
Res
pira
tory
sys
tem
Hae
mat
opoi
etic
syst
em
Bone
Endo
crin
e sy
stem
Mus
cle
syst
em
Eye
Skin
Car
diov
ascu
lar
syst
em
Imm
une
syst
em
Rep
rodu
ctiv
esy
stem
Antimony • • • • •Arsenic • • • • • • • • • • •Barium • • •Beryllium • • •Bismuth • • •Cadmium • • • • • • • • •Calcium • • •Chromium • • •Cobalt • • • •Copper • • •Indium • • • •Iron • • • • • •Lead • • • • • • • • •Manganese • • •Mercury • • • • • • • •Molybdenum • •Nickel • • • •Osmium • • •Platinum • • • • •Rhodium • • • •Selenium • • • • • • • •Silver • • • • •Tantalum • • •Tellurium • • • •Thallium • • • • • • • • •Tin • • • • •Titanium • • •Tungsten • • •Uranium • • • •Vanadium • • • •Yttrium • • • •Zinc • •Zirconium • • • •

36
3.3.3 Target organ systems and toxic responsesAfter a toxic substance has entered the human body, it is distributed to target sites of action,i.e. sites of metabolic change and excretion. This section provides short descriptions of organsystems that respond to the toxicological impacts of occupational pollutants.
3.3.3.1 Renal systemThe kidney is a very efficient filter organ and plays a crucial role in the elimination of toxicantsfrom the body. Anatomically the kidney is a complex arrangement of vascular endothelial cellsand tubular epithelial cells, the blood vessels and tubules being intertwined.
Excretion into the urine involves one of the following three mechanisms:
• Filtration from the blood through the pores in the glomerulus.• Diffusion from the blood stream into the tubules.• Active transport into the tubular fluid.
The kidney is a target organ for metals toxicity for the following reasons:
• The kidney receives 25 per cent of the blood of the cardiac output. Therefore, the exposureof kidney tissue to foreign compounds in the bloodstream, especially the cortex thatreceives more blood than the medulla, is relatively high.
• One of the functions of the kidney is its concentrating ability. After glomerular filtration,many substances are re-absorbed from the tubular fluid. Hence, the concentration offoreign substances in the tubular lumen is considerably higher than that in the blood. Thetubular-to-blood ratio may reach values of 500:1.
• Compounds that are actively transported from the blood into the tubular fluid oftenaccumulate in the proximal tubular cells, even more so where saturation of the transportsystem occurs. This again leads to much higher concentrations than in the blood stream, towhich tubular cells are exposed.
• Although to a lesser degree than the liver, the kidney has sufficient activity to be responsiblefor metabolic activation.
• Exposure to most heavy metals results in renal toxicity. Lead, mercury, platinum, cadmiumand chromium are amongst the most prominent nephrotoxins.
3.3.3.2 Nervous systemThe nervous system consists of cells and fibre, each of which is an extension of the nerve cell. The brain and spinal cord is known as the central nervous system and nerves proceeding fromthem are named cerebrospinal or peripheral nerves. The third division, situated in the neck,thorax and abdomen is known as the autonomic nervous system.
The central nervous system is protected from toxicants by the blood-brain-barrier. This barrieris a functional concept based on the observation that some substances that enter and affectother soft tissue such as the liver and kidney are excluded from the brain. Not all substancesare preferentially excluded from the brain and non-polar, lipid-soluble compounds usuallypenetrate the blood-brain-barrier. The nervous system, both peripheral and central, is acommon target for toxic substances for the following reasons:
• The cells making up the nervous system are particularly susceptible to changes in theenvironment such as pH changes.
• The distribution of blood capillaries in the brain is not uniform, in as much that white matteris less vascularised than grey matter, resulting in a higher sensitivity to foreign compoundsin the grey matter.

37
• It has been proposed that excitatory amino acids may damage hypothalamic neurons byexcessive stimulation and thus metabolic exhaustion of the cells.
• Quantitative differences in essential cell components may make one cell type moresensitive to toxicants than other cells. For example, small neurons are preferentially killedwhen the whole brain is exposed to methyl mercury.
• Certain large cells such as the cortical and hippocampal pyramidal cells and others haveunusually large nuclei and the DNA is largely present as euchromatin. These cells oftenhave several nucleoli. All these structural differences point to high metabolic activity inthese cells and thus increased susceptibility to anoxic damage.
Mercury, lead and manganese are among the most prominent neurotoxic substances.
3.3.3.3 LiverThe liver is the largest visceral organ and is exposed to many potentially toxic substances viathe gastrointestinal tract. The structural and functional unit in the liver is the lobule. In thecentre of this lobule is the terminal hepatic venule and at the periphery the portal space,containing a branch of the portal vein, an hepatic arteriole and a bile duct. Based on thisconfiguration, pathologic lesions of the hepatic parenchyma have been classified ascentrilobular, midzonal or periportal. The simple acinus concept has been developed toindicate the three circulatory zones within each acinus. Zone one first receives blood from theafferent venules and arterides, followed by zone two, and finally zone three. Hence there willbe metabolic differences between the zones, because of the blood flow. The concentration ofoxygen and nutrients will decrease as blood flows from zone one to zone three, which leaveszone three more sensitive to damage from toxic compounds.
The liver is a target organ for toxic substances for the following main reasons:
• The large and diverse metabolic capabilities of the liver enable it to metabolise many foreigncompounds, but as metabolism does not always result in detoxification, this may make it atarget.
• Because of the extensive role that the liver plays in intermediary metabolism and synthesis,it consequently interferes with endogenous metabolic pathways, which may lead to toxiceffects.
• Bile secretion by the liver may also be a factor. Biliary excretion of foreign compounds maylead to high concentrations, especially if saturation occurs, as has been experienced withthe hepatotoxic drug “furosemide”. Alternatively, enterophepatic circulation can give rise toprolonged high concentrations in the liver. Any interference to the bile production or bileflow may lead to damage to the biliary system and surrounding hepatocytes.
• The relatively high blood supply ensures that the liver is exposed to high concentrations oftoxic substances absorbed from the gastrointestinal tract.
3.3.3.4 Gastrointestinal tractThe gastrointestinal tract starts at the mouth and leads to the stomach, which is linked to themouth via the oesophagus. The far end of the stomach ends in the pylorus, a thickcircumferential muscular sphincter that separates the stomach from the duodenum. Theduodenum links the stomach to the ileum, also known as the small intestine, and has thelargest surface area of the gastrointestinal tract, 6,5-m long and 35-mm in width. The ileummouths into the large intestine or colon, which is 1,8-m long and 65-mm in width. The last partof the colon is known as the rectum, which passes straight down through the back of the pelvisto open to the exterior through the anus.
The gastrointestinal tract is the first organ exposed to ingested foreign substances. Consequently, local concentrations at the contact tissue may often be many times higher thanconcentrations elsewhere in the body. However, intoxication normally arises from eitherintentional or accidental overexposure. This is rare in comparison with chronic intoxication,

38
which may induce pathologies elsewhere in the body. The most significant elements that affectthe gastrointestinal tract are cadmium, mercury, lead, and arsenic.
3.3.3.5 Respiratory tractThe pulmonary system may be considered as having three major regions, namely thenasopharyngeal, the tracheobronchial and the pulmonary. The nasopharynx starts at theanterior nares, extending back and down to the level of the larynx. It is lined with vascularmucous epithelium, which is characterised by ciliated columnar epithelium and mucous glands.The function of the nasopharyngeal is to filter out large inhaled particles, to increase the relativehumidity of inhaled air, and to moderate the temperature of inhaled air.
The tracheobronchial region consists of the trachea, bronchi and the bronchioles, and servesas an airway between the nasopharyngeal and the alveoli in the lung. This airway is lined withepithelium cells and a thin layer of mucus. The mucus-covered surface serves as a mucociliaryescalator, moving particles from the deep pulmonary area to the oral cavities to be swallowedand excreated.
In the pulmonary system the bronchioles decrease in diameter, forming the alveoli, which end inan alveoli sac with a complex blood vessel arrangement around the alveoli. Air pockets andcells form a large surface area available for oxygen absorption and gas exchange. It is in theseareas of the lung where gas exchange takes place.
The left lung has two lobes divided by a single fissure, while the right lung is split by two deepfissures, dividing it into three lobes. The two lungs are encapsulated in a pleural cavity formedby two layers of membranes surrounding the lungs, except at the point where the bronchi enter.The respiratory tract is a target organ because:
• Exposure to and absorption of toxic compounds in the lungs are influenced by manyanatomic features, including lung volume and alveolar surface area. The uptake of toxicgases occurs throughout the respiratory system, starting at the nasopharyngeal cavity. Diffusion is the dominant driving force in the absorption of toxicants.
• The lung surface area is approximately 70 m2 in humans and the cellular barrier between airand blood is minimal. Consequently, foreign particles may be absorbed rapidly.
• Since the lungs receive 100 per cent of the cardiac blood output, they are extensivelyexposed to toxins that may be in the blood stream. The function of the lung is to exchangegases between ambient air and the blood, which means it is efficient in absorbing toxicsubstances from the air. The high oxygen concentration in the lung allows it to be sensitiveto reactive oxygen species.
• The lung is particularly vulnerable, because of the various cell types that all exhibit differentsusceptibilities to toxic damage.
For human exposure through inhalation of airborne particulates, three size-dependent fractionshave been defined:
• The inhalable fraction (diameter ≤ 100 µm) is the fraction that enters the body through thenose and mouth during breathing. It may be linked to health effects anywhere in therespiratory tract, such as rhinitis, nasal cancer, or systemic effects.
• The thoracic fraction (diameter ≤ 20 µm) penetrates into the lung below the larynx, and isrelevant for asthma, bronchitis, and lung cancer.
• The respirable fraction (diameter ≤ 10 µm) enters the alveolar region of the lung, and is linkedto such chronic diseases as pneumoconiosis and emphysema. Some agencies also considera fraction ≤ 2.5 µm, suspected to have more serious health consequences than the fraction upto 10 µm.

39
3.3.3.6 Haematopoietic systemThe haematopoietic system is the transport system that supplies substances absorbed from thegastrointestinal tract, as well as oxygen from the lungs, to the tissues. It returns carbon dioxideto the lungs and other products of metabolism to the kidneys. Blood also functions as aregulator for the body temperature and distributes hormones and other agents to regulatetissue cell functions.
Blood consists of cellular components suspended in plasma. In the adult the red blood cells(erythrocytes), white blood cells (leucocytes), and platelets are formed in the bone marrowwhich is one of the largest organs in the body. Approximately 75 per cent of the cells in themarrow belong to the white blood cells and 25 per cent are mature red blood cells. In the bloodcirculation however, there are five hundred times as many red blood cells as there are whiteblood cells. This difference is due to the fact that the red blood cell life span is much longerthan that of the white blood cells. Red blood cells are biconcave discs with a diameter ofapproximately 7,5 µm. They contain haemoglobin, an iron-containing porphyrin compound,which takes up oxygen in the lungs and releases it in the tissues. White blood cells are ofvarious types. They can leave the circulation and move through tissues where they areinvolved in combating infection, wound healing, and rejection of foreign bodies. Platelets arethe smallest cellular components in the haematopoietic system and play an important role inblood coagulation.
As almost all foreign compounds are distributed via the blood stream, the components of theblood are exposed at least initially to toxic compounds. Damage to and destruction of the redblood cells results in a reduced ability to carry oxygen from the lungs to the tissues. Destruction of white blood cells results in an increased susceptibility to bacterial and virusinfections, and may result in death.
As the production of blood cells takes place in the bone marrow, bone marrow suppression ischaracterised by a deficiency of all or some cellular elements in the peripheral blood. Thiscondition results from either a decrease in production of cells, or an inability of bone marrow tomanufacture adequate numbers of these cells. Inorganic arsenic compounds, mercury, cobalt,zinc and lead have all been shown to have effects on bone marrow function.
Several metals are known to have acute and direct haemolytic effects, e.g. arsenic, copper,cobalt, lead, mercury and zinc. Metals may directly impair red cell function either by inhibitingerythropoiesis in bone marrow or by decreasing red cell survival in the circulation, leading toanaemia. Haemolytic anaemia occurs when the rate of cell destruction in peripheral bloodexceeds the normal rate of production in the bone marrow. Other conditions includeleukopenia, polycythemia, thrombocytopenia, decreased haemoglobin, and decreasedhaematocrit.
3.3.3.7 BoneBone tissue is a major receptor for storage of certain toxic substances. It serves as a reservoirfor metals such as lead. The mechanism of skeletal uptake of substances is a surface-chemistry phenomenon, in which the exchange takes place between the bone surface and theextra-cellular fluid in contact with it. The bone surface is the hydroxyapatite crystals of the bonemineral. Because of the dimensions of the crystals the surface area is large in proportion to themass, enhancing the possibility for uptake.
The deposition and storage of toxic elements in bone may or may not be toxic. For example,the accumulation of lead has not been confirmed unambiguously to be toxic to the bone. Undercertain conditions the process of uptake is reversible, leading to release by ion exchange at thecrystal surface and by dissolution of bone crystals through osteoclastic activity. This will bereflected by an increased plasma concentration of the toxicant.

40
Exposure of humans to cadmium has been associated with osteodystrophy. Cadmium tends toreplace calcium from bone, leading to demineralisation, and it also inhibits bone formation. Other effects relate to a disturbance of uptake of essential elements, which may lead toosteotoxicity.
3.3.3.8 Endocrine systemThe endocrine system consists of those organs that secrete hormones into the blood or lymphsystems. These hormones play an important role in the activities of other organs, and generalchemical changes in the human body. The primary endocrine glands are the thyroid, adrenal,pituitary, parathyroid, pancreas, ovaries, and testicles. Although not much is known about theeffects of heavy metals on the endocrine system, some effects have been indicated tentatively,such as the effects of arsenic on the thyroid, and development of diabetes mellitus. This wasshown to be consistent with hyperglycemia and glucose intolerance reported in animal studies(Garcia-Vargas & Cebrian, 1996: 428). Testicular tumours in test animals have beenassociated with exposure to cadmium.
3.3.3.9 MuscleMuscular tissue is divided according to its function into two main groups, i.e. voluntary andinvoluntary muscle. Voluntary muscle, being under control of the will, is mainly attached to theskeleton, and hence often called skeletal muscle. Involuntary muscle functions independently,and is found in the heart, the inner and middle coats of the stomach and intestines, the uretersand urinary bladder, the windpipe and bronchial tubes, the ducts of glands, the gall bladder, theuterus and fallopian tubes, the middle coat of the blood and lymph vessels, the iris and ciliarymuscle of the eye, the dartos muscle of the scrotum, and in association with the various glandsand hairs in the skin. The effects of heavy metals on muscular tissue have not been welldescribed, but it is known that muscle degeneration has been reported for exposure to indium(Doull, Klaassen & Amdur, 1980: 445). Heavy metals such as cobalt interferes with Ca2+ in themuscle tissue, leading to muscle spasma.
3.3.3.10 EyeThe eye is a relatively small, very complex organ, and is the sensory organ of sight. It is anelaborate photoreceptor that detects information in the form of light from the environment, andtransmits this information by a series of electrochemical processes to the brain.
The cornea and the conjunctiva are the portions of the eye directly exposed to external insults. The conjunctiva is a transparent mucous membrane that extends from the lumbus over theanterior sclera. It does not cover the cornea, but passes from the eye onto the inner surface ofthe eyelid. A scar or vascularisation that can be tolerated by other body structures with noadverse effects may, in the case of the cornea, destroy function completely. A very smallamount of a corrosive substance, which would be of no consequence elsewhere in the body,can therefore be the cause of blindness if it reaches the cornea.
The eye can thus be regarded as a target organ, because of its external position in theorganism and direct exposure, as well as from systemic exposure. Exposure to dust andcorrosive substances such as calcium oxide would lead to severe eye irritation. Heavy metalions in high concentrations may combine with protein functional groups, which results in tissuedestruction.
3.3.3.11 SkinThe skin is the largest organ of the body. It consists of two basic elements, i.e. an outerepidermis of which the main function is a protective one. It covers the underlying muscles,protecting them and maintaining a constant body temperature. A secondary function issecreation, the two secreations being sebaceous material and perspiration. The dermis lyingunder the epidermis provides inherent strength to the skin, largely through its collagen content.

41
The waterproofing capability of the epidermis is potentially a problem, as the greasy surfaceaids absorption of fat-soluble materials and hence a ready route of entry for many organicchemicals. Chemicals may also pass through the cells of the sweat glands, or the sebaceousglands or through the hair follicles.
The first phase of absorption is diffusion of the toxicant through the epidermis and it is in thisarea that the rate-limiting barrier for absorption of toxicants exists.
The second phase of absorption is diffusion of the toxicant through the dermis, which is inferiorto the epidermis. The dermis contains a porous, non-selective, watery diffusion medium. Thetoxicants pass through this area by simple diffusion into the systematic system, entering theblood stream.
Dermatosis may be readily divided into two groups, i.e. primary irritant contact dermatitis, andallergic contact dermatitis. Contact dermatitis is normally influenced by immunoregulatorymechanisms.
3.3.3.12 Cardiovascular systemThe heart is known as the pump that circulates blood through the body. It consists of fourcavities, each provided at its outlet with a valve, resulting in a pumping action as blood flowsfrom one cavity to the other, eventually forcing the blood through the circulation systems. Twomain circulation systems are distinguished, i.e. the pulmonary circulatory system and thesystemic circulatory system, with the heart in-between.
The cardiovascular system is occasionally affected by toxic compounds and becomes a targetorgan mainly because of:
• The high concentration of blood flow. Toxic compounds that might be present in the bloodhave to pass through the heart and may damage the heart as well as other vascular tissue.
• The sensitivity of the heart muscles to electrolyte changes. Heavy metals such as cobaltinterferes with Ca2+ in the muscle tissue, leading to muscle spasma.
Artherosclerosis is the primary cause of myocardial infarction and cerebral infarction in theindustrial world. Chemical elements exert biological effects via enzymes, hormones, andvarious messenger molecules. Excess zinc can disrupt the utilisation of copper, an essentialelement in the protection of the cardiovascular system. It also disrupts the metabolism ofcholesterol. Both cadmium and lead have been linked to essential hypertension, that is,hypertension of unknown origin.
3.3.3.13 Immune systemThe immune system consists of a network of cells and chemical mediators, having the primaryfunction of protecting the human body against infections. The major components of theimmune system are the leukocytes, the immunoglobulins and the complement system,consisting of several plasma proteins. They interact with each other to keep the balance ofimmunity. Immunosuppression, autoimmunity, hypersensitivity or allergy, and neoplasia are themain toxic reactions of the immune system. Heavy metals are known to interfere with theimmune system in several ways. The effects may be associated with membrane alterations,modifications in signal transduction, displacement of essential metals, and interactions withcellular proteins or enzymes. In the case of essential elements, both a deficiency and excesscan result in modification of cell-mediated immune responses. In most cases of exposure tometals, effects on the immune system are observed at exposure levels that also cause othersystemic effects. Allergic contact dermatitis is believed to be influenced by both epidermalpenetration and by immunoregulatory mechanisms.

42
3.3.3.14 Reproductive systemMale reproductive systemThe testis is the organ responsible for the male reproductivity. The testis is an ovoid organ andis located at the end of the spermatic cord. The testes are freely moveable in the scrotal sac. This sac is composed of skin, a thin layer of dartos muscle and connective tissue. A thickcapsule, the tunica albuginea, surrounds the testes. Inside the testes a number of smallercompartments are formed by numerous septa. Inside each compartment are two to four highlytortuous seminiferous tubules. The adult testis has two functions:
• Spermatozoa are produced by the seminiferous tubes.• Androgens are produced by cells outside the seminiferous tubes, the Leydig cells.
These two environments are separated from each other by the blood-testis barrier and maintaina special microenvironment within the seminiferous tubules. This microenvironment protectsthe developing germ cells from external noxious substances.
Spermatogenesis starts at puberty with the mitotic division of spermatogonia, and continuesthroughout the life of a human male, although production decreases with age. Thespermatogonia are located next to the basal lamina between the Sertoli cells. However, in thehuman at the onset of spermatogenesis, all spermatogonia in the entire cross section of theseminiferous tubule do not divide, but may become active at a later stage. Eachspermatogonial cell undergoes a number of mitotic divisions, producing a clone of daughtercells.
The structure of the sperm cell is important to ensure proper fertilisation and penetration of theoocyte, as well as the consistence of the androgens. A number of chemicals are known tohave an impact on these processes, thus causing the testis to be a target organ for toxicsubstances. The rapidly growing and dividing tissue of the testis leaves it vulnerable tochemicals such as anti-cancer drugs, which may damage the cells. Because the testes have alimited blood supply, a chemical like cadmium that causes reduced blood flow may causeischaemia in the testes.
Female reproductive systemThe female reproductive tract includes the ovary, uterus, cervix and vagina. Each of theseorgans is highly specialised to ensure the production of normal offspring for the propagation ofthe species. Although these are different organs, their proper functioning depends on thefunctioning of the neroendocrine system as well as the functioning of the ovary itself. Theovaries have a dual function:
• To produce oocytes or eggs, and• To secrete the steroid hormones.
The process of germ cell production in the female is called oogenesis. In the human femaleoogenesis starts long before birth, and undergoes a series of mitoses so that by the time ofbirth the ovaries of the human female will contain a finite number of oocytes. The femalereproductive tract is considered an important target organ, because if these oocytes aredamaged or lost, for example due to exposure to hazardous chemicals or radiation, they cannotbe replaced by stem cells. The particular woman will then be infertile for the rest of her life. Ifexposure to chemicals or radiation injury caused chromosomal damage to the oocytes, therewould be no new oocyte formation. Toxic chemicals causing damage to the femalereproductive system can be divided into two categories:
• Direct-acting toxicants and indirect-acting toxicants. Direct-acting toxicants cause directdamage to the sub-cellular organelles and the micro molecules within the cells.
• Indirect-acting toxicants alter the metabolic activity of a cell or cause hormone imbalance.

43
3.3.4 Toxicology of the elementsThis section provides descriptions and summaries of the toxicology of metals in alphabeticalorder. For each element and its compounds a general description of the metabolism and toxiceffects is given, followed by a summary table listing short-term and long-term effects in targetorgan systems, as well as references to regulatory guidelines.Short-term effects are those adverse health effects observed after short-term exposures, i.e.over hours or days. It is likely that these effects would disappear if the source were removed.Long-term effects occur after short-term or chronic exposures, and the effects may persist if thesource is eliminated.
Several of the elements have not been identified to be of significance in any of the mineralprocesses. In accordance with the overall structure of the document, however, the toxicologicalassessments in this section include all those elements listed in the hazard assessment.
3.3.4.1 Antimony (Sb)Absorption:Inorganic antimony enters the human body through the oral and pulmonary routes (Lauwerys &Hoet, 1993: 19). No quantitative data are available for absorption of antimony after inhalation. Animal studies indicate that absorption after ingestion is of the order of 15 to 50 per cent (rat,hamster) (Elinder & Friberg, 1979a: 285). No similar data for humans have been documented.
Distribution:After absorption the highest levels of antimony were observed in the liver, thyroid, heart, andkidneys (Elinder et al. 1979a: 283, 286).
Excretion:Elimination and excretion depend on the type of antimony compound. Most absorbed antimonyis reportedly excreted rapidly via the urine (mainly Sb5+) and faeces (mainly Sb3+). A small partof the absorbed substance may have a long biological half-life (Elinder et al., 1979a: 283, 286;Van der Voet & de Wolff. 1996a: 458).
Acute effects:Respiratory irritation has been reported after acute occupational exposure to SbCl3 at relativelyhigh concentrations (73 mg/m3). Acute systemic exposure to antimony compounds causes dry,scaly skin, weight loss and hair loss. (Van der Voet et al., 1996a: 457). Severe (fatal)pulmonary oedema was noted after exposure to SbCl5, but the exposure level was not known(Elinder et al., 1979a: 289).
The compound stibine (SbH3) is an odourless toxic gas, which causes haemolysis (Elinder etal., 1979a: 289).
Heavy exposure to smelter fumes was reported to lead to stomach cramps, nausea, vomitingand diarrhoea. (Elinder et al., 1979a: 283).
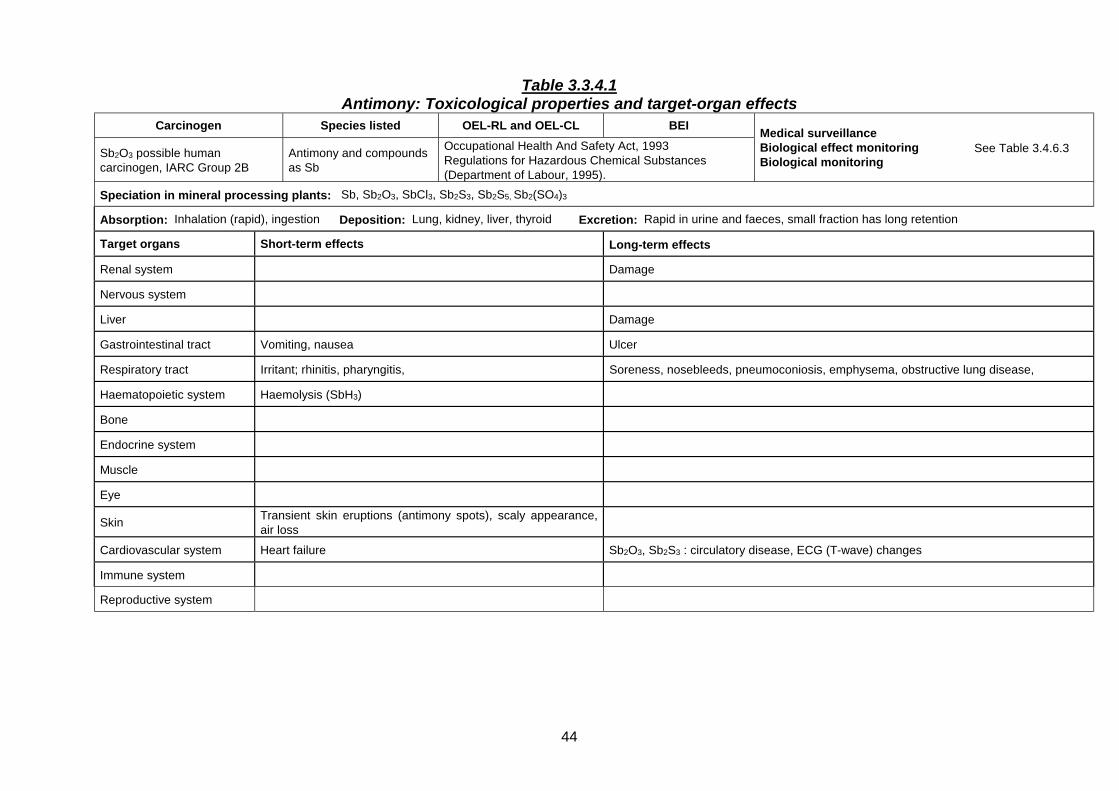
44
Table 3.3.4.1Antimony: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Sb2O3 possible humancarcinogen, IARC Group 2B
Antimony and compoundsas Sb
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Sb, Sb2O3, SbCl3, Sb2S3, Sb2S5, Sb2(SO4)3
Absorption: Inhalation (rapid), ingestion Deposition: Lung, kidney, liver, thyroid Excretion: Rapid in urine and faeces, small fraction has long retention
Target organs Short-term effects Long-term effects
Renal system Damage
Nervous system
Liver Damage
Gastrointestinal tract Vomiting, nausea Ulcer
Respiratory tract Irritant; rhinitis, pharyngitis, Soreness, nosebleeds, pneumoconiosis, emphysema, obstructive lung disease,
Haematopoietic system Haemolysis (SbH3)
Bone
Endocrine system
Muscle
Eye
Skin Transient skin eruptions (antimony spots), scaly appearance,air loss
Cardiovascular system Heart failure Sb2O3, Sb2S3 : circulatory disease, ECG (T-wave) changes
Immune system
Reproductive system

45
Chronic effects:Soreness and nosebleeds were common amongst workers exposed to 4.7 to 11.8 mg/m3 ofantimony during smelting operations. Other respiratory irritations were also reported (Elinder etal., 1979a: 289). The supporting information on chronic studies listed pulmonary toxicity andchronic interstitial inflammation as the critical effects (IRIS, 1999: database).
Pneumoconiosis-like X-ray pictures were noted by several authors in workers with long-termexposure, and antimony seems to accumulate in the lungs. After chronic exposure to SbO3,signs of obstructive lung disease and emphysema were also found (Elinder et al., 1979a: 289;Van der Voet et al., 1996a: 458).
The cardiovascular system can also be affected. Changes in the electrocardiogram and deathfrom heart failure have been documented after exposure to SbS3 (0.6 to 5.5 mg/m3 for 8 to 24months) (Elinder et al., 1979a: 289).
An increased incidence of stomach ulcers was reported for a group of antimony workers incomparison to a control group (Elinder et al., 1979a: 290).
Transient skin irritation (antimony spots) is common amongst people working with antimony orits salts (Elinder et al., 1979a: 289; Van der Voet et al., 1996a: 458).
Carcinogenicity:Evidence for carcinogenic action in laboratory animals was judged by the International Agencyfor Research on Cancer as sufficient for antimony trioxide, and limited for antimony trisulfide. In humans, antimony trioxide is considered a possible carcinogen (Group 2B) (IARC, 1989: Vol. 47). Antimony has not undergone complete review by the USEPA (IRIS, 1999: database).
Reproductive effects:One study has indicated that female workers exposed to antimony were more prone tospontaneous abortions than a control group. In another study, a high incidence of prematuredeliveries was noted amongst women occupied in antimony smelting and processing (IRIS:1999: database). These studies were conducted in 1967 and 1955, respectively, and it isuncertain how the data should be interpreted in terms of dose-response correlation.
3.3.4.2 Arsenic (As)Absorption:The extent of deposition, absorption and distribution in the system depends on the solubility andpossibly the oxidation state of arsenic.
For the inhalation route the size of the aerosols is important. Up to 85 to 90 per cent of water-soluble trivalent arsenic deposited in the lungs can be bio-available (Hrudey, Chen, Rousseaux,1996: 78, 83). Particles larger than 5 microns will be deposited in the upper respiratory tractwhere mucociliary clearance will lead to ingestion and absorption from the gastrointestinal tract(Fowler, Ishinishi, Tsuchiya, Vahter, 1979a: 299). Both organic and soluble inorganic arsenicare easily and rapidly absorbed (70 – 90 per cent) from the gastrointestinal tract (Fowler et al.,1979a: 299; Hrudey et al., 1996: 80).

46
Table 3.3.4.2Arsenic: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Human carcinogen As and compounds (as As)
IARC Group 1 Arsine (AsH3) :
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: As2O3, NaAsO2, AsCl3
Absorption: Inhalation (good); ingestion (high); skin (possible) Deposition: Skin, hair, bone Excretion: Urine (rapid)
Target organs Short-term effects Long-term effects
Renal system High initial concentration, rapid excretion
Nervous system Peripheral neuritis, loss of touch
Liver High initial concentration, rapid excretion Swelling, cancer
Gastrointestinal Tract
Respiratory tract Irritation, cough, dyspnoea, chest pain, bronchitis Ulcers (mucous membranes), lung cancer
Haematopoietic system Anaemia, leucopenia
Bone
Endocrine system
Muscle
Eye
Skin Irritation, contact dermatitis (As2O3) Hyperkeratosis, cancer, pigmentation
Cardiovascular system Abnormal ECG, vascular disorders, gangrene
Immune system
Reproductive system Foetal absorption (bone, skin, liver, brain)

47
Distribution:Once absorbed, arsenic is rapidly cleared from the blood (24 hours) and widely distributed inthe body, mainly to the liver, kidney, spleen, lung and gastrointestinal tract. Over the next 2 - 4weeks the arsenic is then redistributed to the hair, nail, skin and bone (Hrudey et al. 1996: 77). Clearance from the skin and bones is much slower and the major portion of the body burden issituated in the bone, muscle and skin (Fowler et al., 1979a: 300; Hrudey et al., 1996: 80).
Excretion:The major part of absorbed arsenic is excreted in the urine within 48 hours either unchanged,or in detoxified form as methyl-arsenic compounds (Fowler et al., 1979a: 293; Lauwerys &Hoet, 1993 22).
Care must be taken when monitoring arsenic in the urine, as consumption of certain seafoodcan give rise to very high (organic) arsenic levels. For occupational monitoring the levels ofinorganic arsenic should rather be measured (Lauwerys et al., 1993: 23).
Acute effects:Acute or sub-acute exposure to arsenic (especially to arsenic trioxide or arsenic trichloride) cancause coughing, dyspnoea, chest pain and irritation of the skin, mucous membranes and eyes.
Gastrointestinal effects such as vomiting and diarrhoea have been noted (Fowler et al., 1979a:304; Garcia-Vargas & Cebrian, 1996: 424).
Chronic effects:Chronic exposure in the occupational environment can cause melanosis, lesions of the skin andmucous membranes, (including perforation of the nasal septum), palmar and plantarhyperkeratosis, nervous and respiratory disorders and lung cancer. Abnormal ECG,disturbance of peripheral circulation and gangrene of the extremities (Blackfoot disease) havealso been reported (Fowler et al., 1979a: 305; Garcia-Vargas et al., 1996: 424). The likelihoodfor Blackfoot disease has been found to increase with dose and age, especially for personsolder than 40 (IRIS, 1999: database).
Gastrointestinal disturbances such as loss of appetite, cramps, nausea, constipation, ordiarrhoea may occur.
Liver damage with resulting jaundice may occur, as well as disturbances of the blood, kidneysand nervous system (Lewis, 1995: database; Garcia-Vargas et al., 1996: 424).
Painful peripheral nervous disturbance (neuritis) in the extremities, anaemia, and liverdisturbance have also been reported and are symptomatic of chronic arsenic intoxication. Abnormal neurological findings can persist for years after a poisoning incident (Fowler et al.,1979a: 307).
Chronic exposure in the general public can arise from environmental contamination, especiallyfrom drinking water, and consumption of contaminated beverages or food. Studies have shownin such cases an occurrence of skin lesions, vascular disorders, and “black foot” disease(Fowler et al., 1979a: 305).
Carcinogenicity:Arsenic is a Group 1 human carcinogen (IARC 1987: Vol. 1, Suppl. 7), causing tumours of thelung, liver, bladder, prostate and skin (IRIS, 1999: database; Garcia-Vargas et al., 1996: 433).
Reproductive effects:Arsenic seems to cross the placental barrier, as levels in foetal bone, liver, skin and brain havebeen reported to increase with duration of the pregnancy (Fowler et al., 1979a: 300). There are

48
some studies that suggest involvement of the immune system and possible genotoxic effects(Garcia-Vargas et al., 1996: 431-432).
Teratogenic effects have been demonstrated in animal studies (Fowler et al., 1979a: 309).
ArsineArsine (hydrogen arsenide, AsH3) is a colourless flammable gas with a slight garlicky odour andis formed whenever nascent hydrogen is evolved in material containing arsenic. Many orescontain arsenic as impurity and arsine can therefore be generated in the ore processing, non-ferrous metal refining and silicon steel industries when ores being processed could accidentallycome into contact with acids. Arsine can also be formed via the hydrogen ion during hydrolysisreactions, for example between arsenic containing dross and moisture (Fowler et al., 1979a:313; IRIS, 1999: database)
The mechanism of arsine toxicity differs from that of other arsenic compounds. It is a potenthaemolytic poison. The lethal dose is 250 mg/m3 for 30 min. Symptoms appear within a fewhours at exposure levels of 0.5 to ten mg/m3 and include upset stomach, shortness of breath,palpitations and backache, followed by red urine and jaundice (Fowler et al., 1979a: 313).
Arsine is a confirmed human carcinogen (Lewis, 1995: database).
3.3.4.3 Barium (Ba)Absorption:The toxicity of barium salts depends on their solubility. Soluble barium compounds are readilyabsorbed from the respiratory and gastrointestinal tract and act as potassium antagonists in themuscles, causing initial stimulation followed by paralysis (Reeves, 1979a: 321).
Barium sulphate is highly insoluble in water and is routinely used as X-ray contrast medium,with negligible absorption during its residence time in the alimentary canal (Reeves, 1979a:324).
Inhaled barium sulphate seems to be slightly soluble in bodily fluids, possibly in colloidal form. Clearance from the lung (half-life eight to nine days) depends on the specific surface area andthermal history of the particles (Reeves, 1979a: 324).
Distribution:Upon chronic exposure barium is deposited in the bones (three to five times as readily ascalcium or strontium) and pigmented parts of the eye (Reeves, 1979a: 325).
Excretion:After ingestion, barium is excreted mainly via the faeces (91 per cent), with sweat and urinebeing minor routes (Reeves, 1979a: 325).
Acute effects:The Ba2+ ion in toxic doses (0,2 to 0,5 g in adults) is a muscle poison, causing initialstimulation, followed by paralysis. Gastrointestinal symptoms are followed by skeletomuscularand cardiac stimulation. Barium is a potassium antagonist and it appears that the symptomsmay be attributable to severe hypokalemia. (Reeves, 1979a: 326; Lewis, 1995: database).
Barium sulphide, barium carbonate and barium oxide cause respiratory and eye irritation, andincidences of dermatitis after skin contact have been reported (Lewis, 1995: database)..

49
Table 3.3.4.3Barium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Soluble compounds as Ba:Not carcinogenic
BaSO4 respirable dust
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: BaCO3, BaO, BaSO4, BaS, BaCl2
Absorption: Inhalation, ingestion (soluble salts) Deposition: Bone, eye Excretion: Faeces, sweat, urine
Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract Vomiting, colic, diarrhoea (soluble salts)
Respiratory tract Irritant (BaO, BaCO3, BaS) Benign pneumoconiosis (baritosis). Radiologically conspicuous. (BaSO4)
Haematopoietic system
Bone Accumulation
Endocrine system
Muscle Severe hypokalemia, convulsive tremors
Eye Irritant (BaO, BaCO3, BaS) Accumulation
Skin Irritant (BaO, BaCO3, BaS)
Cardiovascular system Slow, irregular heartbeat, transient high blood pressure
Immune system
Reproductive system BaCl2 (male rat)

50
Chronic effects:Although several studies have been conducted to test a connection between barium exposureand elevated blood pressure, no conclusive evidence was found for humans (IRIS, 1999:database).
Inhalation of barium sulphate can lead to a benign, symptomless form of pneumoconiosis(baritosis) with conspicuous radiographic manifestations. There is no apparent impairment ofpulmonary function. There are indications that accumulation of barium in the lungs will diminishafter cessation of exposure (Reeves, A L. 1979a: 321; IRIS, 1999: database.)
Carcinogenicity:Barium is not likely to be carcinogenic to humans (IRIS, 1999: database).
Reproductive effects:Reproductive effects have been observed with BaCl2 and BaCO3 under experimental conditions(Lewis, 1995: database).
3.3.4.4 Beryllium (Be)Absorption:Soluble beryllium compounds are considerably more hazardous by inhalation than by ingestionor skin contact. At physiological pH, most of these compounds are rendered insoluble, and aretherefore not easily absorbed by the body (Reeves, 1979b: 329).
The largest proportion of ingested beryllium is passed through the gastrointestinal tractunabsorbed.
Distribution:Short-term storage of beryllium takes place in the liver, and long-term storage in the skeleton.
Excretion:During the excretion process kidney damage may result.
Elimination of beryllium from the lung seems to be a two-phase process. The first phase has ahalf-life of two to three weeks, leaving a long-term residue.
Acute effects:Inhalation of soluble beryllium compounds can cause acute respiratory tract effects such asrhinitis, pharyngitis, tracheobronchitis and occasionally fatal pneumonitis (Reeves, 1979b: 335;Lewis, 1995: database).
During contact with the skin, beryllium is bound to the epidermis and not easily absorbed intothe system. Contact dermatitis is fairly common when handling soluble beryllium compounds(Reeves, 1979b: 335).
Chronic effects:The chemical reactivity and toxicity of beryllium oxide are inversely related to the firingtemperature during which it is prepared in a calcining process (500 – 1750 °C) (Reeves, 1979b:335). Chronic occupational exposure to so-called “low-fired” beryllium oxide is associated withberylliosis or chronic beryllium disease (CBD). This is a slow-developing pulmonary diseasewhich in the past had a relatively high mortality rate, and can appear from 1 to 25 years afterexposure (Reeves, 1979b: 336).

51
Table 3.3.4.4Beryllium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Human carcinogenIARC Group 1 Beryllium
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: BeO, BeSO4, Be(OH)2, BeCl2, BePO4
Absorption: Mainly lung Deposition: Lung, liver, kidney, bone Excretion: Urine
Short-term effects Long-term effects
Renal system Kidney damage
Nervous system
Liver Short term storage Granulomas
Gastrointestinal tract
Respiratory tract Rhinitis, tracheitis, bronchitis, pneumonitis (BeF2) Berylliosis, (“low-fired” BeO), pulmonary insufficiency
Haematopoietic system Disturbances (animals)
Bone Rickets (animals)
Endocrine system
Muscle
Eye Conjunctivitis
Skin Allergic dermatitis, ulceration Dermatitis, ulceration
Cardiovascular system
Immune system
Reproductive system

52
CBD is characterised by dyspnoea, cough, reduced pulmonary function and weight loss(Benson & Zelikoff 1996: 929; Lewis 1995: database; Reeves, 1979b: 336). CBD has alsobeen reported for people not occupationally exposed, and family members who had beenexposed to workers’ contaminated clothing (IRIS, 1999: database; Lewis, 1995: database). The extreme sensitivity of some individuals towards CBD is thought to be linked to immunefactors (IRIS, 1999: database).
The injurious threshold level (mg Be/m3) for the “high fired” oxide is considered to be about 30,compared to one to three for “low-fired” oxide and 0,1 to 0,5 for the sulphate (Reeves, 1979b:335).
Non-healing skin granuloma from beryllium-contaminated wounds and abnormal lymphocytetests have been reported for occupational exposure (IRIS: 1999: database; Lewis 1995:database). Granulomatous and fibrotic changes to the liver and spleen have been reported(Lewis 1995: database).
Carcinogenicity:Beryllium inhibits phosphatases and other enzymes and is thought to interfere with DNAreplication (Reeves, 1979b: 338 - 339). It is classified as a Group 1 human carcinogen (IARC1993: Vol. 58).
Reproductive effects:No data have been documented to indicate reproductive effects in humans.
3.3.4.5 Bismuth (Bi)Absorption:Bismuth compounds taken up via inhalation and ingestion are slightly to moderately absorbedin the system, depending on their solubility. No quantitative data are available (Fowler et al.,1979b: 348).
Distribution:After absorption it is distributed to the soft tissues and bone, with the highest concentrationbeing found in the kidney and liver (Fowler et al., 1979b: 348).
Excretion:A large proportion of ingested bismuth passes through the gastrointestinal tract unabsorbedand is excreted in the faeces. Absorbed bismuth is excreted mainly in the urine, with the ratedependent on the solubility (Fowler et al., 1979b: 348).
The following biological half-lives have been adopted for humans (Fowler et al., 1979b: 349):
System Biological half-life (days)
Whole body retention 5
Kidney 6
Liver 15
Spleen 10
Bone 13,3

53
Table 3.3.4.5Bismuth: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Bismuth tellurideNot a human carcinogen
Bismuth telluride (Se-doped)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Bi, Bi2O3, Bi2S3, Bi2(SO4)3, BiCl3
Absorption: Poor. Ingestion, inhalation Deposition: Kidney, liver, bone Excretion: Urine, faeces
Target System Short-term effects Long-term effects
Renal system Acute failure Storage
Nervous system Confusion, tremors, clumsiness
Liver Fatty degeneration, hepatitis
Gastrointestinal tract Irritant (BiF5) Gingivitis, lead-like pigmentation of gums
Respiratory tract Irritant (BiF5), (trimethyl bismuth)
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Irritant (trimethyl bismuth)
Skin Irritant (trimethyl bismuth) Eruptions, pigmentation
Cardiovascular system
Immune system
Reproductive system Bi(NO3)3 Vaginal pigmentation

54
Acute effects:In the industrial environment bismuth is considered to be one of the less toxic heavy metals. Up to 1996 no industrial bismuth poisoning had been reported (Lewis, 1995: database). Reported cases of intoxication are mainly due to therapeutic and cosmetic uses of bismuthcompounds (Lewis, 1995: database; Fowler & Vouk, 1979b: 345). During therapeutic use,acute kidney failure and fatty degeneration of the liver have been reported (Fowler et al.,1979b: 350).
Trimethylbismuth has been reported to irritate the upper airways, eyes and broken skin (Fowleret al., 1979b: 349).
Chronic effects:The literature notes the similarity in the pharmacological and toxic behaviour of lead andbismuth. The dark line in the gums, sometimes noted in cases of lead poisoning, can also becaused by exposure to bismuth. This can complicate the diagnosis of plumbism (Lewis, 1995:database).
Some kidney and liver damage and neurological symptoms have been associated withtherapeutic uses (Fowler et al., 1979b: 351). No adverse effects have been reported foroccupational exposure (Lewis, 1995: database).
Carcinogenicity:IARC has not classified bismuth a human carcinogen.
Reproductive effects:Absorbed bismuth can be transported across the placenta (animal studies) (Fowler et al.,1979b: 345).
3.3.4.6 Cadmium (Cd)Absorption:Occupational uptake of cadmium is mainly attributable to inhalation of dust and fumes (CdOparticles, predominantly < 10 µm) (Hrudey, Chen, Rousseaux, 1996: 91). Extensive informationis available on the bioavailability of cadmium by various routes in both animals and man(Hrudey et al., 1996: 96 - 99). The pulmonary absorption rate is dependent on the solubilityand particle size of inhaled material (Hrudey, et al., 1996: 92), and can be up to 50 per cent(Friberg, Kjellstr!m, Nordberg, Piscator, 1979a: 361). A fraction of the dust particles depositedin the respiratory tract will be cleared to the digestive system (Lauwerys & Hoet, 1993: 32).
Absorption from the gastrointestinal tract is low, (more than 90 per cent is excreted in thefaeces), but is increased in persons with a low dietary intake of iron, calcium or protein(Lauwerys, et al., 1993: 32; Hrudey, et al., 1996: 94; Gerhardsson & Skerfving, 1996: 85).
Distribution:Cadmium accumulates in the liver, bone and kidneys. About 50 per cent of the body burdencan be found in the kidney and liver (Friberg, 1979a: 361). The kidney is the critical targetorgan, showing the first signs of damage and urinary analysis will determine whenprecautionary measures are to be taken.
Excretion:Once absorbed, clearance from the body is slow. The literature quotes a biological half-life of10 to more than 20 years (Friberg et al., 1979a: 355; Lauwerys, et al., 1993: 32; Hrudey, et al.,1996: 92).

55
Table 3.3.4.6Cadmium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEICd and compounds (except CdOfume and CdS pigments) (as Cd)Cadmium oxide (CdO) fume (as Cd)Human carcinogen
IARC Group 1Cadmium sulphide (CdS) pigments(respirable dust Cd)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: CdO, CdS, CdSO4, CdCO3, Cd stearate, Cd acetate
Absorption: Inhalation, ingestion Deposition: Kidney, lung, pancreas Excretion: Very slow. Faeces, urine
Short-term effects Long-term effects
Renal system Storage; chronic disease, proteinuria, kidney stones,calcuria
Nervous system Headache
Liver Storage; disturbed function
Gastrointestinal tract Nausea, vomiting, cramps, diarrhoea
Respiratory tract Shortness of breath, pulmonary oedema, pneumonitis Emphysema
Haematopoietic system Anaemia
Bone Mineral depletion, osteoporosis, osteomalacia
Endocrine system
Muscle
Eye
Skin
Cardiovascular system Hypertension
Immune system
Reproductive system Possible prostate cancer; reproductively active
Experimental

56
Acute effects:Brief inhalation of high concentrations can cause acute pulmonary oedema and death. Fatalamounts of fumes and dust can be inhaled without sufficient discomfort to warn workers toleave the area (Lewis, 1995: database). Symptoms may appear only 24 hours after acuteexposure (Friberg et al., 1979a: 367).
Acute poisoning in the industrial environment is usually caused by inhalation during activitieslike welding, brazing or smelting of cadmium-containing metals. An airborne concentration of 1mg/m3 for 8 hours is considered to be sufficient to cause clinical symptoms, whilst levels of 5mg/m3 for 8 hours could possibly be lethal. Symptoms include shortness of breath, generalweakness and fever, and in severe cases, pulmonary insufficiency, shock and death (Friberg,et al., 1979a: 363).
Ingestion can cause acute pulmonary oedema (CdCl2) (Lewis, 1995: database). Cadmiumcompounds are irritants with such a violent emetic effect that there is little chance ofabsorption.(Lewis, 1995: database).
CdO fumes can lead to metal fume fever, similar to that caused by ZnO. Pulmonary effects arecharacterised by coughing, difficult breathing and cyanosis. Inhalation of CdO dust can lead tochanges in pulse rate, sense of smell, elevated blood pressure and proteinuria (Lewis, 1995:database).
Chronic effects:The effects of chronic inhalation exposure seem to depend on the intensity of exposure: themore intense the exposure the more likely lung damage like emphysema is, as opposed toalmost exclusive renal damage seen in chronic low-level exposure (Friberg et al., 1979a: 368).
The primary target organ is the kidney, irrespective of exposure route. Up to 30 per cent of thetotal body burden will normally be stored in the kidneys (Friberg et al., 1979a: 361). The firstsign of chronic cadmium poisoning is an increase of proteins in the urine (proteinuria). Increased levels of amino acids, glucose and phosphates may be seen at a later stage (Friberget al., 1979a: 368). Increased excretion of calcium (calcuria) has been noticed followingexposure to cadmium (Fowler & Nordberg, 1996e: 760). Once kidney damage has occurred,cadmium excretion rises considerably, and in the most severely poisoned people, kidney levelsare almost normal, in contrast to liver levels (Friberg et al., 1979a: 362).
Anaemia and disturbed liver function may also occur. In addition, the lung, bone (Itai-Itaidisease), cardiovascular, and reproductive systems can be affected by chronic ingestion(Friberg et al., 1979a: 368).
Carcinogenicity:Cadmium compounds are Group 1 human carcinogens (IARC 1993: Vol. 58). Occupationalexposure has been shown to increase the risk of prostate cancer (Friberg et al., 1979a: 355,371). Inhalation of cadmium compounds can contribute to the development of lung cancer(Benson, & Zelikoff, 1996: 934).
Reproductive effects:Cadmium does not cross the placental barrier (Friberg et al., 1979a: 362). Experimental datahave shown that cadmium compounds exhibit teratogenic, mutagenic and reproductive effects(Friberg et al., 1979a: 371 - 372).

57
3.3.4.7 Calcium (Ca)Absorption:Calcium compounds are common air pollutants and nuisance dusts and should be consideredtoxic only when they contain toxic components, such as arsenic or cyanide, or as calcium oxideor calcium hydroxide. Calcium carbonate, calcium hydroxide and especially calcium oxide areskin, eye and mucous membrane irritants (Lewis 1995: database). For the purpose of thisinvestigation assessments were limited to calcium hydroxide and calcium oxide. Cyanides,although prominent in mineral processing, were not included in the current assessment.
Distribution:Consider only irritation effects, no systemic distribution.
Excretion:Consider only irritation effects, no systemic distribution.Acute effects:Calcium oxide is an irritant, powerfully caustic to living tissue (Lewis 1995: database).
Calcium hydroxide is a severe eye irritant and a skin, mucous membrane and respiratory irritant(Lewis 1995: database).
Chronic effects:Irritation effects are more concentration dependent than time dependent.
Carcinogenicity:Carcinogenicity of certain calcium compounds is ambiguous and subject to study regardingboth as chemo-preventive agents and co-carcinogens (Poirer & Littlefield., 1996: 290). Calciumarsenate is a confirmed human carcinogen, but this is due to the anion rather than calcium(Lewis 1995: database; IARC 1987: Vol. 23, Suppl. 7).
Reproductive effects:CaF2 has shown experimental reproductive effects (Lewis 1995: database).

58
Table 3.3.4.7Calcium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Calcium carbonate/ silicate total inhalable
Calcium carbonate/silicate total respirable
Calcium hydroxide
Calcium oxide
Ca arsenate confirmed,certain compoundspossible cocarcinogens
Calcium cyanamide
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: CaO, Ca(OH)2, CaCO3, CaSO4, CaS, Ca phosphates
Absorption: No data available Deposition: No data available Excretion: No data available
Target organ Short-term effects Long-term effects
Renal system
Nervous System
Liver
Gastrointestinal tract
Respiratory tract Poison (CaS); irritant (CaO, Ca(OH)2, Ca(NO3)2)
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Irritant (CaO, Ca(OH)2 (severe), CaCO3, Ca phosphates (di, tribasic), Ca(NO3)2)
Skin Irritant (CaO, Ca(OH)2, CaCO3, Ca phosphates (di, tribasic), Ca(NO3)2); dermatitis (Ca(OH)2)
Cardiovascular system
Immune system
Reproductive system

59
3.3.4.8 Chromium (Cr)Absorption:Cr6+ compounds are more readily absorbed from the lungs, gastrointestinal tract and skin thanCr3+ compounds (Langard et al., 1979: 383; Hrudey, Chen, Rousseaux, 1996:103, 105, 107). The bioavailability of chromium is governed by a very complex biochemistry of which thereduction of Cr6+ to Cr3+ in the cells renders it difficult to transport (Klein, 1996: 209). The rateof absorption from the respiratory system depends on solubility. Insoluble compounds tend toremain in the lung (Hrudey et al., 1996: 103).
Cr3+ compounds are poorly absorbed from the gastrointestinal tract (Hrudey et al., 1996: 105).
Distribution:Absorbed chromium compounds (except chromates) are rapidly removed from the blood anddistributed in various tissues (lung, lymph nodes, kidney, liver, bladder, bone), or excreted inthe urine (Hrudey et al., 1996:103).
Animal studies have shown chromium retention to be dependent on the route of administrationand speciation. Accumulation can occur in the hair, reticulo-endothelial system, liver, spleen,bone marrow and kidneys (Langard et al., 1979: 388).
Excretion:Absorbed chromium is excreted mainly in urine. Studies of the kinetics suggest the existenceof three compartments with excretion half-lives of seven hours, 15 to 30 days, and three to fiveyears (Lauwerys & Hoet, 1993: 42).
Acute effects:Bronchial asthma has been reported after inhalation of chromate or chromic acid (Langard etal., 1979: 392).
Irritative dermatitis has been reported after contact with Cr6+ salts. Sensitivity seems todiminish with renewed exposure. Allergic eczematous dermatitis is wide-spread and not onlyassociated with industrial exposure to Cr6+, but is also caused by Cr3+ (Lewis, 1995: database;Langard et al., 1979: 390).
Chronic effects:Chromium accumulates in the lungs with age, while decreasing in all other organs.(Langard etal., 1979: 389; Lauwerys et al., 1993: 42). Long-term effects include damage to the kidneys. Respiratory cancer is associated with inhalation of water-soluble chromium (Benson & Zelikoff,1996: 930).
Deep, slow-healing skin ulcers have been noted in industry, especially after contact of chromiccompounds with broken skin. Ulceration of the nasal mucosa and perforation of the nasalseptum have also been reported (Langard et al., 1979: 390).
Carcinogenicity:Cr6+ compounds are Group 1 human carcinogens (IARC, 1990: Vol. 49). There is a well-established link between inhalation of Cr6+ compounds and lung cancer (Lewis, 1995:database; Lauwerys et al., 1993: 42; Hrudey, et al., 1996: 101; Klein, 1996: 208; Benson et al.,1996: 930). A latency period of 15 to 17 years has been reported (Langard et al., 1979: 393).
Skin cancers have been elicited in animal studies (Langard, 1979: 383).

60
Table 3.3.4.8Chromium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Chromium
Chromium (II) compounds (as Cr)
Chromium (III) compounds (as Cr)Cr6+ is a human carcinogenIARC Group 1
Chromium (VI) compounds (as (Cr)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: Cr, Cr2O3, CrO3, Cr2O6, FeCr, carbides, silicides, flourides, sulphates, nitrates, phosphates
Absorption: Inhalation, ingestion Deposition: Lung, hair, liver, kidney, bladder, lymph nodes, bone Excretion: Urine, multistage
Target organ Short-term effects Long-term effects
Renal system Increased levels Nephrotoxicity
Nervous system
Liver Increased levels
Gastrointestinal tract
Respiratory tract Irritant cough, allergic asthma Accumulation, cancer, allergic asthma, nasal ulceration
Haematopoietic system
Bone Increased levels Increased levels
Endocrine system
Muscle
Eye
Skin Irritative and allergic dermatitis, Cancer, ulceration,
Cardiovascular system
Immune system
Reproductive system Crosses placental barrier

61
Reproductive system:Chromium can cross the placental barrier, (possibly as the glucose tolerance factor) asevidenced by its presence in the newborn (Langard et al., 1979: 388). Some mutation effectshave been reported (Lewis, 1995: database).
3.3.4.9 Cobalt (Co)Absorption:Only limited data are available for the absorption of cobalt from the lung and gastrointestinaltract. The evidence points to solubility and the presence of other metals as possibledetermining factors. Absorption after ingestion varies widely, depending on the amountingested and nutritional factors (Elinder & Friberg, 1979b: 402; Gerhardsson & Skerfving, 1996:99).
Distribution:Absorbed cobalt is distributed mainly to the liver and kidneys (Elinder et al., 1979b: 403;Gerhardsson et al., 1996: 99).
Excretion:After ingestion the major portion of cobalt is excreted, unabsorbed, in the faeces. Absorbedcobalt will be excreted mainly through the urine, irrespective of route of uptake. Renalclearance is thought to be in two phases: fast excretion (half-life 0,5 to 2,7 days), followed bypronounced retention (half-life several years) (Elinder et al., 1979b: 400; Lauwerys & Hoet,1993: 47).
Acute effects:Ingestion of soluble cobalt salts can cause irritation evidenced by nausea and vomiting (Lewis,1995: database). Cases have been reported of cobalt chloride ingestion causingcardiomyopathy (Gerhardsson et al., 1996: 99; Elinder et al., 1979b: 406).
Inhalation of cobalt may lead to irritation of the mucous membranes and allergic reactions(coughing, wheezing, shortness of breath). Skin contact can cause dermatitis. (Elinder et al.,1979b: 405; Gerhardsson et al., 1996: 99; Lewis, 1995: database).
Chronic effects:Progressive lung disease (hard metal disease) was reported amongst workers in the hardmetals industry (Elinder et al., 1979b: 405; Gerhardsson et al., 1996: 99).
Carcinogenicity:Cobalt compounds are classified as possible human carcinogens, Group 2b (IARC 1991: Vol. 52).
Reproductive effects:No data have been documented to indicate reproductive effects in humans.

62
Table 3.3.4.9Cobalt: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Possible human carcinogenIARC Group 2b Cobalt and compounds (as Co)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: Co, CoO, Co(OH)2, CoCl2, CoS, CoSO4, Co(CN)2
Absorption: Inhalation, ingestion Deposition: Liver Excretion: Urine (inhalation)( two-phase); faeces (ingestion)
Target organ Short-term effects
Renal system Accumulation
Nervous system
Liver Accumulation
Gastrointestinal tract Irritant (soluble compounds); nausea, vomiting
Respiratory tract Allergy (wheezing, coughing) Pneumoconiosis ( “hard metal” disease)
Haematopoietic system
Bone
Endocrine system
Muscle
Eye
Skin Irritation
Cardiovascular system Cardiomyopathy
Immune system
Reproductive system

63
3.3.4.10 Copper (Cu)Absorption:Absorption from the gastrointestinal tract is homeostatically controlled (largely by the liver) andvariable, except in copper-related diseases (Wilson’s, and Menke’s diseases). The presence ofother metal ions (Cd, Fe, Zn), age, gender, pregnancy, diet and ascorbic acid can alsocontribute to the variability of copper absorption (Hrudey et al.,1996: 118, 119).
Absorption of copper via dermal exposure has been reported (Hrudey et al., 1996: 120), butthere are no quantitative data available for absorption from copper deposited in the lungs(Hrudey et al., 1996: 119).
Distribution:Once absorbed, copper is transported to the liver which then redistributes part of this to otherorgans, especially the brain, heart and kidneys (Hrudey et al., 1996: 118).
Excretion:Excretion is mainly via the bile in the faeces. Urinary excretion is minor. Biological half-life isabout 4 weeks in humans (Piscator, 1979a: 414, 415).
Acute effects:Copper sulphate is a powerful emetic (Piscator, 1979a: 417). Copper dust and fumes arerespiratory irritants. Copper sulphate and chloride have also been reported to be responsible forirritation of the skin and conjunctivae, possibly due to allergic reaction. Cuprous oxide is an eyeand upper respiratory tract irritant (Lewis, 1995: database). Exposure to copper and copperoxide fumes has been responsible for metal fume fever (fever, chills, dyspnoea, muscularsoreness, nausea and fatigue) (Piscator, 1979a: 416; Benson et al., 1996: 935).
Chronic effects:Industrial exposure has caused congestion of respiratory mucous membranes and perforationof the nasal septum (Benson et al., 1996: 935).
Carcinogenicity:Copper compounds as a group are not classified as carcinogenic by IARC, although an excessof cancer cases has been claimed in the copper smelting industry (Lewis, 1995: database).
Reproductive effects:There is no information in the literature to indicate reproductive effects in humans by excesscopper.

64
Table 3.3.4.10Copper: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Copper fumeNot a human carcinogen
Dusts & mists as Cu
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Cu, Cu(CN)4, Cu2S, CuSO4, CuO, CuFe sulphides, Cu hydroxides, Cu phosphate
Absorption: Unknown Deposition: Liver, brain, heart, kidney, muscles Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal System Storage
Nervous System
Liver Storage Storage
Gastrointestinal Tract Emetic (CuSO4)
Respiratory tract Irritant (fumes) None reported
Haematopoietic System
Bone
Endocrine System
Muscle Storage
Eye Irritant (CuSO4, CuCl2)(possible allergen)
Skin Irritant (CuSO4, CuCl2)(possible allergen)
Cardiovascular system Storage
Immune system
Reproductive system

65
3.3.4.11 Indium (In)Absorption:Absorption of inhaled indium oxide (In2O3) has been shown to be low to moderate ion animalstudies (Fowler, 1979c: 431). In2O3 has low toxicity (Lewis, 1995: database).
Distribution:The chemical form of indium mainly determines distribution in body tissues. Ionic species aremainly concentrated in the kidneys. Colloidal indium oxide is accumulated in the liver, spleenand other organs of the reticulo-endothelial system (Fowler, 1979c: 431).
Excretion:Animal experiments showed a biphasic excretion pattern, with half-lives of about two and 69 to74 days, respectively. In mice, excretion of indium is primarily dependent on the chemical formexposed to. Ionic species are mainly excreted via the kidneys, while colloidal material isexcreted mainly in the faeces (Fowler, 1979c: 431).
Acute effects:Indium affects the liver, heart, kidneys, and the blood. The results of animal studies showedthat the more soluble salts of indium were very toxic (ASOSH, 2000). Inhalation of indiumcompounds may cause damage to the respiratory system (Lewis, 1995: database; Fowler,1979c: 432). No cases have been reported of systemic effects in humans exposed to indium.
Chronic effects:Indium chloride is nephrotoxic (Fowler, 1996f, 725; Yamauchi & Fowler, 1996: 752)
Carcinogenicity:No agency in the world has listed indium as carcinogenic.
Reproductive effects:Teratogenic effects have been observed in animal experiments (Fowler, 1979c: 433), but nohuman cases relating to industrial exposure have been documented.

66
Table 3.3.4.11Indium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen Indium & compounds (as In)Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Not identified
Absorption: Unknown Deposition: Unknown Excretion: Urine (ionic); faeces (colloidal)
Target organ Short-term effects Long-term effects
Renal System Histological damage (animals) Concentration, failure
Nervous System
Liver Damage (colloidal material)
Gastrointestinal tract
Respiratory tract
Haematopoietic system Blood Blood
Bone Storage
Endocrine system
Muscle Storage
Eye
Skin Severe irritant (nitrate) Storage
Cardiovascular system Heart Heart
Immune system
Reproductive system Teratogenic (animals)

67
3.3.4.12 Iron (Fe)AbsorptionIron is potentially toxic by all routes of exposure, and in all dosages and forms. Fe2+ is moretoxic than Fe3+ (Lewis, 1995: database).
Elinder et al., (Elinder & Piscator, 1979c: 439) could not find supporting data for the calculationof the pulmonary absorption of iron. No other reference could be located to more recentstudies.
Absorption of ingested iron is regulated by homeostasis (the level of iron in the bodydetermines the absorption). In addition factors such as age, health of the gastrointestinal tract,chemical speciation and dietary factors also play a role. Absorbed iron is detoxified in theserum by binding to transferrin and transported by this means to storage sites (Elinder et al.,1979c: 439).
Distribution:About two-thirds of the iron in the body is bound to haemoglobin in the blood. Most of theremaining iron is stored as protein complexes in the liver, bone marrow and spleen (Elinder etal., 1979c: 440, 441).
Excretion:About 0,01 per cent of the body burden of iron is excreted per day via the urine, faeces andskin. Large amounts of iron can be lost during haemorrhaging. The normal biological half-lifeof iron is estimated to be 10 to 20 years (Elinder et al., 1979c: 440).
Clearance of particles from the lung takes place at about 20 to 40 per cent of the depositedamount per year (Elinder et al., 1979c: 441).
Acute effects:Acute iron intoxication happens most often by the accidental ingestion of iron-containingmedicine by young children. It is characterised by vomiting and shock, which, if survived, isfollowed by liver damage and kidney failure (Elinder et al., 1979c: 442).
Animal studies have shown irritation of the upper airways, coughing and respiratory difficultiesand after inhalation of iron oxide dust (500 mg Fe/m3). Transient histological changes werealso noticed (Elinder et al., 1979c: 442). With prolonged contact iron dust can causeconjunctivitis, choroiditis, and retinitis (Lewis, 1995: database).
Chronic effects:Chronic inhalation studies on animals resulted in alveolar fibrosis and other cell damage(Elinder et al., 1979c: 442). Excessive inhalation of iron-containing dust can lead to siderosis,which is radiographically similar to silicosis and miliary tuberculosis. Siderosis may be benign,although some cases of pulmonary fibrosis and impaired function were reported amongstwelders and miners. However, other fumes and dusts are usually also present during weldingand mining. It has been shown that iron tends to accumulate in the lungs as a result of chronicexposure (Elinder et al., 1979c: 443).
High dietary intake of absorbable iron amongst South African men has been associated withexcessive haemosiderin deposits in the liver and an increased incidence of cirrhosis of the liver.Excess haemosiderin deposited in the pancreas may be associated with fibrosis and diabetesmellitus (Elinder et al., 1979c: 444; Nieminen & Lemasters, 1996: 895). For these reasons ironoxide dust should not be considered in the same category as nuisance dusts.

68
Table 3.3.4.12Iron: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Iron oxide fume (as Fe)Not a human carcinogen
Iron salts as (Fe)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Fe, FeS, Fe2S3, FeO, Fe2O3, Fe3O4, Fe(CN)63-, FeCr, FeCr3, FeSi, FeMn, FeTi, FeTiO3,FeB, carbide FeSO4, Fe carbides
Absorption: Ingestion, inhalation Deposition: Liver, spleen, bone marrow Excretion: Slow. Faeces, urine
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver Storage, redistribution Storage, cirrhosis, haemosiderosis
Gastrointestinal tract
Respiratory tract Animals : coughing, nasal irritation Pulmonary fibrosis, lung cancer
Haematopoietic system Storage Storage
Bone Storage(marrow)
Endocrine system Diabetis(severe intoxication)
Muscle
Eye Conjunctivitis, choroiditis, retinitis
Skin Discolouration
Cardiovascular system Heart (haemosiderosis)(severe intoxication)
Immune system
Reproductive system

69
Carcinogenicity:Some iron compounds are suspected carcinogens, amongst them iron dust and red iron oxide(Lewis, 1995: database; Elinder, 1979: 445). IARC has not classified these compounds ascarcinogens (Lewis 1995: database), and epidemiological data are not available to support anysuggestion of carcinogenicity. Based on animal experiments it is suspected that iron oxide dustmight serve as a cocarcinogenic substance, i.e. enhancing the development of cancer at asimultaneous exposure to a carcinogenic substance (Elinder, 1979: 435).
Reproductive effects:No conclusive evidence is available to show reproductive effects associated with excess bodyburdens of iron (Keen, 1996: 988).
3.3.4.13 Lead (Pb)Absorption:Lead is absorbed more readily from the lungs than from the gastrointestinal tract and symptomstend to develop sooner (Lewis, 1995: database).
Deposition and absorption of inhaled particles depends on the physicochemical properties(size, solubility, concentration) (Gerhardsson & Skerfving, 1996: 87; Hrudey, Chen, Rousseaux,1996: 136). About ten to 60 per cent of inhaled lead particles in the size range 0,01 to 5 µm isdeposited in the lungs. Larger particles are deposited in the upper airways where the majorpart is cleared and swallowed (Gerhardsson et al., 1996: 87). No evidence could be found toshow that inhaled lead accumulates in the lungs (Tsuchiya, 1979: 457).
Absorption of ingested lead is dependent on biological factors (age, sex, iron store, nutritionalstatus) and can consequently vary widely between individuals (Lauwerys, 1993: 56;Gerhardsson et al., 1996: 87; Hrudey et al., 1996: 137). The major portion of ingested lead ispassed through the gastrointestinal tract unabsorbed. The absorbed portion (about 4 to 13 percent) enters the entero-hepatic cycle and some of this material is eventually excreted in thefaeces (Tsuchiya, 1979: 458, 459; Hrudey et al., 1996: 137).
Some compounds and finely powdered metal can be absorbed through the skin (Lauwerys etal., 1993: 56; Hrudey et al., 1996: 138).
More-detailed information on the bioavailability of lead compounds is available in the citedliterature (Hrudey et al., 1996: 140 - 143).
Distribution:Absorbed lead is distributed to three biological compartments:• Blood (mainly bound to red cells), half-life about 1 month. (Hrudey et al., 1996: 135;
Lauwerys, 1993: 56).• Soft tissues (brain, kidney, lungs, liver, heart, spleen) Half-life about 19 to 40 days
(Tsuchiya, 1979: 460; Lauwerys, 1993: 56)• Bone which contains about 90 per cent of the total body burden (half-life about 10 to 30
years) (Hrudey et al., 1996: 136; Lauwerys et al., 1993: 56).
Excretion:Excretion of absorbed lead takes place mainly via the kidneys. Lesser pathways includegastrointestinal secretions, hair, nails and sweat. Lead concentrations in the bile are high, anda large proportion is probably reabsorbed in the gut and excreted in the urine (Lauwerys et al.,1993: 56).

70
Table 3.3.4.13Lead: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Possible human carcinogenIARC Group 2b
Lead, elemental andinorganic compounds(as Pb)Lead chromate, Leadarsenate
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Pb, PbO, PbS, PbSO4, PbCO3, PbCl2, Pb(NO3)2, Pb(CN)2, phosphates
Absorption: Inhalation, ingestion, skin Deposition: Bone; soft tissue, blood Excretion: Mainly urine
Target organ Short-term effects Long-term effects
Renal System Reversible damage Kidney disease
Nervous System Brain (accumulation, damage), impaired peripheral function
Liver Interim storage, disturbed function
Gastrointestinal Tract Dyspepsia, constipation, anorexia, colic Gastritis, anorexia
Respiratory tract Absorption Interim storage
Hematopoietic System Anaemia,
Bone Deposition, build-up, sore joints
Endocrine System
Muscle Pain
Eye
Skin Absorption
Cardiovascular system Raised blood pressure
Immune system Impairment
Reproductive system Placental transfer, developmental defects, decreased male fertility, stillbirth,miscarriage
71
Acute effects:Acute intoxication is usually accompanied initially by anorexia, dyspepsia, constipation followedby gastrointestinal colic accompanied by paleness and possibly elevated blood pressure.
Neurological symptoms have been noted (Tsuchiya, 1979: 458, 465), and reversible kidneydamage may also occur (Gerhardsson et al., 1996: 88).
Chronic effects:Chronic lead exposure is manifested by a whole range of possible symptoms and effects, e.g.anaemia, kidney diseases, brain damage, high systolic blood pressure (middle-aged men),reproductive abnormalities, developmental defects, anorexia, feelings of unwellness,sleeplesness, headache, irritability, muscle and joint pains, central and peripheral nervousdisturbances, muscle weakness, gastritis and liver changes, abnormal vitamin D metabolismand even death in severe cases (Lewis, 1995: database; Gerhardsson et al., 1996: 88 – 89;Tsuchiya, 1979: 466 - 473). There is also evidence for lead-related cognitive and behaviouraldisturbances (Gerhardsson et al., 1996: 89).
Heavy chronic exposure is often accompanied by a dark lead line on the edges of the gums(Gerhardsson et al., 1996: 88).
Carcinogenicity:Lead and inorganic lead compounds are classified as possible human carcinogens, Group 2B(IARC, 1987: Vol. 23, Suppl. 7). There is no conclusive evidence for mutagenic activity(Cohen, Bowser, Costa, 1996: 261-262).
Reproductive effects:Severe intoxication can cause sterility (male), abortion and increased mortality and morbidityamongst the newborn. A good correlation was found between lead levels in the blood of themother and newborn.
3.3.4.14 Manganese (Mn)Absorption:The solubility of most industrial manganese products is low. Only particles small enough toreach the alveoli are therefore likely to be absorbed from the lungs. Large particles will becleared from the respiratory tract to the digestive system (Inoue & Makita, 1996: 416). Afterabsorption, most manganese seems to be present in the blood as a Mn3+-transferrin complex(Romero, Abbott, Bradbury, 1996: 567).
Absorption of ingested manganese is homeostatically controlled and is normally about 3 percent. It is reduced by simultaneous intake of calcium (Piscator, 1979b: 488) and increased byiron deficiency (Gerhardsson et al., 1996: 101).
Retention half-life for inhaled manganese in the lungs is 2 - 3 months (Gerhardsson et al.,1996: 101). Fairly high absorption from the lungs has been inferred: 40 to 70 per cent of inhaledisotopically labelled manganese was excreted in the faeces of two groups of exposed persons(Piscator, 1979b: 488).
Distribution:After inhalation or ingestion absorbed manganese is quickly eliminated from the blood. It isdistributed to mainly the liver, and to a lesser extent the kidneys and endocrine glands(Piscator, 1979b: 489; Inoue et al., 1996: 416).

72
Table 3.3.4.14Manganese: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Fume (as Mn)Not a human carcinogen
Mn and compounds (as Mn)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Mn, MnO, MnO2, Mn3O4, MnS, MnP, MnCO3, Mn(OH)2, MnSO4, carbides, silicides, phosphates
Absorption: Ingestion, inhalation Deposition: Liver, kidneys, intestine; brain, bone, endocrine system Excretion: Bile (faeces)
Target organ Short-term effects Long-term effects
Renal system
Nervous systemBrain critical organ. Storage (brain, long-term); irreversible Parkinson’s- likedegeneration; motor disturbance, speech disturbance, hallucinations, illusions,delusions
Liver Storage (20%)
Gastrointestinal tract Storage (intestine)
Respiratory tract Increased infections, pneumonia
Haematopoietic system
Bone Storage (45%)
Endocrine system
Muscle Storage (35%); weakness
Eye Irritant
Skin Irritant
Cardiovascular system
Immune system
Reproductive system Crosses placental barrier

73
Animal experiments have shown that minor amounts are taken up in the central nervoussystem. Rate of manganese uptake into the brain is thought to be determined by speciationand transport mechanism, Mn2+ crossing the blood-brain barrier rapidly, and the Mn3+-transferrin complex crossing it slowly. The distribution of manganese species in the blood isnot known (Romero et al., 1996: 567).
Excretion:Absorbed manganese is excreted almost exclusively in the bile and passed with the faeces(Inoue et al., 1996: 416).
Acute effects:IngestionVery few poisonings have occurred by ingestion (Lewis, 1995: database).
RespiratoryManganese pneumonia is associated with acute alveolar inflammation, shortness of breath andoften does not respond to antibiotics. An increase in bronchitis has also been found. Nopermanent pulmonary changes have been reported. Increased susceptibility to respiratoryinfections was also found in animals (Piscator, 1979b: 493).
The following dose-response relationships have been reported:• 0,39 to 16,35 mg/m3: Increased pneumonia, bronchitis (Piscator, 1979b: 493; Lewis, 1995:
database).• 6,7 mg/m3 (average): Nose and throat symptoms have been observed (Piscator, 1979b:
494).• Less than 0,3 mg/m3: No pulmonary symptoms (WHO guideline (1979)) (Piscator, 1979b:
495).
Manganese is a skin and eye irritant (Lewis, 1995: database).
Chronic effects:Chronic effects have been documented for both ingestion and inhalation exposure (8 to 16years). Time of onset can vary from a few months to (usually) 1 to 3 years after exposure. Cases of unusual sensitivity towards manganese have been reported (Piscator, 1979b: 497). There is a possibility to reverse the course of intoxication if it is diagnosed early enough, andthe patient is removed from exposure (Lewis, 1995: database).
The brain is the critical organ. Chronic intoxication (manganism) is characterised by initialprogressive psychiatric and neurological symptoms with continued exposure (Piscator, 1979b:497; Inoue et al., 1996: 416). Symptoms are:
• Asthenia; languor; sleepiness.• Incoherent, slow monotonous speech; aggression; staggering walk, weakness in the legs
mask-like face; increased clumsiness. Neurological examination reveals nothing specific,except increased reflexes in lower limbs.
• Disease fully developed: difficult walking and writing; tremors in upper limbs; nocturnalcramps in legs; symptoms resembling Parkinson’s or Wilson’s disease.
The history of exposure is often the only aid to diagnosis.
Carcinogenicity:IARC has not listed manganese as a human carcinogen.

74
Reproductive effects:Deficiency can cause malformation. There are no indications that inhalation or ingestion willcause malformations in man or animals (Piscator, 1979b: 497). Decreased libido or impotenceis a frequent early symptom of manganese intoxication (Inoue et al., 1996: 416). Decreasedmale fertility has been reported (Corbella & Domingo, 1996: 1085).
3.3.4.15 Mercury (Hg)Absorption:Upon exposure the absorption rate depends on particle size and deposition rate in therespiratory tract.
Metallic mercury• Inhalation: Vapour is rapidly and efficiently (about 80 per cent) absorbed from lungs by
diffusion in the alveoli.(Lauwerys & Hoet, 1993: 74; Gerhardsson & Skerfving, 1996: 93).• Ingestion: Liquid metal is poorly absorbed from the gastrointestinal tract and depends on
the exposed surface area (Berlin, 1979: 510).• Skin: Absorption is possible but unimportant in the workplace compared to inhalation.
Vapour emanating from contaminated skin or clothing will be inhaled, forming a much moreefficient pathway (Berlin, 1979: 510).
Inorganic salts• Inhalation: Little quantitative data are available, but in animals the absorption of inorganic
salts of mercury is lower than for the metal vapour (Hrudey, Chen, Rousseaux, 1996:127).• Ingestion: Mercuric salts are corrosive to mucous membranes, and may cause damage
which can increase absorption from the intestine to more than the 10 per cent which hasbeen reported (Berlin, 1979: 516).
• Skin: Absorption is low (Berlin, 1979: 516).
Organo-mercurials• Inhalation: Methyl mercury can be absorbed by inhalation. In animal experiments (rats,
mice) absorption was rapid and almost complete (Berlin, 1979: 519).• Ingestion: Absorption is almost complete in humans (Berlin, 1979: 519).• Skin: Animal experiments showed low absorption (Hrudey, 1996:128).
Distribution:Mercury has a particular affinity for organs with epithelial cells and glands (gastrointestinal tract,kidney, skin, hair, salivary glands, thyroid, liver, pancreas, sweat glands, testicles, prostate). Inthe brain it accumulates in the grey matter, cerebellum and brain stem (Berlin, 1979: 511).
Metallic mercuryCan penetrate the blood-brain barrier and remain in the brain for a long time (half-life about 1year) causing a wide range of neurological and psychic disorders (Hrudey, 1996:126; Berlin,1979: 512; Lewis, 1995: database).
Mercury saltsMercuric mercury (Hg2+) is not easily transported over the blood-brain or the placental barriers.Uptake in and elimination from the various organ systems vary widely (Berlin, 1979: 516). Mostof the body pool, however, is in the kidney (Nieminen & Lemasters, 1996: 890).
Organo-mercurialsMethyl mercury is carried in the blood bound largely to red blood cells and is slowly distributedto the brain and other organs. Some of the bound mercury in the blood can be transformed tomercuric species, which are distributed to the kidneys and liver. Mercury in the bile is subject toentero-hepatic recirculation (Berlin, 1979: 520; Hrudey, 1996: 126).

75
Table 3.3.4.15Mercury: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Mercury alkylsUnclassifiableIARC Group 3 Mercury and compounds
(as Hg)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Hg, HgS, Hg2S, HgO, Hg2O
Absorption: Inhalation, ingestion, skin Deposition: Liver, spleen, kidneys, bone Excretion: Urine
Target organ Short-term effects Long-term effects
Renal system Target organ : necrosis, acute failure (inorganic compounds)
Nervous system CNS critical organ (vapour). Dizziness, tremors, psychicdisturbances, insomnia
Liver
Gastrointestinal tract Salivation, stomatitis, gums (black rim)
Respiratory tract Lung critical organ: bronchitis, pneumonitis, pulmonary insufficiency
Hematopoietic system
Bone
Endocrine system
Muscle
Eye
Skin Irritation
Cardiovascular system Palpitations
Immune system Allergens (inorganic compounds)
Reproductive system Foetal intoxication: Minamata disease, brain damage. Accumulation in testicle and prostate

76
Excretion:Retention time differs widely amongst different organs. The brain, kidneys and testicles havethe longest retention time. These organs are therefore likely to show accumulation on repeatedexposure. Excretion for all forms of mercury is mainly by way of the faeces and urine. Minorpathways are saliva, sweat, breast milk, tears and exhalation of vapour (Berlin, 1979: 516).
Acute effects:The lung is the critical organ in acute accidental exposure to high levels of mercury vapour,showing erosive bronchitis, bronchiolitis and interstitial pneumonitis, eventually terminating indeath due to respiratory insufficiency. Some central nervous system effects such as tremorsand excitability may accompany these symptoms (Lewis 1995: database; Berlin, 1979: 512).
Soluble salts are violently corrosive to skin and mucous membranes (Lewis 1995: database).
Chronic effects:The brain is the primary target organ for chronic mercury vapour exposure. With increasingdose the symptoms of so-called micro-mercurialism appear:
• Weakness, fatigue, anorexia, loss of weight.• Disturbance of gastrointestinal functions.• At higher exposure levels intentional tremors in the fingers, eyelids and lips are seen, which
may develop into tremors of the whole body with violent spasms of the extremities.• Parallel to these symptoms severe behavioural and personality changes take place,
accompanied by excitability, loss of memory, and insomnia.
Severe intoxication can cause hallucination and delirium, changes to the gums and excessivesalivation (Berlin, 1979: 512; Lewis 1995: database; Gerhardsson, 1996: 93).
Kidney damage may occur in cases of exposure to a combination of mercury vapour and dust. Necrosis and acute failure are possible (Berlin, 1979: 518; Gerhardsson, 1996: 93; Fowler,1996f: 723).
Carcinogenicity:IARC has designated mercury and inorganic mercury compounds to Group 3, unclassifiable asto carcinogenicity to humans (IARC, 1993: Vol. 58).
Reproductive effects:Methyl mercury and inhaled metallic mercury can pass the placental barrier, leading to foetaluptake when the mother is exposed. Brain damage and cerebral palsy (Minamata disease)may result (Berlin, 1979: 511; Hamada & Osame, 1996: 337- 351).
Mercury accumulates in the testicles and prostate (Berlin, 1979: 511).
3.3.4.16 Molybdenum (Mo)Absorption:Soluble compounds are readily absorbed after inhalation and ingestion. Animal experimentswith inhalation of MoS2 and hexavalent molybdenum supported this conclusion. No humandata are available (Friberg, 1979: 533).
Molybdenum compounds are poisonous by ingestion. Gastrointestinal absorption of Mo6+ ishigh in both animals and humans (about 50 per cent) (Friberg, 1979: 533).

77
Table 3.3.4.16Molybdenum: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Molybdenum compounds (soluble) (as Mo)Not a human carcinogen
Molybdenum compounds (insoluble) (as Mo)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Mo, MoO, MoO2, MoS2, Mo(SO4)2, carbides, silicides
Absorption: Ingestion, inhalation Deposition: Kidney, liver, bone Excretion: Mainly urine
Target system Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Irritant (MoO3) Pneumoconiosis, fibrosis, “hard metal disease”
Haematopoietic system
Bone Arthritis
Endocrine system
Muscle
Eye
Skin
Cardiovascular system
Immune system
Reproductive system

78
Distribution:Animal studies showed distribution of ingested MoO3 in the liver, pancreas, kidneys and bones(Friberg, 1979: 534). No data for humans are available.
Excretion:Limited data are available. Animal studies indicate low retention. Two studies with humansindicated that urine is the main route for excretion. Molybdenum is rapidly excreted, showing abiological half-life about 10 days (Friberg, 1979: 534; Lewis, 1995: database).
Acute effects:Acute oral poisoning caused severe gastrointestinal irritation with diarrhoea, coma and deaththrough heart failure (animal experiments) (Lewis, 1995: database).
Precautions are advised against inhalation of the more-soluble compounds like MoO3 andNaMoO4. MoO3 is a powerful irritant causing pulmonary fibrosis and coughing in humans(Lewis, 1995: database; Friberg, 1979: 535).
Chronic effects:High dietary exposure to molybdenum has been seen to increase the incidence of arthritis-likecomplaints and elevated uric acid levels in the blood (Friberg, 1979: 536).
Workers exposed to Mo and MoO3 dust (one to 19 mg Mo/m3) for 3 to 7 years have developedpneumoconiosis. Inhalation of Mo-containing alloy or carbide dust can lead to ”hard metaldisease” (Lewis, 1995: database; Friberg, 1979: 535).
Carcinogenicity:IARC does not classify molybdenum or its compounds as human carcinogens
Reproductive effects:No information is available for humans. Some unspecified effects were noticed (Lewis 1995:database).
3.3.4.17 Nickel (Ni)Absorption:Nickel is not a cumulative toxin (Lauwerys & Hoet, 1993: 82).
InhalationAbout 25 per cent of nickel in particulate matter deposited in the lungs after inhalation isabsorbed (Gerhardsson et al., 1996: 102). Insoluble species are retained in the lung for longperiods, causing associated elevated levels of nickel in the system (Lauwerys, 1993: 84). Soluble species are absorbed and excreted fairly quickly (Lauwerys, 1993: 82).
IngestionGastrointestinal absorption is low (one per cent) and strongly influenced by dietary constituents.Unabsorbed material is excreted in the faeces (Lauwerys, 1993: 82; Gerhardsson et al., 1996:102).
SkinSoluble compounds can penetrate the skin during contact. (Norseth et al., 1979: 549).

79
Table 3.3.4.17Nickel: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Nickel
Inorganic: Soluble compounds
Nickel compounds : Human carcinogensIARC Group 1.Nickel & alloys: Possible humancarcinogensIARC Group 2B Inorganic: Insoluble compounds
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Ni, NiO, Ni(CN)2, Ni(CN)4, NiS, Ni3S2 NiSO4, Ni(NO3)2, NiF2, Ni(OH)2
Absorption: Inhalation, skin, ingestion Deposition: Bone, kidney, liver, lung Excretion: Urine, saliva, sweat; faeces (ingestion)
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Asthma Nasopharingeal cancer, lung cancer, nasal ulceration, asthma, pneumoconiosis
Haematopoietic system
Bone Storage
Endocrine system
Muscle
Eye Conjunctivitis
Skin Irritant, contact dermatitis, eczema Sensitiser, dermatitis
Cardiovascular system
Immune system Sensitiser, experimental immune effects
Reproductive system

80
Distribution:Nickel is bound mainly to albumin and amino acids in the blood stream before being depositedin the bone (the highest concentration), kidney, liver, and lungs. Biological half-life in blood isabout 20 to 34 hours and in urine about 17 to 39 hours (Gerhardsson et al., 1996: 102;Lauwerys, 1993: 82).
Excretion:Urine is the dominant excretion route for absorbed nickel. The predominant fraction of ingestednickel is excreted, unabsorbed, in the faeces (Gerhardsson et al., 1996: 102).
Acute effects:Hypersensitivity to nickel is common, and asthma, dermatitis and conjunctivitis have been notedamongst sensitive workers exposed to mists of soluble Ni compounds in the plating industry(Benson & Zelikoff, 1996: 932; Norseth et al., 1979: 549; Lewis, 1995: database). It was shownto have an adverse effect on the immune system of experimental animals (Zelikoff &Smialowicz, 1996: 816, 821).
Chronic effects:Little data are available on systemic effects of long-term exposure in humans. The criticalorgans for chronic exposure are the upper respiratory tract (nose), skin, and immune system(Gerhardsson et al.,1996: 102).
Soluble salts like nickel sulphate are strong irritants and in nickel refineries and plating plantswhere mists are formed, sinusitis, rhinitis, perforation of the nasal septum and bronchial asthmahave been observed (Lewis, 1995: database; Norseth et al., 1979: 549).
Nickel and its compounds are strong skin sensitisers and are responsible for a significantnumber of eczema-like conditions (Kimber & Basketter, 1996: 827).
Carcinogenicity:Nickel compounds are classified Group 1 carcinogens (IARC, 1990: Vol. 49). Nickel metal andalloys are classified as Group 2B carcinogens (IARC, 1990: Vol. 49).
Long-term exposure to soluble (NiSO4) and insoluble (Ni3S2, NiO) compounds leads to a highrisk of nasal and pulmonary malignancy and an increased risk for liver cancer (Gerhardsson etal., 1996: 102; Costa, 1996: 246). Nickel iron sulfide matte contains a high concentration ofcrystalline nickel subsulphide. This is a potent carcinogen, which has reportedly caused a highincidence of nasal and pharyngeal cancers amongst persons employed in crushing operationswhere they were exposed to crusher dusts. During comparative experiments amorphous nickelsubsulphide (Ni3S2) did not exhibit carcinogenic properties. Black, low-calcined NiO is alsoconsidered to be a potent carcinogen (Costa, 1996: 247).
Reproductive effects:Although an increase in birth defects was noted in animal experiments, there are no reports ofsimilar effects in humans.
3.3.4.18 Osmium (Os)Absorption:The effects of osmium tetroxide relate to local irritation, with systemic effects through inhalationand ingestion.
Distribution:No data available.

81
Table 3.3.4.18Osmium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen Osmium tetraoxide (OsO4) (as Os)Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Os, OsO4, OsF6
Absorption: Inhalation, ingestion, skin Deposition: No data Excretion: No data
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Corrosive, irritant; asthma Bronchitis
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Corrosive, irritant; lacrymation
Skin Corrosive, irritant; dermatitis, ulceration Dermatitis, ulceration
Cardiovascular system
Immune system
Reproductive system

82
Excretion:No data available.
Acute effects:Os metal is not highly toxic, and most data on osmium toxicity relate to osmium tetroxide. It isan eye and mucous membrane irritant, causing asthmatic symptoms upon inhalation, anddermatitis and ulceration upon skin contact. Persons with pre-existing skin disorders orimpaired respiratory function may be more susceptible to the effects of osmium tetroxide.
OsO4 has a nauseating odour as warning of possible toxic concentrations in the air. It ispoisonous by ingestion and inhalation. Pulmonary oedema and unspecified systemic effectshave been noted after inhalation. The oxide is an irritant causing lacrimation and other eyeeffects, and structural and functional changes in the trachea and bronchi (HHMI, 2000).
OsF6 is highly poisonous and a very corrosive irritant to eyes, skin and mucous membranes.
Chronic effects:Long term exposure from inhalation to osmium tetroxide can cause chronic coughs, bronchopneumonia, sterile lung abscess and gangrene. Prolonged exposure can result in damage tothe cornea, blindness, disturbances of the digestive system and inflammatory disorders of thelungs and kidneys (HHMI, 2000).
Carcinogenicity:Osmium and its compounds have not been listed for carcinogenic effects.
Reproductive effects:Experimental reproductive effects have been noted, but no actual cases have beendocumented (Lewis, 1995: database).
3.3.4.19 Platinum (Pt)Absorption:Respiratory and dermal absorption are the primary occupational concerns. It has beenhypothesised that platinum interferes with the antigen recognition step of the immune responsesystem (Kusaka, 1993: 75-87).
Distribution:Distribution data are available only for cisplatin (Van der Voet & de Wolff, 1996: 459). It hasbeen noted that exposure to platinum leads to a relative lymphocytosis.
Excretion:No data describing excretion of platinum are available. Removal from platinum salt exposureresults in almost immediate relief of asthma (see below). The dermatitis may be persistent, butusually clears in a few days (see below).
Acute effects:Pt metal is relatively non-toxic in its pure form (Van der Voet et al., 1996: 459). Exposure tocomplex platinum salts has been shown to cause symptoms of irritation in the eyes, nose andthroat. (Lewis, 1995: database). Toxic effects have however not been indicated fornonsensitised individuals (see below).
Chronic effects:Platinum salts (mainly the ionic platinum chloro compounds) are sensitisers upon chronicexposure causing allergies like rhinitis, conjunctivitis, asthma, urticaria and contact dermatitis(Lewis, 1995: database). The respiratory reaction starts with sneezing and a runny nose. Theeffects may be followed by chest tightness, shortness of breath, blue discolouration of the

83
Table 3.3.4.19Platinum: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Platinum metal (as Pt)Not a human carcinogen
Platinum salts (soluble) (as Pt)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Pt, sulphides, sulphates, chlorides, oxide
Absorption: Unknown Deposition: Unknown Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract Poisonous
Respiratory tract Irritant.; sensitiser Rhinitis, asthma
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Irritant; sensitiser Conjunctivitis
Skin Irritant; sensitiser Dermatitis, urticaria
Cardiovascular system
Immune system
Reproductive system Experimental data

84
skin, and wheezing. The skin shows an itchy red rash. Symptoms become progressivelyworse with the length of employment. Some workers may show several allergic manifestationswith the involvement of the nasal mucosa, bronchi and the skin. Persons with a history ofasthma, allergies, or known sensitisation to platinum salts would be expected to be at increasedrisk from exposure.
Carcinogenicity:Cisplatin (cis-Pt(NH3)2Cl2) is a probable human carcinogen (Group 2a) (IARC, 1987: Vol. 26,Suppl. 7), but platinum and its inorganic salts have not been listed by IARC as carcinogens.Tetrachloroplatinates are mutagens (Lewis, 1995: database).
Reproductive effects:Reproductive effects have not been identified.
3.3.4.20 Rhodium (Rh)Absorption:Rhodium is one of the rarest elements in the earth’s crust, and is found in small quantitiesassociated with platinum and some copper-nickel ores. Because of its rarity of occurrence, littleis known about its toxicology.
Distribution:No data available.
Excretion:No data available.
Acute effects:Most rhodium compounds are only moderately toxic by ingestion (Lewis, 1995: database).
Chronic effects:Rhodium may be a sensitiser, but not necessarily to the same extent as platinum. The ability ofsoluble salts of rhodium to lead to allergic reactions in human has not been adequatelydemonstrated. Occupational exposure limits have been set for rhodium and its salts, based onanalogy with platinum.
Carcinogenicity:Rhodium has not been listed as a carcinogen.
Reproductive effects:Experimental reproductive effects have been noted (Lewis 1995: database), but no actualoccurrence has been documented.

85
Table 3.3.4.20Rhodium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Rhodium metal (as Rh)Not a human carcinogen
Rhodium salts (as Rh)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants:: Not identified
Absorption: No data available Deposition: No data available Excretion: No data available
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract Poisonous
Respiratory tract Sensitiser
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Sensitiser
Skin Sensitiser
Cardiovascular system
Immune system
Reproductive system Experimental effects

86
3.3.4.21 Selenium (Se)Absorption:There is a lack of quantitative data for absorption due to inhalation. Soluble salts are efficientlyabsorbed after ingestion (about 80 per cent). Selenium metabolism may be strongly influencedby dietary and other factors (Glover, Levander, Parizek, Vouk, 1979a: 555), and there does notappear to be any homeostatic control (Lauwerys & Hoet, 1993: 86).
Distribution:Absorbed selenium is distributed mainly to the liver and kidneys (animal studies) (Glover et al.,1979a: 560), but the major portion of the total body burden is stored in the muscle (Lauwerys etal., 1993: 86).
Excretion:Urine excretion is the main route for elimination (Lauwerys et al., 1993: 86). The process canbe described with a three-phasic model, with biological half-times of 24 hours (90 per centexcretion), 103 days and 234 days (Glover et al., 1979a: 562).
Some selenium is excreted through the lungs as volatile compounds, giving rise to acharacteristic garlic odour, which disappears after a few days (Glover et al., 1979a: 568).
Acute effects:Inhalation of selenium dust or fumes can cause serious irritation of the respiratory tract (Lewis,1995: database). On contact, SeO2 can cause pulmonary oedema (sudden large exposure),irritation or burns of the eyes, and skin rashes. Rhinitis, nosebleeds, headache, anorexia,irritability and nervous disturbances have also been reported (Glover et al., 1979a: 568).
Chronic effects:Most of the chronic intoxication cases in humans are described for excessive dietary seleniumintake (Lewis, 1995: database; Glover et al., 1979a: 569). Some of the symptoms are commonto those for occupational exposure (Glover et al., 1979a: 568).
Occupational inhalation exposure can cause a wide range of non-specific symptoms:Irritation of the eyes, nose and throat, gastro-intestinal disturbances, increased bodytemperature, headaches and tiredness, irritability, unstable blood pressure, metallic taste,yellowish skin coloration (Glover et al., 1979a: 568).
At high levels of exposure breath and sweat can assume a garlicky odour due to the excretionof volatile dimethyl selenide. The odour disappears after seven to ten days (Glover et al.,1979a: 568).
Carcinogenicity:There is conflicting epidemiological evidence regarding the role of selenium in carcinogenesis(Cohen, Bowser, Costa, 1996:264 – 265; Poirer & Littlefield, 1996: 292). IARC (1987) hasdetermined that there is inadequate evidence for evaluation and classified selenium and itscompounds as Group 3 substances (IARC, 1987: Vol. 9, Suppl. 7).
Reproductive effects:Although some old observations about miscarriages and birth defects amongst women exposedto selenite powder, this could not later be verified (Keen, 1996: 990).
Other effects:There is experimental evidence that selenium exerts immunological effects (Sharma & Dugyala,1996: 792).

87
Table 3.3.4.21Selenium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
UnclassifiableIARC Group 3
Se and compounds(except H2Se) (as Se)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: Se, sulphides, chlorides, sulphate.
Absorption: Inhalation, ingestion Deposition: Muscle, kidneys, liver, heart Excretion: Two phase. Urine (rapid), faeces, lungs
Taregt organ Short-term effects Long-term effects
Renal system Storage Storage
Nervous system Hyperreflexia, peripheral anaesthesia
Liver Storage Storage
Gastrointestinal tract Nausea, vomiting Indigestion, intestinal disturbances
Respiratory tract Irritant (H2Se), pulmonary oedema (SeO2)
Haematopoietic system Lymphocytosis
Bone
Endocrine system
Muscle Major storage
Eye Irritant
Skin Dermatitis SeO2 : dermatitis, burns, body rash; yellowish skin colour, brittle hair
Cardiovascular system Unstable blood pressure; storage (heart)
Immune system Experimental effects
Reproductive system Women: irregular menses, menostasis

88
3.3.4.22 Silver (Ag)Absorption:No data are available for the deposition rate of inhaled material in humans. Little is knownabout absorption rate, either from the lungs or gastrointestinal tract (Fowler & Nordberg, 1979d:581; Lauwerys & Hoet, 1993: 90). The absorption half-life in the human lung has beenestimated at about 1 day (Fowler et al., 1979d: 582).
In animals, gastrointestinal absorption is low (less than 10 per cent) (Fowler et al., 1979d: 581).
Silver nitrate solution (0,5 per cent) has been extensively used as burn treatment. No evidencehas been found for local or systemic toxicity (Fowler et al., 1979d: 583).
Distribution:Silver is widely distributed in the body. After accidental inhalation of radioactive silver in onecase, about half the body burden was found in the liver after 16 days. It has also been found inthe walls of blood vessels, testes, pituitary, kidneys, mucous membranes and choroid plexus inthe brain (Lewis, 1995: database). In a single reported case, the liver was the main depositionsite, followed by the skin (Fowler et al., 1979d: 582).
Excretion:Excretion of absorbed silver is largely in faeces via the bile (animal studies). Based on limitedinformation, the half-life in human liver has been estimated at 48 to 52 days (Fowler et al.,1979d: 582).
Acute effects:Soluble compounds (especially AgNO3) are corrosive and irritating to skin, eyes and mucousmembranes and may cause death if ingested (Lewis, 1995: database).
Exposure to fine metallic particles causes local pigmentation in broken skin (Lewis, 1995:database).
Chronic effects:Long term inhalation of dusts (two to 25 years) at about one mg Ag/m3 can cause argyrosis, agrey pigmentation of the skin and mucous membranes. The conjunctivae of the eyes show thefirst signs, followed by the mucous membranes of the mouth and skin. The condition developsslowly and shows no systemic symptoms or physical disability. The pigmentation is permanent(Lewis, 1995: database). Argyria may also affect organs such as the cornea and lens of theeye. Reports of systemic effects such as chronic bronchitis and abdominal discomfort have notbeen sufficiently evaluated, and silver is therefore not necessarily the causal factor (Fowler etal., 1979d: 584). In more recent literature argyria is not considered to cause any systemicsymptoms or physical disability (Lewis, 1995: database).
Carcinogenicity:IARC has not classified silver or its compounds as carcinogens.
Reproductive effects:Reproductive effects have not been identified.

89
Table 3.3.4.22Silver: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
SilverNot a human carcinogen
Silver compounds (as Ag)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: Ag, AgCN, AgS
Absorption: Inhalation, ingestion, skin Deposition: Skin, mucous membranes, internal organs, blood vessels Excretion: Bile (faeces)
Target organ Short-term effects Long-term effects
Renal system Deposition (argyria)
Nervous system
Liver Storage, clearance via bile
Gastrointestinal tract Argyria (mouth, gums)
Respiratory tract Absorption Argyria (nose, trachea, bronchi)
Haematopoietic system
Bone
Endocrine system Argyria (pituitary)
Muscle
Eye Irritation Argyria (conjunctivae, cornea, lens)
Skin Irritation Deposition (argyria)
Cardiovascular system Deposition (argyria)
Immune system
Reproductive system Argyria (testes)

90
3.3.4.23 Tantalum (Ta)Absorption:Ingested salts of tantalum are poorly absorbed, but no information is available on absorptionfrom inhalation or dermal exposure.
Distribution:After intramuscular injection the liver, bone, and kidney were shown to contain high levels oftantalum (Doull, Klaassen & Amdur, 1980: 457).
Excretion:Pathways of excretion are not known.
Acute effects:Tantalum has a low order of toxicity but has produced transient inflammatory lesions in thelungs of animals. Intratracheal administration of tantalum oxide to guinea pigs producedtransient bronchitis, interstitial pneumonitis, and hyperemia (ASOSH, 2000). Some industrialskin injuries from tantalum have been reported. TaCl5 is moderately toxic when ingested(Lewis, 1995: database).
Chronic effects:Industrial systemic poisoning is unknown (Lewis, 1995: database). Implantation of tanatlumhas not shown any adverse tissue effects in either humans or animals (Doull, Klaassen &Amdur, 1980: 445).
Carcinogenicity:IARC has not classified tantalum or its compounds as carcinogenic.
Reproductive:Reproductive effects have not been documented in animals or humans.
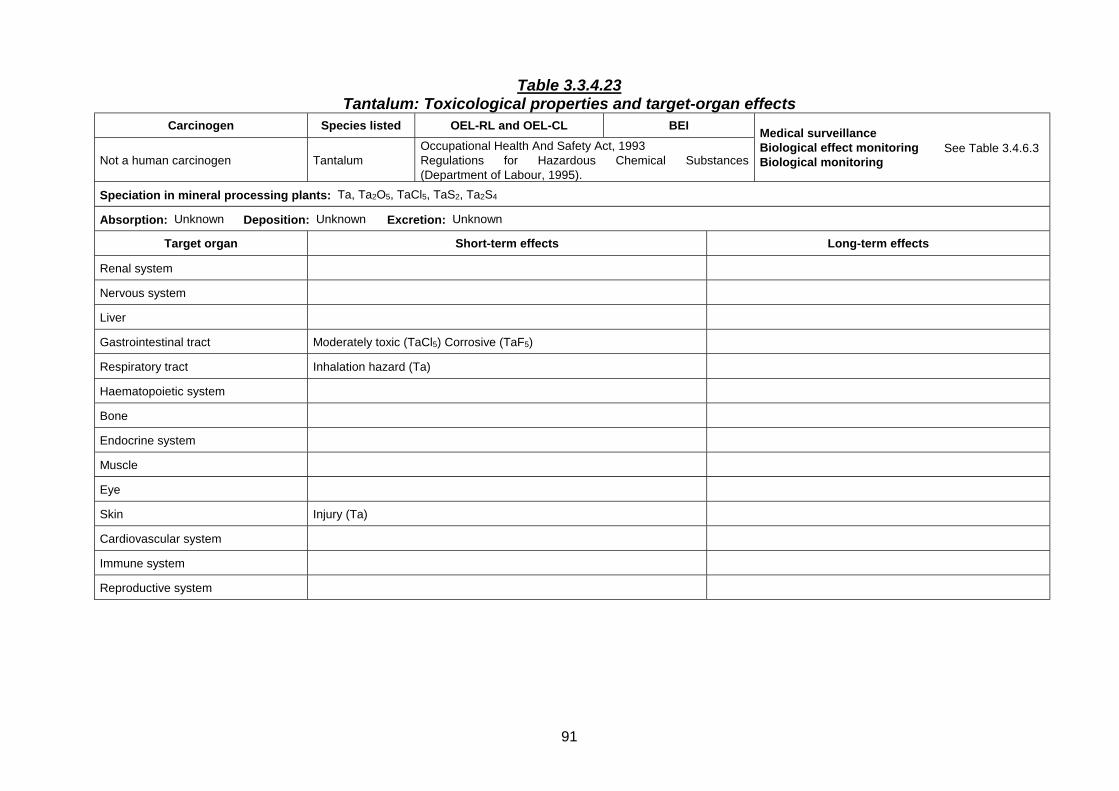
91
Table 3.3.4.23Tantalum: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen TantalumOccupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Ta, Ta2O5, TaCl5, TaS2, Ta2S4
Absorption: Unknown Deposition: Unknown Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract Moderately toxic (TaCl5) Corrosive (TaF5)
Respiratory tract Inhalation hazard (Ta)
Haematopoietic system
Bone
Endocrine system
Muscle
Eye
Skin Injury (Ta)
Cardiovascular system
Immune system
Reproductive system

92
3.3.4.24 Tellurium (Te)Absorption:Tellurium is associated with copper and lead production and is mostly used in metallurgicalapplications and exposure to other metals (Pb, Zn, As, Se, Cd, Tl) as co-factors should beconsidered. Inhalation is the main occupational exposure route (Glover & Vouk, 1979b: 587).Absorption in humans has not been quantifiable with the available information. In animalstudies estimates for gastrointestinal absorption vary from ten to 15 per cent to 25 per cent. Some tellurium compounds can be absorbed through the skin to a great enough extent tocause garlic breath (Glover et al., 1979b: 590; Lauwerys & Hoet, 1993: 91 - 92).
Distribution:The highest concentrations of tellurium are found in the blood, liver, kidneys, lungs, thyroid andspleen, but long-term accumulation takes place in bone (Glover et al., 1979b: 590).
Excretion:Excretion is partly through urine, the faeces and lungs (as dimethyl telluride) (Lauwerys et al.,1993: 92) with a whole-body half time estimated at about 3 weeks (Glover et al., 1979b: 591).
Acute effects:IngestionNausea, vomiting, tremors, convulsions, respiratory arrest, central nervous system depression,garlic odour to breath (Lewis, 1995: database).
InhalationAerosols of Te, TeO2, H2Te cause respiratory irritation, sometimes leading to bronchitis andpneumonia. Heavy exposure can lead to headache, drowsiness anorexia, metallic taste,nausea, tremors, convulsions and respiratory arrest (Lewis, 1995: database; Glover et al.,1979b: 594).
DermalSkin irritation can occur upon direct contact in the form of burns or rashes (Glover et al., 1979b:590). Evidence for skin effects upon occupational exposure to dusts and vapours of TeO2 isnot considered conclusive (Glover et al., 1979b: 592).
Chronic effects:Tellurium tends to accumulate in the choroid plexus in the brain (Zheng, 1996: 618). The metalhas relatively low toxicity. It is converted in the body to dimethyl telluride, which gives a garlickyodour to the urine, breath and sweat. Foundry workers exposed to less than 0,1 mg Te/m3
developed the typical garlicky odour, anorexia, nausea, depression, sleepiness, itchy skin andmetallic taste (Lewis, 1995: database; Glover et al., 1979b: 594).
Carcinogenicity:IARC has not listed tellurium or its compounds as carcinogenic.
Reproductive effects:Tellurium is an experimental teratogen (rats) causing hydrocephalus (Glover et al., 1979b: 594),but no manifestation of this nature has been observed in humans.

93
Table 3.3.4.24Tellurium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen Te and compounds (except H2Te) as (Te)Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Te, TeS, TeSO4, TeCl4
Absorption: Inhalation, ingestion, skin Deposition: Liver, kidneys, lungs, thyroid, spleen Excretion: Urine, faeces, lungs
Target organ Short-term effects Long-term effects
Renal system
Nervous system Tremors, convulsions, CNS depression, headache Accumulation (choroid plexus)
Liver
Gastrointestinal tract Anorexia, nausea, vomiting, metallic taste, Anorexia, nausea, vomiting, metallic taste
Respiratory tract Respiratory irritation, bronchitis, pneumonia, respiratory arrest Garlicky breath
Haematopoietic system
Bone Accumulation
Endocrine system
Muscle
Eye
Skin Irritation, burns, rashes Pruritis
Cardiovascular system
Immune system
Reproductive system

94
3.3.4.25 Thallium (Tl)Absorption:Absorption of soluble salts of thallium from the gastrointestinal tract and respiratory system israpid and almost complete (Kazantzis, 1979b: 602).
Distribution:Absorbed thallium is widely distributed in the human body. The highest concentration afterexposure is usually found in the kidneys (Kazantzis, 1979b: 603). It is also distributed to theheart, brain, skin, liver, bones and brain (Van der Voet & de Wolff, 1996: 457).
Excretion:Excretion is mainly via urine and faeces (Kazantzis, 1979b: 603).
Acute effects:Acute poisoning is manifested in gastrointestinal disturbance (gastro-enteritis, nausea,vomiting, abdominal pain), muscular pain, collapse, peripheral neuropathy, psychologicalchanges (confusion, delirium, fear, lethargy) cardiovascular involvement (tachycardia,hypertension, dysrythmia), respiratory and circulatory collapse, and death.
Survival for more than one week after acute poisoning is characterised by headache, ataxia,tremor, paresthesia, and muscular atrophy. For survival after two to three weeks, hair loss; andmental disturbances (psychosis, paranoia, and hallucinations) occur. Recovery may becomplete or partial, with remaining mental abnormality, ataxia, and tremors (Kazantzis, 1979b:606; Van der Voet et al., 1996: 457).
The lethal dose by ingestion is 0,2 to 1,0 grams of absorbed thallium (Van der Voet et al., 1996:456). The effects are cumulative and with continuous exposure intoxication appears at muchlower levels (Lewis, 1995: database).
Chronic effects:Occupational exposure is usually long-term and at lower levels than for acute intoxication. Effects such as discoloration and loss of hair (alopecia), white bands in nails, skin atrophy,fatigue, anorexia, pains in the legs, visual disturbances (optic neuritis), albuminuria, blooddisturbances, and polyneuropathy have been reported (Kazantzis, 1979b: 608; Lewis, 1995:database; Van der Voet et al., 1996: 456).
Carcinogenicity:IARC does not classify thallium as a carcinogen.
Reproductive effects:Thallium can cross the placental barrier (Van der Voet et al., 1996: 457), and the reproductiveorgans and foetus are highly susceptible to harm (Lewis, 1995: database).

95
Table 3.3.4.25Thallium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen Thallium (soluble compounds) (as Tl)Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: TlO2
Absorption: Rapid by ingestion and inhalation; skin Deposition: Hair, kidneys Excretion: Urine (initial); faeces (long term)
Target organ Short-term effects Long-term effects
Renal system Initial concentration Albuminuria
Nervous system Polyneuropathy, headache, ataxia Polyneuropathy, mental abnormality, ataxia
Liver
Gastrointestinal tract Gastro-enteritis, nausea, vomiting, pain Anorexia
Respiratory tract Respiratory collapse
Hematopoietic system Eosinophilia, lymphcytosis
Bone
Endocrine system
Muscle Pain Pain, atrophy, tremors
Eye Optic neuritis
Skin Absorption Discoloration and loss of hair; atrophy
Cardiovascular system Tachycardia, hypertension, dysrythmia
Immune system
Reproductive system Can cross placental barrier Foetal susceptibility, experimental teratogen

96
3.3.4.26 Tin (Sn)Absorption:Absorption of ingested inorganic and metallic tin is low (Lewis, 1995: database). Animalexperiments have shown a tendency of Sn2+ to be absorbed more readily than Sn4+ (Piscator,1979c: 616).
Organotin compounds are highly toxic (especially triethyltin) and can be absorbed through theskin and from the gastrointestinal tract (Piscator, 1979c: 616).
Distribution:Inhaled tin tends to accumulate in the lungs with age (Zelikoff & Smialowicz, 1996: 817).
In animal experiments the highest concentrations were found in the kidneys, liver and bone. The main deposit was in the bone. Elimination from the soft tissues seemed to be fairly rapid. The deposition pattern in humans was largely the same, with inclusion of the kidneys (Piscator,1979c: 617). Experiments have shown that powdered, crystalline or liquid inorganic tincompounds tend to concentrate in the lymphatic system (Zelikoff et al., 1996: 817).
Excretion:Absorbed tin is excreted mainly in the urine. Excretion of alkyltin compounds varies quitewidely and the route seems to depend on the specific compound in question (Piscator, 1979c:618).
Acute effects:Tin(IV) chloride is a corrosive irritant (skin, eyes, mucous membranes)(Lewis, 1995: database). Several cases of food poisoning due to tin-contaminated food are on record (Piscator, M. 1979c: 622). Experimental results showed that Sn tends to suppress immune reactions (Zelikoffet al., 1996: 818) and cause DNA damage (Sn2+ highly active) (Cohen, Bowser, Costa, 1996:269).
Chronic effects:Chronic inhalation of tin dusts may cause pneumoconiosis (″stannosis″), which in the past wasconsidered benign (Piscator, 1979c: 620) (Lewis, 1995: database).
Animal studies have shown species differences. Systemic effects like neurological and renaldamage and anaemia were reported. In the one human study reported, no effects were found(Piscator, 1979c: 620).
Carcinogenicity:IARC does not classify tin and its compounds as carcinogenic.
Reproductive effects:No data are available that indicate reproductive effects.

97
Table 3.3.4.26Tin: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Tin, compounds, inorganic (except SnH4) as SnNot a human carcinogen Tin compounds, organic (except Cyhexatin (ISO))
(as Sn)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Sulphides, sulphates, hydroxides.
Absorption: Ingestion (low), inhalation Deposition: Lungs, bone Excretion: Urine, faeces
Target organ Short-term effects Long-term effects
Renal system Storage
Nervous system
Liver Storage
Gastrointestinal tract Food poisoning
Respiratory tract Storage, accumulation; benign pneumoconiosis
Hematopoietic system
Bone Storage
Endocrine system
Muscle
Eye Irritant
Skin Irritant
Cardiovascular system
Immune system Suppression (experimental) Suppression
Reproductive system

98
3.3.4.27 Titanium (Ti)Absorption:Absorption of titanium after ingestion is poor (Berlin & Nordman, 1979b: 631). No data areavailable for absorption after inhalation or through the skin.
Distribution:Titanium is consistently found in the lung, probably due to inhalation of dust particles. Titaniumdioxide has been found in the lymph nodes (Berlin et al., 1979b: 631, 632).
Titanium can cross both the blood-brain and placental barriers (Berlin et al., 1979b: 631).
Excretion:No explicit data are available.
Acute effects:Dusts have mainly nuisance value. The dioxide can be a skin irritant in some cases. Thechlorides and sulphate are corrosive irritants to the skin, eyes and mucous membranes (Lewis,1995: database; Berlin, 1979b: 633).
Chronic effects:Workers exposed to TiO2 pigment for several years showed only minor fibrosis of the lungs,which was more probably caused by the presence of silica particles in the dust (Berlin, 1979b:633).
Carcinogenicity:IARC does not list titanium and its compounds. No carcinogenisis could be shown for exposedhumans, although some animal studies have indicated carcinogenic activity (Cohen, Bowser,Costa, 1996: 270).
Reproductive effects:Reproductive effects have been noted in experimental animals (Berlin, 1979b: 634), but noeffects in humans have been documented.

99
Table 3.3.4.27Titanium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Titanium dioxide total inhalable dustNot a human carcinogen
Titanium dioxide total respirable dust
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Ti, TiO2, TiCl4, Ti(SO4)2
Absorption: Ingestion (poor), inhalation Deposition: Lung, lymph nodes Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Nuisance dust (TiO2); corrosive, irritant (chlorides, sulphate) Nuisance dust (TiO2)
Haematopoietic system
Bone
Endocrine system
Muscle
Eye Corrosive, irritant (chlorides, sulphate)
Skin Corrosive, irritant (chlorides, sulphate)
Cardiovascular system
Immune system
Reproductive system Experimental effects (animals)

100
3.3.4.28 Tungsten (W)Absorption:No data are available for humans. In animal studies about 50 per cent of ingested soluble saltand about 30 per cent of inhaled tungstic oxide aerosol were rapidly absorbed, followed byrapid excretion in urine and faeces (Kazantzis, 1979b: 640).
Distribution:The body burden is very small. Absorbed tungsten is initially distributed to the spleen, kidneyand bone, which is also the site for long-term storage (animal studies). (Kazantzis, 1979b:637).
Excretion:Most absorbed tungsten is rapidly excreted via urine (animal studies) (Kazantzis, 1979b: 637).
Acute effects:Most absorbed tungsten is rapidly excreted via urine (animal studies) (Kazantzis, 1979b: 637).
Chronic effects:Industrially tungsten does not constitute an important health hazard (Lewis, 1995: database). Effects and symptoms of exposure are mainly respiratory (cough, expectoration, shortness ofbreath, tightness in the chest, pulmonary fibrosis) (Kazantzis, 1979b: 643). No data is availablefor long-term systemic effects in humans (Kazantzis, 1979b: 645).
Carcinogenicity:IARC has classified the tungsten ore Wollastonite as Group 3 (unclassifiable as humancarcinogen) (IARC, 1997: Vol. 68). Tungsten and its compounds have not been listed ascarcinogenic.
Reproductive effects:No data are available that indicate reproductive effects.

101
Table 3.3.4.28Tungsten: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Tungsten and soluble compounds (as W)Not a human carcinogenIARC Group 3 (Wollastonite ore) Insoluble compounds
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Unknown
Absorption: Rapid by inhalation, ingestion Deposition: Bone; spleen, kidney Excretion: Urine (rapid)
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Cough, expectoration, shortness of breath, tightness in chest, pulmonaryfibrosis.
Hematopoietic system
Bone Storage
Endocrine system
Muscle
Eye Irritation
Skin Irritation
Cardiovascular system
Immune system
Reproductive system

102
3.3.4.29 Uranium (U)Absorption:InhalationThe high density of uranium and its compounds will cause most of the inhaled material to bedeposited in the upper respiratory tract where mucociliary clearance will cause it to be ingested. Measurements of occupational exposure have led to estimates that only about one to five percent of inhaled material will be carried into the lung. Absorption of inhaled uranium is criticallydependent on its solubility in biological media. Soluble material deposited in the alveoli will beabsorbed completely (Berlin et al., 1979c: 651). The uranyl (UO2
2+) species have great affinityfor proteins, nucleotides and bone (Berlin et al., 1979c: 651).
IngestionAbsorption of uranium from the digestive tract varies with solubility, but even solublecompounds are poorly absorbed (Berlin et al., 1979c: 652).
Skin contactAnimal experiments have shown some absorption by dermal contact with soluble compounds. No data are available for humans (Berlin et al., 1979c: 652).
Distribution:On entering the blood stream the absorbed uranium undergoes bio-transformation to watersoluble complexes or colloids and rapidly (66 per cent in six minutes) distributed throughout thebody. Excluding material deposited in the lungs, about 85 per cent of the steady state bodyburden in occupationally exposed persons was found in the bone, about 90 per cent of the restin the kidney, with detectable amounts in the liver (Berlin et al., 1979c: 650, 652).
Inhaled less-soluble products are found in the bronchial lymph nodes and the lung itself (Berlinet al., 1979c: 652)
Excretion:U6+ is rapidly and primarily excreted by the kidneys as a uranium carbonate complex. Theexcretion is a two-phase process with about 70 per cent of the dose after exposure beingexcreted in the first 24 hours and the rest over a period of several months. Re-absorption ofthe uranium is controlled by urinary pH. Acidic conditions are associated with functionalimpairment of the kidneys due to uranium binding to the walls of the tubules. U4+ is bound toproteins in the serum and cleared very slowly (Berlin et al., 1979c: 653; Fowler, 1996f: 726).
Particle size and solubility determine the rate of clearance of uranium from the lungs. Published results show a two-phase process with an initial half-life of somewhere between 11days and three months. The slow phase has a half-life of three months to about five years(Berlin et al., 1979c: 653).
Acute effects:Uranyl nitrate and its hexahydrate are corrosive and irritating to the skin, eyes, and mucousmembranes (Lewis, 1995: database).

103
Table 3.3.4.29Uranium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Carcinogenic due toradioactivity Uranium compounds, natural, soluble (as U)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Oxides, phosphates
Absorption: Inhalation, ingestion Deposition: Bone, kidney Excretion: Urine
Target organ Short-term effects Long-term effects
Renal System Functional impairment, kidney failure, storage
Nervous System
Liver
Gastrointestinal Tract
Respiratory tract Corrosive, irritant (UO2(NO3)2), deposition (insoluble salts) Radiation damage (insoluble compounds)
Haematopoietic System Bound to serum protein (U4+) slow clearance
Bone Main storage
Endocrine System
Muscle
Eye Corrosive, irritant (UO2(NO3)2)
Skin Corrosive, irritant (UO2(NO3)2)
Cardiovascular system
Immune system
Reproductive system Foetal abnormalities (animals)

104
Chronic effects:Chronic effects can arise due to two factors:• The chemical toxicity of soluble uranium compounds leading to kidney damage and possible
failure. Animal experiments have shown that for non-lethal exposure, a form of resistancedevelops through epithelial regeneration in the kidneys. After cessation of exposure, theepithelium gradually returns to normal (Berlin et al., 1979c: 654).
The radiological damage caused by insoluble uranium compounds not cleared from the lungsdepends on the isotope composition of the material (Berlin et al., 1979c: 654).
Carcinogenicity:Uranium and its compounds are carcinogenic as a result of radiological activity.
Reproductive:Some reproductive effects and foetal abnormalities were found in animal experiments. Somereproductive effects in humans were found in World War Two experiments, but they have notbeen repeated (Corbella & Domingo, 1996: 1088 - 1091).
3.3.4.30 Vanadium (V)Absorption:An estimated 25 per cent of soluble compounds may be absorbed from the lungs (WHO(1988)) (Lauwerys & Hoet, 1993: 95). V2O5 is specifically reported to be nearly 100 per centabsorbed by inhalation (Lewis, 1995: database).
Absorption via the oral route appears to be low (less than one per cent) (Vouk, 1979b: 657).
Distribution:The major fraction (about 90 per cent) of vanadium circulating in the blood stream is bound tothe plasma and widely distributed in the tissues. Tissue levels of vanadium are generally low(Lauwerys et al., 1995: 94; Vouk, 1979b: 663), but seem to be highest in the liver, kidney andlungs.
Excretion:Excretion is mainly via urine. Biological half-life is about 20 to 40 hours (Lauwerys et al., 1995:95). Faecal excretion is minor, except in the case of ingested material, where excretion ismainly through the faeces due to the low absorption in the gastrointestinal tract (Vouk, 1979b:654). Older estimates of half-life are about 42 days (Vouk, 1979b: 664).
Acute effects:There is some experimental evidence that respiratory exposure to vanadium can lead tosensitisation (Vouk, 1979b: 665). Responses to industrial exposure are thought usually to beacute rather than chronic, involving irritation of the eyes and respiratory system in the form ofconjunctivitis, bronchospasm, bronchitis and asthma-like diseases. There seems to be somecontroversy over involvement of other organ systems (Lewis 1995: database).
Respiratory symptoms (persistent cough) have an induction period of 12 to 20 hours and arereversible, disappearing within two to five days (Vouk, 1979b: 665).
Chronic effects:The older literature (Vouk, 1979b: 659), mentioned symptoms quoted below that have not beensupported by more recent works (Lewis, 1995: database):
Vague general signsWeakness, nausea, vomiting, tinnitus, headache, dizziness.

105
Table 3.3.4.30Vanadium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Vanadium pentoxide (total inhalable dust)Not a human carcinogen
Vanadium pentoxide (fume and respirable dust)
Occupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: V, oxides, sulphate, sulphide, (Ca, Na, ammonium) vanadates
Absorption: Lungs Deposition: Liver, lungs, kidney Excretion: Urine (rapid)
Target organ Short-term effects Long-term effects
Renal system Deposition Deposition
Nervous system
Liver Deposition Deposition
Gastrointestinal tract
Respiratory tract Deposition, irritation, sneeze, cough Deposition
Haematopoietic system Anaemia, leukopenia, leukcocyte granulation
Bone
Endocrine system
Muscle
Eye Irritation
Skin Irritation
Cardiovascular system Palpitations, extrasystoles, bradycardia, coronaryinsufficiency
Immune system
Reproductive system Experimental effects (mouse, rat, hamster)
106
HeartPalpitations, transient coronary insufficiency, bradycardia, and unexpectedly many extrasystoles.
BloodAnaemia, leukopenia, leucocyte granulation, lowering of cholesterol levels (unconfirmed).
Evidence for long-term respiratory effects of occupational exposure has been mentioned, butthe ecidence is considered inadequate (Vouk, 1979b: 666). Sensitisation is possible asmanifested by increasingly severe symptoms (respiratory, dermatitis) upon repeated exposure,even for shorter duration or at lower levels (Vouk, 1979b: 669).
Carcinogenicity:IARC has not classified vanadium and its compounds as human carcinogens.
Reproductive effects:Experimental reproductive effects have been found (mice, rats, hamsters) (Corbella &Domingo, 1996: 1091 – 1093; Keen, 1996: 995), but no effects have been documented forhumans.
3.3.4.31 Yttrium (Y)Absorption:The rare earth elements have low toxicity by ingestion. Skin and lung granulomas have beennoted after exposure (Lewis, 1995: database). Animal studies showed no accumulation ofyttrium in bones.
Distribution:Animal data suggest that the pulmonary system and liver are the primary target organs.
Excretion:No data are avalable to indicate mechanisms of excretion of yttrium.
Acute effects:Toxic doses cause systemic effects such as writhing, ataxia, laboured respiration, sedation andwalking on the toes with the back arched (animal studies). Yttrium is a possible anticoagulantand the nitrate is a skin and eye irritant (Lewis, 1995: database). Based on effects observed inanimals, acute exposure would lead to fibrotic lung disease, manifested as shortness of breath,cough, chest pain, and cyanosis.
Chronic effects:No signs or symptoms of chronic exposure to yttrium or its compounds have been reported.
Carcinogenicity:Yttrium and its compounds are not included in the IARC classification for carcinogens
Reproductive effects:No data are available to indicate reproductive effects in humans.

107
Table 3.3.4.31Yttrium (and rare earth elements): Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not a human carcinogen Metal and compoundsOccupational Health And Safety Act, 1993Regulations for Hazardous ChemicalSubstances (Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Unknown
Absorption: Lung, skin Deposition: Unknown Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal system
Nervous system Ataxia, sedation
Liver
Gastrointestinal tract Toxic by ingestion
Respiratory tract Laboured respiration
Hematopoietic system Possible anticoagulant (Y)
Bone
Endocrine system
Muscle
Eye Irritant (Y(NO3)2)
Skin Irritant (Y(NO3)2)
Cardiovascular system
Immune system
Reproductive system
108
3.3.4.32 Zinc (Zn)Absorption:The zinc balance in the body is homeostatically controlled (Elinder & Piscator, 1979d: 675). There is insufficient information available to calculate the absorption of zinc after inhalation(Elinder et al., 1979d: 679). Absorption of ingested zinc is highly variable (10 to 90 per cent inanimals) and controlled by the zinc status in the body, dietary, and health factors (Elinder et al.,1979d: 697).
Distribution:In humans the major portion of the body burden of zinc is found in the muscles (60 per cent)and bone (30 per cent). The highest concentration however, is found in the prostate (Elinder etal., 1979d: 679).
Excretion:Excretion takes place mainly via faeces (75 per cent) with urine as a secondary route (25 percent). Excretion rate and biological half-life are regulated according to the zinc status in thebody. In normal persons the biological half-life is 162 to 500 days (Elinder et al., 1979d: 680). Urinary excretion is reported to have a circadian rhythm (Lauwerys, 1993: 97).
Acute effects:Zn metalZinc is a human skin irritant. Ingestion causes systemic effects like coughing, shortness ofbreath and sweating (Lewis, 1995: database).
ZnOInhalation of freshly formed fumes can lead to so-called “metal fume fever” with influenza-likesymptoms (fever, chills, dyspnoea, muscle soreness, nausea, fatigue) (Benson & Zelikoff,1996: 935) which on cessation of exposure disappear completely in about two days. Thepossible presence of contaminants like Pb, As, Cd, Sb complicates the picture (Lewis, 1995:database). The syndrome may be coupled to a sensitisation mechanism and it is possible tobecome temporarily immune to it (Lewis, 1995: database). It is estimated that symptoms willnot develop at air concentrations below 15 mg/m3 (Elinder et al., 1979d: 682).
ZnCl2Inhalation causes irritation and damage to respiratory mucous membranes and grey cyanosis(Lewis, 1995: database).
Chronic effects:Chronic zinc intoxication in humans has not been described in much detail (Elinder et al., 1979:673). Long-term excess zinc intake has led to secondary copper deficiency andimmunosuppression in humans (Keen, 1996: 982).
ZnO dust can block sebaceous gland ducts with resultant pustular skin complaints. Allergy toZnO is extremely rare (Lewis, 1995: database). ZnCl2 and ZnSO4 are caustic and chronicexposure can lead to skin ulcers (Lewis, 1995: database).
Carcinogenicity:Zinc chromates are confirmed carcinogens (Lewis, 1995: database), but this is due to thechromium. Zinc has not been identified as carcinogenic by IARC.
Reproductive effects:Excess zinc intake in animals has reportedly led to foetal secondary copper deficiency, whichhas caused birth defects (Keen, 1996: 982). Similar data are not available for humans.

109
Table 3.3.4.32Zinc: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Zinc chloride fume (ZnCl2)Not a human carcinogen
Zinc oxide fume (ZnO)
Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table 3.4.6.3
Speciation in mineral processing plants: Unknown
Absorption: Inhalation, ingestion Deposition: Muscle, bone Excretion: Faeces, urine
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract
Respiratory tract Acute pneumonitis, pulmonary oedema (ZnCl2)(heavy exposure)
Haematopoietic system
Bone Storage
Endocrine system
Muscle Storage
Eye
Skin Irritant (ZnCl2, ZnSO4) Ulceration (ZnCl2, ZnSO4)
Cardiovascular system
Immune system
Reproductive system Storage in prostate

110
3.3.4.33 Zirconium (Zr)Absorption:Most zirconium compounds in common use are insoluble and considered inert. Metabolicstudies are not available, but tissue concentrations indicate that significant amounts ofzirconium may be adsorbed orally (Doull, Klaassen & Amdur, 1980: 462). Inhalation exposureto water-soluble ZrOCl2 indicated that the highest concentration of zirconium occurred in thelungs and pulmonary nodes.
Distribution:The body burden of zirconium is distributed across the liver, blood (cells and lipids), lung,kidneys, muscle, brain, pancreas, stomach, spleen, and testes (Doull, Klaassen & Amdur,1980: 462).
Excretion:Zirconium is excreted by the intestine, probably in the bile. Milk is a secondary route ofexcretion, but levels in the urine are negligible (Doull, Klaassen & Amdur, 1980: 462).
Acute effects:Soluble zirconium salts are poisonous (Lewis, 1995: database), but the oral toxicity of zirconiumand its compounds is generally considered to be low. No evidence of industrial disease as aresult of zrconium exposure has been documented (Doull, Klaassen & Amdur, 1980: 462). ZrCl4 is a corrosive skin, eye and mucous membrane irritant (Lewis, 1995: database).
Chronic effects:Pulmonary granuloma has been reported in zirconium workers. Inhalation of ZrCl4 (6 mg Zr/m3)for 60 days produced slightly decreased haemoglobin and red blood cell counts and increasedmortality in animals (Lewis, 1995: database).
Carcinogenicity:IARC does not classify zirconium or its compounds as carcinogens.
Reproductive effects:Zr(SO4)2 has been shown to be reproductively active in animal studies (Lewis, 1995: database),but similar data have not been reported for humans.

111
Table 3.3.4.33Zirconium: Toxicological properties and target-organ effects
Carcinogen Species listed OEL-RL and OEL-CL BEI
Not human carcinogen Zirconium compounds (as Zr)Occupational Health And Safety Act, 1993Regulations for Hazardous Chemical Substances(Department of Labour, 1995).
Medical surveillanceBiological effect monitoringBiological monitoring
See Table3.4.6.3
Speciation in mineral processing plants: ZrO2, Zr(SO4)2
Absorption: Ingestion Deposition: Unknown Excretion: Unknown
Target organ Short-term effects Long-term effects
Renal system
Nervous system
Liver
Gastrointestinal tract Toxic, corrosive (Zr(SO4)2)
Respiratory tract Corrosive irritant (ZrCl4) Lung granuloma (NaZr lactate)
Hematopoietic system
Bone
Endocrine system
Muscle
Eye Corrosive irritant (ZrCl4)
Skin Corrosive irritant (ZrCl4, ZrOClH) Granuloma (NaZr lactate)
Cardiovascular system
Immune system
Reproductive system Experimental effects

112
3.4 Exposure assessment: General guidelines foroccupational health risk assessment and management.
3.4.1 ContextAn exposure assessment estimates the magnitude and frequency of actual or potentialexposures to characterised substances, and identifies the pathways by which exposure occurs.The complete exposure assessment also identifies the routes through which the hazardoussubstances may enter the human body.
Exposure under normal working conditions is determined through physical monitoring of theworkplace, personal monitoring using monitoring equipment carried by the workers, orbiological monitoring where exposure is estimated from the analysis of body fluids. A medicalsurveillance programme identifies deterioration of health in employees at an early stage, whensuch effects may still be reversible when the source of exposure is removed. Emergency plansand other health risk management practices should be in place for the handling of incidents.
3.4.2 The relationship between dust and heavy metals in exposureassessment
As a rule, control of exposure to particulates/dust in the occupational environment would alsoprotect against exposure to particulate-associated heavy metals. In some cases, however, theguideline concentration for dust may not be adequately protective for all of the constituents inthe dust. Table 3.4.2 lists the maximum concentrations of heavy metals that can be tolerated atthe highest permissible level of airborne dust in the occupational environment. Values aregiven for particulates as total dust and for the respirable fraction. Where concentrations ofheavy metals in dust exceed the listed values, additional measures have to be introduced toprotect employees against particulate-associated exposure to heavy metals. For example, ifdust is controlled within permissible levels but the concentration of beryllium in the dust exceeds200 parts per million (0.02 per cent), additional protective actions may be required to accountfor exposure to beryllium. Dusts containing more than 20 per cent calcium oxide, as anotherexample, would pose a hazard for irritation effects.
Table 3.4.2Maximum concentrations of heavy metals that can be tolerated at the maximum
permissible dust loads in the occupational environment
Heavy metal TLV mg/m3
total dustTLV mg/m3
respirable dustMass % of metal in
total dustMass % of metal in
respirable dust
Antimony 0.5 5
Arsenic 0.01 0.1
Barium 0.5 5
Beryllium 0.002 0.02
Cadmium 0.01 0.002 0.1 0.006
Calcium oxide 2 20
Chromium (water-soluble) 0.05 0.5
Chromium metal and Cr (III) 0.5 5
Chromium (insoluble in water) 0.01 0.1
Cobalt 0.02 0.2

113
Heavy metal TLV mg/m3
total dustTLV mg/m3
respirable dustMass % of metal in
total dustMass % of metal in
respirable dust
Copper (dust & mist) 1 10
Copper (fume) 0.2 2
Indium 0.1 1
Iron oxide dust & fume as Fe 5 50
Iron (water-soluble) 1 10
Lead 0.05 0.5
Manganese 0.05 0.5
Mercury 0.025 0.25
Molybdenum (water-soluble) 5 50Molybdenum (insoluble inwater) 10 100
Nickel (metal) 1 10
Nickel (water-soluble) 0.1 1
Nickel (insoluble in water) 1 10
Osmium 0.0016 0.016
Platinum (metal) 1 10
Platinum (water-soluble) 0.002 0.02
Rhodium metal 1 10
Rhodium (water-soluble) 0.01 0.1
Rhodium (insoluble in water) 1 10
Selenium 0.2 2
Silver (metal) 0.1 1
Silver (water-soluble) 0.01 0.1
Tantalum 5 50
Tellurium 0.1 1Thallium (metal & water-soluble) 0.1 1
Tin 2 20
Titanium 6 3 60 9
Tungsten (water-soluble) 1 10
Tungsten (insoluble in water) 5 50
Uranium 0.2 2
Vanadium pentoxide (dust) 0.05 0.15
Yttrium 1 10
Zinc oxide dust 10 100
Zirconium 5 50

114
3.4.3 Physical monitoring of the workplace
3.4.3.1 Direct-reading instrumentsWhere exposures may be due to releases from component failures or other incidents, andwhere it is likely that short term exposure limits (or ceiling levels) will be exceeded, direct-reading instruments and alarm systems are the preferable approach to manage employeeexposure and health risks. In the case of managing the risk of exposure to heavy metals,however, exposure is largely in the form of particulate-associated substances, and direct-reading instruments are not widely applicable. Furthermore, concerns are related more toexposures during normal operation of the plants rather than under upset conditions.
3.4.3.2 Detector-tube measurementsA detector tube is a vial that contains a chemical preparation that reacts with the measuredsubstance in a way that produces a colour change (Dräger, 1992: 26). The length of staindiscolouration is an indication of the concentration of the substance. Alternatively, quantitativeindication is based on interpretation of the colour intensity according to a reference standard orset of standards.
The measurement system consists of a detector tube and a gas detector pump. The pumpmust pass the sample through the tube at a prescribed rate until a required volume has beensampled. The measured value shows the actual concentration during the period ofmeasurement. Detector tubes are not intended to be used for quantitative exposuremeasurements. Standard deviations of measurements are frequently in the range of 30 percent, and cross sensitivities commonly occur where compounds are present in mixtures. Thesedevices are nevertheless extremely useful to screen work areas where leaks of hazardoussubstances may occur from time to time, or to determine concentration ranges for ambientsampling.
There are not many detector tubes available for screening assessments for exposure to heavymetals, but Table 3.4.3.2 lists those that are available.
Table 3.4.3.2Some detector tubes for screening assessment of exposure
Substance Reference Product code
Arsenic trioxide 67 28951
Arsine CH 25001
Mercury vapour CH 23101
Nickel
Dr≅ ger, 1997
67 28871
3.4.3.3 Air sampling and analysisAmbient monitoring assesses the health risk by measuring external exposure to the chemical. In industry, ambient monitoring usually means monitoring the airborne concentration of thechemical. Sampling can be stationary, i.e. at selected positions in the workplace. This isknown as area monitoring. Personal sampling is the technique followed when the samplingequipment is carried on the person to be monitored, to measure exposure as a time-weightedaverage over an entire shift. Sampling is usually conducted in the breathing zone, and coversall the work areas in which the person has to perform tasks. Sampling for heavy metals coversvapours, fumes, mists and particulates.

115
Active samplingActive or dynamic sampling for heavy metals normally uses an air sampling pump and a filtersystem, to collect the substances of interest. The collected particulates are then extracted ordissolved, and the metals quantified with an analytical instrument. The National Institute forOccupational Safety and Health (NIOSH) and the Occupational Safety and HealthAdministration (OSHA) have published a range of standard, validated sampling and analyticalmethods. These are listed in Section 3.4.3.6. Where possible, these methods for activesampling and analysis should be used to quantify exposure levels of hazardous substances inoccupational environments.
Passive samplingPassive sampling offers an attractive alternative to dynamic sampling, but the nature of thesamplers limits their use to gases and vapours, thereby leaving very limited application to heavymetals. In contrast to active sampling where forced convection brings the substances ofinterest in contact with the sorbent, a passive sampler collects the species by natural diffusion. Sampling rates are calculated either from predicted diffusion coefficients, or determinedexperimentally in the laboratory. Extraction and analysis are the same as for active sampling. Some of the passive samplers produce colour changes that are proportional to concentrationand exposure time, in which case quantification of exposure can be achieved through calibratedcolour comparisons. The ChromAir passive badge (K&M Environmental, 1996) is available forquantification of mercury exposure.
Categories of samplingSampling can be conducted in three categories, as described below.
Full-period, continuous single samplingThis sampling approach is defined as sampling over the entire sampling period, to collect onlyone sample. The sampling may be for a full-shift sample or for a short period ceilingdetermination.
Full-period, consecutive samplingThe sampling strategy in this case is to use multiple consecutive samples of equal or unequaltime duration which, if combined, equal the total time duration of the required sample. Anexample would be to take four two-hour samples and combine these for assessment of aneight-hour shift. Advantages of this approach are:
• If one of the samples were lost due to pump failure, contamination or other reason, at leastsome data would have been acquired to assess the situation.
• The use of multiple samples has statistical advantages. If a sufficient number of samplesare taken, this may lead to lower errors of observation.
• Collection of several samples may indicate how exposures vary over the workday, and howthis would affect overall exposure.
Grab samplingGrab sampling is defined as collecting a number of short-term samples at various times duringthe sampling period which, when combined, provide an estimate of exposure over the totalperiod. A typical example would be a number of high-volume air samples collected on filtersover a period of time.
3.4.3.4 Selection of appropriate positions for monitoringAll the areas with a potential to release a toxic substance of interest have to be identified. Because of many potential release points, it is sometimes not practical to sample at every pointduring all the surveys. A decision has to be taken on the overall frequency of monitoring, basedon the level of risk and the cost of monitoring. A selection (subgroup) of the sampling points

116
has to be taken for each survey (NIOSH, 1977: 33). On a statistical basis, this subgroup has tobe of adequate size, so that there would be a high probability that the random sample willcontain at least one area with a high exposure level, assuming that such high level is possible.
The sample size drawn from a group is listed in Table 3.43.4a. The philosophy is to ensurewith 90 per cent confidence that at least one sampling point from the highest ten per centpotential release areas is included in the sample.
Table 3.4.3.4aSize of partial sample for the top 10 % potential release points at a confidence
level of 90 %Size of potential release points (N) Number of points to measure (n)
891011 to 1213 to 1415 to 1718 to 2021 to 2425 to 2930 to 3738 to 4950
789
101112131415161718
N = original equal risk group size.n = sample size or subgroup size.n = N if N is less than 7.
To limit any bias to certain positions by the sampler, it is recommended that a system ofrandom sampling be followed. Table 3.4.3.4b lists a selection of random numbers. Of course,where information about specific positions has to be obtained, these can be done as separatesurveys.

117
Table 3.4.3.4bTable of random numbers after NIOSH (1977)
The procedure for random sampling is as follows:
• Assign each potential area of toxicant release a number from one to N, where N is the totalnumber of areas in the facility. During a particular sampling session, a subgroup of nsamples has to be taken.
• Arbitrarily choose a column in Table 3.4.3.4b and read down the list. Ignore zero and allvalues larger than N. If necessary, proceed to the next column until a partial sample of nnumbers has been selected.
Areas that have been assigned the selected numbers will form the randomly selected subgroupfor monitoring.

118
3.4.3.5 Personal samplingSelection of the maximum exposed individualFollowing a positive indication that an employee or employees may be exposed atconcentrations of a toxic substance at or above the action level, then the employer is requiredto determine the exposure level of an employee who would be expected to have the highestexposure. The approach is known as exposure assessment of the maximum exposedindividual. The assessment is an approximate one, and those employees that are expected tohave lower exposure than those at maximum risk are not sampled initially.
The best information for selection is normally obtained from a preliminary survey of the workenvironment, so that a well-informed person can make a valid judgement as to the employeewith the highest exposure. If there are work situations in which the exposures in theassignments vary, either because of the work patterns of employees or the varying nature ofthe production process, the most severe situations are selected for initial sampling.
The employee closest to the source of the hazardous substance would most likely be theperson at maximum risk. Air movement patterns within a workroom should be analysed todetermine the risk potential of employees. The locations of ventilation systems, open doorsand windows, and the size and shape of the work area, would all be factors that could affect airflow patterns and result in higher contaminant concentrations further away from the source. Employee work patterns should also be observed to get an idea of time-concentrationexposures. Differences in work habits of individuals with the same work patterns can affectexposure levels significantly.
If a maximum risk worker cannot be identified for an operation with reasonable certainty, theapproach of random sampling of the group of workers has to be followed.
Random sampling of a homogeneous risk groupThe procedure is to sample the group of workers with similar work patterns randomly. Theapproach is similar to that outlined in Section 3.4.3.4 for statistical selection of monitoringpositions. A subgroup of adequate size is selected, so that there would be a high probabilitythat the random sample will contain at least one person with high exposure, assuming that suchhigh exposure is possible. Initial sampling should begin with at least six (preferably nine)personal samples collected on at least three different days for each job assignment.
The sample size drawn from a group is listed in Table 3.4.3.5. The philosophy is to ensure with90 per cent confidence that at least one individual from the highest ten per cent exposure groupis included in the sample.

119
Table 3.4.3.5Size of partial sample for the top 10 % exposure subgroup at a confidence level
of 90 %Size of group (N) Number of individuals (n)
891011 to 1213 to 1415 to 1718 to 2021 to 2425 to 2930 to 3738 to 4950
789101112131415161718
N = original equal risk group sizen = sample size or subgroup sizen = N if N is less than 7
Random sampling is conducted with the use of a table of random numbers (see Table 3.4.3.4babove).
The procedure for random sampling is as follows:
• Assign each employee a number from 1 to N, where N is the total number of employees inthe group.
• Arbitrarily choose a column in Table 3.6 and read down the list. The subgroup that has tobe selected has a size n. Ignore zero and all values larger than N. If necessary, proceed tothe next column until a partial sample of n numbers has been selected.
Individuals who have been assigned the selected numbers will form the randomly selectedsubgroup for monitoring.
Selection of employees for periodic monitoringIf any of the measurements on the maximum exposed individual or the selected subgroupshows exposures to a toxicant at or above the occupational exposure limit (OEL), the employerhas to follow the guidelines presented below:
• Identify all employees who may be exposed at or above the OEL.• Measure the exposure levels of all the identified employees. The purpose of this approach
is to restrict measurements to those employees with significant exposures. It is notadequate to sample a subgroup and assign the average value to all the employees in theexposure scenario.
• If the exposure level of the maximum exposed individual or those of the selected subgroupwere below the OEL, it is reasonable to assume that exposure levels of the otheremployees would also be lower than the OEL. No further action should be necessary untilsome change in the operation or control measures is introduced.
Personal monitoringSampling should be conducted for an entire shift, minus not more than two hours for equipmentsetup and dismantling, i.e. at least six hours of an eight-hour shift or ten hours of a 12-hour

120
shift. Good occupational hygiene judgement should be used to interpret exposures during theperiod not sampled.
Under regulations of the USA Occupational Health and Safety Administration (OSHA), minimumlegal requirements have been proposed, i.e.:
• The exposure of an employee whose measurement is at or above the action level, but notabove the permissible exposure (or occupational exposure limit), must be measured at leastevery two months. The action level of exposure is usually half or one third of thepermissible level, and necessitates the application of specified precautionary measures. These measures may include biological monitoring and medical examinations. Morefrequent measurements may be made on the basis of professional judgement of theexposure situation.
• For an employee whose exposure measurement exceeds the permissible level, theemployee’s exposure must be measured at least every month until the exposure is reducedto below the standard by appropriate control measures. More frequent measurements maybe made on the basis of professional judgement of the exposure situation.
• If two consecutive exposure measurements on an employee taken at least one week apartreveal that each of the measurements is less than the action level, exposure monitoring onthe particular individual may be terminated.
• In situations of infrequent (non-routine) exposure, the question of how often to monitorinfrequent operations is best answered with professional judgement. The physiological riskfrom the chemical and its toxicological profile should be important considerations indetermining the need to monitor employees with infrequent exposure.
3.4.3.6 Sampling and analytical methods for exposure assessment
Table 3.4.3.6List of NIOSH and OSHA sampling and analytical methods for air monitoring
Element Agency Reference Analytical method
Antimony and compounds NIOSH 2 (S2) AA
Antimony and compounds OSHA ID 121 AA
Antimony and compounds OSHA ID 125 ICP-AES
Antimony particulates NIOSH 4 (261) AA
Arsenic and compounds NIOSH 7900 AA, FLARGN
Arsenic (elements) NIOSH 7300 ICP-AES
Arsenic, inorganic compounds OSHA ID 105 AA-GF
Arsenic, organic compounds OSHA CIM IC-AA
Arsenic organo NIOSH 5022 IC-AA
Arsenic trioxide NIOSH 7901 AA-GF
Barium chloride, soluble compounds NIOSH 7056 AA
Barium, insoluble compounds OSHA ID 121 AA
Barium, soluble compounds NIOSH 7056 AA
Barium, soluble compounds OSHA ID 121 AA
Barium sulphate, respirable fraction OSHA ID 121 GR
Barium sulphate (total dust) OSHA ID 121 GR
Beryllium & compounds OSHA ID125 ICP

121
Element Agency Reference Analytical method
Beryllium & compounds NIOSH 7102 AA-GF
Beryllium (elements) NIOSH 7300 ICP-AES
Bismuth OSHA CIM AA
Bismuth telluride, Se-doped OSHA ID 121 GR-AA
Bismuth telluride, undoped, respirable dust OSHA ID 121 GR-AA
Bismuth telluride, undoped, total dust OSHA CIM GR
Cadmium OSHA ID 189 AA
Cadmium & compounds NIOSH 7048 AA-F
Cadmium (elements) NIOSH 7300 ICP-AES
Calcium & compounds NIOSH 7020 AA-F
Calcium (elements) NIOSH 7300 ICP-AES
Calcium oxide OSHA ID 121 AA
Calcium oxide NIOSH 7020 AA-F
Calcium oxide (elements) NIOSH 7300 ICP-AES
Calcium (see specific compounds) NIOSH 7020 AA-F
Chromium (chromic acid and chromates) OSHA ID 103 POL
Chromium (chromic acid and chromates) NIOSH 7600 VAS
Chromium (chromic acid and chromates) NIOSH 7604 IC-ECN
Chromium acetate OSHA ID 121 AA
Chromium carbonate OSHA ID 121 AA
Chromium & compounds NIOSH 7024 AA-F
Chromium (elements) NIOSH 7300 ICP-AES
Chromium, hexavalent NIOSH 7600 VAS
Chromium, hexavalent NIOSH 7604 IC-ECN
Chromium, hexavalent OSHA ID 103 DPP
Chromium, hexavalent OSHA ID 215 IC
Chromium, metal and insoluble compounds OSHA ID 121 AA
Chromium, metal and insoluble compounds OSHA ID 125 ICP
Chromium, soluble salts OSHA ID 121 AA
Cobalt acetate OSHA ID 125 G ICP-AES
Cobalt carbonyl OSHA ID 121 AA
Cobalt & compounds NIOSH 7027 AA-F
Cobalt (elements) NIOSH 7300 ICP-AES
Cobalt hydrocarbonyl OSHA ID 121 AA
Cobalt, metal dust and fume OSHA ID 121 AA
Cobalt, metal dust and fume OSHA ID 125 G ICP
Copper dust NIOSH 7029 AA-F

122
Element Agency Reference Analytical method
Copper, dusts and mists OSHA ID 125 G ICP-AES
Copper, dusts and mists OSHA ID 121 AA
Copper (elements) NIOSH 7300 ICP-AES
Copper fume NIOSH 7029 AA-F
Copper fume OSHA ID 121 AA
Copper fume OSHA ID 125 G ICP-AES
Indium NIOSH 1 (190) ASV
Iron and compounds OSHA ID 121 AA
Iron (elements) NIOSH 7300 ICP-AES
Iron oxide fume OSHA ID 121 AA
Iron oxide fume OSHA ID 125 ICP
Lead NIOSH 7082 AA
Lead NIOSH 7105 AA-GF
Lead (elements) NIOSH 7300 ICP-AES
Lead, inorganic fumes and dusts OSHA ID 121 AA
Lead, inorganic fumes and dusts OSHA ID 125 G ICP-AES
Lead, inorganic surface dusts OSHA ID 121 AA
Lead sulphide HIOSH 7505 X DIF
Manganese (elements) NIOSH 7300 ICP-AES
Manganese fume OSHA ID 121 AA
Manganese fume OSHA ID 125 G ICP-AES
Manganese tetroxide OSHA ID 121 AA
Manganese tetroxide OSHA ID 125 G ICP-AES
Mercury NIOSH 6009 AA
Mercury, aryl and inorganic OSHA ID 145 AA
Mercury, vapour OSHA ID 140 AA
Molybdenum (elements) NIOSH 7300 ICP-AES
Molybdenum, insolubles OSHA ID 121 AA
Molybdenum, insolubles OSHA ID 125 ICP-AES
Molybdenum, solubles OSHA ID 121 AA
Nickel (elements) NIOSH 7300 ICP-AES
Nickel, metal and insoluble compounds OSHA ID 125 ICP-AES
Nickel, metal and insoluble compounds OSHA ID 121 AA
Nickel, soluble compounds OSHA ID 125 ICP-AES
Nickel, soluble compounds OSHA ID 121 AA
Osmium tetroxide OSHA CIM ICP-AES
Platinum (elements) NIOSH 7300 ICP-AES

123
Element Agency Reference Analytical method
Platinum, soluble salts OSHA CIM AA-GH
Rhodium, metal fume and dust NIOSH 3(S188) AA
Rhodium, metal fume and dust OSHA CIM AA-GF
Rhodium, soluble salts NIOSH 3(S189) AA-HGA
Rhodium, soluble salts OSH CIM AA-GF
Selenium compounds OSHA CIM AA-GF
Selenium (elements) NIOSH 7300 ICP-AES
Silver (elements) NIOSH 7300 ICP-AES
Silver metals and soluble compounds OSHA ID 121 AA
Silver metals and soluble compounds OSHA ID 206 ICP-AES
Tantalum, metal, oxide dusts OSHA CIM GR
Tellurium OSHA ID 121 AA
Tellurium (elements) NIOSH 7300 ICP-AES
Thallium (elements) NIOSH 7300 ICP-AES
Thallium, soluble compounds OSHA ID 121 AA
Tin (elements) NIOSH 7300 ICP-AES
Tin, inorganic compounds except oxides OSHA ID 121 AA
Tin, inorganic compounds except oxides OSHA ID 206 ICP-AES
Tin oxide OSHA ID 121 AA
Titanium dioxide NIOSH 3(S385) AA
Titanium dioxide (total dust) OSHA CIM GR
Titanium (elements) NIOSH 7300 ICP-AES
Tungsten and compounds OSHA ID 213 ICP-AES
Tungsten, insoluble compounds NIOSH 7074 AA-F
Tungsten, insoluble (elements) NIOSH 7300 ICP-AES
Tungsten, soluble compounds NIOSH 7074 AA-F
Uranium, insoluble compounds OSHA CIM ICP-AES
Uranium, soluble compounds OSHA ID 170 POL
Vanadium, fume (pentoxide) OSHA ID 125 G ICP-AES
Vanadium (elements) NIOSH 7300 ICP-AES
Vanadium oxides NIOSH 7504 X DIF
Vanadium, respirable dust OSHA ID 125 G ICP-AES
Yttrium OSHA CIM AA
Yttrium (elements) NIOSH 7300 ICP-AES
Zinc OSHA ID 121 AA
Zinc OSHA ID 125 G ICP-AES
Zinc and compounds NIOSH 7030 AA-F

124
Element Agency Reference Analytical method
Zinc oxide NIOSH 7502 X DIF
Zinc oxide (elements) NIOS 7300 ICP-AES
Zinc oxide fume OSHA ID 121 GR, AA
Zinc oxide fume OSHA ID 125 GR, ICP-AES
Zinc oxide fume OSHA ID 143 GR, X DIF
Zirconium compounds OSHA ID 121 GR, AA
Zirconium (elements) NIOSH 7300 ICP-AES
Atomic absorption spectrometry AAAtomic absorption spectrometry, flame AA-FAtomic absorption spectrometry, graphite furnace AA-GFAtomic emission spectrometry AESGravimetric analysis GRInductively coupled plasma ICPPolarography POLX-ray diffraction X DIF
3.4.4 Medical evaluationMedical evaluation refers to a planned programme of periodic examination, which may includeclinical examinations, biological monitoring, or medical tests of employees by an occupationalhealth practitioner or, in prescribed cases, by an occupational medicine practitioner.
3.4.4.1 Medical surveillanceThe purpose of a medical surveillance programme is to detect a disease at the subclinical orpresymptomatic stage, in order to take appropriate action to reverse the effects, or the slowprogression of the disease towards the clinical status. In industry the objective is not only todetect adverse effects in employees, but also to relate the findings to the effectiveness ofexposure control measures.
The number of validated screening tests associated with exposure to hazardous metals issmaller than tests available in general preventive medicine. Target-organ toxicity associatedwith heavy metals is important to direct medical surveillance. Although interpretation criteriaare available for some of the tests, in many cases occupational health practitioners have todevelop pragmatic approaches in the context of the specific exposure scenario. TheRegulations for Hazardous Chemical Substances under the Occupational Health and Safety Actprovide some guidance for medical surveillance. The programme should include education ofemployers and employees about occupational hazards, placement of staff in positions that donot jeopardise their safety and health, early detection of adverse health effects, and referral ofindividuals for diagnostic confirmation and treatment.
Pre-placement medical evaluationPrior to placing a worker in a job with a potential for exposure, the occupational healthpractitioner or occupational medical practitioner should evaluate and document the worker’sbaseline health status with thorough medical, environmental, and occupational histories, aphysical examination and physiological and laboratory tests appropriate for the anticipatedoccupational risks. This is important even though the exposure may be within the regulatoryguidelines. A pre-placement medical evaluation is recommended in order to detect and assesspre-existing or concurrent conditions that may be aggravated or result in increased risk in otherrespects that may be associated with the exposure.

125
Periodic medical evaluation Workers with potential exposures to chemical hazards should be monitored in a systematicprogramme of medical surveillance intended to prevent or control occupational injury anddisease. Additional examinations may be necessary should a worker develop symptoms thatmay be attributed to exposure. The interviews, examinations and appropriate biological effectmonitoring and/or biological monitoring tests should be directed at identifying an excessive,decrease or adverse trend in the integrity and physiological function of the target organs. Thebaseline health status of the individual, trends in the occupational group, or data on a suitablereference population, serve as reference for comparison and interpretation. Again, the organsof the body that are vulnerable to the exposure determine the elements of the medicalscreening.
The programme should include education of employers and workers about work-relatedhazards, placement of workers in jobs that do not jeopardise their safety and health, earliestpossible detection of adverse health effects, and referral of workers for diagnostic confirmationand treatment.
Intrinsic to a medical surveillance programme is the dissemination of summary data to thosewho need to know, including employers, occupational health professionals, potentially exposedworkers, and regulatory and public health agencies.
The occurrence of disease (a “sentinel health event”, SHE) or other work-related adversehealth effects should prompt immediate evaluation of primary preventive measures, e.g.engineering controls, and personal protective equipment. A medical surveillance programme isintended to supplement, not replace such measures. A medical surveillance programme shouldinclude systematic collection and epidemiologic analysis of relevant environmental andbiological monitoring, medical screening, and morbidity and mortality data. This analysis mayprovide information about the relatedness of adverse health effects and occupational exposurethat cannot be discerned from results in individual workers. Sensitivity, specificity, andpredictive values of biological monitoring and medical screening tests should be evaluated onan industry-wide basis prior to application in any given work group.
Job transfer or termination evaluationThe medical, environmental and occupational history interviews, the physical examination, andselected physiological and laboratory tests which were conducted at the time of placement,should be repeated at the time of job transfer or termination. Any changes in the worker’shealth status should be compared to those expected for a suitable reference population.Because occupational exposure may cause diseases of prolonged induction-latency, the needfor medical surveillance may extend well beyond termination of employment.
3.4.4.2 Biological effect monitoringBiological effect monitoring determines the intensity of biochemical or physiological change dueto exposure, e.g. red cell cholinesterase for exposure to organophosphate pesticides, or zincprotoporphyrin (ZPP) for exposure to inorganic lead.
3.4.4.3 Biological monitoringTraditionally, exposure to hazardous substances in industry has been controlled by settingstandards for the concentration of pollutants in ambient air. This monitoring method considersonly exposure by the pulmonary route and, even for chemicals that enter the human bodymainly with the inspired air, it does not always reflect the true uptake of the exposed workers. Biological monitoring of exposure attempts to estimate the internal dose. It takes into accountabsorption by routes other than the lungs. The greatest advantage of biological monitoring isthe fact that the biological parameter of exposure is more directly related to the adverse healtheffect which one attempts to prevent than any environmental measurement. Therefore, it mayoffer a better estimate of risk than ambient monitoring. Because of its capability to evaluate the
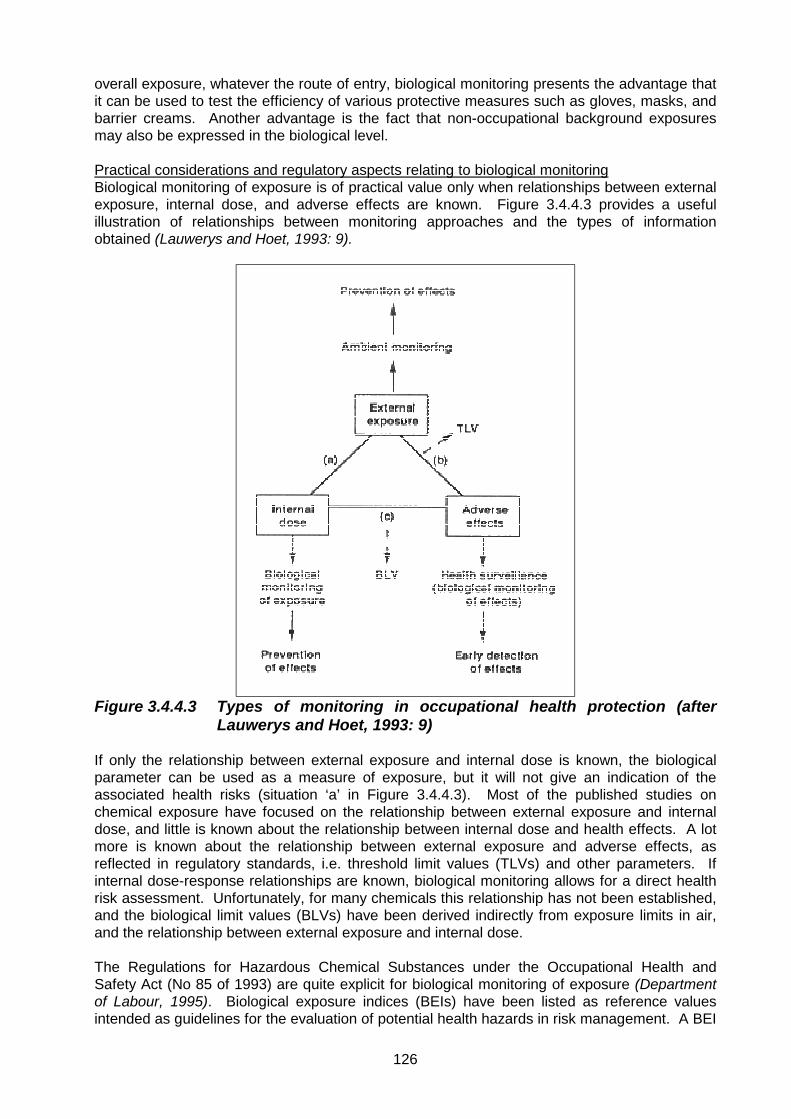
126
overall exposure, whatever the route of entry, biological monitoring presents the advantage thatit can be used to test the efficiency of various protective measures such as gloves, masks, andbarrier creams. Another advantage is the fact that non-occupational background exposuresmay also be expressed in the biological level.
Practical considerations and regulatory aspects relating to biological monitoringBiological monitoring of exposure is of practical value only when relationships between externalexposure, internal dose, and adverse effects are known. Figure 3.4.4.3 provides a usefulillustration of relationships between monitoring approaches and the types of informationobtained (Lauwerys and Hoet, 1993: 9).
Figure 3.4.4.3 Types of monitoring in occupational health protection (afterLauwerys and Hoet, 1993: 9)
If only the relationship between external exposure and internal dose is known, the biologicalparameter can be used as a measure of exposure, but it will not give an indication of theassociated health risks (situation ‘a’ in Figure 3.4.4.3). Most of the published studies onchemical exposure have focused on the relationship between external exposure and internaldose, and little is known about the relationship between internal dose and health effects. A lotmore is known about the relationship between external exposure and adverse effects, asreflected in regulatory standards, i.e. threshold limit values (TLVs) and other parameters. Ifinternal dose-response relationships are known, biological monitoring allows for a direct healthrisk assessment. Unfortunately, for many chemicals this relationship has not been established,and the biological limit values (BLVs) have been derived indirectly from exposure limits in air,and the relationship between external exposure and internal dose.
The Regulations for Hazardous Chemical Substances under the Occupational Health andSafety Act (No 85 of 1993) are quite explicit for biological monitoring of exposure (Departmentof Labour, 1995). Biological exposure indices (BEIs) have been listed as reference valuesintended as guidelines for the evaluation of potential health hazards in risk management. A BEI

127
in this context represents the level of a hazardous chemical substance or metabolite most likelyto be observed in a biological sample from a healthy individual who has been exposed to thesubstance to the same extent as another person with inhalation exposure to an OEL-TWA(occupational exposure limit - time-weighted average). This is a simplified approach, becausemany physicochemical and biological factors preclude the existence of such clear relationships.Great individual variation exists in the absorption rate of a chemical through the variousexposure routes.
Application of biological monitoring methodsA complete overview has been published by the U.S. National Institute for Occupational Safetyand Health (NIOSH) (1998: 52).Normally, where meaningful, pre-placement or baseline samples should be taken from allemployees that may be exposed to hazardous substances in their work environments. Totalbody burdens of all employees that may be exposed have to be determined annually
NIOSH recommends that biological monitoring be done at regular intervals, for example aninterval not exceeding every three months to at least 25 per cent of all employees that may besubject to the exposure. Participating workers at the same exposure level, selected insubgroups for monitoring, should be rotated to provide all workers the opportunity for analysisevery year.
Depending on the particular scenarios, sampling may be done in sets on a totally random basis,to include all possible events, some of which may be scheduled only on certain days. A set ofsamples is understood to be one pre-shift and one post-shift sample of biological fluid from aparticular person. Three sets of samples from unexposed workers (also pre-shift and post-shift) have to be collected as controls, and submitted for analysis with each batch of samplesfrom exposed workers.
List of biological exposure assessment methods
Table 3.4.4.3Analytical methods for biological monitoring
Element Agency Reference Analytical methodBlood or tissueAntimony, cadmium, chromium, cobalt,copper, iron, lead, manganese,molybdenum, nickel, platinum, silver, tin,titanium, zinc
NIOSH 8005 ICP-AES
UrineBarium, cadmium, chromium, copper,iron, Lead, manganese, molybdenum,nickel, platinum, silver, tin, titanium, zinc
NIOSH 8310 ICP-AES
Blood and urineLead NIOSH 8003 AA-F
3.4.4.4 Medical evaluation summary: procedures relevant to the various heavymetals
Table 3.4.4.4 presents a summary of procedures for medical surveillance, biological effectsmonitoring, and biological monitoring. The information should be used as a checklist, with theunderstanding that each item requires specialist knowledge for application and interpretation. The abbreviation APMSP (as per medical surveillance programme) refers to programmes thatshould be developed to address occupational health risk issues that are pertinent to specificexposure scenarios. It is not possible to design a generic medical surveillance programme forall the mineral processing industries.

128
Because medical surveillance and biological effect monitoring rely on a combination ofdiagnostic interpretations, it is beyond the scope of this investigation to provide comprehensiveguidelines for assessment in this field. Biological exposure indices are not listed in Table3.4.4.4, but it is shown for which substances BEI’s have been developed for application inSouth Africa. Only cadmium, chromium and mercury are listed in the Regulations forHazardous Chemical Substances under the Occupational Health and Safety Act (Department ofLabour, 1995). There are many complexities around the interpretation of biological monitoringdata. More information on biological monitoring for metal exposures and some interpretationsare discussed in the sections that deal with the individual mineral processing plants.

129
Table 3.4.4.4Summary of medical surveillance, biological effects monitoring, and biological monitoring
Code:B: BaselineAPMSP: As per medical surveillance programmeE: ExitSHE: Sentinal health eventP: Periodic (A: annual)
Medical surveillance Biological effect monitoring Biological monitoringHazardous substance
Item SHE Frequency Item Frequency Item\ Frequency
Antimony
SkinNose septumRespiratory
BEP
Chest X rayPulmonary function testKidney function testLiver function test
BAPMSP
UrineSerum
No BEI listed
BAPMSP
Arsenic
Hair lossP. neuritisEyesWeightNose septumSkin
BEP
Full blood countLiver function testPulmonary function test(Baseline CXR)
BAPMSP
Urine
BEI for urine
BAPMSP
Barium Sulphate Carbonate
SkinEar Nose Throat
BEP
Chest X rayPulmonary function testECG
BAPMSP
Urine
No BEI listed
BAPMSP
BerylliumSkin contactNose septumRespiratorySkin
BEP
Pulmonary function testLiver function testChest x-ray
BAPMSP
Urine
No BEI listed
BAPMSP
Bismuth inorganic(Mainly by ingestion)
Bismuth organic
Psychiatric BEP
Kidney testLiver function test If largequantities consumed
BAPMSP
Urine
Urine
No BEI listed
BAPMSP

130
Medical surveillance Biological effect monitoring Biological monitoring
Cadmium
DustFume
Nose septumAnosmiaRespiratory
BEP
Pulmonary function testChest X-rayLiver function testKidney function testsFull Blood Count(anaemia)Protein (Low MW)
BAPMSP
Urine
Blood
No BEI listed
BAPMSP
Calcium oxide
SkinLumpEyesNose SeptumVision
BEP
Pulmonary function testBaseline chest X-ray
BAPMSP
No BEI listed
BAPMSP
Chromium (VI)(III)
Nose septumSkinRespiratory
BEP
Chest X-rayPulmonary function testFull blood countKidney function testLiver
BAPMSP
UrineRed cells
BEI for urine,Cr(VI) and total Cr
BAPMSP
Cobalt
DustFume
Nose septumRespiratoryLiver function testSkinCVSKidney functiontest
BEP
Chest X-rayPulmonary function testLiver function testECG
BAPMSP
UrineBlood
No BEI listed
BAPMSP
Copper
Nose septumRespiratoryLiverSkinEyesWilson’s DiseaseKidney functiontest
BEP
BAPMSP
UrineSerum
No BEI listed
BAPMSP
Indium
Nose septumRespiratoryLiver/kidneySkin
BEP
BAPMSP
Urine
No BEI listed
BAPMSP
Iron
Oxide
Respiratory BEP
Pulmonary function testChest X-ray
BAPMSP
No BEI listed
BAPMSP

131
Medical surveillance Biological effect monitoring Biological monitoring
Lead
Radial nerveNeurologicalKidney functiontestReproductiveAnaemia
BEP
Full Blood Count (HB)ZPP
BAPMSP
UrineBlood
No BEI listed
BAPMSP
ManganesePsychologicalNeurologicalSpeech
BEP
Full blood countChest X-rayPulmonary function test
BAPMSP
UrineBloodNo BEI listed
BAPMSP
Mercury (inorganic)
NeurologicalPsychologicalSkinNeurologicalKidney functiontest
BEP
Kidney function testPulmonary function Test
BAPMSP
UrineBlood
BEI for blood andurine
BAPMSP
MolybdenumEyesRespiratory
BEP
Chest X RayPulmonary function Test
BAPMSP
Urine
No BEI listed
BAPMSP
Nickel
Skin allergiesRespiratory
BEP
Chest X RayPulmonary function TestSputum cytologySkin test
BAPMSP
Urine
No BEI listed
BAPMSP
Osmium (tetroxide)
EyeSkinRespiratoryKidney functiontest
BEP
Chest X-rayPulmonary function testSkin
BAPMSP
Urine
No BEI listed
BAPMSP
Platinum
AllergySkin/URTRespiratoryNose Septum
BEP
Chest X-rayPulmonary function testSkin
BAPMSP
Urine
No BEI listed
BAPMSP
Rhodium
AllergySkin/URTRespiratoryNose Septum
BEP
Chest X-rayPulmonary function testSkin
BAPMSP
Urine
No BEI listed
BAPMSP
Selenium
Compounds
SkinEyesNails
BEP
Chest X-rayPulmonary function testUrinalysisALT/AST/GGTFull blood count
BAPMSP
SerumUrine
No BEI listed
BAPMSP
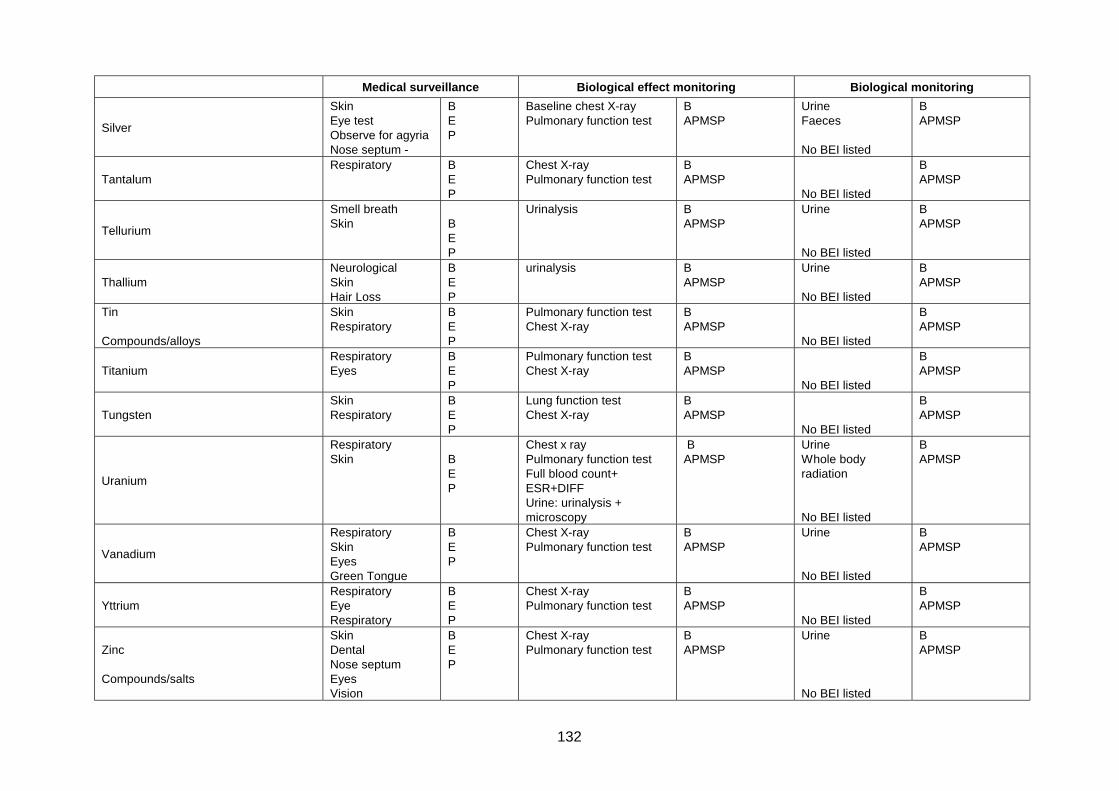
132
Medical surveillance Biological effect monitoring Biological monitoring
Silver
SkinEye testObserve for agyriaNose septum -
BEP
Baseline chest X-rayPulmonary function test
BAPMSP
UrineFaeces
No BEI listed
BAPMSP
TantalumRespiratory B
EP
Chest X-rayPulmonary function test
BAPMSP
No BEI listed
BAPMSP
Tellurium
Smell breathSkin B
EP
Urinalysis BAPMSP
Urine
No BEI listed
BAPMSP
ThalliumNeurologicalSkinHair Loss
BEP
urinalysis BAPMSP
Urine
No BEI listed
BAPMSP
Tin
Compounds/alloys
SkinRespiratory
BEP
Pulmonary function testChest X-ray
BAPMSP
No BEI listed
BAPMSP
TitaniumRespiratoryEyes
BEP
Pulmonary function testChest X-ray
BAPMSP
No BEI listed
BAPMSP
TungstenSkinRespiratory
BEP
Lung function testChest X-ray
BAPMSP
No BEI listed
BAPMSP
Uranium
RespiratorySkin B
EP
Chest x rayPulmonary function testFull blood count+ESR+DIFFUrine: urinalysis +microscopy
BAPMSP
UrineWhole bodyradiation
No BEI listed
BAPMSP
Vanadium
RespiratorySkinEyesGreen Tongue
BEP
Chest X-rayPulmonary function test
BAPMSP
Urine
No BEI listed
BAPMSP
YttriumRespiratoryEyeRespiratory
BEP
Chest X-rayPulmonary function test
BAPMSP
No BEI listed
BAPMSP
Zinc
Compounds/salts
SkinDentalNose septumEyesVision
BEP
Chest X-rayPulmonary function test
BAPMSP
Urine
No BEI listed
BAPMSP

133
Medical surveillance Biological effect monitoring Biological monitoringZirconium
Compounds
RespiratorySkin
BEP
Baseline chest X-rayPulmonary function test
BAPMSP
No BEI listed
BAPMSP

134
3.5 Risk characterisationHuman health risk characterisation is generally divided into the evaluation of carcinogenic andnon-carcinogenic risks.
Carcinogenic risks are interpreted in terms of excess lifetime cancer risks. In the occupationalexposure range the estimated cancer risk is assumed to be linear and proportional to dose. Risks are assumed to be additive per target organ across chemicals and pathways, unless dataare available that would support synergistic or antagonistic effects. Risks are expressed asexcess cancer risk, i.e. risk not taking into account any existing risk as a result of backgroundexposure to substances that have the same carcinogenic properties. Unit cancer risk factorsderived for lifetime exposure (70 years) are adjusted for 30 years’ exposure, following theapproach outlined by Hallenbeck (Hallenbeck, 1993: 102). This is based on the assumptionthat exposure over an occupational lifetime of 30 years covers the latency period of thecarcinogen. The excess cancer risk is calculated as follows:
Excess risk = C1(URF1) + C2(URF2) + ...........+ Cn(URFn)
where the excess risk refers to a particular target organ, and Ci(URFi) refers to the exposureconcentration of substance i multiplied by the unit risk factor for that compound, URFi. It isassumed that substances 1 to i all have carcinogenic effects on the same endpoint.
Noncarcinogenic risks are evaluated by comparison with reference concentrations. If the ratioof the air concentration to the reference concentration (hazard quotient) exceeds one, there is apotential that adverse health effects may occur. For multiple chemical exposures, hazardquotients are summed per target organ, unless data are available to demonstrate synergistic orantagonistic effects. This is based on the assumption that the response of a target organ tomultiple toxic agents is additive in a linear relationship. It is measured in terms of a hazardindex (HI), which is the sum of the hazard quotients (HQ’s) for the individual substances, (i).
Hazard Index (HI) = HQ1 + HQ2 + ......... + HQn
where the hazard quotients HQi = Intake of substance i / reference dose for substance i,where i = 1, 2, ........ , n.
3.6 ReferencesACGIH, 2000. Threshold Limit Values for Chemical Substances and Physical Agents, &Biological Exposure Indices. ACGIH, Cincinnati, OH.
Asante-Duah, D. K. 1996. Management of Contaminated Site Problems. Boca Raton: LewisPublishers, 407p.
ASOSH, 2000. World links, http://www.asosh.org.
Benson, J. M. & Zelikoff, J. T. 1996. Respiratory Toxicology of Metals. (In: Chang, L. W. et al.Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 929 - 930).
Berlin, M 1979a. Mercury. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 503 - 530).
Berlin, M. & Nordman, C. 1979b. Titanium. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 627 - 636).

135
Berlin, M & Rudell, B. 1979c. Uranium. (In: Friberg, L, et al. Handbook on the Toxicology ofMetals. Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 647 - 658).
Bhattacharyya, M. H., Jeffery, E. & Silbergeld, E. K. 1996. Bone Metabolism: Effects ofEssential and Toxic Trace Metals. (In: Chang, L. W. et al. Toxicology of Metals. Boca Raton:CRC Lewis Publishers, p. 959 - 971).
Calabrese, E.J. & Kenyon, E.M. 1991. Air Toxics and Risk Assessment. Chelsea, Michigan:Lewis Publishers, 662p.
Chang, L. W., Magos, L. & Suzuki, T., Editors 1996. Toxicology of Metals. Boca Raton:CRC Lewis Publishers, 1198p.
Cohen, M. D., Bowser, D. H. & Costa, M. 1996. Carcinogenicity and Genotoxicity of Lead,Beryllium, and Other Metals. (In: Chang, L. W. et al. Toxicology of Metals. Boca Raton: CRCLewis Publishers, p. 253 - 284).
Corbella, J. & Domingo, J. L. 1996. Developmental and Reproductive Effects of Aluminium,Manganese, Uranium and Vanadium. (In: Chang, L. W. et al. Toxicology of Metals. BocaRaton: CRC Lewis Publishers, p. 1083 - 1095).
Costa, M. 1996. Mechanism of Nickel Genotoxicity and Carcinogenicity. (In: Chang, L. W. etal. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 245 - 251)
Cross, H.J., Faux, S.P., Sadhra, S., Sorahan, T., Levy, L.S., Aw, T.C., Braithwaite, R.,McRoy, C., Hamilton, L. & Calvert, I. 1997. Criteria Document for Hexavalent Chromium.International Chromium Development Association. Birmingham, U.K.: Institute for OccupationalHealth, University of Birmingham, Edgebaston, 324 p.
Department of Labour, 1995. Occupational Health and Safety Act, 1993. Regulations forHazardous Chemical Substances. Pretoria: Government Notice No R 1179 of 25 August 1995.
Dr≅≅≅≅ ger 1997. Dr≅ ger-Tube Handbook. Lübeck, Germany: Dr≅ gerwerk Aktiengesellschaft,365p.
Doull, J., Klaassen C. D. & Amdur, M. O. 1980. Casarett and Doull’s Toxicology. New York:Macmillan Publishing Co., Inc., 778p.
Elinder, C-G. & Friberg, L. 1979a. Antimony (In: Friberg, L, et al. Handbook on theToxicology of Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 283 - 292).
Elinder, C-G. & Friberg, L. 1979b. Cobalt. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 399 - 410).
Elinder, C-G. & Piscator, M., 1979c. Iron. (In: Friberg, L, et al. Handbook on the Toxicology ofMetals. Amsterdam : Elsevier/North-Holland Biomedical Press, p. 435 - 450).
Elinder, C-G. & Piscator, M. 1979d. Zinc. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 675 - 685).
EPRI, 1994a. Electric Utility Trace Substances Synthesis Report: Volume 4: Appendix P,Toxicology Profiles. Arsenic. Electric Power Research Institute. Alameda, California: ENSRConsulting, pages not numbered.

136
EPRI, 1994b: Electric Utility Trace Substances Synthesis Report : Volume 4: Appendix P,Toxicology Profiles. Beryllium. Electric Power Research Institute. Alameda, California: ENSRConsulting, pages not numbered.
Fowler, B. A., Ishinishi, N., Tsuchiya, K. & Vahter, M. 1979a. Arsenic (In: Friberg, L, et al.Handbook on the Toxicology of Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press,p. 283 - 292).
Fowler, B. A. & Vouk, V. 1979b. Bismuth. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 345 - 353).
Fowler, B. A. 1979c. Indium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 429 - 434).
Fowler, B. A. & Nordberg, G. F. 1979d. Silver. (In: Friberg, L, et al. Handbook on theToxicology of Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 580 - 586).
Fowler, B. A., & Nordberg, M. 1996e. Biomarkers of Metal-Induced Nephrotoxicity. (In:Chang, L. W. et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 759 - 763)
Fowler, B.A. 1996f. The Nephropathology of Metals (In: Chang, L. W., et al. Toxicology ofMetals. Boca Raton: CRC Lewis Publishers, p. 721 - 729).
Friberg, L., Nordberg, G.F. & Vouk, V. B., Editors 1979. Handbook on the Toxicology ofMetals. Amsterdam: Elsevier/North-Holland Biomedical Press, 709p.
Friberg, L., Kjellström, T., Nordberg, G. & Piscator, M. 1979a. Cadmium. (In: Friberg, L, etal. Handbook on the Toxicology of Metals. Amsterdam: Elsevier/North-Holland BiomedicalPress, p. 355 - 381).
Friberg, L. 1979b. Molybdenum. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 531 - 539).
Garcia-Vargas, G. G. & Cebrian, M. E. 1996. Health Effects of Arsenic. (In: Chang, L. W. etal. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 423 - 438).
Gerhardsson, L. & Skerfving, S. 1996. Concepts on Biological Markers and Biomonitoring forMetal Toxicity. (In: Chang et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p.81 - 107).
Glover, J., Levander, O., Parizek, J. & Vouk, V. 1979a. Selenium. (In: Friberg, L, et al.Handbook on the Toxicology of Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press,p 556 - 577).
Glover, J. R. & Vouk, V. 1979b. Tellurium. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 585 - 598).
Hall, K.S., Chakraborty, J. & Ruch, R. J. 1996. Chemical exposure and toxic responses.Boca Raton: CRC Lewis Publishers. 288p.
Hallenbeck, W. H. 1993. Quantitative Risk Assessment for Environmental and OccupationalHealth. Boca Raton: Lewis Publishers, 224p.
Hamada, R. & Osame, M. 1996. Minamata Disease and Other Mercury Syndromes. (In:Chang, L. W. et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 337- 351).

137
HHMI, 2000. LCSS: Osmium tetroxide. HHMI Laboratory Safety, National Academy ofSciences. http://www.grc.com/hhmi/science/labsafe/lcsstxt/lcsstx64.html.
Hrudey, S. E., Chen, W. & Rousseaux, C. G. 1996. Bioavailability in Environmental RiskAssessment. Boca Raton: CRC Lewis Publishers, 294p.
IARC. Monographs Series, Volumes 1 – 74. Overall Evaluations of Carcinogenicity toHumans. International Association for Research on Cancer.http://193.51.164.11/monoeval/crthall.html.
Inoue, N. & Makita, Y. 1996. Neurological Aspects in Human Exposure to Manganese. (In:Chang, L. W. et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 415 - 421).
IRIS (Integrated Risk Information System), 1999. Environmental Protection Agency (EPA).USA. http://www.epa.gov/iris/index.html.
Kazantzis, G. 1979a. Thallium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 599 - 612).
Kazantzis, G. 1979b. Tungsten. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 637 - 646).
Keen, K. L. 1996. Teratogenic Effects of Essential Trace Metals : Deficiencies and Excesses.(In: Chang et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 977 - 1001).
Kimber, I. & Basketter, D. A. 1996. Contact Hypersensitivity to Metals. (In: Chang, et al.Toxicology of Metals. Boca Raton : CRC Lewis Publishers, p. 827 - 833).
Klein, C. B. 1996. Carcinogenicity and Genotoxicity of Chromium. (In: Chang, et al. Toxicologyof Metals. Boca Raton: CRC Lewis Publishers, p. 205 - 215)
K&M Environmental, 1996. ChromAir Direct Read Passive Monitoring System for Mercury. Virginia: K&M Environmental Air Sampling Systems. Brochure.
Kusaka, Y. 1993. Occupational diseases caused by exposure to sensitizing metals. SangyoIgaku, 35 (ISS2): 75-87.
Kusaka, Y. 1996. Cobalt and Nickel-Induced Hard Metal Asthma. (In: Chang, et al. Toxicologyof Metals. Boca Raton: CRC Lewis Publishers, p. 461 -468) .
Langard, S. & Norseth, T. 1979. Chromium. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 383 -397).
Lauwerys, R. R. & Hoet, P. 1993. Industrial Chemical Exposure. Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: CRC Lewis Publishers, 318p.
Leonard, A & Gerber, G B, 1996. Mutagenicity, Carcinigenicity and Teratogenicity ofAntimony Compounds. Mutation Research, 366 (1): p. 1 - 8.
Lewis, R. L., Editor. 1995. SAX’s Dangerous Properties of Industrial Materials. Ninth Edition.New York: Van Nostrand Reinhold, CD ROM Edition.
Nieminen, A-L, & Lemasters, J. J. 1996. Hepatic Injury by Metal Accumulation. (In: Chang etal. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 887 - 899).

138
NIOSH 1977. Occupational Exposure Sampling Strategy Manual. Cicinnati: U.S. Departmentof Health, Education, and Welfare, 131p.
NIOSH 1998. Application of Biological Monitoring Methods. NIOSH Manual of AnalyticalMethods. National Institute for Occupational Safety and Health.
Norseth, T & Piscator, M. 1979. Nickel. (In: Friberg, L, et al. Handbook on the Toxicology ofMetals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 541 - 553).
Patrick, D. R. 1994. Toxic Air Pollution Handbook. Air and Waste Management Association.New York: Van Nostrand Reinhold, 588p.
Piscator, M. 1979a. Copper. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 411 - 420).
Piscator, M. 1979b. Manganese. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 485 - 501).
Piscator, M. 1979c. Tin. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 613 - 626).
Poirer, L. A., & Littlefield, N. A. 1996. Metal Interactions in Chemical Carcinogenesis (In:Chang et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 290 - 291).
Reeves, A. L. 1979a. Barium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 321 - 328).
Reeves, A. L. 1979b. Beryllium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 329 - 343).
Romero, I. A., Abbott, N. J. & Bradbury, M. W. B. 1996. The Blood-Brain Barrier in NormalCNS and in Metal-Induced Toxicity. (In: Chang et al. Toxicology of Metals. Boca Raton: CRCLewis Publishers, p. 561 - 585).
Sharma, R. P. & Dugyala, R. R. 1996. Effects of Metals on Cell-Mediated Immunity andBiological Response Modulators. (In: Chang et al. Toxicology of Metals. Boca Raton: CRCLewis Publishers, p. 785 -796).
Toxline database. http//:www.nlm.nih.gov.
Tsuchiya, K. 1979. Lead. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 451 - 484).
Van der Voet, G. B. & de Wolff, F. A. 1996. Human Exposure to Lithium, Thallium, Antimony,Gold and Platinum. (In: Chang, L. W., et al. Toxicology of Metals. Boca Raton: CRC LewisPublishers, p. 457 - 458).
Vouk, V. 1979a. Indium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 429 - 434).
Vouk, V. 1979b. Vanadium. (In: Friberg, L, et al. Handbook on the Toxicology of Metals.Amsterdam: Elsevier/North-Holland Biomedical Press, p. 659 - 674).
WHO, 1987: Air quality guidelines for Europe. WHO Regional Publications, European SeriesNo. 23. Copenhagen: World Health Organisation Regional Office for Europe.
139
WHO 1993. International Programme on Chemical Safety. Guidelines for drinking waterquality. Second Edition, Vol. 2. Health criteria and other supporting information. Geneva: WorldHealth Organisation.
Yamauchi, H. & Fowler, B. 1996. Metal-Induced Alterations in Renal Gene Expression. (In:Chang, L. W., et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 751 - 757).
Zelikoff, J. T. & Smialowicz, R. L. 1996. Metal-induced Alterations in Innate Immunity. (In:Chang, L. W., et al. Toxicology of Metals. Boca Raton: CRC Lewis Publishers, p. 811 - 826).
Zheng, W. 1996. Choroid Plexus and Metal Toxicity. (In: Chang, L. W., et al. Toxicology ofMetals. Boca Raton: CRC Lewis Publishers, p. 811 - 826).

140

141
4 Carbon steel process with blast furnace and basicoxygen furnace
4.1 IntroductionThis section provides a process description and process diagram of a typical carbon steelprocess employing a blast furnace (BF) and basic oxygen furnace (BOF). The processdescription and process diagram contain data on the process streams and identify thehazardous substances as well as potential exposure points.
Trace elements are commonly distributed in processes according to the following classification(Clarke, 1993: 731):
Group 1 elements are concentrated in coarse residues or may be equally partitioned betweencoarse residues and finer particles. The following elements are in this category:Eu, Hf, La, Mn, Rb, Sc, Sm Th, Zr
Group 2 elements are often volatilised in the process, but may condense downstream. Theyare concentrated in finer particles that may escape particulate control systems. Group 2elements are:As, Cd, Ga, Ge, Pb, Sb, Sn, Te, Ti, Zn
There is considerable overlap between the groups, as shown by the number of elements thatfall into more than one group. Elements classifiable into groups 1 and 2 are:Ba, Be, Bi, Co, Cr, Cs, Cu, Mo, Ni, Sr, Ta, U, V, W
Group 3 elements are the most volatile and are depleted in all solid phases and may remain inthe gas phase during passage through the plant. These include:Hg, Br, Cl, F, Rn
Elements classifiable into groups 2 and 3 are:B, Se, I
Although very generalised, this classification provides some idea of the overall distribution ofmetals in various parts of an industrial process.
4.2 Process descriptionThis section provides a process description and process diagram of a typical production facilityfor carbon steel with blast furnace and basic oxygen furnace. The process description andprocess diagram contain data on the process streams and identify the hazardous substancesas well as potential exposure points.
4.2.1 Coke preparationCoke is produced by heating coal lumps up to a temperature of 1 500 oC which is thenmaintained for a period of 24 hours. This is carried out in the controlled atmosphere ofexternally heated coke oven batteries. The product is then rapidly cooled in a stream of coldwater, screened, dried, and transferred to storage ready for feeding to the blast furnace. Coalconsumption is in the range of 1,5 t per t of coke produced. Gas from the coke oven is used toheat the oven, as well as a number of heat-treatment and re-heat furnaces. The flue gas fromthe furnaces is dry- and/or wet-scrubbed before venting to the stack.
Waste slurry from the scrubber contains phenols, cyanides, sulphides and ammonia.

142
The slurry/dust from the scrubber is either transferred to the sinter and/or the pelletising plant,or is dumped.
Table 4.2.1Coke preparation
Stream Component Typical flow Heavy metals Exposure
Dust from coke ovenTotalCoal dustFly ash (containingmainly SiO2,Al2O3 and carbon)
1 kg/t0,6 kg/t0.4 kg/t
Ash contains 2%trace elements asmetals, chlorides andoxides
Coke oven area/dustcollection
Flue gas
GasDust(containing mainlySiO2
and Al2O3)SO2
NOx
1 500 m3/t0,4 kg/t
0,1 kg/t0,23 kg/t
Dust contains 1%trace elements,mainly as oxides
Stack
Waste water/dust exscrubber
Waste(mainly SiO2and Al2O3)NH3
CN-
S2-
Trace elements
0,35 m3/t
2,8 kg/t0,2 kg/t0,02 kg/t0,001 kg/t
Solids contain traceelements mainly asoxides
Scrubber waste
4.2.2 SinteringSinter is produced by firing a mixture of coke breeze, iron ore fines, lime and/ or dolomite on asinter machine. The sinter is conveyed to storage prior to feeding to the blast furnace.Gas/fume from the sintering machine is wet-scrubbed before being vented to the stack.The residue from the scrubber goes back to the sinter machine, or to the pelletiser, or to awaste site.
Table 4.2.2Sintering
Stream Component Typical flow Heavy metals Exposure
Dust from sinteringmachine
Total dustFine oreResidualsCoke finesReturning finesFluxesDust also containsSiO2 andCaO
0,8 kg/t0,48 kg/t0,05 kg/t0,1 kg/t
0,12 kg/t0,05 kg/t
Fine ore containsmainly Fe2O3
And FeO with 0,1%trace elements asoxides.Residuals contain 1–2% trace elementsas oxides.Fluxes containCaO and 0,1% traceelements as oxides
Sinter machine
Iron ore dust See later See later See later Sinter machine

143
Stream Component Typical flow Heavy metals Exposure
Flue gas dustTotal dustFine oreFly ashFluxes
0,24 kg/t0,08 kg/t0,14 kg/t0,02 kg/t
Fine ore contains0,1% trace elementsas oxides.
Fly ash contains 2%trace elements asoxides.
Fluxes contain CaOand 0,1% traceelements as oxides.
Stack
Lime TotalCaOSiO2
MgOFeOTE
0,1 kg/t95%1%0,4%
0,1%
CaO, FeO, traceelements as oxides
Lime make-up
Scrubber effluent TotalSludgeOrganicsNH3
S2-
CN-
0,1 m3/t0,4 kg/t0,1 kg/t0,1 kg/t0,001 kg/t0,001 kg/t
Sludge contains mainly FeO, Fe2O3,CaO, and 0,1% traceelements as oxides
Scrubber effluent
4.2.3 Storage/blending/material handlingThe main iron ore feed is delivered into storage bins together with coke and sinter, prepared asdescribed above. Material handling facilities are provided to feed the required blend of theseconstituents to the blast furnace.
Table 4.2.3Storage, blending and material handling
Stream Component Typical flow Heavy metals Exposure
Iron ore feed/dust
TotalFe2O3
SiO2
Al2O3
MgOTrace elements
0,008 kg/t94%4%1%1%0,1%
Fe2O3
Trace elements asoxides
Storage area
4.2.4 Blast furnace treatmentIn the blast furnace, iron units are added as lump ore, pellets and sinter. Coke is added inlayers which alternate with the iron ore layers. Pulverised coal, together with preheated air at1 000 oC, which is enriched with two per cent oxygen, is blown into the furnace through tuyereswhich are placed above the furnace hearth. The top gas is used to heat furnace stoves inwhich the air blast is preheated. Hot metal and slag are regularly tapped from the hearth ataround 1 465 oC. The hot metal, which usually contains around 4.5 per cent C, 0.5 per cent Si,0.05 per cent S and 0.03 per cent P, is further refined as described below to control the leveland shape of S and P contaminants.
Blast furnace slag is granulated and removed from the plant and may be used in the buildingindustry.
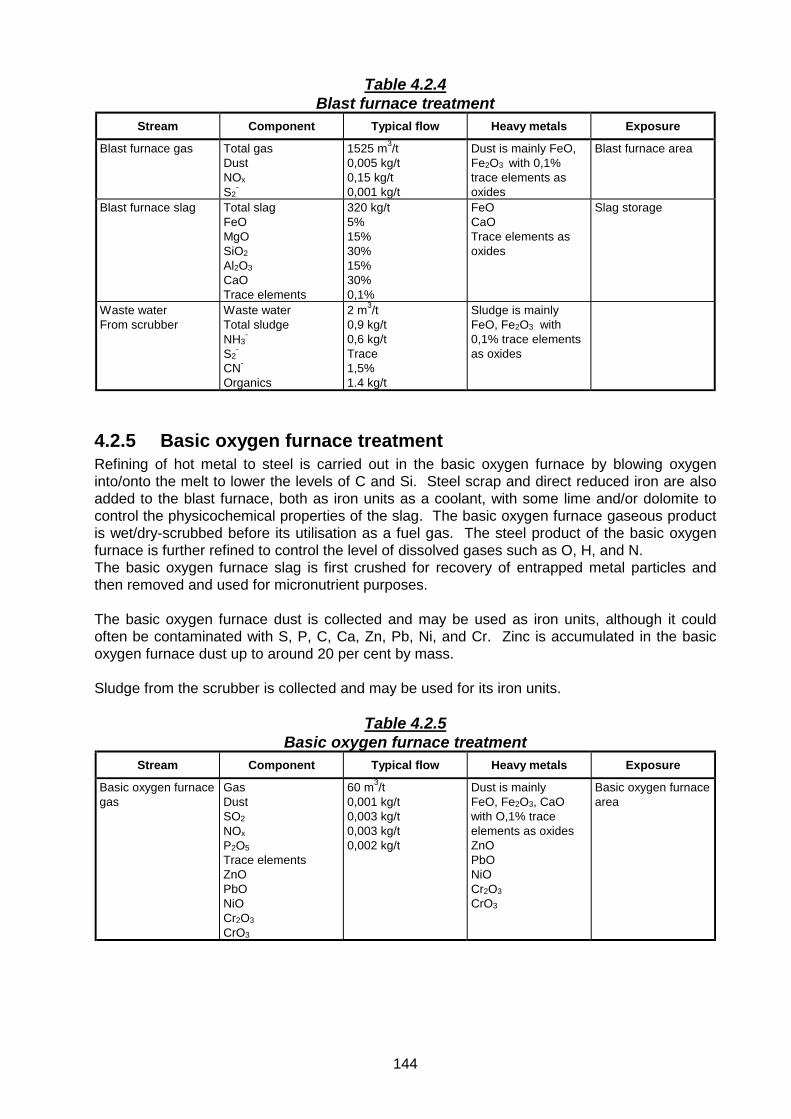
144
Table 4.2.4Blast furnace treatment
Stream Component Typical flow Heavy metals Exposure
Blast furnace gas Total gasDustNOx
S2-
1525 m3/t0,005 kg/t0,15 kg/t0,001 kg/t
Dust is mainly FeO,Fe2O3 with 0,1%trace elements asoxides
Blast furnace area
Blast furnace slag Total slagFeOMgOSiO2
Al2O3
CaOTrace elements
320 kg/t5%15%30%15%30%0,1%
FeOCaOTrace elements asoxides
Slag storage
Waste waterFrom scrubber
Waste waterTotal sludgeNH3
-
S2-
CN-
Organics
2 m3/t0,9 kg/t0,6 kg/tTrace1,5%1.4 kg/t
Sludge is mainlyFeO, Fe2O3 with0,1% trace elementsas oxides
4.2.5 Basic oxygen furnace treatmentRefining of hot metal to steel is carried out in the basic oxygen furnace by blowing oxygeninto/onto the melt to lower the levels of C and Si. Steel scrap and direct reduced iron are alsoadded to the blast furnace, both as iron units as a coolant, with some lime and/or dolomite tocontrol the physicochemical properties of the slag. The basic oxygen furnace gaseous productis wet/dry-scrubbed before its utilisation as a fuel gas. The steel product of the basic oxygenfurnace is further refined to control the level of dissolved gases such as O, H, and N.The basic oxygen furnace slag is first crushed for recovery of entrapped metal particles andthen removed and used for micronutrient purposes.
The basic oxygen furnace dust is collected and may be used as iron units, although it couldoften be contaminated with S, P, C, Ca, Zn, Pb, Ni, and Cr. Zinc is accumulated in the basicoxygen furnace dust up to around 20 per cent by mass.
Sludge from the scrubber is collected and may be used for its iron units.
Table 4.2.5Basic oxygen furnace treatment
Stream Component Typical flow Heavy metals Exposure
Basic oxygen furnacegas
GasDustSO2
NOx
P2O5Trace elementsZnOPbONiOCr2O3
CrO3
60 m3/t0,001 kg/t0,003 kg/t0,003 kg/t0,002 kg/t
Dust is mainlyFeO, Fe2O3, CaOwith O,1% traceelements as oxidesZnOPbONiOCr2O3
CrO3
Basic oxygen furnacearea

145
Stream Component Typical flow Heavy metals Exposure
Basic oxygen furnaceslag
Total slagFeOSiO2
CaOAl2O3MgOTrace elements
150 kg/t25%18%32%10%10%0,1%
FeOCaOTrace elements asoxides
Slag storage area
Waste water/dustFrom scrubber
TotalSludgeFe2O3/FeOCaOSiO2
Al2O3
MgOCSTrace elementsTrace elementsZnO, PbO,NiO, Cr2O3,
CrO3
0,1 m3/t1 kg/t45%30%5%3%10%4%3%0,1%
Fe2O3FeOCaOZnOPbONiOCr2O3
CrO3Trace elements asoxides and chlorides
Scrubber effluent
Lime As before As before As before Lime storage/handling
Flux TotalCaOMgOSiO2
FeOTE
0,07 kg/t47%48%3%2%0,1%
CaOFeOTrace elements asoxides
Flux storage area
4.2.6 Further refining, casting, rolling, pickling, galvanisingThe refining of hot metal and steel for the removal of S and P may be carried out in a torpedoor transfer ladle. The agents used are usually a mix of Mg powder, calcium carbide, sodiumoxide and lime in an oxidising atmosphere (sodium carbonate is commonly used as a source ofsodium oxide). The use of sodium oxide is limited because the reduction of sodium oxide bythe carbon in the melt produces large amounts of sodium fume.
De-oxidation of the steel is usually performed by inserting aluminium wires in the melt in a ladleor crucible.
De-gassing of steel to remove dissolved nitrogen and/or hydrogen may be carried out in a re-heat furnace or by argon arc stirring under vacuum.
Steel ingots are usually abrasion ground and heated in a re-heat furnace before sending themto the rolling mills, although continuous casters accept hot molten steel.
Mill scale from the rolling mills is internally used for iron units.
Pickling is carried out using hydrochloric or sulphuric acid, using an amine-based reagent as aprotector, before hot galvanisation of steel products in zinc melt.

146
Table 4.2.6Further refining, casting, rolling, pickling, galvanising
Stream Component Typical flow Heavy metals Exposure
Dust/fume fromrefining
TotalDesulph.: CO/CO2 SO2
CaO TEDephos.:CO/CO2 SO2
CaO Trace elements
0,001 kg/t
20%40%40%0,1%
40%40%20%0,2%
Dust contains mainlyFeO and CaO withTE as metals, MnSand other sulphides
Dust contains mainlyFeO and CaO withtrace elements asoxides
Finishing area
Pickle liquors 0,0001 kgH2SO4
HCl
0,0001 kg/tH2SO4
HCl
Iron sulphates orchloridesand trace elements
Finishing area
Calcium carbide TotalCCaTrace elements
1 kg/t25%75%0,2%
CaC2
Trace elements asmetals
Finishing area
Lime TotalCaOSiO2
MgOFeOTrace elements
0,1 kg/t95%1%0,4%
0,1%
CaOFeOTrace elements asoxides
Reagent make-uparea
Galvanising fume Zn 80% Zn0,1% trace elementsaschlorides andsulphides
Finishing area
4.3 Process diagramThe process diagram for the carbon steel process with blast furnace and basic oxygen furnaceis shown in Figure 4.3.
4.4 Process assessment
4.4.1 Hazard identificationExposure to dust is a primary concern in this industry. Exposure to iron oxide (Fe2O3) presentas a major constituent in the feed material, and consequently the dust, is controlled byregulations at a level of 5-mg Fe/m3.
The other substances of interest are calcium oxide and zinc oxide. Following the guidance inTable 3.4.2, calcium oxide may be present at levels higher than 20 per cent in basic oxygenfurnace slag, and zinc has to be assessed as fumes in the galvanising area.
Other metals present at trace levels would be significant only in quantities that exceed theirindividual threshold limits. It appears unlikely that the carbon steel process has the potential torelease heavy metals other than those identified above into air at any significant levels.

147
Figure 4.3 Process diagram for the carbon steel process with blast furnaceand basic oxygen furnace.

148
4.4.2 Toxicological assessmentIron oxide is not considered to be inert dust (particulates not otherwise classifiable), becauseinhalation may lead to effects known as siderosis, iron pneumoconiosis, hematitepneumoconiosis, and iron pigmentation of the lung. It appears that the pulmonary effects aresomewhat more serious than those caused by inert dust. Systemic effects relating to excessivehaemosiderin deposits have also been documented. It has not been proved that iron oxidesare carcinogenic following chronic pulmonary exposure. The toxicity of iron and its compoundshas been discussed in Section 3.3.4.12.
Calcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicology of calcium oxide has been discussed in Section 3.3.4.7.
The toxicity of zinc has been discussed in Section 3.3.4.32.
4.4.3 Exposure assessmentExposure to dust containing iron oxide may occur in areas where iron ore is handled, at thesinter machine, and at the blast furnace. Sampling and analytical methods for airborne ironhave been listed in Table 3.4.2.6. There is no biological monitoring method to assess exposureto iron, because iron is an essential element present in the human body.
Exposure to calcium may occur at the lime storage and handling area, in slag from the basicoxygen furnace, and in flux. Sampling and analytical methods have been listed in Table 3.4.2.6for calcium. Biological monitoring would not give an indication of exposure because of the largebody burden of calcium.
Exposure to zinc may be possible in the final galvanising steps. The most widely knownsystemic effect resulting from acute inhalation of freshly formed zinc oxide fumes is a diseasecalled metal fume fever. Table 3.4.2.6 lists sampling and analytical methods for zinc oxide. Zinc is an essential element and is present in abundance in various parts of the human body.Biological monitoring would therefore not provide useful information for exposure assessment.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
4.4.4 Risk quantificationIn controlling exposure to iron oxide, it is not adequate to control dust levels to 10 mg/m3,because the level of iron may be above 5 mg/ m3 at particulate levels slightly lower than 10 mgtotal dust/m3.
Because of its irritation effects, exposure to calcium oxide should be assessed againstmaximum concentration peaks rather than average values.
For exposure to zinc oxide, the concentration at which metal fume fever would develop is notentirely certain, but it has been estimated that symptoms are unlikely to develop at airconcentrations below 15 mg/m3 (Elinder & Piscator, 1979: 682). The ACGIH guidelines of 5mg/m3 for zinc oxide fume and 10 mg/m3 for zinc oxide dust therefore provide adequatemargins of safety.
4.5 ReferencesClarke, L.B. 1993. The fate of trace elements during coal combustion and gasification: anoverview. Fuel, 72 (6):731 - 736.

149
Elinder, C-G. & Piscator, M. 1979d. Zinc. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/ North-Holland Biomedical Press, p. 675 - 685).
Peacey, J.G. & Davenport W.G. 1979. The iron blast furnace: theory and practice. Oxford:Pergamon, 251p.
Von Bogdandy, L. & Engell, H.J. 1971. The reduction of iron ores; scientific basis andtechnology. Dusseldorf: Verlag Stahleissen, 592p.

150

151
5 Carbon steel process with direct reduced iron andelectric arc furnace
5.1 IntroductionA process description and flow diagram of a typical carbon steel process involving the directreduced iron (DRI) process and electric arc furnace (EAF) are included in this section. Theprocess description and flow diagram contain data on the process streams and identify the toxicsubstances as well as the potential exposure points.
Trace elements are commonly distributed in processes according to the following classification(Clarke, 1993: 731):
Group 1 elements are concentrated in coarse residues or may be equally partitioned betweencoarse residues and finer particles. The following elements are in this category:Eu, Hf, La, Mn, Rb, Sc, Sm Th, Zr
Group 2 elements are often volatilised in the process, but may condense downstream. Theyare concentrated in finer particles that may escape particulate control systems. Group 2elements are:As, Cd, Ga, Ge, Pb, Sb, Sn, Te, Ti, Zn
There is considerable overlap between the groups, as shown by the number of elements thatfall into more than one group. Elements classifiable into groups 1 and 2 are:Ba, Be, Bi, Co, Cr, Cs, Cu, Mo, Ni, Sr, Ta, U, V, W
Group 3 elements are the most volatile and are depleted in all solid phases and may remain inthe gas phase during passage through the plant. These include:Hg, Br, Cl, F, Rn
Elements classifiable into groups 2 and 3 are:B, Se, I
Although very generalised, this classification provides some idea of the overall distribution ofmetals in various parts of an industrial process.
5.2 Process descriptionThis section provides a process description and process diagram of a typical production facilityfor carbon steel with direct reduced iron and electric arc furnace. The process description andprocess diagram contain data on the process streams and identify the hazardous substancesas well as potential exposure points.
5.2.1 GrindingIron ore fines, together with additives are continuously ground in a ball mill prior to pelletisation.
Table 5.2.1Grinding
Stream Component Typical flow Heavy metals ExposureOre fines/dust See “lump ore” See “lump ore” See “lump ore” Grinding area

152
5.2.2 PelletisationGround ore fines are mixed with recycled sludge from the slimes dam and bentonite and arethen mixed with water using a paddle mixer. The mixtures are fed to a pelletiser typicallycomprising a rotating disc or drum which pelletises the moist mix into 10 to 25 mm diameterpellets. Wet pellets may be continuously dried in a drier heated by hot gas or fuel burner toabout 120 to 150 °C.
Table 5.2.2Pelletisation
Stream Component Typical flow Heavy metals ExposureFlue gas Gas
DustSO2
NOxTrace elementsin dust
2 500 m3/t0,125 kg/t0,05 kg/t0,25 kg/t0,1%
Mainly Fe2O3, Trace elementsas oxides
Pelletiser area
Waste water SludgeTrace elements
0,95 kg/t0,1%
Mainly Fe2O3,Trace elementsas oxides
Slimes dam
5.2.3 Direct reductionPelletised iron ore, lump ore, coal, and dolomite are fed to rotary kilns where reduction takesplace. Carbon monoxide forms during the reaction. Air is blown into the freeboard of the kiln ateight positions to combust the CO gas and the volatile matter that rise from the bed so that thebed temperature remains at around 1 000 oC. The product is a solid-state reduced iron, and iscalled sponge iron (SI) or directly reduced iron (DRI).
The product from the rotary kiln is cooled, magnetically separated from the ash and char,screened, and sent to the melt-shop. The gaseous byproduct of the kiln is further combusted ina steam boiler, then scrubbed, and finally vented to the stack.
Wastewater is treated in a number of thickeners, using various types of flocculant for removalof the solids as slimes. The slimes are partially de-watered in the slimes dam and recycled tothe pelletising plant. The slimes-dam water is recycled back to the circuit for re-use. Solids arerecycled from the thickener or, occasionally, from the dam.
Table 5.2.3Direct reduction
Stream Component Typical flow Heavy metals Exposure
Lump ore/dust TotalFe2O3
SiO2Al2O3
MgOTraceelements
0,001 kg/t94%4%1%1%0,1%
Fe2O3,Trace elementsas oxides
Ore storage/feed system
Dust from kilns TotalFeOSiO2
Al2O3MgOCaOCTraceelements
0,02 kg/t54%10%15%12%5%5%0,5%
FeOCaOTrace elementsas metals andoxides
Dust cleaning area

153
Stream Component Typical flow Heavy metals Exposure
Solids in stream toslimes dam
TotalFeOSiO2
Al2O3MgOCaOTraceelements
0,004 kg/t54%10%15%12%5%1%
FeOCaOTrace elementsas metals andoxides
Slimes dam
Flocculant Ferric chlorideTraceelements
Approx 100%
0,1%
FeCl3Trace elementsas chlorides
Flocculant storage/make-up
Dust from magneticseparator andscreens
TotalFeFeOCSiO2
MgOAl2O3CaOTraceelements
kg/t35%15%10%25%5%5%5%0,1%
FeFeOCaOTrace elementsas metals
Magnetic separator
Ash TotalFeOSiO2
Al2O3
MgOCaOTraceelements
150 kg/t5%45%35%5%8%2%
FeOTrace elementsas oxides
Magnetic separator/slimes dam
5.2.4 Electric arc furnaceDC-arc furnaces are used and these are usually charged with hot metal from a blast furnace,scrap, and direct reduced iron together with some lime or dolomite. The electric arc furnacemay however use only scrap steel, or DRI only.
Table 5.2.4Electric arc furnace
Stream Component Typical flow Heavy metals Exposure
Electric arcfurnace gas
TotalDust: FeO ZnO PbO MnO SiO2
CaO MgOTrace elementsNOx
SO2
2 000 m3/t0,02 kg/t41%25%3%4%4%8%3%2%0,25 kg/t0,1 kg/t
Dust containsFeOZnOPbOMnOCaOTrace elementsas oxides andchlorides
Dust cleaning area
Electric arcfurnace slag
TotalFeOSiO2
Al2O3
MgOCaOTrace elements
150 kg/t352028350,1%
FeOCaOTrace elementsas oxides
Slag dump

154
Stream Component Typical flow Heavy metals Exposure
Lime TotalCaOSiO2
Al2O3
FeOMgOTrace elements
100 kg/t 95%1%0,5%0,1%0,4%0,1%
CaOFeOTrace elementsas oxides
Reagent storage/make-up
5.2.5 Casting, rolling, pickling, galvanisingRefined, liquid steel is transferred, in molten state, by crucible, from the electric arc furnace orbasic oxygen furnace to the tundish of the continuous casting machine (Concast). In caseswhere billets or blooms are cast they will be re-heated then rolled to the required shape. If theplate sections are to be galvanised, they are cleaned in HCl or H2SO4
and then hot-dipgalvanised.
Table 5.2.5Casting, rolling, pickling, galvanising
Stream Component Typical flow Heavy metals Exposure
Dust/fume fromrefining
De-sulph.: CO/CO2
SO2
CaO Trace elements
De-phosph.: CO/CO2
Na2O CaO Trace elements
0,001 kg/t20%40%40%0,1%
40%40%20%0,2%
Mainly FeO, CaOandTrace elementsmetals andsulphides, MnSetc.
Mainly FeO, CaO,with traceelements asoxides
Finishing area
Pickle liquors TotalSO4
HCl
0,0001% TE Iron sulphatesand chlorideswith traceelements
Finishing area
Galvanisingfume
TotalZn
0,0001 kg/t80%
ZnTrace elementsas metals
Finishing area
5.3 Flow diagramThe flow diagram for the carbon steel process with with direct reduced iron and electric arcfurnace is shown in Figure 5.3.

155
Figure 5.3 Process diagram for the carbon steel process with with directreduced iron and electric arc furnace.

156
5.4 Process assessment
5.4.1 Hazard identificationSimilar to the carbon steel process with blast furnace and basic oxygen furnace, exposure todust is a primary concern in steel production using direct reduced iron and electric arc furnace.Exposure to iron oxide (Fe2O3) present as a major constituent in the feed material, andconsequently the dust, is controlled by regulations at a level of 5-mg Fe/m3.
The other substances of interest are calcium oxide and zinc oxide. Following the guidance inTable 3.4.2, calcium oxide may be present at levels higher than 20 per cent in electric arcfurnace slag, and zinc has to be assessed as fumes in the galvanising area.
Other metals present at trace levels would be significant only in quantities that exceed theirindividual threshold limits. It appears unlikely that the carbon steel process has the potential torelease heavy metals other than those identified above into air at any significant levels.
5.4.2 Toxicological assessmentIron oxide is not considered to be inert dust (particulates not otherwise classifiable), becauseinhalation may lead to effects known as siderosis, iron pneumoconiosis, hematitepneumoconiosis, and iron pigmentation of the lung. It appears that the pulmonary effects aresomewhat more serious than those caused by inert dust. Systemic effects relating to excessivehaemosiderin deposits have also been documented. It has not been proved that iron oxidesare carcinogenic following chronic pulmonary exposure. The toxicity of iron and its compoundshas been discussed in Section 3.3.4.12.
Calcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicity of calcium oxide has been discussed in Section 3.3.4.7.
The toxicity of zinc has been discussed in Section 3.3.4.33.
5.4.3 Exposure assessmentExposure to dust containing iron oxide may occur in areas where iron ore is handled, and atvarious positions during the process as indicated in the process flow diagram. Sampling andanalytical methods for airborne iron have been listed in Table 3.4.2.6. There is no biologicalmonitoring method to assess exposure to iron, because iron is an essential element present inthe human body.
Exposure to calcium oxide may occur in dust at various locations during the direct reductionsteps, and most prominently in slag from the electric arc furnace. Sampling and analyticalmethods have been listed in Table 3.4.2.6 for calcium. Biological monitoring would not give anindication of exposure because of the large body burden of calcium.
Exposure to zinc may be possible in the final galvanising steps. The most widely knownsystemic effect resulting from acute inhalation of freshly formed zinc oxide fumes is a diseasecalled metal fume fever. Table 3.4.2.6 has given sampling and analytical methods for zincoxide. Zinc is an essential element and is present in abundance in various parts of the humanbody. Biological monitoring would therefore not provide useful information for exposureassessment.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
157
5.4.4 Risk quantificationIn controlling exposure to iron oxide, it is not adequate to control dust levels to 10 mg/m3,because the level of iron may be above 5 mg/ m3 at or slightly lower than 10 mg total dust/m3. Because of its irritation effects, exposure to calcium oxide should be assessed againstmaximum concentration peaks rather than average values.
For exposure to zinc oxide, the concentration at which metal fume fever would develop is notentirely certain, but it has been estimated that symptoms are unlikely to develop at airconcentrations below 15 mg/m3 (Elinder & Piscator, 1979: 682). The ACGIH guidelines of 5mg/m3 for zinc oxide fume and 10 mg/m3 for zinc oxide dust therefore provide adequatemargins of safety.
5.5 ReferencesElinder, C-G. & Piscator, M. 1979d. Zinc. (In: Friberg, L, et al. Handbook on the Toxicologyof Metals. Amsterdam: Elsevier/North-Holland Biomedical Press, p. 675 - 685).
Ross, H. U. 1980. Physical chemistry, DRI technology and economics of production and use.Warrendale USA Iron and Steel Section of the AIME, Society of Mining Engineers, pre-print: 9–26.
Kepplinger, W. 1995. Impact on the environment of new and emerging alternative iron makingprocesses. Proceedings of the SAIMM Conference, University of Pretoria.

158

159
6 Typical copper recovery circuit
6.1 IntroductionThis section provides a process description and process diagram of a typical copper productionfacility. The process description and process diagram contain data on the process streams andidentify the hazardous substances as well as potential exposure points.
6.2 Process description
6.2.1 Crushing and millingThe run of mine ore is subjected to primary gyratory dry crushing with a setting of 175 mm andstock piled. Some of the ore is subjected to further dry crushing to provide feed for rod and ballmilling. The other portion of the ore may be taken directly to autogenous wet milling.
The ore does not contain free quartz and thus no toxic SiO2 dust is produced. The ore containsabout 0.7 per cent Cu as copper sulphide minerals. Normal dust control measures areemployed.
The ore is wet milled in closed circuit with hydrocyclone classifiers to produce a feed to flotationat about 55 per cent solids with about 80 per cent passing 300 microns.
Table 6.2.1Crushing and milling
Stream Component Typical concentrations(as % of dry solids) Heavy metals Exposure
Crushed ore/dustfrom ore
Magnetite, Fe3O4TiO2
Calcite, CaCO3Dolomite, CaCO3,
MgCO3Diopside (pyroxenes)CaMg(SiO3)2
Apatite, Ca5F(PO4)3Phlogopite,K2Mg2Al2Si3O10(OH)2Copper sulphides,CuFeS2, Cu5FeS4Cu2Fe4S6, Cu2SBaddeleyite, ZrO2
Uranothoranite,UO2.2ThO2
250.51520201050,7% totalCu~ 0.06% ZrO2<0.01%
Fe3O4
TiO2
CaCO3
CaCO3, MgCO3CaMg(SiO3)2
Ca5F(PO4)3
K2Mg2Al2Si3O10(OH)2CuFeS2, Cu5FeS4,Cu2Fe4S6, Cu2SZrO2
UO2.2ThO2
Crushers
6.2.2 Flotation and magnetic separationSulfhydryl (xanthate-type) collectors are added as dilute solutions to the slurry, which is passedthrough flotation cells. The flotation froth, containing the copper sulphide minerals, is pumpedto the product-thickening and filtration plant. The flotation tailings are treated for separation ofthe magnetite and non-magnetic components prior to further processing and disposal.
Some of the magnetite from the flotation tailings is reground, upgraded and sold for coalwashing and the remainder is deposited on dumps from which it can be recovered in future forsteel-making.The non-magnetic tailings sands are lightly milled and refloated for further copper recovery andgravity separated for heavy mineral (zirconia and urano-thorianite) recovery. Tailings with an

160
economically recoverable phosphate content are pumped to Foskor. The main bulk of the non-magnetic tailings are impounded in a granite-based valley with sand wall construction andexcess supernatant water recycled to the concentrator plant.
Table 6.2.2Flotation and magnetic separation
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Potential exposurepoints
Non-magnetic tailings Calcite, CaCO3Dolomite, CaCO3,MgCO3Diopside(pyroxenes)CaMg(SiO3)2
Apatite, Ca5F(PO4)3Phlogopite,K2Mg2Al2Si3O10(OH)2Copper sulphides,CuFeS2, Cu5FeS4Cu2Fe4S6, Cu2SBaddeleyite, ZrO2
Uranothoranite,UO2.2ThO2
23262914,47,30,3
TraceTrace
CaCO3
CaCO3, MgCO3CaMg(SiO3)2
Ca5F(PO4)3
CuFeS2, Cu5FeS4Cu2Fe4S6, Cu2SZrO2
UO2.2ThO2
Tailings dam
Magnetite frommagneticseparator
Fe3O4
FeTiO3
CaCO3, MgCO3
8848
Fe3O4
FeTiO3
CaCO3, MgCO3
By product storage
Flotation reagents Xanthatefrothers(organic)
25 g/t20 g/t
6.2.3 Liquid/solid separation/dryingCopper concentrate is thickened and filtered on disk filters. Filtrate is recycled and the filtercake is dried, at low temperature, and delivered to the smelter feed stockpile.
Table 6.2.3Liquid/solid separation/drying
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Copper concentrate Total CuCopper containingspecies:Chalcopyrite, CuFeS2
Bornite, Cu5FeS4
Cubanite, Cu2Fe4S6
ChalcociteCu2S
Mainly CaCO3=
34
40401010
Balance
CuFeS2
Cu5FeS4
Cu2Fe4S6,Cu2S
CaCO3
Drier/Concentrate storage
6.2.4 Smelting and convertingThe flotation concentrate containing the copper-iron-sulphide minerals plus some CaCO3-richgangue is blended with SiO2 in the form of river sand and smelted in a coal-fired, reverberatoryfurnace to produce a copper-iron-sulphide matte and a calcium-iron-silicate slag. Gas from thereverberatory furnace, containing 0,5 to 1,0 per cent sulphur dioxide, is passed to a 150 m highstack.The cooled reverberatory slag is disposed of on a stockpile, which, like the magnetite, drainsany run-off water into the main tailings dam.

161
The molten matte from the reverberatory furnace is treated in a converter where introduction ofoxygen oxidises the iron and sulphur components. The molten converter slag is recycled to thereverberatory furnace. The converter metal is cast into anodes. The converter off-gas, whichis rich in SO2, is sent to an acid plant where, using a V2O5 catalyst, it is converted to H2SO4.
Table 6.2.4Smelting and converting
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Gas fromreverberatory furnaceto ESP/stack
1% SO2 Copper dust Stack emissions
Slag fromreverberatoryfurnace
Fayalite,CaFeSiO3 90 CaFeSiO3 Slag dump
Gas from converter( toacid plant)
12 – 18% SO2
Silica SiO2 100
Impurities removedfrom converter off gas(feed to acid plant)
Analysis not available(recycled)
Acid plant
6.2.5 Refining and rod castingAll of the copper in the form of cast anodes is electrolytically refined. The anodes are placed inelectrolytic cells, with dilute sulphuric acid as the electrolyte and copper starter sheets, ontowhich the refined copper is deposited. More recently, certain plants have changed to the use ofpermanent stainless steel cathodes.
Approximately 60 per cent of the production of copper is consumed locally as continuous-castrod. The remainder is exported as cathode.
During the electrorefining process anode slimes, rich in precious metals, particularly silver andgold, is deposited in the cells and is sold as a by-product. Nickel sulphate is recovered duringthe process of removing impurities from the electrolyte solution and this is also sold as a by-product.
Table 6.2.5Refining and rod casting
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Acid mist fromelectrolytic cells
Cu, Ni, As Cu, Ni, As Cell house
Copper product Cu 100 Cu Product storage/handling area
NiSO4 product NiSO4 100 NiSO4 Nickel sulphatebyproduct
Anode slimes Containing Au, Agand PGM’s
Ag, Pt, Rh, Se, Te, As Cell house/handling area
6.3 Flow diagramThe flow diagram for the copper recovery circuit is shown in Figure 6.3.

162
6.4 Process assessment
6.4.1 Hazard identificationIron oxide levels are high in the magnetite from the magnetic separator. Copperconcentrations are high in dust at the drier and concentrate storage areas. The major potentialfor exposure is to copper dust and fumes during smelting and converting, and during refiningand rod casting. The presence of nickel in the electrorefining process may result in exposure,and during refinery bath maintenance employees may be exposed to lead.
6.4.2 Toxicological assessmentIron oxide is not considered to be inert dust (particulates not otherwise classifiable), becauseinhalation may lead to effects known as siderosis, iron pneumoconiosis, hematitepneumoconiosis, and iron pigmentation of the lung. It appears that the pulmonary effects aresomewhat more serious than those caused by inert dust. Systemic effects relating to excessivehaemosiderin deposits have also been documented. It has not been proved that iron oxidesare carcinogenic following chronic pulmonary exposure. The toxicity of iron and its compoundshas been discussed in Section 3.3.4.12.
Copper is an essential element in humans, but copper dust and fumes are respiratory irritants.The toxicity of copper and its compounds is discussed in Section 3.3.4.10.
Certain nickel compounds are classified as human carcinogens, but noncarcinogenicsystemic effects have not been documented. Hypersensitivity to nickel is common, asdiscussed in the summary of nickel toxicity (Section 3.3.4.17).
Lead is a cumulative toxin. It is well known for neurotoxic effects, but has been associated witha whole range of other possible symptoms and effects. Section 3.3.4.13 provides an overviewof lead toxicity.
6.4.3 Exposure assessmentThe dust released during dry crushing of the ore does not contain heavy metals at a level thatrequires exposure protection other than for inert dust. Magnetite from the magnetic separatorcontains a high level of iron oxide, but the material is wet and exposure to particulates wouldnot occur.
Monitoring for copper dust and fumes is needed primarily at the reverberatory furnace and inthe refining and anode casting steps. Methods for sampling and analysis have been listed inTable 3.4.3.6. Data concerning the relationship between occupational exposure to copper andinternal dose and effect are inadequate to suggest reliable biological monitoring values.
Soluble nickel sulphate, a by-product at the refining step, has been linked to cancer, asindicated in the toxicological review for nickel (Section 3.3.4.17). Sampling and analysismethods for airborne nickel compounds have been listed in Table 3.4.3.6. Several studies havedemonstrated that concentrations of nickel and plasma are indicators of recent exposure. Anambient air exposure level of 0.1 mg Ni/m3 corresponds approximately to a concentration ofnickel in plasma and in urine collected at the end of the workshift of 0.7 µg Ni/100 ml and 70 µgNi/l (corrected for a specific gravity of 1.018), respectively (Lauwerys and Hoet, 1993: 82).

163
Figure 6.3 Process diagram for the copper recovery circuit

164
Several sampling and analytical methods have been listed for airborne lead in Table 3.4.3.6. Lead in blood does not necessarily correlate with the total body burden of lead. It has beenestimated, however, that an increase of 1 µg Pb/ m3 in air is reflected by an increase of 1 to 2µg Pb/100 ml in whole blood. The relationship does not hold at higher exposure levels, though.Lead blood levels between 50 and 70 µg Pb/100 ml has been considered acceptable in maleworkers. It has to be noted, however, that subclinical neurotoxic effects can already be detectedat levels exceeding 50 µg Pb/100 ml (Lauwerys and Hoet, 1993: 55).
Lead in urine reflects the amount of lead recently absorbed. A concentration of lead in blood of50 µg /100 ml usually corresponds with a level of 150 µg /g creatinine, but the correlationacross a wider exposure range is poor. The level of 150 µg Pb/g creatinine corresponds withan air concentration of 50 µg Pb/ m3 (Lauwerys and Hoet, 1993: 55).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
6.4.4 Risk quantificationExposure to copper can be assessed directly against the occupational exposure guideline. Exposure to nickel and assessment for irritation effects is assessed on the same basis. It ishowever recommended that exposure to nickel be quantified in order to estimate cancer risks.Biological monitoring would assist in the quantification of dose.
Seeing that it is likely that protective equipment will be used during maintenance activities andpotential exposure to lead at the refinery baths, it should be appropriate to conduct biologicalmonitoring of the employees in that area.
6.5 ReferencesBeale, C.O. 1985. Copper in South Africa - Part I. Journal of the South African Institute ofMining and Metallurgy, 85 (3): 73 – 80.
Beale, C.O. 1985. Copper in South Africa - Part II. Journal of the South African Institute ofMining and Metallurgy, 85 (4): 109 – 124.
Crosson C.C. 1984. Evolutionary development of Palabora. Transactions of the Institute ofMining and Metallurgy, 93: A58 – A69.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.

165
7 Typical ferrochrome production process
7.1 IntroductionA typical flowsheet of processing chromite ore to produce ferrochrome is described, showingheavy metal species where they arise in the process.
The model is generic, using a conventional submerged arc furnace smelting a chromite orecharge of agglomerated ore and lump ore. Variations on the smelting process, i.e. fine oresmelting in a DC plasma arc furnace, pelletisation and sintering or pre-reduction of the ore inshaft furnaces, belt sintering furnaces and/or rotary kilns, are processes prior to smelting andare mentioned where an alteration to the form of the heavy metals may take place.
7.2 Process descriptionThis section provides a process description and process diagram of a typical ferrochromeproduction facility. The process description and process diagram contain data on the processstreams and identify the hazardous substances as well as potential exposure points.
7.2.1 BeneficiationChromite ore, as mined, occurs as competent hard lump, friable lump and fine sandy minerals.South African ores contain at best 25 to 40 percent of hard to friable "lump" (10 mm to 200mm), the balance being an intermediate fraction (6 mm to 10 mm) and a fine fraction (0,124mm to 6 mm).
Ore received from the mine (open cast or underground) contains gangue (pyroxenite, quartzitemainly) which is removed first by crushing the ore to the specified top size (typically 100 mm),and screening the ore, (grizzly bars or screens) into the lump fractions and fine fractions. Orefrom underground is normally damp giving rise to very little dust. Screening and sizingthereafter is normally under water sprays. Should dust arise, there will be silica, silicates andchromite (trivalent chromium) in the air-borne dust. Hand sorting of the gangue material fromthe ore is frequently carried out, but this practice is giving way to dense media separation inrotating drum separators using 15 per cent ferrosilicon as the dense medium. The ferro-siliconis recovered from both the gangue material and the upgraded lump, and thickened to thecorrect density.
Intermediate material is upgraded in a dense medium cyclone, also using 15 per cent FeSi. The fine ore is screened at 1 mm, the -1 mm containing the gangue fraction. Gravityconcentration using spiral concentrators is carried out. The tailings from this process,containing 20 to 25 per cent Cr2O3 is deposited in slimes dams and is typically -0,125 mm insize. As no chemical process has occurred, the chromite is still in the trivalent form.
Lump waste is typically stockpiled for use as road making material, where possible.

166
Table 7.2.1Beneficiation
Stream Component
Typicalconcentrations
(as % of drysolids) Heavy metals Potential exposure points
Run-of mine ore(chromite)/dust
Al2O3CaOCr2O3
FeOMgOMnOSiO2NiTiO2
ZnOAsBi
13 – 151 – 1,535 – 4522 – 2510 – 120,1 – 0,39.7 – 9.8Traces
CaOCr2OFeOMnONiONiSTiO2
ZnOAsBi
CrushersStockpiles
Waste rock Similar to oreexcept lower Cr
< 5% of chromitein input ore
Similar to ore Waste rock pile
Slimes Similar to wasterock
Similar to wasterock
Similar to wasterock
Slimes dam
Flocculant e.g.Magnafloc
Long chainorganiccompound
10 ppm
7.2.2 Material HandlingChromite is delivered to the smelter by road or rail. Lump ore is generally dry (approximately 2per cent moisture) and gives off dust when off-loaded, transported to stockpiles, recovered forconveyance to the furnaces and weighed off with the other materials required for smelting. Thedust will contain some free quartz, silicates (mainly iron-silicates) and chromite (trivalent). Fluxes, quartzite and limestone are received via the same material handling system, as are thecarbonaceous reductants, coal, coke, anthracite and char. Dusts from this source obviously willbe typically quartzite, limestone and reductant. Until this point chromite will not have undergoneany chemical change and is generally regarded as non-toxic in the trivalent state.
Table 7.2.2Material handling
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Quarzite Al2O3CaOFeOMgOMnOSiO2
0,40.20,30,50,397 - 98
CaOFeOMnO
Road boxes/railtipplers/conveyor transfer points/weigh hoppers and bins
Limestone Al2O3CaOFeOMgOMnOSiO2
0,553,00,51,50,21,0
CaOFeOMnO
Road boxes/railtipplers/conveyor transfer points/weigh hoppers and bins

167
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Dolomite Al2O3CaOFeOMgOMnOSiO2
0,330,01,020,00,52,0
CaOFeOMnO
Road boxes/railtipplers/conveyor transfer points/weigh hoppers and bins
7.2.3 SmeltingFine chromite ore may be agglomerated by briquetting, pelletising, or sintering. Commonbinders for briquettes are 3,5 - 4 per cent hydrated lime/3 - 4 per cent molasses; 3 - 5 per centbentonite/2 per cent molasses.
Pelletising requires that the ore be milled to 80 per cent passing 360 µm to 530 µm, andpelletised with coke breeze, ~ 2000 µm and two per cent bentonite binder. As milling is dry,dust containing chromite (trivalent), coke, quartzite and silicates can occur. The pellets caneither be pre-heated and pre-reduced in a rotary kiln or sintered in a steel-belt sintering plant orshaft kiln. Pre-heating of these pellets using furnace gas is frequently carried out.
Cold charging requires the weighing off of the ore, flux and carbonaceous reductant by weigh-cones or continuous weigh-belts. Dust from these materials arises and is collected in filters tobe returned to the weigh-feed hoppers.
Chromite is proportioned at 1,85 to 2,3 t/t FeCr, the ore containing typically 44 to 48 per centCr2O3. Hot charging is via insulated cylinders through a hot charging system. Dust can occurat this point.
The smelting operation can take place in open; semi-closed or closed top AC submerged arcfurnaces ranging from 10 MVA to 60 MVA capacity and DC plasma arc furnaces (closed-top)ranging from 40 MVA to 63 MVA capacity. Electrical energy is supplied to heat the raw materialto reaction temperature, and the products, slag and FeCr alloy to tapping temperatures of theorder of 1 650 °C to 1 750 °C.
During smelting the reaction gases, CO/CO2 and in the case of open furnaces excess air, carryfine ore and dust from the furnace. The dust loading varies form 50 mg/Nm3 to 150 mg/Nm3 atnormal operating conditions. Dust contains carbon, chromium and volatile metals such as Zn,Ge, which occur as trace elements in the raw materials.
Molten alloy and slag are tapped at predetermined intervals. During the tapping period (20 to35 minutes normally) dust and fumes will come off the tapping launder, from the tap hole andoff the molten alloy/slag. This fume is normally extracted back into the furnace.
Dust from the furnace is collected by wet-scrubbing systems in the case of the closed-topfurnaces, and bag-filters in the case of open to semi-closed top furnaces.
The scrubber sludges and effluents contain some dissolved heavy metals notably hexavalentchromium, which can occur in concentrations of one to five ppm Cr6+.

168
Table 7.2.3Smelting
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Ferrochromeproduct
CrFeSiCMnSPAsBiCaCoCuPbMoNiSbAgTaTeTiWVZnZr
51 – 5435 – 372 – 56 – 7,50,020,040,0225 ppm70 ppm2000 ppm500 ppm40 ppm70 ppm30 ppm2000 ppm40 ppm<500 ppm55 ppm<1 ppm4000 ppm200 ppm3000 ppm70 ppm70 ppm
FeCrCr3C2
Cr7C3Cr3SiCrSiCr5Si3Cr23C6CrFe
Furnace area/crushers
Slag Al2O3CaOCr2O3
FeOMgOMnOSiO2
TiO2C
20212 – 146 – 8120,230 - 350,52,0
CaOCr2O3
FeOMnOTiO2Fe2SiO4
Ca2SiO4
Ca3SiO7MgCr2O4
Mg2SiO4
Slag ex furnace
Furnace dust Al2O3CaOCr2O3
FeOMgOMnOSiO2
TiO2ZnOCrO3AsBiCSAs2O3
Bi2O3
2,00,22,01,21,9 – 100,330 – 350,00210,0<5 ppm18 ppm630 ppm1,02,0TraceTrace
CaOCr2O3
FeOMnOTiO2ZnOCrO3 (hexavalentchrome)As2O3
Bi2O3
Furnace tappingplatform
Baghouse dust collector
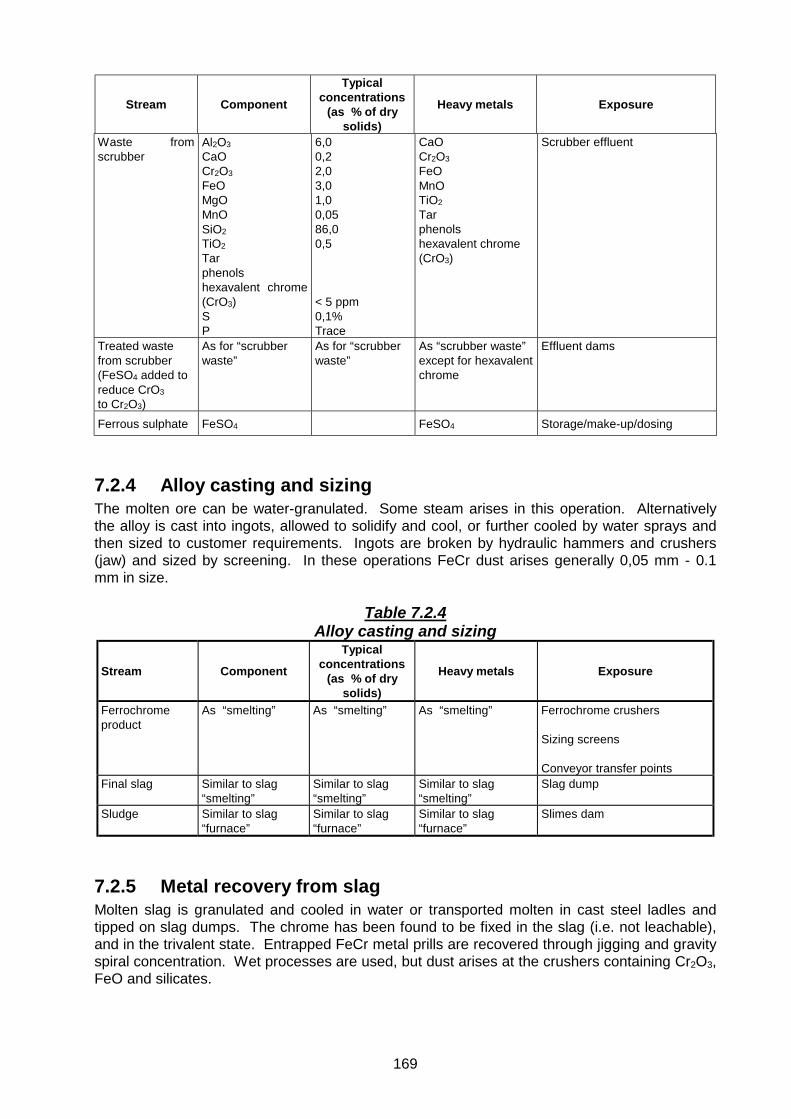
169
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Waste fromscrubber
Al2O3CaOCr2O3
FeOMgOMnOSiO2TiO2
Tarphenolshexavalent chrome(CrO3)SP
6,00,22,03,01,00,0586,00,5
< 5 ppm0,1%Trace
CaOCr2O3
FeOMnOTiO2
Tarphenolshexavalent chrome(CrO3)
Scrubber effluent
Treated wastefrom scrubber(FeSO4 added toreduce CrO3to Cr2O3)
As for “scrubberwaste”
As for “scrubberwaste”
As “scrubber waste”except for hexavalentchrome
Effluent dams
Ferrous sulphate FeSO4 FeSO4 Storage/make-up/dosing
7.2.4 Alloy casting and sizingThe molten ore can be water-granulated. Some steam arises in this operation. Alternativelythe alloy is cast into ingots, allowed to solidify and cool, or further cooled by water sprays andthen sized to customer requirements. Ingots are broken by hydraulic hammers and crushers(jaw) and sized by screening. In these operations FeCr dust arises generally 0,05 mm - 0.1mm in size.
Table 7.2.4Alloy casting and sizing
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Ferrochromeproduct
As “smelting” As “smelting” As “smelting” Ferrochrome crushers
Sizing screens
Conveyor transfer pointsFinal slag Similar to slag
“smelting”Similar to slag“smelting”
Similar to slag“smelting”
Slag dump
Sludge Similar to slag“furnace”
Similar to slag“furnace”
Similar to slag“furnace”
Slimes dam
7.2.5 Metal recovery from slagMolten slag is granulated and cooled in water or transported molten in cast steel ladles andtipped on slag dumps. The chrome has been found to be fixed in the slag (i.e. not leachable),and in the trivalent state. Entrapped FeCr metal prills are recovered through jigging and gravityspiral concentration. Wet processes are used, but dust arises at the crushers containing Cr2O3,FeO and silicates.

170
7.3 Flow diagramThe flow diagram for the ferrochrome recovery circuit is shown in Figure 7.3.
7.4 Process assessment
7.4.1 Hazard identificationDust generated during off-loading, transport to stockpiles, and other activities involving thechromite ore, does not contain heavy elements in a form that would be bioavailable, and thedust should be assessed as inert particulates (not otherwise classifiable).
The elemental distribution in furnace slag dust is such that it can be regarded as inertparticulates. Hexavalent chromium is present in scrubber sludges and effluents. Chromiumthroughout the other stages of the process is in the trivalent state.
7.4.2 Toxicological assessmentChromium is an essential element in humans. Hexavalent chromium is a human carcinogen,as outlined in the toxicity assessment for chromium (see Section 3.3.4.8). Trivalent chromiumis poorly absorbed, but allergic eczematous dermatitis has been observed following industrialexposures.
7.4.3 Exposure assessmentHexavalent chromium levels in scrubber sludges and effluents are low, and should not pose acancer risk if dust concentrations are managed according to dust exposure guidelines. At thesmelting and alloy casting areas chromium may be present in air associated to particulates,possibly in the hexavalent state. Exposure can be quantified using sampling and analyticalmethods listed in Table 3.4.3.6. Determination of chromium in urine is the preferred method forassessing exposure to hexavalent chromium. Exposure to an air concentration of 0.05 mgCr/m3 would be reflected in a urine concentration of 30 µg Cr/g creatinine at the end of theexposure period. Exposure to trivalent chromium compounds does not correlate with levels ofchromium in urine (Lauwerys and Hoet, 1993: 42).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
7.4.4 Risk quantificationExposure to total chromium can be assessed directly against the occupational exposureguideline. For assessment of exposure to hexavalent chromium, biological monitoring andquantification of cancer risk should be the preferred approach.

171
Figure 7.3 Process diagram for the ferrochrome recovery circuit

172
7.5 ReferencesElyutin, V.P., Pavlov, Y. A., Levin B. E. & Alekseev E. M. 1957. Production of ferroalloyselectrometallurgy, 2nd Ed. Translated from Russian, National Science Foundation, WashingtonDC, Israel Program for Scientific Translators, 450.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.
Woollacott, L. C. & Eric, R. H. 1994. Mineral and metal extraction, an overview. SAIMMMonograph Series M8, Johannesburg, 412p.

173
8 Typical ferromanganese production process
8.1 IntroductionManganese ores are smelted in submerged arc furnaces, which can be totally closed–top orpartly closed. The ores smelted are in lumpy form or sintered fine ore. The furnace chosen willdetermine the pollution abatement system employed on the furnace and in turn will influencethe effluent composition of the streams from these systems. Sintering generally takes place atthe mines, but will be dealt with in this section as part of the processing.
8.2 Process descriptionThis section provides a process description and process diagram of a typical ferromanganeseproduction facility. The process description and process diagram contain data on the processstreams and identify the hazardous substances as well as potential exposure points.
8.2.1 BeneficiationThe South African manganese ore used by the major ferromanganese producers are those ofthe Jaspilite type found in and near Kuruman. They are composed chiefly of braunite, withsmall amounts of hausmanite and hematite. The gangue material consists mainly of calciumcarbonate and magnesium carbonate.
Manganese ores as mined, occur as competent lump and a fine product, which is the result ofboth the mining operation and crushing to size. Mining operations can be both open cast andunderground. In a typical open cast operation in-pit crushing in jaw or gyratory cone crushers isperformed. Crushing and sorting is also carried out underground.
Ore from the mining areas is transported via conveyers to be crushed to –150 mm. Furthercrushing and screening processes follow to produce a series of sized material to customerspecifications and to enable further beneficiation. In the beneficiation process dense mediumseparation of gangue from a typically –19 mm size ore is carried out. The medium used is aslurry of fine ferrosilicon 15 per cent Si. This medium is fed together with the sized ore todense medium cyclones. The gangue separated from the ore is washed clean and depositedon waste stockpiles. Slimes arising from the screening and washing processes, typically –0,15mm, are pumped to slimes dams.
The slimes dams and waste rock dumps will contain the carbonates of manganese, some ironoxides, and calcium and magnesium carbonates
Potential exposure points to dust arising from the ore mining and beneficiation process are inthe open cast pit and underground workings at the crushers, at screens and at conveyertransfer points. Material deposited on waste stockpiles and in slimes dams may leach, but asthe ore has not been altered in any way, chemically, there should not be a contamination risk.

174
Table 8.2.1Beneficiation
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Manganeseore/dust
Al2O3
CaOFe2O3
MgOMnOMnO2SiO2
Na2OK2OP2O5BaOTiO2
CO2Combined waterSO3
0,1-0,42-146-150,3-2,524-3733-403-50,2-0,30.1-0.40,05-0,120.15-0.70,02-0,0251-14
1-30,03-0,06
CaCO3
MnCO3
Fe2O3
MnOMnO2
BaOBaCO3
TiO2
CrushersScreensConveyor transfer points
Waste rock Similar to ore Similar to ore Similar to ore Waste rock dump
Slimes Similar to wasterock
Similar to wasterock
Similar to wasterock
Slimes dam
8.2.2 SinteringSintering is required to agglomerate the –6 mm ore and dusts collected throughout thebeneficiation process and to upgrade the manganese content of the ore. The ore is – 6 mm insize. Coke is milled in a rod mill and screened to pass through three-mm mesh. Ore and cokeare proportioned and conveyed to a nodulising drum and agglomerated using water. Thismixture is sintered on a moving grate sintering machine. The sinter product is crushed in atooth roll crusher and screened, and the undersize (- 6 mm) is returned to the sintering process. On-size material is stockpiled for shipment to the users. Dedusting of the waste gas from thesintering windboxes is through electrostatic precipitators, the dust collected and returned to thesintering process. The air from the sinter cooling section is cleaned by cycloning, the dustreturned to the sintering process. Screens and belts are usually covered and sealed and dustcollected from these areas returned to the sintering process.
Table 8.2.2Sintering
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Sinter dust Similar to orePlus carbon
Similar to ore Similar to ore Sinter machineElectrostatic precipitatorsCrushers
8.2.3 Material handlingManganese ore and sinter are delivered to the smelter by rail and road. Ores are usuallyblended as they are stockpiled in blending and reclaiming systems. Here dust arises which isof a similar nature to those found at the mines. Fluxes, quartzite and dolomite are received viaa separate handling system, together with coke and coal, transported to stockpiles or storagesilos and recovered for conveyance to the furnace storage bins. Dusts arising from these areas

175
arise from transfer points and would be mixtures of the ore, sinter, fluxes and carbonaceousreducing agents.
Table 8.2.3Material handling
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Quartzite Al2O3
CaOFe2O3
MgOMnOSiO2
0,40,20,50,50,397-98
CaOFe2O3
MnO
Conveyor transfer pointsWeigh hoppersFurnace bins
Limestone Al2O3
CaOMgOMnOSiO2
0,553,01,2-1,50,21,0-1,5
CaCO3
Fe2O3
MnO
Conveyor transfer pointsWeigh hoppersFurnace bins
Dolomite Al2O3
CaOFe2O3
MgOSiO2
0.3301.5-2.0200.52
CaOFe2O3
MnOCaCO3
FeCO3
Conveyor transfer pointsWeigh hoppersFurnace bins
8.2.4 SmeltingThe feed materials are batch or continuously weighed and blended and fed to bunkers abovethe furnaces. The mix is gravity fed to the furnaces through multiple feed ports in the furnaceroof.
Manganese ores are proportioned at 2.0 to 2.2 tons/ ton ferromanganese.
Smelting takes place in open, semi-closed and closed top furnaces ranging in capacity from 10to 80 MVA. Electricity is supplied to heat the burden to the reaction temperature, and theferromanganese and slag tapped at temperatures of 1 650 oC to 1 750 oC. During tapping thereaction gases, CO and CO2 and volatilised manganese, carry fine ore and other dusts from thefurnace. These dusts are removed by water scrubbing systems, bag house filters or electro-precipitators.
Discharge gas could contain 50 to 100 mg/ Nm3 of dust at normal operating conditions. Dustscontain carbon, manganese, Zn, Ge, Fe, Ni, Co, and K.
Dust from the furnaces is collected in bag house filters in the case of open-top furnaces andscrubber systems in the case of closed-top furnaces.
The scrubber effluents and sludges contain dissolved heavy metals, coal tars, phenols andthiocyanates.

176
Table 8.2.4Smelting
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Ferromanganeseproduct
MnFeSiCSPAsBiCoCuNiZn
14 - 160,56,5-7,50,050,1TraceTraceTraceTraceTraceTrace
Metallics:Mn, Si, Co, Fe, Cu,Ni, Zn.
Intermetallics:Mn3C, Mn3Si,MnC3, MnP3,MnS, MnAs,MnSi, Fe2As,Fe3P, Fe3C,Fe3Si, FeAsS,FeS, FeSi,FeSi2
Furnace/product area
Furnace slag Al2O3
CaOFeOMgOSiO2
MnOK2ONa2O
4,5-5,535 - 380,1 - 0,38 - 1031 - 3318 - 22
CaOFe2O3Fe2SiO4
FeAl2O4
FeOFeSMnSFeSiO3MnO
Furnace area
Furnace dust Al2O3
CaOFeOMgOSiO2
MnOK2ONa2OC
5 – 66 – 711– 1210 – 1215 – 1738 – 401,3 – 1,60,3 – 0,75 – 10
CaOFeOMnOMn3O4MnO2
MnSMnSiO3
C
Bag house/electro static precipitator
Scrubbereffluent/slimes dam
Al2O3
CaOFeOMgOSiO2
MnOK2ONa2O
6 – 76 – 78 – 910 – 1212 – 1428 – 320,5 - ,50,2 - 0,4
CaOFeOMnOMn3O4MnO2
MnSMnSiO3
C
Scrubber dischargeSlimes dam
Flocculant e.g.Magnafloc
Long chainorganiccompound
10 ppm
8.2.5 Alloy casting, crushing and sizingThe molten alloy can be cast into ingots via a casting machine or into moulds fashioned fromfine ferromanganese alloy. The solidified alloy is sized by crushing and screening tospecifications. In this operation ferromanganese dust will arise. The dust particles are of theorder of 0.05 – 0.1 mm in size.

177
Table 8.2.5Alloy casting, crushing and sizing
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Ferromanganesedust
As ferro-manganeseproduct – seeSection 8.2.4
As ferro-manganeseproduct – seeSection 8.2.4
As ferro-manganeseproduct – seeSection 8.2.4
CrushersScreensTransfer points
8.2.6 Metal recovery from slagMolten slag is separated from the alloy during the tapping operation and tapped into cast steelladles. The slag is transported to a slag dump where it is tipped and solidifies. Entrapped alloyis recovered through a crushing jigging and gravity separation operation. Wet processes areused, but crushing does give rise to dust of the composition of the slag.
Table 8.2.6Metal recovery from slag
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Ferromanganeseproduct
As ferro-manganeseproduct – seeSection 8.2.4
As ferro-manganeseproduct – seeSection 8.2.4
As ferro-manganeseproduct – seeSection 8.2.4
Product storage
Final slag/slimes towaste dump
Similar to slag fromfurnace – seeSection 8.2.4
Similar to slagfrom furnace –see Section 8.2.4
Similar to slag fromfurnace – seeSection 8.2.4
Waste dump
Flocculant Long chain organiccompound
8.3 Flow diagramThe flow diagram for the ferromanganese production process is shown in Figure 8.3.
8.4 Process assessment
8.4.1 Hazard identificationManganese is the primary element of concern in the ferromanganese production process. Particulates containing more than 0.5 per cent of manganese should not be considered to beinert, and management according to guidelines for particulates would not be adequate.
8.4.2 Toxicological assessmentManganese compounds in various forms are considered to be neurotoxic, with subclinicaleffects occurring at low exposure levels. Section 3.3.4.14 presents an overview of the toxicityof manganese.

178
Figure 8.3 Process diagram for the ferromanganese production process

179
8.4.3 Exposure assessmentDust from manganese ore contains high levels of manganese, but it is unlikely that themanganese would be in a form that is bioavailable. Various manganese oxides have howeverbeen shown to be neurotoxic, and in the assessment of exposure all forms of manganese arenormally considered. Exposure may occur in the furnace/product area as a result of highmanganese levels in furnace slag and dust. Manganese levels are also high in scrubbereffluents. Sampling and analytical methods to quantify airborne manganese have been listed inTable 3.4.3.6.
The normal concentration of manganese in urine is usually less than 3 µg/l, and in whole bloodand plasma less than 1 µg/100 ml and 0.1 µg/100 ml, respectively. There is however noconsistent relationship between manganese exposure and blood levels, and it appears thatmeasurement of urinary levels is the preferred method for assessment. The relationship withexposure is however not that well-defined and no biological threshold limit value has beenproposed (Lauwerys and Hoet, 1993: 71).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
8.4.4 Risk quantificationThe potential for development of neurotoxic effects is assessed through determination of ahazard quotient on the basis of the guideline concentration for manganese in air.
8.5 ReferencesElyutin, V.P., Pavlov, Y. A., Levin B. E. & Alekseev E. M. 1957. Production of ferroalloyselectrometallurgy, 2nd Ed. Translated from Russian, National Science Foundation, WashingtonDC, Israel Program for Scientific Translators. 450p.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.
Potgieter, F. J. 1980. Operation of an 81 MVA high carbon ferromanganese furnace atSamancor, Meyerton Works. Proceedings of the International Ferro-alloys Conference,Lausanne Switzerland: IPFED, p. 244 – 252.

180

181
9 Bacterial oxidation circuit for the pre-oxidation ofrefractory gold ores
9.1 IntroductionThis section provides a process description and process diagram of a typical bacterial oxidationcircuit for the pre-oxidation of refractory gold ores. The process description and flow diagramcontain data on the process streams and identify the toxic substances as well as the potentialexposure points.
9.2 Process description
9.2.1 Crushing, Screening and MillingPhysical size reduction of run-of mine ore is usually carried out in several stages of jaw and/orcone crushing. The ore is crushed to a P100 (100 per cent passing) size of 20 to 50 mm (P80 often to 30mm). Crusher product is then wet-milled in rod or ball mills to a P100 of 212 to 300 µm(P80 of 75 to 106 µm), and transferred to the bacterial oxidation section. Flotation and bacterialoxidation may also be done in the reverse order.
Table 9.2.1Crushing, screening, wet milling
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Crushed ROM(run-of mine)ore/dust
Silicates, SiO2
Carbonates, CaCO3 etc.OxidesSulphides
801 – 105max 2 %
Pyrite, FeS2
Arsenopyrite,FeAsSCaCO3
Metal sulphides
Crushers
Milled oreslurry
Solids – same as ROM ore Solids – sameas ROM ore
Solids – same asROM ore
Mill
9.2.2 Gravity concentrationFree, coarse gold is removed from the milled ore using Knelson concentrators, jigs, or shakingtables.
9.2.3 FlotationThe gold-containing sulphide minerals in the milled ore are separated from the gangue materialby a froth flotation process. Thickener underflow is pumped to the bacterial oxidation section. Overflow water is recycled. The flotation concentrate is then re-ground to a P100 of 106 to 150µm (P80 of 45 to 75 µm).

182
Table 9.2.3Flotation
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Flotation tails SilicatesCarbonatesOxidesMinor sulphides
Variable – sitespecific
0.04
CaCO3Trace metalsulphides as inconc.
Concentrator/tailings dam
Flotationconcentrate
PyriteArsenopyriteBase metal sulphidesSilicatesCarbonatesOxides
20 – 402 – 250 – 1020 – 502 – 152 – 15
CuFeS2
NiSZnSFeS2
FeAsSCaCO3
Concentrator
Flotationreagents
Not known – site specific Not known Flotation reagentmake-up
Flocculant Not known - site specific Not known Flocculant make-up
9.2.4 Bacterial oxidation and gold recoveryIn the bacterial oxidation section a portion of the sulphide minerals (pyrite and arsenopyrite) inthe thickener underflow is oxidised due to the presence of bacteria which are introduced as aninitial inoculum, to form sulphates, thus freeing gold entrapped in the sulphide minerals. This iscarried out in mechanically agitated, aerated, open-top tanks at a temperature of 35 to 45 oCand at a pH of 1,0 to 1,6. Minor quantities of nutrients are fed to the reactors in order to feedthe bacteria.
In the bacterial oxidation process, the pyrite and arsenopyrite are solubilised, and largequantities of iron, arsenic, sulphate, and sulphuric acid appear in solution. Smaller amounts ofmetals such as cobalt, nickel, copper, and zinc will also be solubilised if they are present in thefeed concentrate. Table 9.2.4 shows typical concentrations that the dissolved metals will reachin the bacterial oxidation process, as well as the typical quantities of these metals that willremain in the solid residue.
As mentioned, the bacterial oxidation process is carried out in large, mechanically agitated,aerated, open-top tanks. Exposure to the dissolved metals could occur if there is an aerosoleffect at the top of the tank owing to the aeration. Exposure to both dissolved species and thesolids could occur if there is foam on the top of the tank, and the foam is lifted and transportedby the wind action.
In some applications, pH levels in the bacterial oxidation process will be controlled by theaddition of lime. If this is the case, partial precipitation of iron, arsenic, and sulphate will occurin the bacterial oxidation process. Some gypsum will also be precipitated. These precipitateswill then report to the solids residue, and will pass through the gold recovery process beforereporting to the tailings.
The residue from bacterial oxidation is fed to three or four thickeners where it is washed by acounter-current flow of water. Thickened slurry, at about 20 to 35 per cent solids, andcontaining the freed gold, is transferred to a conventional cyanide-leach/carbon-in-pulp goldrecovery plant, described as a separate process package (see Section 10). The final wastefrom the gold recovery plant is transferred to a slimes dam. Thickener overflow is pumped tothe neutralisation section.

183
Table 9.2.4Bacterial oxidation and gold recovery
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Solution inslurry afterbacterialoxidation
Fe3+
Fe2+
As5+
As3+
H2SO4
CoNiCuZnMgCa+ other metal species inminor to trace amounts
10 - 50 g/l< 0.5 g/l3 - 25 g/l< 20 mg/l2 - 20 g/l< 1 g/l< 1 g/l1 – 5 g/l< 1 g/l< 1 g/l1 –2 g/l
Fe2(SO4)3
FeSO4
H3AsO3
CoSO4NiSO4
CuSO4
ZnSO4
CaSO4
H2SO4
Bacterial oxidationtanks; aerosol andfoam from the opentanks
Solids in slurryafter bacterialoxidation
PyriteArsenopyriteBase metal sulphidesSilicatesOxides +Iron-arsenic-sulphateprecipitates +Gypsum (CaSO4).2H2O)
0.04 – 20 – 10.04 – 220 – 5050 – 80
Approx 20
FeS2
FeAsSFe(OH)3
FeAsO4
Ca3(AsO4)2
FeAsO4.0,8Fe(OH)3.0,2Fe(OH)SO4
FeAsO4.Fe(OH)3
FeAsO4.2Fe(OH)3.Fe(OH)SO4
FeAsO4.3Fe(OH)3
CaSO4.2H2OH3O.Fe3(SO4)2(OH)6K3Fe3(SO4)2(OH)6
(NH4)3Fe3(SO4)2(OH)6
NiSCuFeS2
ZnS
Slimes dam
Lime Al2O3
CaOMgOMnOSiO2
0,553,01,2-1,50,21,0-1,5
CaCO3
Fe2O3
MnO
Limemake-up/transfer
Nutrients Di-ammonium phosphatePotassium sulphateMagnesium sulphate
Flocculant Not known - site specific Not known Flocculant make-up
9.2.5 Bioliquor neutralisation/thickening and disposalThe acid in the bioliquor is neutralised, and iron and arsenic are precipitated, by the addition oflimestone and possibly lime. This is carried out in a series of four mechanically agitated,aerated, open-top tanks. The slurry from the tanks is transferred to a thickener. Thickenerunderflow is pumped to a tailings dam and clear liquor overflow is recycled.

184
Table 9.2.5Bioliquor neutralisation/thickening and disposal
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Thickenerunderflow/tailings dam solids
Iron-arsenic-sulphateprecipitates.GypsumFeAsSO4
2-
Ca
10 – 201 – 1030 – 4010 – 20
Iron-arsenic-Sulphur precipitatesAnd gypsum(CaSO4.2H2O)Ferric arsenate
Tailings dam
Lime CaOMgOAl2O3
FeOMnOSiO2Fe2O3
91,31,70,30,30,10,8
CaOMnOFeOFe2O3
Lime make-up/transfer
Flocculant Not known - sitespecific
Not known Flocculant make-up
9.3 Flow diagramThe flow diagram for the bacterial oxidation circuit for the pre-oxidation of refractory gold ores isshown in Figure 9.3.
9.4 Process assessment
9.4.1 Hazard identificationExposure to inert dust and arsenic in certain areas presents the primary focus for health riskmanagement. Normally, material pumped to the slimes dam does not contain any hazardoussubstances that would be leachable, and by implication, bioavailable. The toxicity characteristicleaching procedure (TCLP) may be used to confirm these properties. Arsenic is the substanceof primary concern in the process.
9.4.2 Toxicological assessmentDust at the positions of potential exposure is considered inert, and should be assessedaccording to guidelines for management of particulates.
Arsenic is a confirmed human carcinogen, and is known to cause contact dermatitis. SeeSection 3.3.4.2 for a description of arsenic toxicity.
9.4.3 Exposure assessmentThe primary areas of potential exposure are at the bacterial oxidation tanks, where arsenic ispresent in the foam and mist. The arsenic is present in the process in forms that are highlybioavailable.
Area monitoring and personal sampling may be conducted using NIOSH Method 7901, as listedin Table 3.4.3.6. NIOSH Method 7900 is valid only for particulate-associated inorganic arseniccompounds.

185
Figure 9.3 Process diagram for the bacterial oxidation circuit for the pre-oxidation of refractory gold ores

186
Mean serum and blood levels of arsenic vary greatly depending on the level of seafood contentin the diet. Therefore, when employees have not been instructed to refrain from eating fish orshellfish for two to three days before biological monitoring, high levels of arsenic may be foundthat might not be associated with occupational exposure. In the past, biological monitoring forassessment of occupational exposure was conducted by measuring the total amount of arsenicin urine at the end of a shift. It is however now well established that inorganic arsenic,monomethylarsonic acid, and cacodylic acid in urine is the method of choice. Monitoring ofemployees exposed to inorganic arsenic using this method is not influenced byorganoarsenicals from marine origin.
Some controversial results may be obtained in the correlation between air-concentrationexposure assessment and biological monitoring. It has been established that backgroundlevels of the sum of the three metabolites of arsenic (inorganic arsenic, monomethylarsonicacid, and cacodylic acid) in urine vary between 10 µg/l and 50 µg/l. It appears that the bestrelationship for occupational exposure at air concentrations between 50 and 200 µg As/m3
would lead to post-shift concentrations of the total metabolites between 54 and 88 µg/gcreatinine (Lauwerys and Hoet, 1993: 25).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
9.4.4 Risk quantificationOccupational exposure levels have to be assessed through interpretation of area and personalmonitoring data, in conjunction with biological monitoring and exposure effects monitoring. Cancer risks can be quantified through interpretation of exposure data and arsenic dose-response information.
9.5 ReferencesClaassen, R., et al. 1991. The effect of mineralogy on the bacterial oxidation of refractory gold-bearing sulphides from a Barberton deposit. Also 10 other papers. Colloquium, BacterialOxidation. Randburg, Megawatt Park, 18 June. Johannesburg: The South African Institute ofMining and Metallurgy.
Lauwerys, R. R. & Hoet, P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring: Second Edition. Boca Raton: Lewis Publishers, 318p.
Nicholson, H. & Oti-atakorah, S.& Lunt, D.J. & Ritchie, I.C. 1993. Selection of a refractorygold treatment process for the Sansu project. Biomine’93. Glenside, Australia: AustralianMineral Foundation, p. 20.1 – 20.11
Nicholson, H.M., Lunt, D.J., Ritchie, I.C. & Marais, H.J. 1994 The design of the Sansuconcentrator and BIOX facility. XVth CMMI Congress. Johannesburg: South African Instituteof Mining and Metallurgy, Vol. 2, p. 393 – 402.
Van Aswegen, P.C. 1993. Biooxidation of refractory gold ores – the Genmin experience. Biomine’93. Glenside, Australia: Australian Mineral Foundation, p. 15.1 – 15.14.

187
10 Carbon-in-pulp circuit for gold recovery
10.1 IntroductionThis section provides a process description and process diagram of a typical carbon-in-pulpcircuit for gold recovery. The process description and flow diagram contain data on the processstreams and identify the toxic substances as well as the potential exposure points.
10.2 Process description
10.2.1 CrushingRun of mine ore from the shaft head is fed by a conveyor system to the primary crushingstation. Tramp waste material is removed either by hand or in the case of metallic constituents,by means of electro-magnets. The crushed product is delivered to a vibrating grizzly screen. The oversize material from this primary screening unit is sent to a jaw-crusher. The grizzlyundersize fraction (-150mm) together with the crushed product is conveyed to a stockpile. From this storage area, the material is transported to mill surge bins.
The analysis of the ore provided in Table 10.2.1 is the best obtainable at this stage. It appearsthat operating companies do not analyse for heavy metals and such an analysis was not in thepossession of the plant manager. It is likely that the original geological survey of the depositwould have to be retrieved in order to obtain more specific data. As the main constituentremoved from the ore by the process is gold, the slimes dam/waste dump should have a similarheavy metal analysis to that of the ore.
Table 10.2.1Crushing
Stream Component Typicalconcentrations Heavy metals Exposure
ROM ore Quartz, SiO2
Pyrite, FeS2+ Arsenopyrite,FeAsS + traces ofPyrophylite, mica,calcite, dolomiteincluding majority ofheavy metals in tracequantities as sulphides,oxides and sulphates
> 90%
5 – 20%
FeS2
FeAsSCaCO3
Majority of heavymetals in tracequantities as sulphides,oxides and sulphates
Ore storage/handling/crushing
10.2.2 MillingThe crusher product is delivered to the milling circuit and introduced into the mill via a hopperfeeder system, which may be either static or mobile. A variety of different comminution processoptions are applied. In instances in which the ore itself is sufficiently competent to act as thegrinding media, autogenous milling may be applied. In other instances, grinding media, in theform of steel ball (50 to 100mm) are added to the mill together with the ore. Process water andlime (CaO), either as a dry powder or as a slurry, is added at the inlet feed trunnion (i.e. point ofore entry) of the mill. The mills are generally operated in closed circuit with hydro-cycloneclassifiers that serve to separate the ground ore particles according to size and solids density. The coarser or heavier fraction is recycled back into the mill for further size reduction while thefiner overflow fraction is delivered to a tramp removal section utilising linear belt screens to
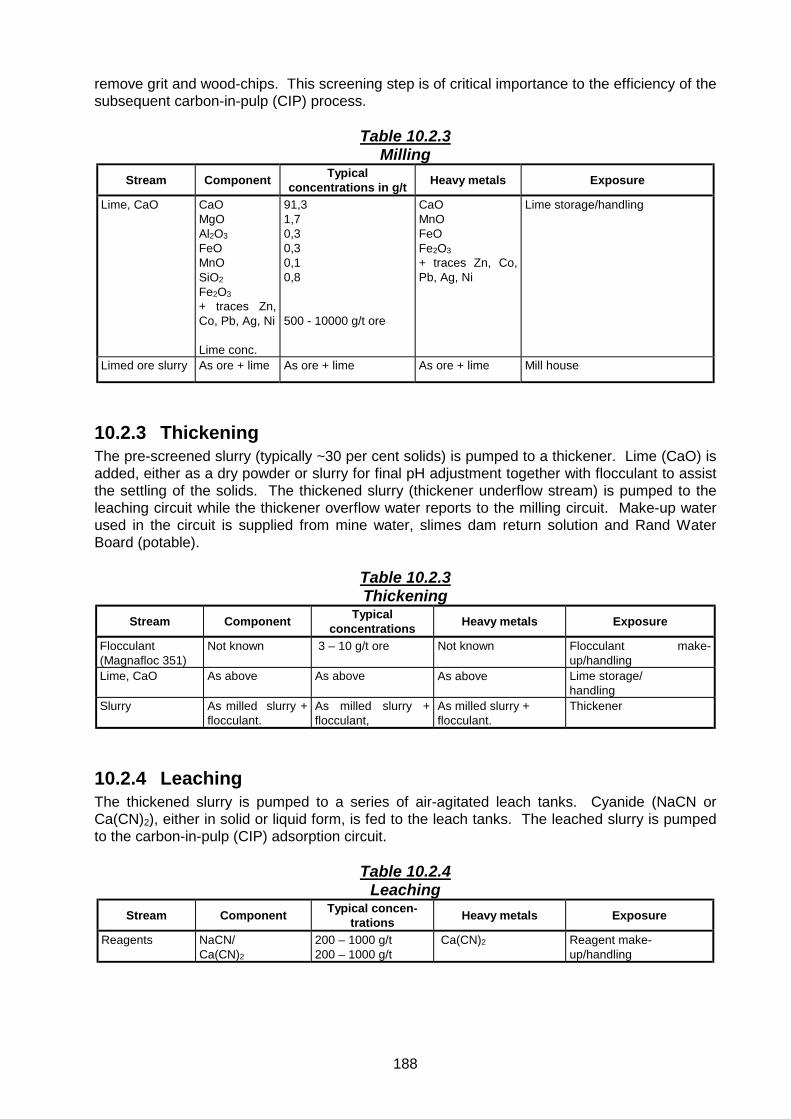
188
remove grit and wood-chips. This screening step is of critical importance to the efficiency of thesubsequent carbon-in-pulp (CIP) process.
Table 10.2.3Milling
Stream Component Typicalconcentrations in g/t Heavy metals Exposure
Lime, CaO CaOMgOAl2O3
FeOMnOSiO2
Fe2O3+ traces Zn,Co, Pb, Ag, Ni
Lime conc.
91,31,70,30,30,10,8
500 - 10000 g/t ore
CaOMnOFeOFe2O3+ traces Zn, Co,Pb, Ag, Ni
Lime storage/handling
Limed ore slurry As ore + lime As ore + lime As ore + lime Mill house
10.2.3 ThickeningThe pre-screened slurry (typically ~30 per cent solids) is pumped to a thickener. Lime (CaO) isadded, either as a dry powder or slurry for final pH adjustment together with flocculant to assistthe settling of the solids. The thickened slurry (thickener underflow stream) is pumped to theleaching circuit while the thickener overflow water reports to the milling circuit. Make-up waterused in the circuit is supplied from mine water, slimes dam return solution and Rand WaterBoard (potable).
Table 10.2.3Thickening
Stream Component Typicalconcentrations Heavy metals Exposure
Flocculant(Magnafloc 351)
Not known 3 – 10 g/t ore Not known Flocculant make-up/handling
Lime, CaO As above As above As above Lime storage/handling
Slurry As milled slurry +flocculant.
As milled slurry +flocculant,
As milled slurry +flocculant.
Thickener
10.2.4 LeachingThe thickened slurry is pumped to a series of air-agitated leach tanks. Cyanide (NaCN orCa(CN)2), either in solid or liquid form, is fed to the leach tanks. The leached slurry is pumpedto the carbon-in-pulp (CIP) adsorption circuit.
Table 10.2.4Leaching
Stream Component Typical concen-trations Heavy metals Exposure
Reagents NaCN/Ca(CN)2
200 – 1000 g/t200 – 1000 g/t
Ca(CN)2 Reagent make-up/handling

189
Stream Component Typical concen-trations Heavy metals Exposure
Leach slurry Elements insolution:AuAgSiCaNiFeCuAlMgZnCoPb
CyanideComplexes insolution:
Zn(CN)2-6
Cu(CN)3-4
Ni(CN)2-4
Au(CN)-2
Fe(CN)3-6
Co(CN)2-6
CN-
SCNCNO
mg/l
101.68.52575.5<112<0.5<0.55<0,5<0,5
mg/l
<0,16002,5 – 15<0,12 – 60<0,1 – 3200 – 400700 – 1000<0,1 – 3,5
Complexed cyanidesolutions and vapours
Elements in solution:AgCaNiFeCuZnCoPb
Cyanide complexes insolution:
Zn(CN)2-6
Cu(CN)3-4
Ni(CN)2-4
Fe(CN)3-6
Co(CN)2-6
Leach tanks
10.2.5 AdsorptionThe leached slurry gravitates through a number of CIP stages with a typical pulp residence timeof about one-hour per stage. Reactivated carbon, at a particle size of between 1 and 3 mm, isadded to the final stage of the CIP train and flows upstream, counter current to the pulp flow. As the carbon inventory makes its way up the cascade train, the solubilised gold adsorbs ontothe carbon. Batches of loaded carbon are periodically removed from the upper-most stage(stage 1) of the circuit. Carbon is prevented from flowing back downstream by inter-stagescreens, which allow free passage to the slurry, but retain the carbon. The pulp containing theloaded carbon transferred from the head CIP contactor is delivered to a linear screen where thecarbon is separated from the pulp. The pulp gravitates back to the adsorption circuit. Theresidue pulp exiting the final stage of the adsorption train is passed over linear screens torecover any carbon particles that may have escaped the circuit. This carbon product isreturned back to the adsorption circuit. The undersize from this screen is pumped either to thebackfill preparation plant or to the slimes dam.
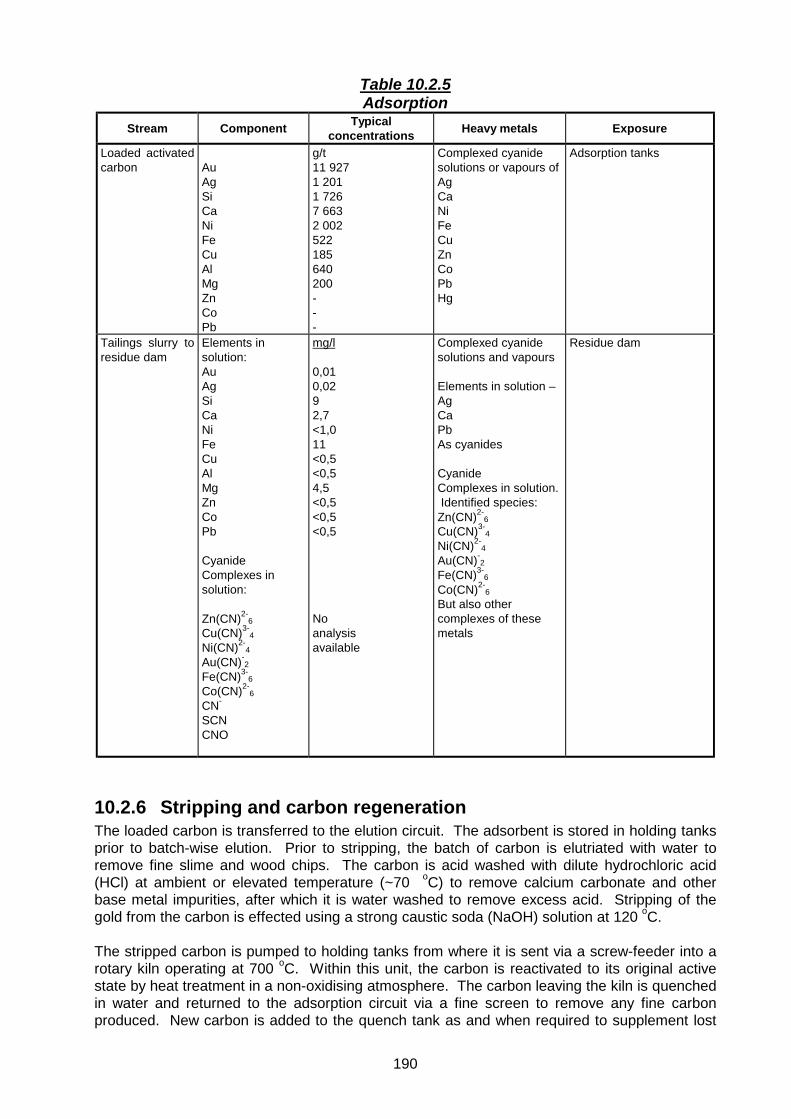
190
Table 10.2.5Adsorption
Stream Component Typicalconcentrations Heavy metals Exposure
Loaded activatedcarbon Au
AgSiCaNiFeCuAlMgZnCoPb
g/t11 9271 2011 7267 6632 002522185640200---
Complexed cyanidesolutions or vapours ofAgCaNiFeCuZnCoPbHg
Adsorption tanks
Tailings slurry toresidue dam
Elements insolution:AuAgSiCaNiFeCuAlMgZnCoPb
CyanideComplexes insolution:
Zn(CN)2-6
Cu(CN)3-4
Ni(CN)2-4
Au(CN)-2
Fe(CN)3-6
Co(CN)2-6
CN-
SCNCNO
mg/l
0,010,0292,7<1,011<0,5<0,54,5<0,5<0,5<0,5
Noanalysisavailable
Complexed cyanidesolutions and vapours
Elements in solution –AgCaPbAs cyanides
CyanideComplexes in solution. Identified species:Zn(CN)2-
6Cu(CN)3-
4
Ni(CN)2-4
Au(CN)-2
Fe(CN)3-6
Co(CN)2-6
But also othercomplexes of thesemetals
Residue dam
10.2.6 Stripping and carbon regenerationThe loaded carbon is transferred to the elution circuit. The adsorbent is stored in holding tanksprior to batch-wise elution. Prior to stripping, the batch of carbon is elutriated with water toremove fine slime and wood chips. The carbon is acid washed with dilute hydrochloric acid(HCl) at ambient or elevated temperature (~70 oC) to remove calcium carbonate and otherbase metal impurities, after which it is water washed to remove excess acid. Stripping of thegold from the carbon is effected using a strong caustic soda (NaOH) solution at 120 oC.
The stripped carbon is pumped to holding tanks from where it is sent via a screw-feeder into arotary kiln operating at 700 oC. Within this unit, the carbon is reactivated to its original activestate by heat treatment in a non-oxidising atmosphere. The carbon leaving the kiln is quenchedin water and returned to the adsorption circuit via a fine screen to remove any fine carbonproduced. New carbon is added to the quench tank as and when required to supplement lost

191
adsorbent. The water used for quenching is filtered to remove the carbon fines and is treatedfor gold recovery.
Table 10.2.6Stripping and carbon regeneration
Stream Component Typicalconcentrations Heavy metals Exposure
HCl solution HCl 10 %
Cyanide solution NaCNNaOH Gases: HCN,H2, NH3,
1%0,5%
EluateAuAgSiCaNiFeCuMgZn
NaCN solution,NaCN vapours,NaOH solution,NaOH vapours
mg/l347425235965<1<1
AgCaNiFeCuZnas cyanides
Eluate handling
Activated carbonAuAgSiCaNiFeCuAlMgZn, Co, Pb
g/t6311010204634030474318130
CaCO3
Ag, Ni, Fe, Cu,Zn, Co, Pb,typically ascyanide complexes
Activated carbon handling
Steam andactivatedcarbon
CO, CO2Decompositionproducts
Carbon regeneration
10.2.7 ElectrowinningThe gold bearing eluate is circulated through the electrowinning cells following pH adjustment.The gold plates out onto steel wool cathodes, which are digested in H2SO4 to dissolve the steel.
Table 10.2.7Electrowinning
Stream Component Typicalconcentrations Heavy metals Exposure
Spent electrolyte NaCN solution,NaCN vapours,NaOH solution,NaOH vapours,Gases: HCN,H2, NH3, CO2
2% (50% drybasis)
2% (50% drybasis)
Traces of Ag, Ni,Fe, Cu, Zn, Co,Pb, as cyanides
Electrowinning cells
Gold sludge AuAgFe, Cu, Ni
70%3%low %
Traces of Ag, Ni,Fe, Cu, Zn, Co,Pb, Hg, inmetallic form
Cells

192
10.2.8 SmeltingThe gold-rich sludge is filtered, dried, fluxed and smelted to bullion in an induction furnace.
Table 10.2.8Smelting
Stream Component Typicalconcentrations Heavy metals Exposure
Smelting flux Na2CO3
BoraxSiO2
Gold bullion AuAg, Ni, Fe, Cu,Zn, Co, Pb
85% Ag, Ni, Fe, Cu,Zn, Co, Pb inMetallic form
Smelter/storage
Slag Au, Ag Ag Slag disposal
10.2.9 Residue disposalThe residue from the adsorption circuit is pumped to a storage tank. If designated for back-fill,the fine fraction of solids is removed using high-pressure cyclones. The cyclone overflowfraction is thickened in Double-V thickeners and pumped to a slimes dam. The cycloneunderflow fraction is pumped to a shaft storage pachuca. The residual cyanide is destroyedusing ferrous sulphate or Ca(OCl)2 prior to backfilling underground. Portion of the residueslurry, when deemed necessary is pumped directly to the slimes dam. The slimes dam water isrecycled back to the process circuit for reuse.
Table 10.3.9Residue disposal
Stream Component Typicalconcentrations Heavy metals Exposure
Ca(OCl)2 Ca(OCl)2 Ca(OCl)2 Reagent storage/handling
Flocculant(Magnafloc 351)
Not known Not known Flocculant make-up/handling
Residue slurry SiO2
Traces of heavymetals ascontained in ore
Bulk FeS2
FeAsSCaCO3
Majority of heavymetals in tracequantities assulphides, oxidesand sulphates
Residue dam
10.3 Flow diagramThe flow diagram for the carbon-in-pulp circuit for gold recovery is shown in Figure 10.3.

193
Figure 10.3 Process diagram for the carbon-in-pulp circuit for gold recovery

194
10.4 Process assessment
10.4.1 Hazard identificationHeavy metals in the ore are present at trace levels. The dust at ore storage, handling, andcrushing, should therefore be assessed as inert particulates (not otherwise classifiable).Calcium oxide is of concern for its irritation effects. The process is largely wet, with a low riskof exposure to heavy metals.
10.4.2 Toxicological assessmentCalcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicology of calcium oxide has been discussed in Section 3.3.4.7.
10.4.3 Exposure assessmentExposure to calcium oxide may occur at the milling section and lime storage areas. Samplingand analytical methods have been listed in Table 3.4.2.6 for calcium. Biological monitoringwould not give an indication of exposure because of the large body burden of calcium.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
10.4.4 Risk quantificationBecause of its irritation effects, exposure to calcium oxide should be assessed againstmaximum concentration peaks rather than average values.
10.5 ReferencesAll authors/chapters. 1972. (In: Adamson, R.J. Gold metallurgy in South Africa. SouthAfrica: Chamber of Mines of South Africa, Cape and Transvaal Printers, all pages).
All authors/chapters. 1987. (In: Stanley, G.G. The extractive metallurgy of gold in SouthAfrica. South Africa: South African Institute of Mining and Metallurgy, Monograph Series, allpages).

195
11 Nickel, copper, cobalt refining processes
11.1 IntroductionThe processes described are typical of those used in base metal refineries in the South Africanplatinum industry. The technology is adapted in each application to meet specific productrequirements, which may in turn be dictated by the composition of the feed material and thescale of operation, and consequently flowsheets differ significantly in each installation. Two orthree stage pressure leaching may be employed. In some applications, the first stage pressureleach may be replaced with an atmospheric leach for economic or other reasons.
The process described as Option 1 includes first stage atmospheric leaching with a secondstage pressure leach. Products are nickel sulphate crystals, cathode copper and an upgradedPGM concentrate. This flowsheet is suited to a smaller operation with a relatively low basemetal output, such as may be produced from a UG2 ore. Comment will be made in thefollowing text of alternative unit operations to produce upgraded products.
The feed to the refinery is a converter matte with the typical composition shown in the tablebelow. Solutions containing the salts of the base metals present occur throughout the process.
The process described here as Option 2 varies quite significantly from Option 1. Althoughmuch of the equipment is similar, involving atmospheric and pressure leaching and multiplesolid-liquid separation stages, the chemical and physical principles employed to achieve theseparation of PGMs, copper, nickel etc., differ.
The PGMs are produced as a concentrate and the copper as metal, as before. Nickel ishowever produced as a metal and cobalt is produced as a byproduct. Sulphur is removed in aprocess that produces a saleable sodium sulphate crystal.
The feed is again a converter matte having a fairly similar composition to that for Option 1.Copper electrowinning is also a common operation to that described in Option 1. Solutionscontaining the salts of the base metals present occur throughout the process.
11.2 Process description: option 1
11.2.1 Matte grindingCrushed or granulated white matte delivered from the smelter is ground in water in a ball mill. The fine material is then thickened to typically 80 per cent solids in a settler cone or thickenerand pumped to the first stage leach.

196
Table 11.2.1Matte grinding
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
White matte CopperIronNickelCobaltSeleniumSulphurPGM’s + Au
27 – 351 – 235 – 450,3 – 0,70,0520 – 252000–3000 ppm
Cu, Fe, Ni, Co,Se, Te and othermetal sulphidese.g. Ni3S2,Cu2SSome Ni-Cu-Fealloy and manyothers
Matte handling/mill area
11.2.2 Atmospheric Pressure Leach and Nickel SulphateCrystallisation
The atmospheric pressure leach is designed to extract nickel and iron contained in the matte,while simultaneously precipitating copper and any PGM’s contained in recycled spentelectrolyte leachate.
The matte slurry is mixed with pre-heated spent electrolyte. Oxygen is sparged into the slurryto promote the reaction between the nickel in the matte and the sulphuric acid. The terminalleach solution pH is maintained at about 4 to allow copper precipitation, which co-precipitatesdissolved PGM’s. Retention time is 6-8 hours at about 80oC.
The slurry and solution contain dissolved base metals, principally nickel and copper from thispoint onwards.
The leach discharge is transferred to a thickener.
In the selected flowsheet, the nickel bearing solution is clarified and transferred to a nickelsulphate evaporator/crystalliser where nickel is recovered as nickel sulphate hexahydrate whilethe thickened slurry is pumped to the pressure leach circuit.
Solution feed to the crystalliser is controlled on level. Steam ejectors supply the vacuumrequired to operate the crystalliser at about 50oC, which ensures the hexavalent product. Theslurry of nickel sulphate crystals and mother liquor is circulated through a steam heated heatexchanger. Larger crystals are separated from the circulating slurry by means of an elutriationleg in the crystalliser. These are typically centrifuged, then dried in a rotary dryer. Gases fromthe dryer are scrubbed with water.
A number of alternative process options are available. Depending on product requirements andits economics, cobalt may be precipitated and separated from the nickel sulphate solutionbefore nickel crystallisation. The precipitate could then be purified for the production of a cobaltproduct, for example cobalt sulphate heptahydrate (CoSO4.7H2O). Alternative nickel productsmay also be produced, including nickel oxide, nickel cathode or nickel powder.

197
Table 11.2.2Atmospheric pressure leach and nickel sulphate crystallisation
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Thickenerunderflow
CuNiCoS
40 – 4525 – 350,522 – 26
Cu, Ni, Co,sulphides andmetallics
Thickener/slurry handling
Thickener overflow CuNiCo
Al, As, Cd, Cr,Fe, Mg, Mn, Mo,Pb, Se, Te
0,1 – 0,3 g/l90 - 100 g/l0,1 – 0,5 g/l
Total 0,0001 –0,5 g/l
Cu, Ni, Co,Se, Al, As, Cd, Cr,Fe, Mg, Mn, Mo,Pb, Te sulphates
Se precipitate handling, nickelsulphatecrystalliser area
Nickel sulphate Ni/Co sulphate NiSO4
CoSO4
Storage/handling
11.2.3 Pressure leachLeach solution, comprising a blend of spent electrolyte, water and sulphuric acid is added to thethickened slurry, and the mixture fed to the pressure leach autoclave. The objective is toquantitatively leach the remaining copper and nickel sulphides to yield a high-grade PGMconcentrate. The charge make-up is adjusted to yield a discharge solution containing about100g/l of copper plus nickel and 20g/l of sulphuric acid.
Oxygen is sparged into the leach slurry to maintain oxidising conditions. The slurry is heated bysteam injection while cooling coils are provided to control temperature. Leach retention time is4-6 hours at a total pressure of about 1100kPa and a temperature of 140 to 160oC.
The discharge slurry is filtered to recover the PGM concentrate, while the filtrate is transferredto selenium removal and copper electrowinning unit operations.
Table 11.2.3Pressure leach
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Solids from filter PGM + AuNi + Cu + CoFeSSiO2
Other
20 – 3012 – 1515 – 205 – 105 – 1020 - 30
Ni, Cu, Co, Pt,Pd, Rh, Os, Ru,Se, Te,Fe sulphides,oxides, arsenatesand metallics
Filter cake/handling
Filtrate NiCuCoFePtPdRhRuSeTe
65 - 70 g/l40 – 50 g/l0,5 – 1,0 g/l0,5 g/l0,05 mg/l0,2 mg/l4 mg/l10 mg/l40 mg/l10 mg/l
Ni, Cu, Co, Pt,Pd, Rh, Ru, Se,Te sulphates
Filter

198
11.2.4 Selenium removalThe filtered pressure leach solution is treated with sulphur dioxide in a reactor to precipitateselenium, tellurium, palladium plus some copper, and some of the other PGM’s which partlydissolve in the pressure leach.
The copper selenide precipitate is filtered off, roasted and caustic-leached to extract seleniumand tellurium. The PGM containing residue may be recycled to the pressure leach, or treatedfor copper removal for direct transfer to the PGM refinery.
Table 11.2.4Selenium removal
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Filter cake Se, TeCuPGM’s
30 – 3560 – 703 - 5
Not known Filter and filter cake handling
11.2.5 Copper electrowinningCopper is recovered from the purified pressure leach solution by electrowinning. The copperlevel in solution is typically reduced from about 50 g/l to about 20 g/l.
Table 11.2.5Copper electrowinning
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Copper product Cu 99+ Cu Cell house/Product storage
Cell house mist CuSO4
NiSO4
Not known CuSO4
NiSO4
Cell house
11.3 Flow diagram: option 1The flow diagram for the nickel, copper, and cobalt refining process (Option 1) is shown inFigure 11.3.

199
Figure 11.3 Process diagram for the Ni, Cu, Co refining process – option 1

200
11.4 Process assessment: option 1
11.4.1 Hazard identificationBecause of variations in process conditions at different installations, all the potential hazardshave been identified in this section. The hazards may not be applicable in all cases.
The matte grinding process is wet, and exposure to heavy metals should not be possible. Theatmospheric pressure leach and nickel sulphate crystallisation steps are also done under wetconditions. If the nickel and cobalt products produced in this area are in a dry powder orcrystalline form, the possibility of exposure should be considered. The filter cake producedfrom the pressure leach would contain nickel, copper and cobalt, and also the platinum groupmetals, and exposure may occur if dry filter cake is handled. Similarly, the filter cake producedfrom the selenium removal step would contain high levels of both selenium and to a lesserextent tellurium. In the electrowinning cell house, exposure would be largely to copper andnickel in mists.
11.4.2 Toxicological assessmentCertain nickel compounds are classified as human carcinogens, but noncarcinogenicsystemic effects have not been documented. Hypersensitivity to nickel is common, asdiscussed in the summary of nickel toxicity (Section 3.3.4.17).
Copper is an essential element in humans, but copper dust and fumes are respiratory irritants.The toxicity of copper and its compounds is discussed in Section 3.3.4.10.
The critical effects associated with the inhalation of cobalt as metal, dust, or fume arepulmonary fibrosis and pulmonary sensitisation. The toxicity of cobalt and its compounds isdiscussed in Section 3.3.4.9.
Salts of the platinum group metals are sensitisers upon chronic exposure, causing allergieslike rhinitis, conjunctivitis, asthma, urticaria and contact dermatitis. See Sections 3.3.4.18,3.3.4.19, and 3.3.4.20 for descriptions of the toxicity of platinum group metals.
Occupational exposure to selenium may cause a wide range of non-specific symptoms, asdescribed in Section 3.3.4.21.
Tellurium has relatively low toxicity, but can be converted in the body to form dimethyl telluride,which gives a garlicky odour to the urine, breath and sweat. Section 3.3.4.24 provides anoverview of tellurium toxicity.
11.4.3 Exposure assessmentSoluble nickel sulphate has been linked to cancer, as indicated in the toxicological review fornickel (Section 3.3.4.17). Sampling and analysis methods for airborne nickel compounds havebeen listed in Table 3.4.3.6. Several studies have demonstrated that the concentration ofnickel in plasma is an indicator of recent exposure. An ambient air exposure level of 0.1 mgNi/m3 corresponds approximately to a concentration of nickel in plasma and in urine collected atthe end of the workshift of 0.7 µg Ni/100 ml and 70 µg Ni/l (corrected for a specific gravity of1.018), respectively (Lauwerys and Hoet, 1993: 82).
Methods for sampling and analysis of copper in ambient air have been listed in Table 3.4.3.6. Data concerning the relationship between occupational exposure to copper and internal doseand effect are inadequate to suggest reliable biological monitoring values.

201
Methods for sampling and analysis of cobalt in ambient air have been listed in Table 3.4.3.6. Itis believed that normal levels of cobalt are below 2 µg/g creatinine for urine and 0.05 µg/100 mlfor serum and plasma (Lauwerys and Hoet, 1993: 47). The concentration of cobalt in bloodand urine below which the risk of adverse effects is negligible has not yet been clarified. Forrefinery exposure it has been shown that a time-weighted average of 50 µg Co/m3 leads to anaverage concentration of 33 and 46 µg/g creatinine in the urine collected at the end of shift onMonday and Friday, respectively. Exposure at this air concentration is expected to lead to amean blood level of 2.5 µg/l (Lauwerys and Hoet, 1993: 47).
Area monitoring and personal sampling for the platinum group metals and compounds maybe conducted using NIOSH Method 7300 and OSHA CIM. The most appropriate method has tobe selected for the particular exposure scenario.
Platinum can be determined in blood or tissue using NIOSH Method 8005, but the relationshipbetween these levels and exposure has not been established.
Area monitoring and personal sampling for selenium and its compounds may be conductedusing NIOSH Method 7300 and OSHA CIM.
The biological significance of selenium in blood and urine is not clear, but it appears that theconcentration in serum (or plasma) and urine reflects short-term exposure, whereas theselenium content of erythrocytes may be associated with long-term exposure. There is noindication that selenium in hair may be used to assess the selenium body burden. A biologicalthreshold limit of 100 µg/l for selenium in urine has been proposed, but this is associated withgreat uncertainty (Lauwerys and Hoet, 1993:86). There is no guideline for biological monitoringin South Africa.
Area monitoring and personal sampling for tellurium and its compounds may be conductedusing NIOSH Method 7300 and OSHA ID 121.
Little is known about the human metabolism of tellurium, and concentrations in urine may berelated to amounts absorbed. Direct correlations are however unknown. It has beensuggested that levels in urine below 1 µg/l would prevent the tellurium-associated garlic odourof breath. No guideline for biological monitoring has been set in South Africa.
11.4.4 Risk quantificationDepending on the specific nickel compounds, it is appropriate to quantify cancer risks.
Copper, cobalt, the platinum group metals, selenium, and tellurium exposures can beassessed on the basis of hazard quotients, using the documented occupational exposure limits.For cobalt, biological monitoring may add some information to the assessment.
11.5 References: option 1Brugman, C, F. & Kerfoot, D.G. 1986. Treatment of nickel matte at Western Platinum by theSherritt acid leach process. Nickel extraction and refining: Proceedings of the 25th AnnualConference of Metallurgists, 1986, Toronto, Ontario, 17 – 20 August: CIM.
Hofirek, Z. & Kerfoot, D. G. E. 1992. The chemistry of the nickel-copper matte leach and itsapplication to process control and optimisation. Hydrometallurgy, 29(1): 357 – 381. (Paperpresented at the Ernest Peters International Symposium, Hydrometallurgy. Theory and practice.
Lauwerys, R. R. & Hoet, P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.

202
Plasket, R.P. and Ramandruk, S. 1978. Recovery of nickel and copper from high-grade matteat Impala Platinum by the Sherritt process. Hydrometallurgy, 3 (2): 135 – 151.
11.6 Process description: option 2
11.6.1 Slow cool/crush/mill/magnetic concentrationWhite matte from the smelter/converter is cast into moulds and slow cooled for a period of 3days. During this process a Ni-Cu-Fe alloy (mainly Ni) separates out as platelets. This alloyacts as a collector for PGMs of which around 99 per cent migrate into the alloy. After the slowcooling process the matte is crushed and wet milled and passes to magnetic separation. Thealloy formed in the slow cooling process is magnetic and this fraction amounts to approximately15 per cent of the total matte. The non-magnetic fraction comprises Cu2S and Ni3S2 and tracesof PGMs. The Se and Te sulphides are also included in the non-magnetics. The magneticfraction is subjected to a leaching process from which a solid PGM concentrate, containingapproximately 60 per cent PGMs is produced. This is fed to a precious metals refinery forseparation/refining into the final products. The solution from the leach process, containingcopper and nickel, together with the larger stream of non-magnetics, containing the bulk of thecopper, nickel and cobalt, are transferred to the base metals refinery.
Table 11.6.1Slow cool/crush/mill/magnetic concentration
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals* Exposure
White matte CopperIronNickelCobaltSeleniumSulphurPGM’s + Au
Sb, As, Bi, Cr,Pb, Mn, Ag, Te,Sn, Zn
292450,60,05212000 ppm
10 to 300 ppm levels
Cu, Fe, Ni, Co,Se, Te and othermetal sulphidese.g. Ni3S2,Cu2SSome Ni-Cu-Fealloy and manyothers.Sb, As, Bi, Cr,Pb, Mn, Ag, Te,Sn, Zncompounds insmall amounts
Matte crushing/handling
PGM concentrate Pt, Pd, Rh, Ru, Ir,Os
60% in solids (smallquantity)
Pt, Pd, Rh, Ru, Ir,Os
Filter cake
11.6.2 Copper cementationThe non-magnetic material is fed to a copper removal (cementation) stage, which is carried outin reactors operating at atmospheric pressure. Here the matte is contacted with primary leachdischarge solution and solution from the sulphur removal stage. Copper and iron are cementedout of solution and some of the nickel in the matte is dissolved. The slurry undergoes solid-liquid separation in a thickener. The thickener underflow solids, containing 35 per cent Ni and30 per cent Cu, are fed to the first stage leach and the nickel-rich solution (thickener overflow)passes to nickel solution purification.
The atmospheric pressure leach is designed to extract nickel and iron contained in the matte,while simultaneously precipitating copper and any PGM’s contained in recycled spentelectrolyte leachant.

203
11.6.3 Primary pressure leachIn the primary leach the copper residue is subjected to a pressure leach at 1000 kPa and 135oCin autoclaves. Spent electrolyte from copper electrowinning, containing sulphuric acid, is usedto leach further nickel and cobalt. Solution from the magnetic fraction leach process is alsoadded at this point. Nickel dissolves to the point of a total dissolution of 80 to 85 per cent overthe cementation and first stage leach operations. Copper is retained out of solution byoperating the final stages of the autoclave in a non-oxidsing mode. Slurry from the autoclavepasses to a thickener and overflow from which it is recycled to the cementation stage. Underflow solids, containing copper and residual nickel and cobalt, is filtered on a belt filter andwashed before being transferred to the second stage leach.
Table 11.6.3Primary pressure leach
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Lead-containingwaste
Lead hydroxide Not known Lead hydroxide, someZn, Mn and Fe species
Filter cake/handling
Barium hydroxide Ba(OH)2 ~100 Ba(OH)2 Storage/handling
11.6.4 Secondary pressure leachThe second stage leach is carried out at 1000 kPa and 145oC in autoclaves. Oxygen-enrichedair is fed to the autoclaves. Here copper, nickel and cobalt are leached up to the point ofachieving an overall copper dissolution, for all operations, of > 98 per cent and an overall nickeldissolution of > 99 per cent. Iron is precipitated as hematite (Fe2O3). Exit slurry passes tosolid-liquid separation (plate and frame press). The residue, comprising mainly iron but alsocontaining many of the impurities in the feed (Se, Te, As, Sb, Bi), together with the traces ofPGMs which were contained in the non-magnetic fraction, is exported. Selenium remaining inthe liquor is removed by the addition of sulphur dioxide, which results in the formation of Cu2Se.This is filtered off and combined with the waste iron stream for export.
Table 11.6.4Secondary pressure leach
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Mainiron/seleniumresidue
Cu2Se, Te, Sb,Bi compoundswith iron, tracePGMs
Mainly Fe Fe2O3, Cu2Se, Te, Sb,Bi compounds withiron, trace PGMs
Filter cake
11.6.5 Copper electrowinningCopper is recovered from the purified pressure leach solution by electrowinning. The feedsolution typically contains 75g/l Cu, 30 g/l Ni, and 60 g/l sulphuric acid . The electrowinningcells have lead anodes and copper starter sheet cathodes. The starter sheets are formed byplating copper onto titanium cathodes to form thin copper sheets. These are stripped from thecathodes, trimmed, and fabricated into starter sheet cathodes. After copper deposition on thecathode the copper spent electrolyte is reduced to a Cu content of 25 g/l and acid content of 90g/l.

204
Table 11.6.5Copper electrowinning
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Copper product Cu 99.9 Cu Cell house/Product storage
Cell house mist CuSO4
NiSO4
Not known CuSO4
NiSO4
Cell house
11.6.6 Cobalt removalThe nickel-containing liquor exiting the thickener downstream of the cementation processrequires the removal of lead, copper and cobalt prior to the recovery of nickel by electrowinning.Lead (from the lead anodes used in copper electrowinning) is removed by precipitation withbarium hydroxide and the precipitate is recycled back to the smelter. Cobalt is removed byprecipitation as cobalt hydroxide by the addition of nickelic hydroxide. The nickelic hydroxide isproduced by taking a portion of the main nickel sulphate stream, adding sodium hydroxide andthen passing the nickelous hydroxide formed through an electrolytic cell. The cobalt hydroxidecake is filtered off and leached in nickel spent electrolyte to dissolve nickel hydroxides. Thecake is then washed and leached in sulphuric acid to dissolve the remaining nickel and thecobalt. The solution is then purified to remove Cu, Fe and Pb. Manganese is also removed bythe addition of sodium persulphate to form manganese dioxide, which is recycled to thesmelter. The cobalt sulphate in the solution is then separated from the nickel sulphate bysolvent extraction. Cobalt sulphate is then crystallised as CoSO4.7H2O and marketed.
Table 11.6.6Cobalt removal
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Cobalt sulphateproduct
CoSO4.7H2O ~100 CoSO4.7H2O Product storage
MnO2 recycle MnO2 Not known MnO2 Filter cake
11.6.7 Nickel electrowinningThe main solution, after cobalt removal, is clarified and transferred to nickel electrowinning. This is carried out in electrolytic cells with lead anodes. The cathodes are nickel starter sheetsmade by depositing a thin sheet of nickel onto titanium blanks. The cathodes are enclosed inpermeable bags and the feed liquor is introduced into the bags. A positive head of liquor iskept in the cathode bag which separates the relatively acidic solution at the anode (anolyte)from the relatively neutral feed solution. This ensures the predominant reaction at the cathodeis the deposition of nickel rather than the evolution of hydrogen which would otherwisepreferentially occur if the solution were acidic. Sulphur from the feed matte is now present atthe anode as sulphuric acid and must be removed from the circuit. Evolution of acid mist whichwill contain copper and nickel sulphates is kept very low by covering the liquid surface of thecells with small polystyrene beads. Operators are required to wear masks to ensure thatexposure levels are brought down below maximum permissible TLV levels.

205
Table 11.6.7Nickel electrowinning
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Nickel cathodeproduct
Ni 99.9 Ni Cell house/Product storage
Cell housemist
NiSO4 Not known NiSO4 Cell house
11.6.8 Sulphur removalApproximately half of the nickel spent electrolyte leaving the electrowinning cells is reacted withsodium hydroxide to neutralise the acid and in so doing sulphur is removed from the circuit inthe form of sodium sulphate solution. This solution is transferred to an evaporator/crystalliserthat produces anhydrous sodium sulphate for sale as a byproduct. Nickel in the spentelectrolyte is precipitated as nickelous hydroxide which is filtered off and re-dissolved in theother half of the spent electrolyte and the solution produced is then returned to primary leach.
11.7 Flow diagram: option 2The flow diagram for the nickel, copper, cobalt refining process (Option 2) is shown in Figure11.7.
11.8 Process assessment: option 2
11.8.1 Hazard identificationThe process in option 2 is largely a closed system, with minimal exposure to employees. Forcompleteness, however, the species that are present in filter cake have been listed in Tables11.6.1, 11.6.4, and 11.6.6. It appears that the areas of primary interest are the electrowinningsteps for nickel, copper, and cobalt, and the assessment of exposure therefore will focus onthese metals.
11.8.2 Toxicological assessmentCertain nickel compounds are classified as human carcinogens, but noncarcinogenicsystemic effects have not been documented. Hypersensitivity to nickel is common, asdiscussed in the summary of nickel toxicity (Section 3.3.4.17).
Copper is an essential element in humans, but copper dust and fumes are respiratory irritants.The toxicity of copper and its compounds is discussed in Section 3.3.4.10.
The critical effects associated with the inhalation of cobalt as metal, dust, or fume arepulmonary fibrosis and pulmonary sensitisation. The toxicity of cobalt and its compounds isdiscussed in Section 3.3.4.9.

206
Figure 11.7 Process diagram for the Ni, Cu, Co refining process – option 2

207
11.8.3 Exposure assessmentSoluble nickel sulphate has been linked to cancer, as indicated in the toxicological review fornickel (Section 3.3.4.17). Sampling and analysis methods for airborne nickel compounds havebeen listed in Table 3.4.3.6. Several studies have demonstrated that concentrations of nickeland plasma are indicators of recent exposure. An ambient air exposure level of 0.1 mg Ni/m3
corresponds approximately to a concentration of nickel in plasma and in urine collected at theend of the workshift of 0.7 µg Ni/100 ml and 70 µg Ni/l (corrected for a specific gravity of1.018), respectively (Lauwerys and Hoet, 1993: 82).
Methods for sampling and analysis of copper in ambient air have been listed in Table 3.4.3.6. Data concerning the relationship between occupational exposure to copper and internal doseand effect are inadequate to suggest reliable biological monitoring values.
Methods for sampling and analysis of cobalt in ambient air have been listed in Table 3.4.3.6. Itis believed that normal levels of cobalt are below 2 µg/g creatinine for urine and 0.05 µg/100 mlfor serum and plasma (Lauwerys and Hoet, 1993: 47). The concentration of cobalt in bloodand urine below which the risk of adverse effects is negligible has not yet been clarified. Forrefinery exposure it has been shown that a time-weighted average of 50 µg Co/m3 leads to an
average concentration of 33 and 46 µg/g creatinine in the urine collected at the end of shift onMonday and Friday, respectively. Exposure at this air concentration is expected to lead to amean blood level of 2.5 µg/l (Lauwerys and Hoet, 1993: 47).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
11.8.4 Risk quantificationDepending on the specific nickel compounds, it is appropriate to quantify cancer risks in theoccupational exposure scenario.
Copper and cobalt exposures can be assessed on the basis of hazard quotients, using thedocumented occupational exposure limits. For cobalt, biological monitoring may add someinformation to the assessment.
11.9 References: option 2Anonymous. 1981. Matthey Rustenburg Refiners. Journal of the South African Institute forMining and Metallurgy, 81:11-14.
Hofirek, Z. and Halton, P. 1990. Production of high quality electrowon nickel at RustenburgBase Metals Refiners (Pty) Ltd. Theory and practice. (In: Claessens, P.L. and Harris, G.B. Electrometallurgical plant practice. New York: Pergamon, p. 233-251).
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.

208
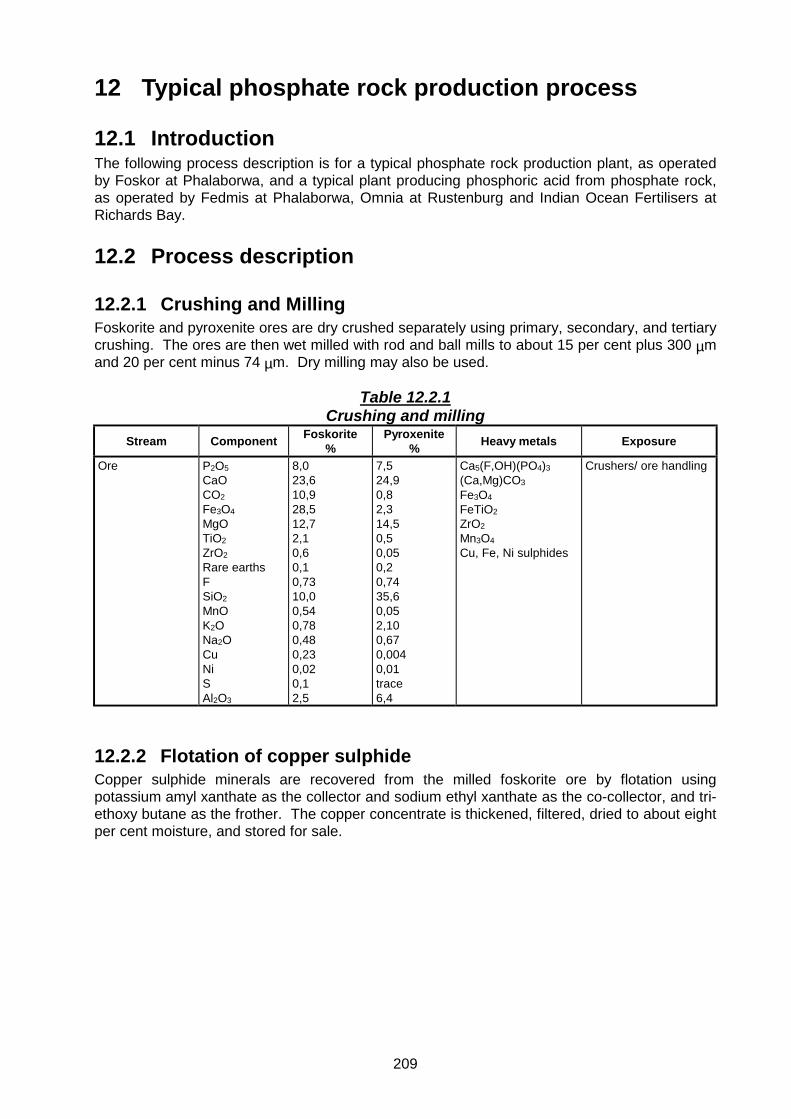
209
12 Typical phosphate rock production process
12.1 IntroductionThe following process description is for a typical phosphate rock production plant, as operatedby Foskor at Phalaborwa, and a typical plant producing phosphoric acid from phosphate rock,as operated by Fedmis at Phalaborwa, Omnia at Rustenburg and Indian Ocean Fertilisers atRichards Bay.
12.2 Process description
12.2.1 Crushing and MillingFoskorite and pyroxenite ores are dry crushed separately using primary, secondary, and tertiarycrushing. The ores are then wet milled with rod and ball mills to about 15 per cent plus 300 µmand 20 per cent minus 74 µm. Dry milling may also be used.
Table 12.2.1Crushing and milling
Stream Component Foskorite%
Pyroxenite% Heavy metals Exposure
Ore P2O5CaOCO2
Fe3O4
MgOTiO2
ZrO2
Rare earthsFSiO2
MnOK2ONa2OCuNiSAl2O3
8,023,610,928,512,72,10,60,10,7310,00,540,780,480,230,020,12,5
7,524,90,82,314,50,50,050,20,7435,60,052,100,670,0040,01trace6,4
Ca5(F,OH)(PO4)3
(Ca,Mg)CO3
Fe3O4
FeTiO2ZrO2
Mn3O4
Cu, Fe, Ni sulphides
Crushers/ ore handling
12.2.2 Flotation of copper sulphideCopper sulphide minerals are recovered from the milled foskorite ore by flotation usingpotassium amyl xanthate as the collector and sodium ethyl xanthate as the co-collector, and tri-ethoxy butane as the frother. The copper concentrate is thickened, filtered, dried to about eightper cent moisture, and stored for sale.

210
Table 12.2.2Flotation of copper sulphide
Stream ComponentTypical
concentrationsas % dry solids
Heavy metals Exposure
Copperconcentrate
CuS+CuFeS2 +Cu5FeS4+Cu2S
+ lowconcentrations ofheavy metals insame species asfound in ore
35,0 CuS+CuFeS2
+Cu5FeS4+Cu2S
+ low concentrations ofheavy metals in samespecies as found in ore
Copper concentratestorage/handling
12.2.3 Magnetic separation of magnetiteAfter removal of copper by flotation, magnetite (Fe3O4) is removed from the foskorite streamusing low-intensity drum magnets.
Table 12.2.3Magnetic separation of magnetite
Stream ComponentTypical
concentrationsas % dry solids
Heavy metals Exposure
Magnetite product Fe2O3
FeOMgOTiO2
NiOLow concentrationsof “heavy” metals insame species asfound in ore
73,023,52,53.00,01
Fe3O4
NiOTiO2
Low concentrations ofheavy metals in samespecies as found in ore
MagnetiteProduct storage/handling
12.2.4 Phosphate flotationA stream of phosphate-containing slurry joins the non-magnetic stream of foskorite from themagnetic concentrator. This slurry originates from a foskorite ore (10 per cent P2O5) fromwhich copper and magnetite have been removed.
Flotation reagents, comprising sodium silicate as dispersant, nonyl phenyl tetraglycol ether as amodifier and depressant, and distilled tall-oil fatty acid as a collector are added to the combinedstream and concentrates, designated 88S and 88SL are produced.
The milled pyroxenite ore is treated with sulphonate and tall-oil as flotation reagents andconcentrate designated 88P is produced.
12.2.5 Phosphate rock concentrate treatmentThe flotation concentrates are thickened. A portion is utilised for local phosphoric acidproduction. The remainder is filtered, dried, and stored in various stockpiles (according tomarket specification) for domestic and overseas sale.

211
Table 12.2.5Phosphate rock concentrate treatment
Stream Component
88S%by
mass
88P%by
mass
88SL%by
mass
Heavymetals Exposure
Concentrates P2O5CaOMgOAl2O3
Fe2O3
FCl (ppm)SiO2
La2O3
CeO2
ThO2 (ppm)TiO2 (ppm)SrOY2O3
Na2OK2O
40,253,00,540,060,192,486700,370,110,241501300,452140,130,03
40,353,90,440,120,142,82400,820,140,301321280,472400,130,07
40,253,90,650,050,212,416700,410,090,21<1001300,552140,130,03
Apatite:Ca5(F,OH)(PO4)3Monazite:(Ce, La, Y, Th)PO4
Magnetite:Fe3O4TiO2
Phosphate rockproduct handling/storage
12.2.6 Phosphoric acid productionThe phosphate rock concentrate, containing fluorapatite, Ca10(PO4)6F2, is despatched locally viaslurry pipeline. Phosphoric acid is manufactured by acidulation using sulphuric acid. Thereaction results in the formation of mainly phosphoric acid (H3PO4) and gypsum (CaSO4.2H2O),in this case known as phosphogypsum.
Phosphogypsum comprises mainly CaSO4.2H2O with P2O5. The table below shows the heavymetals present.
Table 12.2.6Phosphoric acid production
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Phosphoric acid P2O5MgOFe2O3
Al2O3
K2ONa2OSO4
FClAsCdCuPbVMnSrThUCr
5520,450,050,040,053,180,28175 ppm14 ppm2 ppm200 ppm1 ppm20 ppm250 ppm2 ppm8 ppm5 ppm30 ppm
As, Cd, Cu, FePb,V, Mn,Sr, Th, U,Cr - present asionic species inhighly acidicmedium , probablyas phosphates
Phosphoric acidproduct storage
Waste from scrubber Similar to phos-phogypsum
Similar to phos-phogypsum
Similar to phos-phogypsum
Waste storage/handling

212
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Phosphogypsum CaSiO2
P2O5
H2SiF6FSO4
VCrCuSeYZrLaCePrNdSmEuGdTbDyHoErTmYbLuThU
26 – 340,1 - 21,00,35455 – 5910 ppm50 ppm30 ppm75 ppm200 ppm700 ppm1600 ppm240 – 3000 ppm1000 ppm150 ppm25 ppm120 ppm10 ppm35 ppm4 ppm7 ppm1 ppm3 ppm0,4 ppm< 1 ppm50 – 150 ppm5 – 10 ppm
CaSO4
V, Cr, Cu,Se, Y, Zr, Uas sulphates
Phosphogypsumhandling/wastedump
12.3 Flow diagramThe flow diagram for the phosphate rock production process is shown in Figure 12.3.
12.4 Process assessment
12.4.1 Hazard identification`The major concern in the phosphate rock production plant is the possibility of exposure to dustin some areas. The copper sulphide concentrate from the flotation step is stored atapproximately 8 per cent moisture, thereby minimising the potential for dust dispersion. At themagnetite storage and handling facilities dust may be generated. This contains approximately73 per cent Fe2O3, and 23.5 per cent FeO. Because of the high iron content, the dust shouldbe managed to lower ambient air concentrations than for particulates not classified in terms ofspecific toxic elements (see Table 3.4.2). At the phosphogypsum handling and waste dumpareas levels of heavy elements are so low that management of dust would also effectivelycontrol exposure to heavy metals. Most of the process steps are under wet conditions withoutany potential for generating dust or airborne heavy metals.

213
Figure 12.3 Process diagram for the phosphate rock production process

214
12.4.2 Toxicological assessmentIron oxide is not considered to be inert dust (particulates not otherwise classifiable), becauseinhalation may lead to effects known as siderosis, iron pneumoconiosis, hematitepneumoconiosis, and iron pigmentation of the lung. It appears that the pulmonary effects aresomewhat more serious than those caused by inert dust. Systemic effects relating to excessivehaemosiderin deposits have also been documented. It has not been proved that iron oxidesare carcinogenic following chronic pulmonary exposure. The toxicity of iron and its compoundshas been discussed in Section 3.3.4.12.
12.4.3 Exposure assessmentSampling and analytical methods for airborne iron have been listed in Table 3.4.2.6. NIOSHMethod 7300 and OSHA ID 121 are appropriate for quantification of particulate-associated iron. There is no biological monitoring method to assess exposure to iron, because iron is anessential element present in the human body.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
12.4.4 Risk quantificationIn controlling exposure to iron oxide, it is not adequate to control dust levels to 10 mg/m3,because the level of iron may be above 5 mg/ m3 at particulate levels lower than 10 mg totaldust/m3.
12.5 ReferencesRoux et al. 1989. Phosphate in South Africa. Journal of the South African Institute of Miningand Metallurgy, 89 (5):129 -139.
Schorr, M. et al. 1997. Wet process phosphoric acid:production, problems and solutions. Industrial Minerals, 355: 61-71.
Rutherford, P.M., Dudas, M.J. & Samek R.A. 1994. Science of the Total Environment, 149: 1– 38.

215
13 Platinum group metal refining
13.1 IntroductionThe platinum group metals (PGM), platinum, palladium, rhodium, ruthenium, iridium andosmium together with gold and silver generally occur in nature associated with base metalssuch as iron, copper, nickel and cobalt, as well as a wide range of minor elements such asselenium, tellurium and arsenic. Initial processing of PGM ores (e.g. flotation, smelting andbase metal leaching) results in a concentrate containing 30 per cent to 60 per cent PGM plusvarying amounts of base metals, minor elements and silica. Where impurity levels are high, theconcentrate may be subjected to an upgrade step such as a sulphate roast/acid leach toremove remaining heavy metals, followed by a reductive roast of the residue to remove oxygen. Obviously where such roasting takes place, the roaster gases will contain toxic materials, suchas arsenic and selenium.
Classical refining processes are based on leaching and complex selective precipitationtechniques. These often have poor separation efficiencies, complicated by the presence ofimpurities. As a result of the multiple filtration and washing steps which generate recycledliquids and residues, which also have to be processed, primary yields are low and there is asignificant ‘lock-up’ of PGM’s. Because of the multiple handling, the process is labour intensivewith a high risk of exposure to allergenic platinum salts.
Extensive research by refining companies into newer, more selective separation technologiessuch as solvent extraction and ion exchange, has led to the development of more continuous,‘single-stream’ processing. The advantages of the new processes include a very much smallerlock-up, reduced operating costs and a lower occupational health risk resulting from the use ofenclosed plant and equipment.
Because of the competitive nature of the business and the high value of the products, very littledetail of the processes used by the individual South African refiners has been published. It istherefore not possible to identify species and specific health hazards associated with individualunit operations. Without input from the producers about their specific processes, theoccupational health risk can only be dealt with in general terms.
It is known that all dusts containing PGM salts are hazardous and the industry takes stringentprecautions to prevent emissions.
13.2 Process descriptionAs noted above, details of the South African producers’ refining processes are not published inthe open literature, and the sequence in which the PGM’s are extracted and the processesused differ from refiner to refiner. The ‘side-stream’ processes for the production of the finalproduct may also be different.
The health risk in the ‘single-stream’ extraction area is likely to be a function of how well theprocesses are enclosed, ventilation efficiency, and process liquor spillage control. Greaterexposure is likely in the ‘side-stream’ processing areas where there is more intensive handlingof the products.
13.2.1 LeachingThe first stage of the newer processes is the total leaching of the PGM’s and gold. Ahydrochloric acid-chlorine medium is used. Leaching is carried at above ambient temperatures. Silver remains as insoluble silver chloride and is recovered from the residue after filtration.

216
The filtrate containing the dissolved precious metals proceeds through the unit operationswhere the individual metals are extracted.
Table 13.2.1Leaching
Stream ComponentTypical
concentrations%
Heavy metals Exposure
PGM concentrate
Leach solution
PGM + AuCu + Ni + CoFeSSiO2Other
GoldPlatinumPalladiumRhodiumRuthenium
IridiumOsmiumBase metals
20 - 3012 - 1515 – 205 – 105 – 1020 - 30
Base metal and PGMsulphides, oxides andmetallics
(AuCl4)-
(PtCl4)2-, (PtCl6)2-
(PdCl4)2-, (PdCl6)2
(RhCl6)3-
(RuCl6)2-, (RuCl6)3-
(Ru2OCl10)4-,(RuCl5H2O)2-
(IrCl6)2-, (IrCl6)3-
(OsCl6)2-
Base metal cations
13.2.2 Gold extractionGold is extracted on a selective ion exchange resin. When the resin is loaded, solution flow isswitched to a standby resin column and the gold eluted from the loaded column, possibly afteran initial resin wash.
Some refiners use solvent extraction to extract gold.
Gold is recovered from the eluate or scrubbed solvent by reduction.
Table 13.2.2Gold extraction
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Au extraction PGM salts No data PGM salts Handling areas
13.2.3 Palladium extraction Following gold extraction, the solution is pumped to the palladium separation circuit wherepalladium is extracted using “Molecular Recognition Technology”. This is also an ion exchangeprocess. Palladium is recovered from an eluate by means of ‘palladium salting’.
Solvent extraction is also an option for palladium extraction. Alternative recovery processesinclude the precipitation of palladium as a salt.
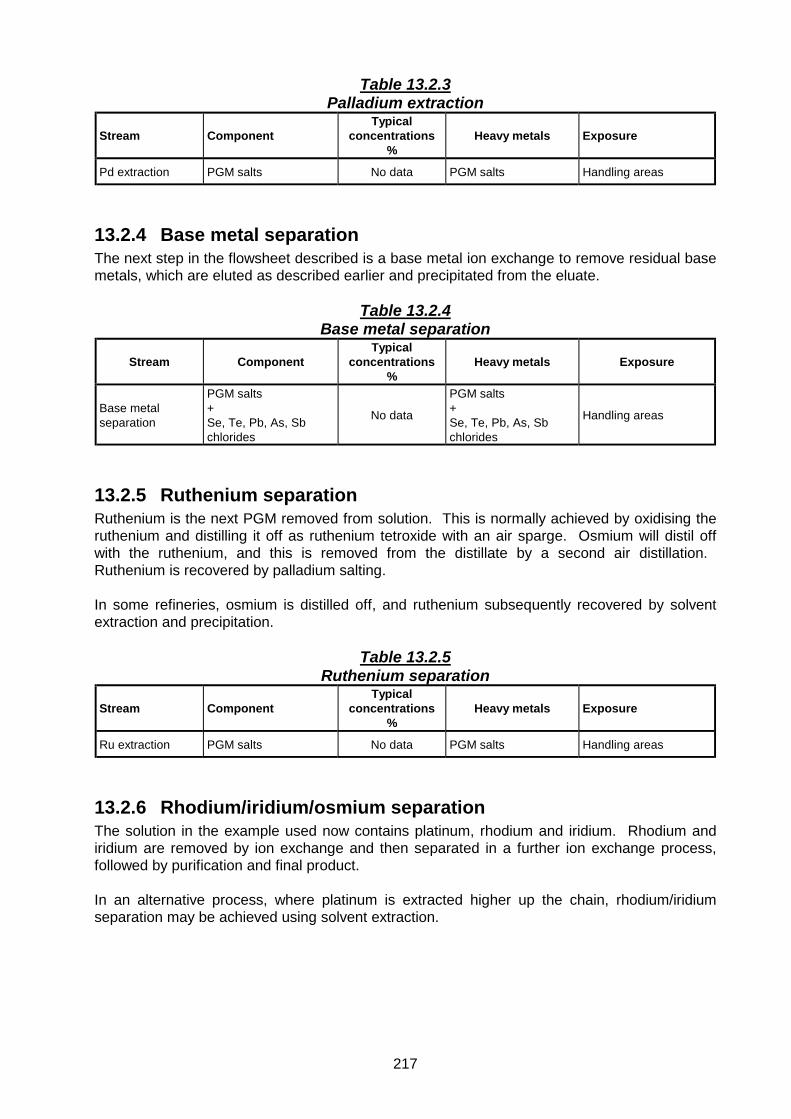
217
Table 13.2.3Palladium extraction
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Pd extraction PGM salts No data PGM salts Handling areas
13.2.4 Base metal separationThe next step in the flowsheet described is a base metal ion exchange to remove residual basemetals, which are eluted as described earlier and precipitated from the eluate.
Table 13.2.4Base metal separation
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Base metalseparation
PGM salts+Se, Te, Pb, As, Sbchlorides
No data
PGM salts+Se, Te, Pb, As, Sbchlorides
Handling areas
13.2.5 Ruthenium separationRuthenium is the next PGM removed from solution. This is normally achieved by oxidising theruthenium and distilling it off as ruthenium tetroxide with an air sparge. Osmium will distil offwith the ruthenium, and this is removed from the distillate by a second air distillation. Ruthenium is recovered by palladium salting.
In some refineries, osmium is distilled off, and ruthenium subsequently recovered by solventextraction and precipitation.
Table 13.2.5Ruthenium separation
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Ru extraction PGM salts No data PGM salts Handling areas
13.2.6 Rhodium/iridium/osmium separationThe solution in the example used now contains platinum, rhodium and iridium. Rhodium andiridium are removed by ion exchange and then separated in a further ion exchange process,followed by purification and final product.
In an alternative process, where platinum is extracted higher up the chain, rhodium/iridiumseparation may be achieved using solvent extraction.

218
Table 13.2.6Rhodium/iridium/osmium separation
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Rh, Ir, Os PGM salts No data PGM saltsParticularly OsO4
Handling areas
13.2.7 Platinum recoveryThe barren solution, after rhodium/iridium removal, still contains the platinum values. Thesolution is purified ahead of final platinum production.
Platinum may be recovered higher up the chain by solvent extraction, and as with palladium,precipitated as a salt.
Table 13.2.7Platinum recovery
Stream ComponentTypical
concentrations%
Heavy metals Exposure
Pt extraction PGM salts No data PGM salts Handling areas
Barren brine Se, Te, Pb, As, Sbchlorides No data Se, Te, Pb, As, Sb
chloridesHandling/evaporation ponds
13.3 Flow diagramThe flow diagram for the platinum group metal refining process is shown in Figure 13.3.
13.4 Process assessment
13.4.1 Hazard identificationAlthough the extraction and separation processes are conducted in closed reactor systems,certain reaction conditions are at elevated temperatures and it is known that leaks may occur atvalves and flange seals. Exposure may also occur during maintenance activities on ventilationsystems. This may lead to exposure not only to the platinum group metals, but also to otherelements, for example arsenic, selenium, and others as indicated in the tables above. Itappears that apart from the platinum group metals, arsenic is the major element of concern. Abetter understanding of potential hazards would however require investigation of particularprocess steps and materials, relying on confidential information. The following discussionscover all the elements that may be of interest, leaving it up to the particular plant health riskmanager to select the priorities for monitoring and control.
The elements below have been identified to be of potential concern:• The platinum group, i.e. Pt, Pd, Rh, Ru, Ir and Os.• Associated elements Au and Ag.• Base metals Fe, Co, Cu and Ni.• Minor elements such as As, Pb, Sb, Se and Te.
It is unlikely that exposure will be relevant in all cases, but the exposure assessmentnevertheless provides information on all the elements of interest. Gold has not been included inthe selection of hazardous heavy metals (see Section 3.2), and silver is unlikely to be present at

219
Figure 13.3 Process diagram for a platinum group metal refining process
220
levels of concern except where refining is specifically for silver. The base metals Fe, Co, Cuand Ni are normally separated from the platinum group metals and are processed separately,as described in Section 11.
13.4.2 Toxicological assessmentSalts of the platinum group metals are sensitisers upon chronic exposure, causing allergieslike rhinitis, conjunctivitis, asthma, urticaria and contact dermatitis. See Sections 3.3.4.18,3.3.4.19, and 3.3.4.20 for a description of the toxicity of platinum group metals.
Arsenic is a confirmed human carcinogen, and is known to cause contact dermatitis. SeeSection 3.3.4.2 for a description of arsenic toxicity.
Lead is a cumulative toxin. It is well known for neurotoxic effects, but has been associated witha whole range of other possible symptoms and effects. Section 3.3.4.13 provides an overviewof lead toxicity.
Occupational exposures to antimony compounds have been associated with the developmentof pneumoconiosis as well as impairment of the lung function, and some antimony compoundsare considered to be possible carcinogens. See Section 3.3.4.1 for an overview of antimonytoxicity.
Occupational exposure to selenium may cause a wide range of non-specific symptoms, asdescribed in Section 3.3.4.21.
Tellurium has relatively low toxicity, but can be converted in the body to form dimethyl telluride,which gives a garlicky odour to the urine, breath and sweat. Section 3.3.4.24 provides anoverview of tellurium toxicity.
13.4.3 Exposure assessmentArea monitoring and personal sampling for antimony and its compounds may be conductedusing NIOSH Methods 2(S2) and 4(261), and OSHA ID 121 and ID 125.
NIOSH has developed Method 8005 to determine antimony in blood or tissue, and Method 107for determination in urine. Based on somewhat limited data on exposure to pentavalentantimony, it has been estimated that an airborne concentration of 0.5 mg/m3 would lead to aurinary concentration of 35 µg/g creatinine during a shift. Background concentrations in urinehave been determined in the range of 0.2 and 1 µg/g creatinine (Lauwerys and Hoet, 1993:19).Antimony has not been listed for biological monitoring in South Africa.
Area monitoring and personal sampling for arsenic and its compounds may be conductedusing NIOSH Methods 7300, 7900 and 7901, and OSHA ID 105 and OSHA CIM. NIOSHMethod 7900 is valid only for particulate-associated inorganic arsenic compounds. The mostappropriate method for the exposure scenerio has to be selected.
Mean serum and blood levels of arsenic vary greatly depending on the level of seafood contentin the diet. Therefore, when employees have not been instructed to refrain from eating fish orshellfish for two to three days before biological monitoring, high levels of arsenic may be foundthat might not be associated with occupational exposure.
In the past, biological monitoring for assessment of occupational exposure was conducted bymeasuring the total amount of arsenic in urine at the end of a shift. It is however now wellestablished that inorganic arsenic, monomethylarsonic acid, and cacodylic acid in urine is themethod of choice. Monitoring of employees exposed to inorganic arsenic using this method isnot influenced by organoarsenicals from marine origin.

221
Some controversial results may be obtained in the correlation between air-concentrationexposure assessment and biological monitoring. It has been established that backgroundlevels of the sum of the three metabolites of arsenic (inorganic arsenic, monomethylarsonicacid, and cacodylic acid) in urine vary between 10 µg/l and 50 µg/l. It appears that the bestrelationship for occupational exposure at air concentrations between 50 and 200 µg As/m3
would lead to post-shift concentrations of the total metabolites between 54 and 88 µg/gcreatinine (Lauwerys and Hoet, 1993: 25).
Medical surveillance for monitoring of effects include full blood count, liver function tests, urinetests for creatinine and proteinurea, spirometry, and electrocardiography in selected cases
Area monitoring and personal sampling for the lead and its compounds may be conductedusing NIOSH Methods 7082, 7105, 7300, 7505, and OSHA ID 121 and ID 125 G G (see Table3.4.3.6). The most appropriate method has to be selected for the particular exposure scenario.
Approximately 50 per cent of the lead deposited in the lung is absorbed, whereas less than 10per cent of ingested lead normally gets into the systemic circulation. Dermal absorption of leadis also a significant route of exposure. Biological tests for lead exposure can be divided intotwo groups, i.e. those directly reflecting the exposure through assessment of the amount storedin blood, urine, hair, and bone, and those indicating the early biological effects of lead inrelation to exposure. These effects are shown in haemoglobin, haematocrit, stippled cells,coproporphyrin in urine, etc. In a steady-state situation, lead in blood is considered to be thebest indicator of recent exposure. It has been shown that under low exposure conditions(environmental levels) an increase of 1 µg/m3 in air leads to an increase of 1 to 2 µg/100 ml ofwhole blood. There is however not a clear correlation between air concentrations and bloodlead at higher exposure concentrations, and it is therefore difficult to assess occupationalexposures. The situation is further complicated by the fact that lead is a ubiquitous pollutant,leading also to nonoccupational exposures. As a rule, it is accepted that blood-lead levels ofnon-occupationally exposed individuals lie between 15 and 30 µg/100 ml of whole blood. Levels up to 70 µg/100 ml in lead-related occupations are normally considered acceptable. However, subclinical effects may occur at levels exceeding 50 µg/100 ml of whole blood. TheWorld Health Organisation has proposed 40 µg/100 ml as the maximum tolerable lead value inblood for adult male workers, and 30 µg/100 ml for women of childbearing age (Lauwerys andHoet, 1993:86). No guideline has been proposed for biological monitoring of lead exposure inSouth Africa.
Lead in urine is often preferred to blood analysis, and reflects the amount of lead recentlyabsorbed. There is however a poor association between lead in blood and lead in urine, andblood-lead is considered the more reliable measure for routine assessment of lead exposure. Aconcentration of lead in blood of 50 µg /100 ml usually corresponds with a level of 150 µg /gcreatinine, but the correlation across a wider exposure range is poor. The level of 150 µg Pb/gcreatinine corresponds with an air concentration of 50 µg Pb/ m3.
Although it has been suggested that hair provide a time-integrated index of lead absorption, ithas drawn limited interest because of potential lead contamination in hair-washing procedures(Lauwerys and Hoet, 1993:86).
Area monitoring and personal sampling for the platinum group metals and compounds maybe conducted using NIOSH Method 7300 and OSHA CIM. The most appropriate method has tobe selected for the particular exposure scenario.
Platinum can be determined in blood or tissue using NIOSH Method 8005, but the relationshipbetween these levels and exposure has not been established.

222
Area monitoring and personal sampling for selenium and its compounds may be conductedusing NIOSH Method 7300 and OSHA CIM.
The biological significance of selenium in blood and urine is not clear, but it appears that theconcentration in serum (or plasma) and urine reflects short-term exposure, whereas theselenium content of erythrocytes may be associated with long-term exposure. There is noindication that selenium in hair may be used to assess the selenium body burden. A biologicalthreshold limit of 100 µg/l for selenium in urine has been proposed, but this is associated withgreat uncertainty (Lauwerys and Hoet, 1993:86). There is no guideline for biological monitoringin South Africa.
Area monitoring and personal sampling for tellurium and its compounds may be conductedusing NIOSH Method 7300 and OSHA ID 121.
Little is known about the human metabolism of tellurium, and concentrations in urine may berelated to amounts absorbed. Direct correlations are however unknown. It has beensuggested that levels in urine below 1 µg/l would prevent the tellurium-associated garlic odourof breath. No guideline for biological monitoring has been set in South Africa.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
13.4.4 Risk quantificationTraditionally, the primary concern in refining of the platinum group of metals has beensensitisation of employees. This is manifested primarily as bronchial dysfunction, which mayrequire from a few days to several years of exposure to develop. The platinum group metals,as well as lead, selenium and tellurium, can be assessed against occupational threshold limitsusing the hazard-quotient approach. Exposure to lead can also be quantified through biologicalmonitoring.
Occupational exposure levels for arsenic have to be assessed through interpretation of areaand personal monitoring data, in conjunction with biological monitoring and exposure effectsmonitoring. Cancer risks can be quantified through interpretation of exposure data and arsenicdose-response information.
13.5 ReferencesAnonymous. 1988. The development and implementation of novel refining processes for theplatinum group metals (including the refining of anode slimes). Mintek Application Report No.14. Randburg: Mintek,
Anonymous. 1998. Impala platinum metals refinery at Springs upgraded. Mining Mirror. August.
Anonymous. 1999. Impala refinery completes its upgrade. SA Mining, Coal, Gold and BaseMetals, May.
Charlesworth, P. 1981. Separating the platinum group metals by liquid-liquid extraction.Platinum Metal Review, 25(3): 106 – 112..
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.
Republic of South Africa, Mintek. 1988. The development and implementation of novelrefining processes for the platinum group metals. . Application Report No. 14.

223
Rimmer, B.F. 1987. Refining of platinum group metals. Transactions of the Institution ofMining and Metallurgy, Section A, 96: A117 – A119.

224

225
14 Typical stainless steel process
14.1 IntroductionStainless steel is produced in a series of process functions viz. melting, refining, casting ofingots, ingot conditioning, ingot re-heating prior to rolling, hot rolling, de-scaling, annealing andpickling, cold rolling, annealing and pickling after cold rolling, skin passing, levelling, cutting tosize and packing. Bright annealing is also done for some steel grades and applications.
14.2 Process descriptionThe process description and flow diagrams of a typical stainless steel process are included inthis section. The process description and diagrams contain data on the process streams andidentify the species containing heavy metals, which occur on the plant, as well as the potentialexposure points.
14.2.1 Raw material receipts and charge preparationStainless steel is made by melting steel scrap in an electric arc furnace together with stainlesssteel scrap and ferroalloys. Fluxes are added to aid the removal of impurities and to produce aslag, which will allow clean separation of the slag-forming constituents in the furnace chargefrom the crude stainless steel.
Many of the alloys charged are friable and attrition of the surface causes dust formation. Thedusts formed naturally have an analysis typical of the alloy from which they are abraded. Ferrochrome or charge chrome, and ferrosilicon are fairly friable compared withferromanganese, ferroboron, ferrotitanium, low carbon ferrochromium and ferromolybdenum. Typical fluxes used in the operation are burnt lime and fluorspar. The dusts occur in theprocess of off-loading the materials on receipt and in recovering the materials when weighingthem off for charging into the electric arc furnace. The heavy elements are in the alloy form,often in solid solution with iron. The elements chromium, iron, manganese and silicon will be inhigher concentration than titanium, molybdenum and other minor alloys. Table 14.2.1 showsthe composition of the more usual alloys.
The alloys are weighed off together with steel scrap, stainless steel scrap and flux and can becharged directly into the electric arc furnace or via feed ports in the furnace roof.
Table 14.2.1Raw material receipts and charge preparation
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Stainless steel scrap FeCMnPSSiCrNiMoTiN
Balance0,03 – 0,1520,0450,031 – 1,516 – 266 – 222 – 40,70,1
FeMnCrNiMoTi
Raw material off-loading/storage/handling

226
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Steel scrap CrFeCMnSP
<1990,150,2<0,05< 0,5
CrFeMnFeCr3
Cr7C3
Raw material off-loading/storage/handling
Nickel NiCuCo
100TraceTrace
NiCuCo
Raw material off-loading/storage/handling
Ferrochrome CrFeSiCSPAl
52332 – 46 – 8< 0,03< 0,02< 0,03
CrFeCr3C2,Cr7C3,Cr3Si, CrSi,Cr5Si3, Cr23C6,CrFe (solid solution)
Raw material off-loading/storage/handling
Ferromanganese FeSiCMnSPAl
15< 1,27,5> 75< 0,02< 0,02<0,02
FeMnMn3C, Mn3Si,Mn5Si3, Mn7C3,MnC2, MnC12,MnS. MnP,MnSi, MnC12
Raw material off-loading/storage/handling
Ferrosilicon FeSiSPAl
24>75<0,02< 0.02< 0,5
FeSi, FeSi2,Fe3Si, Fe3Si7,
Raw material off-loading/storage/handling
Ferrotitanium FeSiCTiSPAl
60< 5<0,1525<0.02< 0,02< 8
TiFe, TiFe2,TiAl, TiAl3,
TiC, TiS2,TiS3, TiSi2,Ti5Si3 TiS2,TiS3
Raw material off-loading/storage/handling
Ferronickel FeNiCSPAl
7425< 0,1<0,02<0,02<0.02
FeNiNiSFe3C
Raw material off-loading/storage/handling
Ferroboron FeBAlSi
Balance15 – 171 – 3< 1
FeBIntermetalliccompoundsFeB, Fe2B
Raw material off-loading/storage/handling
Ferromolybdenum FeMoCSiSPSbCuSn
Balance> 550,1 – 0,21 – 20,20,1 – 0,20,05 – 0,10,08 – 2,50,05 – 0,1
Fe, Sb, Cu.Mo, Mo2C,Mo3Si, Mo5Si,MoC, MoS2,MoSi2
Raw material off-loading/storage/handling

227
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Lime CaOMgOAl2O3
FeOMnOSiO2Fe2O3
91,31,70,30,30,10,8
CaOMnOFeOFe2O3
Raw material off-loading/storage/handling
Fluorspar CaF2
SiO2
SulphidesPbPhosphateDolomite
85 min5 max0,3 max0,5 max0,3 max0,2 max
CaF2
PbORaw material off-loading/storage/handling
Dolomite (burnt) MgOCaOAl2O3
Loss on ignition
38.253.30,46,3
CaO Storage/handling
14.2.2 Furnace charging and meltingThe charge weighed off for the furnace may be in several charging boxes and some of thealloys could be charged via a charging port in the furnace roof. Dust will occur in the furnacewhen charging, and should under normal circumstances be retained in the furnace or besucked of into the furnace dust collection system. Stray dust plumes can arise from the side-charging door of the furnace.
The initial arc struck in the furnace is unstable as the scrap is melted. This causes more dustand gas evolution than normal. Once the bath is molten a steady arc is formed and gas anddust evolutions are low. Some refining of the crude stainless steel can be done in the furnaceby lancing the bath with oxygen. During this operation heavy fumes can be formed, some ofwhich can escape the furnace. These fumes contain the oxides of the easily oxidized alloys,manganese, molybdenum, silicon, chromium and iron. When melting has been completed,fluxes are added, the melt heated to the tapping temperature of 1600 to 1700 OC and tappedinto a transfer ladle. Ferrosilicon and lime are added to the ladle to reduce oxidized chromiumand manganese, with the evolution of reaction gases containing some volatilised oxides, mainlysilicon and manganese, with some iron and chromium. The reaction is normally carried outunder an extraction hood and the dust and fume captured in the dust collection system.
The slag produced from the melting operations is transported in the molten state, in ladles, to aslag dump, where it is tipped out and solidifies. The slag is recovered, crushed, and the metalremoved magnetically or by gravity separation techniques. The recovered stainless steel is re-melted, whilst the slag is deposited on a slag dump.

228
Table 14.2.2Furnace charging and melting
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Furnace dust Fe2O3
MnOCr2O3
NiOZnOPbOCaOMgOAl2O3
CSK2ONa2O
40 – 421,5 – 2,511 – 130,5 – 1,522 – 280,5 – 14 – 61 – 20,5 – 1,00,1 – 0,20,2 – 0,50,35 – 0,450,5 - 1
FeOFe2OMoO2Fe2O3
MnOCr2O3CrO3
NiOZnOPbOCaO
Furnace area/bag house
Melting furnace slag Cr2O3
FeOSiO2
CaOMgOAl2O3
NiO
10 –120,730 – 3212 - 1518 – 2020 – 24< 1
Cr2O3
FeOCaONiOFe2SiO4
Fe2TiO5
Ca2SiO4
Ca3SiO7
Magnesia - carbonrefractories – newand spent
MgOC
88 – 955 - 12
Storage/handling
Dolomite –magnesiterefractories – newand spent
MgOCaO
38,058,0
CaO Storage/handling
14.2.3 Stainless steel refiningAfter removing the slag from the molten steel, the metal is transferred to a refining vessel. Thiscould be an Argon-Oxygen Decarburisation (AOD) converter, a Creusot-Loire Uddeholm (CLU)converter or a Vacuum Oxygen Decarburisation (VOD) unit. In the case of the CLU, refining iscarried out using oxygen and superheated steam as refining agents, which are introducedthrough tuyeres placed in the bottom of the vessel. The reaction is controlled at 1680 to 1780OC through the introduction of argon or nitrogen into the gas mixture at various ratios to theoxygen and steam. After decarburisation has been completed, the steel is purged with argon oran argon and nitrogen gas mixture and lime and ferrosilicon are added to reduce chromium andmanganese oxides from the slag.
Oxygen is blown into the top of the converter to aid post combustion of the reaction gases. Specific consumption rates for a typical stainless steel are:
Oxygen 35 m3/tonNitrogen 25 m3/tonNitrogen 15 m3/tonArgon 4 m3/ton
(m3 refers to normal cubic meters, i.e. at 25 °C and atmospheric pressure.) Refining of a 100-ton load takes approximately 60 minutes.

229
The oxides of all the heavy metals in the scrap and ferroalloys are present in the off-gases fromthis process. The fume is captured and collected in a dust collection system. Slag from thisprocess is dumped onto a slag dump that may be processed to recover metal.
Slag produced from the converting operation is transported in the molten state, in ladles, to thesame slag dump as used for the furnace slag, and stainless steel is recovered in the same way.
Table 14.2.3Stainless steel refining
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Dust and fume fromconverter
Fe2O3
MnOCr2O3
NiOPbOCaOMgOAl2O3
CSK2ONa2OZnO
35 – 405 – 1012 – 200,5 – 0,20,4 – 0,66 – 120,5 – 10,4 – 0,60,5 – 1,20,20,2 – 0,40,4 – 0,5Not known
FeOFe2O3
MnOCr2O3
NiOPbOCaOZnO
Refining area/dust cleaning plant
Slag Similar tofurnace slag
Similar to furnaceslag
Similar to furnaceslag
Slag dump
Magnesia - carbonrefractories – newand spent
MgOC
88 – 955 - 12
Storage/handling
Dolomite –magnesiterefractories – newand spent
MgOCaO
38,058,0
CaO Storage/handling
14.2.4 Continuous castingThe refined steel is transferred to the continuous casting machine where the molten steel istapped into an oscillating mould via a tundish. Controlled solidification of the slab cast occurs inthe mould and caster. The string of slab is cut to length for further processing. The cooled slabis surface ground to remove casting defects. In the casting process various mould powders areused. These have a low melting point and coat the mould so as to promote a defect-freesurface. Fumes will be emitted from the casting process and will contain the oxides of theheavy metals in the stainless steel. In the slab grinding bay the metal removed is in the form ofswarf, a mixture of metal and metal oxides and grinding wheel compound. This material is re-melted.
Table 14.2.4Continuous casting
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Dust/fume Same as refining Same as refining Same as refining Casting machine

230
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Grindings fromslab
NiCrFeMoTiSi
8 – 2018 – 25Balance0,1 – 30,2 – 0,50,3 – 0,5
NiCrFeMoTi
Slab grinding station
14.2.5 Hot rollingSlabs are charged into a walking-beam furnace for re-heating before rolling. The slabsdischarge from the furnace at the required temperature, approximately 1300 oC for austeniticstainless steel grades, and 1150 oC for ferritic grades.
Hot ingots are rolled from 150 to 250 mm to two to ten mm thick steel which is cooled andcoiled. Ingots are also rolled to plate more than ten mm thick.
Fuel gas from Sasol is used to fire the furnaces. The gas is a synthetic gas containing 80percent methane with a calorific value of 31 to 35 MJ/m3. The slab is rolled down in a roughermill and finished off by rolling to the required thickness in a Steckle tandem mill. This mill has acoil-heating furnace where coils are kept hot during the rolling process. Water is used to breakthe scale formed during the re-heating and rolling process. Millscale is collected from thesump, supplying the de-scaling water for recycling to the process. This will typically containchromium, nickel, manganese and iron oxides.
Table 14.2.5Hot rolling
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Millscale FeOCr2O3NiOMnO2
MoOSiO
53 – 7020 - 278 – 190,3 – 0,50,3 – 0,50,5 – 0,7
FeOCr2O3NiOMnO2
MoO
De-scaling water pit
14.2.6 Annealing and picklingCoils and plate rolled on the mills require scale removal. Plates could be annealed in anannealing furnace at 1 050 to 1 120oC for austenitic steels, followed by pickling in acids. Thesecould be a dilute sulphuric acid pickle followed by a mixed acid, 100 to 220 g/l nitric acid and 15to 60 g/l hydrofluoric acid solution.
The spent acids are neutralised with lime and treated in an acid recovery plant. Hot mill coilcan be annealed and pickled in a continuous process electrolytically using a 150 – 200 g/lsodium sulphate solution followed by a mixed acid nitric acid and hydrofluoric acid pickling. Ferritic steels are annealed in a batch-anneal furnace at 850- 950 oC before pickling.

231
Table 14.2.6Annealing and pickling
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Waste picklingacid
HNO3
H2SO4HFNi, Fe, Cr,salts
Not known Ni, Fe, Cr,sulphates,nitrates,fluorides +Fe scale
Pickling/reagent recovery area
Acid recovery HNO3
H2SO4
HF
Not known Similar to wastepickling acid
Acid recovery area/wastedisposal
Lime As previous As previous As previous Lime storage/handling
14.2.7 Cold rolling and bright annealingThe annealed and pickled coil is transported to cold-rolling mills, which are normally of theSendzimar type or 4-high mills. The cold-rolled band is annealed and pickled or brightannealed. Bright annealing requires the annealing of the band in an inert atmosphere, which isprovided by a cracked ammonia atmosphere. The gas from this furnace is recovered andrecycled.
For special finishes grinding and polishing is carried out. Emery cloth of varying grit is used. Inthis process fine stainless steel and corundum arises, but as the process is carried out under ahood and the dusts extracted, there is a low probability of the dust becoming a hazard. Thedust is recycled to the melting process.
Table 14.2.7Cold rolling and bright annealing
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Steelproduct/dust
FeCMnPSSiCrNiMoTiN
Balance0,03 – 0,1520,0450,031 – 1,516 – 266 – 222 – 40,70,1
FeMniCrNiMoTi
Cold rolling areaBright annealing area
14.2.8 Cutting to length, slitting, packing and despatchingAfter annealing and pickling, or bright annealing the cold rolled band goes to the finishing lines,which consist of skin, pass mills, cut-to-length, slitting and packing lines. The finished productis dispatched to customers.

232
Table 14.2.8Cutting to length, slitting, packing and despatching
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Steelproduct/dust
As previous As previous As previous Cut – to-length,packing,despatch areas
14.2.9 Effluent treatment plantThe effluents from pickling and annealing are treated by adjusting the liquor pH with causticsoda. Nickel, chromium and iron are precipitated as metal hydroxides and filtered. The filtercake is deposited in a registered disposal site. Hexavalent chromium in the pickling effluent isreduced with ferric chloride before precipitation with caustic soda.
14.2.10 Water treatment/handlingA central water-treatment plant is usually installed, which would contain a pre-treatment plant, aprocess water plant and a high quality water plant. The process water is used mainly as amake-up water for re-circulation to direct cooling systems serving e.g. continuous casting watersprays, cold-mill roll cooling and rinsing, scrubbing and strip quenching in the annealing andpickling circuit. High quality water is used as steam–boiler feed, finished product rinsing andcooling water for critical cold mill parts. The water is firstly softened using lime and apolyelectrolyte, the sludge going to a sludge disposal area. The softened water will be furthertreated by filtration and cation and anion exchange systems to produce the high quality water.
14.3 Flow diagramThe flow diagrams for a typical stainless steel process are shown in Figures 14.3.1 and 14.3.2.

233
Figure 14.3.1 Process diagram for a typical stainless steel process, sheet 1 of 2

234
Figure 14.3.2 Process diagram for a typical stainless steel process, sheet 2 of 2

235
14.4 Process assessment
14.4.1 Hazard identificationIt is not certain how much dust can actually form due to the friability of the scrap metals in theraw materials handling area. The following discussion is based on the assumption that somedust may form, and that exposure to metals would therefore be of interest for assessment. Themetals in this context are iron, chromium, nickel, manganese and lead. Furnace dust thatforms during charging and melting may also lead to exposure to manganese oxide, chromiumtrioxide, nickel oxide, and zinc oxide.
Calcium oxide and calcium fluoride are present in certain areas, and exposure should beassessed for the potential development of irritation effects.
14.4.2 Toxicological assessmentIron oxide is not considered to be inert dust (particulates not otherwise classifiable), becauseinhalation may lead to effects known as siderosis, iron pneumoconiosis, hematitepneumoconiosis, and iron pigmentation of the lung. It appears that the pulmonary effects aresomewhat more serious than those caused by inert dust. Systemic effects relating to excessivehaemosiderin deposits have also been documented. It has not been proved that iron oxidesare carcinogenic following chronic pulmonary exposure. The toxicity of iron and its compoundshas been discussed in Section 3.3.4.12.
Chromium is an essential element in humans. Hexavalent chromium is a human carcinogen,as outlined in the toxicological assessment for chromium (see Section 3.3.4.8). Trivalentchromium is poorly absorbed, but allergic eczematous dermatitis has been observed followingindustrial exposures.
Certain nickel compounds are classified as human carcinogens, but noncarcinogenicsystemic effects have not been documented. Hypersensitivity to nickel is common, asdiscussed in the summary of nickel toxicity (Section 3.3.4.17).
Lead is a cumulative toxin. It is well known for neurotoxic effects, but has been associated witha whole range of other possible symptoms and effects. Section 3.3.4.13 provides an overviewof lead toxicity.
The primary concern of exposure to zinc is the oxide (ZnO), associated with what is known asmetal fume fever. Metal fume fever is generally considered to be transitory, but the possibilityof chronic respiratory effects resulting from ZnO inhalation cannot be dismissed.
Calcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicology of calcium oxide has been discussed in Section 3.3.4.7. Calcium fluoride isalso an irritant.
14.4.3 Exposure assessmentIron levels in the scrap stainless steel used as a raw material may be around 50 per cent.Taking exposure to iron oxide as a guideline, it can be shown that control of the dust should beadequate for control of exposure to iron in this area.
Levels of chromium and nickel in the scrap stainless steel are however high, and exposureshould be controlled not only for dust. For steel scrap the concern is for iron in the metal form. In nickel and ferrochrome the concern is also for nickel, chromium and iron.

236
Manganese levels are high in ferromanganese. In ferrosilicon and ferrotitanium, iron levels arehigh, and nickel and iron are present at high concentrations in ferronickel.
Calcium oxide is present at the raw materials storage and handling areas as lime and in burntdolomite, and exposure should be assessed for its irritation effects. Inorganic fluorides such ascalcium fluoride are generally highly irritating, and exposure is normally assessed on the basisof exposure to the fluoride. Exposure to lead from fluorspar would not exceed guidelineconcentrations if dust levels were controlled within the guideline concentrations. Please seeTables 3.4.2 and 14.2.1 for the concentrations of metals in dust and the relationship withmaximum levels that would be controlled adequately when dust exposure is controlled.
Furnace dust that forms during charging and melting appears to be the highest priority forcontrol of exposure. Table 14.2.2 indicates that exposure to manganese oxide, chromiumtrioxide, nickel oxide, and zinc oxide is of potential concern in this area. Also at the refiningvessel that operates at over 1 600 °C, similar exposure may occur. Although at relatively lowlevels, exposure to lead may be possible in this area. Although this appears to be of lowprobability, it is neverthesless listed as a precautionary item for discussion and assessment.
Sampling and analytical methods for airborne iron have been listed in Table 3.4.2.6. NIOSHMethod 7300 and OSHA ID 121 are appropriate for quantification of particulate-associated iron. There is no biological monitoring method to assess exposure to iron, because iron is anessential element present in the human body.
Exposure to chromium can be quantified using sampling and analytical methods listed in Table3.4.3.6. Determination of chromium in urine is the preferred method for assessing exposure tohexavalent chromium. Exposure to an air concentration of 0.05 mg Cr/m3 would be reflected ina urine concentration of 30 µg Cr/g creatinine at the end of the exposure period. Exposure totrivalent chromium compounds does not correlate with levels of chromium in urine.
Some nickel compounds have been linked to cancer, as indicated in the toxicological reviewfor nickel (Section 3.3.4.17). Sampling and analysis methods for airborne nickel compoundshave been listed in Table 3.4.3.6. Several studies have demonstrated that the concentrationsof nickel in plasma and urine are indicators of recent exposure. An ambient air exposure levelof 0.1 mg Ni/m3 corresponds approximately to a concentration of nickel in plasma and in urinecollected at the end of the workshift of 0.7 µg Ni/100 ml and 70 µg Ni/l (corrected for a specificgravity of 1.018), respectively.
Area monitoring and personal sampling for the lead and its compounds may be conductedusing NIOSH Methods 7082, 7105, 7300, 7505, and OSHA ID 121 and ID 125 G (see Table3.4.3.6). The most appropriate method has to be selected for the particular exposure scenario.
Approximately 50 per cent of the lead deposited in the lung is absorbed, whereas less than 10per cent of ingested lead normally gets into the systemic circulation. Dermal absorption of leadis also a significant route of exposure. Biological tests for lead exposure can be divided intotwo groups, i.e. those directly reflecting the exposure through assessment of the amount storedin blood, urine, hair, and bone, and those indicating the early biological effects of lead inrelation to exposure. These effects are shown in haemoglobin, haematocrit, stippled cells,coproporphyrin in urine, etc. In a steady-state situation, lead in blood is considered to be thebest indicator of recent exposure. It has been shown that under low exposure conditions(environmental levels) an increase of 1 µg/m3 in air leads to an increase of 1 to 2 µg/100 ml ofwhole blood. There is however not a clear correlation between air concentrations and bloodlead at higher exposure concentrations, and it is therefore difficult to assess occupationalexposures. The situation is further complicated by the fact that lead is a ubiquitous pollutant,leading also to nonoccupational exposures. As a rule, it is accepted that blood-lead levels ofnon-occupationally exposed individuals lie between 15 and 30 µg/100 ml of whole blood.

237
Levels up to 70 µg/100 ml in lead-related occupations are normally considered acceptable. However, subclinical effects may occur at levels exceeding 50 µg/100 ml of whole blood. TheWorld Health Organisation has proposed 40 µg/100 ml as the maximum tolerable lead value inblood for adult male workers, and 30 µg/100 ml for women of childbearing age (Lauwerys andHoet, 1993:86). No guideline has been proposed for biological monitoring of lead exposure inSouth Africa.
Lead in urine is often preferred to blood analysis, and reflects the amount of lead recentlyabsorbed. There is however a poor association between lead in blood and lead in urine, andblood-lead is considered the more reliable measure for routine assessment of lead exposure. Aconcentration of lead in blood of 50 µg /100 ml usually corresponds with a level of 150 µg /gcreatinine, but the correlation across a wider exposure range is poor. The level of 150 µg Pb/gcreatinine corresponds with an air concentration of 50 µg Pb/ m3 (Lauwerys and Hoet,1993:55).
Although it has been suggested that hair provide a time-integrated index of lead absorption, ithas drawn limited interest because of potential lead contamination in hair-washing procedures(Lauwerys and Hoet, 1993:86).
Various manganese oxides have been shown to be neurotoxic, and in the assessment ofexposure all forms of manganese are normally considered. Exposure may occur in thefurnace/product area as a result of high manganese levels in furnace slag and dust. Manganese levels are also high in scrubber effluents. Sampling and analytical methods toquantify airborne manganese have been listed in Table 3.4.3.6. The normal concentration ofmanganese in urine is usually less than 3 µg/l, and in whole blood and plasma less than 1µg/100 ml and 0.1 µg/100 ml, respectively. There is however no consistent relationshipbetween manganese exposure and blood levels, and it appears that measurement of urinarylevels is the preferred method for assessment. The relationship with exposure is however notthat well-defined and no biological threshold limit value has been proposed (Lauwerys andHoet, 1993: 71).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
14.4.4 Risk quantificationIn controlling exposure to metals and metal oxides in some of the materials, it is not adequateto control dust levels to 10 mg/m3, because the levels of the metals may be above theirexposure threshold concentrations at particulate levels lower than 10 mg total dust/m3.
14.5 ReferencesJohansson, S. E. E. 1994. Columbus Joint Venture. Proceedings of the XVth CMMICongress, Johannesburg, SAIMM, 2: 191 – 202.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.

238

239
15 Typical titanium dioxide production process
15.1 IntroductionThis section provides a process description and process diagram of a typical titanium dioxideproduction process. The example is a highly condensed version of a plant producing pigmentfrom a typical 85 per cent titania slag as produced by Richards Bay Minerals or NamakwaSands. The process description and flow diagram contain data on the process streams andidentify the toxic substances as well as the potential exposure points.
15.2 Process descriptionWhile sulphate-route pigment plants produce substantial amounts of wastes, with those usingilmenite being much bigger waste producers than where slag is the feedstock, they are notregarded as being hazardous to any great extent. For example, in the UK, untreated wastesfrom two plants were discharged directly into rivers in 1987. For the plant under consideration,acidic wastes are neutralised with sodium hydroxide and lime.
To put some perspective on the situation, a plant producing 50 000 t/a of final titanium dioxidepigment product was considered. Wastes arising from the feed slag will be silica (SiO2) andgypsum (CaSO4). Other metals will be present in the insoluble hydroxide form afterneutralisation. Totals in all exit streams will amount to around 5 000 t/a of iron, 780 t/a of Mn,400 t/a of Al, 150 t/a of vanadium and 40 t/a of chromium.
15.2.1 MillingTitania slag is received in bulk and stored under cover. It is conveyed to the comminutionstation where continuous air-swept ball mills yield a product of less than 40 micron, which isstored in intermediate hoppers.
The approximate analysis of the titania slag is shown in Table 15.2.1 below. Traces of uranium(1 to 4 ppm) and thorium (10 to 25 ppm) may also be present.
Table 15.2.1Milling
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Titania slag TiO2 (total)Fe (total)SiO2
Al2O3
CaOMgOV2O5
Cr2O5MnOTrace U, Th
85 - 878,31,91,40,21,10,50,11,8
TiO2
Ti2O3
FeOCaOV2O5
Cr2O5MnO
Storage/handling/milling areas
15.2.2 Digestion/production of digester residue byproductWeighed amounts of 98 to 100 per cent H2SO4 and slag are batched to lined digesters inparallel. Steam or water is added to cause a rise in temperature. At about 100 °C a violentreaction occurs with the emission of copious quantities of water vapour (with entrained acid mistetc.), SO2, SO3, and H2S.

240
The gas stream is scrubbed with sodium hydroxide in scrubbing towers to absorb SO2 and H2Sand to neutralise any acid present. The sulphur is subsequently stripped from the solution inpacked columns and passes to the “Sulphacid” process where it is converted into dilutesulphuric acid (about 20%), for re-use. Neutralised solution from the stripping towers ispumped out to sea via a pipeline. It has been assumed that there will some carry over ofdissolved metals due to the violent reaction in the digesters and these will be present in thiswaste stream as shown in the table below.
After some 8-9 hours the reaction is complete and the porous, sticky mass is leached withdilute sulphuric acid over a prolonged period to solubilise TiO2 and to dissolve TiOSO4 and themetal sulphates. The liquor is transferred to the next stage. The residue is separatelysubmitted to a digester residue-treatment process in which it is reacted with slaked lime(Ca(OH)2 ) to form a byproduct which is used in brick and clinker manufacture.
Apart from activities during normal operation, it should be noted that safety precautions/healthmonitoring procedures have to be applied to maintenance operations, one of these being leadburning which takes place during the maintenance and repair of lead-lined equipment.
Table 15.2.2Digestion
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Discharge to sea TiO2FeMnZnVCr
Cu, Pb, Ni, CdHg, As
1370140,41,60,9
Traces
Ti, Fe, Ca, Mg, V,Cr, Mn, Zn, Cu,Pb, Ni, Cd, Hg, As-as hydroxides
Pipeline discharge
Digester residue SiO2Fe2O3
MgOCaONa2OK2OV2O5TiO2
MnO
42,01,40,32,00,30,70,950,50,5
CaSO4
Ti, Fe, Mg, V, Cr,Mn as hydroxides
Byproduct storage/handling area
Lime, CaOadded as slakedlime (Ca(OH)2)
CaOMgOAl2O3
FeOMnOSiO2
Fe2O3
91,31,70,30,30,10,8
CaOMnOFeOFe2O3
Lime storage/handling area
15.2.3 Hydrolysis/leaching/washingLiquor from the digesters is transferred to hydrolysis reactors where, by means of the additionof NaOH and seed (nuclei) material, the titanium present is converted into titanium hydroxide.

241
This pulp is cooled and transferred to a re-pulp vessel where it is washed with washings fromthe post-leach wash stage.
The washed pulp is transferred to the leach section where dilute sulphuric acid and a reducingagent (possibly zinc) are used to dissolve remaining iron.
The pulp is then washed with fresh water to remove dissolved impurities and most of theexcess acid and is then filtered.
Table 15.2.3Hydrolysis/Leaching/Washing
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Filter cake afterhydrolysis/leach
Ti(OH)4
TiO(OH)2
TiOSO4
Fe, Al, Mg, Mn,Ca, Cr, V,Zn as sulphates
Some H2SO4
in solution
0,732
15
Ti(OH)4
TiO(OH)2
TiOSO4
Cr2(SO4)3FeSO4
MnSO4
ZnSO4Vanadiumsulphate
Filter cake from hydrolysis/leach
15.2.4 Production of gypsum byproductThe washings from hydrolysis and leach are reacted with lime to form a byproduct which isbasically gypsum. As much as possible of this is sold for use in cement and brick manufacture,excess being stored on a dump.
Table 15.2.4Production of Gypsum Byproduct
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
Limestone,CaCO3
CaCO3MgCO3
SiO2Other metaloxides (Al, Fe,Mn)
94,52,02,01,7
CaCO3MnOFeOFe2O3
Limestone storage/handling area

242
Stream Component
Typicalconcentrations
(as % of drysolids)
Heavy metals Exposure
GypsumByproduct Ca
MgKFeMnZnCuAlCdCNAsCrNaHgVSrSi
mg/kg100 400
1 95317
29 100933203.4
2 8230.2
< 0.330.4457114
< 0.0658476
737
CaSO4.2H2OCaSO3
Ca, Fe, Mn, Zn, Cu,Cd, As, Cr, Hg, V, ashydroxides
Gypsum byproduct storage/handling area
15.2.5 CalciningTitanium hydroxide filter cake is calcined in a rotary kiln. There is a small addition of modifiersto ensure that the desired crystal formation is obtained. Any residual sulphate in the reactionmass is driven off as SO2 or SO3. The gases pass to the “sulphacid” plant for conversion ofSO2/SO3 to dilute sulphuric acid.
Table 15.2.5Calcining
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Calcined TiO2 TiO2 approx 99% TiO2 Calcining kiln
15.2.6 Pigment finishingCalcined TiO2 is sent to the so called "white end" for production of the final pigment. Duringthis process it goes through 3 to 9 comminution steps, e.g. hammer milling, sand milling andmicronising. It is important that the end product is very fine with a closely controlled particlesize range. Depending on the end use, the TiO2 particles may be coated with a range ofoxides, e.g. SiO2, ZrO2, and Al2O3. Finally, dried pigment is bagged for sale.
Table 15.2.6Pigment Finishing
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
TiO2 product TiO2
Al2O3Amorphous silicateZrO2
80 to 99,50 to 7,00 to 11,0
0 to 1,0
TiO2ZrO2
Product storage/handling area

243
15.3 Flow diagramThe flow diagram for a typical titanium dioxide production process is shown in Figure 15.3.
15.4 Process assessment
15.4.1 Hazard identificationThe primary substance of interest in the milling process is titanium dioxide. The digestion,hydrolysis, leaching and washing steps are wet processes with insignificant potential forexposure to heavy metals. Handling of calcium oxide in the lime storage and handling areasmay be a source of exposure.
Potential exposure to lead during maintenance operations is an important factor to consider.
15.4.2 Toxicological assessmentNo data on dose-response or dose-effect relationships are available for systemic changes inhumans on exposure to titanium compounds. It has been shown in epidemiological surveys ofworkers that titanium dioxide exposure does not increase the risk of developing lung or distalcancers, or other fateal repiratory diseases (Cohen, Bowser and Costa, 1996: 253). Toxicological information on titanium and its compounds is summarised in Section 3.3.4.28.
Calcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicology of calcium oxide has been discussed in Section 3.3.4.7.
The toxicity of lead is related to interference with different enzyme systems. For this reason,almost all organ systems may be considered potential targets for lead toxicity, and a wide rangeof biological effects have been documented. Among these are effects on haem biosynthesis,the kidneys, the immune system, neurotoxic effects, reproductive effects, and alsocardiovascular, hepatic, endocrynal and gastrointestinal effects. The toxic effects of lead havebeen summarised in Table 3.3.4.13.

244
Figure 15.3 Process diagram for a typical titanium dioxide productionprocess

245
15.4.3 Exposure assessmentArea monitoring and personal sampling for titanium dioxide may be conducted using NIOSHMethods 3(S385) and 7300, and OSHA CIM. Methods for biological monitoring have not beendeveloped.
Area monitoring and personal sampling for the lead and its compounds may be conductedusing NIOSH Methods 7082, 7105, 7300, 7505, and OSHA ID 121 and ID 125 G (see Table3.4.3.6). The most appropriate method has to be selected for the particular exposure scenario.
Approximately 50 per cent of the lead deposited in the lung is absorbed, whereas less than 10per cent of ingested lead normally gets into the systemic circulation. Dermal absorption of leadis also a significant route of exposure. Biological tests for lead exposure can be divided intotwo groups, i.e. those directly reflecting the exposure through assessment of the amount storedin blood, urine, hair, and bone, and those indicating the early biological effects of lead inrelation to exposure. These effects are shown in haemoglobin, haematocrit, stippled cells,coproporphyrin in urine, etc. In a steady-state situation, lead in blood is considered to be thebest indicator of recent exposure. It has been shown that under low exposure conditions(environmental levels) an increase of 1 µg/m3 in air leads to an increase of 1 to 2 µg/100 ml ofwhole blood. There is however not a clear correlation between air concentrations and bloodlead at higher exposure concentrations, and it is therefore difficult to assess occupationalexposures. The situation is further complicated by the fact that lead is a ubiquitous pollutant,leading also to nonoccupational exposures. As a rule, it is accepted that blood-lead levels ofnon-occupationally exposed individuals lie between 15 and 30 µg/100 ml of whole blood. Levels up to 70 µg/100 ml in lead-related occupations are normally considered acceptable. However, subclinical effects may occur at levels exceeding 50 µg/100 ml of whole blood. TheWorld Health Organisation has proposed 40 µg/100 ml as the maximum tolerable lead value inblood for adult male workers, and 30 µg/100 ml for women of childbearing age (Lauwerys andHoet, 1993:86). No guideline has been proposed for biological monitoring of lead exposure inSouth Africa.
Lead in urine is often preferred to blood analysis, and reflects the amount of lead recentlyabsorbed. There is however a poor association between lead in blood and lead in urine, andblood-lead is considered the more reliable measure for routine assessment of lead exposure. Aconcentration of lead in blood of 50 µg /100 ml usually corresponds with a level of 150 µg /gcreatinine, but the correlation across a wider exposure range is poor. The level of 150 µg Pb/gcreatinine corresponds with an air concentration of 50 µg Pb/ m3 (Lauwerys and Hoet,1993:55).
Although it has been suggested that hair provide a time-integrated index of lead absorption, ithas drawn limited interest because of potential lead contamination in hair-washing procedures(Lauwerys and Hoet, 1993:86).
Calcium oxide can be determined using NIOSH Method 7021, or OSHA ID 121. BecauseCaO is of interest for its irritation effects, biological monitoring of exposure is not relevant.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
15.4.4 Risk quantificationBecause of its irritation effects, exposure to calcium oxide should be assessed againstmaximum concentration peaks rather than average values.

246
15.5 ReferencesAdams, R. 1988 Titanium and Titanium Dioxide. Financial Times Business Information, London, 243p.
Klein, J. & Rechman, H. 1995. 50 Years of the Titanium Dioxide Pigment Industry.Leverkusen: Kronos Titan GmbH, 16p.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.
Roskill, 1996. The Economics of Titanium Minerals and Pigments. London: RoskillInformation Services, 338p.

247
16 The salt-roast process for vanadium pentoxideproduction
16.1 IntroductionThe process description and flow diagram of a typical salt-roast circuit for production ofvanadium pentoxide are included in this section. The process description and flow diagramcontain data on the process streams and identify the species containing heavy metals, whichoccur on the plant, as well as the potential exposure points.
16.2 Process description
16.2.1 Crushing and millingCrushing is the first of the ore comminution steps and is followed by milling.
From field stockpiles, ore is delivered to the ore treatment plant using trucks. Here the ore isfirst crushed and screened, before being sent to an intermediate stockpile. The crushed ore isdelivered to the milling circuit where it is wet-milled in a ball or rod mill and then conveyed to themagnetic separation plant.
Table 16.2.1Crushing and milling
Stream Component Typical concentrations(as % of dry solids) Heavy metals Exposure
Crushed ore/dust V2O5Fe (total)TiO2
Cr2O3
SiO2
Al2O3
0.52 - 0.6716.5 - 183.5 - 4.50.1 - 0.365 - 754.8 - 11.2
Vanadium occurs asV3+ in solid solution inthe magnetite –ulvospinel, Fe2TiO4
where the V3+ replacesFe3+. Since the V islocked in the spinel it isnot considered asbeing toxic.TiO2
Cr2O3
Crushers/mill/loading/Storage
16.2.2 Magnetic separation and de-wateringThe crushed ore is delivered to the milling circuit where it is wet-milled in a ball or rod mill andthen sent to the magnetic separation plant. Here the vanadium-containing magnetite fraction isseparated from the silica- and alumina-rich gangue by high-intensity magnetic separation. Theconcentrate is de-watered to yield a filter cake that analyses from 1.6 to 2.4 per cent V2O5. Thenon-magnetic fraction, about 70 to 80 per cent of the mill feed, is pumped to the slimes dam,and the clear water returned to the mills.

248
Table 16.2.2Magnetic separation and de-watering
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Gangue frommagneticseparation
Mainly SiO2and Al2O3
with smallamounts of otherspecies in ore(see ore analysis)
Mainly SiO2and Al2O3
with small amounts ofother species in ore(see ore analysis)
Mainly SiO2and Al2O3
with small amountsof other species inore (see oreanalysis)
Slimes dam
Magnetiteconcentrate
Similar to oreexcept SiO2,
Al2O3 removed
Similar to ore exceptSiO2,
Al2O3 removed
Similar to ore exceptSiO2,
Al2O3 removed
Filter cake
16.2.3 RoastingOn the feed tables, sodium carbonate, sodium sulphate, or a mixture of the two is added to themilled ore before it is charged to the roasting units. The roasting units consist of coal- or gas-fired rotary kilns, with a maximum temperature of > 1000 oC. The sodium salts react with thevanadium in the magnetite to form a water-soluble sodium metavanadate during the oxidativeroast.
Table 16.2.3Roasting
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Calcine/dust Hematite, Fe2O3
Pseudobrookite,Fe2TiO5
Nepheline,NaAlSiO4
Calcium titanateCaTiO3NaVO3
66
14
10
55
Fe2O3
Fe2TiO5
CaTiO3NaVO3
Kiln area
Kiln off-gases Dust may containparticles of calcinewith composition asabove
Dust may containparticles of calcinewith composition asabove
Fe2O3
Fe2TiO5
CaTiO3NaVO3
Gas to stack
Scrubber liquor V3+ and V4+
complexesScrubber/dam
16.2.4 LeachingThe hot discharge from the kilns (calcine) is mixed with water, and transported to leach dams. During the filling of these dams, the sodium vanadate, which is soluble in water, is leached fromthe ore. The leach liquor or pregnant solution is pumped to storage tanks once a concentrationof 50 to 60 g/l V2O5 is reached. After several displacement washes, the leached calcine isremoved from the leaching dams and discarded onto the tailings dumps.

249
Table 16.2.4Leaching
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Pregnant leachliquor
High concentration of V, Na,and SO4 in solution, lowconcentration of other metalsas follows:VNaSO4
Ca, Al, Si, Ti, Cr,Fe(Al, Si inert as locked intoglassy phase)
20 g/l40 g/l60 g/l
Low ppm levels
HVO42-
Ca, Ti, Cr, Fesulphates
Leach dams,storage tanks
Spent calcine Similar to calcine but lower Vconcentration
Similar to calcine butlower Vconcentration
Fe2O3
Fe2TiO5Residual V isinsoluble , existing ina variety of formse.g. CaO.V2O5,CaTiO3
Waste dump
16.2.5 Precipitation and vanadium pentoxide productionVanadium is recovered from the leach liquor by precipitation as ammonium metavanadate(AMV) or ammonium polyvanadate (APV).
In the AMV-precipitation process, an excess of ammonium sulphate is added to a continuousflow of pregnant solution inside an air-agitated reactor. The overflow from this precipitationreactor passes to a second reactor and finally into a thickener, where the settled AMV is rakedtowards the centre discharge port and pumped into filter boxes. The barren solution is pumpedto evaporators where the solution is evaporated to produce ammonium sulphate and sodiumsulphate that is returned to the precipitation plant for re-use. After filtration and washing, theAMV is discharged from the box filters and fed to electrically heated rotary dryer de-ammoniators. During this process, the white AMV powder is converted into vanadiumpentoxide powder with the loss of water and ammonia. The vanadium pentoxide powder ismelted in a glowbar-heated furnace at 850oC and tapped onto a cooling wheel, where the meltsolidifies into a flake that is scraped off into a bucket elevator for drumming.
In the APV-precipitation process, pregnant leach liquor is pumped into a cylindrical reactorwhere sulphuric acid is added until a pH of 5.5 is reached. The required quantity of ammoniumsulphate is then added, followed by further additions of sulphuric acid to give a final pH of 2. The solution is steam-heated and maintained at temperature until the vanadium level of themother liquor has dropped to about 0.5 g/l V2O5. Once this value has been reached, thecoarse, bright-orange precipitate is pumped into box filters, filtered and washed. The APV isprocessed further to vanadium pentoxide flake via deammoniation and fusion furnaces as forthe AMV route.

250
Table 16.2.5Precipitation and V2O5 production
Stream ComponentTypical
concentrations(as % of dry solids)
Heavy metals Exposure
Barren solutions VAlCaKSiSO4
50 – 500 mg/l HVO42-
CaSO4
Filters, storage tanks,evaporators
V2O5 powder V2O5
AlFeSiSO4
99 %
TraceTraceTraceTrace
V2O5Fe
Rotary dryer-de-ammoniator
V2O5 flake V2O5
AlFeSiSO4
99 %
TraceTraceTraceTrace
V2O5Fe
Fusion furnace, coolingwheel, drumming plant
16.3 Flow diagramThe flow diagram for the vanadium pentoxide production circuit is shown in Figure 16.3.
16.4 Process assessment
16.4.1 Hazard identificationThe primary occupational hazard relating to the vanadium industry is the irritation effects ofvanadium pentoxide. Exposure of employees would occur mostly in the final product zones ofthe vanadium pentoxide production process. Filter cake, which is handled as waste, in the finalproduction stages, may contain small quantities of V2O5. In other areas the primary concern isexposure to respirable dust. It has to be noted that where feed materials are imported fromother sources, it may be necessary to monitor for other heavy metals, for example hexavalentchromium. The ore dust contains high levels of iron, and as such can not be managed asparticulates without particular toxicity.
16.4.2 Toxicological assessmentChromium is an essential element in humans. Hexavalent chromium is a human carcinogen,as outlined in the toxicological assessment for chromium (see Section 3.3.4.8). Trivalentchromium is poorly absorbed, but allergic eczematous dermatitis has been observed followingindustrial exposures.
Most of the reported clinical symptoms of vanadium exposure reflect irritation effects on therespiratory tract. There is insufficient evidence that vanadium causes generalised systemiceffects in humans, except at extremely high concentrations (WHO, 1987: 366). Thetoxicological assessment for vanadium has been summarised in Table 3.3.4.30.

251
Figure 16.3 Process diagram for the vanadium pentoxide production circuit

252
16.4.3 Exposure assessmentLauwerys and Hoet (1993:95) have summarised the available biological exposure information ofvanadium. It has been estimated that 25 per cent of soluble vanadium compounds may beabsorbed through exposure by the pulmonary route. Dermal absorption is very small. Approximately 90 per cent of circulating vanadium is associated to plasma transferrin. It isexcreted in urine with a biological half-life of 20 to 40 hours. Some excretion may also occur infeces, and there are data that suggest slow accumulation in the body in the course of chronicexposure.
Limited data are available on the relationship between vanadium in blood and urine andairborne concentration levels, and considerable variations have been reported betweenvanadium in serum, whole blood and urine. It appears that the background level in whole bloodshould lie below 0.1 µg/100 ml, and in urine it is lower than 1 µg/g creatinine. Vanadium levelsin urine are believed to be a better reflection of exposure than blood vanadium. It has beenproposed that exposure assessment is best conducted through pre- and post-shift sampling ofurine, and accumulation may be assessed through monitoring two days after cessation ofexposure. A biological threshold limit of 50 µg/g creatinine has been proposed.
Exposure to chromium can be quantified using sampling and analytical methods listed in Table3.4.3.6. Determination of chromium in urine is the preferred method for assessing exposure tohexavalent chromium. Exposure to an air concentration of 0.05 mg Cr/m3 would be reflected ina urine concentration of 30 µg Cr/g creatinine at the end of the exposure period. Exposure totrivalent chromium compounds does not correlate with levels of chromium in urine (Lauwerysand Hoet, 1993: 42).
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
16.4.4 Risk quantificationThe proposed biological threshold limit is tentative, and results of biological monitoring and thecalculated hazard quotients for air monitoring should be considered together to estimate thesignificance of exposure.

253
16.5 ReferencesGupta, C. K. & Krishnamurthy, N. 1992. Extractive Metallurgy of Vanadium, Elsevier, 689p.
Lauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Lewis Publishers, 318p.
Rohrmann, B. 1985. Vanadium in South Africa, Journal of the South African Institute forMining and Metallurgy, 85 (5): 141–150.
Slotvinskii-Sidak, N. P. 1962. Extraction of vanadium directly from iron-vanadium (titanomagnetite) concentrates. Stal 1: 7-10.
WHO 1987. Air quality standards for Europe. Geneva, World Health Organisation, p. 361-371.

254
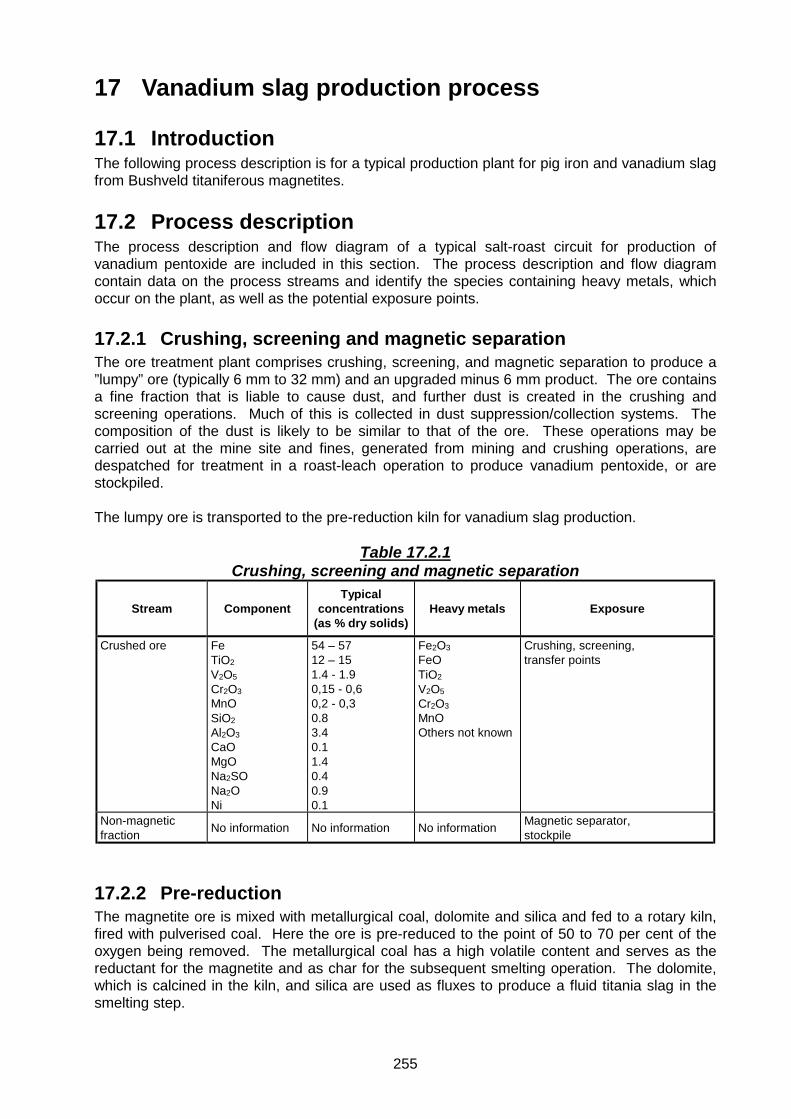
255
17 Vanadium slag production process
17.1 IntroductionThe following process description is for a typical production plant for pig iron and vanadium slagfrom Bushveld titaniferous magnetites.
17.2 Process descriptionThe process description and flow diagram of a typical salt-roast circuit for production ofvanadium pentoxide are included in this section. The process description and flow diagramcontain data on the process streams and identify the species containing heavy metals, whichoccur on the plant, as well as the potential exposure points.
17.2.1 Crushing, screening and magnetic separationThe ore treatment plant comprises crushing, screening, and magnetic separation to produce a”lumpy” ore (typically 6 mm to 32 mm) and an upgraded minus 6 mm product. The ore containsa fine fraction that is liable to cause dust, and further dust is created in the crushing andscreening operations. Much of this is collected in dust suppression/collection systems. Thecomposition of the dust is likely to be similar to that of the ore. These operations may becarried out at the mine site and fines, generated from mining and crushing operations, aredespatched for treatment in a roast-leach operation to produce vanadium pentoxide, or arestockpiled.
The lumpy ore is transported to the pre-reduction kiln for vanadium slag production.
Table 17.2.1Crushing, screening and magnetic separation
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Crushed ore FeTiO2
V2O5
Cr2O3MnOSiO2Al2O3
CaOMgONa2SONa2ONi
54 – 5712 – 151.4 - 1.90,15 - 0,60,2 - 0,30.83.40.11.40.40.90.1
Fe2O3
FeOTiO2
V2O5
Cr2O3MnOOthers not known
Crushing, screening,transfer points
Non-magneticfraction No information No information No information Magnetic separator,
stockpile
17.2.2 Pre-reductionThe magnetite ore is mixed with metallurgical coal, dolomite and silica and fed to a rotary kiln,fired with pulverised coal. Here the ore is pre-reduced to the point of 50 to 70 per cent of theoxygen being removed. The metallurgical coal has a high volatile content and serves as thereductant for the magnetite and as char for the subsequent smelting operation. The dolomite,which is calcined in the kiln, and silica are used as fluxes to produce a fluid titania slag in thesmelting step.

256
The kiln temperature is maintained at about 1 120 0C by controlling the air flow to the kiln.
Waste gas from the kiln, which contains dust, is extracted, cooled and cleaned in dust collectionsystem, e.g. an electrostatic precipitator. The dust that is collected is slurried and pumped to atailings dam.
Table 17.2.2Pre-reduction
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Pre-reduced ore Similar to ore,but Fe nowmainly reducedto FeO, alsoCaO,MgO, andSiO2
Similar to ore,some FeO, alsoCaO,MgO, andSiO2
Similar to ore, butFe now mainly asFeO
Kiln/pre-reduced ore handling
Dust from kiln Similar to pre-reduced ore
Similar to pre-reduced ore
Similar to pre-reduced ore
Kiln/Electrostatic precipitator/slimesdam
17.2.3 Electric arc smeltingThe pre-reduced magnetite from the kiln is charged hot to an electric submerged arc smeltingfurnace operating at about 1 350o C. Here the magnetite is converted to vanadium pig iron andtitania-rich slag. The pig iron is tapped into transfer ladles and taken to the shaking ladle plant.The slag is tapped into slag pots, transported to cooling beds and then stockpiled.
The furnace off-gas, which is rich in carbon monoxide (50 to 90 per cent CO, 5 to 25 per centCO2), is extracted, washed to remove particulates and pumped to a gas tank for distribution forheating purposes. The collected dust is slurried and pumped to a tailings dam.
The furnace is normally fitted with an extraction system, but stray dust and fume could escape.
Table 17.2.3Electric arc smelting
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Dust in furnaceoff-gas
Mixture of pre-reduced ore, titaniaslag, andvanadium pigiron
Mixture of pre-reduced ore,titania slag, andvanadium pigiron
As contained inpre-reduced ore,titania slag, andvanadium pigIron
Furnace/gas handling system
Titania slag TiO2SiO2
CaOMgOAl2O3FeOV2O5
S
29.62116.714.113.92.61.20,2
TiO2
CaOFeOV2O5
Furnace/Titania-rich slag stockpile

257
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Vanadium pig iron FeVTiCrMnSiNiCuSPC
94 to 951,10,210,330,140,30,10,030.10.033.0
FeVTiCrMnNiCu
Furnace/pig iron handling
17.2.4 Shaking ladles/vanadium slag upgradingIn this operation, the melt is blown with oxygen while the ladle is agitated in a speciallydesigned cradle. Scrap and mill scale are added to control the bath temperature at a maximumof 1 400 oC, and small amounts of anthracite are added to compensate for carbon losses fromthe pig iron. The vanadium transfers to the slag phase, leaving a blown metal (pig iron) productwhich can be converted to steel.
The operation is carried out under an extraction hood that extracts fume to a scrubber system. This ensures that there is virtually no escape of fume during the blowing operation. Someescape of fume, which will contain oxides of the heavy metals present, occurs during pouring ofhot metal into the shaking ladle and during transfer of the blown metal into the basic oxygenfurnace at the end of the operation. The dust that is collected is slurried and pumped to atailings dam.
Table 17.2.4Shaking ladles
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Dust and fumefrom shaking ladle
Mixture ofvanadium pigiron, pig iron andvanadium richslag
Mixture ofvanadium pig iron,pig iron andvanadium richslag
As contained invanadium pig iron,pig iron andvanadium richslag
Shaking ladle area
Pig iron FeMnVNiCrCuAlCSP
92.50.030.190.110.110.030.203.310.110.02
FeMnVNiCrCu
Shaking ladle, pig iron handling/storage

258
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Vanadium rich slag V2O5FeOSiO2
FeCr2O3
TiO2
Al2O3MnOMgOCaO
24,526171054,54432
V2O5FeOFeCr2O3
TiO2
MnOCaO(spinel – slag-metal composite)
Shaking ladleVanadium-rich slag handling/storage
17.3 Flow diagramThe flow diagram for the vanadium slag production process is shown in Figure 17.3.

259
Figure 17.3 Process diagram for the vanadium slag production process

260
17.4 Process assessment
17.4.1 Hazard identificationThe primary occupational hazards relating to vanadium slag production is the generation ofdust and exposure to constituents in the dust. During crushing, screening and magneticseparation, and in the pre-reduction step, the dust has a composition similar to the ore. Vanadium and chromium oxides are the primary substances of interest for exposure control.Table 3.4.2 shows that very low concentrations in dust may exceed threshold limits duringoccupational exposure to the dust. Chromium is likely to be in the trivalent state, which is lesshazardous than hexavalent chromium. Although effective ventilation is expected to controlhuman exposure to dust and fumes in the furnace and ladle areas, some discretion should beapplied in the assessment of potential exposure.
17.4.2 Toxicological assessmentMost of the reported clinical symptoms of vanadium exposure reflect irritation effects on therespiratory tract. There is insufficient evidence that vanadium causes generalised systemiceffects in humans, except at extremely high concentrations (WHO, 1987: 366). Thetoxicological assessment for vanadium has been summarised in Table 3.3.4.30. The toxiceffects of chromium have been listed in Table 3.3.4.8.
Chromium is an essential element in humans. Hexavalent chromium is a human carcinogen,as outlined in the toxicological assessment for chromium (see Section 3.3.4.8). Trivalentchromium is poorly absorbed, but allergic eczematous dermatitis has been observed followingindustrial exposures.
17.4.3 Exposure assessmentSampling and analytical methods for vanadium fume and in dust have been listed in Table3.4.3.6. Lauwerys and Hoet (1993:95) have summarised the available biological exposureinformation of vanadium. It has been estimated that 25 per cent of soluble vanadiumcompounds may be absorbed through exposure by the pulmonary route. Dermal absorption isvery small. Approximately 90 per cent of circulating vanadium is associated to plasmatransferrin. It is excreted in urine with a biological half-life of 20 to 40 hours. Some excretionmay also occur in feces, and there are data that suggest slow accumulation in the body in thecourse of chronic exposure.
Limited data are available on the relationship between vanadium in blood and urine andairborne concentration levels, and considerable variations have been reported betweenvanadium in serum, whole blood and urine. It appears that the background level in whole bloodshould lie below 0.1 µg/100 ml, and in urine it is lower than 1 µg/g creatinine. Vanadium levelsin urine are believed to be a better reflection of exposure than blood vanadium. It has beenproposed that exposure assessment is best conducted through pre- and post-shift sampling,and accumulation may be assessed through monitoring two days after cessation of exposure. A biological threshold limit of 50 µg/g creatinine has been proposed.
Exposure to chromium can be quantified using sampling and analytical methods listed in Table3.4.3.6. Determination of chromium in urine is the preferred method for assessing exposure tohexavalent chromium. Exposure to an air concentration of 0.05 mg Cr/m3 would be reflected ina urine concentration of 30 µg Cr/g creatinine at the end of the exposure period. Exposure totrivalent chromium compounds does not correlate with levels of chromium in urine.
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.

261
17.4.4 Risk quantificationThe proposed biological threshold limit for vanadium is tentative, and results of biologicalmonitoring and the calculated hazard quotients for air monitoring should be considered togetherto estimate the significance of exposure.
Exposure to total chromium can be assessed directly against the occupational exposureguideline. For assessment of exposure to hexavalent chromium, biological monitoring andquantification of cancer risk should be the preferred approach.
17.5 ReferencesLauwerys, R. R. & Hoet P. 1993. Industrial Chemical Exposure, Guidelines for BiologicalMonitoring. Second Edition. Boca Raton: Lewis Publishers, 318p.
Rohrmann, B. 1985. Vanadium in South Africa. Journal of the South African Institute forMining and Metallurgy, 85 (5): 141-150.
WHO 1987. Air quality standards for Europe. Geneva: World Health Organisation, p. 361-371.

262

263
18 Typical circuit for zinc recovery from concentrate
18.1 IntroductionThis section provides a process description and process diagram of a typical zinc productionfacility. The process description and process diagram contain data on the process streams andidentify the hazardous substances as well as potential exposure points.
18.2 Process descriptionThe roast-leach-electrowinning process accounts for at least 80 per cent of annual primary zincproduction. The process consists of five major steps, namely:
• Roasting of sulphide concentrates to produce acid-soluble zinc oxide• Leaching of acid soluble zinc oxide• Precipitation of dissolved iron and other impurities as hydroxides by neutralisation• Purification of solution to remove all impurities by zinc dust cementation• Recovery of zinc from purified electrolyte by electrowinning onto aluminium cathode sheets,
followed by stripping, melting
18.2.1 RoastingConcentrates containing zinc sulphide and several other impurities are roasted in air at 800 to975 oC to form acid-soluble zinc oxide, other less-soluble oxides and sulphur dioxide gas. Atypical analysis of zinc concentrate and calcine (the oxidised roaster product) is given in thefollowing table.
After cleaning, the SO2 gas is converted to liquid SO2 or sulphuric acid.
Table 18.2.1Roasting
Stream Component Typical concentrations(as % dry solids) Heavy metals Exposure
Concentrate ZnSPbSiO2
Al2O3
AgFeAsSbGeSnCdCuCoNiCaMnMgClFHgTeTh
46 – 6030 – 34
1 – 80,1 – 50,1 – 2<0,014 – 12< 0.5< 0.5< 0.5< 0.5
O,1 – 10,1 – 1,5
< 0.5< 0.5
0,1 – 10,1 – 0,30,05 – 1
< 0,1<0,1<0,1
ZnS, PbS, FeS,Fe2O3,+ Ag, As, Sb, Ge,Sn, Cd, Cu, Co, Ni,Ca, Mn, and Hg,Te, Th - mainly assulphides
CaCO3
MnCO3MnO2
MgCO3
Storage/handling/roasting area
Roaster off gas SO2,F, Cl, Hg, Te, Th
10 Traces of Hg, Te,Th - species notknown
Gas cleaning –eventually slimes dam

264
Stream Component Typical concentrations(as % dry solids) Heavy metals Exposure
Calcine/dust ZnSPbSiO2
Al2O3
AgFeAsSbGeSnCdCuCoNiCaMnMgClFHg
60 – 651 - 2
1 – 100,1 – 70,1 – 3< 0,124 – 15< 0.03< 0.03< 0,03< 0.03
< 0.1 – 0,50,1 – 2< 0.05< 0.05
0,1 – 1,5< 0,1
0,05 – 1< 0,1<0,1
<0,001
ZnO +
Pb, Ag, Fe, AsSb, Sn, Cd, Cu,Co, Ni, Ca, Mn,Hg mostly asoxides with somesulphides+ zinc ferrites(ZnO.Fe2O3)
Roasting area
18.2.2 Leaching and precipitationThe calcine is leached in a 2-stage process using sulphuric acid contained in electrolyterecycled from the electrowinning step. The first stage leach is a mildly acidic leach, (referred toas neutral leach) where approximately 80% of the zinc and most of the other trace metals aredissolved. After filtration the residue from the first stage leach is then re-leached in a secondstage leach under more aggressive conditions (higher acid concentration and highertemperature) to dissolve the remaining zinc and all the iron. This second stage leach isreferred to as the hot-acid leach (HAL).
The remaining residue from the second stage leach (hot acid leach) is referred to as Pb-Agresidue. After filtration and washing, this residue is limed and pumped onto a slimes dam.
The filtrate from the hot acid leach contains high levels of iron in the ferric state. This isprecipitated out as ferric hydroxide, which after filtration is limed and pumped onto a slimesdam. The iron residue will contain trace of other elements such as As, Sb, Ge and Sn. Theiron-free zinc sulphate filtrate is pumped back to neutral leach.
Although both the Pb-Ag and Fe residues are washed thoroughly during filtration, some solublelosses do occur and as a result traces of the various elements end up on the slimes dams.
Table 18.2.2Leaching and precipitation
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Neutral leachliquor
ZnMnMg
As, Sb, Ge, Sn, Cd,Cu, Co, Mn, Ni
140 g/l5 g/l5 g/l
ZnSO4Mn, As, Sb, Sn, Cd,Cu, Co, Ni, assulphates
Leach area

265
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
Neutral leachresidue
Zn
Pb, SiO2, Al2O3,Ag, ZnO.Fe2O3,As, Sb, Ge, Sn, Cd,Cu, Co, Mn, Ni
15% of solids ZnO + ZnO.Fe2O3
Small amounts ofPb, Ag, As, Sb, Ge,Sn, Cd, Cu, Co, Mn,Ni as sulphides
Thickener solids
Hot acid leachliquor
ZnFe
As, Sb, Ge, Sn, Cd,Cu, Co, Mn, Ni
100 g/l20 g/l
traces < 10 mg/l
ZnSO4
As, Sb, Sn, Cd, Cu,Co, Mn, Ni assulphates
Leach area
Hot acid leachresidue
Pb/Ag cake:Pb, AgZnO.Fe2O3
SiO2+As, Sb, Ge, Sn, Cd,Cu, Co, Mn, Ni assulphides
Iron cake:Fe2O3.SO3.H2O+FeO.OH
Traces of solubleZn, Ge, As, Sb, Sn,Cd, Cu, Co, Mn, Nias sulphates andhydroxides
Major portion
Traces
Major portion
Traces
Pb and Ag assulphidesZnO.Fe2O3
As, Sb, Ge, Sn, Cd,Cu, Co, Mn, Ni assulphides
Fe2O3.SO3.H2O+FeO.OH
Traces of soluble Zn,Ge, As, Sb, Sn, Cd,Cu, Co, Mn, Ni assulphates andhydroxides
Filter cake
Filter cake
18.2.3 PurificationThe filtrate from the neutral leach is pumped to a purification circuit where dissolved impuritiessuch as Cd, Cu, Co and Ni are removed from the zinc solution by zinc dust cementation. Arsenic is usually added in the purification step to catalyse the cementation of Co and Ni. Tworesidues are typically produced during purification, namely, a Cd-Zn cake and a Cu-Ni-Co-As-Zn cake. Both cakes may be stockpiled, processed, upgraded or sold.
Table 18.2.3Purification
Stream ComponentTypical
concentrations(as % dry solids)
Heavy metals Exposure
1 st stagepurificationresidue
Zn
Co, Ni, Cu, As,Zn
Majority Zn, Cu, Ni, Co, asmetals (cementedout)+ As species
Co, Cu, As, Znetc. as sulphates
Purification area
2 nd stagepurificationresidue
CdZn
30 – 60 Zn/Cd as metals(cemented out)
Purification area
Zinc dust Zn 100 Zn Zn storage/handling area
Reagent As2O3 As2O3 As2O3 Reagent storage/handling

266
18.2.3 ElectrowinningThe purified solution from the purification step is then pumped to the electrowinning circuitwhere the zinc is recovered as metal sheets on aluminium cathodes.
During electrowinning zinc sulphate is reduced to zinc metal and sulphuric acid is generated. This sulphuric acid is recycled to the leach step. The electrowinning time may vary from 24hours to 96 hours. After the desired electrowinning time has elapsed the zinc deposits arestripped as sheets from the cathodes, melted and cast into ingots. Alloying elements may beadded during the melting process to produce numerous alloys.
Table 18.2.4Electrowinning
Stream Component
Typicalconcentrationsas % dry solids
basis
Heavy metals Exposure
Zinc product Zn 99,99 Zn Cell house/Melting/casting area
Acid mist ZnSO4
MnSO4
MgSO4H2SO4
Not known ZnSO4
MnSO4
Cell house
18.2.4 Effluent treatmentA bleed is taken from the spent electrolyte to control the build up of impurities such as Mg andMn. The bleed solution is neutralised with lime and pumped onto a slimes dam. Zinc isselectively precipitated from solution as Zn(OH)2. These solids are returned to the neutralleach.
Table 18.2.5Effluent treatment
Stream Component
Typicalconcentrationsas % dry solids
basis
Heavy metals Exposure
Slimes Gypsum
+ trace amountsof heavy metals
Zn
Majority CaSO4.2H2OMn(OH)2
CuO
Traces of “toxicmetals”as hydroxides
Slimes dam
Zn(OH)2 Zn(OH)2+Mn, Mg, Ca ashydroxides+ CaSO4.2H2O
Majority
Traces
Zn(OH)2CaSO4.2H2O +Mn as hydroxides
Recycle liquor
Lime CaOMgOAl2O3
FeOMnOSiO2Fe2O3
91,31,70,30,30,10,8
CaOMnOFeOFe2O3
Lime storage/handling
Calcine See previous See previous See previous Calcine handling

267
18.3 Flow diagramThe flow diagram for a typical circuit for zinc recovery from concentrate is shown in Figure18.3..
18.4 Process assessment
18.4.1 Hazard identificationOccupational exposure assessment will be determined by the composition of the concentratefeed. Specifying the feed composition can control the presence of heavy metals, and thediscussion below does not infer that exposure would in fact occur in all zinc production facilities.In the generic example discussed here, the presence of lead with zinc in nature is reflected byits presence in the concentrate at a level of up to eight per cent. Other heavy metals areexpected to be present at low concentrations in the concentrate. In the roasting area, zincoxide may be present in the occupational environment, as well as lead as an oxide or sulphate. The purification step is a closed system, but exposure to zinc, copper, nickel and cobalt, aswell as arsenic (possibly as arsine) should be considered. In the electrowinning step zincsulphate could be carried in the acid mist, as well as manganese. The concentration ofmanganese is however unknown and it is uncertain whether it would be of any significance. Calcium oxide may be of importance in the lime storage and handling areas. Manganese andcopper may be present in dust at the slimes dams.
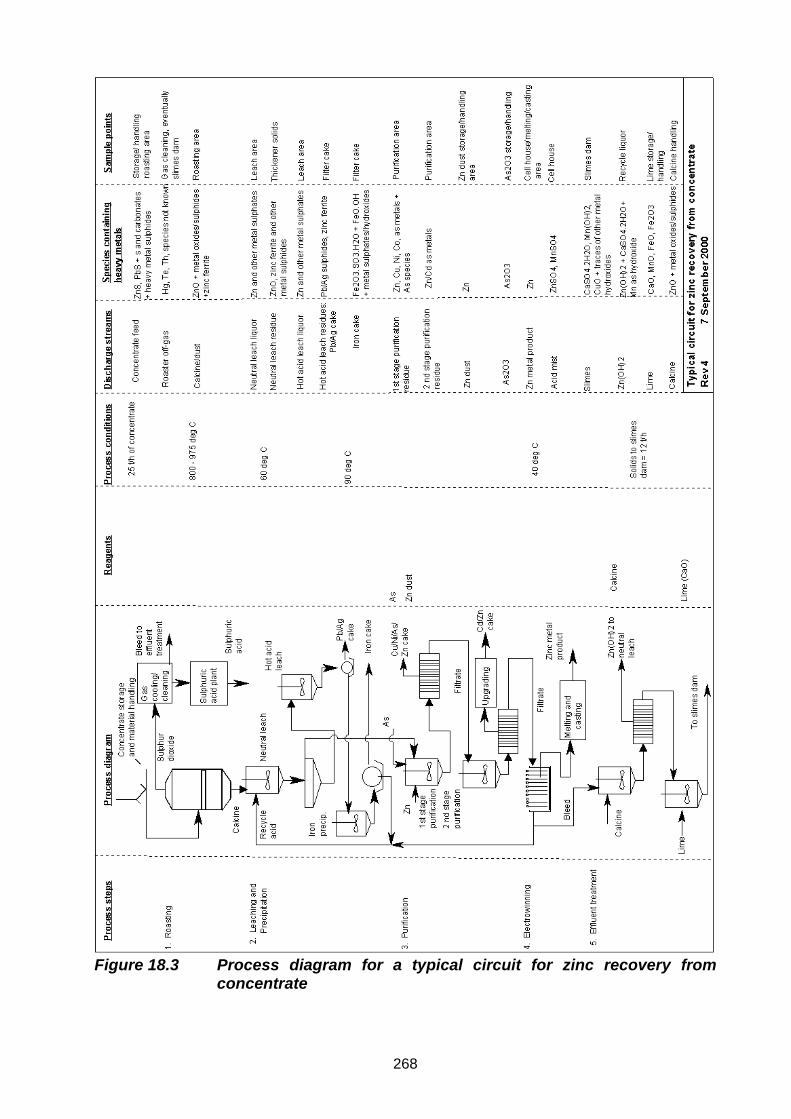
268
Figure 18.3 Process diagram for a typical circuit for zinc recovery fromconcentrate

269
18.4.2 Toxicological assessmentArsenic and its compounds have been confirmed as carcinogens.
There are no quantitative data available for absorption from copper deposited in the lungs. Atrelatively high occupational exposures, copper dust and fumes are respiratory irritants.Exposure to copper and copper oxide fumes at high concentrations has been responsible formetal fume fever. Toxic effects of copper have been documented in Table 3.3.4.10.
The toxicity of lead has a relationship with the interference with different enzyme systems. Forthis reason, almost all organ systems may be considered potential targets for lead toxicity, anda wide range of biological effects have been documented. Among these are effects on haembiosynthesis, the kidneys, the immune system, neurotoxic effects, reproductive effects, andalso cardiovascular, hepatic, endocrynal and gastrointestinal effects. The toxic effects of leadhave been summarised in Table 3.3.4.13.
Manganese compounds in various forms are considered to be neurotoxic, with subclinicaleffects occurring at low exposure levels. Section 3.3.4.14 presents an overview of thetoxicology of manganese.
Calcium in itself is not toxic to humans, but in the form of calcium oxide it acts as an irritant.The toxicology of calcium oxide has been discussed in Section 3.3.4.7.
Occupational exposure to cobalt metal, dust and fume is associated mainly with pulmonaryfibrosis and sensitisation. The toxicicity of cobalt and its compounds has been discussed inSection 3.3.4.9.
The most widely known systemic effect resulting from acute inhalation of freshly formed zincoxide fumes is a disease called metal fume fever. The toxicity of zinc has been discussed inSection 3.3.4.32.
18.4.3 Exposure assessmentArea monitoring and personal sampling for arsenic and its compounds may be conductedusing NIOSH Methods 7300, 7900 and 7901, and OSHA ID 105 and OSHA CIM. NIOSHMethod 7900 is valid only for particulate-associated inorganic arsenic compounds. The mostappropriate method for the exposure scenerio has to be selected.
Mean serum and blood levels of arsenic vary greatly depending on the level of seafood contentin the diet. Therefore, when employees have not been instructed to refrain from eating fish orshellfish for two to three days before biological monitoring, high levels of arsenic may be foundthat might not be associated with occupational exposure.
In the past, biological monitoring for assessment of occupational exposure was conducted bymeasuring the total amount of arsenic in urine at the end of a shift. It is however now wellestablished that inorganic arsenic, monomethylarsonic acid, and cacodylic acid in urine is themethod of choice. Monitoring of employees exposed to inorganic arsenic using this method isnot influenced by organoarsenicals from marine origin.
Some controversial results may be obtained in the correlation between air-concentrationexposure assessment and biological monitoring. It has been established that backgroundlevels of the sum of the three metabolites of arsenic (inorganic arsenic, monomethylarsonicacid, and cacodylic acid) in urine vary between 10 µg/l and 50 µg/l. It appears that the bestrelationship for occupational exposure at air concentrations between 50 and 200 µg As/m3

270
would lead to post-shift concentrations of the total metabolites between 54 and 88 µg/gcreatinine (Lauwerys and Hoet, 1993: 25).
Area monitoring and personal sampling for the lead and its compounds may be conductedusing NIOSH Methods 7082, 7105, 7300, 7505, and OSHA ID 121 and ID 125 G (see Table3.4.3.6). The most appropriate method has to be selected for the particular exposure scenario.
Approximately 50 per cent of the lead deposited in the lung is absorbed, whereas less than 10per cent of ingested lead normally gets into the systemic circulation. Dermal absorption of leadis also a significant route of exposure. Biological tests for lead exposure can be divided intotwo groups, i.e. those directly reflecting the exposure through assessment of the amount storedin blood, urine, hair, and bone, and those indicating the early biological effects of lead inrelation to exposure. These effects are shown in haemoglobin, haematocrit, stippled cells,coproporphyrin in urine, etc. In a steady-state situation, lead in blood is considered to be thebest indicator of recent exposure. It has been shown that under low exposure conditions(environmental levels) an increase of 1 µg/m3 in air leads to an increase of 1 to 2 µg/100 ml ofwhole blood. There is however not a clear correlation between air concentrations and bloodlead at higher exposure concentrations, and it is therefore difficult to assess occupationalexposures. The situation is further complicated by the fact that lead is a ubiquitous pollutant,leading also to nonoccupational exposures. As a rule, it is accepted that blood-lead levels ofnon-occupationally exposed individuals lie between 15 and 30 µg/100 ml of whole blood. Levels up to 70 µg/100 ml in lead-related occupations are normally considered acceptable. However, subclinical effects may occur at levels exceeding 50 µg/100 ml of whole blood. TheWorld Health Organisation has proposed 40 µg/100 ml as the maximum tolerable lead value inblood for adult male workers, and 30 µg/100 ml for women of childbearing age (Lauwerys andHoet, 1993:86). No guideline has been proposed for biological monitoring of lead exposure inSouth Africa.
Lead in urine is often preferred to blood analysis, and reflects the amount of lead recentlyabsorbed. There is however a poor association between lead in blood and lead in urine, andblood-lead is considered the more reliable measure for routine assessment of lead exposure. Aconcentration of lead in blood of 50 µg /100 ml usually corresponds with a level of 150 µg /gcreatinine, but the correlation across a wider exposure range is poor. The level of 150 µg Pb/gcreatinine corresponds with an air concentration of 50 µg Pb/ m3.
Although it has been suggested that hair provide a time-integrated index of lead absorption, ithas drawn limited interest because of potential lead contamination in hair-washing procedures(Lauwerys and Hoet, 1993:86).
The normal concentration of manganese in urine is usually less than 3 µg/l, and in whole bloodand plasma less than 1 µg/100 ml and 0.1 µg/100 ml, respectively. There is however noconsistent relationship between manganese exposure and blood levels, and it appears thatmeasurement of urinary levels is the preferred method for assessment. The relationship withexposure is however not that well-defined, and no biological threshold limit value has beenproposed (Lauwerys and Hoet, 1993: 71).
Table 3.4.2.6 lists sampling and analytical methods for zinc oxide. Zinc is an essential elementand is present in abundance in various parts of the human body. Biological monitoring wouldtherefore not provide useful information for exposure assessment.The levels of zinc in healthy,nonexposed individuals in serum and plasma are in the order of 0.1 mg/100 ml. Urinaryexcretion is in the range of 0.1 to 1.2 mg over a period of 24 hours. Zinc in blood (whole blood,plasma and serum) and urine have been used as biological indicators of exposure, but nocorrelation has been established between these values and the levels of exposure, and nobiological threshold has been set. In general, after exposure the levels in blood and urine aresignificantly higher than the controls.

271
Section 3.4.4 provides an overview of medical evaluation procedures that are relevant forexposure assessment and interpretation of health effects.
18.4.4 Risk quantificationIn controlling exposure to lead at the concentrate storage and handling steps it is not adequateto control dust levels to 10 mg/m3, because the level of lead may be above its occupationalexposure limit at particulate levels lower than the 10 mg total dust/m3 threshold.
Because of its irritation effects, exposure to calcium oxide should be assessed againstmaximum concentration peaks rather than average values.
For exposure to zinc oxide, the concentration at which metal fume fever would develop, is notentirely certain, but it has been estimated that symptoms are unlikely to develop at airconcentrations below 15 mg/m3 (Elinder & Piscator, 1979: 682). The ACGIH guidelines of 5mg/m3 for zinc oxide fume and 10 mg/m3 for zinc oxide dust therefore provide adequatemargins of safety. It is recommended that exposure to zinc oxide, as well as for cobalt andcopper, be assessed against maximum concentration peaks rather than average values. Thisis because the manifestation of irritation effects is more concentration dependent than timedependent.
Cancer risks relating to exposure to arsenic and its compounds can be quantified throughinterpretation of exposure data and the respective dose-response information.
18.5 ReferencesKirk-Othmer, Encyclopaedia of Chemical Technology. Zinc and zinc alloys. Fourth EditionVolume 25 P 789 – 835.
Van Niekerk, C. J. & Begley, C. C. 1991. Zinc in South Africa. Journal of the South AfricanInstitute for Mining and Metallurgy, 91 (7): 233-248.


















